Embed Size (px)
DESCRIPTION
Ilhan Ece, Huseyin Yilmaz, Hüsnü Alptekin, Serdar Yormaz, Mustafa Sahin. Laparoscopic partial cystectomy for the treatment of hepatic hydatid cysts. IAIM, 2014; 1(4): 16-20.
Citation preview

Laparoscopic partial cystectomy for
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
Original Research Article
Laparoscopic partial cystectomy for the
treatment of hepatic hydatid cysts
Ilhan Ece1*
, Huseyin Yilmaz
1Department of Surgery, Selcuk
*Corresponding author email:
How to cite this article: Ilhan Ece, Huseyin Yilmaz, Hüsnü Alptekin, Serdar Yormaz, Mustafa Sahin
Laparoscopic partial cystectomy for the treatment of hepatic hydatid cysts
Available online at
Received on: 17-11-2014
Abstract
Background: The laparoscopic approach for the treatment of hepatic hydatid cysts is increasingly
gaining importance. The aim of this study was to report a series of 27 patients with hepatic hydatid
cyst managed with laparoscopic partial cystectomy.
Methods: A retrospective review of patients treated at a university clinic for hepatic hyd
from March 2010 to May 2014 was performed. Operative time, blood loss, length of hospital stay,
post-operative complications, and early follow
Results: Laparoscopic surgical intervention was performed on 27 patients (17 females and 10 males)
who were diagnosed with hydatid cysts by ultrasonography and computed tomography (CT). Except
3 of the cysts, were located in the right lobe of the liver. No
Two surgical site infections were observed and no abscesses developed in the cystic cavity.
Recurrence was not noted during the mean follow
Conclusion: Laparoscopic partial cystectomy is a safe
hepatic hydatid cyst.
Key words
Hepatic hydatid cyst, Laparoscopy, P
Introduction
Hydatid cysts of the liver are frequently
encountered in endemic regions, such as Turkey.
There are a variety of treatment modalities for
cystectomy for hepatic hydatid cysts
International Archives of Integrated Medicine, Vol. 1, Issue. 4, December, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
Laparoscopic partial cystectomy for the
treatment of hepatic hydatid cysts
, Huseyin Yilmaz1, Hüsnü Alptekin
1, Serdar Yormaz
Mustafa Sahin1
Department of Surgery, Selcuk University, Faculty of Medicine, Konya, Turkey
*Corresponding author email: [email protected]
Ilhan Ece, Huseyin Yilmaz, Hüsnü Alptekin, Serdar Yormaz, Mustafa Sahin
cystectomy for the treatment of hepatic hydatid cysts. IAIM, 2014; 1(4
Available online at www.iaimjournal.com
2014 Accepted on:
The laparoscopic approach for the treatment of hepatic hydatid cysts is increasingly
gaining importance. The aim of this study was to report a series of 27 patients with hepatic hydatid
cyst managed with laparoscopic partial cystectomy.
pective review of patients treated at a university clinic for hepatic hyd
ay 2014 was performed. Operative time, blood loss, length of hospital stay,
operative complications, and early follow-up outcomes were evaluated.
: Laparoscopic surgical intervention was performed on 27 patients (17 females and 10 males)
who were diagnosed with hydatid cysts by ultrasonography and computed tomography (CT). Except
3 of the cysts, were located in the right lobe of the liver. No mortality was noted during the study.
Two surgical site infections were observed and no abscesses developed in the cystic cavity.
Recurrence was not noted during the mean follow-up period of 22 months.
: Laparoscopic partial cystectomy is a safe and effective method for the treatment of
Hepatic hydatid cyst, Laparoscopy, Partial cystectomy.
Hydatid cysts of the liver are frequently
encountered in endemic regions, such as Turkey.
There are a variety of treatment modalities for
hepatic hydatid cysts, including medical therapy
and open or laparoscopic surgery, depending on
the size and characteristics
Surgical treatment techniques include
aspiration, drainage, marsupialization, and total
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 16
Laparoscopic partial cystectomy for the
treatment of hepatic hydatid cysts
, Serdar Yormaz1,
University, Faculty of Medicine, Konya, Turkey
Ilhan Ece, Huseyin Yilmaz, Hüsnü Alptekin, Serdar Yormaz, Mustafa Sahin.
IAIM, 2014; 1(4): 16-20.
Accepted on: 26-11-2014
The laparoscopic approach for the treatment of hepatic hydatid cysts is increasingly
gaining importance. The aim of this study was to report a series of 27 patients with hepatic hydatid
pective review of patients treated at a university clinic for hepatic hydatid cysts
ay 2014 was performed. Operative time, blood loss, length of hospital stay,
: Laparoscopic surgical intervention was performed on 27 patients (17 females and 10 males)
who were diagnosed with hydatid cysts by ultrasonography and computed tomography (CT). Except
mortality was noted during the study.
Two surgical site infections were observed and no abscesses developed in the cystic cavity.
and effective method for the treatment of
hepatic hydatid cysts, including medical therapy
and open or laparoscopic surgery, depending on
istics of the cyst [1].
Surgical treatment techniques include
aspiration, drainage, marsupialization, and total

Laparoscopic partial cystectomy for
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
cyst excision combined with segmental liver
resection [2]. The main purpose of the surgery is
to provide elimination of scolices in the cyst
cavity, removal of all viable parts of the cyst, and
obliteration of the remaining cavity [3]
an ongoing controversy concerning the
laparoscopic treatment of hepatic hydatid c
due to limited experience [4].
The aim of this study was to examine
feasibility and safety of laparoscopic partial
cystectomy for the treatment of hepatic hydatid
cyst.
Material and methods
Laparoscopic surgical intervention was
performed on 27 patients (17 females and 10
males) who were diagnosed with hepatic
hydatid cyst between March 2010 and May 2014
in our institute. Preoperative radiologic
evaluation of the cysts was performed using
abdominal ultrasonography and computed
tomography in all patients. Hepatic infestation
with E. granulosus was confirmed histologically
in all patients. All patients in the study were
consulted by radiology and confirmed that were
unsuitable for PAIR treatment
liver cirrhosis, peritonitis, previous upper
abdominal surgery, severe obesity, or patients
who were high-risk for general
excluded. All patients received oral albendazole
(10 mg/kg) for 10 days before surgery.
The patients’ demographics, operative time,
blood loss, length of hospital stay, post
operative complications, and early follow
outcomes were evaluated. All patients were
followed up for at least 22 months.
Surgical procedure
Prophylaxis was provided with 1 g of c
sodium administered 30 minutes prior to
surgery. Patients were placed on the operating
cystectomy for hepatic hydatid cysts
International Archives of Integrated Medicine, Vol. 1, Issue. 4, December, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
with segmental liver
. The main purpose of the surgery is
to provide elimination of scolices in the cyst
ity, removal of all viable parts of the cyst, and
ration of the remaining cavity [3]. There is
an ongoing controversy concerning the
laparoscopic treatment of hepatic hydatid cysts
The aim of this study was to examine the
feasibility and safety of laparoscopic partial
cystectomy for the treatment of hepatic hydatid
Laparoscopic surgical intervention was
performed on 27 patients (17 females and 10
males) who were diagnosed with hepatic
hydatid cyst between March 2010 and May 2014
in our institute. Preoperative radiologic
evaluation of the cysts was performed using
ominal ultrasonography and computed
tomography in all patients. Hepatic infestation
with E. granulosus was confirmed histologically
All patients in the study were
consulted by radiology and confirmed that were
unsuitable for PAIR treatment. Patients with
liver cirrhosis, peritonitis, previous upper
abdominal surgery, severe obesity, or patients
risk for general anesthesia were
All patients received oral albendazole
(10 mg/kg) for 10 days before surgery.
demographics, operative time,
blood loss, length of hospital stay, post-
operative complications, and early follow-up
outcomes were evaluated. All patients were
followed up for at least 22 months.
Prophylaxis was provided with 1 g of cefazolin
sodium administered 30 minutes prior to
surgery. Patients were placed on the operating
table in the right lateral position for hydatid
cysts of the right lobe of the liver and in the left
lateral position for hydatid cysts of th
of the liver. A 1.5 cm infra umbilical incision was
made and a laparoscope was inserted after
insufflation through a 10 mm trocar inserted
into the abdominal cavity. In cases with hydatid
cysts of the right lobe, the other trocars were
inserted into the abdominal
junction of the subcostal line and midclavicular
line, and in the subxiphoid area. Gauze pads
soaked with hypertonic saline (20% NaCl) were
placed around the site where the cyst protruded
from the surface of the liver, in Morrison’s
pouch, and in the subhepatic area. The content
of the cyst was aspirated as much as possible
using a laparoscopic needle and hypertonic
saline was injected into the cyst and left for 10
minutes. The hypertonic solution in the cyst was
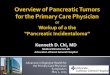
re-aspirated. The cyst wall w
perforator grinder aspirator
daughter vesicles in the cyst were aspirated
completely (Photo - 2). The puncture site was
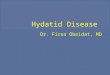
enlarged by a 10 mm Ligasure™ (
Boulder, CO, USA). The protruding wall of the
cyst was excised by the Ligasure
placed in a plastic bag, and removed with the
trocar. If the bile duct communication seen, it
routinely sutured with non-
After assuring that there was no evidence of a
biliary leak, the operation was completed by
inserting a 20-F Nelaton drain into the posterior
of the liver.
Results
A total of 27 patients with 34 hydatid cysts were
treated with laparoscopic partial cystectomy.
There were 17 male and 10 female patients,
with a mean age of 44 years (range, 28
years). The mean cyst diameter was 6.3 cm
ranging from 3 to 10 cm. Thirty
the cysts were located in the right lobe, whereas
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 17
table in the right lateral position for hydatid
cysts of the right lobe of the liver and in the left
lateral position for hydatid cysts of the left lobe
cm infra umbilical incision was
made and a laparoscope was inserted after
insufflation through a 10 mm trocar inserted
into the abdominal cavity. In cases with hydatid
cysts of the right lobe, the other trocars were
inserted into the abdominal cavity at the
junction of the subcostal line and midclavicular
line, and in the subxiphoid area. Gauze pads
soaked with hypertonic saline (20% NaCl) were
placed around the site where the cyst protruded
from the surface of the liver, in Morrison’s
nd in the subhepatic area. The content
of the cyst was aspirated as much as possible
using a laparoscopic needle and hypertonic
saline was injected into the cyst and left for 10
minutes. The hypertonic solution in the cyst was
aspirated. The cyst wall was punctured with a
(Photo – 1), and the
daughter vesicles in the cyst were aspirated
. The puncture site was
enlarged by a 10 mm Ligasure™ (Valleylab,
). The protruding wall of the
Ligasure™ (Photo - 3),
placed in a plastic bag, and removed with the
trocar. If the bile duct communication seen, it
-absorbable sutures.
After assuring that there was no evidence of a
leak, the operation was completed by
F Nelaton drain into the posterior
A total of 27 patients with 34 hydatid cysts were
treated with laparoscopic partial cystectomy.
There were 17 male and 10 female patients,
a mean age of 44 years (range, 28-69
years). The mean cyst diameter was 6.3 cm
ranging from 3 to 10 cm. Thirty-one (91.2%) of
the cysts were located in the right lobe, whereas

Laparoscopic partial cystectomy for
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
3 (8.8%) was located in the left lobe. Cysts were
multiple in 5 of 27 patients.
All patients were administered 15 mg/day of
albendazole until the 3rd
post-operative month
follow-up visit. No mortality was noted during
the study. Endoscopic sphincterotomy was
performed in 1 patient on the 4
day due to the appearance of bile in the drain;
biliary leak ceased on the 8th
post
Two surgical site infections were observed and
no abscesses developed in the cystic cavity. The
operative datas including operative time, blo
loss, complications, length of hos
recurrence rate were as per Table
site infection is the most common complication
that occurred in 2 patients, followed by a low
output bile leakage in 1 patient, and 1 patient
with minimal pleural effusion was treated
conservatively. No recurrence was noted during
the mean follow-up period of 22 months (range,
12-48 months).
Table - 1: Patient demographics and operative
datas.
Parameters Partial cystectomy
(n = 27)
Age (years) 44 ±
Gender, n (%)
-Males
-Females
17 (62.9%)
10 (37.1%)
Diameter of cysts (cm) 6.3 (3
Operative time (minutes) 108 ± 21.4
Blood loss (mL) 55.5
Hospital stay (days) 4.8
Complications, n (%)
-Bile leakage
-Surgical site infection
-Pleural effusion
-Intra-abdominal abscess
-Mortality
1 (3.7
2 (7.4
1 (3.7
-
-
cystectomy for hepatic hydatid cysts
International Archives of Integrated Medicine, Vol. 1, Issue. 4, December, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
3 (8.8%) was located in the left lobe. Cysts were
All patients were administered 15 mg/day of
operative month
up visit. No mortality was noted during
the study. Endoscopic sphincterotomy was
performed in 1 patient on the 4th
post-operative
day due to the appearance of bile in the drain;
post-operative day.
Two surgical site infections were observed and
no abscesses developed in the cystic cavity. The
operative datas including operative time, blood
loss, complications, length of hospital stay and
Table - 1. Surgical
site infection is the most common complication
that occurred in 2 patients, followed by a low-
output bile leakage in 1 patient, and 1 patient
leural effusion was treated
conservatively. No recurrence was noted during
up period of 22 months (range,
Patient demographics and operative
Partial cystectomy
(n = 27)
44 ± 11.3 (28-69)
17 (62.9%)
10 (37.1%)
6.3 (3-10)
108 ± 21.4
55.5 ± 15.9
4.8 ± 2.4
1 (3.7%)
2 (7.4%)
1 (3.7%)
Photo - 1: The use of perforator grinder
aspirator.
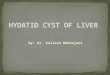
Photo - 2: Cyst wall was punctured with a
perforator grinder aspirator and
Photo - 3: Cystic content evacuated completely
and partial cystectomy was performed with
LigasureTM
.
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 18
The use of perforator grinder
Cyst wall was punctured with a
perforator grinder aspirator and enlarged.
Cystic content evacuated completely
and partial cystectomy was performed with

Laparoscopic partial cystectomy for
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
Discussion
There has been widespread use of laparoscopic
interventions, following the confirmation of
their reliability in laparoscopic cholecystectomy
[5]. Laparoscopic surgery of hydatid cysts has
become an effective procedure in the treatment
of uncomplicated hydatid cysts which are not
suitable for percutaneous aspiration.
Cystectomy and drainage procedures were
common in previous practice; however, with the
recent development in laparoscopic techniques
and increasing surgeon experience, there has
been increased use of pericystectomy and
radical resection of hepatic hydatid cysts in
many centers [4]. The use of laparoscop
ultrasonography is known to facilitate surgical
interventions in cysts with a posterior
localization and in those neighboring large
vessels [6]. The main principles of conventional
liver hydatid surgery including inactivation,
prevention of spillage, elimination of viable
elements of the cyst, and management of the
residual cavity have been strictly implemented
in the laparoscopic treatment of liver hydatid
disease. However, there are still some concerns
for spillage and anaphylactic shock under the
high abdominal pressure induced by the
pneumoperitoneum until the evidence that the
increase in intracystic pressure was no greater
than the increase intra-abdominal pressure and
that pneumoperitoneum was protective against
spillage [7], and various studies ha
demonstrated that the surgically
pneumoperitoneum does not cause sprea
the cyst into the abdomen [8].
Most of the surgeons have limited patient
selection criteria for the laparoscopic treatment
of hepatic hydatid cyst, and, with the increa
experience they are relaxing their inclusion
criterias. In this study, patients with history of
previous upper abdominal surgery, patients with
cysts deeply located and diameter >10 cm were
cystectomy for hepatic hydatid cysts
International Archives of Integrated Medicine, Vol. 1, Issue. 4, December, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
There has been widespread use of laparoscopic
interventions, following the confirmation of
n laparoscopic cholecystectomy
. Laparoscopic surgery of hydatid cysts has
become an effective procedure in the treatment
of uncomplicated hydatid cysts which are not
suitable for percutaneous aspiration.
Cystectomy and drainage procedures were
n previous practice; however, with the
recent development in laparoscopic techniques
and increasing surgeon experience, there has
been increased use of pericystectomy and
hydatid cysts in
. The use of laparoscopic
ultrasonography is known to facilitate surgical
interventions in cysts with a posterior
hose neighboring large
. The main principles of conventional
liver hydatid surgery including inactivation,
imination of viable
elements of the cyst, and management of the
residual cavity have been strictly implemented
in the laparoscopic treatment of liver hydatid
disease. However, there are still some concerns
for spillage and anaphylactic shock under the
abdominal pressure induced by the
pneumoperitoneum until the evidence that the
increase in intracystic pressure was no greater
abdominal pressure and
that pneumoperitoneum was protective against
, and various studies have
demonstrated that the surgically-created
pneumoperitoneum does not cause spread of
Most of the surgeons have limited patient-
selection criteria for the laparoscopic treatment
of hepatic hydatid cyst, and, with the increased
experience they are relaxing their inclusion
criterias. In this study, patients with history of
previous upper abdominal surgery, patients with
cysts deeply located and diameter >10 cm were
not included. The main advantages of
laparoscopy include less post
shorter duration of hospital stay, and better
cosmetic results. On the other hand, similar
results have been reported concerning intra
abdominal spread and related recurrences when
performed by experienced surgeons, compared
to the open surgical technique [
the mortality rate is lower [11
Conclusion
In conclusion, the laparoscopic drainage and
partial cystectomy for the surgical treatment of
hepatic hydatid cysts is safe and effective
techniques in selected patien
further multi centric, prospective and
randomized studies are needed to define the
role of laparoscopy as the gold standard for the
treatment of hepatic hydatid cysts.
References
1. Menezes da Silva. Hydatid cyst of the
liver-criteria for the selection of
appropriate treatment. Acta Tropica,
2003; 85: 237-42.
2. Salinas SG, Velasquez HC, Saavedra TL.
Laparoscopic treatment of the hydatid
liver cysts. Rev Gastroenterol Peru,
2001; 21: 306-11.
3. Sayek I, Cakmakcı M. Laparoscopic
management of echinococcal cysts of
the liver. Zentralbl Chir, 1999; 124:
1143-6.
4. Manterola C, Fernandez O, Munoz S,
Vial M, Losada H, Carrasco R, Bello N,
Barroso M. Laparoscopic pericystectomy
for liver hydatid cysts. Surg
2002; 16: 521-4.
5. Seven R, Berber E, Mercan S, Eminoglu
L, Budak D. Laparoscopic treatment of
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 19
not included. The main advantages of
post-operative pain, a
shorter duration of hospital stay, and better
cosmetic results. On the other hand, similar
results have been reported concerning intra-
abdominal spread and related recurrences when
performed by experienced surgeons, compared
technique [9, 10]. However,
11].
In conclusion, the laparoscopic drainage and
partial cystectomy for the surgical treatment of
hepatic hydatid cysts is safe and effective
techniques in selected patients. However,
entric, prospective and
randomized studies are needed to define the
role of laparoscopy as the gold standard for the
treatment of hepatic hydatid cysts.
Silva. Hydatid cyst of the
criteria for the selection of
appropriate treatment. Acta Tropica,
Salinas SG, Velasquez HC, Saavedra TL.
Laparoscopic treatment of the hydatid
liver cysts. Rev Gastroenterol Peru,
I, Cakmakcı M. Laparoscopic
management of echinococcal cysts of
the liver. Zentralbl Chir, 1999; 124:
Manterola C, Fernandez O, Munoz S,
Vial M, Losada H, Carrasco R, Bello N,
Barroso M. Laparoscopic pericystectomy
for liver hydatid cysts. Surg Endosc,
Seven R, Berber E, Mercan S, Eminoglu
L, Budak D. Laparoscopic treatment of

Laparoscopic partial cystectomy for
International Archives of Integrated Medicine, Vol.
Copy right © 2014, IAIM, All Rights Reserved.
hepatic hydatid cysts. Surgery, 2000;
128: 36-40.
6. Sansonetti A, Baghini S, Lai G, Zeno V,
Valente U, Nardi D, Pochini M, Casciani
CU. Update on laparoscopi
the treatment of hydatid cyst of the liver
and peritonitis caused by a perforated
duodenal ulcer. Minerva Chir, 1993; 48:
1249-51.
7. Bickel A, Loberant N. The feasibility of
safe laparoscopic treatment of hydatid
cysts of the liver. Surg Endosc
934–935.
8. Khoury G, Abiad F, Geagea T, Nabout G,
Jabbour S. Laparoscopic treatment of
hydatid cysts of the liver and spleen.
Surg Endosc, 2000; 14: 243
9. Bickel A, Daud G, Urbach D, Lefler E,
Barasch EF, Eitan A. Laparoscopic
approach to hydatid liver cysts: is it
logical? Physical, experimental and
cystectomy for hepatic hydatid cysts
International Archives of Integrated Medicine, Vol. 1, Issue. 4, December, 2014.
Copy right © 2014, IAIM, All Rights Reserved.
hepatic hydatid cysts. Surgery, 2000;
Sansonetti A, Baghini S, Lai G, Zeno V,
Valente U, Nardi D, Pochini M, Casciani
Update on laparoscopic surgery: On
the treatment of hydatid cyst of the liver
and peritonitis caused by a perforated
duodenal ulcer. Minerva Chir, 1993; 48:
Bickel A, Loberant N. The feasibility of
safe laparoscopic treatment of hydatid
cysts of the liver. Surg Endosc., 1995; 9:
Khoury G, Abiad F, Geagea T, Nabout G,
Jabbour S. Laparoscopic treatment of
hydatid cysts of the liver and spleen.
Surg Endosc, 2000; 14: 243-5.
Bickel A, Daud G, Urbach D, Lefler E,
Barasch EF, Eitan A. Laparoscopic
d liver cysts: is it
logical? Physical, experimental and
practical aspects. Surg Endosc, 1998; 12:
1073-7.
10. Strauss M, Schmidt J, Boedeker H,
Zirngibl H, Jauch KW. Laparoscopic
partial pericystectomy of Echinococcus
granulosus cysts in the liver.
Hepatogastroenterology, 1999; 46:
2540-4.
11. Bickel A, Loberant N, Shtamler B.
Laparoscopic treatment of hydatid cyst
of the liver: initial experience with a
small series of patients. J Laproendosc
Surg, 1994; 4: 127-33.
Source of support: Nil
Conflict of interest: No
ISSN: 2394-0026 (P)
ISSN: 2394-0034 (O)
Page 20
practical aspects. Surg Endosc, 1998; 12:
Strauss M, Schmidt J, Boedeker H,
Zirngibl H, Jauch KW. Laparoscopic
partial pericystectomy of Echinococcus
granulosus cysts in the liver.
roenterology, 1999; 46:
Bickel A, Loberant N, Shtamler B.
Laparoscopic treatment of hydatid cyst
of the liver: initial experience with a
small series of patients. J Laproendosc
33.
Nil
None declared.