Embed Size (px)
Citation preview
A
K
ehnke
u
WM
1d
Original article
Large Arterial Elasticity Varies as a Function of Gender and Racism-Related Vigilance in Black Youth
Rodney Clark, Ph.D.,a,† Ramona A. Benkert, Ph.D., A.P.R.N., B.C.,b,* andJohn M. Flack, M.D., M.P.H.c
aDepartment of Psychology, Wayne State University, Detroit, MichiganbCollege of Nursing, Wayne State University, Detroit, Michigan
cDepartment of Internal Medicine, School of Medicine, Wayne State University, Detroit, Michigan
Manuscript received July 15, 2005; manuscript accepted February 23, 2006
bstract Background: This exploratory study examined the relationship of gender and racism-relatedvigilance to baseline and task-induced changes in large arterial elasticity (LAE).Methods: The convenience sample consisted of 153 black youth (M age � 11.5 years, SD � 1.4)who were normotensive. Large arterial elasticity was measured via pulse wave contour analysis,before, during, and after a sequentially administered digit forward and digit backward task.Racism-related vigilance was reported by participants.Results: Although findings from general linear models indicated that the independent effects ofgender and racism-related vigilance were not significantly related to LAE (baseline, reactivity, orrecovery) (all p � .05), these analyses showed that gender and racism-related vigilance interactedto predict baseline LAE (p � .02) and task-induced changes (reactivity only) in LAE (p � .006).Follow-up regression analyses explicating the pattern of these interaction effects indicated that 1)racism-related vigilance was marginally and inversely related to baseline LAE among boys (p �.06) but not in girls (p � .21); and, 2) racism-related vigilance was positively and significantlyassociated with task-induced changes (reactivity) in LAE among boys (p � .008) but not in girls (p� .30).Conclusions: The relationship between racism-related vigilance and LAE varies as a function ofgender, and may have longer-term implications for between and within-group disparities in cardio-vascular health. © 2006 Society for Adolescent Medicine. All rights reserved.
Journal of Adolescent Health 39 (2006) 562–569
eywords: Racism; Vigilance; Gender; Arterial elasticity; Black youth
amactaoc
ceb
Primary hypertension (HTN) afflicts nearly one out ofvery three adults in the United States [1], with Blacksaving disproportionately higher rates than other major eth-ic groups [2]. Although the cause of HTN remains un-nown, the precursors of this prevalent disorder emerge asarly as adolescence [3]. Large arterial elasticity (LAE) is
†This article is dedicated to the memory of Dr. Clark, who diednexpectedly in May 2006.
*Address correspondence to: Dr. Ramona Benkert, College of Nursing,ayne State University, 5557 Cass Avenue, 370 Cohn Building, Detroit,I 48202.
rE-mail address: [email protected]
054-139X/06/$ – see front matter © 2006 Society for Adolescent Medicine. Alloi:10.1016/j.jadohealth.2006.02.012
n important factor in hemodynamic health, and compro-ised elasticity, due to stress or disease, affects not only
rterial dynamics but also myocardial functioning. De-reased arterial elasticity is one biological index of endo-helial dysfunction that precedes cardiovascular events andtherosclerosis [4,5], and might help to identify subgroupsf individuals who are at higher risk of developing suchonditions as HTN [6].
Although the causal role of psychological stress-inducedardiovascular reactivity (reactivity) and post-stress recov-ry (recovery) to arterial dysfunction continues to be de-ated [7], prospective studies indicate that reactivity and
ecovery predict changes in blood pressure status [8] (i.e.,rights reserved.

nbvococsscp
iwsalbstpfaicaol
aytbsosedisea
leicivafgepm
iv
tboiptgoasidsILa
M
S
y2tffwgtlwdaebnwfltrplgtnaf
w
563R. Clark et al. / Journal of Adolescent Health 39 (2006) 562–569
ormal, high-normal, and hypertensive), and differentiateetween individuals at increased risk for negative cardio-ascular events [9]. For instance, in a normotensive samplef black and white young adults, reactivity to psychologicalhallenges predicted blood pressure status during 13 yearsf follow-up [8]. Schuler and O’Brien [10] also found re-overy to distinguish between blood pressure status groupsuch that delayed recovery was observed among hyperten-ive but not normotensive participants. Reactivity and re-overy have been hypothesized to reflect psychological andhysiological mechanisms that are clinically relevant [9,11].
Vigilance, the tendency to attend to a stressor that is notmmediately present, is one psychological mechanismhose relationship to arterial functioning warrants further
tudy. As a psychological predisposition that is activated innticipation of or in response to perceived stressors, vigi-ance might increase the risk for adverse arterial outcomesy way of more marked and protracted activation of theympathetic nervous system [11–13]. In one study that usedhe Social Competence Interview to assess vigilance to aersisting individual-level stressor in youth, Ewart et al [14]ound that vigilance elicited pronounced vascular reactivitynd resistance. If chronically occurring, this vigilance-nduced reactivity and resistance has the potential to in-rease vascular sensitivity (e.g., arterial elasticity) to thedverse effects of arterial pressure [4] and the eventualnset of HTN [11] via elevated prevailing blood pressureevels [15].
Research indicates that racism is a persisting, individual-nd group-level stressor to which many Blacks, includingouth, are exposed [16–19]. Although sympathetic activa-ion is the predominant physiological mechanism triggeredy such psychological stressors as perceived racism [20,21],ympathetic activation has complex and competing effectsn conduit artery vasomotor tone, including direct vasocon-trictor effects on vascular smooth muscle and vasodilatorffects influenced by endothelial-dependent and indepen-ent processes [22]. Studies differ as to whether psycholog-cal stress impairs endothelial-dependent vasodilator re-ponses [22,23]. A recent study by Gottdiener et al [24], forxample, found that psychological stress was positivelyssociated with reactivity and arterial vasodilation.
As a psychological predisposition that might be particu-arly relevant for Blacks, given the group’s disproportionatexposure to racism, racism-related vigilance, operational-zed as the propensity to attend to environmental events thatould be perceived as involving racism, might help to clar-fy the relationship of vigilance to vasoconstriction andasodilation in this group. Moreover, if perceived racismnd racism-related stress are greater for black males thanemales, as some [25–27] but not all [28,29] research sug-ests; if gender differences in arterial elasticity emerge asarly as adolescence [30]; and, if the relationship betweensychological predispositions and arterial functioning is
itigated by such constitutional factors as gender [31–33], pt is possible that the vascular correlates of racism-relatedigilance vary as a function of gender.
This study extends the current knowledge base in at leastwo ways. First, as opposed to examining the relationshipetween racism-related vigilance and such cardiovascularutcomes as the prevalence or incidence of HTN, this studynvestigates the association of racism-related vigilance to areclinical index of cardiovascular dysfunction. Second,his will be the first known study to explore the effects ofender and racism-related vigilance to LAE. This researchffers an opportunity to help explicate the probable mech-nisms involved in perceived racism ‘getting under thekin,’ which might increase the risk of more negative phys-ological profiles, long before structural changes and car-iovascular disease are established. The two primary re-earch questions for this exploratory study are as follows: 1)s racism-related vigilance an independent predictor ofAE; and 2) Do racism-related vigilance and gender inter-ct to predict LAE?
ethods
tudy Population
The convenience sample for this study included 153outh (girls: 48%, n � 74) who were drawn from a pool of25 black students who are participating in a larger longi-udinal study, which examines correlates of biobehavioralunctioning in black youth. The larger cohort was recruitedrom three elementary/middle schools in an urban, Mid-estern city. Potential youth participants who were able toive informed assent and parent participants who were ableo give informed consent were eligible to take part in thearger study, and potential youth or parent participants whoere taking medication for a psychotic disorder, bipolarisorder, or dementia, or who reported being diagnosed withpsychotic disorder, bipolar disorder, or dementia were not
ligible for participation in the larger study. Additionally,ecause the current investigation was interested in LAE in aormotensive sample, 72 participants from the larger studyho had elevated blood pressure, per published guidelines
or youth (i.e., average systolic and diastolic blood pressureevels above the 90th percentile) [3,34], were excluded fromhe analyses. T-test and chi-square analyses indicated thatelative to participants who were included in the analyses,articipants who were excluded from the analyses had aower BMI (p � .0001), were older (p � .04), and had areater proportion of girls (p � .05). Prescription medica-ions use and racism-related vigilance scores were not sig-ificantly different for participants who were included in thenalyses compared with participants who were excludedrom the analyses (both p � .59).
With average systolic and diastolic pressure levels thatere within normal limits, per parent report, none of the
articipants in the current study were taking prescription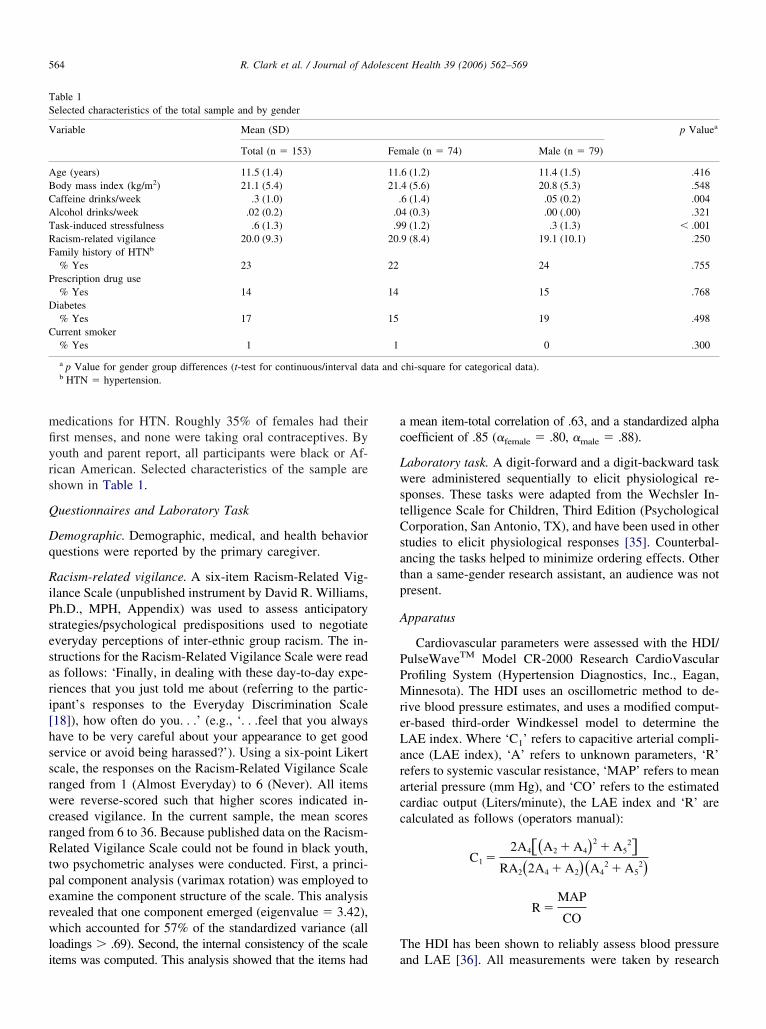
mfiyrs
Q
Dq
RiPsesari[hssrwcrRtperwli
ac
LwstCsatp
A
PPMreLaracc
T
TS
V
ABCATRF
P
D
C
564 R. Clark et al. / Journal of Adolescent Health 39 (2006) 562–569
edications for HTN. Roughly 35% of females had theirrst menses, and none were taking oral contraceptives. Byouth and parent report, all participants were black or Af-ican American. Selected characteristics of the sample arehown in Table 1.
uestionnaires and Laboratory Task
emographic. Demographic, medical, and health behavioruestions were reported by the primary caregiver.
acism-related vigilance. A six-item Racism-Related Vig-lance Scale (unpublished instrument by David R. Williams,h.D., MPH, Appendix) was used to assess anticipatorytrategies/psychological predispositions used to negotiateveryday perceptions of inter-ethnic group racism. The in-tructions for the Racism-Related Vigilance Scale were reads follows: ‘Finally, in dealing with these day-to-day expe-iences that you just told me about (referring to the partic-pant’s responses to the Everyday Discrimination Scale18]), how often do you. . .’ (e.g., ‘. . .feel that you alwaysave to be very careful about your appearance to get goodervice or avoid being harassed?’). Using a six-point Likertcale, the responses on the Racism-Related Vigilance Scaleanged from 1 (Almost Everyday) to 6 (Never). All itemsere reverse-scored such that higher scores indicated in-
reased vigilance. In the current sample, the mean scoresanged from 6 to 36. Because published data on the Racism-elated Vigilance Scale could not be found in black youth,
wo psychometric analyses were conducted. First, a princi-al component analysis (varimax rotation) was employed toxamine the component structure of the scale. This analysisevealed that one component emerged (eigenvalue � 3.42),hich accounted for 57% of the standardized variance (all
oadings � .69). Second, the internal consistency of the scale
able 1elected characteristics of the total sample and by gender
ariable Mean (SD)
Total (n � 153)
ge (years) 11.5 (1.4)ody mass index (kg/m2) 21.1 (5.4)affeine drinks/week .3 (1.0)lcohol drinks/week .02 (0.2)ask-induced stressfulness .6 (1.3)acism-related vigilance 20.0 (9.3)amily history of HTNb
% Yes 23rescription drug use% Yes 14
iabetes% Yes 17
urrent smoker% Yes 1
a p Value for gender group differences (t-test for continuous/interval dab HTN � hypertension.
tems was computed. This analysis showed that the items had a
mean item-total correlation of .63, and a standardized alphaoefficient of .85 (�female � .80, �male � .88).
aboratory task. A digit-forward and a digit-backward taskere administered sequentially to elicit physiological re-
ponses. These tasks were adapted from the Wechsler In-elligence Scale for Children, Third Edition (Psychologicalorporation, San Antonio, TX), and have been used in other
tudies to elicit physiological responses [35]. Counterbal-ncing the tasks helped to minimize ordering effects. Otherhan a same-gender research assistant, an audience was notresent.
pparatus
Cardiovascular parameters were assessed with the HDI/ulseWaveTM Model CR-2000 Research CardioVascularrofiling System (Hypertension Diagnostics, Inc., Eagan,innesota). The HDI uses an oscillometric method to de-
ive blood pressure estimates, and uses a modified comput-r-based third-order Windkessel model to determine theAE index. Where ‘C1’ refers to capacitive arterial compli-nce (LAE index), ‘A’ refers to unknown parameters, ‘R’efers to systemic vascular resistance, ‘MAP’ refers to meanrterial pressure (mm Hg), and ‘CO’ refers to the estimatedardiac output (Liters/minute), the LAE index and ‘R’ arealculated as follows (operators manual):
C1 �2A4��A2 � A4�2
� A52�
RA2�2A4 � A2��A42 � A5
2�
R �MAP
CO
he HDI has been shown to reliably assess blood pressure
p Valuea
ale (n � 74) Male (n � 79)
6 (1.2) 11.4 (1.5) .4164 (5.6) 20.8 (5.3) .5486 (1.4) .05 (0.2) .0044 (0.3) .00 (.00) .3219 (1.2) .3 (1.3) � .0019 (8.4) 19.1 (10.1) .250
24 .755
15 .768
19 .498
0 .300
chi-square for categorical data).
Fem
11.21.
..0.9
20.
22
14
15
1
ta and
nd LAE [36]. All measurements were taken by research

ao
P
ratiaqgrtapaaawptanoamd
D
OrmDmtroC(t
P2wmrgomseavb
alttds
A8spertteTvheidpwvwpfsm�d(
R
D
tv.wspaos
M
ise
565R. Clark et al. / Journal of Adolescent Health 39 (2006) 562–569
ssistants of the same gender and ethnicity who were trainedn the apparatus.
rocedure
Students who had informed parental consent (83% returnate) were scheduled for psychosocial and physiologicalssessments in designated rooms at the school. On average,he psychosocial assessment was separated from the phys-ological assessment by 2.5 weeks. During the psychosocialssessment, informed assent was secured from students, anduestionnaire instructions and items were read aloud in aroup format by a research assistant. Students were told toefrain from consuming caffeine products six hours beforehe physiological assessment. The research assistant placed
blood pressure cuff on the upper portion of the partici-ant’s nondominant arm to take cardiovascular assessments,nd placed a calibrated proprietary tonometer on the radialrtery (approximately one inch below the wrist) of the samerm. The tonometer was held in place with a wrist stabilizer,hich minimized movement artifacts. To verify accuratelacement of the tonometer, reliability checks (observinghe wave form and signal strength) were conducted beforessessments were taken. Manual adjustments were made aseeded. After the task period, participants completed a sec-nd set of visual analog scales. The larger investigation waspproved by the University’s Human Investigation Com-ittee, including the questionnaires and reactivity protocol
escribed herein.
ata Reduction and Analyses
utcome variables. Throughout the 10-minute baseline pe-iod, five LAE measurements were taken every otherinute, and were averaged to obtain mean baseline levels.uring the three-minute task period, the three LAE assess-ents were assessed every other minute, and were averaged
o determine mean task levels. For the 12-minute post-taskecovery period, the six LAE measurements taken everyther minute were averaged to obtain mean recovery levels.hange scores (task level minus baseline level), � LAE
reactivity and recovery), were then calculated and used ashe outcome variables in the analyses.
redictor variables. Gender (dummy coded as 1 for boys orfor girls) and the raw score for racism-related vigilanceere the primary predictor variables in the general linearodels. Multiplying the relevant gender (class variable) and
acism-related vigilance score (interval variable) created theender by racism-related vigilance interaction term. Basedn prior research and clinical knowledge [11,37], age, bodyass index, prescription drug use (e.g., albuterol, cromolyn
odium, fexofenadine, loratadine, methyphenidate, parox-tine HCL, and risperidone), and the period-specific systolicnd diastolic blood pressure variables were used as controlariables in the general linear models. The period-specific
lood pressure control variables included baseline systolic and diastolic blood pressure in the model predicting base-ine LAE and � systolic and diastolic blood pressure (reac-ivity and recovery) in the models predicting � LAE (reac-ivity and recovery). The change scores (�) for systolic andiastolic blood pressure were assessed and calculated in theame manner described above for LAE.
nalyses. Statistical analyses were computed using SAS.01 (SAS Institute, Inc., Cary, North Carolina). Usingelected cardiovascular parameters (LAE, systolic bloodressure, diastolic blood pressure, mean arterial pressure,stimated cardiac output, pulse rate, and systemic vascularesistance) as outcome variables, a repeated measures mul-ivariate analysis of variance was conducted to determine ifhe laboratory protocol elicited the desired cardiovascularffects across the baseline, reactivity, and recovery periods.o examine the relationship of gender and racism-relatedigilance to LAE (baseline, reactivity, and recovery), threeierarchical general linear models were used. In each gen-ral linear model, the control variables (age, body massndex, prescription drug use, systolic blood pressure, andiastolic blood pressure) were entered in Step 1; the primaryredictor variables (gender and racism-related vigilance)ere entered in Step 2; and, the gender by racism-relatedigilance interaction term was entered in Step 3. Consistentith procedures described by Aiken and West [38], theattern of significant interaction effects were explored withollow-up regression models. The criterion of statisticalignificance in these models was p � .05. Because ofissing outcome data for the baseline (n � 3), reactivity (n
3), and recovery (n � 7) periods, the corrected totalegrees of freedom for the general linear models were 150baseline and reactivity) and 146 (recovery).
esults
escriptive and Bivariate Analyses
As shown in Table 1, a t-test analysis indicated that thewo primary predictor variables, gender and racism-relatedigilance, were not significantly related to one another (p �25). Also illustrated in Table 1, t-test analyses revealed thatith the exception of higher subjective stress and caffeine
cores in girls compared with boys (both p � .004), therimary predictor variables were not significantly related toge, body mass index, alcohol drinks/week, family historyf hypertension, prescription drug use, diabetes status, ormoking status (all p � .30).
ultivariate Analysis of Variance: Time Effects
The repeated measures multivariate analysis of variancendicated that the laboratory protocol was associated with aignificant (overall) time effect (baseline, task, and recov-ry) for boys, Wilks’ Lambda F(14,61) � 7.10, p � .0001,
nd girls, Wilks’ Lambda F(14,56) � 3.18, p � .001.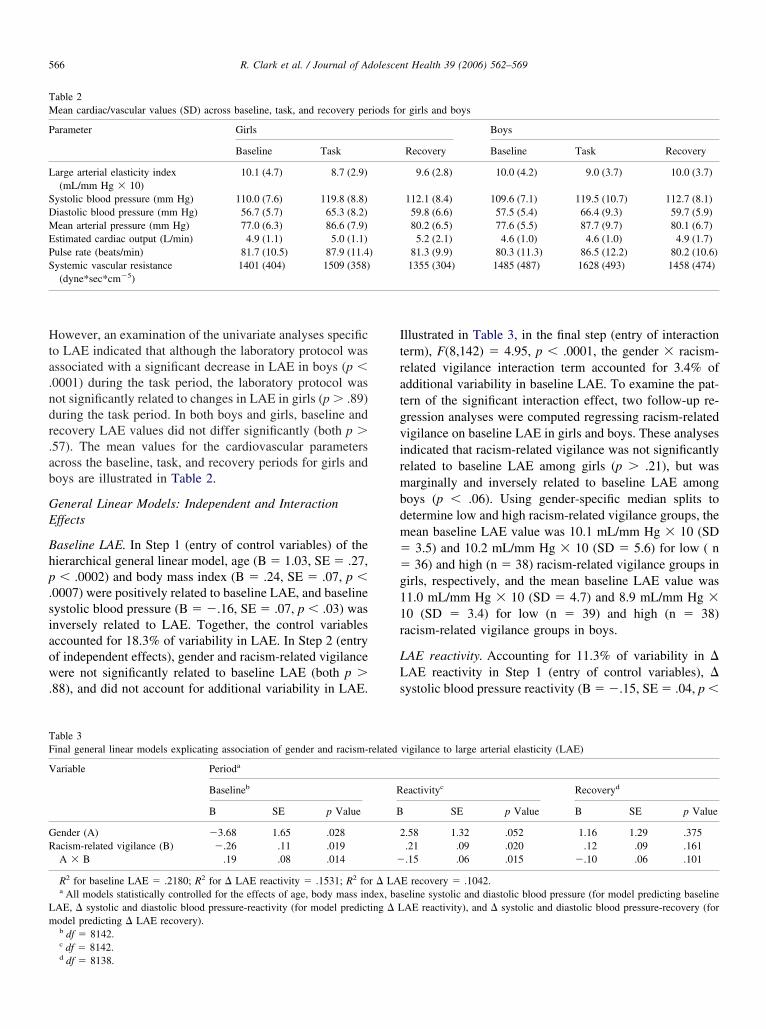
Hta.ndr.ab
GE
Bhp.siaow.
Itratgvirmbdm��g11r
LLs
TM
P
L
SDMEPS
TF
V
GR
Lm
566 R. Clark et al. / Journal of Adolescent Health 39 (2006) 562–569
owever, an examination of the univariate analyses specifico LAE indicated that although the laboratory protocol wasssociated with a significant decrease in LAE in boys (p �0001) during the task period, the laboratory protocol wasot significantly related to changes in LAE in girls (p � .89)uring the task period. In both boys and girls, baseline andecovery LAE values did not differ significantly (both p �57). The mean values for the cardiovascular parameterscross the baseline, task, and recovery periods for girls andoys are illustrated in Table 2.
eneral Linear Models: Independent and Interactionffects
aseline LAE. In Step 1 (entry of control variables) of theierarchical general linear model, age (B � 1.03, SE � .27,� .0002) and body mass index (B � .24, SE � .07, p �
0007) were positively related to baseline LAE, and baselineystolic blood pressure (B � �.16, SE � .07, p � .03) wasnversely related to LAE. Together, the control variablesccounted for 18.3% of variability in LAE. In Step 2 (entryf independent effects), gender and racism-related vigilanceere not significantly related to baseline LAE (both p �
88), and did not account for additional variability in LAE.
able 2ean cardiac/vascular values (SD) across baseline, task, and recovery per
arameter Girls
Baseline Task
arge arterial elasticity index(mL/mm Hg � 10)
10.1 (4.7) 8.7 (2.9)
ystolic blood pressure (mm Hg) 110.0 (7.6) 119.8 (8.8)iastolic blood pressure (mm Hg) 56.7 (5.7) 65.3 (8.2)ean arterial pressure (mm Hg) 77.0 (6.3) 86.6 (7.9)
stimated cardiac output (L/min) 4.9 (1.1) 5.0 (1.1)ulse rate (beats/min) 81.7 (10.5) 87.9 (11.4ystemic vascular resistance(dyne*sec*cm�5)
1401 (404) 1509 (358)
able 3inal general linear models explicating association of gender and racism-
ariable Perioda
Baselineb
B SE p Value
ender (A) �3.68 1.65 .028acism-related vigilance (B) �.26 .11 .019A � B .19 .08 .014
R2 for baseline LAE � .2180; R2 for � LAE reactivity � .1531; R2 foa All models statistically controlled for the effects of age, body mass in
AE, � systolic and diastolic blood pressure-reactivity (for model predictodel predicting � LAE recovery).b df � 8142.c df � 8142.
d df � 8138.llustrated in Table 3, in the final step (entry of interactionerm), F(8,142) � 4.95, p � .0001, the gender � racism-elated vigilance interaction term accounted for 3.4% ofdditional variability in baseline LAE. To examine the pat-ern of the significant interaction effect, two follow-up re-ression analyses were computed regressing racism-relatedigilance on baseline LAE in girls and boys. These analysesndicated that racism-related vigilance was not significantlyelated to baseline LAE among girls (p � .21), but wasarginally and inversely related to baseline LAE among
oys (p � .06). Using gender-specific median splits toetermine low and high racism-related vigilance groups, theean baseline LAE value was 10.1 mL/mm Hg � 10 (SD3.5) and 10.2 mL/mm Hg � 10 (SD � 5.6) for low ( n36) and high (n � 38) racism-related vigilance groups in
irls, respectively, and the mean baseline LAE value was1.0 mL/mm Hg � 10 (SD � 4.7) and 8.9 mL/mm Hg �0 (SD � 3.4) for low (n � 39) and high (n � 38)acism-related vigilance groups in boys.
AE reactivity. Accounting for 11.3% of variability in �AE reactivity in Step 1 (entry of control variables), �ystolic blood pressure reactivity (B � �.15, SE � .04, p �
r girls and boys
Boys
Recovery Baseline Task Recovery
9.6 (2.8) 10.0 (4.2) 9.0 (3.7) 10.0 (3.7)
112.1 (8.4) 109.6 (7.1) 119.5 (10.7) 112.7 (8.1)59.8 (6.6) 57.5 (5.4) 66.4 (9.3) 59.7 (5.9)80.2 (6.5) 77.6 (5.5) 87.7 (9.7) 80.1 (6.7)
5.2 (2.1) 4.6 (1.0) 4.6 (1.0) 4.9 (1.7)81.3 (9.9) 80.3 (11.3) 86.5 (12.2) 80.2 (10.6)
1355 (304) 1485 (487) 1628 (493) 1458 (474)
vigilance to large arterial elasticity (LAE)
eactivityc Recoveryd
SE p Value B SE p Value
.58 1.32 .052 1.16 1.29 .375
.21 .09 .020 .12 .09 .161
.15 .06 .015 �.10 .06 .101
E recovery � .1042.eline systolic and diastolic blood pressure (for model predicting baselineAE reactivity), and � systolic and diastolic blood pressure-recovery (for
iods fo
)
related
R
B
2
�
r � LAdex, basing � L

.��iw(iI.w3gwrnbrsar�hr��r
Ls.d.cLesStr2
D
ibtttwatcse
actltsi
daiSrmrltirieau
t[twcmaasbvtTafdibhpl
tipaFabp
567R. Clark et al. / Journal of Adolescent Health 39 (2006) 562–569
0008) was inversely associated with � LAE reactivity, anddiastolic blood pressure reactivity (B � .19, SE � .05, p.0007) was positively related to � LAE reactivity. The
ndependent effects of gender and racism-related vigilanceere not significantly associated with � LAE reactivity
both p � .46), and did not account for additional variabilityn � LAE reactivity in Step 2 (entry of independent effects).n Step 3 (entry of interaction term), F(8,142) � 3.21, p �003, the gender � racism-related vigilance interaction termas significant (Table 3), and accounted for an additional.6% of variability in � LAE reactivity. The significantender by racism-related vigilance effect was examinedith two follow-up regression models in girls and boys. The
esults indicated that racism-related vigilance was not sig-ificantly related to � LAE reactivity among girls (p � .30),ut was positively and significantly associated with � LAEeactivity among boys (p � .008). Using the same gender-pecific median splits referenced above to determine lownd high racism-related vigilance groups, the mean � LAEeactivity value was �0.9 mL/mm Hg � 10 (SD � 3.2) and2.0 mL/mm Hg � 10 (SD � 5.2) for low (n � 36) and
igh (n � 38) racism-related vigilance groups in girls,espectively, and the mean � LAE reactivity value was1.5 mL/mm Hg � 10 (SD � 1.6) and �0.4 mL/mm Hg10 (SD � 2.3) for low (n � 39) and high (n � 38)
acism-related vigilance groups in boys.
AE recovery. In Step 1 (entry of control variables), �ystolic blood pressure recovery (B � �.15, SE � .06, p �02) was inversely associated with � LAE recovery, and �iastolic blood pressure recovery (B � .17, SE � .08, p �03) was positively related to � LAE recovery. Together, theontrol variables accounted for 7.0% of variability in �AE recovery. In Step 2 (entry of independent effects), theffects of gender and racism-related vigilance were notignificant predictors of � LAE recovery (both p � .14).imilarly, the gender � racism-related vigilance interaction
erm in Step 3 was not significantly associated with � LAEecovery. The results from this final model, F(8,138) �.01, p�.050, are shown in Table 3.
iscussion
This study explored the relationship of gender and rac-sm-related vigilance to LAE in a normotensive sample oflack youth. Overall, the laboratory task used in this inves-igation was associated with increased cardiovascular func-ioning (i.e., blood pressure, pulse rate, and vascular resis-ance) in both boys and girls. Consistent with Tsai et al [39],ho examined hemodynamic and arterial properties associ-
ted with mental stress in normotensives and mild hyper-ensives, this task was also related to a statistically signifi-ant decrease in arterial elasticity among boys in the presenttudy. Future studies should explore the possible mitigating
ffects of sex steroids on the association between gender tnd task-induced changes in LAE. That is, if the increasedirculation of sex steroids associated with puberty is relatedo more elastic large arteries in girls and with less elasticarge arteries in boys [30], gender might serve as a proxy forhe presence of sex steroids (estrogen and testosterone)—teroids whose effects have the potential to modulate task-nduced changes in LAE.
Gender and racism-related vigilance were not indepen-ent predictors of LAE in this study. Rather, LAE (baselinend reactivity) was shown to vary as a function of thenteractive effects of gender and racism-related vigilance.pecifically, a significant relationship between racism-elated vigilance to LAE was relegated to boys. If theagnitude and duration of stress-induced reactivity and
ecovery are influenced by multiple physiological, psycho-ogical, and constitutional factors, which in turn are positedo increase the risk of cardiac/vascular dysfunction [6,11], its probable that the association of gender (and racism-elated vigilance) to arterial functioning depends on thenteractive effects of these factors [40]. Future researchxploring the predictive utility of these interactive effects torterial functioning across different laboratory tasks andsing ambulatory measurements is suggested.
Similar to studies indicating that the tendency to attendo perceived threats is associated with vascular parameters14], the findings in this study (re: baseline LAE) suggesthat more chronic perceptions of these threats are associatedith the development of cardiovascular dysfunction in pre-
linical boys. Given select research showing that 1) blackales tend to perceive more racism than black females [18];
nd 2) psychological predispositions that are related to moredaptive cardiovascular outcomes in black females are as-ociated with less adaptive cardiovascular outcomes inlack males [31,32], the cumulative effect of racism-relatedigilance-induced sympathetic activation on arterial func-ioning in black males might become more compromised.hat is, it is possible that the magnitude and duration ofnticipatory stress-induced sympathetic activation vary as aunction of gender. Over time, this sympathetic activationifferential might contribute to relatively more endothelialmpairment (e.g., decreased resting LAE) and elevatedlood pressure in males compared with females. This postoc explanation is consonant with research indicating thatsychological stress impairs endothelial-dependent vasodi-ator responses [22].
The observation in the current study of a positive rela-ionship between racism-related vigilance and LAE reactiv-ty underscores the need for additional research exploringlausible mechanistic pathways by which perceived racismnd associated anticipatory strategies ‘get under the skin.’or example, it is possible that the increased stress-inducedrterial responsiveness seen in this investigation amongoys high in racism-related vigilance is more adaptive (i.e.,rospectively associated with increased resting LAE) than
he blunted responsiveness seen among boys low in racism-
rdtpt
Ftrommiaetatdnetc
A
nMIgBd
A
UW
ey
a
h
yr
R
[
[
[
[
[
[
[
[
568 R. Clark et al. / Journal of Adolescent Health 39 (2006) 562–569
elated vigilance. It is also possible that a more vigilantisposition better enables black boys to avoid or minimizehe untoward psychological effects associated with sucherceived threats as racism, thereby favorably contributingo arterial muscle tone.
Several methodological caveats should be considered.irst, the cross-sectional study design precluded causal in-
erpretations of the relationship of gender and racism-elated vigilance to LAE. Second, although a task effect wasbserved, a lengthier task period and multiple assessmentsight have further increased the reliability of the measure-ents. Third, the unique variability accounted for by the
nteraction terms was only equivalent to a small effect size,nd underscores the need for additional research. Fourth,ven though the noninvasive measurement of arterial elas-icity with the HDI has been shown to be a reliable and validssessment tool [36], additional psychometric and norma-ive data are needed, especially with youth. Psychometricata for the racism-related vigilance measure are alsoeeded. The aforementioned caveats notwithstanding, thisxploratory study highlights the potential longer-term con-ribution of constitutional and psychological parameters toardiovascular health in black youth.
cknowledgments
Preparation of this manuscript was supported by grantumbers 1 K01 MH01867 from the National Institute ofental Health and S P50 ES012395 from the National
nstitute of Environmental Health Sciences. The authors arerateful to Lesley Goins, Charles Williams, Karen Freeman,rian Pitts, Jr., and Abraham Hagos for their assistance withata collection and entry.
ppendix
npublished racism-related vigilance scale of D.R.illiams, Ph.D.
Instructions: Finally, in dealing with these day-to-dayxperiences that you just told me about, how often doou . . .
Response Scale: Almost everyday (1)At least once a week (2)A few times a month (3)A few times a year (4)Less than once a year (5)Never (6)Questions:1) . . . think in advance about the kinds of problems you
re likely to experience?2) . . . try to prepare for possible insults before leaving
ome?
3) . . . feel that you always have to be very careful aboutour appearance (to get good service or avoid being ha-assed)?
4) . . . carefully watch what you say and how you say it?5) . . . carefully observe what happens around you?6) . . . try to avoid certain social situations and places?
eferences
[1] Fields LE, Burt VL, Cutler JA, et al. The burden of adult hypertensionin the United States 1999 to 2000: a rising tide. Hypertension 2004;44:398–404.
[2] National Center for Health Statistics. Health, United States, 2003.Hyattsville, MD: U.S. Government Printing Office, 2003.
[3] National Heart, Lung, and Blood Institute. NIH Publication No.96-3790. Hyattsville, MD: U.S. Government Printing Office, 1996.
[4] Cohn JN. Pathophysiologic and prognostic implications of measuringarterial compliance in hypertensive disease. Prog Cardiovasc Dis1999;41:441–50.
[5] Gosse P, Lasserre R, Minifie C, et al. Arterial stiffness evaluated bymeasurement of the QKD interval is an independent predictor ofcardiovascular events. Am J Hypertens 2005;18:470–6.
[6] Harris KF, Matthews KA. Interactions between autonomic nervoussystem activity and endothelial function: a model for the developmentof cardiovascular disease. Psychosom Med 2004;66:153–64.
[7] Treiber FA, Kamarck T, Schneiderman N, et al. Cardiovascularreactivity and development of preclinical and clinical disease states.Psychosom Med 2003;65:46–62.
[8] Matthews KA, Katholi CR, McCreath H, et al. Blood pressure reac-tivity to psychological stress predicts hypertension in the CARDIAstudy. Circulation 2004;110:74–8.
[9] Haynes SN, Gannon LR, Orimoto L, et al. Psychophysiologicalassessment of post-stress recovery. Psychol Assess 1991;3:356–65.
10] Schuler JLH, O’Brien WH. Cardiovascular recovery from stress andhypertension risk factors: a meta-analytic review. Psychophysiology1997;34:649–59.
11] Anderson NB, McNeilly M, Myers H. Autonomic reactivity andhypertension in Blacks: a review and proposed model. Ethn Dis1991;1:154–70.
12] Schneider GM, Jacobs DW, Gevirtz RN, et al. Cardiovascular hemo-dynamic response to repeated mental stress in normotensive subjectsat genetic risk of hypertension: evidence of enhanced reactivity,blunted adaptation, and delayed recovery. J Hum Hypertens 2003;17:829–40.
13] Smith TW, Ruiz JM, Uchino BN. Vigilance, active coping, andcardiovascular reactivity during social interaction in young men.Health Psychol 2000;19:382–92.
14] Ewart CK, Jorgensen RS, Schroder KE, et al. Vigilance to a persistingpersonal threat: unmasking cardiovascular consequences in adoles-cents with the Social Competence Interview. Psychophysiology 2004;41:799–804.
15] Ewart CK, Kolodner KB. Negative affect, gender, and expressivestyle predict ambulatory blood pressure in adolescents. J Person SocPsychol 1994;66:596–605.
16] Scott LD Jr. Correlates of coping with perceived discriminatoryexperiences among African American adolescents. J Adolesc 2004;27:123–37.
17] Clark R. Significance of perceived racism: toward understandingethnic-group disparities in health, the later years. In: Anderson NB,Bulatao RA, Cohen B, eds. Critical Perspectives on Racial and EthnicDifferences in Health in Late Life. National Research Council, Panelon Race, Ethnicity and Health in Later Life. Committee on Popula-tion. Division of Behavioral and Social Sciences and Education
Washington, DC: National Academies Press, 2004: 540–66.
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
569R. Clark et al. / Journal of Adolescent Health 39 (2006) 562–569
18] Forman TA, Williams DR, Jackson JS. Race, place, and discrimina-tion. Perspect Soc Prob 1997;9:231–61.
19] Clark R, Coleman AP, Novak JD. Initial psychometric properties ofthe Everyday Discrimination Scale in Black adolescents. J Adolesc2004;27:363–8.
20] Harrell JP, Hall S, Taliaferro J. Physiological responses to racism anddiscrimination: an assessment of the evidence. Am J Public Health2003;93:243–8.
21] Brondolo E, Rieppi R, Kelly KP, et al. Perceived racism and bloodpressure: a review of the literature and conceptual and methodolog-ical critique. Ann Behav Med 2003;25:55–65.
22] Sarabi M, Lind L. Mental stress opposes endothelium-dependentvasodilation in young healthy individuals. Vasc Med 2001;6:3–7.
23] Spieker LE, Hurlimann D, Ruschitzka F, et al. Mental stress inducesprolonged endothelial dysfunction via endothelin-A receptors. Circu-lation 2002;105:2817–20.
24] Gottdiener JS, Kop WJ, Hausner E, et al. Effects of mental stress onflow mediated brachial arterial dilation: an influence of behavioralfactors and hypercholesterolemia in subjects without cardiovasculardisease. Am J Cardiol 2003;92:687–91.
25] Clark R. Inter-ethnic group and intra-ethnic group racism: perceptionsand coping in Black university students. J Black Psychol 2004;30:506–26.
26] Sigelman L, Welch S. Black Americans’ Views of Racial Inequality:The Dream Deferred. New York, NY: Cambridge University Press,1991.
27] Utsey SO, Payne YA, Jackson ES, et al. Race-related stress, qualityof life indicators, and life satisfaction among elderly African Amer-icans. Cultur Divers Ethnic Minor Psychol 2002;8:224–33.
28] Landrine H, Klonoff EA. Racial discrimination and cigarette smokingamong Blacks: findings from two studies. Ethn Dis 2000;10:195–202.
29] Thompson VL. Racism: perceptions of distress among African Amer-icans. Community Ment Health J 2002;38:111–8.
30] Ahimastos AA, Formosa M, Dart AM, et al. Gender differences inlarge artery stiffness pre- and post puberty. J Clin Endocrinol Metab
2003;88:5375–80.31] Dressler WW, Bindon JR, Neggers YH. John Henryism, gender, andarterial blood pressure in an African American community. Psycho-som Med 1998;60:620–4.
32] James SA, Thomas PE. John Henryism and blood pressure in BlackPopulations: a review of the literature. Afr Am Perspect 2000;6:1–10.
33] Clark R, Adams JH. Moderating effects of perceived racism on JohnHenryism and blood pressure reactivity in Black college females. AnnBehav Med 2004;28:126–31.
34] Fernandes E, McCrindle BW. Diagnosis and treatment of hyperten-sion in children and adolescents. Can J Cardiol 2000;16:801–11.
35] Ballard ME, Cummings EM, Larkin K. Emotional and cardiovascularresponses to adults’ angry behavior and to challenging tasks in chil-dren of hypertensive and normotensive parents. Child Dev 1993;64:500–15.
36] Zimlichman R, Shargorodsky M, Boaz M, et al. Determination ofarterial compliance using blood pressure waveform analysis with theCR-2000 system. Reliability, repeatability, and establishment of nor-mal values for healthy European population: the Seven EuropeanSites Study (SESS). Am J Hypertens 2004;18:65–71.
37] Chobanian AV, Bakris GL, Black HR, et al. Joint National Commit-tee on Prevention, Detection, Evaluation, and Treatment of HighBlood Pressure. National Heart, Lung, and Blood Institute; NationalHigh Blood Pressure Education Program Coordinating Committee.Seventh report of the Joint National Committee on Prevention, De-tection, Evaluation, and Treatment of High Blood Pressure. Hyper-tension 2003;42:1206–52.
38] Aiken LS, West SG. Multiple Regression: Testing and InterpretingInteractions. Newbury Park, CA: Sage, 1991.
39] Tsai PS, Yucha CB, Nichols WW, et al. Hemodynamics and arterialproperties in response to mental stress in individuals with mild hy-pertension. Psychosom Med 2003;65:613–9.
40] Clark R, Anderson NB, Clark VR, et al. Racism as a stressor forAfrican Americans: a biopsychosocial model. Am Psychol 1999;54:
805–16.