Embed Size (px)
Citation preview
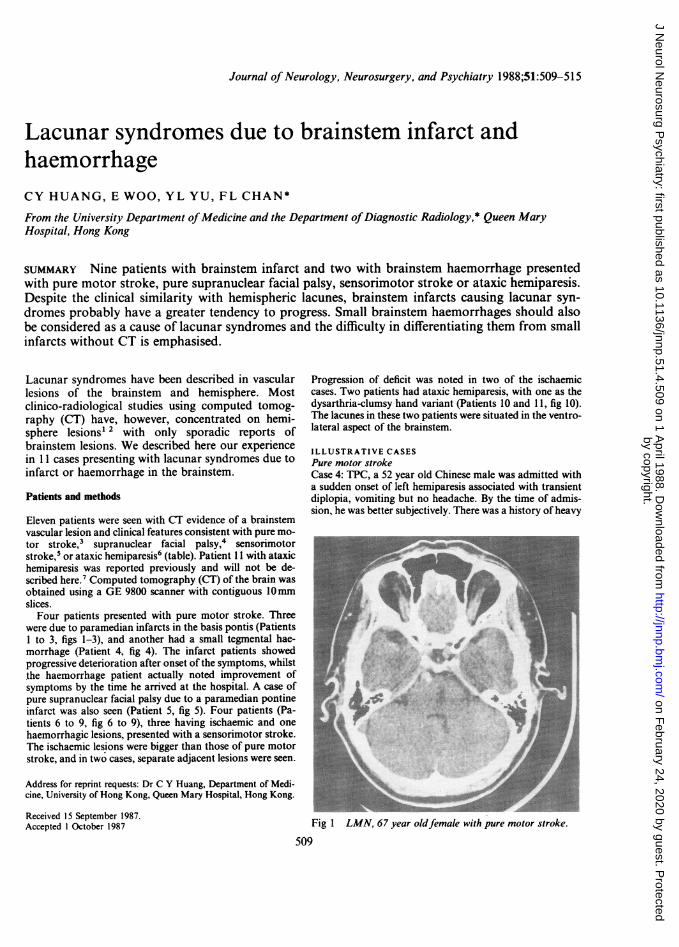
Journal of Neurology, Neurosurgery, and Psychiatry 1988;51:509-515
Lacunar syndromes due to brainstem infarct andhaemorrhageCY HUANG, E WOO, YL YU, FL CHAN*
From the University Department ofMedicine and the Department ofDiagnostic Radiology,* Queen MaryHospital, Hong Kong
SUMMARY Nine patients with brainstem infarct and two with brainstem haemorrhage presentedwith pure motor stroke, pure supranuclear facial palsy, sensorimotor stroke or ataxic hemiparesis.Despite the clinical similarity with hemispheric lacunes, brainstem infarcts causing lacunar syn-
dromes probably have a greater tendency to progress. Small brainstem haemorrhages should alsobe considered as a cause of lacunar syndromes and the difficulty in differentiating them from smallinfarcts without CT is emphasised.
Lacunar syndromes have been described in vascularlesions of the brainstem and hemisphere. Mostclinico-radiological studies using computed tomog-raphy (CT) have, however, concentrated on hemi-sphere lesions' 2 with only sporadic reports ofbrainstem lesions. We described here our experiencein 11 cases presenting with lacunar syndromes due toinfarct or haemorrhage in the brainstem.
Patients and methods
Eleven patients were seen with CT evidence of a brainstemvascular lesion and clinical features consistent with pure mo-tor stroke,3 supranuclear facial palsy,4 sensorimotorstroke,5 or ataxic hemiparesis6 (table). Patient 11 with ataxichemiparesis was reported previously and will not be de-scribed here.' Computed tomography (CT) of the brain wasobtained using a GE 9800 scanner with contiguous 10mmslices.
Four patients presented with pure motor stroke. Threewere due to paramedian infarcts in the basis pontis (Patients1 to 3, figs 1-3), and another had a small tegmental hae-morrhage (Patient 4, fig 4). The infarct patients showedprogressive deterioration after onset of the symptoms, whilstthe haemorrhage patient actually noted improvement ofsymptoms by the time he arrived at the hospital. A case ofpure supranuclear facial palsy due to a paramedian pontineinfarct was also seen (Patient 5, fig 5). Four patients (Pa-tients 6 to 9, fig 6 to 9), three having ischaemic and onehaemorrhagic lesions, presented with a sensorimotor stroke.The ischaemic lesions were bigger than those of pure motorstroke, and in two cases, separate adjacent lesions were seen.
Address for reprint requests: Dr C Y Huang, Department of Medi-cine, University of Hong Kong, Queen Mary Hospital, Hong Kong.
Received 15 September 1987.Accepted 1 October 1987
Progression of deficit was noted in two of the ischaemiccases. Two patients had ataxic hemiparesis, with one as thedysarthria-clumsy hand variant (Patients 10 and 11, fig 10).The lacunes in these two patients were situated in the ventro-lateral aspect of the brainstem.
ILLUSTRATIVE CASESPure motor strokeCase 4: TPC, a 52 year old Chinese male was admitted witha sudden onset of left hemiparesis associated with transientdiplopia, vomiting but no headache. By the time of admis-sion, he was better subjectively. There was a history of heavy
Fig I LMN, 67 year oldfemale with pure motor stroke.
509
by copyright. on F
ebruary 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.51.4.509 on 1 April 1988. D
ownloaded from
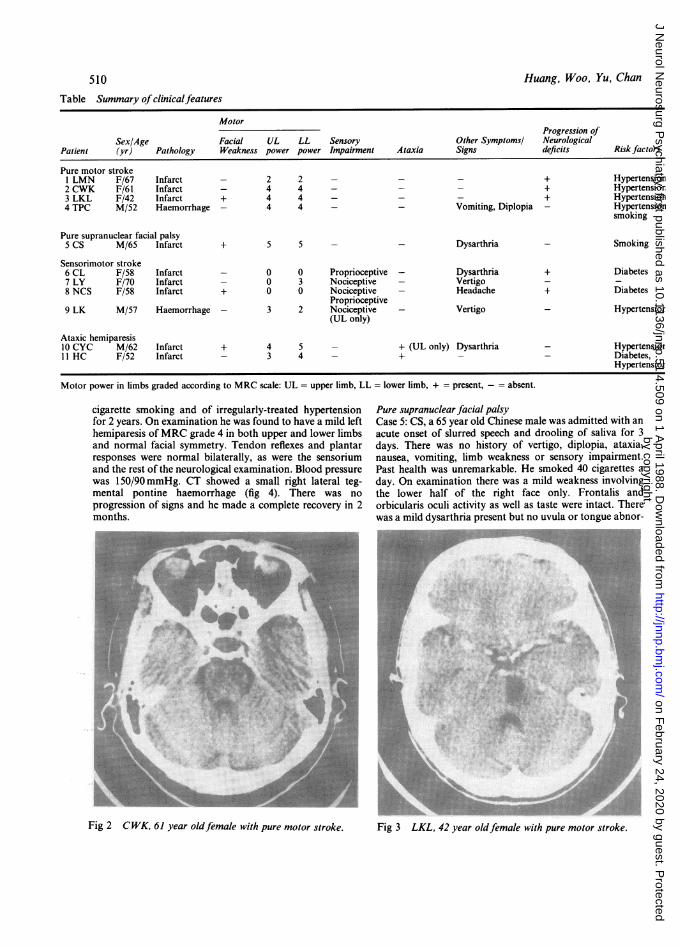
Table Summary ofclinicalfeatures
MotorProgression of
Sex/Age Facial UL LL Sensory Other Symptomsl NeurologicalPatient (yr) Pathology Weakness power power Impairment Ataxia Signs deficits Risk factors
Pure motor stroke1 LMN F/67 Infarct - 2 2 - - - + Hypertension2 CWK F/61 Infarct - 4 4 - - - + Hypertensior3 LKL F/42 Infarct + 4 4 - - - + Hypertension4 TPC M/52 Haemorrhage - 4 4 - - Vomiting, Diplopia - Hypertension
smoking
Pure supranuclear facial palsy5 Cs M/65 Infarct + 5 5 - - Dysarthria - Smoking
Sensorimotor stroke6 CL F/58 Infarct - 0 0 Proprioceptive - Dysarthria + Diabetes7 LY F/70 Infarct - 0 3 Nociceptive - Vertigo8 NCS F/58 Infarct + 0 0 Nociceptive - Headache + Diabetes
Proprioceptive9 LK M/57 Haemorrhage - 3 2 Nociceptive - Vertigo - Hypertensior
(UL only)
Ataxic hemiparesis10 CYC M/62 Infarct + 4 5 - + (UL only) Dysarthria - Hypertensior11 HC F/52 Infarct - 3 4 - + - - Diabetes,
Hypertensior
Motor power in limbs graded according to MRC scale: UL = upper limb, LL = lower limb, + = present, absent.
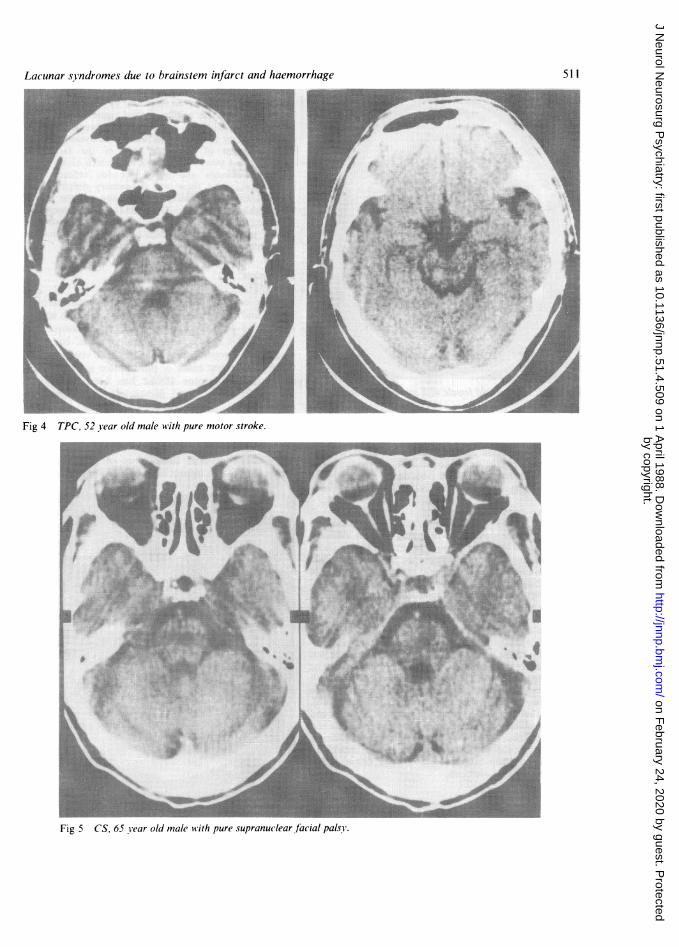
cigarette smoking and of irregularly-treated hypertensionfor 2 years. On examination he was found to have a mild lefthemiparesis ofMRC grade 4 in both upper and lower limbsand normal facial symmetry. Tendon reflexes and plantarresponses were normal bilaterally, as were the sensoriumand the rest of the neurological examination. Blood pressurewas 150/90 mmHg. CT showed a small right lateral teg-mental pontine haemorrhage (fig 4). There was noprogression of signs and he made a complete recovery in 2months.
Pure supranuclear facial palsyCase 5: CS, a 65 year old Chinese male was admitted with anacute onset of slurred speech and drooling of saliva for 3days. There was no history of vertigo, diplopia, ataxia,nausea, vomiting, limb weakness or sensory impairment.Past health was unremarkable. He smoked 40 cigarettes aday. On examination there was a mild weakness involvingthe lower half of the right face only. Frontalis andorbicularis oculi activity as well as taste were intact. Therewas a mild dysarthria present but no uvula or tongue abnor-
Fig 2 CWK, 61 year oldfemale with pure motor stroke.
Huang, Woo, Yu, Chan510
1 3K,6 .:Iw %-I
Fig 3 LKL, 42 year oldfemale with pure motor stroke.
by copyright. on F
ebruary 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.51.4.509 on 1 April 1988. D
ownloaded from
Lacunar syndromes due to brainstem infarct and haemorrhage
Fig 4 TPC, 52 Year old male with pure motor stroke.t.....:: 21'."1. M .._ w fI_ _
:..~~~~~~~~~somm
_~~~~~~U" Af_~~~~~~l W
Fig 5 CS, 65 Year old male with pure supranuclear facial pals!y.
511
by copyright. on F
ebruary 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.51.4.509 on 1 April 1988. D
ownloaded from

512
Fig 6 CL,..8 year oldfemak with sensorimotorstr....Fig 6 CL, 58 year oldfemale with sensorimotor stroke.
mality and the gag reflex was normal. The rest of the nervoussystem was also normal. Blood pressure was 130/80 mmHg,no bruits were heard and the heart was normal. CT per-formed 10 days after onset showed a small hypodense areajust lateral to the middle of the pons on the left (fig 5). Thefacial weakness resolved completely over the next few weeks.
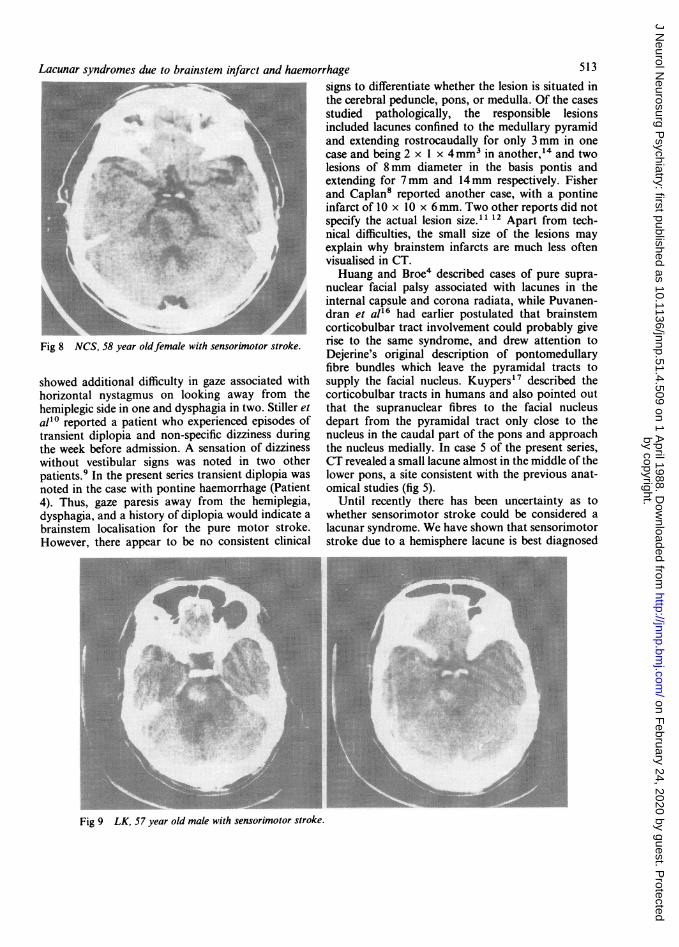
Sensorimotor strokeCase 8: NCS, a 58 year old Chinese woman found that shehad a mild left hemiparesis upon waking up in the morning.She had a mild headache the night before, but there were novertigo, diplopia, or other symptoms. She had been toldsome years ago that she had mild diabetes which did notrequire drug treatment. On admission there was a MRCgrade 3 left hemiparesis, with mild left supranuclear facialweakness and dysarthria, accompanied by decreased touch,pin prick, temperature and position sense on the left.Vibration sense was absent below the knees and distal to theelbows bilaterally. Cardiovascular examination was un-remarkable: pulse was 80/min regular, blood pressure was150/80 mmHg and there was no bruit heard in the heart orneck. After admission, the weakness progressed steadily tillshe became hemiplegic by the next day. CT performed onday 2 revealed a large right pontine infarct (fig 8).Investigation revealed a blood glucose of 12-9 mmol anddiabetes mellitus was confirmed by persistent glycosuria andhyperglycaemia. The sensory deficits gradually abated andat 3 months she was able to walk with a quadripoddespite a foot drop. She remained however devoid of lefthand function or movements.
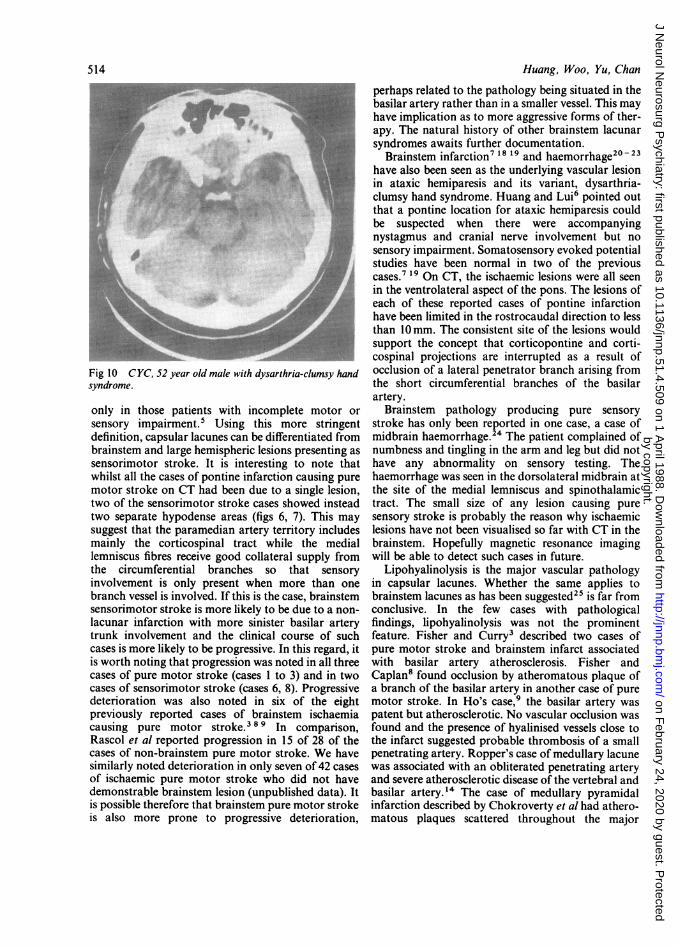
Ataxic hemiparesisCase 10: CYC, a 62 year old Chinese male was known to behypertensive and receiving anti-hypertensive treatment for
Huang, Woo, Yu, Chanover 20 years. He had an episode of spontaneous vertigolasting an hour and not accompanied by other symptoms 2years previously. He neither smoked cigarettes nor drankalcohol. He developed a sudden left sided weakness in thedaytime and on admission was found to be dysarthric, withmild weakness of the right side of the face, andMRC grade 4 power in the right arm which also showeddysdiadochokinesia and ataxia. Tendon reflexes wereunremarkable and there was no sensory deficit. Bloodpressure was 160/90mmHg on admission and the rest ofcardiovascular examination was normal. A hypodense lesionwas visualised in the ventrolateral region of the brainstem onthe CT scan performed 17 days later (fig 10). He made agood recovery over the next 3 months.
Discussion
In their original description of pure motor stroke,Fisher and Curry described pontine infarction as theunderlying pathology in three cases.3 SubsequentlyFisher and Caplan8 added another case. In morerecent years, pontine infarction has been visualised onCT in four other cases of pure motor stroke.9 10 Inaddition pure motor stroke has been seen withinfarcts in the cerebral peduncle" and medullarypyramid.'2 -15 As in the previous cases, our threecases of pure motor stroke were found to have anischaemic lesion in the paramedian aspect of the pons(fig 1 to 3). In addition to the motor weakness, Fisherand Curry's original three cases of pathologicallyproven brainstem infarct causing pure motor stroke3
Fig 7 L Y, 70 year oldfemale with sensorimotor stroke.
by copyright. on F
ebruary 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.51.4.509 on 1 April 1988. D
ownloaded from
Lacunar syndromes due to brainstem infarct and haemorrhage
Fig 8 NCS, 58 year oldfemale with sensorimotor stroke.
showed additional difficulty in gaze associated withhorizontal nystagmus on looking away from thehemiplegic side in one and dysphagia in two. Stiller etal'0 reported a patient who experienced episodes oftransient diplopia and non-specific dizziness duringthe week before admission. A sensation of dizzinesswithout vestibular signs was noted in two otherpatients.9 In the present series transient diplopia wasnoted in the case with pontine haemorrhage (Patient4). Thus, gaze paresis away from the hemiplegia,dysphagia, and a history of diplopia would indicate abrainstem localisation for the pure motor stroke.However, there appear to be no consistent clinical
signs to differentiate whether the lesion is situated inthe cerebral peduncle, pons, or medulla. Of the casesstudied pathologically, the responsible lesionsincluded lacunes confined to the medullary pyramidand extending rostrocaudally for only 3 mm in onecase and being 2 x 1 x 4mm3 in another,"4 and twolesions of 8mm diameter in the basis pontis andextending for 7mm and 14mm respectively. Fisherand Caplan8 reported another case, with a pontineinfarct of 10 x 10 x 6 mm. Two other reports did notspecify the actual lesion size. " 12 Apart from tech-nical difficulties, the small size of the lesions mayexplain why brainstem infarcts are much less oftenvisualised in CT.Huang and Broe4 described cases of pure supra-
nuclear facial palsy associated with lacunes in theinternal capsule and corona radiata, while Puvanen-dran et al'6 had earlier postulated that brainstemcorticobulbar tract involvement could probably giverise to the same syndrome, and drew attention toDejerine's original description of pontomedullaryfibre bundles which leave the pyramidal tracts tosupply the facial nucleus. Kuypers"7 described thecorticobulbar tracts in humans and also pointed outthat the supranuclear fibres to the facial nucleusdepart from the pyramidal tract only close to thenucleus in the caudal part of the pons and approachthe nucleus medially. In case 5 of the present series,CT revealed a small lacune almost in the middle of thelower pons, a site consistent with the previous anat-omical studies (fig 5).
Until recently there has been uncertainty as towhether sensorimotor stroke could be considered alacunar syndrome. We have shown that sensorimotorstroke due to a hemisphere lacune is best diagnosed
Fig;: -' :-::LK::57 y a oldmalew..itenoi-:otor s ok:e:... -:.e-: --: ::-n- :- -- - . ..
Fig 9 LK, 57 year old male with sensorimotor stroke.
513
by copyright. on F
ebruary 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.51.4.509 on 1 April 1988. D
ownloaded from
514
Fig 10 CYC, 52 year old male with dysarthria-clumsy handsyndrome.
only in those patients with incomplete motor orsensory impairment.' Using this more stringentdefinition, capsular lacunes can be differentiated frombrainstem and large hemispheric lesions presenting assensorimotor stroke. It is interesting to note thatwhilst all the cases of pontine infarction causing puremotor stroke on CT had been due to a single lesion,two of the sensorimotor stroke cases showed insteadtwo separate hypodense areas (figs 6, 7). This maysuggest that the paramedian artery territory includesmainly the corticospinal tract while the mediallemniscus fibres receive good collateral supply fromthe circumferential branches so that sensoryinvolvement is only present when more than onebranch vessel is involved. If this is the case, brainstemsensorimotor stroke is more likely to be due to a non-lacunar infarction with more sinister basilar arterytrunk involvement and the clinical course of suchcases is more likely to be progressive. In this regard, itis worth noting that progression was noted in all threecases of pure motor stroke (cases 1 to 3) and in twocases of sensorimotor stroke (cases 6, 8). Progressivedeterioration was also noted in six of the eightpreviously reported cases of brainstem ischaemiacausing pure motor stroke.389 In comparison,Rascol et al reported progression in 15 of 28 of thecases of non-brainstem pure motor stroke. We havesimilarly noted deterioration in only seven of 42 casesof ischaemic pure motor stroke who did not havedemonstrable brainstem lesion (unpublished data). Itis possible therefore that brainstem pure motor strokeis also more prone to progressive deterioration,
Huang, Woo, Yu, Chan
perhaps related to the pathology being situated in thebasilar artery rather than in a smaller vessel. This mayhave implication as to more aggressive forms of ther-apy. The natural history of other brainstem lacunarsyndromes awaits further documentation.
Brainstem infarction7 18 19 and haemorrhage20 - 23have also been seen as the underlying vascular lesionin ataxic hemiparesis and its variant, dysarthria-clumsy hand syndrome. Huang and Lui6 pointed outthat a pontine location for ataxic hemiparesis couldbe suspected when there were accompanyingnystagmus and cranial nerve involvement but nosensory impairment. Somatosensory evoked potentialstudies have been normal in two of the previouscases.7 19 On CT, the ischaemic lesions were all seenin the ventrolateral aspect of the pons. The lesions ofeach of these reported cases of pontine infarctionhave been limited in the rostrocaudal direction to lessthan 10mm. The consistent site of the lesions wouldsupport the concept that corticopontine and corti-cospinal projections are interrupted as a result ofocclusion of a lateral penetrator branch arising fromthe short circumferential branches of the basilarartery.
Brainstem pathology producing pure sensorystroke has only been reported in one case, a case ofmidbrain haemorrhage.24 The patient complained ofnumbness and tingling in the arm and leg but did nothave any abnormality on sensory testing. Thehaemorrhage was seen in the dorsolateral midbrain atthe site of the medial lemniscus and spinothalamictract. The small size of any lesion causing puresensory stroke is probably the reason why ischaemiclesions have not been visualised so far with CT in thebrainstem. Hopefully magnetic resonance imagingwill be able to detect such cases in future.
Lipohyalinolysis is the major vascular pathologyin capsular lacunes. Whether the same applies tobrainstem lacunes as has been suggested25 is far fromconclusive. In the few cases with pathologicalfindings, lipohyalinolysis was not the prominentfeature. Fisher and Curry3 described two cases ofpure motor stroke and brainstem infarct associatedwith basilar artery atherosclerosis. Fisher andCaplan8 found occlusion by atheromatous plaque ofa branch of the basilar artery in another case of puremotor stroke. In Ho's case,9 the basilar artery waspatent but atherosclerotic. No vascular occlusion wasfound and the presence of hyalinised vessels close tothe infarct suggested probable thrombosis of a smallpenetrating artery. Ropper's case of medullary lacunewas associated with an obliterated penetrating arteryand severe atherosclerotic disease of the vertebral andbasilar artery. 4 The case of medullary pyramidalinfarction described by Chokroverty et al had athero-matous plaques scattered throughout the major
by copyright. on F
ebruary 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.51.4.509 on 1 April 1988. D
ownloaded from

Lacunar syndromes due to brainstem infarct and haemorrhage
cerebral arteries,"2 whilst the case studied by Ho andMeyer had patent vertebral arteries and basilararteries with narrowing of the lumen by patchy areasof calcified atheromatous changes.'5 Thus, basilarartery atherosclerosis appears to accompany brain-stem infarcts frequently even when they presentclinically as lacunar syndromes. Indeed, there is atpresent no pathological correlation for the CT visual-ised infarcts. Whether they are really lacunes or muchlarger lesions due to occlusion ofmore than one vesselremains to be answered.
Prior to the availability of CT the prognosis ofbrainstem haemorrhage had been held to be dismal.Since the advent of CT more benign cases havebeen described.26 27 A lateral tegmental brainstemhaemorrhage syndrome has been recognised featuringipsilateral conjugate gaze palsy, ipsilateral inter-nuclear ophthalmoplegia, a small reactive pupil,ipsilateral ataxia and contralateral sensorimotorimpairment.26 The present cases (Patients 4 and 9)and the others in the literature underline the evenmore benign presentation of brainstem haemorrhage,presenting as pure motor stroke,28 pure sensorystroke,24 sensorimotor stroke,23 or ataxic hemi-paresis.20-23 It is noteworthy that there were nouseful symptoms or signs in our two cases or those inthe literature which would allow confident separationof these small haemorrhages from ischaemic brain-stem lesions presenting as lacunar syndromes. Thedorsolateral location of most of these haemorrhageswould suggest that they are due. to rupture of thecircumferential branches rather than the paramedianarteries. Unlike ischaemic lesions, the clinicalsyndromes did not correspond to sites ofhaemorrhages, thus suggesting that pressure effectrather than tit$ue destruction may have beenresponsible for the symptoms and signs.
References
I Nelson RF, Pullicino P, Kendall BE, Marshall J. Computedtomography in patients presenting with lacunar syndromes.Stroke 1980;11:255-61.
2 Donnan GA, Tress BM, Bladin P. A prospective study of lacunarinfarction using computerized tomography. Neurology1982:32;49-56.
3 Fisher CM, Curry HB. Pure motor hemiplegia of vascular origin.Arch Neurol 1965;13:30-44.
4 Huang CY, Broe G. Isolated facial palsy: a new lacunar
syndrome. J Neurol Neurosurg Psychiatry 1984;47:84-6.5 Huang CY, Woo E, Yu YL, Chan FL. When is sensorimotor
stroke a lacunar syndrome? J Neurol Neurosurg Psychiatry1987;50:720-6.
6 Huang CY, Lui FS. Ataxic-hemiparesis, localization and clinicalfeatures. Stroke 1984;15:363-5.
7 Huang CY, Chan KH. Pontine ataxic hemiparesis, a lateralpenetrator syndrome? J Neurol Neurosurg Psychiatry1984;47: 1046-7.
8 Fisher CM, Caplan LR. Basilar artery branch occlusion: A causeof pontine infarction. Neurology 1971;21:900-5.
9 Rascol A, Clanet M, Manelfe C, Guiraud B and Bonafe A. Puremotor hemiplegia: CT study of 30 cases. Stroke 1982;13:11-7.
10 Stiller J, Shanzer S, Yang W. Brainstem lesions with pure motorhemiparesis. Computed tomographic demonstration. ArchNeurol 1982;39:660-1.
11 Ho KL. Pure motor hemiplegia due to infarction of the cerebralpeduncle. Arch Neurol 1982;39:524-6.
12 Chokroverty S, Rubino FA, Haller C. Pure motor hemiplegia dueto pyramidal infarction. Arch Neurol 1985;32:647-8.
13 Leestma JE, Noronha A. Pure motor hemiplegia, medullarypyramid lesion, and olivary hypertrophy. J Neurol NeurosurgPsychiatry 1976;39:877-84.
14 Ropper AH, Fisher CM, Kleinman GM. Pyramidal infarction inthe medullar: A cause of pure motor hemiplegia sparing theface. Neurology 1979;29:91-5.
15 Ho KL, Meyer KR. The medial medullary syndrome. ArchNeurol 1981;38:385-7.
16 Puvanendran K, Wong PK, Ransome GA. Syndrome ofDejerine's fourth reich. Acta Neurol Scand 1978;58:345-53.
17 Kuypers HGJ. Corticobulbar connexions to the pons and lowerbrain-stem in man. An anatomical study. Brain 1958;81:364-88.
18 Fisher CM. Ataxic hemiparesis. A pathological study. ArchNeurol 1978;35:126-8.
19 Delgado G, Gallego J, Zubieta JL. High-resolution CT scan inpontine ataxic hemiparesis. J Neurol Neurosurg Psychiatry1985;48:1069.
20 Schnapper RA. Pontine hemorrhage presenting as ataxic hemi-paresis. Stroke 1982;13:518-9.
21 Tuhrim S, Yang WC, Rubinowitz H, Weinberger J. Primary pon-tine hemorrhage and the dysarthria-clumsy handsyndrome. Neurology 1982;32:1027-8.
22 Kobatake K, Shinohara Y. Ataxic hemiparesis in patients withprimary pontine hemorrhage. Stroke 1983;14:762-4.
23 Mori E, Tabuchi M, Yamadori A. Lacunar syndrome due tointracerebral hemorrhage. Stroke 1985;16:454-9.
24 Tuttle PV, Reinmuth OM. Midbrain hemorrhage producing puresensory stroke. Arch Neurol 1984;41:794-5.
25 Fisher CM. The arterial lesions underlying lacunes. Acta Neu-ropathol (Berl) 1969;12:1-15.
26 Caplan LR, Goodwin JA. Lateral tegmental brainstem hemor-rhages. Neurology 1982;32:252-60.
27 Masiyama S, Niizuma H, Suzuki J. Pontine haemorrhage: aclinical analysis of 26 cases. J Neurol Neurosurg Psychiatry1985;48:658-62.
28 Lee KY, Lie SK, Chiang TR. Small intracerebral hemorrhageclinically simulating lacunar infarction. J Formosan Med Assoc1983;82:993-1 000.
515
by copyright. on F
ebruary 24, 2020 by guest. Protected
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.51.4.509 on 1 April 1988. D
ownloaded from