-
7/29/2019 Late pregnancy bleeding.pptx
1/28
LATE-PREGNANCY BLEEDING
-
7/29/2019 Late pregnancy bleeding.pptx
2/28
ETIOLOGY
The most common cause of late-pregnancy bleeding is aproblem
with the PLACENTA : Placenta Praevia
Abruptio Placentae Vasa Praevia
Less common causes of late-pregnancy bleeding include : Uterine
Rupture
Injuries or lesions of the CERVIX and VAGINA,
Polyps, cancer, and Varicose
Inherited bleeding problems, such as : HEMOPHILIA, are very
rare, occurring in 1 in 10,000 women.
-
7/29/2019 Late pregnancy bleeding.pptx
3/28
PLACENTA PRAEVIA The placenta, can PARTIALLY or COMPLETELYcover
the
cervical opening
Late in pregnancy called the cervix, THINS ANDDILATES (widens)
in preparation for labor, some blood
vessels of the placenta stretch and rupture. This causes about
20% OF THIRD-TRIMESTER
BLEEDING and happens in about 1 in 200 pregnancies.
Risk factors for placenta previa include these
conditions: Multiple pregnancies
Prior placenta previa
Prior Cesarean delivery
-
7/29/2019 Late pregnancy bleeding.pptx
4/28
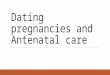
CLASSIFICATION
COMPLETE PLACENTA PREVIArefers to the situation in which the
placentacompletely covers the opening from the womb to the
cervix.
PARTIAL PLACENTA PREVIArefers to the placenta that partially
covers thecervical opening (since the cervical opening is not
dilated until time fordelivery approaches, this type of placenta
previa occurs after the cervix
has begin to dilate). MARGINAL PLACENTA PREVIA refers to a
placenta that is located adjacent
to, but not covering, the cervical opening.
The term LOW-LYING PLACENTA or LOW PLACENTAhas been used to
referboth to placenta previa and marginal placenta previa.
The terms ANTERIOR PLACENTA PREVIA and POSTERIOR PLACENTA
PREVIAare sometimes used after ULTRASOUND EXAMINATION to further
define theexact position of the placenta within the uterine
cavity.
-
7/29/2019 Late pregnancy bleeding.pptx
5/28
PLACENTA
PREVIA
-
7/29/2019 Late pregnancy bleeding.pptx
6/28
PLACENTA PREVIA SYMPTOMS
VAGINAL BLEEDING after the 20th week of gestation is the
primary
symptom of placenta previa. Although the bleeding is typically
PAINLESS and
Recurrent and the more intense
Can be associated with other complications of pregnancy
including:
PLACENTA ACCRETA occurs when the placental tissues grows too
deeplyinto the womb, attaching to the muscle layer,
Can cause LIFE-THREATENING BLEEDING and commonly requires
HISTERECTOMY.
Placenta accrete occurs in 5% to 10% of women with placenta
previa.
PRETERM PREMATURE RUPTURE OF THE MEMBRANES (PPROM)
Other abnormalities of the placenta or umbilical cord
BREECH or ABNORMAL PRESENTATION OF THE FETUS.
a REDUCTION IN FETAL GROWTH associated with placenta previa.
-
7/29/2019 Late pregnancy bleeding.pptx
7/28
-
7/29/2019 Late pregnancy bleeding.pptx
8/28
PLACENTAL ABRUPTION
A normal placenta separates from the wall of
the uterus prematurely and blood collects
between the placenta and the uterus. Such separation occurs in 1
in 200 of all
pregnancies.
The cause is unknown.
-
7/29/2019 Late pregnancy bleeding.pptx
9/28
CLASSIFICATION OF PLACENTAL ABRUPTION
Classification of placental abruption is based on :
EXTENT OF SEPARATION (ie, partial vs complete) and
LOCATION OF SEPARATION (ie, marginal vs central).
Clinical classification is as follows: Class 0 -
Asymptomatic
Class 1 - MILD (represents approximately 48% of all cases)
Class 2 - MODERATE (represents approximately 27% of all
cases) Class 3 - SEVERE (represents approximately 24% of all
cases)
-
7/29/2019 Late pregnancy bleeding.pptx
10/28
DIFFERENTIAL DIAGNOSIS
ABDOMINAL TRAUMA
ACUTE APPENDICITIS
DISSEMINATED INTRAVASCULAR
COAGULATION
TORSION OVARIAN CYST
PLACENTA PREVIA
ECTOPIC PREGNANCY
-
7/29/2019 Late pregnancy bleeding.pptx
11/28
A DIAGNOSIS OF CLASS 0 IS MADERETROSPECTIVELY BY FINDING AN:
ORGANIZED BLOOD CLOT OR A
DEPRESSED AREA
ON A DELIVERED PLACENTA.
-
7/29/2019 Late pregnancy bleeding.pptx
12/28
CLASS 1 : MILD
CHARACTERISTICS
1. No vaginal bleeding to mild vaginal bleeding
2. Slightly tender uterus
3. Normal maternal BP and heart rate
4. No coagulopathy
5. No fetal distress
-
7/29/2019 Late pregnancy bleeding.pptx
13/28
CLASS 2 : MODERATE
CHARACTERISTICS
1. No vaginal bleeding to moderate vaginal
bleeding2. Moderate to severe uterine tenderness with
possible tetanic contractions
3. Maternal tachycardia with orthostatic changes in
BP and heart rate
4. Fetal distress
5. Hypofibrinogenemia (ie, 50-250 mg/dL)
-
7/29/2019 Late pregnancy bleeding.pptx
14/28
CLASS 3 : SEVERE
CHARACTERISTICS
No vaginal bleeding to heavy vaginal bleeding
Very painful tetanic uterus
Maternal shock
Hypofibrinogenemia (ie, < 150 mg/dL)
Coagulopathy
Fetal death
-
7/29/2019 Late pregnancy bleeding.pptx
15/28
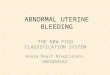
A. CONCEALED BLEEDING B. REVEALED BLEEDING C.MIXED BLEEEDING
-
7/29/2019 Late pregnancy bleeding.pptx
16/28
COMPLICATION
Potential MATERNAL COMPLICATIONS include thefollowing:
1. Hemorrhagic shock
2. Coagulopathy/disseminated intravascularcoagulation (DIC)
3. Uterine rupture
4. Renal failure5. Ischemic necrosis of distal organs (eg,
hepatic,
adrenal, pituitary)
-
7/29/2019 Late pregnancy bleeding.pptx
17/28
COMPLICATION
Potential FETAL COMPLICATIONS include the
following:
1. Hypoxia
2. Anemia
3. Growth retardation
4. CNS anomalies5. Fetal death
-
7/29/2019 Late pregnancy bleeding.pptx
18/28
LAB STUDIES IN
ABRUPTIO PLACENTAE
Hemoglobin
Hematocrit
Platelets Prothrombin time/activated partial
thromboplastin time
Fibrinogen Fibrin/fibrinogen degradation products
Blood type
-
7/29/2019 Late pregnancy bleeding.pptx
19/28
ULTRASONOGRAPHY and MRI
Ultrasonography helps to determine the location of the placenta
inorder to EXCLUDE PLACENTA PREVIA.
Ultrasonography is NOT VERY USEFUL in diagnosing
placentalabruption (and normal ultrasonographic findings do not
exclude the
condition).[4]
RETROPLACENTAL HEMATOMA may be recognized in 2-25% of
allabruptions.
This recognition depends on the degree of hematoma and on
theoperator's skill level.
MRI is DIAGNOSTICALLY EFFECTIVE and can ACCURATELY
depictplacental abruption. Consider using MRI in cases where
ultrasonography findings in the
presence of late pregnancy bleeding are negative, but
positivediagnosis of abruption would change patient
management.[7]
-
7/29/2019 Late pregnancy bleeding.pptx
20/28
MANAGEMENT
Initial Management of Abruptio Placentae
1. Begin continuous external fetal monitoring for thefetal heart
rate and contractions.
2. Obtain intravenous access using 2 large-boreintravenous
lines.
3. Institute crystalloid fluid resuscitation for the
patient.
4. Type and crossmatch blood.
5. Begin a transfusion if the patient is hemodynamicallyunstable
after fluid resuscitation.
6. Correct coagulopathy, if present.
-
7/29/2019 Late pregnancy bleeding.pptx
21/28
VAGINAL DELIVERY
This is the preferred method of delivery for afetus that has
DIED secondary to placentalabruption.
The ability of the patient to undergo vaginaldelivery depends on
her remainingHEMODYNAMICALLY STABLE.
Delivery is USUALLY RAPID in these patientssecondary to
increased uterine tone andcontractions.
-
7/29/2019 Late pregnancy bleeding.pptx
22/28
CESAREAN DELIVERY
Is often necessary for fetal and maternal stabilization.
While cesarean delivery facilitates rapid delivery and direct
access to the
uterus and its vasculature, it can be complicated by the
patient's coagulation
status.
Because of this, a vertical skin incision, which has been
associated with less blood loss, is
often used when the patient appears to have DIC.
The type of uterine incision is dictated by the GESTATIONAL AGE
of the fetus, with a vertical
or classic uterine incision often being necessary in the preterm
patient.
If hemorrhage cannot be controlled after delivery, a
CESAREAN
HYSTERECTOMY may be required to save the patient's life.
Before proceeding to hysterectomy, other procedures, including
correction of coagulopathy,
ligation of the uterine artery,
administration of uterotonics (if atony is present),
packing of the uterus, and
other techniques to control hemorrhage,
may be attempted.
-
7/29/2019 Late pregnancy bleeding.pptx
23/28
UTERINE RUPTURE
An abnormal splitting open of the uterus, causing the baby to be
partially
or completely expelled into the abdomen.
About 40% of women who have uterine rupture had prior surgery on
their
uterus, including Cesarean delivery.
The rupture may occur before or during labor or at the time of
delivery. Other risk factors for uterine rupture are these
conditions:
More than four pregnancies (MULTIPARITY)
Trauma
Excessive use of OXYTOCIN (Pitocin), a medicine that helps
strengthen
contractions A baby in any position other than head down
Having the baby's shoulder get caught on the pubic bone during
labor
Certain types of forceps deliveries
-
7/29/2019 Late pregnancy bleeding.pptx
24/28
FETAL VESSEL RUPTURE
Occurs in about 1 of every 1,000 pregnancies.
The baby's blood vessels from the umbilical
cord may attach to the membranes instead ofthe placenta.
The baby's blood vessels pass over the
entrance to the birth canal. This is called VASA PREVIA and
occurs in 1 in
5,000 pregnancies
-
7/29/2019 Late pregnancy bleeding.pptx
25/28
PLACENTA BILOBATA
-
7/29/2019 Late pregnancy bleeding.pptx
26/28
PLACENTA SUCCENTERIATA
-
7/29/2019 Late pregnancy bleeding.pptx
27/28
DIAGNOSIS
The classic triad of the vasa praevia is:
Membrane rupture,
Painless vaginal bleeding and
Fetal bradycardia. This is rarely confirmed before delivery but
may be suspected when
antenatal sono-gram with color-flow Doppler reveals a
vesselcrossing the membranes over the internal cervical
os.[2][3]
The diagnosis is usually confirmed after delivery on examination
ofthe placenta and fetal membranes
MOST OFTEN THE FETUS IS ALREADY DEAD when the diagnosis ismade;
because the blood loss (say 300ml) constitutes a major bulkof blood
volume of the fetus (80-100ml/kg i.e. 300ml approx for a3kg
fetus)[citation needed].
http://en.wikipedia.org/wiki/Vasa_praeviahttp://en.wikipedia.org/wiki/Vasa_praeviahttp://en.wikipedia.org/wiki/Wikipedia:Citation_neededhttp://en.wikipedia.org/wiki/Wikipedia:Citation_neededhttp://en.wikipedia.org/wiki/Wikipedia:Citation_neededhttp://en.wikipedia.org/wiki/Vasa_praevia
-
7/29/2019 Late pregnancy bleeding.pptx
28/28
THANK YOU
dr.Bambang Widjanarko, Sp OGDept.Obstetri Gynecology
School of Medicine & Health
Muhammdiyah University of Jakarta