Embed Size (px)
Citation preview

EPIDEMIOLOGY
Aneurysms, which are the 13th leading cause of death in the U.S., most commonly occur in the infrarenal abdominal aorta (95%), while 5% or less will occur above the renal arteries. Although most AAA’s begin below the renal arteries and end above the aortic bifurcation, many extend to the iliac arteries. The majority are fusiform and saccular; the latter, once more common, occur infrequently. (Figure 1)
Aneurysms are approximately five times more common in men than in women and 2.5 time more common in Caucasian men than African-American men. Aortic aneurysms are generally found in the more elderly population with the average age being approximately 65
years. Risk factors that have been known to be associated with aortic aneurysms include age, male sex in white race, as previously noted, a positive family history, cigarette smoking, COPD, hypertension, hypercholesterolemia, peripheral artery disease and coronary artery disease. Interestingly, diabetes mellitus is associated with a negative relative risk for abdominal aortic aneurysms. Of note, patients with peripheral arterial aneurysms, (especially those involving the popliteal and/or femoral arteries) have a prevalence of aortic aneurysms that approaches 60%.
There have now been a number of studies that document the familial or inherited risks of abdominal aneurysms. A positive family history is present in approximately 15 to 30% of
JEFFREY REED RUBIN, md, facs
Board Certified in Vascular and Endovascular Surgery
Dr. Rubin is board certified in Vascular and Endovascular Surgery. He has devoted his entire medical career to the study and treatment of vascular problems and is an expert in minimally invasive endovascular (catheter-based) procedures as well as conventional surgical procedures.
Dr. Rubin has authored more than 70 papers and book chapters related to vascular disease. He has held several faculty and professional appointments, including Chief of Vascular Surgery and Associate Professor of Surgery with tenure at Case Western Reserve Univer-sity Hospitals in Cleveland, Ohio; Chairman of the Department of Surgery and Program Director at Western Reserve Care System in Youngstown, Ohio; Professor of Surgery with tenure at Northeastern Ohio Universities Col-lege of Medicine, Rootstown, Ohio; Director of Vascular Center at Mary Black Health System in Spartanburg, South Carolina and Professor of Surgery and Chief of Vascular Surgery at Wayne State University School of Medicine and Detroit Medical Center.
East CoopER VasCUlaR sURgERY
Laptop EastCooperVascularSurgery.com
Phone-Square 843-936-5951 Fax 843-936-5952 Map-Marker-Alt East Cooper Medical Center, Mullis Building
851 Leonard Fulghum Blvd., Suite 100 Mt. Pleasant, SC 29464
ABDOMINAL AORTIC ANEURYSMS An arterial aneurysm is defined as a permanent localized dilatation of an artery, although the amount of arterial enlargement, before it is categorized as an aneurysm, is controversial. We have generally considered an artery to be aneurysmal if there is an increase in its diameter of at least 50% as compared to the expected normal diameter. The expected normal diameter of an artery will, of course, depend upon sex, total body surface area and multiple other factors. On the average, an infrarenal abdominal aorta measures 2.0 cm and is usually smaller in women than they are in men.
FIGURE 8: Entire graft including contralateral limb extension are fully deployed
FIGURE 9: Completion Angiogram
Conventional repair of abdominal aortic aneurysms (Figures 10, 11 and 12) consists of replacement of the abdominal aorta with a graft. The graft is generally made of either Dacron or polytetrafluoroethylene (PTFE). With conventional techniques, a 3-4 hour operation is required and patients are generally in the hospital between five and seven days, and they cannot return to their normal activities for a total of six weeks following surgery. Long-term success is excellent with graft patency reaching 95% at five years.
East Cooper Vascular Surgery has been involved with the placement of stent grafts since the early 1990’s and have enjoyed excellent operative results with an average length of stay for these patients of 29 hours.
SCREENING
The U.S. Preventive Services Task Force (USPSTF) now recommends a single abdominal ultrasound for AAA’s for men > 65 years of age who have smoked; men > 65 years of age who have not smoked but who have other risk factors; and there is inadequate evidence to determine if screening is helpful in women.
For consultation, questions, or referral, please call: JEFFREY R. RUBIN, md, facs Director, The Vascular Center
East CoopER MEDICal gRoUp
East CooperVascular SurgeryLaptop EastCooperVascularSurgery.com Phone-Square 843-936-5951 Fax 843-936-5952
Map-Marker-Alt East Cooper Medical Center | 851 Leonard Fulghum Blvd., Suite 100 | Mt. Pleasant, SC 29464
FIGURE 5: Wrap is tethered to main (long) limb
CARET-UP FIGURE 10 Caret-Down FIGURE 11 FIGURE 12 Caret-Right
FIGURE 6: Seam opens up when string is pulled (asymmetric)
FIGURE 7: Graft of Main Body and ipsilateral limb is fully deployed
The Vascular A PUBLICATION OF EAST COOPER VASCULAR SURGERY / / S p r i n g 2 0 2 0
FIGURE 1
Continued inside

patients undergoing abdominal aortic aneurysm repair. The 15th chromosome has been identified as the area that carries this gene and it is felt this gene is responsible for the synthesis and degradation of collegan and elastin, which are obviously fundamental in the maintenance of integrity of the artery wall. Research has noted autosomal dominant, autosomal recessive and sex-linked inheritance or modes of transmission as possible for passing aneurysms on.
Approximately 25% of patients with abdominal aortic aneurysms have a first- degree relative also affected. Atherosclerosis has also been identified as a potential etiology for AAA formation. It is present in a majority of patients with aneurysms and may act to weaken the vessel wall causing dilatation. No direct link has been confirmed.
It is important to note the incidence of abdom-inal aortic aneurysms is increasing. Studies performed at the Mayo Clinic, that evaluated patients between 1951 and 1980, showed a three-fold increase in aneurysm prevalence from 12.2 to 36.2 per year.
NATURAL HISTORY
There are three major complication of abdom-inal aortic aneurysms. The most common complication is aneurysm rupture. Embolization and aneurysm thrombosis are the second and third most common complications.
RUPTURE
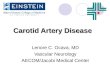
The risk of aneurysm rupture increases directly with increases in arterial diameter. Although aneurysms are not ideal cylinders, they do appear to follow the Law of Laplace. As aneurysms increase in size, there is decreased wall strength and/ or thickness which will increase the risk of rupture. (Figure 2)
Despite the presence of multiple studies pertaining to aneurysm rupture, it is impossible to precisely determine rupture rates for aneu-rysms at various diameters. Abdominal aortic
aneurysms expand an average 2-3 mm per year; however, the growth rate increases steadily as the aortic diameter increases. Anything greater than 2-3 mm increases in diameter per year would constitute rapid expansion, which poses a greater risk for rupture.
Most authors, at this time, estimate 5 to 6 cm abdominal aortic aneurysm carries rupture risk between 2 and 15% per year or about 45% over five years. Larger sized aneurysms would obviously carry a greater risk of rupture.
Most abdominal aortic aneurysms are asymptomatic, whereas, acute and rapid expansion or abdominal aortic aneurysm rupture will cause severe and dramatic abdominal, flank and back pain. These symptoms are generally not associated with intact abdominal aortic aneurysms. Occasionally, an aneurysm that has eroded posteriorly into an adjacent verte-brae, which is extremely rare, can cause vague abdominal and back pain. On the other hand, some patients present with proven abdominal aortic aneurysm rupture and this unfortunate situation is fre-quently not preventable. Family members with a history of abdominal aortic aneu-rysms should be properly evaluated in an attempt to prevent missing an aneurysm.
Patients who present with rupture usually demonstrate syncope, hypotension and frequently circulatory collapse and frank shock. Most patients (> 90%) who experience rupture both at home and while hospitalized die secondary to the complications of refrac-tory hypotension. As alluded to earlier, most aneurysms are diagnosed incidentally, when patients are referred for radiologic tests for vague abdominal, back and flank discomfort. In a review of 243 patients who underwent elective aortic aneurysm repair at the University of Texas Southwest, only 38% were initially discovered by physical examination, whereas, 62% were detected by incidental radiological studies. Notably, 23% of these clinically signif-icant aneurysms were not palpable even when the diagnosis was already established. In obese patients, 2/3 of the abdominal aortic aneurysms were not palpable.
EMBOLISM
Patients who present with “blue toe syndrome” must be considered to have abdominal aortic aneurysms unless proven otherwise. Blue toe syndrome is characterized as a diffuse, mottled, bluish discoloration of the skin that is usually located in the digits of the lower extremities. This is due to atheroembolization and the most common source of this problem is an abdominal aortic aneurysm. Therefore, patients who are found to have “blue toe syndrome” must be worked up for aneurysms.
THROMBOSIS
With aneurysm thrombosis, which is extremely rare, patients generally present with signs of severe bilateral lower extremity ischemia and not infrequently with renal failure or mesen-teric ischemia. As one would imagine, this is usually a surgical emergency requiring prompt aortic and lower extremity revascularization within six hours of presentation.
DIAGNOSIS
In general, there are several tests that may assist physicians in diagnosing an abdominal aneurysm. Ultrasound is an excellent test for screening patients for abdominal aortic aneurysms. It is a sensitive and reliable testing modality, is noninvasive, easy to obtain and not painful. While an excellent screening test, its limitations may include an inability to reliably visualize the iliac arteries, the suprarenal aorta and detect rupture. Therefore, ultrasound should generally be used as a screening test.
Computerized axial tomography (CT) (Figures 3 and 4) has an accuracy rate of more than 90% for demonstrating the presence of an abdominal aortic aneurysm. Sensitivity and specificity are also in excess of 90%. In addition, CT scanning may be performed expeditiously, noninvasively and provides very important information with regard to the location of the aneurysm or aneu-rysms and the proximity to the renal arteries. CT Scans also provide invaluable information with regard to iliac and femoral arteries. Three-dimen-sional imaging software now provides additional visual tools for planning a surgical approach. Although CT scans are more expensive than ultrasound, involve radiation and require intravenous contrast, the test is extremely accurate and provides more information than ultrasound. Therefore, this is the test of choice.
Magnetic resonance imaging (MRI/MRA) also provides information similar to CT scanning in the diagnosis of an abdom-inal aortic aneurysm. Although it avoids radiation exposure, it is more expensive, and frequently is not well tolerated by claustrophobic patients.
Lastly, arteriography may assist one in determin-ing and defining arterial anatomy but should not be used as a diagnostic test for aneurysms. It provides very little to no information regard-ing the diameter of the aneurysm.
FIGURE 3
FIGURE 4
These computerized axial tomography (CT) images clearly demonstrate a large abdominal aortic aneurysm.
TREATMENT
The treatment of abdominal aortic aneurysms generally involves surgical intervention either endovascular (minimally invasive) or open surgery. We prefer to intervene prior to aneurysm rupture since the mortality is reduced by more than 90%.
Deciding whether or not to repair an aneurysm electively is dependent upon the life expectancy of the patient, the operative risk for the patient and the risk of rupture of the aneurysm. The patient’s risk factors need to be evaluated prior to discussing how one will treat the aneu-rysm. In general, standard preoperative testing includes chest x ray, CBC,
electrolytes, renal and liver function tests, EKG and selectively, a cardiac stress test, pulmonary function test and noninvasive vascular testing. The risk fac-tors will then be stratified to help make a decision as to whether or not a repair will be performed. In general, the risk of oper-ative mortality, with elective aneurysm repair, in an otherwise healthy patient, ranges from 1% to 5%. Obviously the expected mortality rate increases with the presence of additional risk factors.
Endovascular repair of abdominal aortic aneurysms has gained increasing popularity since the early 1990s when the development of this technique was brought to clinical trials. Endografts, or “stent grafts,” have been used throughout the world over the past 25 years with excellent results. Endoluminal aneurysm repair is performed with regional, local or general anesthesia using two small groin incisions or needle sticks, with the graft being delivered through stiff plastic sheaths. (Figures 5, 6, 7, 8 and 9 on the back page). Patients are usually hospitalized for less than 48 hours. This procedure can be performed with less operative morbidity and mortality than standard open repair which requires a large abdominal incision, general anesthesia, and is a much more invasive procedure. As of 2018, the Society for Vascular Surgery recommends Endovascular Aneurysm Repair (EVAR) as the preferred treatment for AAA’s. There are several anatomic qualifications that need to be reviewed and include: the length of the neck of normal abdominal aorta below the renal arteries and before the aneurysm starts, the diameter of the aorta in this location and the ability to pass this very rigid, large delivery device up through the femoral and iliac arteries in order to seat the graft. With advances in technology over the past three decades we are now able to offer EVAR to a larger number of patients; however, open repair is still requested in some patients.
The Vascular East CoopER MEDICal gRoUp
East CooperVascular Surgery
0 2 4 6 8 10Equal to or greater than in diameter (cm.)
5 ye
ar r
isk
of ru
ptur
e (p
erce
nt)
100908070605040302010
FIGURE 2