Embed Size (px)
Citation preview

Language network dysfunction as a predictor of outcome in youth at clinicalhigh risk for psychosis
Fred W. Sabb a, Theo G.M. van Erp b, Molly E. Hardt b, Mirella Dapretto a, Rochelle Caplan a,Tyrone D. Cannon a,b, Carrie E. Bearden a,b,⁎a Department of Psychiatry and Biobehavioral Sciences, University of California, Los Angeles, Box 956968, Rm 2265, 300 Medical Plaza, Los Angeles, CA 90095-6968,United Statesb Department of Psychology, University of California, Los Angeles, 1285 Franz Hall, Box 951563, Los Angeles, CA 90095-1563, United States
a r t i c l e i n f o a b s t r a c t
Article history:Received 23 May 2009Received in revised form 27 September 2009Accepted 30 September 2009Available online 27 October 2009
Objectives: Language processing abnormalities are a hallmark feature of schizophrenia. Yet, nostudy to date has investigated underlying neural networks associated with discourseprocessing in adolescents at clinical high risk (CHR) for developing psychosis 1.Methods: Forty CHR youth and 24 demographically comparable healthy controls underwentfunctional magnetic resonance imaging while performing a naturalistic discourse processingparadigm. We assessed differences in blood oxygenation level-dependent (BOLD) activitybetween task conditions (TopicMaintenance vs. Reasoning) and between groups. Furthermore,we examined the association of regional brain activity with symptom severity and socialoutcome at follow-up, 6 to 24 months after the scan.Results: Relative to controls, CHR participants showed increased neural activity in a network oflanguage-associated brain regions, including the medial prefrontal cortex bilaterally, leftinferior frontal (LIFG; BA44/45, 47) andmiddle temporal gyri, and the anterior cingulate (BA24and 32). Further, increased activity in the superior temporal gyrus (STG), caudate, and LIFGdistinguished those who subsequently developed psychosis. Within the CHR sample, severityof positive formal thought disorder at follow-upwas positively correlated with signal change inthe LIFG, superior frontal gyrus, and inferior/middle temporal gyri, whereas social outcomewasinversely correlated with signal change in the LIFG and anterior cingulate.Conclusions: These findings are consistent with a neural inefficiency hypothesis in those atgreatest risk for psychosis, and additionally suggest that baseline activation differences maypredict symptomatic and functional outcome. These results highlight the need to furtherinvestigate the neural systems involved in conversion to psychosis, and how languagedisruption changes over time in at-risk adolescents.
© 2009 Elsevier B.V. All rights reserved.
Keywords:fMRISchizophreniaInferior frontal gyrusPsychosis prodromeDiscourseFunctional neuroimaging
1. Introduction
Investigating those who are at high risk for developingpsychosis is one way to examine potential markers for theonset, etiology, and progression of impairments in the earlyphases of psychosis, and offers the potential to identify thosemost likely to become ill (Whalley et al., 2006). By ascertainingindividuals at risk for imminent onset of psychosis (i.e., clinicalhigh risk or prodromal patients) and following them over time(McGlashan, 1996; McGorry et al., 2003), we can improve
Schizophrenia Research 116 (2010) 173–183
⁎ Corresponding author. Semel Institute for Neuroscience and HumanBehavior, University of California, Los Angeles, Box 956968, Rm 2265, 300Medical Plaza, Los Angeles, CA 90095-6968, United States.
E-mail address: [email protected] (C.E. Bearden).1 Please note that our journal previously published the following papers
with similar methodology in people at genetic high-risk for schizophrenia:
Li, X., Branch, C.A., Bertisch, H.C., Brown, K., Szulc, K.U., Ardekani, B.A.,DeLisi, L.E., 2007. An fMRI study of language processing in people at highgenetics risk for schizophrenia. Schizophr. Res. 91: 62–72.Bhojraj, T.S., Francis, A.N., Rajarethinam, R., Eack, S., Kulkarni, S. Prasad, K.M.,Montrose, D.M., Dworakowski, D., Diwadkar, V., Keshavan, M.S., 2009. Verbalfluencydeficits andaltered lateralizationof languagebrain areas in individualsgeneticallypredisposedtoschizophrenia. Schizophr.Res.115(2009)202–208.
0920-9964/$ – see front matter © 2009 Elsevier B.V. All rights reserved.doi:10.1016/j.schres.2009.09.042
Contents lists available at ScienceDirect
Schizophrenia Research
j ourna l homepage: www.e lsev ie r.com/ locate /schres

understanding of the mechanisms of disease onset andprogression.
Cannon et al. (2008) recently found that a predictionalgorithm incorporating combinations of baseline clinicalpredictor variables (genetic risk for schizophrenia with recentfunctional decline, higher levels of unusual beliefs orsuspiciousness, and greater social impairment) dramaticallyincreased positive predictive power for determining subse-quent conversion to psychosis. However, specificity of themodel was low. Functional neuroimaging phenotypes may beable to improve our ability to identify those at greatest risk, asneural systems dysfunction may be closer to the underlyingpathophysiology of the illness than behavioral phenotypes.
Very few studies, however, have examined functionalneuroimaging phenotypes in youth at high risk for psychosis,and existing studies are not well-powered to predict outcomeover time (Morey et al., 2005; Seiferth et al., 2008;Whalley et al.,2006). For instance, using a sentence completion paradigm insubjects at genetic high risk, Whalley et al. (2006) found thatthose who subsequently developed schizophrenia (n=4)demonstrated increased parietal activity, decreased cingulateactivity, and smaller increases in fMRI signalwith increasing taskdifficulty in the right lingual gyrus andbilateral temporal regions.Applying a visual oddball task to clinical high-risk individuals,Moreyet al. (2005)notedsmallerdifferential activation in frontalregions between task-relevant and irrelevant stimuli in frontalregions; however, as only two of the ten putatively prodromalparticipants subsequently developed psychosis, this study wasunable to examine baseline predictors of outcome.
Given the fundamental role of language processing abnor-malities in schizophrenia, as both a key diagnostic sign (Caplanet al., 2000) and a vulnerability marker (Arboleda andHolzman1985; Miklowitz et al., 1991), altered patterns of neural activa-tion during language processing may be a valuable prognosticindicator. Formal thought disorder, a disruption in the flow ofconscious thought inferred from disorganization of spokenlanguage, reflects the most severe manifestation of disturbedlanguage processing (Kuperberg et al., 2006). This disorganiza-tion may result from abnormalities in semantic processingnetworks, ormaybe tied to executive control functions involvedin planning and monitoring speech (Kerns et al., 2004). Inpatients with established illness, these deficits are oftenassociated with structural and functional brain abnormalities,in both prefrontal and temporal regions (Fletcher, 1998; Frith etal., 1995; Kircher et al., 2001; Shenton et al., 2001), which areputative neural correlates for executive (Carter et al., 1999;Glahn et al., 2008; Karlsgodt et al., 2007; Sabb et al., 2007) andsemantic (Bookheimer, 2002;Chao et al., 1999;Mummery et al.,1999; Warrington and Shallice, 1984) processing, respectively.Several structural neuroimaging studies have also identifiedvolumetric reduction in the left superior temporal gyrus (STG)in schizophrenia, themagnitude of which is associatedwith theseverity of formal thought disorder (Hirayasu et al., 1998; Pettyet al., 1995; Rossi et al., 1994; Shenton et al., 1992).
Thought disorder has been shown to be a sensitive andspecific predictor of schizophrenia and schizophrenia-spectrumdisorder in a variety of studies (Caplan, 1994; Caplan et al.,2000; Taylor and Amir, 1994). The severity of such abnormal-ities is also associated with long-term functional outcome(Racenstein et al., 2002; Racenstein et al., 1999; Richardsonet al., 2002). Moreover, sub-clinical disturbances in the natural
speech of healthy relatives of schizophrenic patients have beenreported, supporting the notion that communication distur-bances may be one manifestation of a genetic vulnerability topsychosis (Docherty and Gordinier, 1999). In addition, using aword/pseudo-word discrimination task, Li et al. (2007) foundthat—unlike healthy controls—schizophrenia patients and theirnon-ill siblings activated Brodmann's area 44 similarly for bothlanguage and non-language tasks, suggesting that fMRI mea-sures of language processing may be valuable for use in theprediction of risk for developing psychosis. Similarly, in a cross-sectional study of clinical high-risk individuals, patients withfirst episode psychosis and healthy volunteers, Broome et al.(2009) found that the at-risk group showed an intermediatepattern of activation in the inferior frontal cortex and anteriorcingulate during an overt verbalfluency task. Yet, whether suchabnormalities are predictive of illness onset remains unknown.
Thought disorder is typically measured behaviorally throughclinical interviews,making itmore challenging toevaluateduringa functional imaging study. In order to passively challenge similarcognitiveprocesses to those employed innatural speech, hereweevaluated the neural correlates of language processing, using anaturalistic task that involves listening to question and answersentence pairs, in individuals identified as putatively prodromalfor psychosis. This study represents the largest functional neuro-imaging study to date of clinical high-risk (CHR) individuals, andthe first to examine baseline neural predictors of outcome. Wehypothesized that CHR youth would show evidence of abnor-mality in brain regions critical for language function (i.e., inferiorfrontal and superior temporal regions), and that these alterationswould be exacerbated in those who subsequently developedpsychosis.Wealso examined the relationshipbetween activity inthese brain regions at baseline and severity of positive formalthought disorder and psychosocial outcome at follow-up.
2. Materials and methods
2.1. Subjects
Participants were 43 individuals at clinical high-risk forpsychosis (CHR) and 26 demographically matched healthy con-trols (HC) froma longitudinal prospective study at theCenter forthe Assessment and Prevention of Prodromal States (CAPPS) atUCLA (see Table 1 for sample characteristics). The CHR and HCgroup did not differ in terms of age, IQ, sex, handedness, norwere there significant differences in baseline symptom severityor medication usage between the CHR subjects who subse-quently converted to psychosis (CHR-P) and those who did not(CHR-NP). However, there was a trend for more males toconvert to psychosis (p=0.07); as such, region of interest (ROI)analyses of the CHR group included sex as a covariate.
Participantswere screenedwith the Structured Interview forProdromal Syndromes (SIPS, McGlashan et al., 2001) for thepresence of one of three putative prodromal syndromes, basedon attenuated subthreshold psychotic symptoms, transientpsychotic symptoms, or a substantial drop in social/rolefunctioning in conjunction with a diagnosis of schizotypalpersonality disorder or the presence of a first-degree relativewithapsychoticdisorder.HCyouthdidnotmeetDSM-IV criteriafor a psychiatric disorder as determined by the StructuredClinical Interview for DSM-IV—Patient Version (SCID-I/P; Firstand Pincus, 2002), did not have a first-degree family history of a
174 F.W. Sabb et al. / Schizophrenia Research 116 (2010) 173–183

psychoticdisorder, ormeet criteria for anyof the threeprodromalstates defined above. Additionally,we excludedparticipantswithany neurological disorder, drug or alcohol abuse/dependencewithin the past 6 months, or Full Scale IQ below 70. BaselineDSM-IV diagnoses in the clinical high risk (CHR) group are asfollows: Major Depressive Disorder (N=18), Social Phobia(N=3), Obsessive–compulsive Disorder (N=2), AlcoholAbuse, in full remission (N=2), Attention Deficit HyperactivityDisorder (ADHD; N=1), Adjustment Disorder (N=1), AnxietyDisorder—Not Otherwise Specified (NOS; N=5), DepressiveDisorder NOS (N=3), Pervasive Developmental Disorder NOS(N=2), Bipolar Disorder NOS (N=1), Psychosis NOS (N=1),and Eating Disorder NOS (N=1). All clinical interviews wereconducted by Master's-level or Ph.D. mental health specialists,after being trained to rigorous standards of reliability(ICC≥0.85). Detailed information on recruitment, inclusioncriteria, inter-rater reliability, and case consensus proceduresare described in detail elsewhere (Meyer et al., 2005; Niendamet al., 2006). All participants completed informed consentapproved by the UCLA Institutional Review Board.
One healthy and two CHR subjects were excluded fromanalysis due to relatively stringent criteria for motion (≥2 mmof absolute movement, and/or 0.5 mm of relative movementbetween brain volumes). Additionally, one healthy and oneCHR subject were excluded due to technical difficulties duringthe scan; thus, 40 CHR youth and 24 controls were included instatistical analyses.
2.2. Clinical follow-up
While we report only on baseline performance here, allparticipants also completed follow-up assessments approxi-mately every 6 months, up to a maximum of 24 months, duringwhich SCID and SIPS interviews were repeated, to determinechanges in symptom status. In addition, the Schedule forAssessment of Positive and Negative Symptoms (SANS/SAPS)
and measures of psychosocial functioning were rated by a Ph.D.or Master's-level clinician, Social functioning was assessed withthe Social Attainment Survey (SAS; Goldstein, 1978), whichcontains seven 5-point items evaluating peer and romanticrelationships and participation in activities. Scores on SAPSThought Disorder items (Illogical Thinking and Global FormalThought Disorder) and social functioning ratings from the finalfollow-up assessment point for each subject were used incorrelational analyses to assess whether baseline functionalimaging activitywas predictive of subsequent symptomseverityand social functioning.
Fifteen of our participants converted to psychosis during afollow-up assessment. Participants were considered ‘convertedto psychosis’ at follow-up based on SIPS diagnosis of a PsychoticSyndrome. Diagnosis of a psychotic syndrome refers to psychoticsymptomsof particular intensity (e.g., delusional conviction) andfrequencyorduration (1 h/dayat anaverage frequencyof4 days/week during the past month) or of particular impact (seriouslydisorganizing or dangerous), designed to operationalize thethreshold for a DSM-IV Axis I psychotic disorder diagnosis [i.e.,schizophrenia-spectrum disorder, mood disorder with psychoticfeatures, or psychosis not otherwise specified (NOS)]. DSM-IVdiagnoses attained at the point of conversion were determinedby direct SCID (First and Pincus, 2002) interview of the patientand their parent or guardian. During the course of follow-up,15 (35%) of the CHR participants converted to a psychoticdisorder: 5 (33%) were diagnosed with schizophrenia; 3 (20%)with schizoaffective disorder, depressive type; 1 (7%) withschizophreniform disorder; 1 (7%) with delusional disorder;2 (13%) with Bipolar I Disorder with psychotic features; and3 (20%)with Psychosis Not Otherwise Specified (NOS). Of the 40CHR subjects included in data analyses, the majority(N=22; 55%) completed follow-up assessments up to24 months, eight (20%) completed follow-up assessments up to12 months and ten (25%) completed 6-month follow-upassessments.
Table 1Baseline demographic characteristics: CHR subjects who did not develop psychosis (CHR-NP), CHR subjects who developed psychosis (CHR-P), and HealthyControls (HC).
Characteristic CHR not converted (N=25) CHR converted (N=15) HC (N=24) F/χ2 statistic, p-value
Demographic characteristicsAge at examination, mean (±SD) 16.8 (3.1) 18.4 (4.2) 18.5 (3.2) F=1.7, p=0.17% Female (N) a 40% (10) 13% (2) 50% (12) χ2=2.56, p=0.11% Right handed (N) 90% (22) 100% (15) 9% (23) χ2=2.59, p=0.27IQ b 107.0±17.2 109.1±14.5 110.9±14.5 F=1.7, p=0.71
Task performanceReasoning RT (ms) 4053 (487.0) 3985 (492.9) 4103 (257.8) F=0.37, p=0.69Reasoning % correct 0.80 (0.18) 0.79 (0.16) 0.84 (0.08) F=0.75, p=0.47Topic Maintenance RT (ms) 4386 (540.9) 4492 (365.9) 4587 (255.7) F=1.5, p=0.24Topic Maintenance % correct 0.85 (0.11) 0.83 (0.17) 0.86 (0.14) F=0.26, p=0.77
Clinical characteristicsSOPS mean positive symptom score (±SD) 2.2 (0.66) 2.6 (1.2) N/A F=2.0, p=0.17SOPS mean negative symptom (±SD) 1.9 (0.97) 2.5 (1.4) N/A F=2.24, p=0.14GAF score, mean (±SD) c 46.2 (12.5) 41.6 (16.3) 82.3 (10.2) F=66.8, p<0.001Current atypical antipsychotic use, n (%) 4 (16%) 3 (20%) N/A χ2=1.16, p=0.28Current mood stabilizer use, n (%) 2 (8%) 3 (21%) N/A χ2=1.45, p=0.23Current SSRI use, n (%) 7 (28%) 2 (14%) N/A χ2=0.95, p=0.33Current benzodiazepine use, n (%) 12% 14% N/A χ2=0.04, p=0.83a There was a trend toward a gender difference between CHR-P and CHR-NP (p=0.07).b IQ Estimate based on Wechsler Abbreviated Scale of Intelligence (WASI).c GAF scores did not differ significantly between CHR-P and CHR-NP (F=0.98, p=0.33).
175F.W. Sabb et al. / Schizophrenia Research 116 (2010) 173–183

2.3. Image acquisition
Scanning was performed on a Siemens 3-Tesla Allegrahead-only magnet. Subjects were placed in the scanner and asecond order shimming protocol was performed in order tominimize magnetic field inhomogeneities. We performedlocalizer scans from which we prescribed the functionalslices. Prior to functional scanning, we acquired a full brainhigh-resolution matched-bandwidth spin-echo echo-planarscan for between-subject registration (TR: 4 s, TE: 54 ms,1282 matrix, 3 mm/1 skip, 30 oblique-axial [AC-PC aligned]slices). From this volume, 28 slices were chosen co-planar tothe high-resolution structural scan to examine BOLD contrastacross time using a Gradient Echo echo-planar sequence (TR:3 s, TE:35 ms, 642 matrix, 3 mm/1 skip, 70 timepoints).
2.4. Task procedure
Given our aim to assess neural and clinical differencesbetween youth who convert and do not convert to psychosis,we required a reliable biomarker that would activate brainregions involved in language processing in young subjects.We chose a blocked naturalistic language processing taskpreviously validated in young subjects that assesses theability to comprehend discourse (Caplan and Dapretto, 2001;Dapretto et al., 2005). Briefly, the task consisted of twocondition blocks, ‘Topic Maintenance’ (TM) and ‘Reasoning’(R), with 24s of rest preceding each block, and 18s of restafter the second condition block. Each condition blockconsisted of a set of 12 question and answer pairs recordedby two female native-English speakers, presented at a rate of6s per pair (resulting in two 72 second blocks) over head-phones (Magnetic Resonance Technologies) and controlledusing E-prime software (Pittsburgh Software Tools) on aDELL-D810 computer. The order of the two conditions (TM orR) was counterbalanced across subjects. We instructedparticipants to respond as quickly as possible as to whethereach question–answer pair made sense by pushing a ‘yes’ or a‘no’ button on a button-box. In the TM block, we variedsentence features based on appraising whether the responseto the question was ‘on-topic’, thus tapping executivecomponents of language processing (context processing,monitoring, and working memory), while in the R block wevaried features of the underlying semantic logic of theconversation, which putatively involve both anterior andposterior language systems (Sabb et al., 2007; Bookheimer,2002; see Table 2). The order of on/off topic and logical/illogical answers within each block was randomized, with nomore than three answers of one kind occurring in a row.Participants' responses were later scored for accuracy andresponse times and compared using analysis of covariance(ANCOVA) with group (UHR-P, UHR-NP, HC) as the between-subject variable, covarying for sex.
2.5. Post-processing and statistical analysis
We processed the data using the FSL (v4) suite's FEAT tool(http://www.fMRIb.ox.ac.uk/fsl/). Following correction formovement between brain volumes (MCFLIRT), the datawere registered for group comparison in a two-step processusing first the high-resolution matched-bandwidth scan and
then a common reference brain (in MNI space) afterundergoing skull stripping (BET).
We modeled single subject data with a high-pass filter of144 s, a six-millimeter (FWHM) Gaussian smoothing kerneland pre-whitening (to account for the intrinsic temporalautocorrelation of the fMRI signal) with FMRIB's ImprovedLinear Model (FILM). Analyses used a mixed effects generallinear model (GLM), in which task condition (Reasoning orTopic Maintenance) was modeled as a within-subjects factorand diagnostic category was modeled as a between-subjectsfactor, using FSL's Local Analysis of Mixed Effects (FLAME,v5.91). After modeling individual subject data (i.e. FILM: level1), second level analyses (between subjects) were run usingFLAME-stage 1, providing z-maps of activity in each conditionfor each diagnostic group separately, and direct comparisonsof conditions between groups. Group contrasts were thre-sholded based on both the magnitude (minimum z-thresholdof 2.0, except where noted) and extent (all analyses used acorrected cluster threshold of p<0.05) of active voxels.
We additionally performed region of interest (ROI)analyses to explore relationships of neural activity to clinicaloutcome in brain regions that showed significant whole-braingroup differences between CHR and control subjects. Ana-tomical ROIs were chosen from the Laboratory of Neuroima-ging probabilistic atlas (Shattuck et al., 2008) for the leftinferior frontal gyrus (LIFG), the left temporal lobe (middleand inferior gyri), bilateral representation of the anteriorcingulate (ACC), the caudate, and superior frontal gyrus(SFG). Only voxels in these anatomical regions that hadpassed significant cluster thresholding in the general linearmodel (GLM) analysis of CHR vs. HC for either R–rest or R–TMwere included. This was done to increase localization of ourROIs to distinct neuroanatomical regions, as our activatedclusters frequently spanned multiple brain regions.
Table 2Example stimuli of question–answer pairs for each condition, TopicMaintenance and Reasoning.
Topic maintenance
On-topicQ How would you feel in an earthquake?A I run to my parents' room and I'm scaredQ What are you doing today?A I am playing tennis
Off topicQ How would you feel in an earthquake?A I go to Disneyland in the summerQ What are you doing today?A I call my mom sweetie
Reasoning
CongruentQ Do you like having fun?A Yeah, because it makes me happyQ Why are you wearing a raincoat?A So I won't get wet.
IncongruentQ Do you like having fun?A No, because it makes me happy.Q Why are you wearing a raincoat?A So I won't get sad.
176 F.W. Sabb et al. / Schizophrenia Research 116 (2010) 173–183

In order to perform an independent analysis of therelationship between brain activity and behavior (e.g.,Kriekesgort et al., 2009), we extracted parameter estimatesfrom the whole-brain GLM for each subject in the CHR groupusing the Featquery tool in FSL, which were then interrogatedin SPSS (v. 16.0) using Pearson partial correlations (adjustingfor sex) with Sidak's adjustment for multiple comparisons(Sankoh et al. 1997). Because the outcome variables weexamined (clinical and social functioning scores withinsubjects) are not independent, we used a corrected p-valueof 0.01 for these analyses, based on the mean correlation ofthe outcome variables (r=0.50).
3. Results
3.1. Behavioral results
There were no significant differences in reaction time oraccuracy between the three groups (CHR-P, CHR-NP, and HC),for either the Topic Maintenance or Reasoning conditions(see Table 1).
3.2. fMRI whole-brain analyses
Two whole-brain GLM analyses were conducted, the firstof which compared Topic Maintenance (TM) and Reasoning(R) conditions within and between the two groups (all CHRparticipants vs. HC; see Materials and methods section formodel details). The second analysis examined only the CHRgroup, directly comparing fMRI data at baseline for CHRindividuals who converted to psychosis at follow-up (CHR-P;n=15) with those who did not (CHR-NP; n=25). In each ofthese two whole-brain analyses, contrasts were set up toinvestigate group differences for each active task conditioncompared to rest (Reasoning–rest, Topic Maintenance–rest),as well as direct contrasts between task conditions (Reason-ing–Topic Maintenance, and the reverse). Following theseanalyses, we performed ROI analyses to further interrogateneural activity in regions showing significant between-groupdifferences.
3.2.1. Clinical high risk (CHR) vs. healthy controls (HC)To assess reliability of the task, our first contrast compared
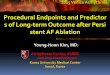
Reasoning (R) vs. rest and Topic Maintenance (TM) vs. rest inCHR and HC subjects (see Fig. 1). Consistent with previousstudies (Caplan and Dapretto, 2001; Dapretto et al., 2005),this contrast revealed a bilateral network of brain regionsinvolved in discourse processing across all CHR participants(Fig. 1, left) and healthy controls (Fig. 1, right). These regionswere qualitatively similar between task conditions, andincluded the bilateral inferior temporal lobe, middle temporalgyrus, hippocampus, inferior frontal gyrus, and precentralgyrus.
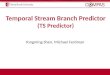
Direct comparison of the groups (CHR, HC) and conditions(R, TM) revealed two contrasts in which the CHR groupshowed significantly more activity than HC (see Fig. 2). First,the CHR group showed significantly more activity than HC inthe Reasoning condition (vs. rest) in the left inferior frontalgyrus, anterior cingulate, left inferior and middle temporalgyri, and occipital cortex (z voxel height threshold of >1.7,and corrected cluster threshold of p<0.05). Similarly, we
found an interaction in the direct contrast of Reasoning vs.Topic Maintenance between groups (R>TM for CHR>HC);the CHR group showed more activity than HC in medialprefrontal regions, anterior cingulate, left inferior frontalgyrus, bilateral caudate, and posterior brain structures(lingual gyrus and occipital lobe; z>1.7, p<0.05).
3.2.2. CHR intra-group comparison: converters (CHR-P) vs.nonconverters (CHR-NP)
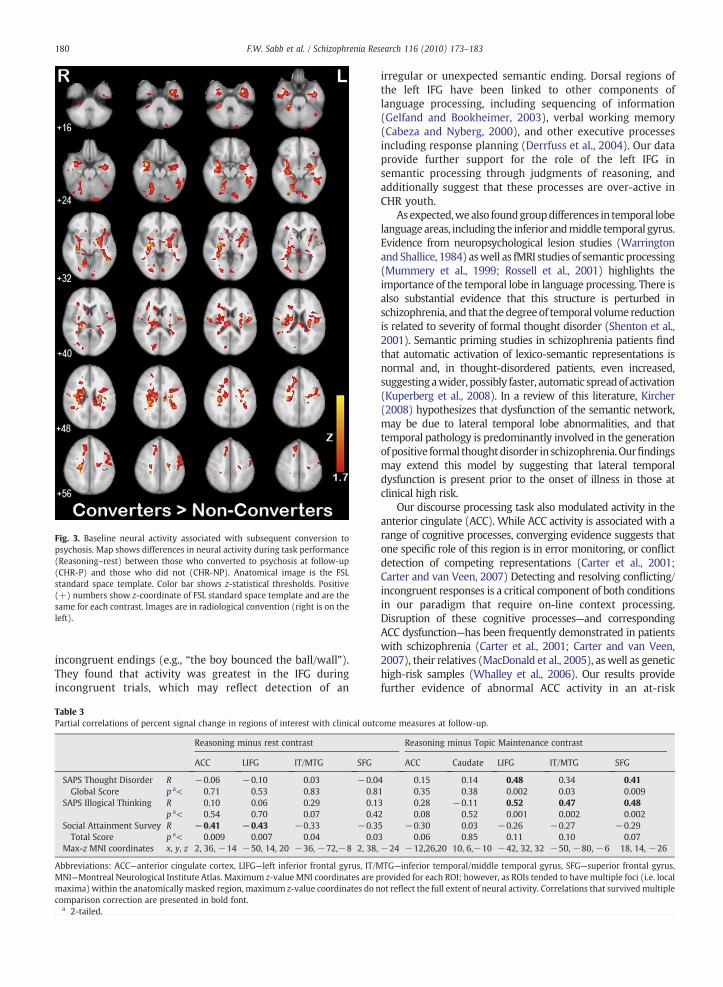
Given the smaller sample size in this analysis, whenexamining interactions between group (CHR-P, CHR-NP) andcondition (TM, R), we used a mask comprised of voxels thatwere previously active in the CHR-P group main effectcontrast of all minus rest, in order to reduce noise fromvoxels that did not pass significance within group. In theReasoning condition (minus rest), the CHR-P group showedsignificantly more activity than CHR-NP in a network of brainregions including bilateral temporal lobe, frontal operculum,left precentral gyrus, caudate, and other striatal regions (seeFig. 3; voxel height threshold of z>1.7, and corrected clusterthreshold of p<0.05). In contrast, there were no regionswhere the CHR-NP group demonstrated increased activityrelative to the CHR-P group, and no other condition showedsignificant differences between the groups.
3.3. Neural activity and clinical outcome
All regions of interest (ROIs) were determined fromsignificantly active voxels in the (first) whole-brain analysisthat directly compared the entire CHR group and healthycontrols (see Fig. 2). Thus, only voxels that were significantlyrelated to performance of the task (i.e. all-rest) were includedin the ROI analysis. From these contrasts, we used function-ally thresholded anatomical ROIs of the left inferior frontalgyrus (LIFG), left temporal lobe (middle and inferior gyri),bilateral representation of the anterior cingulate (ACC),caudate, and superior frontal gyrus (SFG), as described inthe Materials and methods section.
The relationship between percent signal change in theseROIs during task performance at baseline to clinical outcome(psychosocial functioning and severity of thought disorder)was then examined within the CHR group, with sex as acovariate. We found significant relationships—which sur-vived multiple comparison adjustment—between signalchange in the Reasoning minus Topic Maintenance contrastfor the LIFG, temporal lobe, and superior frontal gyrus andthought disorder scores, as assessed by the SAPS (IllogicalThinking and Global Formal Thought Disorder). In addition,signal change in the ACC and left IFG was inversely correlatedwith Social Attainment Survey scores at follow-up, indicatingthat greater activation in these regions during task perfor-mance predicted poorer social function at follow-up (Rea-soning minus rest; see Table 3 and Fig. 4).
4. Discussion
This is the first study to our knowledge to demonstratepredictors of outcome in a clinically at-risk sample forpsychosis using a baseline functional neuroimaging pheno-type. Here we identified a network of brain regions that wasdifferentially involved for those at risk for developing
177F.W. Sabb et al. / Schizophrenia Research 116 (2010) 173–183
psychosis compared to healthy matched controls duringperformance on a naturalistic discourse processing task.Overall, the task elicited activity in the expected network ofregions typically engaged in language tasks, including theinferior frontal gyrus (IFG), bilateral medial prefrontal regions,inferior and middle temporal gyri, as well as the anteriorcingulate. However, clinical high risk (CHR) participantsshowed increased neural activity relative to healthy controls,in the medial prefrontal lobe bilaterally and anterior cingulate,as well as left IFG and left inferior and middle temporal gyri.Further, relative to CHR participants who did not developpsychosis, CHR subjects who subsequently developed psycho-
sis showed a pattern of relative over-activation in language-associated brain regions, including the left inferior frontalgyrus and inferior temporal lobe, as well as bilateral striatumand thalamus, and the frontal operculum. Our findings ofrelative hyper-activation of language-related brain regionsduring discourse processing in youth at high risk for psychosisare consistent with a hypothesis of neural inefficiency in thesevulnerable individuals (Karlsgodt et al., 2007; Potkin et al.,2009). These patterns are consistent with data from high-functioning patients with schizophrenia who show compen-satory increases in brain activity during task performance(Karlsgodt et al., 2009).
Fig. 1. Discourse processing activity for Reasoning and Maintenance conditions in each group. Depicts four contrasts: Reasoning minus rest for clinical high-risk(CHR) participants (top left) and healthy controls (HC; top right), and Topic Maintenance minus rest for each group (bottom). Anatomical image is the FSLstandard space template. Color bar shows z-statistical thresholds. Maps were thresholded with a z-statistic greater than 2.0 and a corrected cluster threshold ofp<0.05. Positive (+) numbers show z-coordinate of FSL standard space template and are the same for each contrast. Images are in radiological convention (rightis on the left).
178 F.W. Sabb et al. / Schizophrenia Research 116 (2010) 173–183
Our results also indicate that baseline neural activity duringdiscourse processing was related to severity of positive formalthought disorder at follow-up, as well as social outcome. Inparticular, increased activity in the left ventral inferior frontalgyrus (during task performance in theReasoning condition)wasassociated with increased severity of formal thought disorder atfollow-up. Conversely, increased activity in the dorsal region ofthe inferior frontal gyrus was associated with poorer socialoutcome at follow-up, indicating that the observed patterns ofrelative hyper-activation in language-related brain regions haveprognostic significance. Interestingly, cross-sectional associa-tions between neural activity in these regions and concurrentclinical status (psychosocial functioning and severity of thoughtdisorder) were not nearly as robust as were these predictiverelationships. Specifically, there was only a significant inversecorrelation (at the p<0.01 level) between neural activity in theanterior cingulate and Social Attainment scores (r=−0.39;p<0.008). The significant associations between baseline neuralactivity in frontal and temporal ROIs and measures of thoughtdisorder thatwere observed at follow-updid not reach this level
of significance in the cross-sectional baseline comparisons.Because thought disorder scores tended to increase over thefollow-up period in those who converted, the range of scores atbaselinewas restricted,which likely attenuated thefindings. Theresults of ourpredictive analysesmayhelp improve the accuracyof existing algorithms that attempt to predict those at greatestrisk for psychosis based on clinical characteristics. Developingmultivariate prediction algorithms for determining risk—thatinclude functional and structural neuroimaging data—couldprovide additional information, as changes in neural activitycould predate symptoms.
In this study, we found that portions of both dorsal andventral left inferior frontal gyrus were activated to a greaterdegree during semantic reasoning judgments in CHRindividuals relative to healthy controls. Numerous fMRIstudies have revealed the contributions of the left ventralaspects of IFG to language processing (Badre and Wagner,2004; Dapretto and Bookheimer, 1999; Sabb et al., 2007),and specifically the evaluation of semantic incongruencies insentence processing. For example, Cardillo et al. (2004) used
Fig. 2. Discourse processing–group×condition interaction. Statistical maps showing regions in which activity in the comparison of conditions differed betweengroups (healthy controls vs. CHR participants). Reasoning minus rest is presented on the left, and the direct comparison of the two task conditions (Reasoningminus Topic Maintenance) is presented on the right. These maps determined regions that were further interrogated in ROI analyses. Anatomical image is the FSLstandard space template. Both maps were thresholded with a z-statistic greater than 1.7 and a corrected cluster threshold of p<0.05. Positive (+) numbers showz-coordinate of FSL standard space template and are the same for each contrast. Images are in radiological convention (right is on the left).
179F.W. Sabb et al. / Schizophrenia Research 116 (2010) 173–183
a sentence processing task with semantically congruent and
incongruent endings (e.g., “the boy bounced the ball/wall”).They found that activity was greatest in the IFG duringincongruent trials, which may reflect detection of an
irregular or unexpected semantic ending. Dorsal regions ofthe left IFG have been linked to other components oflanguage processing, including sequencing of information(Gelfand and Bookheimer, 2003), verbal working memory(Cabeza and Nyberg, 2000), and other executive processesincluding response planning (Derrfuss et al., 2004). Our dataprovide further support for the role of the left IFG insemantic processing through judgments of reasoning, andadditionally suggest that these processes are over-active inCHR youth.
As expected,wealso foundgroupdifferences in temporal lobelanguage areas, including the inferior andmiddle temporal gyrus.Evidence from neuropsychological lesion studies (Warringtonand Shallice, 1984) aswell as fMRI studies of semantic processing(Mummery et al., 1999; Rossell et al., 2001) highlights theimportance of the temporal lobe in language processing. There isalso substantial evidence that this structure is perturbed inschizophrenia, and that thedegree of temporal volume reductionis related to severity of formal thought disorder (Shenton et al.,2001). Semantic priming studies in schizophrenia patients findthat automatic activation of lexico-semantic representations isnormal and, in thought-disordered patients, even increased,suggestingawider, possibly faster, automatic spreadof activation(Kuperberg et al., 2008). In a review of this literature, Kircher(2008) hypothesizes that dysfunction of the semantic network,may be due to lateral temporal lobe abnormalities, and thattemporal pathology is predominantly involved in the generationofpositive formal thoughtdisorder in schizophrenia.Ourfindingsmay extend this model by suggesting that lateral temporaldysfunction is present prior to the onset of illness in those atclinical high risk.
Our discourse processing task also modulated activity in theanterior cingulate (ACC). While ACC activity is associated with arange of cognitive processes, converging evidence suggests thatone specific role of this region is in error monitoring, or conflictdetection of competing representations (Carter et al., 2001;Carter and van Veen, 2007) Detecting and resolving conflicting/incongruent responses is a critical component of both conditionsin our paradigm that require on-line context processing.Disruption of these cognitive processes—and correspondingACC dysfunction—has been frequently demonstrated in patientswith schizophrenia (Carter et al., 2001; Carter and van Veen,2007), their relatives (MacDonald et al., 2005), as well as genetichigh-risk samples (Whalley et al., 2006). Our results providefurther evidence of abnormal ACC activity in an at-risk
Fig. 3. Baseline neural activity associated with subsequent conversion topsychosis. Map shows differences in neural activity during task performance(Reasoning–rest) between those who converted to psychosis at follow-up(CHR-P) and those who did not (CHR-NP). Anatomical image is the FSLstandard space template. Color bar shows z-statistical thresholds. Positive(+) numbers show z-coordinate of FSL standard space template and are thesame for each contrast. Images are in radiological convention (right is on theleft).
Table 3Partial correlations of percent signal change in regions of interest with clinical outcome measures at follow-up.
Reasoning minus rest contrast Reasoning minus Topic Maintenance contrast
ACC LIFG IT/MTG SFG ACC Caudate LIFG IT/MTG SFG
SAPS Thought DisorderGlobal Score
R −0.06 −0.10 0.03 −0.04 0.15 0.14 0.48 0.34 0.41p a< 0.71 0.53 0.83 0.81 0.35 0.38 0.002 0.03 0.009
SAPS Illogical Thinking R 0.10 0.06 0.29 0.13 0.28 −0.11 0.52 0.47 0.48p a< 0.54 0.70 0.07 0.42 0.08 0.52 0.001 0.002 0.002
Social Attainment SurveyTotal Score
R −0.41 −0.43 −0.33 −0.35 −0.30 0.03 −0.26 −0.27 −0.29p a< 0.009 0.007 0.04 0.03 0.06 0.85 0.11 0.10 0.07
Max-z MNI coordinates x, y, z 2, 36, −14 −50, 14, 20 −36, −72,−8 2, 38, −24 −12,26,20 10, 6,−10 −42, 32, 32 −50, −80, −6 18, 14, −26
Abbreviations: ACC—anterior cingulate cortex, LIFG—left inferior frontal gyrus, IT/MTG—inferior temporal/middle temporal gyrus, SFG—superior frontal gyrus,MNI—Montreal Neurological Institute Atlas. Maximum z-value MNI coordinates are provided for each ROI; however, as ROIs tended to have multiple foci (i.e. localmaxima) within the anatomically masked region, maximum z-value coordinates do not reflect the full extent of neural activity. Correlations that survivedmultiplecomparison correction are presented in bold font.
a 2-tailed.
180 F.W. Sabb et al. / Schizophrenia Research 116 (2010) 173–183

population, although further studies are needed to address theprecise nature of this dysfunction.
Certain limitations of this study should be noted. We used anaturalistic task that had previously been validated in adole-scents, in order to maximize comprehension and accurateperformance. While we found strong activation patterns in theReasoning condition, results were less consistent in the TopicMaintenance condition, with much more variability in fMRIsignal between subjects. This could be due partially to the blockdesign employed here. Although this design allowed maximumpower to detect subtle differences in conditions between groups,we were unable to investigate the timecourse of processing ofincongruous information. Future investigations using trial-baseddesigns in CHR populations are clearly warranted to furthercharacterize the contributionof thenetworkofbrain regions seenhere that are putatively important for a complex phenotype suchas discourse processing. In addition, as with all studies involvingpsychiatric populations, medication is a potential confound. Inour study, several of the CHR participants were taking psycho-active medication although only a minority were taking atypicalantipsychotics. However, baseline medications did not differbetween those who later converted and those who did not, andtherefore could not account for group differences in activationpatterns. In addition, there was no relationship betweenantipsychotic medication use and activation in the brain regionsthat were differentially engaged across groups (p>0.20).Nevertheless, we fully acknowledge that our study was notdesigned to examine differential effects of medications, and thiscould be better addressed in the context of a randomized clinicaltrial in which treatment is standardized.
5. Conclusions
Identifying predictors and mechanisms of conversion topsychosis among individuals ascertained in a clinical high risk orprodromal state is a critical next step along the pathway toprevention strategies. Our results suggest that neural activityduring discourse processing has important predictive implica-tions, as it is associated with subsequent thought disorderseverity and social outcome. This is the first study, to ourknowledge, to demonstrate functional differences in activitybetween those who convert to psychosis and those who do not,prior to illness onset. These findings may suggest strategies forthedevelopmentof novel preventive treatments that cancorrector compensate for the specific neurodevelopmental andpsychological changes associated with the formation of psy-chotic symptoms during late adolescence and early adulthood.
Role of funding sourceNone of the sources of funding had any role in the design, collection,
analysis, nor interpretation of data. Nor did they have a role in writing thereport or the decision to submit the manuscript for publication.
ContributorsCEB designed and directed the study, and contributed to collaborative
writingof themanuscript. FWSperformedfinalmodelingandanalysis of thedataand collaborative writing of the manuscript. TvE and MEH performed theexperimentandprovided initial quality assurance, scoring, andanalysis ofprojectdata, as well as manuscript edits. MD and RC designed the task and edited themanuscript. TDCprovided input into the studydesignand edited themanuscript.
Conflict of interestNone of the authors report any biomedical financial interests or potential
conflicts of interest.
Fig. 4. Correlations between clinical characteristics and ROI activity in the LIFG. Brains depict neural activity for Reasoning vs. rest comparison (yellow) andReasoning vs. Maintenance (orange) for CHR>controls. Left panel displays left dorsal IFG activity for Reasoning vs. rest, while right panel displays left ventral IFGactivity (Reasoning vs. Maintenance contrast). Graphs show correlation of percent signal change (x-axis) in these ROIs with scores on clinical measures at follow-up(y-axis). Top graph shows relationship of neural activity in dorsal IFG to follow-up Social Attainment Survey (SAS) scores,while bottomgraph shows correlation of %signal change in ventral IFGwith SAPS Thought Disorder Global Score at follow-up. As shown in Table 3, correlationswere significant within the entire group of CHRparticipants. Those who subsequently converted to psychosis (CHR-P) and those who did not (CHR-NP) are shown separately here (blue= CHR-NP, red= CHR-P).Bothmaps were thresholded with a z-statistic greater than 1.7 and a corrected cluster threshold of p<0.05. Images are in radiological convention, displayed on theFSL standard brain.
181F.W. Sabb et al. / Schizophrenia Research 116 (2010) 173–183

AcknowledgementsThe authors would like to thank the following individuals for their
contributions to this project: Adrienne Gallet, Maria Garcia, Sandra DeSilva,Ph.D., Tara Niendam, Ph.D., and Jamie Zinberg, M.A. This research wassupported by the following grants: NARSAD Young Investigator Award(Maxine and Jack Zarrow Investigator Award to C.E.B.), NIMH MH65079 andNIMH P50 MH066286, as well as donations from the Rutherford CharitableFoundation and Staglin Music Festival for Mental Health to the UCLAFoundation.
References
Arboleda, C., Holzman, P.S., 1985. Thought disorder in children at risk forpsychosis. Arch. Gen. Psychiatry 42 (10), 1004–1013.
Badre, D., Wagner, A.D., 2004. Selection, integration, and conflict monitoring;assessing the nature and generality of prefrontal cognitive controlmechanisms. Neuron 41 (3), 473–487.
Bookheimer, S., 2002. Functional MRI of language: new approaches tounderstanding the cortical organization of semantic processing. Annu.Rev. Neurosci. 25, 151–188.
Broome,M.R.,Matthiasson,P., Fusar-Poli, P.,Woolley, J.B., Johns, L.C., Tabraham,P.,Bramon, E., Valmaggia, L.,Williams, S.C.R., Brammer,M.J., Chitnis,X.,McGuire,P.K., 2009. Neural correlates of executive function and working memory inthe ‘at-risk mental state’. Br. J. Psychiatry (194), 25–33.
Cabeza, R., Nyberg, L., 2000. Imaging cognition II: an empirical review of 275PET and fMRI studies. J. Cogn. Neurosci. 12 (1), 1–47.
Cannon, T.D., Cadenhead, K., Cornblatt, B.,Woods, S.W., Addington, J., Walker, E.,Seidman, L.J., Perkins, D., Tsuang,M.,McGlashan, T., et al., 2008. Prediction ofpsychosis in youth at high clinical risk: a multisite longitudinal study inNorth America. Arch. Gen. Psychiatry 65 (1), 28–37.
Caplan, R., 1994. Thought disorder in childhood. J. Am. Acad. Child Adolesc.Psych. 33 (5), 605–615.
Caplan, R., Dapretto,M., 2001.Making sense during conversation: an fMRI study.NeuroReport 12 (16), 3625–3632.
Caplan, R., Guthrie,D., Tang, B., Komo, S., Asarnow,R.F., 2000.Thoughtdisorder inchildhood schizophrenia: replication and update of concept. J. Am. Acad.Child Adolesc. Psych. 39 (6), 771–778.
Cardillo, E.R., Aydelott, J., Matthews, P.M., Devlin, J.T., 2004. Left inferiorprefrontal cortex activity reflects inhibitory rather than facilitatory priming.J. Cogn. Neurosci. 16 (9), 1552–1561.
Carter, C.S., van Veen, V., 2007. Anterior cingulate cortex and conflict detection:an update of theory and data. Cogn. Affect. Behav. Neurosci. 7 (4), 367–379.
Carter, C.S., Botvinick, M.M., Cohen, J.D., 1999. The contribution of the anteriorcingulate cortex to executive processes in cognition. Rev. Neurosci. 10 (1),49–57.
Carter, C.S., MacDonald III, A.W., Ross, L.L., Stenger, V.A., 2001. Anterior cingulatecortex activity and impaired self-monitoring of performance in patientswith schizophrenia: an event-related fMRI study. Am. J. Psychiatry 158 (9),1423–1428.
Chao, L.L., Haxby, J.V., Martin, A., 1999. Attribute-based neural substrates intemporal cortex for perceiving and knowing about objects. Nat. Neurosci.2 (10), 913–919.
Dapretto, M., Bookheimer, S.Y., 1999. Form and content: dissociating syntaxand semantics in sentence comprehension. Neuron 24 (2), 427–432.
Dapretto,M., Lee, S.S., Caplan, R., 2005. A functionalmagnetic resonance imagingstudy of discourse coherence in typically developing children. NeuroReport16 (15), 1661–1665.
Derrfuss, J., Brass, M., von Cramon, D.Y., 2004. Cognitive control in the posteriorfrontolateral cortex: evidence from common activations in task coordina-tion, interference control, and working memory. Neuroimage 23 (2),604–612.
Docherty, N.M., Gordinier, S.W., 1999. Immediate memory, attention andcommunication disturbances in schizophrenia patients and theirrelatives. Psychol. Med. 29 (1), 189–197.
First, M.B., Pincus, H.A., 2002. The DSM-IV Text Revision: rationale and potentialimpact on clinical practice. Psychiatr. Serv. 53 (3), 288–292.
Fletcher, P., 1998. The missing link: a failure of fronto-hippocampal integrationin schizophrenia. Nat. Neurosci. 1 (4), 266–267.
Frith, C.D., Friston,K.J., Herold, S., Silbersweig, D., Fletcher, P., Cahill, C., Dolan, R.J.,Frackowiak, R.S., Liddle, P.F., 1995. Regional brain activity in chronicschizophrenic patients during theperformance of a verbalfluency task. Br. J.Psychiatry 167 (3), 343–349.
Gelfand, J.R., Bookheimer, S.Y., 2003. Dissociating neural mechanisms oftemporal sequencing and processing phonemes. Neuron 38 (5), 831–842.
Glahn, D.C., Laird, A.R., Ellison-Wright, I., Thelen, S.M., Robinson, J.L.,Lancaster, J.L., Bullmore, E., Fox, P.T., 2008. Meta-analysis of gray matteranomalies in schizophrenia: application of anatomic likelihood estima-tion and network analysis. Biol. Psychiatry 64 (9), 774–781.
Goldstein, M., 1978. Further data concerning the relation between premorbidadjustment and paranoid symptomatology. Schizophr. Bull. 4, 236–241.
Hirayasu, Y., Shenton, M.E., Salisbury, D.F., Dickey, C.C., Fischer, I.A., Mazzoni, P.,Kisler, T., Arakaki, H., Kwon, J.S., Anderson, J.E., et al., 1998. Lower lefttemporal lobe MRI volumes in patients with first-episode schizophreniacompared with psychotic patients with first-episode affective disorder andnormal subjects. Am. J. Psychiatry 155 (10), 1384–1391.
Karlsgodt, K.H.,Glahn,D.C., vanErp, T.G., Therman, S.,Huttunen,M.,Manninen,M.,Kaprio, J., Cohen, M.S., Lonnqvist, J., Cannon, T.D., 2007. The relationshipbetween performance and fMRI signal during working memory in patientswith schizophrenia, unaffected co-twins, and control subjects. Schizophr. Res.89 (1–3), 191–197.
Karlsgodt, K.H., Sanz, J., vanErp, T.G., Bearden, C.E., Nuechterlein, K.H., Cannon, T.D.,2009. Re-evaluating dorsolateral prefrontal cortex activation during workingmemory in schizophrenia. Schizophr. Res. 108 (1–3), 143–150.
Kerns, J.G., Cohen, J.D., MacDonald III, A.W., Cho, R.Y., Stenger, V.A., Carter, C.S.,2004. Anterior cingulate conflict monitoring and adjustments in control.Science 303 (5660), 1023–1026.
Kircher, T., 2008. Neurobiological foundations of thought and languagedisorder in schizophrenia. Fortschr. Neurol. Psychiatr. 76 (Suppl 1),S24–S32.
Kircher, T.T., Liddle, P.F., Brammer,M.J.,Williams, S.C.,Murray, R.M.,McGuire, P.K.,2001. Neural correlates of formal thought disorder in schizophrenia:preliminary findings from a functional magnetic resonance imaging study.Arch. Gen. Psychiatry 58 (8), 769–774.
Kriekesgort, N., Simmons, W.K., Bellgowan, P.S.F., Baker, C.I., 2009. Circularanalysis in systems neuroscience—the dangers of double dipping. NatNeurosci. 12 (5), 535–540.
Kuperberg, G.R., Lakshmanan, B.M., Caplan, D.N., Holcomb, P.J., 2006. Makingsense of discourse: an fMRI study of causal inferencing across sentences.Neuroimage 33 (1), 343–361.
Kuperberg, G.R., West, W.C., Lakshmanan, B.M., Goff, D., 2008. Functionalmagnetic resonance imaging reveals neuroanatomical dissociationsduring semantic integration in schizophrenia. Biol. Psychiatry 64 (5),407–418.
Li, X., Branch, C.A., Ardekani, B.A., Bertisch, H., Hicks, C., DeLisi, L.E., 2007. fMRIstudy of language activation in schizophrenia, schizoaffective disorder andin individuals genetically at high risk. Schizophr. Res. 96 (1–3), 14–24.
MacDonald III, A.W., Carter, C.S., Kerns, J.G., Ursu, S., Barch, D.M., Holmes, A.J.,Stenger, V.A., Cohen, J.D., 2005. Specificity of prefrontal dysfunction andcontext processing deficits to schizophrenia in never-medicated patientswith first-episode psychosis. Am. J. Psychiatry 162 (3), 475–484.
McGlashan, T.H., 1996. Early detection and intervention in schizophrenia:research. Schizophr. Bull. 22 (2), 327–345.
McGlashan, T.H., Miller, T.J., Woods, S.W., 2001. Pre-onset detection andintervention research in schizophrenia psychoses: current estimates ofbenefit and risk. Schizophr. Bull. 27 (4), 563–570.
McGorry, P.D., Yung, A.R., Phillips, L.J., 2003. The “close-in” or ultra high-riskmodel: a safe and effective strategy for research and clinical intervention inprepsychotic mental disorder. Schizophr. Bull. 29 (4), 771–790.
Meyer, S.E., Bearden, C.E., Lux, S.R., Gordon, J.L., Johnson, J.K., O'Brien, M.P.,Niendam, T.A., Loewy, R.L., Ventura, J., Cannon, T.D., 2005. The psychosisprodrome in adolescent patients viewed through the lens of DSM-IV. J.Child Adolesc. Psychopharmacol. 15 (3), 434–451.
Miklowitz, D.J., Velligan, D.I., Goldstein, M.J., Nuechterlein, K.H., Gitlin, M.J.,Ranlett, G., Doane, J.A., 1991. Communication deviance in families ofschizophrenic and manic patients. J. Abnorm. Psychology 100 (2),163–173.
Morey, R.A., Inan, S., Mitchell, T.V., Perkins, D.O., Lieberman, J.A., Belger, A.,2005. Imaging frontostriatal function in ultra-high-risk, early, andchronic schizophrenia during executive processing. Arch. Gen. Psychi-atry 62 (3), 254–262.
Mummery, C.J., Shallice, T., Price, C.J., 1999. Dual-process model in semanticpriming: a functional imaging perspective. Neuroimage 9 (5), 516–525.
Niendam, T.A., Bearden, C.E., Johnson, J.K., McKinley, M., Loewy, R., O'Brien, M.,Nuechterlein, K.H., Green, M.F., Cannon, T.D., 2006. Neurocognitiveperformanceand functional disability in thepsychosisprodrome. Schizophr.Res. 84 (1), 100–111.
Petty, R.G., Barta, P.E., Pearlson, G.D., McGilchrist, I.K., Lewis, R.W., Tien, A.Y.,Pulver, A., Vaughn, D.D., Casanova, M.F., Powers, R.E., 1995. Reversal ofasymmetry of the planum temporale in schizophrenia. Am. J. Psychiatry152 (5), 715–721.
Potkin, S.G., Turner, J.A., Brown, G.G., McCarthy, G., Greve, D.N., Glover, G.H.,Manoach, D.S., et al., 2009. Working memory and DLPFC inefficiency inschizophrenia: the FBIRN study. Schizophr. Bull. 35 (1), 19–31.
Racenstein, J.M., Penn, D., Harrow, M., Schleser, R., 1999. Thought disorder andpsychosocial functioning in schizophrenia: the concurrent and predictiverelationships. J. Nerv. Ment. Disabil. 187 (5), 281–289.
Racenstein, J.M., Harrow, M., Reed, R., Martin, E., Herbener, E., Penn, D.L.,2002. The relationship between positive symptoms and instrumental
182 F.W. Sabb et al. / Schizophrenia Research 116 (2010) 173–183

work functioning in schizophrenia: a 10 year follow-up study. Schizophr.Res. 56 (1–2), 95–103.
Richardson, J.L., Martin, E.M., Jimenez, N., Danley, K., Cohen, M., Carson, V.L.,Sinclair, B., Racenstein, J.M., Reed, R.A., Levine, A.M., 2002. Neuropsy-chological functioning in a cohort of HIV infected women: importance ofantiretroviral therapy. J. Int. Neuropsychol. Soc. 8 (6), 781–793.
Rossell, S.L., Bullmore, E.T., Williams, S.C., David, A.S., 2001. Brain activationduring automatic and controlled processing of semantic relations: apriming experiment using lexical-decision. Neuropsychologia 39 (11),1167–1176.
Rossi, A., Serio, A., Stratta, P., Petruzzi, C., Schiazza, G., Mancini, F., Casacchia, M.,1994. Planum temporale asymmetry and thought disorder in schizophre-nia. Schizophr. Res. 12 (1), 1–7.
Sabb, F.W., Bilder, R.M., Chou, M., Bookheimer, S.Y., 2007. Working memoryeffects on semantic processing: priming differences in pars orbitalis.Neuroimage 37 (1), 311–322.
Sankoh, A.J., Huque, M.F., Dubey, S.D., 1997. Some comments on frequentlyused multiple endpoint adjustments methods in clinical trials. Stat. Med.16, 2529–2542.
Seiferth, N.Y., Pauly, K., Habel, U., Kellermann, T., Shah, N.J., Ruhrmann, S.,Klosterkotter, J., Schneider, F., Kircher, T., 2008. Increased neural response
related to neutral faces in individuals at risk for psychosis. Neuroimage40 (1), 289–297.
Shattuck, D.W., Mirza, M., Adisetiyo, V., Hojatkashani, C., Salamon, G., Narr, K.L.,Poldrack, R.A., Bilder, R.M., Toga, A.W., 2008. Construction of a 3Dprobabilistic atlas of human cortical structures. Neuroimage 39 (3),1064–1080.
Shenton,M.E., Kikinis, R., Jolesz, F.A., Pollak, S.D., LeMay,M.,Wible, C.G.,Hokama,H., Martin, J., Metcalf, D., Coleman, M., et al., 1992. Abnormalities of the lefttemporal lobe and thought disorder in schizophrenia. A quantitativemagnetic resonance imaging study. N. Engl. J. Med. 327 (9), 604–612.
Shenton, M.E., Dickey, C.C., Frumin, M., McCarley, R.W., 2001. A review of MRIfindings in schizophrenia. Schizophr. Res. 49 (1–2), 1–52.
Taylor, M.A., Amir, N., 1994. Are schizophrenia and affective disorder related?:the problem of schizoaffective disorder and the discrimination of thepsychoses by signs and symptoms. Compr. Psychiatry 35 (6), 420–429.
Warrington, E.K., Shallice, T., 1984. Category specific semantic impairments.Brain 107 (Pt 3), 829–854.
Whalley,H.C., Simonotto, E.,Moorhead,W.,McIntosh,A.,Marshall, I., Ebmeier, K.P.,Owens, D.G., Goddard, N.H., Johnstone, E.C., Lawrie, S.M., 2006. Functionalimaging as a predictor of schizophrenia. Biol. Psychiatry 60 (5), 454–462.
183F.W. Sabb et al. / Schizophrenia Research 116 (2010) 173–183








![Critical Ultrasound Journal · According to the ‘Neurosonology in Acute Ischemic Stroke study,’ TCCS is an independent predictor for stroke patient's outcome [17]. Assessment](https://img.pdfslide.us/doc/110x75/5f0e68317e708231d43f1868/critical-ultrasound-journal-according-to-the-aneurosonology-in-acute-ischemic.jpg)