Upload
soumen
View
267
Download
5
Embed Size (px)
Citation preview
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
1/573
LASERS in Dermatological Practice
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
2/573
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
3/573
LASERS in Dermatological Practice
Editors
Kabir Sardana MD DNB MNAMS
ProfessorDepartment of Dermatology and SD
Maulana Azad Medical CollegeNew Delhi, India
Vijay K Garg MD MNAMS
Director–Professor and HeadDepartment of Dermatology and SD
Maulana Azad Medical CollegeNew Delhi, India
Forewords
Ganesh S Pai
B Krishna Rau
JAYPEE BROTHERS MEDICAL PUBLISHERS (P) LTD
New Delhi • London • Philadelphia • Panama
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
4/573
Jaypee Brothers Medical Publishers (P) Ltd
Headquarters
Jaypee Brothers Medical Publishers (P) Ltd4838/24, Ansari Road, Daryaganj
New Delhi 110 002, India
Phone: +91-11-43574357
Fax: +91-11-43574314
Email: [email protected]
Overseas Ofces
J.P. Medical Ltd
83 Victoria Street, London
SW1H 0HW (UK)
Phone: +44-2031708910
Fax: +44 (0)20 3008 6180
Email: [email protected]
Jaypee Medical Inc.
The Bourse
111 South Independence Mall East
Suite 835, Philadelphia, PA 19106, USA
Phone: +1 267-519-9789
Email: [email protected]
Jaypee-Highlights Medical Publishers Inc
City of Knowledge, Bld. 237, Clayton
Panama City, Panama
Phone: +1 507-301-0496
Fax: +1 507-301-0499
Email: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd
17/1-B Babar Road, Block-B, Shaymali
Mohammadpur, Dhaka-1207
Bangladesh
Mobile: +08801912003485
Email: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd
Bhotahity, Kathmandu
Nepal
Phone: +977-9741283608Email: [email protected]
Website: www.jaypeebrothers.com
Website: www.jaypeedigital.com
© 2014, Jaypee Brothers Medical Publishers
The views and opinions expressed in this book are solely those of the original contributor(s)/author(s) and
do not necessarily represent those of editor(s) of the book.
All rights reserved. No part of this publication may be reproduced, stored or transmitted in any form or by
any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission in
writing of the publishers. All brand names and product names used in this book are trade names, service marks, trademarks or
registered trademarks of their respective owners. The publisher is not associated with any product or
vendor mentioned in this book.
Medical knowledge and practice change constantly. This book is designed to provide accurate,
authoritative information about the subject matter in question. However, readers are advised to check the
most current information available on procedures included and check information from the manufacturer
of each product to be administered, to verify the recommended dose, formula, method and duration of
administration, adverse effects and contraindications. It is the responsibility of the practitioner to take all
appropriate safety precautions. Neither the publisher nor the author(s)/editor(s) assume any liability for
any injury and/or damage to persons or property arising from or related to use of material in this book.
This book is sold on the understanding that the publisher is not engaged in providing professional medical
services. If such advice or services are required, the services of a competent medical professional should
be sought.Every effort has been made where necessary to contact holders of copyright to obtain permission to
reproduce copyright material. If any have been inadvertently overlooked, the publisher will be pleased to
make the necessary arrangements at the frst opportunity.
Inquiries for bulk sales may be solicited at: [email protected]
Lasers in Dermatological Practice
First Edition: 2014
ISBN 978-93-5152-300-0
Printed at
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
5/573
Dedicated to
My colleagues, friends and foes, the last of which goad us to better ourselves
constantly……
My wife Dr Supriya, who helps me to keep the balance between family and
academicsMy daughter Zoya, who is the ‘zing’ in my life
My parents, Mrs Amba Sardana and Major General Sardana who have
instilled discipline in my life
and
Lastly, the Department where over the years we have honed the skills in laser
intervention
My family and friends
My wife Mrs Manju Garg, who has stood by me through times of strife
My son Devansh, who is pursuing his MBBS
and
My daughter Dr Ekta, who is a dentist
—Kabir Sardana
—Vijay K Garg
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
6/573
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
7/573
Anil Aggrawal MD Forensic Medicine (AIIMS)
Director-Professor
Forensic Medicine
Maulana Azad Medical College
New Delhi, India
Anil Ganjoo MBBS MD
Senior Consultant Dermatologist andHead of Dermatology
Sunderlal Jain Hospital
Saroj Hospital and INMAS
New Delhi, India
Anjali Madan MD
Senior Resident
Department of Dermatology
Maulana Azad Medical College
and Lok Nayak HospitalNew Delhi, India
Anuj Tenani MBBS PGY-II
Department of Dermatology
Maulana Azad Medical College
and Lok Nayak Hospital
New Delhi, India
Anusha H Pai MD
Consultant Dermatologist
Derma-Care Skin andCosmetology Center
Mangalore, Karnataka, India
Atul M Kochhar MD DNB MNAMS FAAD
Senior Specialist–Grade I
Department of Dermatology and SD
Maulana Azad Medical College
and Lok Nayak Hospital
New Delhi, India
Banwari Jangid MDDepartment of Dermatology and
Venereology
All India Institute of Medical Sciences
New Delhi, India
Dharmendra Karn MD
Dermatologist
Dhulikhel Hospital
Kathmandu University
eaching Hospital
Kavre, Nepal
Ganesh S Pai MD DVD
Senior Consultant Dermatologist
Derma-Care Skin and
Cosmetology Center
Mangalore, Karnataka, India
Inder Raj S Makin
MBBS (India) Dipl-Ing (Germany) RDMS PhD (USA)
Associate Professor
A Still University
School of Osteopathic Medicine in
Arizona (SOMA)
Arizona School of Dentistry and
Oral Health (ASDOH)
Mesa, USA
Jaspriya Sandhu MBBS PGY-I
Department of Dermatology
Maulana Azad Medical College
and Lok Nayak Hospital
New Delhi, India
Kabir Sardana MD DNB MNAMS
Professor
Department of Dermatology
Maulana Azad Medical College
and Lok Nayak Hospital
New Delhi, India
Khushbu Goel MD
Pool OfficerDepartment of Dermatology
Maulana Azad Medical College
and Lok Nayak Hospital
New Delhi, India
Contributors
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
8/573
viii Lasers in Dermatological Practice
Narendra Kamath MD DVD
Consultant Dermatologist
Cutis Skin Care CenterMangalore, Karnataka, India
Pavithra S Bhat MD
Kovai Medical Center and Hospital
Coimbatore, amil Nadu, India
Payal Chakravarty MD
Senior Resident
Department of Dermatology
Maulana Azad Medical College
and Lok Nayak HospitalNew Delhi, India
Rashmi Ranjan MD
Senior Resident
Department of Dermatology
Maulana Azad Medical College
and Lok Nayak Hospital
New Delhi, India
Rashmi Sarkar MD MNAMS
ProfessorDepartment of Dermatology
Maulana Azad Medical College and
LN Hospital
New Delhi, India
Chief Founder and Honorary Secretary
Pigmentary Disorders Society
New Delhi, India
Shahin S NooreyezdanMBBS MS MCh (Plastic Surgery)
PGIMER ChandigarhSenior Consultant
Department of Plastic, Cosmetic and
Reconstructive Surgery
Indraprastha Apollo Hospitals
New Delhi, India
Shikha Bansal MD DNB MNAMS
Specialist
Department of Dermatology
Safdarjung Hospital
New Delhi, India
Shivani Bansal MD
Senior Resident
Department of Dermatology
Maulana Azad Medical College
and Lok Nayak Hospital
New Delhi, India
Simal SoinPG Dermatology (St Johns Institute of
Dermatology) London
MPhil Cambridge University UK
Medical Director and
Chief Cosmetic Dermatologist
Tree Graces
New Delhi, India
Soni Nanda MD (Dermatology)
Shine and Smile Skin Clinic
Max Super Specialty Hospital
New Delhi, India
Sujay Khandpur MD DNB MNAMS
Professor
Department of Dermatology and
Venereology
All India Institute of Medical Sciences
New Delhi, India
Twinkle Daulaguphu MBBS PGY-I
Department of Dermatology
Maulana Azad Medical College
and Lok Nayak HospitalNew Delhi, India
Vanya Narayan MBBS PGY-III
Department of Dermatology
Maulana Azad Medical College
and Lok Nayak Hospital
New Delhi, India
Vijay K Garg MD MNAMS
Director-Professor and Head
Department of Dermatology
Maulana Azad Medical College
and Lok Nayak Hospital
New Delhi, India
Vivek Nair MBBS MD
Consultant Dermatologist
Dr Nair’s Skin Clinic (Palam Vihar)
Clinic Dermatech (Vasant Vihar
and Gurgaon)
Metro Hospital (Palam Vihar)New Delhi, India
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
9/573
Lasers have moved from the fringe of dermatology to a more
centrist path over the past decade. Fifteen years ago, when
lasers trickled into our country, they were considered to
be exotic and perhaps accessible to a select few. Cosmetic
dermatology and lasers have grown by leaps and bounds and
that necessitates that they are absorbed in the mainstream.
With close to half of the dermatologists now owning or having access tolasers, it is important that our younger generation of dermatologists have
access to good practical textbooks as well as high quality equipment. Tis
book, Lasers in Dermatological Practice is best suited to educate our specialty
about the perils and pitfalls of using lasers.
Indian skin is unique since it comes commonly in 3 types—IV, V, VI.
Parameters will therefore vary depending on the skin types, a dilemma that
western books do not address. Postinflammatory hyperpigmentation will
vary in each skin type and even show variation among patients in a single skin
type. Such unpredictability and perplexing results are a cause of anxiety in acosmetologist at an inflexion point in his career. A comforting thought is that
our patients, except for a miniscule minority, are forgiving and compliant.
Most cases of tissue damage by laser will heal over time, nature coming to
our rescue. Our patience and reassurance will comfort patients in the interim
period.
In clinical dermatology, we have a chance to assess, judge and treat
patients. If there is an error of management, we can apply a midcourse
correction and modify therapy. Unfortunately, this is not true of lasers. A
mistake made, a poor assessment, using more or less power than requiredcan lead to laser burns and scarring. If it is on the face, as it is most of the
time, the consequences are not difficult to portend. Since there is no second
chance to repair damage, it is important to understand the basics of lasers
and the specifics of equipment much like reading a car manual before driving
your new car. Tis book does both and will hopefully lead to confident
cosmetologists and happy patients.
Foreword
Ganesh S Pai MD DVD FAADMedical DirectorDerma-Care Skin and Cosmetology Center, Te rade Center
Director-Professor, Department of Dermatology KS Hegde Medical College, Deralakatte
Mangalore, Karnataka, India
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
10/573
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
11/573
I thank the authors for giving me the opportunity to write the
Foreword to this excellent book, Lasers in Dermatological
Practice . Te editors along with the co-authors have put
down their vast experience in the use of laser in various
dermatological conditions. It is a book of international
standards and, in particular, reference to the application
of lasers in brown and dark skin patients. Basics of laser in relation to skinlesions are well-written.
Te use of the different lasers in different dermatological lesions and the
step-by-step approach to each and every lesion is superb. Te practical tips
to avoid wrong outcome is well-documented. Te use of non-laser energy
sources in dermatological practice is very illuminating. Te references at the
end of each chapter are apt and to the point.
Te chapter on medicolegal aspects is pertinent and informative. On the
whole, it is the end result of the vast experience over the years that the editors
have acquired to write this book. I am confident that this book will find aplace in all dermatologists library.
Foreword
B Krishna Rau
MS FRCS (Eng and Edin) FRCS (Tailand) (Hon) FIAMS FACG FICS FIGSC
Professor-Emeritus, Dr MGR Medical University Honorary Fellow, American Surgical Association
President, World Federation of Society for Laser and Surgery MedicineChennai, amil Nadu, India
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
12/573
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
13/573
Te genesis of this book arose from the common mechanistic approach where we learn which buttons to push, in courses provided by the more reputabledevice manufacturers just after a laser is purchased. Tis approach is foolish
beyond words, and can harm patients, and worse create medicolegal hazards.Tere are some excellent books that we have referred to but most of them
deal with technologies that are nice to hear but too expensive to use in India.
Our book was initially planned as a companion to the hands on workshop where the nitty gritty was left out while the topic in focus was discussed. Tusthe first edition was done with the help of Sun Pharmaceuticals. Tis editionis the combined effort of Abbot and the vision of Shri Jitendar P Vij, who
convinced us to make it an elaborate yet compact book. Te book answers the three basic questions, what to do, why to do it andhow to do it? But our basic target is the dermatologists who need a step-by-step approach to the technology commonly used and not the laser that a
speaker in most conferences uses, which as a thumb rule is expensive, the
reason why the company sponsors the talk in the first place! Tough the FDAgives clearance of a device for a particular labeled indication, this cannot be
taken as any assurance that it will work safely and effectively enough to satisfythe patients. ragically, it may not be an understatement that a majority oflasers bought in this country are not US FDA approved in the first place!
Te book will also look at some questions that we rarely ask. What is the
histological depth of fractional lasers? Which type of atrophic scar actuallyresponds? Is Fr CO
2 superior to Er:Glass? And many others.
As the field of cosmetic intervention usually encompasses indications
where novel non-laser technologies are used, we have covered radio-frequency, focused USG, plasma resurfacing and LED. Te book is planned in such a way where the commonly performedprocedures are discussed which gradually move on the advanced techniques.
Practical aspects like medicolegal hazards and pearls are discussed inthe latter half of the book. Some very useful information is provided in theappendices. Our contributors are largely those who are experts in their field of interest.
Our own work spanning over 8 years, with almost 5,000 procedures helped us
to bridge the gap between theory and practice. But this is not a “Cook Book” and only a guide on the best approach isprovided. Individual laser parameters can vary, thus there is no substitute
for hands-on training, which cannot be obtained in this book or sitting in alecture hall more so when there are hundreds sitting in it! Hope you like the effort. More will follow soon…
Preface
Kabir Sardana
Vijay K Garg
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
14/573
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
15/573
We would like to thank our faculty residents and students of the department
some who have left to join other institutions, for their role in establishing and
developing the Laser Clinic at Maulana Azad Medical College (MAMC), New
Delhi, India.
Special thanks to Dr Vijay K Garg, Director-Professor and Head,
Department of Dermatology and SD, MAMC, who through his administra-
tive acumen, managed to get the lasers. He has given me great support andhas served as a mentor throughout my professional career. His guidance and
encouragement over the years have influenced my efforts.
A special thanks to the team at M/s Jaypee Brothers Medical Publishers
(P) Ltd, New Delhi, India, especially Shri Jitendar P Vij (Group Chairman)
and Mr Ankit Vij (Managing Director), for latching on to the project, Mr PN
Venkatraman (Vice President-International), Mr Shashikumar Sambhoo, for
handling the publicity and sales and Mr arun Duneja (Director-Publishing),
Mr Subrata Adhikary (Commissioning Editor), Mr Lalit kumar (DP Operator)
for helping with the deadlines. A big thanks to our contributors, some of whom who have worked on their
chapter on a one month deadline! Each of them is an expert in their field.
Dr Simal Soin, Dr Shahin Nooreyezdan, Dr Inder Raj S Makin and Dr
Vivek Nair have worked on such a deadline. Dr Inder Raj S Makin has also
been kind enough to review two chapters for us and his comments have been
an asset to the chapters.
Dr Khandpur and Dr Anil Agarwal have also contributed after taking out
time from their busy schedule. Dr Atul M Kochhar who is also the Purchase
Officer at our Hospital has given nuances of buying lasers. A big thanks to Dr Antje Katzer (Ascepelion), for letting us use the images
of the company’s devices.
And lastly, our tributes to the countless patients who have taught us
dermatology and helped us to learn and relearn lasers!
Acknowledgments
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
16/573
xvi Lasers in Dermatological Practice
Real knowledge is to know the extent of one’s ignorance
—Confucius
Never sacrifice your dignity to make money, but charge what you areworth
—Christopher B Zachary
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
17/573
Contents
Section 1: Conventional Laser Interventions
1. Basics of Laser-issue Interactions 3
2. Ablative Lasers 25
Overview 25
Ablative Laser Treatment of Common Conditions 52
Step by Step Approach 86 Atlas 93
3. Pigmented Lesions and attoos 101
Overview 101
Lasers For Tattoo Removal 115
Laser Treatment of Common Pigmented Conditions 131
Step by Step Approach 160
Atlas 163
4. Fractional Photothermolysis 172
Overview 172 Laser Treatment of Common Conditions 204
Step by Step Approach 229
Atlas 233
5. Vascular Lasers 236
6. Lasers for Hair Removal 252
Section 2: Advanced Laser Interventions
7. Nonablative and Subsurface Rejuvenation 275
Step by Step Approach 291 8. Nonsurgical ightening 294
9. Aesthetic Intense Focused Ultrasound (IFUS): Clinical Perspective
on Fitzpatrick Skin ypes III–VI 319
10. Noninvasive Body Contouring 336
11. Lasers for Scars, Keloids, and Stretch Marks 361
Section 3: Practical Aspects and Advances
12. Miscellaneous Laser Responsive Disorders 379
13. How to Start a Laser Practice (Private Setup) 416
14. How to Set up a Laser Clinic in a Public Funded Institution 421
15. Terapeutic Pearls in Lasers 432
16. Medicolegal Aspects of Lasers in Dermatological Practice 441
17. Complications and their Management 455
18. New Aspects and Controversies in Lasers 471
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
18/573
xviii Lasers in Dermatological Practice
Appendices
Appendix 1: Laser Safety/Eye Care 493 Appendix 2: Consent Form 504
Appendix 3: Procedure Checklist 506
Appendix 4: Postoperative Care 507
Appendix 5: Sample Operative Note 512
Appendix 6: Sample Postoperative Instructions (Ablative Lasers) 513
Appendix 7: Patient Information Sheet 514
Appendix 8: Local Anesthetics 528
Appendix 9: Select Bibliography 538
Laser and Medical Devices (Index) 541
Index 543
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
19/573
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
20/573
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
21/573
CHAPTER 1
Basics of
Laser-Tissue Interactions
Kabir Sardana, Vijay K Garg, Shivani Bansal, Jaspriya Sandhu, winkle Daulaguphu
Medical lasers have evolved over the years with numerous applications.Dermatologic laser surgery is regarded as one of the fastest growing areasin the emerging fields of photomedicine and biomedical optics. As with anydevice, the most efficacious and appropriate use requires an understandingof the basic photobiological and photophysical principles of laser-tissueinteraction as well as the properties of the laser itself. Tis chapter provides abrief description of the nature of the laser, how it works, and the fundamentalmechanisms of its interaction with human skin.
LIGHT
Light represents one portion of a much broader electromagnetic spectrum.Light can be divided into the UV (200–400 nm), VIS (400–700 nm), NIR “I”(755–810 nm), NIR “II” (940–1,064 nm), MIR (1.3–3 mm), and Far IR (3 mmand beyond) (Fig. 1.1). Normally, the percentage of incident light reflected from the skin surfaceis determined by the index of refraction difference between the skin surface
(stratum corneum n = 1.55) and air (n = 1). About 4–7% of light is typicallyreflected and is called the Fresnel reflectance because it follows Fresnel’sequations relating reflectance to the angle of incidence, plane of polarization,and refractive index. Te angle between the light beam and the skin surfacedetermines the percentage of reflected light. More light is reflected at “grazing”angles of incidence. It follows that, to minimize surface losses, in most laserapplications, one should deliver light approximately perpendicular to theskin. One can deliberately angle the beam, on the other hand, to decreasepenetration depth and also attenuate the surface fluence by “spreading” the
beam. On the other hand, the surface of dry skin reflects more light becauseof multiple skin-air interfaces (hence the white appearance of a psoriasisplaque). Te light penetration into the epidermis depends on the wave-length dependent absorption and scattering. Because of scattering, muchincident light is remitted (remittance refers to the total light returned to the
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
22/573
4 Lasers in Dermatological Practice
environment due to multiple scattering in the epidermis and dermis, as wellas the regular reflection from the surface). In laser surgery, light reflectedfrom the surface is typically “wasted”. Tis “lost” energy varies from 15% to asmuch as 70% depending on the wavelength and the skin type. For example,for 1,064 nm, 60% of an incident laser beam may be remitted.
issue effects occur only when light is absorbed. Te absorption
coefficient is defined as the probability per unit path length that a photon at aparticular wavelength will be absorbed and it depends on the concentrationof chromophores (absorbing molecules) present. Te three primary skinchromophores are water, hemoglobin and melanin (Fig. 1.1). Chromophoresexhibit characteristic bands of absorption at certain wavelengths. Forexample, melanin absorbs broadly across the visible and ultraviolet (UV)spectrum, the oxyhemoglobin and reduced hemoglobin in blood exhibitstrong bands in the UV, blue, green and yellow regions. Water has strongabsorption in the infrared (IR) region (Fig. 1.1).
Optical properties of the epidermis and dermis are different. Inpigmented epidermis, melanin absorption is usually the dominant processover the majority of the optical spectrum (200–1000 nm) (Fig. 1.1). In thedermis, there is strong, wavelength-dependent scattering by collagen fibers,
which attenuates penetration of light. Tis scattering varies inversely with wavelength. Tus as a thumb rule , between 280 nm and 1300 nm, the depth
Fig. 1.1: Absorption spectrum of various lasers in
relation to the major chromophores
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
23/573
Basics of Laser-issue Interactions 5
of penetration increases with wavelength. Above 1300 nm, penetrationdecreases due to the absorption of light by water. Te most deeply penetrating
wavelengths are 650–1200 nm, while the least penetrating wavelengths are within the far-UV and far-IR regions.
Types of Light Devices
Lasers contain four main components, the lasing medium, the excitationsource, feedback apparatus and an output coupler. Te amplier of a laseris the laser material that can be a solid, a gas, or a liquid. Te feedbackmechanism is produced by the resonator, where the light is reected by two
mirrors so that the photons pass several times through the laser material. Tenumber of photons within the resonator increases exponentially due to thestimulated emission (Fig 1.2). With respect to lasing media, there are diode lasers, solid-state lasers, dyeand gas lasers. Solid-state lasers include the Nd:YAG laser, Er:YAG laser, alexandritelaser and the ruby laser. Te gas lasers include the carbon dioxide (CO
2)
laser, argon ion laser and the excimer lasers, while the diode and dye lasers are singular in their class.
Light Device Terminology
Basic parameters for light sources are power, time and spot size for continuous wave lasers and for pulsed sources, the energy per pulse, pulse duration, spotsize, fluence, repetition rate and the total number of pulses (able 1.1). At least for most ablative lasers, the effect of the laser beam on humanskin can be affected by any of three variables: power, time and spot size. Teeffects of power and time are proportional whereas that of spot size (radius)is an inverse square. If either the power or time is doubled, fluence increases
by a factor of 2. However, if the spot size is decreased by a factor of 2, fluenceincreases by a factor of 4. Doubling the spotsize results in a four-fold reductionin fluence.
Fig. 1.2: Various output modes of a conventional laser
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
24/573
6 Lasers in Dermatological Practice
Energy: Measured in Joules (J).Fluence: Te amount of energy delivered per unit area is the fluence,sometimes called the dose or radiant exposure, given in J/cm2
Power: Te rate of energy delivery is called power, measured in watts (W).One watt is one joule per second (W = J/s).
Density: Te power delivered per unit area is called the irradiance or powerdensity, usually given in W/cm2.Pulse width :Laser exposure duration (called pulse width for pulsed lasers) isthe time over which energy is delivered.Tus the lasers may be continuous, pulsed, quasi continuous and Q-switched(Fig. 1.3). Te older lasers had pulse durations that varied from seconds tomilliseconds (0.01s/10-3). Millisecond CO
2 lasers are gated lasers but largely
continuous wave in nature. Te CO2 laser is a classic example of a continuous
mode laser. Microsecond lasers (0.000001 sec/10-6
) are the ideal ultrapulselasers. Most Er:YAG lasers are also microsecond lasers. Another example isthat of the PDL where a single or a train of pulses is emitted. Pseudocontinuous lasers (KP) have very short pulses of light repeated at
very high repetition rates. Extremely short pulses are achieved by Q-switching.Tese nanosecond lasers (0.000000001 s/10–9) are used in pigmented lesions(Q-switched lasers). Recently picoseconds (0.000000000001 s/10-12) havebeen used in tattoos.Power density: It is a critical parameter, for it often determines the action
mechanism in cutaneous applications. For example, a very low irradianceemission (typical range of 2–10 mW/cm2) does not heat tissue and isassociated with diagnostic applications, photochemical processes andbiostimulation. On the other extreme, a very short nanosecond (ns) pulse cangenerate high peak power densities associated with shock waves and evenplasma formation.
Table 1.1 Various terminologies used in lasers
Power P (W) For Cw lasers
Energy E = (J) For Cw lasers
Power density W/A (irradiance)(W/cm2) (A = effective area)
For Cw lasers
Peak power P max (W) For pulsed lasers
Energy E per pulse (J) For pulsed lasers
Pulse duration t [fs (10−15)to ms (10−3)]
For pulsed lasers
Energy density E/A (radiantexposure) (J/cm2) (A = effective area)
For pulsed lasers
Cw: continuous wave, fs: femtosecond, ms: millisecond
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
25/573
Basics of Laser-issue Interactions 7
Spot Size: Another factor is the laser exposure spot size (which greatly affectsthe beam strength inside the skin). Other important factors include aspects of the incident light (convergent,divergent or diffuse) and the uniformity of irradiance over the exposure area(spatial beam profile). Te pulse profile, that is, the character of the pulseshapes in time (instantaneous power versus time) also affects the tissue
response.Operational modes: Te Operational modes of lasers are Cw, pulsed asinterrupted radiation (in ms), pulsed free running (in hundreds of ms),Q-switched (in ns) or mode-locked (in fs). Continuous wave (Cw) laser may be differentiated from a pulsed laser,
which provides bursts of energy. In the Cw mode, the laser delivers acontinuous beam of light with little or no variation in power output overtime (Fig. 1.3). In Cw operation, laser output is controlled by the physician,typically by depressing a foot pedal.
Interrupted radiation of a Cw laser is done by mechanical or electronicswitching with modification of the pulse length. Te pulse frequency is lowto moderate, up to 100 Hz. Flash lamp pumped solid-state lasers in the free-running mode have pulse lengths of 50 ms up to several hundred micro-seconds. Pulses of medical dye lasers systems can vary from microsecondsto 50 ms. Superpulse is a term specific to some carbon dioxide lasers that
Fig. 1.3: A figurative depiction of the energy and duration of
lasers based on the pulse width
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
26/573
8 Lasers in Dermatological Practice
have been modified to produce very short pulses with high peak powers in arepetitive fashion, commonly several hundred pulses per second.
Q-switching: Shorter pulses with very high intensities in the nanosecondrange are produced by Q-switching of the laser. Te single, intense pulse witha duration on the order of nanoseconds is produced. With Q-switching (theQ-factor stands for “quality factor,” used in electronics theory terminology), afast electromagnetic switch (Pockel cell) in the laser cavity causes excitationof the active medium to build-up far in excess of the level of the medium
when the shutter is open. In operation, the flashlamp is turned on and thepopulation inversion gradually grows. Lasing is prevented by the shutter.
When the population inversion is at a maximum, the shutter is opened so
that lasing occurs and a large burst of energy is emitted as the cavity rapidlydepletes the population inversion. Te net result is an extremely high peakpower (greater than 106 W) nanosecond duration pulse or series of pulses. Ultrashort laser pulses are generated by mode-coupling due to thecoherent properties of the laser. Compared to Q-switching, where the shortestpulse durations are in the range of the resonator period, mode-coupling cangenerate even shorter laser pulses.
BEAM PROFILES: TOP HAT VERSUS GAUSSIAN
Laser beam profiles vary based on intercavity design, lasing medium and thedelivery system. A common profile is Gaussian or bell-shaped (Fig. 1.4). For
Fig. 1.4 : Comparison of the beam types of lasers. In most indications, the top hat
profile is preferred. Te lower half of the figure demonstrates the conversion of a
Gaussian beam into a top hat beam, which can be achieved in certain laser
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
27/573
Basics of Laser-issue Interactions 9
many lasers, this profile represents the fundamental optimized “mode” ofthe laser. Tis shape is usually observed when the beam has been delivered
through an articulated arm. For some wavelengths, this is an effective way todeliver energy (CO
2 and Erbium). Te disadvantage of the rigid arm is limited
flexibility, the typically short arm length, the possibility of misalignment fromeven minor impact and a tendency for nonuniform heating across the spot.Te top hat beam ideally is better as there is uniform heating of the tissue.
Sometimes a bell-shaped profile is desirable, for example, when applyinga small spot FIR beam with a scanner. In this scenario, the wings of the beamallow for some overlap without delivering “too much” energy at points ofoverlap. Te Gaussian profile can be modified outside the cavity, which is
desirable in many applications. With a fiber equipped delivery system, thebeam is mixed within the fiber and can be shaped to be more flat-topped.
WAVELENGTH RANGES AND CLINICAL APPLICATION
A useful way of understanding the effects and clinical application of wavelength is to understand the interaction and depth of the different wavelength in relation to the primary chromophores (Fig. 1.5). 1. UV laser and light sources have been used primarily for treatment of
inflammatory skin diseases and/or vitiligo, as well as striae. Te XeCIexcimer laser emits at 308 nm, near the peak action spectrum forpsoriasis. Te penetration is restricted to the epidermis (Fig. 1.5).
2. Violet IPL emissions, low power 410 nm LED and fluorescent lamps areused either alone or with ALA.
Fig. 1.5: Optical penetration depth of common lasers used in dermatology
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
28/573
10 Lasers in Dermatological Practice
3. Green Yellow (GY): Tese wavelengths are highly absorbed byhemoglobin (Hgb) and melanin and are especially useful in treating
epidermal pigmented lesions and superficial vessels (Figs. 1.1 and 1.5). Tere are two issues concerning these lasers, one is their poor penetration
in skin (and the even poorer penetration in blood) which makes thempoor choices for treatment of deeper pigmented lesions or deeper larger
vessels. Similarly they are not useful for permanent hair reduction (withthe possible exception of very large spots (i.e., IPL) that enhance lightdepth). Te effective portions of many IPL spectra include the GY range.By the proper manipulation of a laser delivery device, one can optimizeparameters for selective heating of pigmented versus vascular lesions.
Practical aspects of GY laser manipulation: A. Applying a compression handpiece without cooling with 595 nm,
blood is depleted as a target and pigment is preferentially heated. B. If the pulse duration is reduced to the nanosecond range,
melanosomes are preferentially heated over vessels. For example,extremely short Q-switched 532 nm pulses will cause fine vessels torupture, but inadequate heat diffusion to the vessel wall precludeslong-term vessel destruction. On the other hand, melanosomesare sufficiently heated for single-session lentigo destruction. By
choosing specific wavelengths with respect to hemoglobin andmelanin, one can achieve some degree of selective melanin orhemoglobin heating.
4. Red and Near IR (I) (630, 694, 755, 810 nm): Deeply penetratingred light (630 nm) continuous wave devices are efficient activators ofprotoporphyrin after topical application of ALA. Te 694 nm (ruby)laser is optimized for pigment reduction and hair reduction in lighterskin types. Te 810 nm diode and 755 nm alexandrite laser, dependingon spot size, cooling, pulse duration and fluence can be configured
to optimize outcomes for hair reduction, lentigines or blood vessels.Tey are positioned in the absorption spectrum for blood and melaninbetween the GY wavelengths and 1,064 nm (Fig. 1.5). Tey will penetratedeeply enough in blood to coagulate vessels up to 2 mm; also, theyare reasonably tolerant of epidermal pigment in hair reduction (withsurface cooling) as long as very dark skin is not treated. By decreasingthe pulse width into the nanosecond range, the alexandrite laser is a firstline treatment for many tattoo colors.
5. Near IR (II) 940 and Nd:YAG (1,064 nm): Tese two wavelengths
have been used for a broad range of vessel sizes on the leg and face.Tey occupy a unique place in the absorption spectrum of the “3”chromophores, that is blood, melanin and water. Because of the depthof penetration (on the order of mm), they are especially useful for hairreduction and coagulation of deeper blood vessels. By varying fluenceand spot size, reticular ectatic veins, as well as those associated with
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
29/573
Basics of Laser-issue Interactions 11
nodular port wine stains or hemangiomas, can be safely targeted. On theother hand, they are not well-suited for epidermal pigmented lesions.
6. Mid infrared lasers and deeply penetrating halogen lamps: Teselasers and lamps heat tissue water. Te absorption coefficients for the1320, 1450, and 1540 nm systems are –3, 20 and 8 cm-1, respectivelyand the corresponding penetration depths are –1500, 300 and 700 mm.It follows that for equal surface cooling and equal fluences, the mostsuperficial heating will occur with the 1450 nm laser, followed by the1540 and 1320 nm lasers. Te MIR spectral subset has become themainstay for fractional non-ablative technologies.
7. Far infrared systems: Te major lasers are the CO2, Erbium YAG and
Erbium:YSGG (chromium:yttrium-scandium-gallium-garnet) lasers.Overall, the ratio of ablation to heating is much higher with the erbium
YAG laser. However, one can enhance the thermal effects of the Er:YAG laser byextending the pulse or increasing the repetition rate and likewise one candecrease residual thermal damage (RD) of the CO
2 laser by decreasing pw
(pulse width). Details of the two lasers are given in the chapter on ablativelasers.
LASERTISSUE INTERACTIONS
Te actual laser interaction is characterized by a dissipation of energy thoughan ideal situation is characterized by a direct straight line transfer of energy(z) (Fig. 1.6). When photons strike the surface of the tissue, because of therefractive index change, a portion (4–10%) of the photons are reflected
Fig. 1.6: Laser tissue interaction. Ideal laser penetration is a straight line (z) which is
not normally seen as the skin is not an optical window
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
30/573
12 Lasers in Dermatological Practice
according to the angle of incidence. Photons penetrating the surface initiallyare refracted, obeying the law of Snellius, which states that photons entering
a medium with a higher refractive index are refracted towards the vertical axisto the surface. Of all the different interactions, the most important is absorption orscattering.
Absorption
Te coefficient μa (cm-1) characterizes the absorption. Te inverse, Ia,
defines the penetration depth (mean free path) into the absorbing medium
and is typically given as cm–1
. Te absorption coefficient is chromophoreand wavelength-dependent. Absorbing molecular components of thetissue are porphyrin, hemoglobin, melanin, flavin, retinol, nuclear acids,deoxyribonucleic acid (DNA)/ribonucleic acid (RNA) and reducednicotinamide adenine dinucleotide. Te absorption spectra of differentchromophores of biological tissue and water are plotted in Figure 1.1 whilethe penetration is shown in Figure 1.5.
Chromophores
Blood, water and melanin are the main absorbing components in the tissue
(Fig. 1.1). Terefore, dye lasers and diode lasers effectively interact with blood,the alexandrite laser with melanin and MIR lasers with the water content ofthe tissue.
Hemoglobin: Tere is a large HgbO (oxyhemoglobin) peak at 415 nm,
followed by two smaller peaks at 540 and 577 nm. An even smaller peak isat 940 nm. For deoxyhemoglobin (Hgb), the peaks are at 430 nm and 555nm. Te discrete peaks of hemoglobin absorption allow for selective vessel
heating. Although the 410 nm peak achieves the greatest theoretical vascularto pigment damage ratio among the other peaks, scattering is too strong for violet light to be a viable option for vascular applications.
Melanin: Most pigmented lesions result from excessive melanin in the
epidermis. By choosing almost any wavelength (< 800 nm), one can pre-ferentially heat epidermal melanin. Shorter wavelengths will create very highsuperficial epidermal temperatures, whereas longer wavelengths tend tobypass epidermal melanin (i.e. 1,064 nm).
Fat: Fat shows strong absorption at 1,200 and 1,700 nm. Although the ratios of
fat to water absorption are small, the small differences are exploited with theproper choice of parameters.
1,200 nm might represent the best choice due to decreased overall waterabsorption and therefore, increased penetration. Sebum is similar to fat butalso is comprised of wax esters and squalene.
Carbon: Carbon is a product of prolonged skin heating.
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
31/573
Basics of Laser-issue Interactions 13
Once carbon is formed at the skin surface, the skin becomes “opaque” tomost laser wavelengths (that is, most energy will be absorbed very superficially.
It follows that the dynamics of surface heating changes immediately oncecarbon is formed. Tis can be used creatively as an advantage. For example,one can convert a deeply penetrating laser to one that would only affect thesurface by using a carbon dye. Tis has been accomplished with a laser peelusing a Q-switched Nd:YAG laser, though is is not commonly used now.Collagen: Dry collagen has absorption peaks near 6 and 7 mm. With a freeelectron laser operating at these wavelengths, collagen can be directly heated.
Scattering
Te scattering behavior of biological tissue is important because it determinesthe volume distribution of light intensity in the tissue. Tis is the primary stepfor tissue interaction, which is followed by absorption and heat generation.Scattering of a photon is accompanied by a change in the propagationdirection without loss of energy. Scattering leads to an increase in the light intensity directly below thetissue surface is enhanced by a factor of 2–4 as compared with the intensity ofthe incident beam. Te increased fluence rate is caused by scattered photonsoverlapping with the incident photons. Another observation is that due to thescattering effect, the penetration depth depends on the irradiated area.
Practical Implications
It has been shown that the light intensity directly below the tissue surface isenhanced by a factor of 2–4 as compared with the intensity of the incidentbeam. Te increased uence rate is caused by scattered photons overlapping
with the incident photons. Because of the scattering effect, the penetrationdepth depends on the irradiated area. Tus, the penetration depth will double
if for the same irradiance, the beam diameter increases from 1 mm to 5 mm.Tus for treating port wine stains or for hair removal, 10 mm to 15 mmspot diameters of the laser are recommended as it increases the depth of thelaser beam. In tattoos and nevus of Ota in case there is inadequate response ,it is wise to increase the diameter of the probe to increase the depth.
Reaction Mechanisms
Te rst systematic presentation of the reaction mechanisms of lasers withtissue was by Boulnois and is depicted in the Figure 1.7. Tis highlights the
different tissue effects and thus smaller the pulse duration of the interactionmore the energy. Tus the Q-switched lasers like Nd:YAG can generatephotodisruptive fluencies due to the short time of impact. Te various tissue reactions include, Nonthermal reaction, chemicalreactions, thermal reactions (based on relaxation time), tissue ablation orphotodisruption.
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
32/573
14 Lasers in Dermatological Practice
Once the local subsurface energy density has been determined, heatgeneration can be predicted by energy balance (conservation of energy), pulse
duration, thermal relaxation time and the wavelength specific absorption forthat target. We will focus largely on the interactions relevant to commonly usedmedical lasers.
1. Photothermal Reactions
Photothermal effects (1 ms–100 s; 1–106 W/cm2; Fig. 1.7) Te energy of the laser irradiation is transferred into heat due to the
absorption of the photons by tissue components, DNA/RNA, chromophores,proteins, enzymes and water. According to the degree of heating, stepwiseand selective thermal damage can be achieved:
¾ 42–45°C: Beginning of hyperthermia, conformational changes andshrinkage of collagen;
¾ 50°C: Reduction of enzymatic activity; ¾ 60°C: Denaturation of proteins, coagulation of the collagens, membrane
permeabilization; ¾ 100°C: issue drying and formation of vacuoles;
¾
>100°C: Beginning of vaporization and tissue carbonization; ¾ 300–1,000°C: Termoablation of tissue, photoablation and disruption.
Fig. 1.7: A figurative depiction of the plot of laser tissue interaction
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
33/573
Basics of Laser-issue Interactions 15
Termal diffusion is responsible for heat ow into the tissue. If theexposure time with a laser pulse, tp, is short compared to the diffusion time,
td, then we have “thermal confinement” and the pulse energy is convertedinto heat. Termal diffusion and the extent of tissue necrosis are related. With lowlaser power and long irradiation time, thermal necrosis is large. Shorteningthe laser application time reduces the time for thermal diffusion and the zoneof necrosis becomes smaller. Minimum thermal necrosis is reached when theirradiation time is equal to the thermal diffusion time or thermal relaxationtime. Tis is demonstrated by the laser interactions with pulsed CO
2 lasers
(Fig. 1.8).
Termal damage of the tissue is described by the Arrhenius rate equation(Fig. 1.9). Te consequence of this equation is that the threshold for tissuedamage depends on the laser power and the application time. Tis thresholdcan be reached with high laser power in a very short time, resulting in a highertemperature or with low power but long irradiation, where the threshold isreached with lower temperature.
2. Tissue Ablation
Te preconditions for tissue ablation are high absorption and very shortlaser pulses. Analogous to the thermal confinement, one can define a “stressconnement” when tissue is heated up so fast that the pulse duration is
Fig. 1.8: Example of the effect of pulse duration on tissue effect. (A) 3 J/cm 2; 0.01 sec
(whitening); (B) 3 J/cm2; 0.40 sec (coagulation); (C) 9 J/cm2; 0.50 (cogulation with
ablation). Lower the irradiation time, lesser the coagulation the thermal necrosis
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
34/573
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
35/573
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
36/573
18 Lasers in Dermatological Practice
the heat produced diffuses away despite its origin in the target structure. Te
target does not become appreciably warmer than its surroundings becausethe absorbed energy is invested almost uniformly in heating of the tissueduring exposure. As a result, longer pulse durations offer a more generalizedheating and therefore, less spatial selectivity resulting in nonspecific thermaldamage to adjacent structures regardless of how carefully one has chosena wavelength (Fig. 1.10). However, if the laser pulse is suitably brief, itsenergy is invested in the target chromophore before much heat is lost bythermal diffusion out of the exposure field (Fig. 1.10). A transient maximumtemperature differential between the target and adjacent structures is then
achieved. Shorter pulse durations confine the laser energy to progressivelysmaller targets with more spatial selectivity. Te transition from specific tononspecific thermal damage occurs as the laser exposure equals and thenexceeds R.
When defining thermal relaxation time, the target size and geometry areimportant (Box 1.1). For most targets, a simple rule can be used: Te thermal
relaxation time in seconds is about equal to the square of the target dimensionin millimeters. Tus a 0.5 mm melanosome (5 × 10-4 mm) should cool in about
25 × 10-8 s, or 250 ns, whereas a 0.1 mm PWS vessel should cool in about 10–2 s,
or 10 ms. Tis provides an approximate pulse width for varying degrees ofthermal confinement.
Te often used term “thermal relaxation time of the skin” is meaningfulonly when used for specific wavelengths (or specific skin structures, i.e., theepidermis). With a ubiquitous absorber such as tissue water, it should beconsidered within the context of the laser source. For example, if one uses
Fig. 1.10: Relation of pulse duration (p) and R (thermal relaxation time). p = R,
heat is confined to the vessel, p > R, there is dissipation energy outside the vessel
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
37/573
Basics of Laser-issue Interactions 19
the 1,540 nm laser, the entire epidermis and large portions of the dermisare heated and the R is on the order of seconds, because the thickness isseveral hundred millimeters. So even though R of the epidermis is about10 ms based on its thickness, a thicker slab of skin is heated at 1,540 nm, the
epidermis will take several seconds to cool because there is no temperaturegradient between it and that of the dermis. A summary of the R of majortarget tissues is given in Box 1.1.
Application
With a very short pulsewidths (pw), lasers vaporize targets. For example, intreating blood vessels, rapid heating results in acute vessel wall damage andpetechial hemorrhage (with Q-switched 532 nm). With intermediate lengthpulses (0.1–1.5 ms), one can gently heat targets without immediate ruptureof the vessels. But intravascular thrombosis can create purpura and delayedhemorrhage. With longer pulses (6–100 ms), the ratio of contraction tothrombosis increases and side effects are less likely. oo long pulses with verysmall targets can create two problems. With highly absorbing targets, (i.e.,tattoo inks), the heat generation is so great and long-lived that significantdiffusion occurs to the surrounding dermis. On the other hand, using a longpulse YAG for a nevus of Ota results in an insufficient temperature rise as thepigmented nevus cells cool off too fast during the delivery of the pulses (alsomelanin absorption is much weaker than black ink).
Selective Photothermolysis of Tattoos
Amorphous carbon, graphite, India ink and organometallic dyes, typicallyfound in dark blue-black amateur and professional tattoos, have a broadabsorption in the visible and near-infrared portions of the spectrum. At visible
Box 1.1 R of potential targets used in dermatology
Melanosome (0.5 μm) 0.25 μsMelanocyte (7μm) 1 μs
Nevus cell (10 μm) 0.1 ms
Collection of nerves cells (100 μm) 10 ms
Epidermis (100–200 μm) (dermoepidermal junction10 μm)
10 ms
Erythrocyte 2 μs
Hair follicle (200 μm ) 40 ms
Vessel (0.1 mm diameter) 10 ms
Vessel (0.8 mm diameter) 300 ms
Vessel (0.1 mm diameter) 10 ms
attoo (0.5–100 μm) 20 ns–3 ms
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
38/573
20 Lasers in Dermatological Practice
wavelengths longer than 600 nm, hemoglobin and melanin light absorptionis minimized and tattoo dyes can be targeted selectively.
Te pigment granules characteristically found in tattoos have diametersof 0.5–100 mm, which correspond to R of 20 ns to 3 ms. With thedevelopment of the Q-switched ruby (694 nm), alexandrite (755 nm), andNd:YAG (1.06 mm) lasers, tattoo removal without scarring can be achieved.Te frequency-doubled, Q-switched Nd:YAG laser (KP laser) emits at a
wavelength of 532 nm, which provides improved removal of red dye. Recentlypicosecond lasers have been used for tattoos.
Selective Photothermolysis of Pigmented Lesions
Pigmented lesions can be divided in to epidermal and dermal. Althoughhighest in the ultraviolet portion of the spectrum, melanin absorption is alsosignificant in the visible and near-infrared wavelengths. Te diameters ofindividual melanosomes (0.5–1.0 μm) and melanocytes (7 μm) correspondto R of 20–1,000 ns. Terefore, Q-switched green, red, and near-infrared
wavelengths have been utilized for this indication. Tough Q-switched lasersare used most commonly the gentle heating by the millisecond laser can alsotreat epidermal disorders. With longer pulses (ms), the dermal melanocytedoes not become hot enough to achieve pigment reduction, thus ensuringselective epidermal damage.
Selective Photothermolysis and Laser Assisted Hair Removal
Te human hair follicle is a complex structure derived from both epidermaland dermal components. Te target chromophores, primarily melanin-richhair shafts, are located deep in human skin (bulge around 1.5 mm and bulbat 2–7 mm). At this depth, only red and near-infrared wavelengths are useful(690–900 nm). Te follicular structure responsible for regeneration has not
been conclusively identified and therefore, current systems target the entirefollicle. As a result, long pulse widths on the order of milliseconds and highfluences capable of heating large volumes of tissue are required. Millisecond-domain ruby, alexandrite, diode and Nd:YAG lasers using high light dosescan produce selective injury to human hair follicles resulting in prolongedgrowth delay and in some cases, permanent hair loss after a single treatment.
Selective Photothermolysis of Cutaneous Blood Vessels
Te pulsed dye lasers at 577–595 nm wavelengths well absorbed by the
targeted hemoglobin molecule relative to other optically absorbing structures,cause selective thermal damage to dermal blood vessels while minimizingepidermal melanin absorption. Furthermore, because the R for cutaneousblood vessels varies between 10–300 ms a variable pulse duration is requiredfor optimal results.
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
39/573
Basics of Laser-issue Interactions 21
But there are numerous variations in pulse duration and absorptionof various chromophores (bloodless dermis, oxyhemoglobin and
deoxyhemoglobin) that can complicate this simplistic interpretation.
Practical Clinical Applications
Tere are numerous clinical applications that have been given in the textabove and the chapters that follow. wo examples are given below: 1. Te geometry (and therefore the microscopic characteristics) of lesions
is important. For example, in the treatment for a nevus versus a lentigo,the nevus is composed of melanocytes in aggregates as (collectively
of a size of 100 μm in diameter) whereas the lentigo is a mere sheet ofmelanocytes some 10 μm thick. So the R of the nevus cell is about10 ms while that of the lentigo is about 0.1 ms (Box 1.1).
Tus, in treating nevus with a long pulsed alexandrite laser with a highfluence, the R will approach a second. From the above equation, itfollows that thermal confinement will be high, and the peak temperature
will rise accordingly. More importantly, the thick slab of melanocytes will take long to cool, such that there will be considerable heat diffusionaway from the target. On the other hand, the lentigo represents a slab
only tens of microns thick; there will be heat diffusion during the longpulse and rapid cooling after the pulse. Tus, with ms-domain fluences,the nevus case might result in scarring and a lighter lentigo might notbecome hot enough for clearance. If one applies ns pulses to the twolesion types, the lentigo shows a good response with possibly completeclearing, whereas the nevus will require multiple sessions, as each laserapplication will result in heat confined to the most superficial part of thelesion. Conversely a microsecond laser might work for nevi.
2. Spot diameter: In general, the spot size should be 3–4 X > d (target
diameter), as larger spots make it more likely that photons will bescattered back into the incident collimated beam. Photons scatteredout of the beam are essentially wasted. Larger beams (with the samesurface fluence as smaller beams) create deeper subsurface cylinders of
injury because there is less surface versus volume for photons to escape.Basically, for small beams (narrow), scattered photons are carried outof the beam path after only a few scattering events. Tus, as a thumbrule, larger the spot, more the dermal/epidermal damage ratio but also
higher is the epidermal damage thus the fluence should be reduced.
For shallow penetrating lasers such as CO2 and erbium where the d
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
40/573
22 Lasers in Dermatological Practice
How to use the Knowledge Practically?
Te vast amount of data is of little meaning if used correctly. Tus in practice,three principles have to be remembered on which laser applications areapplied. 1. Absorption spectra of various chromophores: It is important to
understand the wavelength that is absorbed by the target chromophore.Tis is specially relevant in tattoos, thus accounting for the use of 532nm (green) for a red tattoo and 1,064 nm (blue) for a black pigment. Tisalso accounts for the use of Er:YAG as an ablative tool for dermal tumors
where the target chromophore is water.
2. Pulse duration of the lasers: Tis is directly dependent on the size ofthe target. Tis explains, why a Q-switched laser is used for a nanosizedtattoo and this also explains the logic of using a microsecond laser(Er:YAG) is used for epidermal ablation (R 10 ms).
3. Penetration depth of laser: Te optical penetration depth is a importantconsideration specially in pigmented skin. As melanin has a wide rangeof absorption spectrum, most lasers can be used, based on the abovetwo principles. Te reason most of us use the Q-switched Nd:YAG is asit penetrates deeper and thus would not interact with the competing
epidermal pigment, which is a competing factor in pigmented skin. A summary of the indications and lasers used that largely conform to theabove principles is given able 1.2.
Table 1.2 A summary of lasers used for common disorders
Vascular lesions Pigmented lesions attoo
removal
Photoepilation Resurfacing
Ablation
PDL* (585–600 nm) QS Ruby (694 nm) QS Ruby
(694 nm)
Long-Pulse
Ruby (694 nm)
Carbon
dioxide *(10,600 nm)
Long-pulse Nd:YAG(1,064 nm)
QS Nd:YAG *(532, 1,064 nm)
QS Nd:YAG*(532, 1,064nm)
LongPulseNd:YAG *(1,064 nm)
Er:YAG *(2,490 nm)
Long-pulse KP(532 nm)
QS Alexandrite(755 nm)
QS Alexandrite *(755 nm)
LongPulse Alexandrite(755 nm)
Fractional*(1540 nm)
IPL† IPL † Long PulseDiode * (800
nm)IPL*
* Used preferentially in pigmented skin
†Not very effective
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
41/573
Basics of Laser-issue Interactions 23
Exceptions
Inspite of these principles numerous laser applications are there which do notalways conform to these basic principles. Tis includes plasma resurfacing,laser lipolysis, use of Q-switched lasers for melanocytic nevi and ablativefractional lasers. In some, the target size have changed like for hair removallasers where the initial work focused on the bulge area but it now targets thediameter and the hair shaft. In PWS, multiple issues arise including the sizeof the vessels, the presence of deoxy or oxyHb and the depth of the vessels.Te pulse duration is being tweaked to adapt to the needs of the PDL. Inattoo cases, after the first few sessions, the optical property of the pigment
changes and macrophage engulfment changes the target size. Te use ofthe R20R technique for tattoos is a example where in all likelihood after thefirst impulse the optical properties of the particle changes and the repetitiveimpaction do not conform to the basic principles of laser tissue interaction. One illustrative example is of the AFR (ablative fractional) lasers. Teapproximate optical penetration depth (OD) in water for such lasers isminimal, e.g., 1µm for the Er:YAG laser (2,940 nm) and 10 µm for the CO
2
laser (10,600 nm). But they are used for acne scars which can involve thelower dermis. Tis is as high volumetric energy densities are reached virtually
instantaneously within the focus of the laser beam, and therefore such laserscan quickly advance a cavity deep into the tissue during the pulse. Due to thisprocess, it is possible that the resulting depth of an MZ can greatly exceedthe optical penetration depth of any particular laser wavelength. Also theoptical penetration depths provided are approximations of the penetrationdepth in water which can vary substantially and is approximately 30% for theepidermis and 70% for the dermis. As the optical properties of water are alsotemperature, dependent, it has been reported that the rapid change of tissuetemperature during a laser pulse can dynamically alter the penetration depth
substantially.
CONCLUSION
Tere are numerous other interesting scenarios that can affect the lasertissue interactions like optical clearing with hyperosmolar solutions, photonrecycling, using a polarizing lamp to enhance illumination and selectivecell targeting. But the basic principles that are used are an understanding ofthe laser wavelength and chromophore interaction, the R and the pulse
duration.
BOOKS
1. Nelson JS. An Introduction to Lasers and Laser-issue Interactions in
Dermatology. Principles and practices in cutaneous laser surgery. Editor: Arielle
NB Kauvar; Associate editor, George J Hruza; 2005.
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
42/573
24 Lasers in Dermatological Practice
2. Ross EV, Anderson RR. Laser issue Interactions. Cutaneous And Cosmetic laser
Surgery, Ist Edn. Mitchel P Goldman; 2006.
3. Ronald G. Wheeland Basic Laser Physics and Safety. In: Goldberg DJ (Ed). LaserDermatology. 2005.
4. Steiner R. Laser-issue Interactions. In: Raulin C, Karsai S (Eds). Laser and IPL
echnology in Dermatology and Aesthetic Medicine; 2011.
BIBLIOGRAPHY
1. Boulnois JL. Photophysical processes in recent medical laser developments: a
review. Lasers Med Sci. 1986;1:47-66.
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
43/573
Kabir Sardana, Vanya Narayan, Rashmi Ranjan
OVERVIEW
Skin resurfacing is not a new concept; various methods have been usedextensively for almost a century. Dermabrasion, in its various forms, has beenused successfully for treating wrinkles and acne scars for several decades. Ithas recently lost popularity due to the introduction of laser resurfacing, thedifficulty in obtaining precise depth control, and the release of blood-borne
viruses into the aerosol. Chemical peeling, which still enjoys popularity, is largely a blind
procedure and is greatly dependent on multiple variables to obtain desirablepenetration depths. Although superficial (i.e., epidermal) peeling is very safeand predictable, deeper chemical peels are less precise and can lead to eitherinadequate or excessive penetration depth. Phenol and augmented phenolpeels can produce spectacular results in removing heavily sun-damagedskin but are less suitable for darker and skinned patients, males and youngerpatients. Carbon dioxide laser resurfacing was favored as the preferred methodof skin resurfacing by many experts in aesthetic surgery. Although the short
and long-term improvement in sun damage and wrinkles can be extremelydramatic, carbon dioxide laser resurfacing has significant morbidity, even
when performed by well-trained doctors. Tis includes redness, temporaryhyperpigmentation, permanent hypopigmentation and dermal pacification. Tough fractional lasers have largely replaced ablative laser resurfacing,out interest is in using these lasers for common epidermal and dermaldisorders, where their role is paramount. At present, three laser are used for ablative indications and as thechromphore in all is water the difference lies in their relative affinity. As shown
in the Figure 2.1, the Er:YAG has a higher affinity than Er:YSSG with the CO 2 having the least absorption for water. Tus the safest of all is the Er:YAG laser.
CARBON DIOXIDE LASERS
Te continuous-wave carbon dioxide laser, producing infrared light with a wavelength of 10,600 nm, was the first to be used for resurfacing procedures.
CHAPTER 2
Ablative Lasers
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
44/573
26 Lasers in Dermatological Practice
Its wavelength is strongly absorbed by water, which is the most abundantchromophore in the skin and comprises approximately 70 percent of itstotal volume. Tis seemed to make it an ideal tool for generalized superficialablation. But its tissue-dwell time could not be precisely controlled andfar exceeded the 1 millisecond thermal relaxation time of the 20 to 30 μmof cutaneous tissue that absorbs CO
2 light. Excessive thermal diffusion and
concomitant unintended tissue damage were the common results. However, in the early 1990s, new pulsed and scanning CO
2 lasers were
developed that could deliver very high peak fluences of at least 5 J/cm highenough to vaporize cutaneous tissue in less than 1–2 milliseconds (Fig. 2.2).Te energy required for vaporization of the epidermis is 5 J/cm. For thethickness of the tissue (20–60 μm), the R is about 800 μs. Tis is achieved bythe ultrapulse lasers where a 250 mJ pulse using a 2.5 mm probe size achievesmuch higher fluencies in a shorter time as compared to the continuous wave(Cw) CO
2. Te superpulse laser is a mechanically shuttered laser whose
peak power is higher than Cw lasers but the average power over time is thesame. Tese pulsed systems can precisely and safely remove thin layers ofskin, between 20 μm and 30 μm with each pass, while leaving an acceptablynarrow zone of residual thermal damage: 25 μm to 70 μm, in contrast to the200 μm to 600 μm zone produced by the continuous-wave CO
2 laser.
Principles of Carbon dioxide Lasers
R Rox Anderson and Parrish coined the term ‘selective photothermolysis’
in 1983 to describe the process by which a chromophore is heated by laserlight absorption in a time period shorter than its thermal relaxation time.Te latter is the amount of time required for a material to lose 50% of its heatby conduction to its surroundings. Tus, when a chromophore is heated byselective photothermolysis, only the intended target is damaged and thereis minimal diffusion of heat and no consequent injury to the surrounding
Fig. 2.1: Absorption spectrum of the three commonly used ablative lasers
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
45/573
Ablative Lasers 27
structures. Te mechanism of injury involves both thermal coagulation and/or photoacoustic injury in the form of supersonic high pressure shock waves.For both the CO
2 and Er:YAG lasers, the predominant mechanism is
photothermal. Te pulse fluence necessary to achieve vaporization and thusablation of skin tissue with the CO
2 laser is 5 J/cm2 with a calculated R of
800 µs. Te unique aspect of CO2 laser is that for each 20 µm that is ablated,
3–4 times this amount is damaged. It is this latter effect that allows for thepurported collagen remodeling and wound healing. Tis zone of coagulationis modest compared to 1000 µm layer of damage that results from Cw CO
2
lasers.
Pulse Duration of Carbon Dioxide Lasers
Laser dwell time is the amount of time that the beam is on in one location.Low power densities require longer dwell times to achieve the same effect ashigh power densities. Te longer the dwell time and the slower the heating, themore desiccation and charring of tissue that results. Further heating of charredtissue results in extremely high temperatures of 300–600°C. Tis is becausecarbonized and desiccated tissue acts as a heat sink for laser absorption. Tereis no buffer of water to absorb the heat and thus temperatures escalate rapidly.Te significance is that if a non-pulsed laser is used, a low pulse duration shouldbe used to minimize thermal injury.
Types of Lasers
Most clinicians use the superpulsed CO2 lasers, which deliver pulse energies
in the 10–50 mJ range. Te peak power per pulse is 2–10 times higher than CwCO
2 lasers, but the average power over time is similar (Fig. 2.2).
Fig. 2.2 : A comparison of the waveform of CO2 laser. Note that for the same energy
(X) generated by a ultraPulse (
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
46/573
28 Lasers in Dermatological Practice
Te UltraPulse laser introduced by Coherent (now Lumenis) solvedthe problem of having to create second (duty cycles pulses of pulses) with
the superpulsed lasers. Tis was the first laser capable of delivering veryhigh fluence pulses (–200–500 mJ) with large spot sizes capable of tissue
vaporization with a single pulse Te depth of vaporization with an UltraPulselaser was studied in pig skin using pulses of 250–450 mJ. In human skin, thedepth of thermal damage using the ultrapulse laser was 20 µm after one pass,40 µm after two passes, and 70 µm after three passes. Various modifications have been used with the CO
2laser. Te Nova-Pulse
can generate 7 J/cm2 of fluence by rapidly moving a small spot size througha computer pattern generator. Te ruPulse (issue echnologies) laser
can produce peak powers up to 10,000 watts at very short pulse durations(65–125 µs). Another laser system that can achieve results similar to those ofthe UltraPulse is the Sharplan SilkLaser. Tis device offers two modes: theFeatherouch and Silkouch. Tis scanned laser uses a continuous wave CO
2
laser beam that is scanned over a defined pattern so rapidly that the tissuedwell time in any given spot is less than 1 ms. Tus the effect is essentially thesame as that of a high-energy pulsed system.
How do the Different CO2 Lasers Compare?
Alster et al. compared four resurfacing lasers and found that they weresimilar in histologic and clinical outcomes. Kauvar et al. studied the histologyof superpulsed, Silkouch, and UltraPulse lasers in human skin and foundthat after three passes, the SP and Silkouch RDs (residual thermal damage)
were both 150 µm, the UltraPulse RD was 70 µm, and the Cw laser RD(10 W and 0.2 s exposure) was 400 µm. Many investigators have comparedthe various levels of RD after three passes in LSR: a summary of which isprovided in the able 2.1. Te important aspect to note is the variation in the
thermal coagulation as shown in able 2.2.
Can a Cw CO2 be Used Like an UltraPulse Laser?
As most laser practitioners rarely acquire a true ultraPulse laser, this isa relevant practical point. It must be understood that the Silk laser andUniPulse (able 2.1) are essentially Cw lasers but achieve comparable RD asthe UltraPulse. But the importance of setting cannot be overemphasized. Tisis as a high dose or a high pulse duration can change the profile of the lasercompletely. Putting simply a higher pulse duration can cause coagulation
upto 1000 µm making it akin to a radiofrequency (RF) device. A comparisonis given below (able 2.2) between the UltraPulse and Cw CO
2. Tis shows
that if the optimal settings are used a Cw CO2 can behave like a UltraPulse
CO2 with little clinical difference.
A simple thumb rule is that energy levels from 7–9 J/cm2 with a pulseduration of 0.3 ms (0.03 s) can safely replicate the results of most UltraPulse
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
47/573
Ablative Lasers 29
CO2 lasers. And most importantly, with most CO
2 lasers, there is no advantage
of exceeding 3 passes. A detailed explanation of the modes of Cw CO2 laser
in conventional dermatological indications will be discussed in the nextchapter.
What is the Comparison of UltraPulse CO2 with
Conventional Cosmetic Procedures?
A comparison between the ultrapulsed CO2 laser with various pulse energiesand numbers of pass and CA peeling, dermabrasion, and Baker’s phenolpeel on a porcine model showed that at typical pulse energies, one to threepasses produced a wound depth intermediate between a 35% CA peeland dermabrasion, but more superficial-than a phenol peel (Fig. 2.3). Tusby varying the dose, epidermal or dermal depth can be achieved to target
able 2.1 Comparison of available CO2 lasers
Lasers Typical “settings” Typical safe
fluence (J/cm2 )
Typical RTD
after two to
three passes (µm)
UltraPulse Density 6, 300 mJ 7.5 90–110
NovaPulse Computer scannerE16, 7 W
6–7 60–80
Silk Laser 18 W/36 W (with 200 mmhandpiece)
15/8 110/70
ruPulse 500 mJ 5 50
UniPulse 16–18 W/20%overlap
14 70
able 2.2 Comparison of UltraPulse and Cw CO2
Lasers UltraPulse SilkTouch* FeatherTouch**
Ist Pass Epidermal vaporization+20 µm of dermal necrosis
Epidermal vaporization+70 µm of dermalnecrosis
Epidermal vaporization+10 µm of dermalnecrosis
2nd pass Epidermal vaporization+40 µm of dermal necrosis
Epidermal vaporization+100 µm of dermalnecrosis
Epidermal vaporization+30 µm of dermalnecrosis
3rd pass Epidermal vaporization+60 µm of dermal necrosis
Epidermal vaporization+50 µm of dermalnecrosis
300 mJ, 2.25 mm spot, 100 W, density 6
*28 J/cm2, **10 J/cm2
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
48/573
30 Lasers in Dermatological Practice
the condition to be treated. Tis also highlights the fact that the CO2 laser, in
optimal settings, can match most conventional tools with better precision. Apoint that is to be emphasized that the pulse duration of electrocautery andRF is in seconds while the most rudimentary CO
2
lasers have a maximum of0.9 seconds. Tus, the thermal damage and consequent cosmesis of the CO
2
is superior to any RF machine or electrocautery device.
Technique Tips
As most of the laser surgeons employ CO2 to treat dermal tumors we will
focus on this, though a similar principle can be applied to other indications.For individual lesions, the growth is vaporized by using relatively low powersettings in the 3 W to 5 W range with a spot size that matches the size of the
lesion.Importantly, as there is a concomitant thermal damage the entire lesion
may not be destroyed. Ablation should be carried to the level of the dermis. As some residual thermal damage will extend 0.5 to 1 mm beyond the level ofablation, this suffices in most cases and can be reliably achieved in 3–4 passes(able 2.3).
Fig. 2.3: A comparison of the dose depth analysis of UltraPulse CO2 laser with
conventional modalities
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
49/573
Ablative Lasers 31
End Points
At the end of the day most surgeons do not use fixed settings but look for end
points to reliably ascertain when to stop the ablation procedure. Publishedreports have correlated clinical signs with anatomic depths of ablation. A pink color was found to correlate with superficial papillary dermis, a “chamois-cloth” appearance with papillary dermis and “ waterlogged” cotton-thread appearance for reticular dermis. Tis is true only for deep ablation such as
with treatment of plantar warts. When thinner layers of ablation are used,
able 2.3 A comparison of salient aspects of CO2 (pulsed) and Er:YAG lasers
Parameters CO2
Er:YAG
OD (Opticalpenetration)
20 μm 1 μm
Ablation TresholdR
5 J/cm2 800 μs
0.5–1.5 J/cm2
1 μs/Pulse duration 250 μs
AblationDepth/pulse
20–60 μm*Plateau at 4th pass
5–50 μmNo Plateau
Range of thermalInjury/pass
75–150 μm** 15–50 μm
issue Effects Photothermal Photomechanical
issue Levels Epidermis = an opalescent aspect isobtainedPapillary dermis = Pink colorDeep Papillary dermis = Chamoisleather appearanceReticular dermis = Cotton threadappearance due to collagen
Epidermis = WhiteningPapillary dermis = Pin pointbleedingReticular dermis = Unevensurface (sebaceous glands)brisk bleeding
Histological effect Coagulation-crater around theablated area (necrosis, deepthermal effect)
Precise and safe ablation(limited thermal effect)
Safety of treatment Necrosis makes control of ablationdepth difficult
High visibility of treatmentrange, ablation depth caneasily be controlled
Depth of treatment reatment is not restricted to theepidermis because of thermaleffect. Tus good for dermaldisorders
Superficial ablation ofepidermal lesions
Termal effects Collagen shrinkage because ofthermal effect
Less thermal damage
Wound healing Prolonged wound healing due to
necrosis areas
Shorter healing time
Side effects More Less
*In human skin the depth of ablation peaks at 225–250 μm after 4 passes using 1–3 pulses, dose of
250–500 mJ (ultraPulse)
**the coagulation varies from 20 µm (1 pass) to 70 μm at 3–4 pass, maximum 100 μm
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
50/573
32 Lasers in Dermatological Practice
as in resurfacing, these subtle clinical signs are not seen. Also it must beunderstood that this also depends on the laser being used. If a UltraPulse
laser is used little residual thermal necrosis (less than 30 µm) exists, thusthe thermal reaction will not be sufficient to coagulate fine papillary vessels,and the tissue will be pink because of the visible capillary blood flow. Tis istypical of the appearance of the tissue after a single laser pass removing theepidermis. After a second or third laser pass, the laser reacting with the dermisleaves almost 70–100 µm of thermal necrosis thus leading to hemostasis, thusgiving a whitish appearance. If further passes are given a yellowish brownlook will actually indicate thermal injury ! Tus it is advisable as far as CO
2
lasers are concerned, that such signs should be abandoned and the laser
surgeon should aim at primarily ablating the dermatological indication,restricting the dose and settings to a maximum of 3–4 passes.
A few simple rules to follow are: 1. Use a pulsed laser or ultrapulse laser at the lowest dosage and pulse
duration. 2. Aim for ablation of the tumor first or level it down to the surrounding
skin. 3. A low energy and pulse duration will ensure erythema of the papillary
dermis, which is a reliable end point.
4. Do not aim for a yellowish discoloration, as that sign in most non-pulsedlasers is a reliable indicator of thermal necrosis!
ERBIUM:YAG LASER
Introduction
Te Erbium:YAG laser, with its wavelength of 2940 nm, is absorbed by water10 times more readily than the carbon dioxide laser (wavelength, 10,600 nm).
Consequently, it is absorbed more superficially within the skin, leading toextremely precise ablation of the epidermis and dermis (Fig. 2.4). Te threshold fluence required for clean ablation is 1.5 J/cm, compared
with 4–5 J/cm2 for the carbon dioxide laser. Te thermal relaxation time is 50μsec for the Erbium:YAG laser; the carbon dioxide R is 1 millisecond. Tethermal injury is markedly less for the erbium:YAG lasers. Te predictive depth (5 μm/J), the less thermal damage, the progressivedepth achieved and faster healing it is preferred, specially for mostdermatological indications. Newer modified Er:YAG have been invented to
bridge the gap between the tissue effects with added coagulation (Box 2.1) which is consequent to the variable pulse duration. Te principle employedis that if the pulse duration is less there is less coagulation while if the pulseduration is increased the coagulation increases. Tis can lead to variousdiverse settings (Fig. 2.5) and can closely approximate the CO
2 laser.
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
51/573
Ablative Lasers 33
Box 2.1 An overview of modulated Er:YAG lasers
Conventional Er:YAG Short-pulsed(250–350 μs)
1. Derma 20 (ESC Medical SystemsHaifa, Israel )
2. Continuum (ContinuumBiomedical Dublin, Calif)
3. Dermablate (Asclepion-MeditecInc, Jena, Germany)
Modulated Er:YAG Variable pulse(500 μs–10 ms)
Contour Sciton Laser Corp
Combined CO2 and Er:YAG
(50 ms/350 μs)Derma K ESC/Sharplan
Dual Mode* (350 μs/Termal mode
Dermablate MCL 30(Asclepion- Meditec Inc, Jena,Germany )(1μs 20 Hz)
Variable Pulse(100–1000 µs)
Dermablate MCL 31
* In the thermal mode, the frequency is firmly set to 20 Hz, which leads to rapid heating of tissue bysubablative pulses 2 (1 J/cm)
Fig. 2.4: Er:YAG ablation occurs after the threshold dose of about 1.8 J/cm2. Te dose
and settings indicate both linear depth and coagulative effect of modified Er:YAG
system
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
52/573
34 Lasers in Dermatological Practice
Laser-Tissue Interaction
Te short pulsed Er:YAG laser is a flashlamp-pumped yttrium-aluminum-garnet (YAG) crystal laser system doped with atoms of the element erbium.Laser energy is generated within a cavity containing the flashlamp-excited
YAG crystal rod, mirrors at each end, and a cooling system. On exiting thecavity, the laser light is focused into a beam delivery system that typicallyincorporates an articulated arm which allows the use of hand pieces capableof producing highly collimated beams. Erbium:YAG lasers used in cutaneousresurfacing typically have a bell-shaped Gaussian laser beam profile. Teerbium:yttrium-aluminum-garnet (Er:YAG) laser produces light in thenear-infrared (IR) portion of the electromagnetic spectrum at 2.94 µm. Tis
wavelength was discovered by Soviet researchers in 1975 and its clinical usedeveloped in Europe. Te broad water-absorption band extends from justunder 2 µm to beyond 10 µm, ensuring superficial absorption of near-IR light.
Te energy delivered by the Er:YAG laser with a pulse duration of 250 to350 µs is far below the 1 millisecond thermal relaxation time calculated forthat layer of human skin heated by the pulsed CO
2 laser. However, because
of the “short penetration depth” the laser heated tissue is only 1 µm thickand this has a R of 1 µm. Tus to minimize thermal damage the Er: YAGlaser emits approximately twenty 1 µs micropulses in a macropulse burst ofapproximately 200 µs.
In contrast to the CO2 laser, the Er:YAG laser has 16 times greater affinity
for water and a significantly lower tissue ablation threshold (1.6 J/cm2) whichallows the Er:YAG to be operated at 8 to 10 times above its ablation thresholdin most resurfacing applications. Terefore, most of the energy delivered withthe Er:YAG laser is used to ablate and the residual thermal damage (RD)
Fig. 2.5: Variable Pulse duration and the consequent tissue effect using
various modes (Er:YAG Dermablate 31)
8/18/2019 Lasers in Dermatological Practice [PDF] [UnitedVRG]
53/573
Ablative Lasers 35
is narrow. Te Er: YAG laser causes vasodilation of dermal blood vessel andcauses transudation of fluid that maintains enough water to ensure efficient
ablation. Te absence of coagulation results in bleeding as the vessels of thesuperficial dermal plexus are severed. Te unique advantage of the laser is minimum thermal damage butthe disadvantage is minimum coagulation. Tough modulated Er:YAGlasers with increasing pulse duration are useful, another option is to givesubablative pulses (Fig. 2.4 ) which will achieve coagulation, but no ablation.Most Er:YAG lasers have a ablation threshold 2 J/cm². At this flue

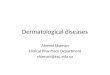


![Viva in Oral Surgery for Dental Students, 1E (2012) [UnitedVRG]](https://img.pdfslide.us/doc/110x75/577c7ea91a28abe054a20b7f/viva-in-oral-surgery-for-dental-students-1e-2012-pdfunitedvrg.jpg)
![Endocrine Pathology, 4E (2014) [UnitedVRG]](https://img.pdfslide.us/doc/110x75/577c7de31a28abe054a00b57/endocrine-pathology-4e-2014-pdf-unitedvrg.jpg)




![Ramadan and Diabetes Care (2014) [UnitedVRG].pdf](https://img.pdfslide.us/doc/110x75/577ca58c1a28abea748b94fd/ramadan-and-diabetes-care-2014-pdf-unitedvrgpdf.jpg)
![Chassin's Operative Strategy in Colon and Rectal Surgery,(2006) [UnitedVRG]](https://img.pdfslide.us/doc/110x75/56d6c06f1a28ab30169a63d7/chassins-operative-strategy-in-colon-and-rectal-surgery2006-unitedvrg.jpg)
![Jaypee Gold Standard Mini Atlas Series® Embryology (2010) [UnitedVRG]](https://img.pdfslide.us/doc/110x75/5695d4de1a28ab9b02a31b00/jaypee-gold-standard-mini-atlas-series-embryology-2010-pdf-unitedvrg.jpg)
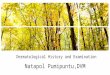

![Pocket Tutor Understanding ABGs and Lung Function Tests (2012) [UnitedVRG]](https://img.pdfslide.us/doc/110x75/55cf8f07550346703b9830c6/pocket-tutor-understanding-abgs-and-lung-function-tests-2012-pdf-unitedvrg.jpg)
![Jaypee Gold Standard Mini Atlas Series Pe-dodontics (2008) [UnitedVRG]](https://img.pdfslide.us/doc/110x75/577cc19d1a28aba7119377c8/jaypee-gold-standard-mini-atlas-series-pe-dodontics-2008-pdf-unitedvrg.jpg)




![Radiology 101 the Basics & Fundamentals of Imaging - 4E [UnitedVRG]](https://img.pdfslide.us/doc/110x75/577c86ac1a28abe054c2290f/radiology-101-the-basics-fundamentals-of-imaging-4e-pdf-unitedvrg.jpg)





![Principles of oral and maxillofacial surgery, 6 e (2011) [unitedvrg]](https://img.pdfslide.us/doc/110x75/55c46e40bb61eb020d8b45da/principles-of-oral-and-maxillofacial-surgery-6-e-2011-pdf-unitedvrg.jpg)
![Textbook of Dental Anatomy, Physiology and Occlusion, 1E (2014) [UnitedVRG]](https://img.pdfslide.us/doc/110x75/5695d3d81a28ab9b029f6402/textbook-of-dental-anatomy-physiology-and-occlusion-1e-2014-pdfunitedvrg.jpg)
![Davis's NCLEX-RN® Success 3E (2012) [UnitedVRG]](https://img.pdfslide.us/doc/110x75/577cbfe01a28aba7118e56bf/daviss-nclex-rn-success-3e-2012-pdf-unitedvrg.jpg)