-
7/28/2019 Laligham Cav
1/13
Surgical Resection of Cavernous Malformations of the Brainstem:
Evolution ofa Minimally Invasive Technique
Jeffrey C. Mai, Dinesh Ramanathan, Louis J. Kim, Laligam N.
Sekhar
INTRODUCTION
Cavernous malformations (cavernomas)
have an estimated prevalence of approxi-
mately 0.4% to 0.8% in the population (4,
25, 29, 37, 38, 40, 43), with approximately
40% discovered incidentally(28). Prospec-
tive observation has indicated an overall
symptomatic rate of hemorrhage of 0.22%
to 0.7% per year for these lesions (15, 26,
37). Nevertheless, data from cavernous
malformations situatedin thebrainstem sug-
gest a markedly greater propensity for bleed-
ing.In retrospective analyses of patientswith
such lesions, a calculated annual average
symptomatic hemorrhage rate of 2.7% to 5%and re-hemorrhage rate
of 21% to 60% per
year and per lesion was discovered (1, 14, 23,
25,27, 33). In accordance withtheir location,
hemorrhages of brainstemcavernousmalfor-
mationscarriedwiththemahighlevelofmor-
bidity and mortality(14,23).
Given the significant risk of death and
disability presented by expectant manage-
ment of cavernous malformations of the
brainstem (CMBs), surgical resection has
been increasingly advocated for therapy(2,
13, 14, 16, 33, 39, 42). Over this timeframe,
imaging technologies have significantly
improved (5, 10-12, 43), and surgical tech-
niques have been refined for approaching
lesions of the brainstem (6, 13, 14, 24, 25,
32, 35, 39, 42). Here, we report our case
series of 22 surgically treated brainstem
cavernomas, their presentation, and out-
comes, as well as describe the general prin-
ciples guiding surgical resection.
PATIENTS AND METHODSFrom 2005 to 2010, 22 consecutive
patients
underwent 27 procedures for resections of
brainstem cavernous malformations. Of
these patients, 7 were men and 15 women,
with a mean age of 43 years (SD 15 years;
range, 8-69 years). Patients were drawn
fromHarborview Medical Center at the Uni-
versity of Washington in Seattle. Patient re-
cords wereretrospectivelyreviewed, includ-
ing outpatient, clinical, and surgicalrecords and radiologic
imaging.
Diagnostic workup for all patients in-
cluded magnetic resonance (MR) studies,
usually with computed tomography scans
at the time of initial presentation as well as
Table 1. Deficits at Time ofPresentation
Deficit %
CN deficit 77
Ataxia 59
Headache 55
Diplopia 41
Weakness 27
Sensory changes 27
Vertigo or dizziness 23
Dysphagia 14
CN, cranial nerve.
OBJECTIVE: The purpose of this study is to provide an
institutional retrospec-tive review of surgically treated brainstem
cavernous malformations.
METHODS: Between 2005 and 2010, 22 consecutive patients with
brainstemcavernous malformations (15 female and 7 male) with a mean
age of 43 yearsunderwent surgical treatment. Mean volume of the
resected cavernous malfor-mations was 0.65 cm3. A minimally
invasive resection technique was used forthese cases, in
conjunction with skull base approaches.
RESULTS: The mean follow-up period was 26.6 months (range, 4-68
months). Ofthe 22 patients, 9% did not have clear evidence of
hemorrhage at the time of
presentation. Of the remainder, 22% had two or more instances of
hemorrhagedocumented by magnetic resonance imaging. After resection
and during follow-up,54% of patients had an improvement in their
modified Rankin scale, whereas 14%were worse compared with their
preoperative presentation; 32% were unchangedand 9% of patients
were found to have residual cavernoma post-surgery.
CONCLUSION: Our longitudinal experience has guided us to
emphasizeminimally invasive approaches during resection of the
brainstem cavernousmalformations, occasionally at the expense of
achieving a complete resection, toimprove patient outcomes.
Key words Brainstem
Cavernoma
Cavernous malformation
Skull base
Abbreviations and AcronymsCMB: Cavernous malformation of the
brainstemGd: GadoliniummRS: Modified Rankin scaleMR: Magnetic
resonance
Department of Neurosurgery, University of
Washington School of Medicine, Seattle,Washington, USA
To whom correspondence should be addressed:
Laligam N. Sekhar, M.D.
[E-mail: [email protected]]
Citation: World Neurosurg. (2013) 79, 5/6:691-703.
http://dx.doi.org/10.1016/j.wneu.2012.04.030
Supplementary digital content available online.
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter 2013 Published by
Elsevier Inc.
PEER-REVIEW REPORTS
WORLD NEUROSURGERY 79 [5/6]: 691-703, MAY/JUNE 2013
www.WORLDNEUROSURGERY.org 691
mailto:[email protected]:[email protected]://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://www.worldneurosurgery.org/http://www.sciencedirect.com/http://www.sciencedirect.com/http://www.worldneurosurgery.org/http://dx.doi.org/10.1016/j.wneu.2012.04.030mailto:[email protected]
-
7/28/2019 Laligham Cav
2/13
Table 2. Surgical Approaches to Brain Stem Cavernous
Malformations
Sex Age Location Approach
Volume,
cm3 Depth Entry Corridor
Intraoperative
Neurophysiology
Preoperative
Symptoms
Postope
Sympto
F 23 Mesencephalothalamic Orbitozygomatic 1.2 At pial
surface
Lateral midbrain SEPs, MEPs, BAEPs
unchanged
Left hemiparesis, left
hyperreflexia.
Left hemipare
improvement
F 50 Mesencephalic Lateralsupracerebellar
0.05 Justbeneath
pial
surface
Dorsal lateralmidbrain
SEPs, MEPs, BAEPsunchanged
Headache, ataxia,diplopia.
Headaches pDiplopia on e
lateral gaze w
functional im
M 58 Mesencephalic Lateral
supracerebellar
1 .1 At pial
surface
Lateral midbrain SEPs, MEPs, BAEPs
unchanged
Multiple hemorrhages in
past with rebleed and
worsening of diplopia,
gait ataxia, and right
hemibody numbness.
Diplopia reso
Right hemibo
numbness sli
worse than p
now stable. N
impairment in
M 8 Mesencephalic Occipital
transtentorial
0.08 At pial
surface
Tectal plate; inferior
to superior colliculus
SEPs, MEPs, BAEPs
unchanged
Vertigo, diplopia,
headaches, nausea,
emesis, syncopal
events.
Diplopia reso
minor headac
F 60 Mesencephalic Transpetrosal 1.3 Justbeneath
pial
surface
Lateral midbrain Left tibial and left mediannerve SSEP
responses
showed a marked decline.
No change in MEPs or
BAEPs.
Somnolence, gait ataxia,left arm weakness and
left hemibody numbness.
Postoperativehydrocephalu
requiring shu
placement. A
pneumonia. P
left hemipare
to ambulate w
assistance. R
nursing home
M 3 7 Mesence phalic Orb itozygomatic 0 .2 Be neath
the pial
surface
Medial crus cerebri SEPs, MEPs, BAEPs
unchanged
Mild left limb numbness.
Partial right CN III and
CN VI palsy.
Post-operativ
infection. Rig
and diplopia
on follow-up.
F 6 0 Mesen ce phalic Orbitozygomatic 0.85 5 mm Ante rolatera
l
midbrain
SEPs, MEPs, BAEPs
unchanged
Diplopia, gait ataxia,
headache, right
hemiparesis.
Right hemipa
improved, dip
resolved.
M 57 Mesen ce phalic Orbitozygomatic 0.48 At pial
surface
Anterolateral
midbrain
Right MEPs transiently
decreased. SEPs and
BAEPs unchanged.
Headache, dizziness,
impaired tandem gait.
Post-operativ
malocclusion
managed
conservativel
F 38 Mesencephalic Orbitozygomatic 1.3 At pial
surface
Anterolateral
midbrain
SEPs, MEPs, BAEPs
unchanged
Severe headache,
tremors, dysphagia.
Mild right CN
palsy. Tremo
dysphagia re
R
692
www.SCIENCE
DIRECT.com
WORLD
N
EUROSURGERY,http://dx.doi.org/10
.1016/j.wneu.2012.04.030
R
http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030
-
7/28/2019 Laligham Cav
3/13
F 40 Pontome se ncephal ic Suboccipital 0. 44 At pial
surface
Posterolateral
midbrain
Right SEPs declined to
40% of baseline. MEPs
and BAEPs unchanged.
Left hemibody numbness,
diplopia, headaches.
Hydrocephalu
requiring shu
venous throm
aspiration pn
Feeding tube
placement. P
diplopia. Nur
home for car
F 2 4 Pon tome sencepha lic Subte mporal 0 .84 Justbeneath
pial
surface
Superior andanterior to
trigeminal root entry
zone
SEPs, MEPs, BAEPsunchanged
Severe headaches, leftdysmetria, gait ataxia.
Left CN V numbness.
Post-operativinfection. Imp
baseline.
M 39 Pontomesencephalic Combined
transtemporal,
transpetrosal
2 .0 At pial
surface
Posterior to
trigeminal root entry
zone
Poor to absent cortical
SEPs on left consistent
with pre-operative left
hemibody numbness.
MEPs unchanged from
baselines.
Two previous
hemorrhages with left
facial and hemibody
numbness, now
progressively worsening.
Left numbnes
unchanged. N
weakness an
left dysmetria
F 45 Pontine Combined
transtemporal,
transpetrosal
0.56 Just
beneath
pial
surface
Pontomesencephalic
junction
SEPs, MEPs, BAEPs
unchanged
Dysarthria, diplopia, left
hemipareis, gait ataxia,
severe headaches.
Left hemibod
neuropathic p
Headaches re
F 69 Pontine Transmaxillary-transclival
0.38 Justbeneath
pial
surface
Mid-ventral pons SEPs, MEPs, BAEPsunchanged
Headaches, lefthemibody numbness and
hemiparesis. Gait ataxia,
dysphagia, vertigo.
Resolution ofoperative sym
M 35 Pontine 1) Retrosigmoid
2) Presigmoid,
Transsigmoid
0.07 6 mm 1) Lateral pons,
anterior to CN VII/
VIII root entry zone
2) More posterior
and inferior
approach to same
region
1) SEPs, MEPs, BAEPs
unchanged 2) Transient
changes in the left BAEP
and right thenar MEP
with recovery at closing.
Lightheadedness,
dizziness, diplopia,
headaches. Left CN VI
palsy.
Cerebrospina
leak requiring
drain. Left he
loss. Persiste
CN VI palsy.
F 42 Pontine Suboccipital 0.13 At pial
surface
Floor of the fourth
ventricle, superior to
facial colliculus
SEPs, MEPs, BAEPs
unchanged
Left torsional nystagmus,
gait ataxia.
Right CN VI a
palsy, requiri
gold weight.
hyperacusis alimb coordina
problems.
F 43 Pontine Transpetrosal 0.32 Just
beneath
pial
surface
Posterior and inferior
to trigeminal root
entry zone
SEPs, MEPs, BAEPs
unchanged
Numbness of the right
face, dizziness, ataxia,
diplopia and weakness.
Right CN V1
decreased se
and diminish
corneal reflex
Diplopia reso
C
WORLD
NEUROSURG
ERY79
[5/6]:691-703,MAY/JUNE
2013
www.WORLDNEU
ROSURGERY.org
693
C
-
7/28/2019 Laligham Cav
4/13
http://dx.doi.org/10.1016/j.wneu.2012.04.030
-
7/28/2019 Laligham Cav
5/13
cerebral angiography. Episodes of hemor-
rhage related to the cavernomas were con-
firmed by an acute change in neurologic ex-
amination in correspondence with MR
findings suggestive of acute bleeding (T2
hypointensity) (39). Suspected episodes of
bleeding in the past not confirmed by MR
imaging were excluded from the calcula-
tions. The volume of the lesions was calcu-
lated by estimating the volume of an ellip-soid (4/3 1/2
sagittal diameter 1/2
axial diameter 1/2 coronal diameter) as
determined by MR measurements.
Follow-up information included outpa-
tient neurologic examinations and calls to
patients and their relatives. A mean fol-
low-uptimeof 26.6months (SD18 months;
range, 4-68 months) was obtained. Patient
outcomes pre- and postsurgery and during
long-term follow-up were assessed by use
of the modified Rankinscale (mRS) (8,34).
RESULTS
Preoperative History
Allpatientswho were included in this study
were symptomatic from their brainstemcavernomas; only three
patients did not
have an overt hemorrhage beforecomingto
medical attention (Table 1). The three pa-tients who did not
have a clearly docu-
mented recent hemorrhage with acute
neurologic deterioration were offered
surgery because their lesions appeared to
come to the surface of the brain stem on
MR imaging. The vast majority presented
with cranial nerve deficits (77%), many of
which associated with diplopia (41%). A
total of 55% of patients presented with
headache.Thesenumbers aregenerallyin
keeping with other previously published
data (2, 39, 42).
On the basis of MR findings in conjunc-tionwith patient reports
of neurologic dete-
rioration, 64% of the patients had a single
bleed at the time of presentation, and 22%
hadsustained twoor more hemorrhages by
the time they were taken to the operating
room. In this series, 31% of cavernomas
were located in the midbrain, 35% in the
pons,and19%inthemedulla(Table2).Theremainder of lesions spanned
multiple
brainstem regions. The mean volume of
these lesions was0.65 cm3, with a standard
deviationof 0.69 cm3. Multiple cavernomas
were found in six patients (27%), with one
of these individuals undergoing separate
surgical procedures for their CMBs.
Surgical Approaches
A broad range of approaches was used dur-
ing surgical resection of brainstem caver-
nomas, as shown in Table 2. The primaryaim of surgery was to
provide safe resec-
tion of the lesion through as small an
access point through the brainstem as
possible, that is, the minimal access
technique. Approaches were chosen to
maximize exposure with as little brain re-traction as possible
as well as facilitate
ready entry through brainstem safeentry
zones (6, 7, 21, 24, 35). Developmental
venous anomalies associated with these
cavernomas, identified either on preoper-
ative workup or intraoperatively, were left
extant during surgery(2).
All lesions wereresected under frameless
stereotaxy, with coregistration to the oper-
ating microscope used whenever possible.
Intraoperative bilateral somatosensory and
motor-evoked potentials were combined
with cranial nerve monitoring, including
brainstem auditory evoked responses, aswell as direct
stimulation (44).
Minimal Access Technique
The entry to the brainstem cavernoma is
made through a pial opening if the lesion
points to the surface through a defined
safe entry zone (24, 35). The approach is
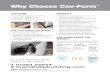
Figure 1. Case 1: CMB situated in the right midbrain peduncle.
Axial T2-weighted (A), sagittal (B), and
coronal (C) T1-weighted, post-gadolinium (Gd) enhancement views
demonstrate the location of thelesion. Red overlay depicts the
operative corridor available for resection of the lesion via a
right
orbitozygomatic osteotomy approach. Three-month postoperative
axial T2-weighted image
demonstrating gross total resection (D).
PEER-REVIEW REPORTS
JEFFREY C. MAI ET AL. RESECTION OF CAVERNOUS MALFORMATIONS OF
THE BRAINSTEM
WORLD NEUROSURGERY 79 [5/6]: 691-703, MAY/JUNE 2013
www.WORLDNEUROSURGERY.org 695
-
7/28/2019 Laligham Cav
6/13
best determined with careful consideration
of the anatomy and any available additional
imaginginformation,such as diffusionten-
sor imaging. Intraoperative neuronaviga-
tion is indispensable in delineating the
entry approach, in conjunction with neuro-
anatomical landmarks. The incision into
the brainstem and the tract are kept as nar-
row as possible until the cavernoma is
reached. Once inside the cavernoma, any
liquefied hematoma is drained. Solid por-
tions of the cavernoma are removed piece-
meal, starting centrally, and gradually pro-
gressing to the margins, until the lesion is
completely removed (Video 1). Most caver-nomas are removed in
three to five pieces,
depending on their size and consistency.
Care is taken toremove allof thecavernoma
elements while preserving any major veins
or en passage arteries. Vigorous removal of
the gliotic, hemosiderin-stained margin of
the cavernoma is not attempted, especially
with large lesions, because the risk of sei-
zures triggered by these residual tissues is
nonexistent.
Operative ResultsA total of 27 operative procedures were
per-
formed for the 22 patients in the series for
their brainstem cavernomas; 31% of the
cavernomas weremesencephalic, 35%were
pontine, and 19% were located in the me-
dulla (Table 2). Four lesions were largeenough to span adjoining
domains, includ-
ing one mesencephalothalamic and three
Figure 2. Case 2: left tectal plate cavernous malformation.
Sagittal T1-weighted post-Gd (A) and axial T2-weighted preoperative
(B) and
postoperative scans at 2 months (C). Red overlay depicts the
operative
approach via a left occipital transtentorial approach.
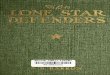
Figure 3. Case 3: left lateral supracerebellar infratentorial
approach (red transparent overlay) to dorsalmidbrain cavernoma.
Sagittal (A), coronal (B), and axial (C) T2-weighted images and
axial T2-
weighted image 14 months postoperatively (D) demonstrating no
obvious residual cavernoma.
PEER-REVIEW REPORTS
JEFFREY C. MAI ET AL. RESECTION OF CAVERNOUS MALFORMATIONS OF
THE BRAINSTEM
696 www.SCIENCEDIRECT.com WORLD NEUROSURGERY,
http://dx.doi.org/10.1016/j.wneu.2012.04.030
http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030
-
7/28/2019 Laligham Cav
7/13
pontomesencephalic cavernomas. A 91%
gross total resection rate was achieved, as
assessed by serial MR imaging. In 9% of
patients, residual cavernoma was identified
on post-operative imaging. No postopera-
tive mortality was observed in
this series, andno further sur-
geries were required in these
patients.
Midbrain. Case 1. This 23-
year-old woman developed
left hemiparesis with distal weakness
greater than proximal in the arms in legs
(graded 4/5) and hyperreflexia on the ipsi-
lateral side. As her cavernoma was situated
in the right peduncle, a right frontotempo-
ral orbitozygomatic approach was under-
taken (Figure 1). She developed transientleft facial weakness
and worsening of her
left hemiparesis postoperatively. At 20
months after the procedure, she has pro-
gressed from an mRS 4 to an
mRS2 with persistence of her
mild left-sided weakness.
Case 2. An 8-year-old boypre-sented with vertigo, head-
aches, nausea, and vomiting
and was found to have at least
seven supra- and infratentorial cavernous
malformations, including the largest in the
tectum, which had evidence of recent hem-
orrhage on MR imaging, andanotherin the
medulla. The tectal plate cavernoma was
approached via a left occipital, transtento-
rial approach using frameless stereotaxy
(Figure2). Asthe lesioncameto thesurface,
gross totalresection was possible,with new
postoperative diplopia noted at 2 months
follow-up, and at 1 year, he was asymptom-
atic, mRS 0.
Case 3. A 58-year-old man with known his-
toryof CMBand multiple hemorrhages pre-
sented with rebleed accompanied by diplo-
pia, right hemibody numbness, and gait
ataxia, mRS 2. The cavernoma was located
on the left dorsal mesencephalon (Fig-
ure3). Weapproachedthe lesionby a lateral
supracerebellar infratentorial approach. At
25 months follow-up, patient has resolu-
tion of diplopia but slight worsening of
right body numbness, mRS 1.
Pons. Case 4. A 43-year-old woman pre-
sented with right V1-V3 facial numbness,diplopia, ataxia, and
weakness with two
symptomatic hemorrhages from a right
middle cerebellar peduncle cavernous mal-
formation(Figure4). Given thelocation,we
opted for a right transpetrosal approachfor
the lesion. In thisinstance, diffusion tensor
imaging was used during preoperative
planning to map the direction of displaced
tracts in a rostral-caudal axis.In comparing
the side of the brainstem with the caver-
noma to the contralateral unaffected side,
we found these fibers to be medially dis-
placed, confirming that entry from a lateral
approach would be safest. At 27 months
postoperatively, her diplopia had resolved,
but she has developed a right diminished
corneal reflex and slightly worsened V1-V3
numbness. Nevertheless, she is able to
drive a vehicle, and hermRS improved from
a 2 to a 1.
Case 5. A 69-year-old woman presented
with acute onset of headache,left hemibody
numbness and weakness (4/5), left dysme-
tria, ataxia, dysphagia, and vertigo with a
central pontine hemorrhage secondary to a
cavernoma (Figure 5). Because the lesion
was located in the midline and did notclearly reach the surface,
we opted for a
transmaxillarytransclival approach, as il-
lustrated in Figure 5. In this case, a transfa-
cial LeFort I maxillotomy was used, with a
clivectomy performed with neuronaviga-
tion used to guide the trajectory directly to
the lesion. This approach, although techni-
cally demanding, affords an excellent work-
Figure 4. Case 4: CMB located in the right cerebellar peduncle.
T2-weighted sagittal (A) and axial (B)images. Three-dimensional
diffusion tensor imaging demonstrates medial displacement of
rostral-
caudal fibers with cavernoma coming to surface of the lateral
pons (C). Red overlay illustrates a right
transpetrosal approach. (D) Axial T2-weighted image at 10-month
postoperative follow-up.
Video available at
WORLDNEUROSURGERY.org
PEER-REVIEW REPORTS
JEFFREY C. MAI ET AL. RESECTION OF CAVERNOUS MALFORMATIONS OF
THE BRAINSTEM
WORLD NEUROSURGERY 79 [5/6]: 691-703, MAY/JUNE 2013
www.WORLDNEUROSURGERY.org 697
-
7/28/2019 Laligham Cav
8/13
ing view of the ventral pontine surface, in-
cluding the basilar artery and its associated
paramedian perforators, thereby facilitat-
ing their preservation. In addition, it repre-
sents the most direct pathway to the lesion,
without the need to traverse normal brains-
tem tissue to reach the lesion. Here, the
basilar artery was moved gently aside, ex-
posing a small area of discoloration in the
midline representing the cavernomas
emergence at the surface of the pons. Afterresection, the defect
in the clival dura was
repaired with placement of two pieces of
abdominal fascia beneath the inner surface
of dura,followed by application of DuraSeal
(Confluent Surgical Inc., Waltham, Massa-
chusetts, USA). An additional two layers of
fascia were applied to the outside, secured
again with a layer of DuraSeal and Gelfoam
(Pfizer, NewYork,New York, USA), and the
sphenoid rostrum was covered with a mu-
cosal flap. A right frontal externalventriculo-
stomydrainwas placedat thetime of surgery
to minimize risk of CSFleak and wasweaned
by postoperative day 9. Her mRS improved
from 2 to 1 at 44 months follow-up.Case 6. A 57-year-old man who
developed
sudden onset of headache, dizziness, and
gait disturbance was found to have a left
lateral pontine hemorrhage as the result ofunderlying cavernoma
(Figure 6). A leftsubtemporal approach with zygomatic os-
teotomy was used to gain access to the lat-
eral pons, where the cavernous malforma-
tion wasobserved to come to thesurface.At
22 months follow up, the patient had im-
proved from an mRS score of 2 to an mRS
of 1.
Case 7. A 39-year-old man with two previ-
ous hemorrhages of a right dorsal lateral
pontine cavernoma re-presented with pro-
gressive left facial droop, left hemibody
numbness, and truncal ataxia. As shown in
Figure 7, a right transpetrosal and presig-moid approach was
used for extirpation of
thelesion. At 7 months postoperatively, thepatient had improved
from an mRS of 3 to
an mRSof 1 andreported improvingnumb-
ness onthe left side and mild left dysmetria.
Medulla. Case 8. A 37-year-old woman pre-
sented with baseline disequilibrium and
previous subtotal resection of dorsal med-
ullary brainstem cavernoma by another
neurosurgeon. She represented with sud-
den deterioration, including numbness in
her right arm, intermittent dysphagia, and
difficulty breathing. A far lateral retrosig-
moid approach was used, and gross total
resection was achieved (Figure 8). At 42months follow-up, she
has now made a
complete recovery (mRS 0).
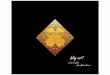
Long-Term Outcomes
During the course of follow-up, 54% of pa-
tients were noted to improve compared
with their preoperative status, whereas 32%
remained generally unchanged from a neu-
rologic standpoint. During this time, 14%
of patients had declined compared with
their preoperative status. The distribution
of preoperative mRS and long-term mRS is
shown in Figure 9. Of the 9% of patientswith residual brainstem
cavernomas, no in-
stances of rehemorrhage were recorded. At
present, both of these patients have de-
clined reoperation.
DISCUSSION
Indications for Removal
The vast majority of brainstem cavernous
malformations come to attention after a
hemorrhage. In general, we are willing to
delay surgical management of these lesions
after a single bleeding ictus unless the pa-tients cardiac or
neurologic instability ne-
cessitatesemergent evacuation or thelesion
clearly abuts the pial or ependymal surface
on T1-weighted MRimaging(18, 39, 42). For
deeper seated lesions, a second bleed or pro-
gressiveneurologic deficit necessitatessurgi-
cal extirpation of the brainstem cavernoma
because it suggests the propensity of the
Figure 5. Case 5: Midline, ventral pontine cavernoma approached
via a transmaxillary-transclivalapproach (red transparent overlay).
T1-weighted post-Gd sagittal (A), coronal (B), and axial (C)
images. (D) T2-weighted axial scan at 3-year follow-up.
PEER-REVIEW REPORTS
JEFFREY C. MAI ET AL. RESECTION OF CAVERNOUS MALFORMATIONS OF
THE BRAINSTEM
698 www.SCIENCEDIRECT.com WORLD NEUROSURGERY,
http://dx.doi.org/10.1016/j.wneu.2012.04.030
http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030
-
7/28/2019 Laligham Cav
9/13
lesion to rebleed in the future. In these in-
stances, carefully weighingthe risk of mor-
bidity from surgery compared with that of
future re-hemorrhage, on the basis of the
natural history of these lesions, tips thebal-
ance in favor of surgical intervention (18).
This is especially true if deep-seated lesions
can be approached through safe entry
corridors.
The use of radiosurgery for cavernous
malformations has been reported, withmixed results (27, 30). As
such, the use of
radiosurgery as a primary treatment modal-
ity for cavernous malformations, including
those of the brainstem, remains controver-
sial. At present, we advocate surgical resec-
tion as the primary means for treatment for
high-risk cavernomas of the brainstem.
With regard to timing of surgery after a
hemorrhage, although some surgeons ad-
vocate delaying surgery until the subacute
phase, when the blood products will un-
dergo liquefaction (13, 18, 39); waiting
much beyond the first several weeks risks
development of gliosis, which may hinder
complete resection.
Approaches to the Brainstem
Unlike with supratentorial cavernous mal-formations, those
associated with CMBs
present a special challenge to the surgeon
due to the presence of surrounding brains-
temnuclei andtracts (7, 17, 24, 35). As with
others, we advocate carefully tailoring the
surgical approach to each individuals le-
sion. It is incumbent upon the surgeon to
recognize the normal anatomy of the region
surrounding the cavernomas, as well as
take into careful consideration the distor-
tionin surroundinganatomy thatcan arise as
a result of the lesion as well as associated
hemorrhage. Unless the cavernoma comes
clearly to the pial surface,the direction of ap-
proach may not always be optimally defined
as the shortest path from the surface to thelesion.Given the
eloquence of the brainstem,
even a thin parenchymal layer overlying the
cavernoma canharbor criticaltracts.Compli-
cating this situation is the paucity of widely
used and reliable intraoperative methods to
identify these displaced and distorted struc-
tures. Broadly, we have subcategorized ap-
proaches to the brainstem with respect to the
midbrain, pons, and medulla.
Midbrain. The midbrain is subdivided into
three general approaches: anteromedial,
lateral, and posterior. In the anteromedial
approach for interpeduncular lesions, anextended transsylvian
corridor is used,with
the assistance of an orbitozygomatic crani-
otomy (18). Slightly more laterally, a sub-
temporal approach can be used, or in com-
bination with a transsylvian route (31).
Laterally, a supracerebellar-infratentorial
or petrosal approach can be used to reach
mesencephalic cavernomas. Posteriorly, a
suboccipital or occipital transtentorial ap-
proach can be used to reach lesions cen-
tered near the posterior midbrain, includ-
ing the tectal plate. From a posterior
approach, dependingon the location of the
cavernomas, entry at the lateral mesen-
cephalic sulcus may be used to avoid injur-
ing oculomotor and trochlear nuclei and
the medial longitudinal fasciculus situated
more medially (17, 21, 35). The supracol-
licular and infracollicular lines that delin-
eate therostralandcaudal extentof thelam-
ina quadrigemina represent other potential
corridors of entry along the midline (9, 17).
Otherwise, midline approaches through
the tectal plate should be avoided whenever
possible given their postoperative morbid-
ity.Throughexperience,we andothers have
learned that avoidance of injury to the cen-
tral tegmentum and adjacent medial longi-
tudinal fasciculus is vital, as the resultant
postoperative complications of nystagmus
and internuclear ophthalmoplegia, respec-
tively, are particularly debilitating during
recovery(17).
Pons. The pons is the largest region of the
brainstem andthe most commonlocation for
Figure 6. Case 6: Left, lateral pontine cavernoma with a left
subtemporal approach with zygomatic
osteotomy depicted with the red overlay. Fluid-attenuated
inversion recovery sagittal (A), T1-weighted post-Gd coronal (B),
and T2-weighted axial preoperative (C) and 22 months
postoperative
(D) images.
PEER-REVIEW REPORTS
JEFFREY C. MAI ET AL. RESECTION OF CAVERNOUS MALFORMATIONS OF
THE BRAINSTEM
WORLD NEUROSURGERY 79 [5/6]: 691-703, MAY/JUNE 2013
www.WORLDNEUROSURGERY.org 699
http://-/?-http://-/?-http://-/?-
-
7/28/2019 Laligham Cav
10/13
brainstemcavernomas (13,18, 33, 42). Given
its size, a variety of surgical approaches are
available to the surgeon, depending on the
precise location of the cavernous malforma-
tion(Table2). Wehavedefinedapproachesto
the pons intofour categories: dorsal, central,
anterolateral, and lateral.
From a dorsal approach, a midline sub-
occipital approach can be used. In such
cases,it is paramountto minimize dividing
the vermis given associated complications,
including truncal ataxia (44). Alternately, a
subtonsillar-transcerebellomedullary (te-
lovelar) approach can be used (13, 44),
which involves dividing the cerebellomed-
ullary fissure. This approach is useful in ac-
cessing pontomedullary and medullary le-
sions. Unfortunately, unless the cavernoma
clearly emerges at thesurface of thefloor of
the fourth ventricle, injury to the medial
longitudinal fasciculus, facial, and abdu-cens nerve are common
when operating
along thisregion (3,44). As withothers (13,
17, 18, 33), we view the floor of the fourth
ventricle with great caution when ap-
proaching CMBs, despite the published
morphometric descriptions of safe entry
zones in the infra- and supra-abducental or
facial regions (6, 7, 24). These lesions can
be approached if the locations of the facial,
vagal, and hypoglossal nuclei are carefully
established intraoperatively by direct stim-
ulation. Nevertheless, it may be difficult to
avoidthe intrinsicportionof thefacial nerve
tract or the abducens nucleus when resect-ing cavernomas in
immediate vicinity. Post-
surgical brainstem tract and nucleus-re-
lated complications have been reduced as
we have shifted away from posterior ap-
proaches to the pons over time.
We prefer more lateral or anterolateral
approaches to the brainstem, particularly
when dealing with deep-seated lesions of
the pons. The anterior and anterolateral
brainstem tracts are generally more resil-
ient to surgical manipulation than the dor-
sal pontineand medullarysurfaces. A trans-
petrosal (19, 22, 31, 45) or retrosigmoid
approach will enable accessto themore an-teriorsurface of the
pons (16, 31). A presig-
moid approach will yield a more lateral, al-
beit more direct, view of the pons (20).
From any of these approaches, the peritri-
geminal area, a safe entry zone, can be
accessed and safely traversed horizontally,
followingalong theplane of thefibers. This
triangular region is bound medially by the
Figure 7. Case 7: Right transpetrosal and presigmoid approach
(red overlay) to a right dorsal lateralpontine cavernoma.
T1-weighted post-Gd axial (A), T2-weighted axial (B), T1-weighted
post-Gd
sagittal (C), and postoperative 3-month T2-weighted axial image
(D). Intraoperative image
demonstrating bimanual removal of cavernoma through a small
portal in the brainstem (E) and image
after gross total resection (F).
PEER-REVIEW REPORTS
JEFFREY C. MAI ET AL. RESECTION OF CAVERNOUS MALFORMATIONS OF
THE BRAINSTEM
700 www.SCIENCEDIRECT.com WORLD NEUROSURGERY,
http://dx.doi.org/10.1016/j.wneu.2012.04.030
http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030
-
7/28/2019 Laligham Cav
11/13
pyramidal tract, inferiorly by the pon-
tomedullary sulcus out to the flocculus,and
laterallyjustmedial tothe root entry zone of
cranial nerve V (35).
Cavernomas situated directly on the ven-
tral midline surface of the pons require a
central approach. For these difficult, but
fortunately rare, lesions, we advocate a
transmaxillary-transclival approach, which
we used during the resection of one of our
pontine cavernomas in ourseries (Table 2).
Medulla. The medulla can be approached
from the following routes: dorsal, anterior,
and anterolateral corridors. As with the
pons, a midline suboccipital craniotomy
with a telovelar approach can be used to
reach the dorsal medullary surface (17, 31).
In theupper dorsalmedulla,alongthe infe-
rior floor of the fourth ventricle, risk of in-
jury to the nucleus of XII medially and the
nucleus X laterally with resultant ipsilateraltongue weakness
and cardiac/respiratory
instability, respectively, makes entry from
thisdirection generallycontraindicated (13,
17, 18, 33). Furthermore, the medial longi-
tudinal fasciculus underlies these struc-
tures medially. For the lower dorsal me-
dulla, safe entry zones are defined by
Bricolo as the posterior median fissure and
the posterior intermediate and posterior
lateral sulci (9, 17).
Generally, a far lateral retrosigmoid ap-
proach will suffice for reaching pontomed-
ullary lesions (13). An extreme far lateral
approach with the resection of the jugular
tubercle (thetranstubercular approach) will
enable access to the anterolateral lesionsoriginating in the
medulla down to the up-
per cervical spinal cord(18, 31). Fromeither
approach, safe medullary access is realized
by way of entry through the retro-olivary
sulcus, which does not result in clinically
evidence deficits (35). Finally, strictly ante-
rior cavernomas of the ventral medulla can
be reached via a transoral route (36, 44).
This was not used in our series due to the
absence of any cases requiringit. Because of
the concern for CSF leak and associated in-
fection, an alternative is the subtemporal
infratemporal approach for these lesions
(41).In each case, the guiding principle is to
avoid breaching major brainstem tracts or
nuclei. If there is no option, then traversing
the most accessible route to the brainstem
cavernoma must then be chosen on a case-
by-case basis.
Evolution of a Minimally Invasive
Resection Technique
Once the decision has been made to pro-
ceed with resection, careful preoperative
planning is essential. When possible, we
have useddiffusiontensor imaging to studythe distortion of the
underlying white mat-
ter tracts surrounding the lesion (11). It is
performed when lesions do not appear to
cometo the pial surface onMR imaging,so
that the corridor for entry through the
brainstem maynot be as apparent.The util-
ity of such imaging can be limited by sus-
ceptibility artifact when one is resecting a
relatively fresh hemorrhage, which pre-
vents adequate tractography. Nevertheless,
in such cases, comparing the contralateral
side tractsas a pointof reference and com-
pensating for anticipated displacementof
the tracts on the ipsilateral side can behelpful.
Intraoperative cranial nerve monitoring
is generally more important for dorsal ap-
proaches. For anterior and lateral ap-
proaches to the brainstem, motor-evoked
potentials are obligatory. Intraoperatively,
real-time guidance with frameless stereo-
taxy registered to the operating microscope
Figure 8. Case 8: Suboccipital approach (red transparent
overlay) to cavernous malformation of thedorsal medulla previously
with subtotal resection. T2-weighted sagittal (A), coronal (B), and
axial
preoperative (C), and 3 year postoperative (D) images shown.
Figure 9. Bar graph showing the distributionof the preoperative
mRS scores for the 22
patients compared with the distribution at
last follow-up. Mean follow-up time was 26.6
months with a range of 2-68 months, SD of
17.7 months.
PEER-REVIEW REPORTS
JEFFREY C. MAI ET AL. RESECTION OF CAVERNOUS MALFORMATIONS OF
THE BRAINSTEM
WORLD NEUROSURGERY 79 [5/6]: 691-703, MAY/JUNE 2013
www.WORLDNEUROSURGERY.org 701
http://-/?-http://-/?-http://-/?-
-
7/28/2019 Laligham Cav
12/13
field of view is ofparticular importance dur-
ing resection of small cavernomas.
In the senior authors experience
(L.N.S.), a general approach to brainstem
cavernous malformations is to create as
small a portal for access to the lesion asfeasible, a minimal
access technique.
Through this window, the cavernoma is re-
sected as much as possible, given the con-
straints of the surrounding anatomic struc-
tures. In these cases, the cavernoma
generally is internally debulked to decom-
press the lesion, and the wall is then gently
taken down from the surrounding brains-
tem and disconnected with the use of a bi-
manual technique (Figure 10). Any associ-ated developmental
venous anomalies,
which are commonly associated with these
lesions (1, 3, 32), or hemosiderin-stained
tissue is preserved.This method has been able to yield gen-
erally favorable results in the majority of
brainstem cavernomas, with the drawback
that given the small surgical window, a
gross total resection may be impossible to
achieve. Reviewing the retrospective data
shown above, there have been two recur-
rences after surgery: both were managed
conservativelywith monitoring by serial im-
aging. These recurrences are tempered
against the reduction of expected post-op-
erative complications. We have generally
opted for repeated resections, if indicated,
for residual brainstem cavernomas, as they
do present a risk of rehemorrhage.
Future Developments
As technology advances, we anticipate the
development of specialized microsurgical
instrumentation, including flexible endo-
scopes and other articulated devices that
will facilitate working through highly con-
strained operative corridors, thereby mini-
mizing damage to the surrounding brains-
temtracts andnuclei.The useof thecarbon
dioxide laser hasalready been employed for
selected cavernomas in the brainstem (G.
Steinberg, personalcommunication, 2010),
and we are presently exploring the utility ofthe flexible CO
2laser (OmniGuide, Cam-
bridge, Massachusetts, USA) at our institu-
tion.
CONCLUSION
Our approach to cavernous malformations
of the brainstem represents a progressive
and iterative refinement of surgical tech-
niques during the past two decades. We
have sought to incorporate new technolo-
gies, such as image guidance and diffusion
tensor imaging, wherever practical. Fromexperience, we have
opted to eschew mid-
line approaches to the dorsal midbrain and
to the floor of the fourth ventricle, instead
selecting operative corridors that are di-
rected more laterally and anteriorly to the
brainstem. Finally, we recommend a mini-
mal access technique, wherever possible,
which reduces the likelihood of postopera-
tive morbiditydue to brainstemnuclear and
tractinjuryat theexpenseof achievinggross
total resection.
REFERENCES
1. Abla AA, Lekovic GP, Turner JD,de OliveiraJG, Porter
R,SpetzlerRF. Advancesinthe treatmentand outcomeof brainstem
cavernous malformation surgery: a sin-
gle-center caseseries of300 surgically
treatedpatients.Neurosurgery682011;403-414discussion 414-405.
2. AblaAA, Turner JD,Mitha AP,Spetzler RF:Surgical
approachesto brainstemcavernous malformations.Neurosurg Focus
29:E82010.
Figure 10. General technique for resection of brain stem
cavernomas. A small window to thecavernous malformation is created,
with the direction of access defined by the safest anatomical
corridor possible. In this example, for a deep seated lesion in
the pons, a lateral ventral approach is
chosen (A, inset). From this minimally invasive portal, the
cavernoma is initially centrally debulked,
and gradually, the wall is gently liberated from the surrounding
brainstem parenchyma and removed
piecemeal to minimize injury to the surrounding tracts and
nuclei (A-E).
PEER-REVIEW REPORTS
JEFFREY C. MAI ET AL. RESECTION OF CAVERNOUS MALFORMATIONS OF
THE BRAINSTEM
702 www.SCIENCEDIRECT.com WORLD NEUROSURGERY,
http://dx.doi.org/10.1016/j.wneu.2012.04.030
http://dx.doi.org/10.1016/j.wneu.2012.04.030http://dx.doi.org/10.1016/j.wneu.2012.04.030
-
7/28/2019 Laligham Cav
13/13
3. Asaad WF, WalcottBP, NahedBV,Ogilvy CS:Oper-ative management
of brainstem cavernous malfor-
mations. Neurosurg Focus 29:E102010.
4. Batra S, Lin D, Recinos PF, Zhang J, Rigamonti D:
Cavernous malformations: natural history, diagno-sisand
treatment. NatRev Neurol 5:659-670,2009.
5. Beltramello A, Lombardo MC, Masotto B, Bricolog
A: Imaging of brain stem tumors. Op Tech Neuro-surg 3:87-105,
2000.
6. Bogucki J, Czernicki Z: Surgical treatment of brain-
stem tumours with special emphasis on the opera-
tiveapproach throughthe fourth ventriclefloor.Fo-lia Neuropathol
41:227-230, 2003.
7. BoguckiJ, Czernicki Z, GieleckiJ: Cytoarchitectonicbasis for
safe entry into the brainstem. Acta Neuro-
chir (Wien) 142:383-387, 2000.
8. BonitaR, Beaglehole R: Recoveryof motor function
after stroke. Stroke 19:1497-1500, 1988.
9. Bricolo A: Surgical management of intrinsic brain
stemgliomas.Op TechNeurosurg3:137-154, 2000.
10. Campbell PG, Jabbour P, Yadla S, Awad IA: Emerg-ing clinical
imaging techniques for cerebral cavern-ous malformations: a
systematic review. Neurosurg
Focus 29:E62010.
11. ChenX, WeigelD, Ganslandt O,BuchfelderM, Nim-
sky C. Diffusion tensor imaging and white mattertractography in
patients with brainstem lesions.
Acta Neurochir (Wien) 1492007;1117-1131discus-
sion 1131.
12. Dammann P, Barth M, Zhu Y, Maderwald S, Schla-
mann M, Ladd ME, Sure U: Susceptibility weightedmagnetic
resonance imaging of cerebral cavernous
malformations: prospects, drawbacks, and first ex-perience at
ultra-high field strength (7-Tesla) mag-
netic resonance imaging. Neurosurg Focus 29:
E52010.
13. Ferroli P, Sinisi M, Franzini A, Giombini S, Solero
CL,Broggi G. Brainstem cavernomas: long-termre-sultsof
microsurgicalresection in 52 patients. Neu-
rosurgery 562005;1203-1212discussion 1212-1204.
14. Fritschi JA, Reulen HJ, Spetzler RF, Zabramski JM:
Cavernous malformations of the brain stem. A re-view of 139
cases. Acta Neurochir(Wien) 130:35-46,
1994.
15. Garner TB, Del Curling O, Jr., Kelly DL, Jr., Laster
DW:The naturalhistory ofintracranial venous angi-
omas. J Neurosurg 75:715-722, 1991.
16. Garrett M, Spetzler RF. Surgical treatment of brain-stem
cavernous malformations. Surg Neurol
72suppl 22009;S3-S9discussion S9-10.
17. Giliberto G, Lanzino DJ, Diehn FE, Factor D, Flem-
ming KD, Lanzino G: Brainstem cavernous malfor-
mations: anatomical, clinical, and surgical consid-erations.
Neurosurg Focus 29:E92010.
18. Gross BA, Batjer HH, Awad IA, Bendok BR. Brains-tem
cavernous malformations. Neurosurgery
642009;E805-E818discussion E818.
19. Harsh GR, Sekhar LN: The subtemporal, transcav-
ernous, anterior transpetrosal approach to the up-
per brain stem and clivus. J Neurosurg 77:709-717,1992.
20. Hauck EF, Barnett SL, White JA, Samson D: Thepresigmoid
approach to anterolateral pontine cav-
ernomas. J Neurosurg 2010.
21. IshiharaH, Bjeljac M, Straumann D,Kaku Y,Roth P,Yonekawa Y:
The role of intraoperative monitoringof oculomotor and trochlear
nuclei-safe entry zone
to tegmental lesions.MinimInvasive Neurosurg 49:
168-172, 2006.
22. Kawase T: Technique of anterior transpetrosal ap-
proach. Op Tech Neurosurg 2:10-17, 1999.
23. Kim DS, Park YG, Choi JU, Chung SS, Lee KC. An
analysis of the natural history of cavernous malfor-mations.Surg
Neurol481997;9-17discussion 17-18.
24. Kyoshima K, Kobayashi S, Gibo H, Kuroyanagi T:
A studyof safeentry zonesvia thefloor ofthefourth
ventricle for brain-stem lesions. Report of threecases. J
Neurosurg 78:987-993, 1993.
25. MathiesenT,EdnerG, KihlstromL:
Deepandbrain-stemcavernomas:aconsecutive8-yearseries.JNeu-
rosurg 99:31-37, 2003.
26. McLaughlin MR, Kondziolka D, Flickinger JC,
Lunsford S, Lunsford LD. The prospective naturalhistory of
cerebral venous malformations. Neuro-
surgery 431998;195-200discussion 200-191.
27. Monaco EA,KhanAA, NiranjanA, KanoH, Grandhi
R, Kondziolka D, Flickinger JC, Lunsford LD: Ste-
reotactic radiosurgery for the treatment of symp-tomatic
brainstem cavernous malformations. Neu-
rosurg Focus 29:E112010.
28. Moriarity JL, Wetzel M, Clatterbuck RE, Javedan S,
SheppardJM, Hoenig-RigamontiK, Crone NE,Bre-iterSN, LeeRR,
Rigamonti D.The naturalhistory of
cavernousmalformations:a prospective study of 68patients.
Neurosurgery 441999;1166-1171discus-sion 1172-1163.
29. Otten P, Pizzolato GP, Rilliet B, Berney J: [131 casesof
cavernous angioma (cavernomas) of the CNS,
discovered by retrospective analysis of 24,535 au-topsies].
Neurochirurgie 35(82-83):128-131, 1989.
30. Pollock BE, Garces YI, Stafford SL, Foote RL,Schomberg PJ,
Link MJ: Stereotactic radiosurgery
for cavernous malformations. J Neurosurg 93:987-
991, 2000.
31. Porter RW, Detwiler PW, Spetzler RF: Surgical ap-
proaches to the brain stem. Op Tech Neurosurg3:114-123,
2000.
32. PorterRW, DetwilerPW, SpetzlerRF: Surgicaltech-nique for
resection of cavernous malformations of
the brain stem. Op Tech Neurosurg 3:124-130,2000.
33. Porter RW, Detwiler PW, Spetzler RF, Lawton MT,Baskin JJ,
Derksen PT, Zabramski JM: Cavernous
malformations of the brainstem: experience with100 patients. J
Neurosurg 90:50-58, 1999.
34. Rankin J: Cerebral vascular accidents in patients
over the age of 60. II. Prognosis. Scott Med J 2:200-215,
1957.
35. Recalde RJ,Figueiredo EG,de OliveiraE.
Microsur-gicalanatomyof thesafe entryzoneson theantero-
lateral brainstem related to surgical approaches to
cavernousmalformations. Neurosurgery 622008;9-
15discussion 15-17.
36. Reisch R, Bettag M, Perneczky A. Transoral tran-sclival
removal of anteriorly placed cavernous mal-
formations of the brainstem. Surg Neurol 562001;
106-115discussion 115-106.
37. Robinson JR, Awad IA, Little JR: Natural history of the
cavernousangioma.J Neurosurg 75:709-714, 1991.
38. Robinson JR, Jr., Awad IA, Magdinec M, Paranandi
L. Factors predisposing to clinical disability in pa-tients with
cavernous malformations of the brain.
Neurosurgery 321993;730-735discussion 735-736.
39. SamiiM, EghbalR, CarvalhoGA,Matthies C: Surgi-
calmanagementof brainstemcavernomas.J Neuro-surg 95:825-832,
2001.
40. SarwarM, McCormickWF:Intracerebralvenousan-
gioma. Casereport andreview. ArchNeurol 35:323-325, 1978.
41. Sen CN, Sekhar LN: The subtemporal and
preauricularinfratemporalapproach
tointraduralstructuresventralto
thebrainstem.J Neurosurg 73:345-354,1990.
42. WangCC,Liu A,Zhang JT,SunB, Zhao YL.Surgical
management of brain-stem cavernous malforma-
tions: report of 137cases. SurgNeurol592003;444-454discussion
454.
43. Washington CW, McCoy KE, Zipfel GJ: Update
onthenaturalhistoryof cavernousmalformations and
factors predicting aggressive clinical presentation.
Neurosurg Focus 29:E72010.
44. Ziyal IM, Sekhar LN, Salas E, Sen C: Surgical man-
agement of cavernous malformations of the brainstem. Br J
Neurosurg 13:366-375, 1999.
45. Zubay G,Porter RW,Spetzler RF:Transpetrosal ap-proaches. Op
Tech Neurosurg 4:24-29, 2001.
Conflict of interest statement: The authors declare that the
article content was composed in the absence of any
commercial or financial relationships that could be
construed as a potential conflict of interest.
Received 12 September 2011; accepted 14 April 2012
Citation: World Neurosurg. (2013) 79, 5/6:691-703.
http://dx.doi.org/10.1016/j.wneu.2012.04.030
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter 2013 Published by Elsevier
Inc.
PEER-REVIEW REPORTS
JEFFREY C. MAI ET AL. RESECTION OF CAVERNOUS MALFORMATIONS OF
THE BRAINSTEM
WORLD NEUROSURGERY 79 [5/6]: 691-703, MAY/JUNE 2013
www.WORLDNEUROSURGERY.org 703
http://dx.doi.org/10.1016/j.wneu.2012.04.030http://www.worldneurosurgery.org/http://www.sciencedirect.com/http://www.sciencedirect.com/http://www.worldneurosurgery.org/http://dx.doi.org/10.1016/j.wneu.2012.04.030