Embed Size (px)
Citation preview

Late Coil Migration Due to Thrombolysis AfterSuccessful Implantation of a Coil for
Persistent Ductus Arteriosus
Ta-Cheng Huang, MD, Kai-Sheng Hsieh,* MD, and Cheng-Liang Lee, MD
Transcatheter coil occlusion of persistent ductus arteriosus (PDA) is now a widelyaccepted treatment for PDA. However, late complication might occur due to thrombolytictreatment during the interventional period. We discuss a case with late coil migration dueto thrombolysis after successful implantation of a coil. It should be emphasized that earlythrombus formation is important for successful closure of PDA shunt using coil. Cathet.Cardiovasc. Intervent. 50:334–336, 2000. © 2000 Wiley-Liss, Inc.
Key words: persistent ductus arteriosus; interventional catheterization
INTRODUCTION
Transcatheter occlusion of persistent ductus arteri-osus (PDA) has become a widely used and effectivemethod recently [1,2]. The results of coil implantationto close the PDA shunt have been encouraging [3].However, there are some serious complications suchas coil migration into the pulmonary or systemic ar-teries and hemolysis [4]. We report here a case of latecoil migration 1 week after successful implantation ofthe coil and discuss possible etiology and preventionof this complication.
CASE REPORT
A 10-month-old female infant was admitted to ourhospital for coil implantation of PDA. Progressivedyspnea and poor oral feeding developed, which werepoorly controlled by conventional medical therapy.Cardiac auscultation revealed a Gr 4/6 continuousmurmur over left infraclavicular area. She was sched-uled for coil implantation to occlude the PDA shunt atthis admission. Diagnostic catheterization and angiog-raphy were performed before coil implantation. Shehas received 50-units/Kg heparin given by intravenousroute during catheterization study. Hemodynamicstudy revealed that pulmonary artery pressure was39/20 mm Hg and Qp/Qs was 2.0. Aortogram revealeda elongated, conical type of ductus (type E) [5], withnarrowest width of 4.5 mm on the lateral projection.We used a 0.0520 coil with 10-mm diameter and 13-cmlength (Cook, Bloomington, TX) to occlude the duc-tus. After the aortogram, a 6 Fr delivery catheter(Judkins coronary catheter, right) was advanced fromthe descending aorta, across the ductus and into the
pulmonary trunk. The catheter was then exchanged forthe 7 Fr multipurpose angiographic catheter (Cook)designed for 0.0520 coil delivery. The coil was pushedout and positioned so that the first loop was on thepulmonary side, and three loops were in the aorticampulla. Aortogram was repeated 10 min after coilimplantation and showed a trivial leak from the duc-tus. Due to our experience of coil implantation, thetrivial residual shunt often closed spontaneously dur-ing follow-up (Fig. 1). The angiographic catheter wasthen withdrawn and the patient was allowed to recoverin the pediatric ward. After coil implantation, cardiacauscultation revealed a Gr 1/6 systolic ejection mur-mur over left upper sternal border. Follow-up echo-cardiogram next day revealed a trivial residual PDAshunt and coil in situ. Nonetheless, the infant wasfound to have poor pulsation of the pedis dorsalisartery 6 hr after removal of the 7 Fr sheath. Soon afterwe found the femoral artery occluded, hourly uroki-nase infusion (1,500 units/Kg) was started to preventfurther thrombosis of the right femoral artery. Unfor-tunately, after 4 days of infusion, incidental removalof the clot by family caused a hematoma to developover the right inguinal area. Urokinase was discontin-ued with supportive care. However, the patient wasirritably crying due to the hematoma. Two days later,
Department of Pediatrics, Veterans General Hospital-Kaohsi-ung, Kaohsiung, Taiwan
*Correspondence to: Dr. Kai-Sheng Hsieh, Department of Pediatrics,Veterans General Hospital-Kaohsiung, No. 386, Ta-Chung First Road,Kaohsiung, Taiwan. E-mail: [email protected]
Received 7 September 1999; Revision accepted 16 January 2000
Catheterization and Cardiovascular Interventions 50:334–336 (2000)
© 2000 Wiley-Liss, Inc.

the heart murmur became Gr 4/6 continuous murmur,which is the same characteristic murmur mentionedbefore coil implanted and repeated echocardiogramshowed reopening of the ductus. Chest roengenogramconfirmed that the coil has migrated to the proximalleft pulmonary artery (Fig. 2). Because of the family’spreference, she was referred for surgical removal ofthe coil and ligation of the PDA shunt. The postoper-ative course was uneventful and there were no PDAshunt and no pulmonary artery stenosis during follow-up.
DISCUSSION
Reopening of PDA after successful coil occlusion hasbeen reported by Daniels et al. [6], which concluded thatshort PDA length and type B PDA were associated withreopening. However, no late migration of coil has beenreported. Our case demonstrates that despite initiallysuccessful coil implantation for PDA, late migrationcould occur. There is little information regarding latemigration after coil implantation for PDA, although mal-position of coil immediately after coil delivery was notunusual. The malpositioned coil could be retrieved bysnare or forceps methods during catheterization.
There are several factors that determine a successfulcoil closure for PDA. Owada et al. [7] had discussedthat PDA size, PDA shape, and the degree of left-to-right shunt may influence the results of coil occlusionfor PDA. Shim et al. [3] also discussed that the dy-namic changes in thrombus formation may be involvedin the process of successful closure of PDA. In thiscase, our patient had received thrombolytic agent thatprevents thrombus formation of the PDA shunt aftercoil implantation. In addition, the pain at the right
inguinal hematoma could elevate the systemic pres-sure that results in significant increase of left-to-rightshunt. Because the thrombolytic dissolved the clot,late migration has occurred secondary to a reduction ofoccludable PDA surface area in contact with the coil.With the resolution ofthrombus, high-pressure jet be-tween aorta and pulmonary artery could result in increasingmobility of the coil, which causes implantation failure de-spite early successful result.
To avoid this complication, we now use the trans-venous antegrade method for delivery of 0.0520 coil toavoid complication of arterial thombosis, thus reducingthe risk of using thrombolytic agents. On the other hand,with the balloon occlusion technique reported by Davli etal. [8], we hope it may promote thrombosis within thePDA and help in eliminating the shunt early in the courseof coil implantation. Hopefully, this could reduce the riskof coil migration. Furthermore, future improvement ofcoil design and deploying technique to ensure immediate,complete closure could reduce the embolization rate as-sociated with large left-to-right shunt.
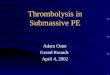
Fig. 1. Lateral view of descending aorta angiogram. Coil wasimplanted in PDA with trivial left-to-right shunt.
Fig. 2. Posterior-anterior view of CXR revealed coil migrationto proximal left pulmonary artery.
Late Migration After Occlusion of PDA Coil 335

REFERENCES
1. Hijazi ZM, Lloyd TR, Beekman RH, Geggel RL. Transcatheterclosure with single or multiple Gianturco coils of patent ductusarteriosus in infants weighing# 8 Kg: retrograde versus antegradeapproach. Am Heart J 1996;132:827–835.
2. Rothman A, Lucas VW, Sklansky MS, Cocalis MW, Kashani IA.Percutaneous coil occlusion of patent ductus arteriosus. J Pediatr1997;130:447–454.
3. Shim D, Fedderly RT, Beekman RH III, Ludomirsky A, YoungML, Schork MA, Lloyd TR. Follow-up after coil occlusion ofpatent ductus arteriosus. J Am Coll Cardiol 1996;8:207–211.
4. Henry G, Danilowicz D, Verma R. Severe hemolysis followinngpartial coil occlusion of patent ductus arteriosus. Cathet Cardio-vasc Diagn 1996;39:410–412.
5. Krichenko A, Benson LN, Burrows P, Moes CAF, McLaughlin P,Freedom RM. Angiographic classification of the isolated, persis-tently patent ductus arteriosus and implications for percutaneouscatheter occlusion. Am J Cardiol 1989;63:877–880.
6. Daniels CJ, Cassidy SC, Teske DW, Wheller JJ, Allen HD.Reopening after successful coil occlusion for patent ductus arte-riosus. J Am Coll Cardiol 1998;31:444–450.
7. Owada CY, Teitel DF, Moore P. Evaluation of Gianturco coils forclosure of large ($ 3.5 mm) patent ductus arteriosus. J Am CollCardiol 1997;30:1856–1862.
8. Dalvi B, Goyal V, Narula D, Ramakanthan R, Kulkari H. Newtechnique using temporary balloon occlusion for transcatheterclosure of patent ductus arteriosus with Gianturco coils. CathetCardiovasc Diagn 1997;41:62–70.
336 Huang et al.