Embed Size (px)
Citation preview
L’anziano complesso: esiste un nuovo paradigma per la
farmacoterapia evidence‐based?
Graziano OnderCentro Medicina dell’InvecchiamentoUniversità Cattolica del Sacro Cuore
Roma

Marengoni et al. JAGS 2009
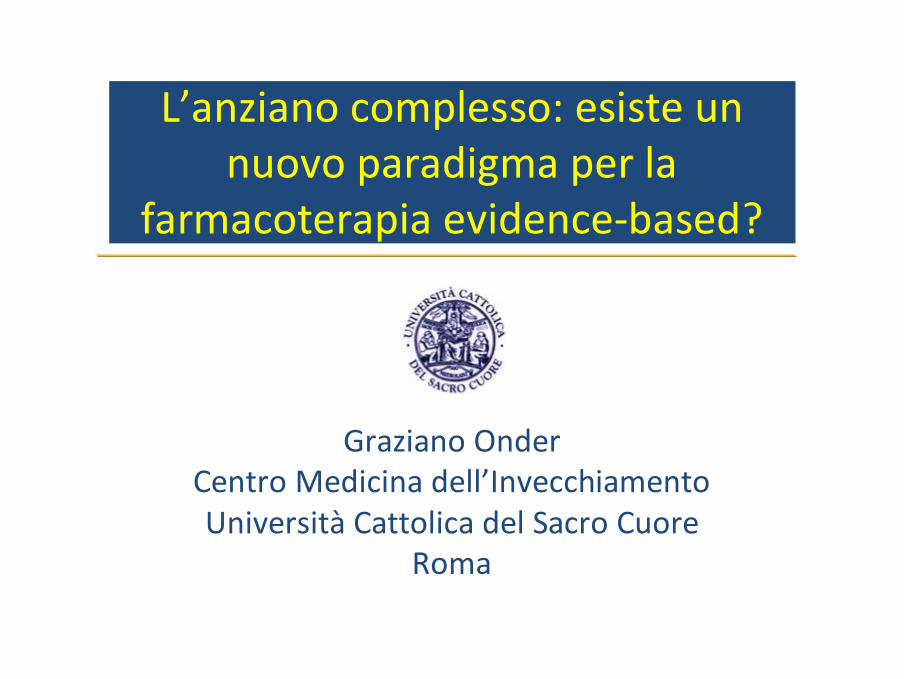
Marengoni A., Karolinska Institutet, 2008
Cluster analysis testing the distribution of chronic diseases
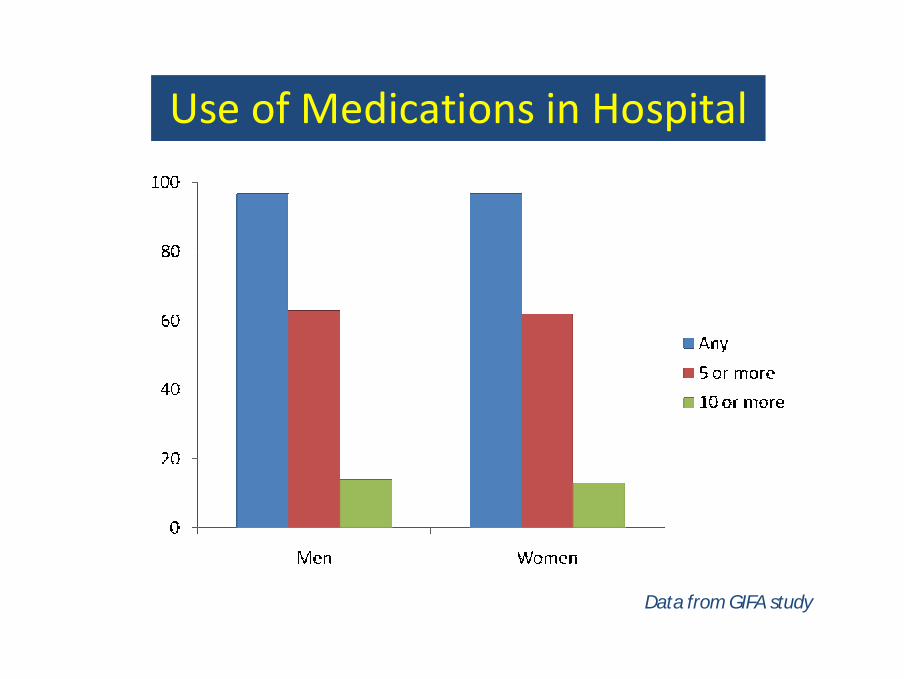
Use of Medications in Hospital
Data from GIFA study

Predictors of ADRGerontoNET ADR risk score
Use of drugs (vs. < 5)5-78 or more
1.904.07
1.584.09
14
Previous ADR 2.41 2.18 2
Any ADR Severe ADR ScoreOR OR
≥ 4 diseases 1.36 1.72 1Heart failure 1.79 1.61 1Liver disease 1.31 1.32 1Renal failure* 1.21 1.24 1
Onder G et al. Arch Intern Med 2010

Onder G et al. JAGS 2002
Drugs responsible for ADR: results from the GIFA study
… current guidelines do not provide anappropriate, evidence‐based foundation for assessing quality of care in older adults with several chronic diseases… the recommended regimens may present thepatient with an unsustainable treatmentburden, making independent self‐management and adherence difficult
Boyd, C. M. et al. JAMA 2005;294:716‐724.
Clinical Practice Guidelines and Quality of Care for Older Patients With Multiple Diseases
… clinicians would benefit from a number of tools to assist them in decision making for older persons with multiple conditions… the concept of tailoring therapy based on a consideration of patients' ability to adhere has not received much attention in the medical literature. Such tailoring suggests the need for explicit assessment of the complexity of the interventions recommended by CGL and for simplified alternatives.
Fried et al. Arch Intern Med 2010
Strumenti a disposizione del medico:
1. Computerized provider order entry systems
• Programmi che consentono di registrare e trasmettere le prescrizioni terapeutiche direttamente alle farmacie;• Possono contenere una serie di warning in caso di prescrizioni non appropriate;• Particolarmente diffusi nel mondo anglossassone con lo scopo di ridurre il rischio di errori medici e supportare il medico nelle scelte terapeutiche.
Computerized provider order entry systems (CPOE)
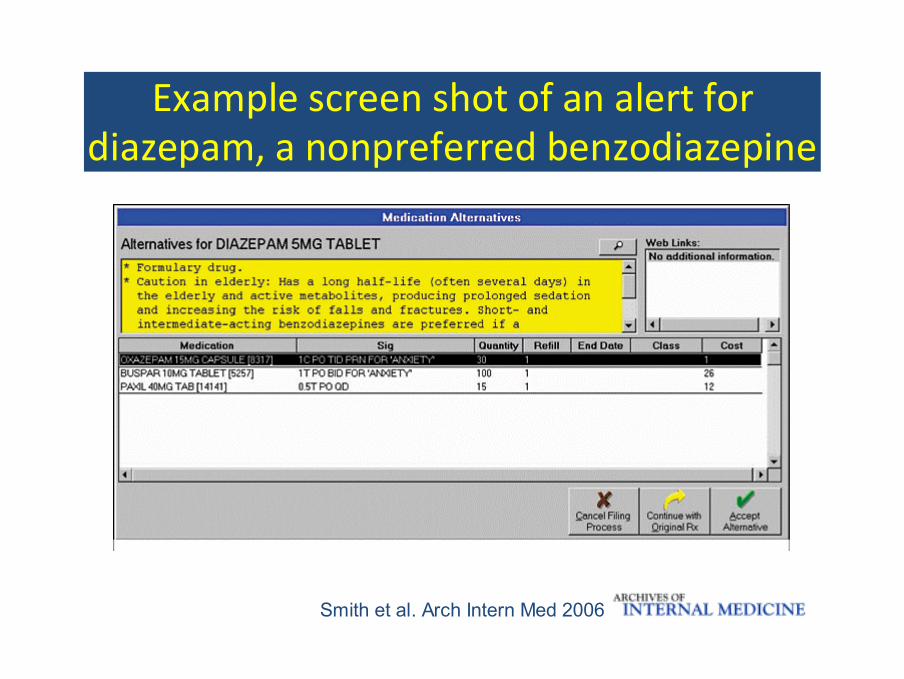
Smith et al. Arch Intern Med 2006
Example screen shot of an alert for diazepam, a nonpreferred benzodiazepine
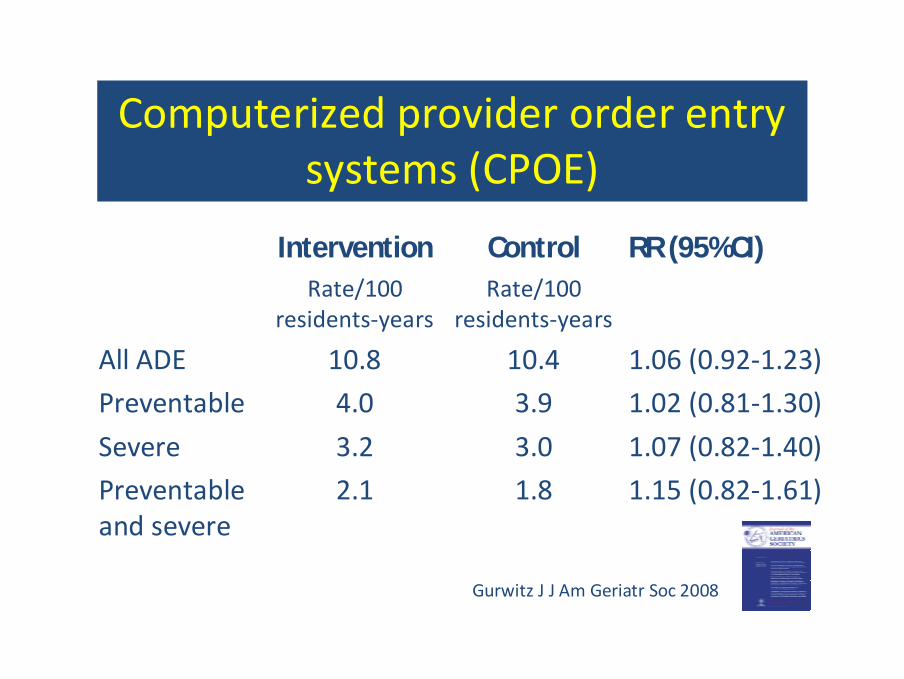
Computerized provider order entry systems (CPOE)
Intervention Control RR (95%CI)Rate/100
residents‐yearsRate/100
residents‐years
All ADE 10.8 10.4 1.06 (0.92‐1.23)
Preventable 4.0 3.9 1.02 (0.81‐1.30)
Severe 3.2 3.0 1.07 (0.82‐1.40)
Preventable and severe
2.1 1.8 1.15 (0.82‐1.61)
Gurwitz J J Am Geriatr Soc 2008
…alerts in an outpatient electronic medical record may be an effective method of reducing prescribing of contraindicated medications. The effect of the alerts on patient outcomes is less certain and deserves further investigation.
Computerized provider order entry systems (CPOE)
Smith et al. Arch Intern Med 2006
…the evidence for the impact of CPOE needs to be improved to support scientific generalizability
Weir et al. Int J Med Inform. 2009
…CPOE have the potential to change health care provider behaviour, but very few studies show improvement in patient outcomes
BMC Med Inform Decis Mak. 2009
Strumenti a disposizione del medico:
1. Computerized provider order entry systems
2. Algoritmi
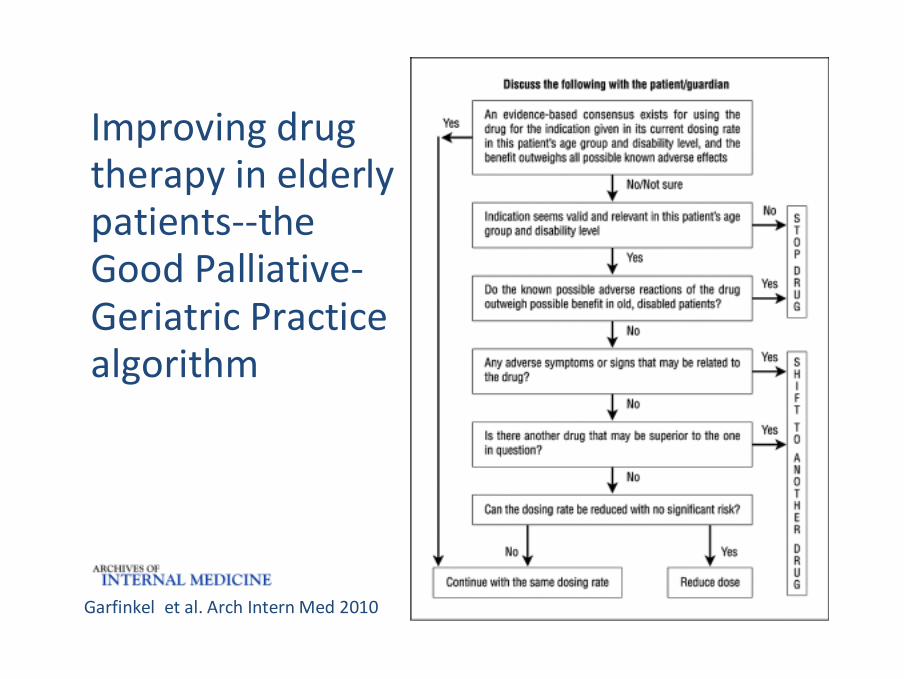
Improving drug therapy in elderly patients‐‐the Good Palliative‐Geriatric Practice algorithm
Garfinkel et al. Arch Intern Med 2010
Strumenti a disposizione del medico:
1. Computerized provider order entry systems
2. Algoritmi
3. Criteri di qualità ed appropriatezza della prescrizione farmacologica
Criteri di qualità ed appropriatezzadella prescrizione farmacologica
• In passato vari criteri sono stati sviluppati per identificare l’uso di farmaci inappropriati (Beers, ACOVE, UKNHS, START & STOPP);• Identificano comportamenti prescrittivi inappropriati relativi
all’utilizzo di farmaci i cui rischio superano i potenziali benefici (drugs to avoid);
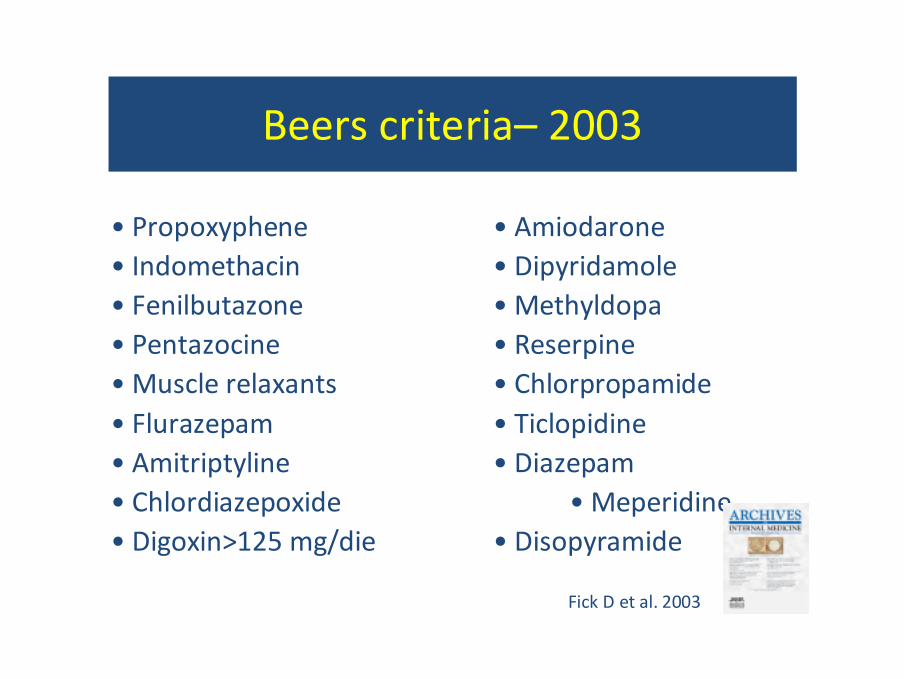
Beers criteria– 2003
• Propoxyphene • Amiodarone• Indomethacin • Dipyridamole• Fenilbutazone • Methyldopa• Pentazocine • Reserpine• Muscle relaxants • Chlorpropamide• Flurazepam • Ticlopidine• Amitriptyline • Diazepam• Chlordiazepoxide • Meperidine• Digoxin>125 mg/die • Disopyramide
Fick D et al. 2003
Criteri di qualità ed appropriatezzadella prescrizione farmacologica
• In passato vari criteri sono stati sviluppati per identificare l’uso di farmaci inappropriati (Beers, ACOVE, UKNHS, START & STOPP);• Identificano comportamenti prescrittivi inappropriati relativi
all’utilizzo di farmaci i cui rischio superano i potenziali benefici (drugs to avoid);
al sottoutilizzo di farmaci potenzialmente benefici (underuse).
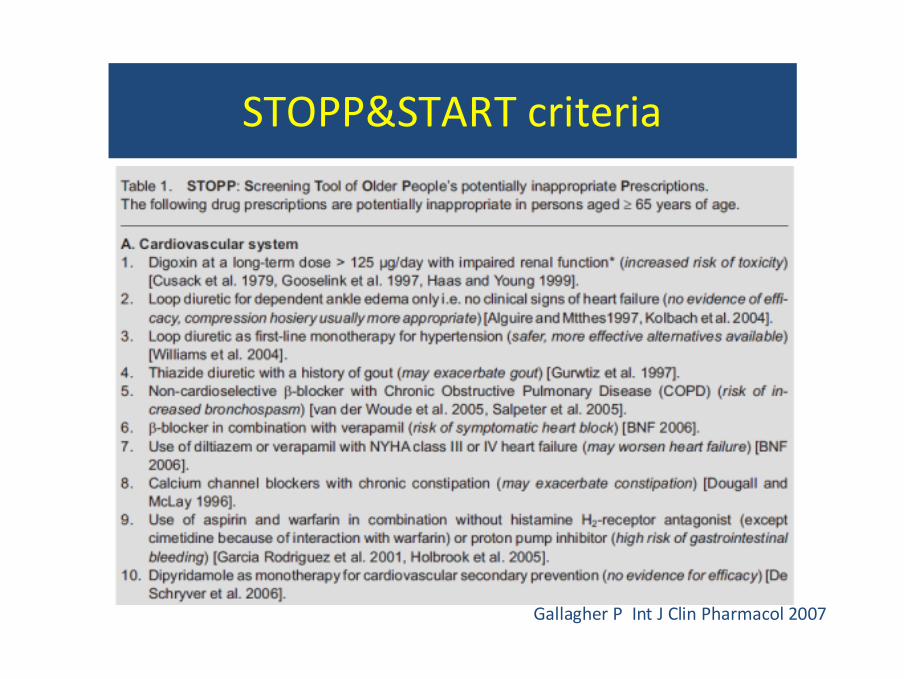
STOPP&START criteria
Gallagher P Int J Clin Pharmacol 2007

STOPP&START criteria
Gallagher P Int J Clin Pharmacol 2007
Limiti dei criteri esistenti
• Validità
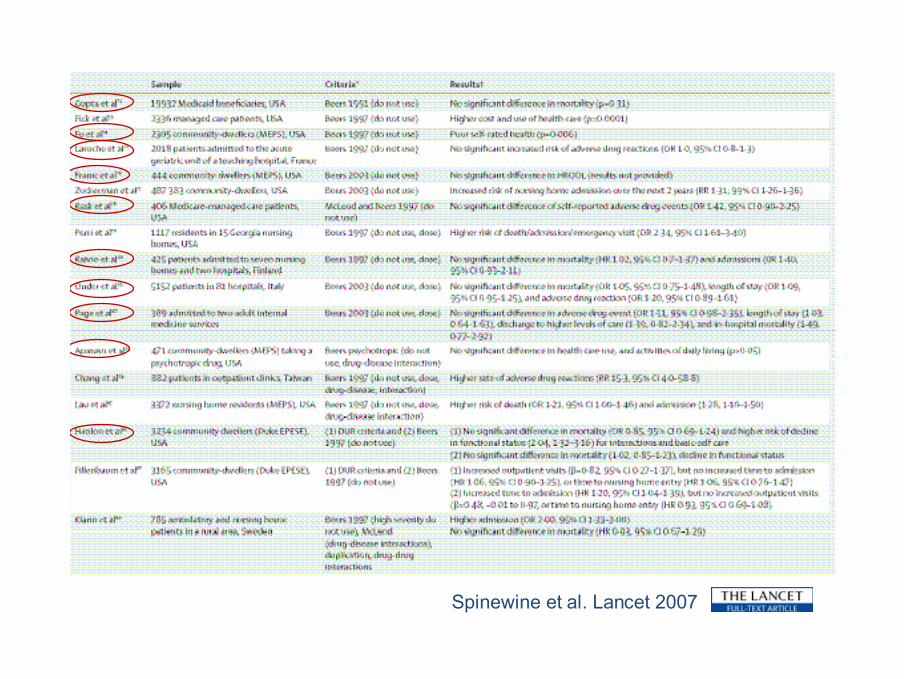
Spinewine et al. Lancet 2007

Limiti dei criteri esistenti
• Validità
• Non valutano importanti aree della prescrizione farmacologica:‐ Aderenza ‐ Interazioni farmacologiche
‐ Cascata prescrittiva‐ Prescrizioni duplicate
Criteri AIFA ‐ Scopo
Identificare alcuni indicatori che descrivano nella popolazione italiana ultra65enne:
1. l’utilizzo dei farmaci;2. il ricorso a comportamenti prescrittivi inappropriati, che non portano benefici al paziente, ma possono potenzialmente comportare anche elevati rischi iatrogeni.
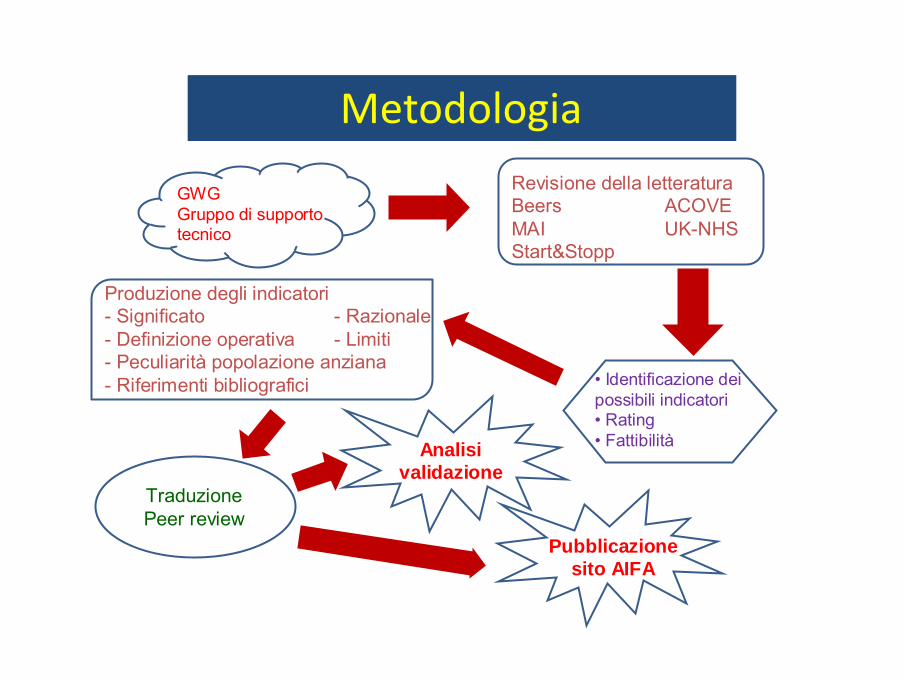
Metodologia
GWG Gruppo di supporto tecnico
Revisione della letteraturaBeers ACOVEMAI UK-NHSStart&Stopp
• Identificazione dei possibili indicatori• Rating• Fattibilità
Produzione degli indicatori- Significato - Razionale- Definizione operativa - Limiti- Peculiarità popolazione anziana- Riferimenti bibliografici
TraduzionePeer review
Pubblicazione sito AIFA
Analisi validazione
INDICATORI EPIDEMIOLOGICI
POLIFARMACOTERAPIA– Livello di prescrizione per classe farmaco terapeutica e polifarmacoterapia
ADERENZA ALLA TERAPIA– Aderenza al trattamento con antidepressivi
– Aderenza al trattamento con antipertensivi– Aderenza al trattamento con antidiabetici
– Aderenza al trattamento con antiosteoporotici
Indicatori
INDICATORI SENTINELLA
CASCATA PRESCRITTIVA– Farmaci antipsicotici ed antiparkinson
SOTTOPRESCRIZIONE– Utilizzo di statine in soggetti affetti da diabete mellito
INTERAZIONE FARMACOLOGICA– Interazione tra dicumarolici + FANS/Inibitori Cox‐2 + ASA/Antiaggreganti
piastrinici
– Interazione tra ACE‐Inibitori/Sartani + Antialdosteronici+ FANS/Inibitori Cox‐2– Combinazione di farmaci che allungano l’intervallo QT
Indicatori
INDICATORI SENTINELLA
FARMACI DA EVITARE– Uso in monoterapia di doxazosina, clonidina, metildopa; uso di calcio
antagonisti a breve durata d’azione
– Digitale > 0.125 mg– Clorpropamide e glibenclamide
PRESCRIZIONI DUPLICATE– Duplice prescrizione di singole classi di antiipertensivi
Indicatori
Limiti dei criteri esistenti
• Validità
• Non valutano importanti aree della prescrizione farmacologica:‐ Aderenza ‐ Interazioni farmacologiche
‐ Cascata prescrittiva‐ Prescrizioni duplicate
‐ Uso di farmaci in pazienti con particolari condizioni

Geriatric conditions and medication appropriateness:
1. Limited life expectancy
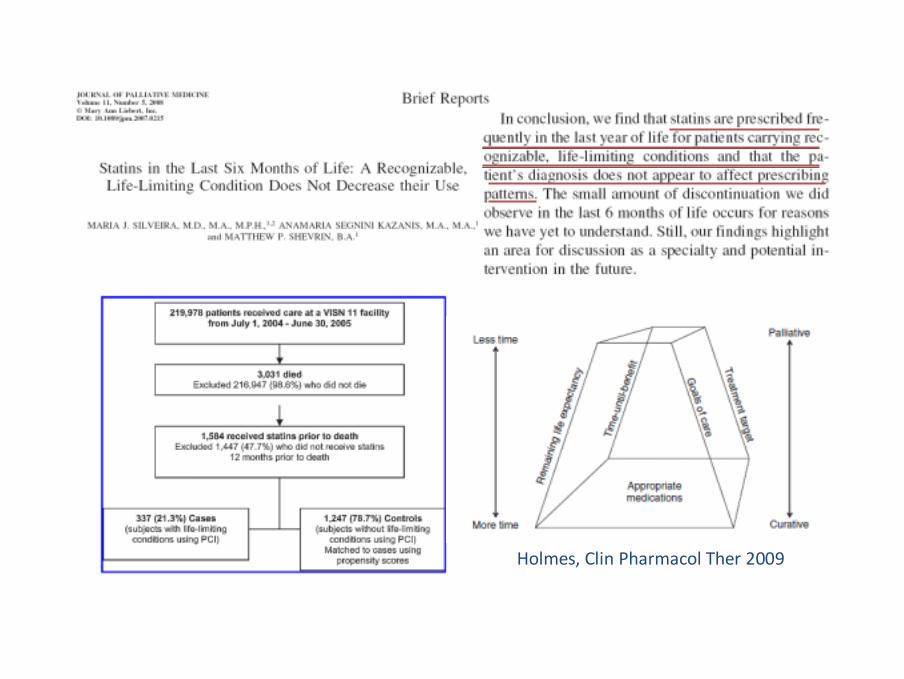
Holmes, Clin Pharmacol Ther 2009

Geriatric conditions and medication appropriateness:
1. Limited life expectancy
2. Functional and cognitive limitation

Treatment of non dementia illnessin patients with dementia
Brauner et al. JAMA 2000
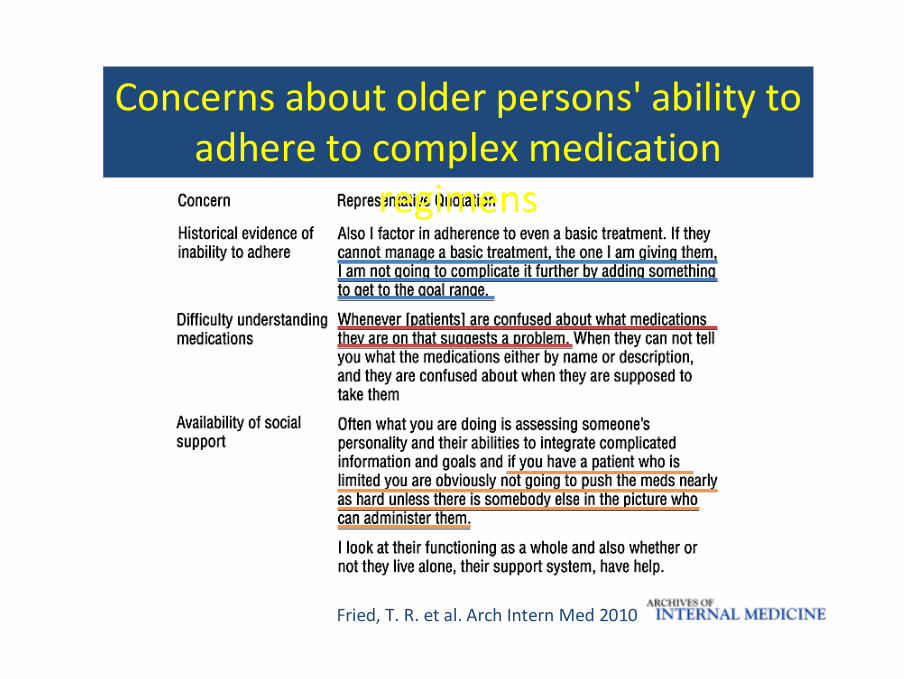
Fried, T. R. et al. Arch Intern Med 2010
Concerns about older persons' ability to adhere to complex medication
regimens
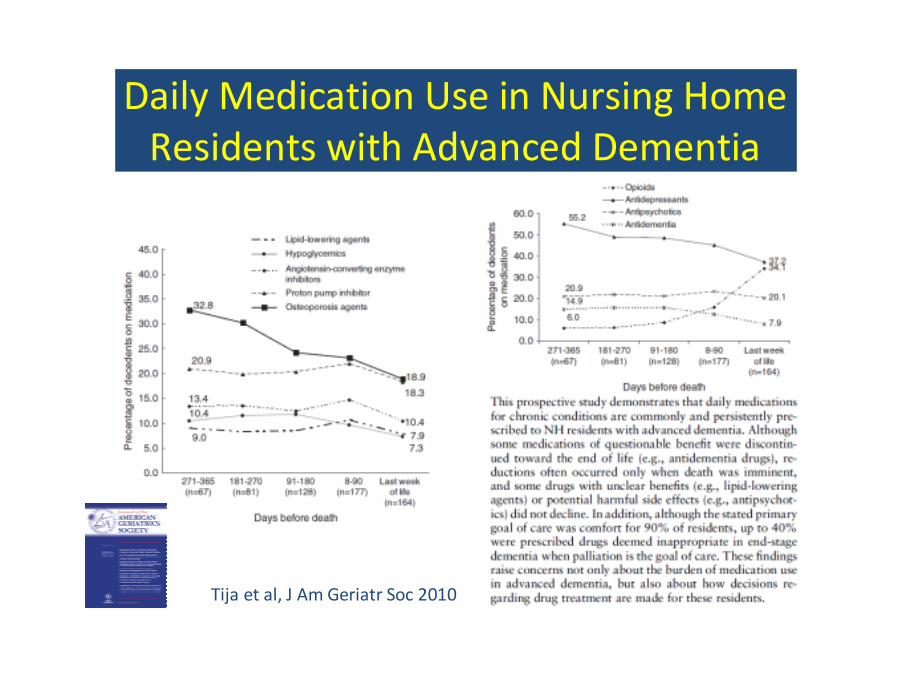
Daily Medication Use in Nursing Home Residents with Advanced Dementia
Tija et al, J Am Geriatr Soc 2010
Geriatric conditions and medication appropriateness:
1. Limited life expectancy
2. Functional and cognitive limitation
3. Geriatric syndromes
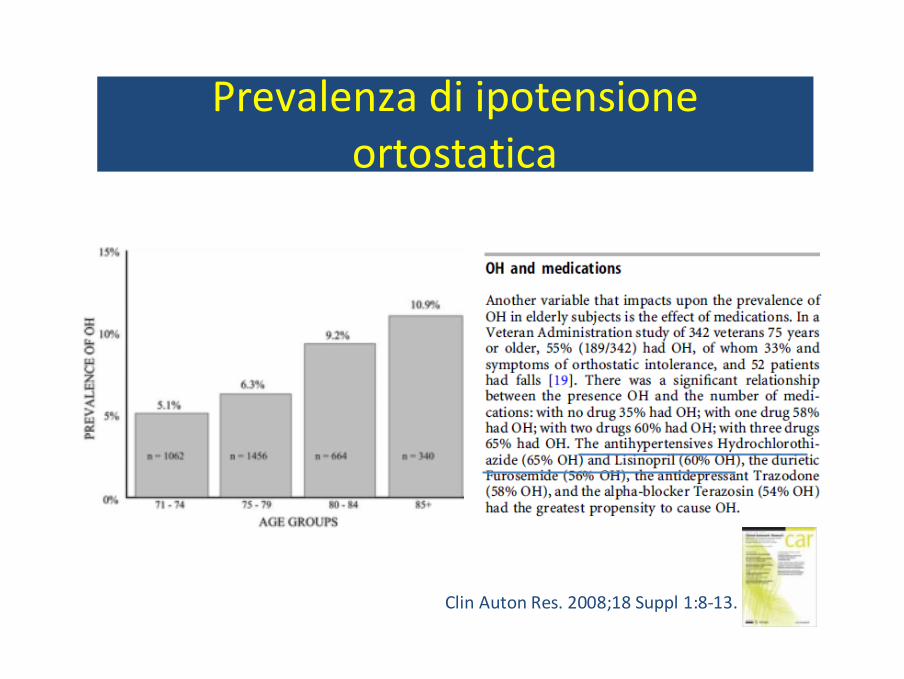
Prevalenza di ipotensioneortostatica
Clin Auton Res. 2008;18 Suppl 1:8‐13.
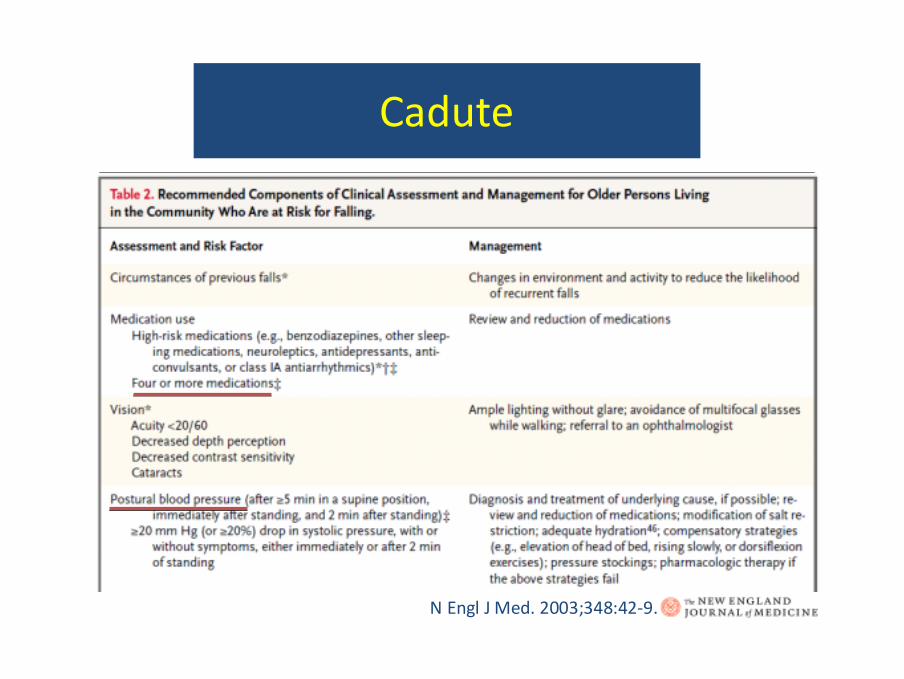
Cadute
N Engl J Med. 2003;348:42‐9.

CRIME study
CRIME: CRIteria for appropriate MEdication use in complex older adults
Bando Giovani Ricercatori 2009 – Ministero della SalutePI: G. Onder, UCSC
Co‐investigatori: A. Corsonello, INRCAC. Ruggiero, U. Perugia
C. Maraldi, U. Ferrara
CRIME
Scopo: fornire dei criteri per la valutazionel’appropriatezze della prescrizionefarmacologica in pazienti anziani complessi, in rapporto a:– attesa di vita;
– stato funzionale e cognitivo;– sindromi geriatriche;
Inizio: Luglio 2009
CRIME studyCRIME
Onder G et al Drugs & Aging 2009

Linee guida comuni patologie croniche
CRIME studyCRIME
‐ ipertensione arteriosa ‐ BPCO‐ scompenso cardiaco ‐ cardiopatia isch. ‐ fibrillazione atriale/ictus ‐ diabete‐ osteoartrosi ‐ osteoporosi
Onder G et al Drugs & Aging 2009
Linee guida comuni patologie croniche
CRIME studyCRIME
Presenza di specifiche indicazioni per anziani complessi?
• limitata attesa di vita• deficit funzionale • deficit cognitivo• sindromi geriatriche
Onder G et al Drugs & Aging 2009
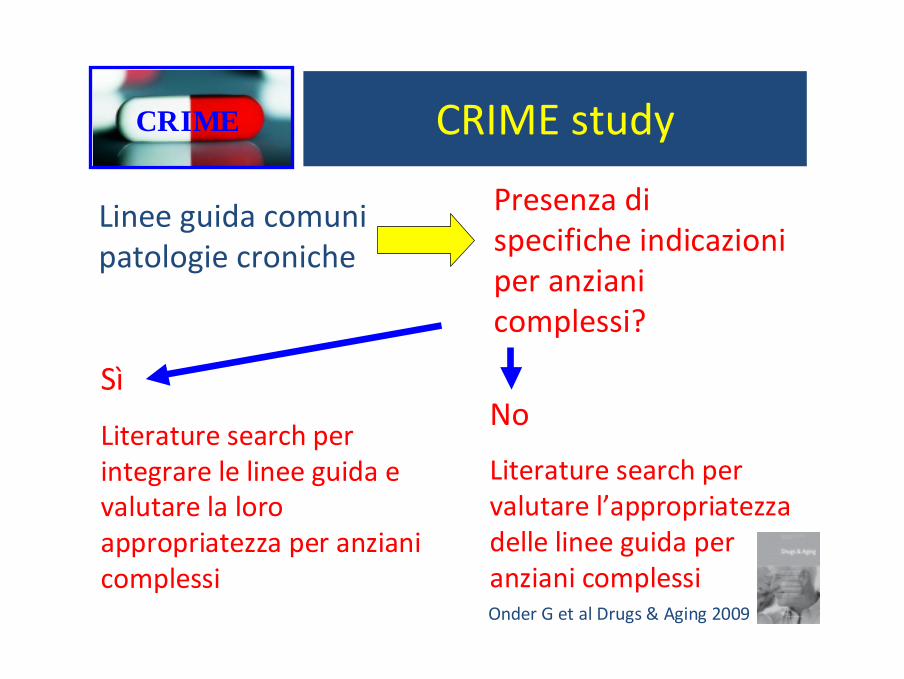
Linee guida comuni patologie croniche
CRIME studyCRIME
Presenza di specifiche indicazioni per anziani complessi?
Sì
Literature search per integrare le linee guida e valutare la loro appropriatezza per anziani complessi
No
Literature search per valutare l’appropriatezza delle linee guida per anziani complessiOnder G et al Drugs & Aging 2009
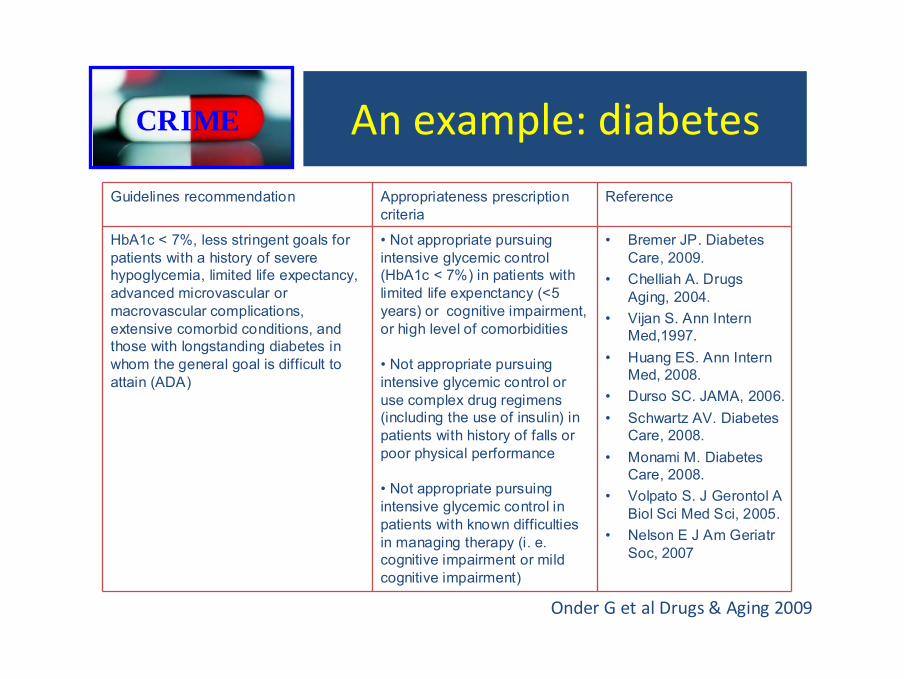
An example: diabetesCRIME
Guidelines recommendation Appropriateness prescription criteria
Reference
HbA1c < 7%, less stringent goals for patients with a history of severe hypoglycemia, limited life expectancy, advanced microvascular or macrovascular complications, extensive comorbid conditions, and those with longstanding diabetes in whom the general goal is difficult to attain (ADA)
• Not appropriate pursuing intensive glycemic control (HbA1c < 7%) in patients with limited life expenctancy (<5 years) or cognitive impairment, or high level of comorbidities
• Not appropriate pursuing intensive glycemic control or use complex drug regimens (including the use of insulin) in patients with history of falls or poor physical performance
• Not appropriate pursuing intensive glycemic control in patients with known difficulties in managing therapy (i. e. cognitive impairment or mild cognitive impairment)
• Bremer JP. Diabetes Care, 2009.
• Chelliah A. Drugs Aging, 2004.
• Vijan S. Ann Intern Med,1997.
• Huang ES. Ann Intern Med, 2008.
• Durso SC. JAMA, 2006.• Schwartz AV. Diabetes
Care, 2008.• Monami M. Diabetes
Care, 2008.• Volpato S. J Gerontol A
Biol Sci Med Sci, 2005.• Nelson E J Am Geriatr
Soc, 2007
Onder G et al Drugs & Aging 2009
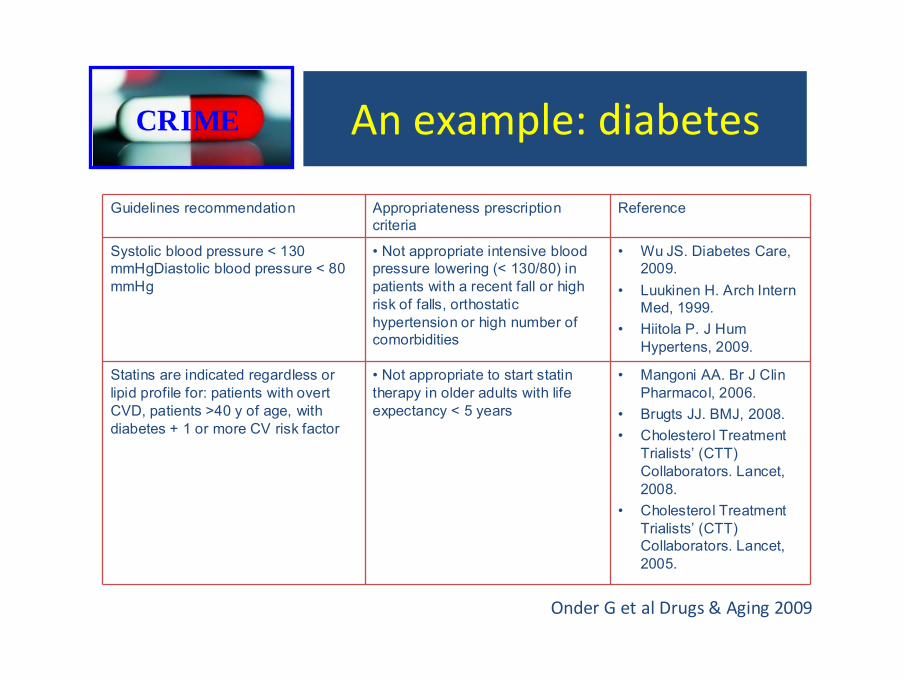
An example: diabetesCRIME
Guidelines recommendation Appropriateness prescription criteria
Reference
Systolic blood pressure < 130 mmHgDiastolic blood pressure < 80 mmHg
• Not appropriate intensive blood pressure lowering (< 130/80) in patients with a recent fall or high risk of falls, orthostatic hypertension or high number of comorbidities
• Wu JS. Diabetes Care, 2009.
• Luukinen H. Arch Intern Med, 1999.
• Hiitola P. J Hum Hypertens, 2009.
Statins are indicated regardless or lipid profile for: patients with overt CVD, patients >40 y of age, with diabetes + 1 or more CV risk factor
• Not appropriate to start statin therapy in older adults with life expectancy < 5 years
• Mangoni AA. Br J Clin Pharmacol, 2006.
• Brugts JJ. BMJ, 2008. • Cholesterol Treatment
Trialists’ (CTT) Collaborators. Lancet, 2008.
• Cholesterol Treatment Trialists’ (CTT) Collaborators. Lancet, 2005.
Onder G et al Drugs & Aging 2009
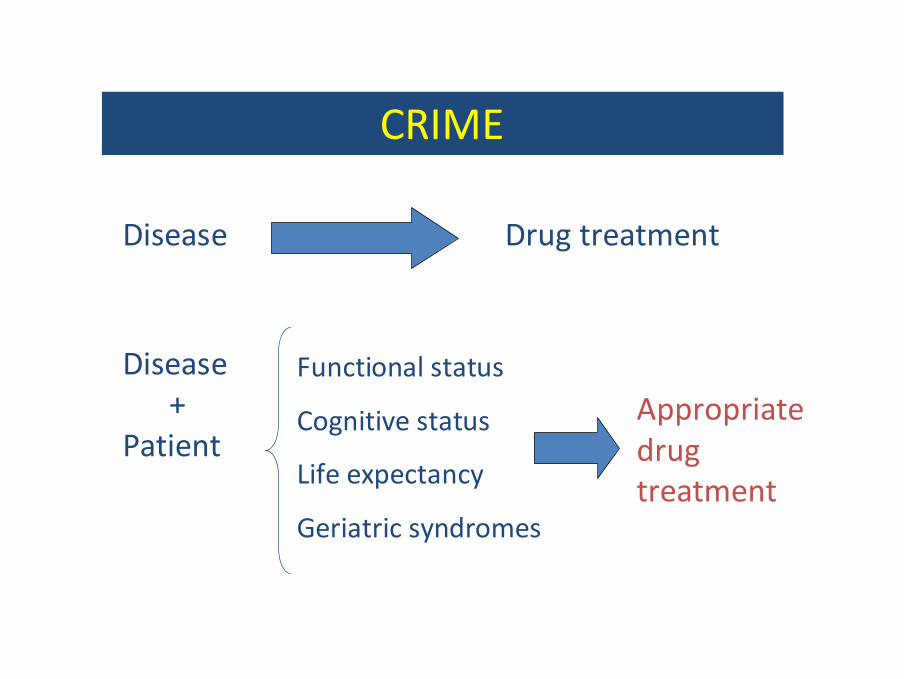
Functional status
Cognitive status
Life expectancy
Geriatric syndromes
Disease Drug treatment
CRIME
Disease+
PatientAppropriate drug treatment

Strumenti a disposizione del medico:
1. Computerized provider order entry systems
2. Algoritmi
3. Criteri di qualità ed appropriatezza della prescrizione farmacologica
4. Valutazione Multidimensionale
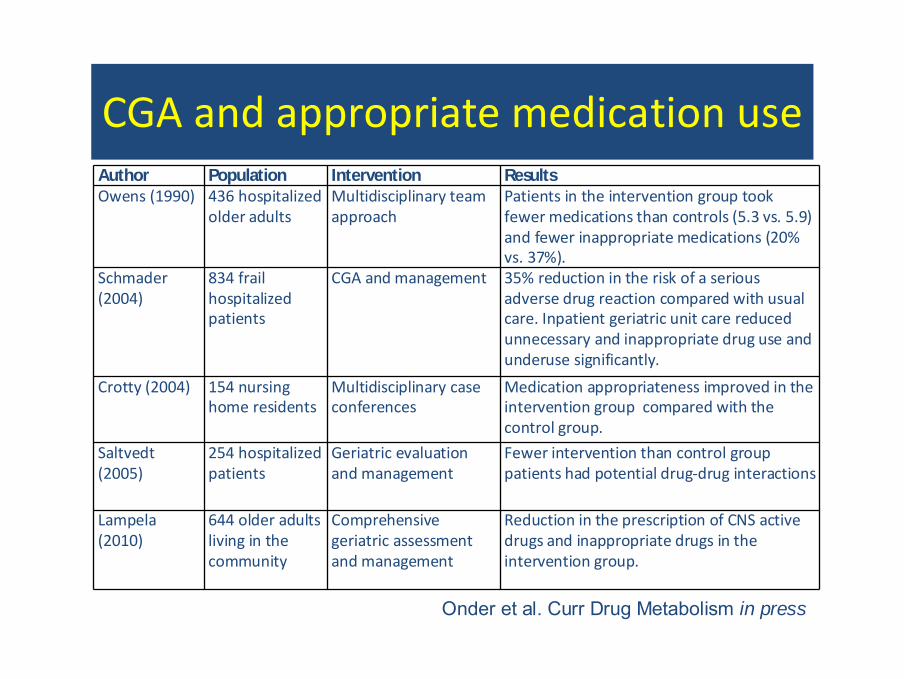
CGA and appropriate medication useAuthor Population Intervention ResultsOwens (1990) 436 hospitalized
older adultsMultidisciplinary team approach
Patients in the intervention group took fewer medications than controls (5.3 vs. 5.9) and fewer inappropriate medications (20% vs. 37%).
Schmader (2004)
834 frail hospitalized patients
CGA and management 35% reduction in the risk of a serious adverse drug reaction compared with usual care. Inpatient geriatric unit care reduced unnecessary and inappropriate drug use and underuse significantly.
Crotty (2004) 154 nursing home residents
Multidisciplinary case conferences
Medication appropriateness improved in the intervention group compared with the control group.
Saltvedt (2005)
254 hospitalized patients
Geriatric evaluation and management
Fewer intervention than control group patients had potential drug‐drug interactions
Lampela (2010)
644 older adults living in the community
Comprehensive geriatric assessment and management
Reduction in the prescription of CNS active drugs and inappropriate drugs in the intervention group.
Onder et al. Curr Drug Metabolism in press
Conclusioni
1. La prescrizione farmacologica nell’anziano complesso rappresenta una sfida per il medico;
2. La prescrizione farmacologica deve essere orientata sulle caratteristiche cliniche del paziente;
3. Tra gli strumenti disponibili, nessuno ha dimostrato in maniera inequivocabile di avere un impatto sugli outcomes di salute;
4. Integrazione?
Progetto AIFA 2008
Titolo: ‘Effetto di un intervento di e‐learning centrato sulla VMD e sulla farmacologia clinica nel migliorare la qualità della prescrizione farmacologica’
Partecipanti: Istituto Mario Negri, SIGG, SIGO, SIMI, FADOI, UCSC
Disegno: RCTOutcomes: qualità della prescrizione
farmacologica, outcomes clinici

Boyd, C. M. et al. JAMA 2005;294:716‐724.
Treatment Regimen for a 79‐Year‐Old Woman With Hypertension, Diabetes Mellitus, Osteoporosis,
Osteoarthritis, and COPD

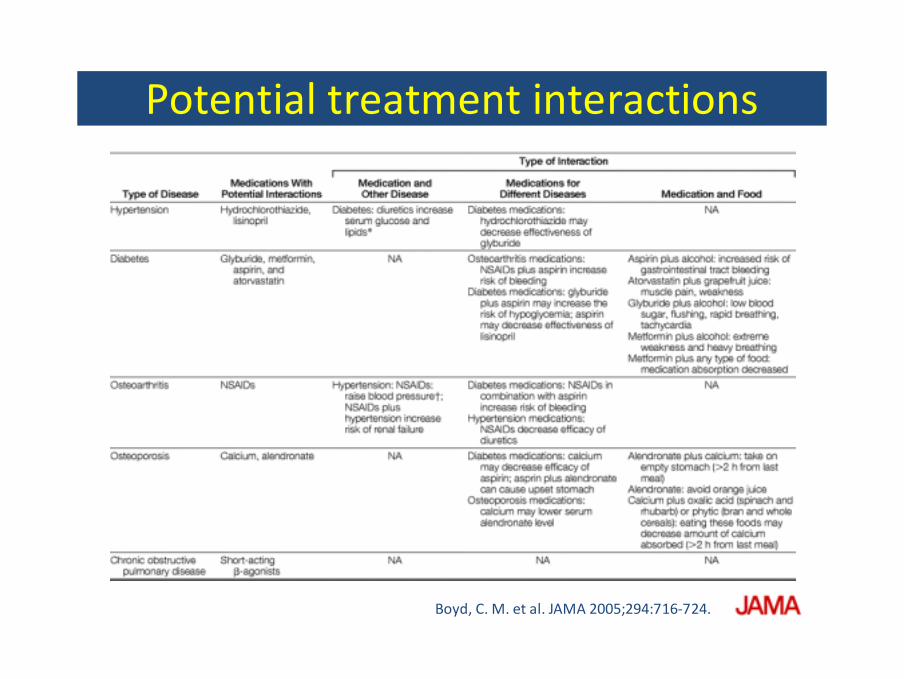
Potential treatment interactions
Boyd, C. M. et al. JAMA 2005;294:716‐724.