Embed Size (px)
Citation preview
Labour Management
Neil Vanes
StR5 Obs and Gynae
Labour & Monitoring & Management
Learning Aims:
What is normal labour?
What is abnormal labour?
How is abnormal labour managed?
How is abnormal labour monitored?
Early take home points
IMPOSSIBLE to cover all abnormality in one!!
• Specialist Training takes 7-10yrs
Don’t think that majority of labours are abnormal, they are NOT
JUMP IN – don’t be shy
What is normal labour?Spontaneous onset of contractions at term
with a normally grown fetus
in cephalic presentation
progressing to full dilatation
with a spontaneous vaginal delivery
of a live infant
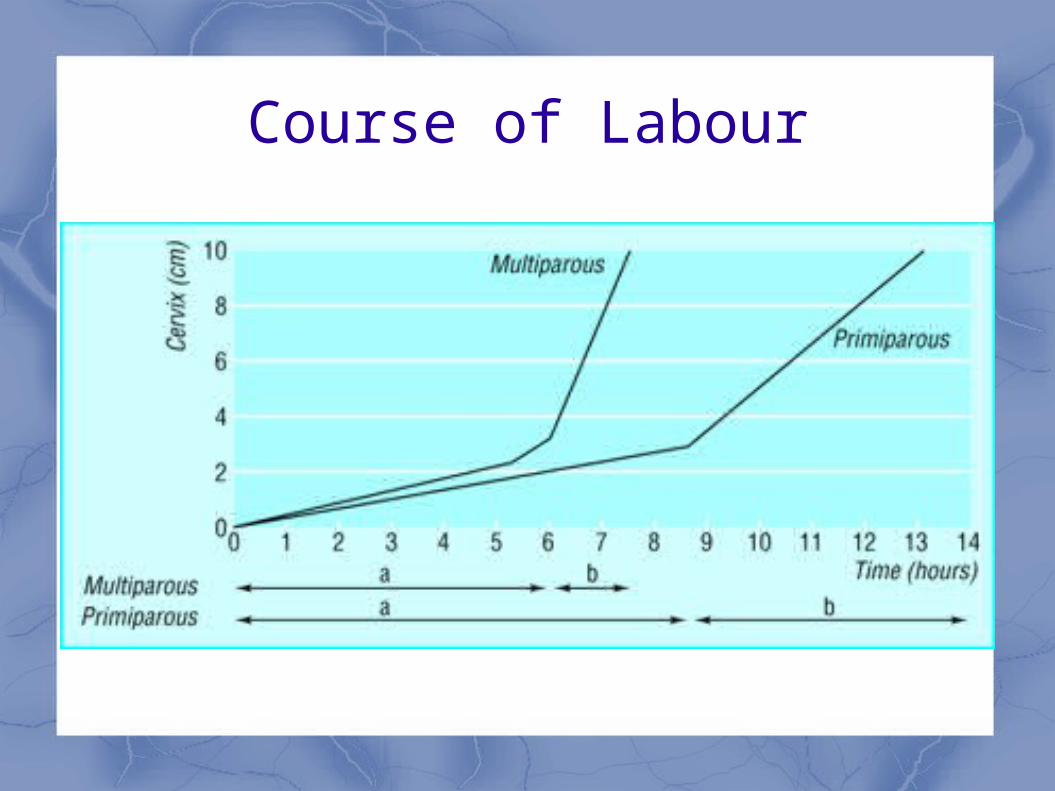
Course of Labour
What is abnormal labour?
Prolonged rupture of membranesProlonged pregnancy with induction of labourIntra-uterine growth restriction / macrosomia
Abnormal presentation Failure to progress
Operative vaginal deliveryRetained Placenta
ABBREVIATIONS
PROM: prelabour rupture of membranes, sometimes referred to as premature rupture of membranes. Can also be used to mean prolonged rupture of membranes
PPROM: preterm prelabour rupture of membranes, ie before 37 weeks
SROM: spontaneous rupture of membranes
ROM: rupture of membranes
Prelabour / prolonged rupture of membranes (PROM)
Definition:
spontaneous rupture of membranes (SROM) at term without the onset of spontaneous contractions
Prelabour rupture of the membranes (PROM) occurs in 6-19% of term pregnancies.
Risks of PROM at term
1. maternal/neonatal infection
2. prolapsed cord.
• Epidemiological data on time interval from PROM to spontaneous labour suggests that most (86%) women go into spontaneous labour within 24hrs of rupturing their membranes.
• The rate of spontaneous labour after this is about 5% per day.
• As the time between the rupture of the membranes and the onset of labour increases, so do
the risks of maternal and fetal infection.
• Induction of labour reduces these risks.
CHOICES for PROM
1.immediate induction of labour
2.expectant management (should not exceed 96 hours)
Prolonged pregnancy with induction of labour
Term between 37 completed weeks and 42
weeks Prolonged pregnancy
after 42 weeks Risks:
Stillbirth Meconium liquor / aspiration
Induction of Labour
Methods Prostaglandins – ripen cervix and prime
uterus for contractions Artificial rupture of membranes Syntocinon infusion
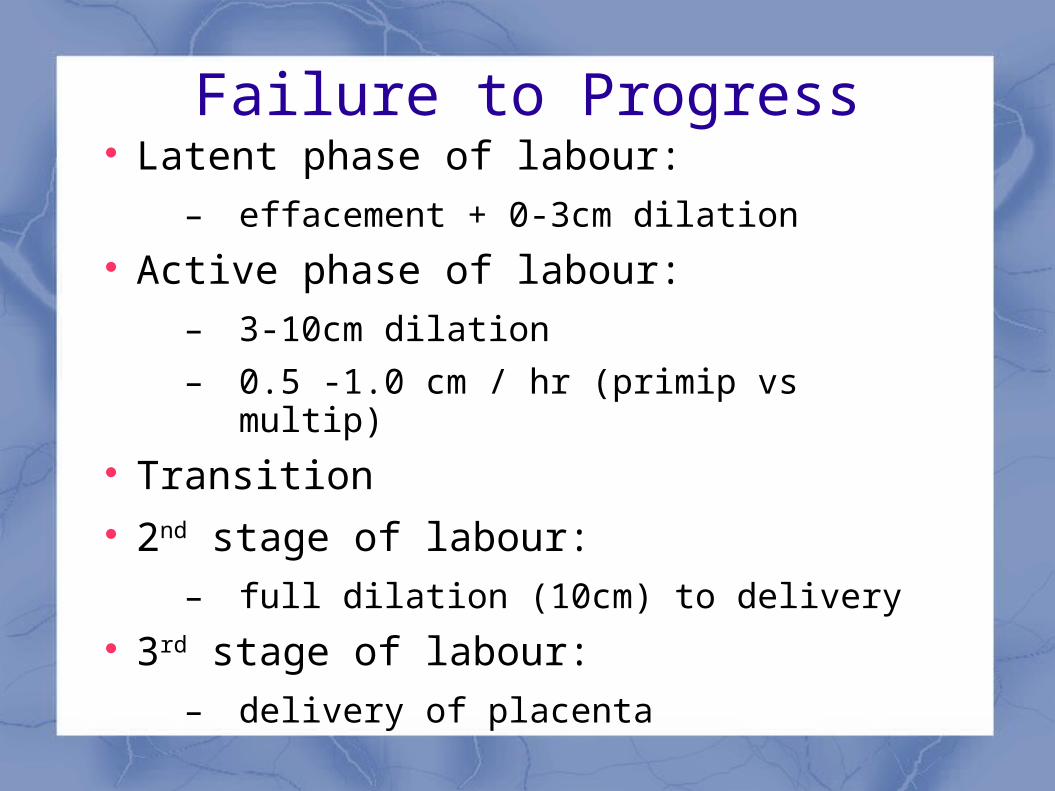
Failure to Progress Latent phase of labour:
– effacement + 0-3cm dilation Active phase of labour:
– 3-10cm dilation
– 0.5 -1.0 cm / hr (primip vs multip) Transition 2nd stage of labour:
– full dilation (10cm) to delivery 3rd stage of labour:
– delivery of placenta
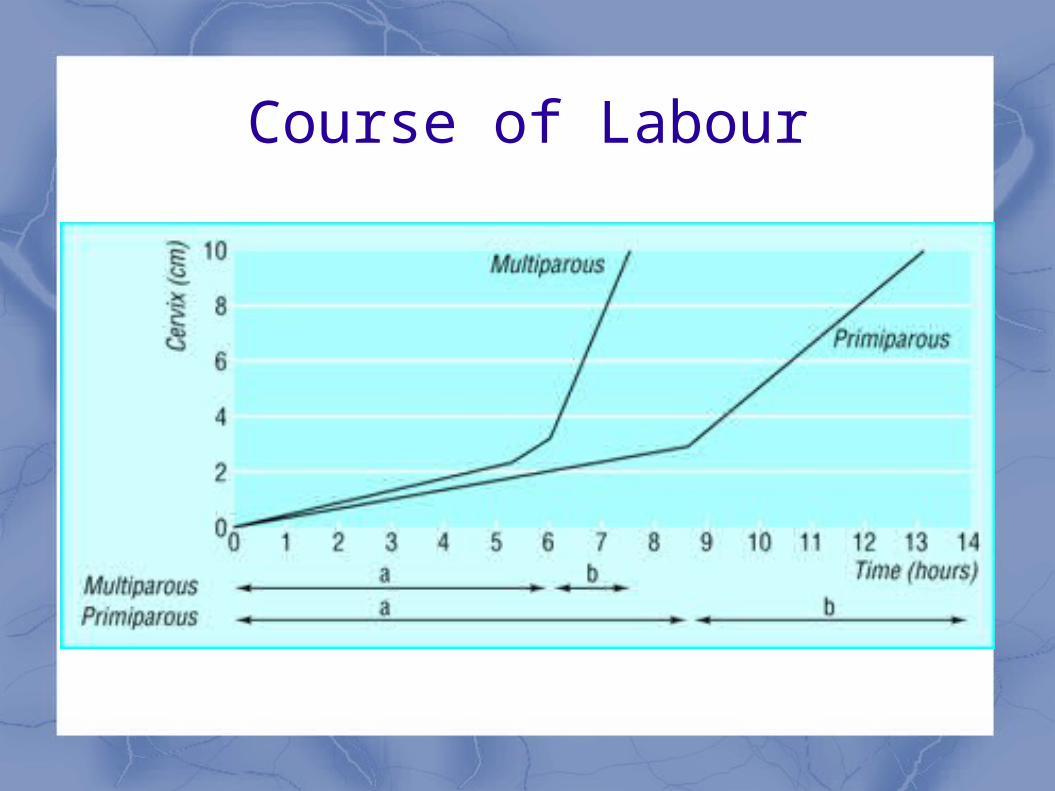
Course of Labour

Failure to Progress Assess progress in labour by
PA (abdominal palpation) VE (vaginal examination)
Engagement / station of fetal head PA:
engagement (fifths palpable: 5/5 to 0/5) VE:
descent of fetal head (station: -3 to +3) Fetal position: LOA, LOT, DOP, ROP,
ROT, ROA
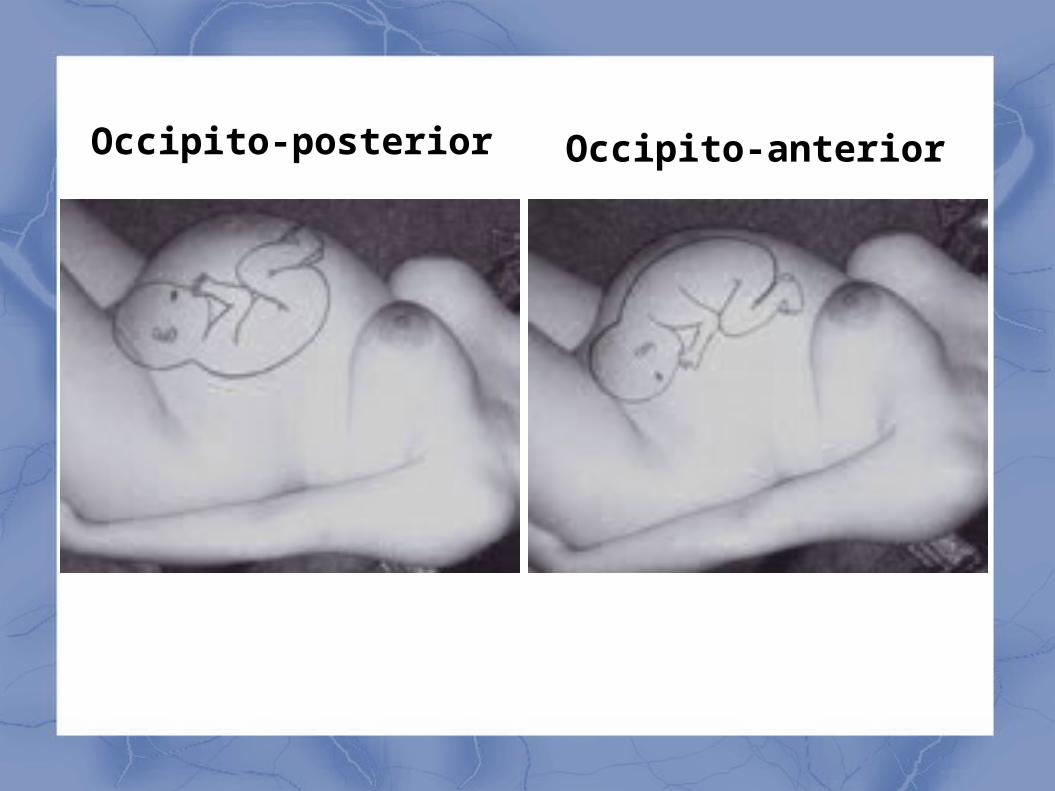
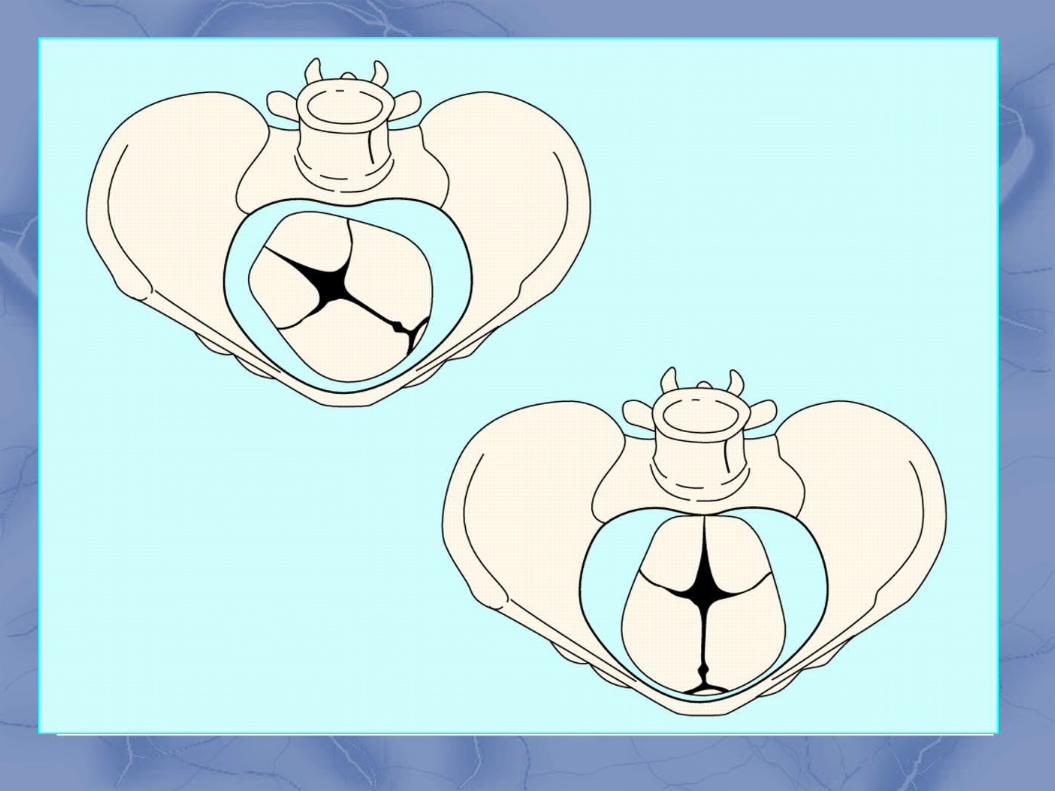
Occipito-posterior Occipito-anterior
How is abnormal labour managed?
Power Passage Passenger
How is abnormal labour managed?
Power: Effective contractions Maternal factors: e.g. hydration Membranes intact? Augment contractions e.g. syntocinon
How is abnormal labour managed?
Passenger Fetal size Fetal position (OA vs OP)
Encourage OA position (all fours, upright) Epidural
How is abnormal labour managed?
Passage Assess pelvis: Cephalo-pelvic disportion
(CPD) Retrospective diagnosis:
normal size baby in occipito-posterior position big baby in occipito-anterior position
Promote anterior occipito position
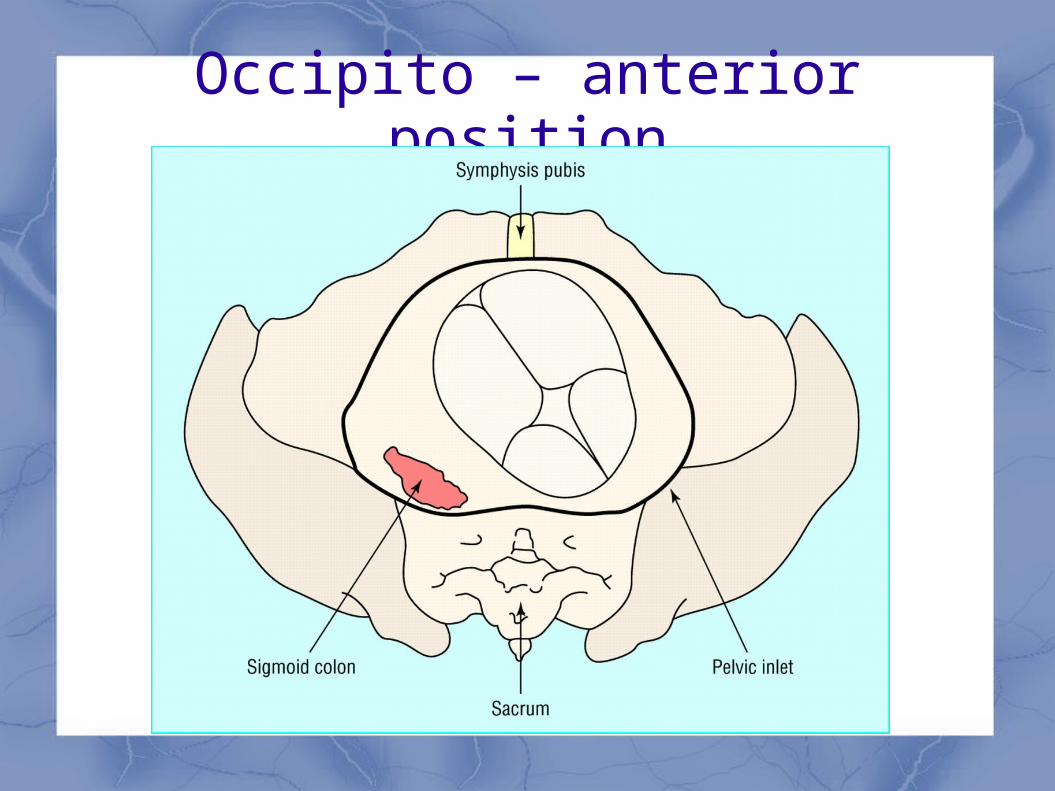
Occipito – anterior position
How is abnormal labour monitored?
Maternal monitoring Partogram
Fetal monitoring CTG
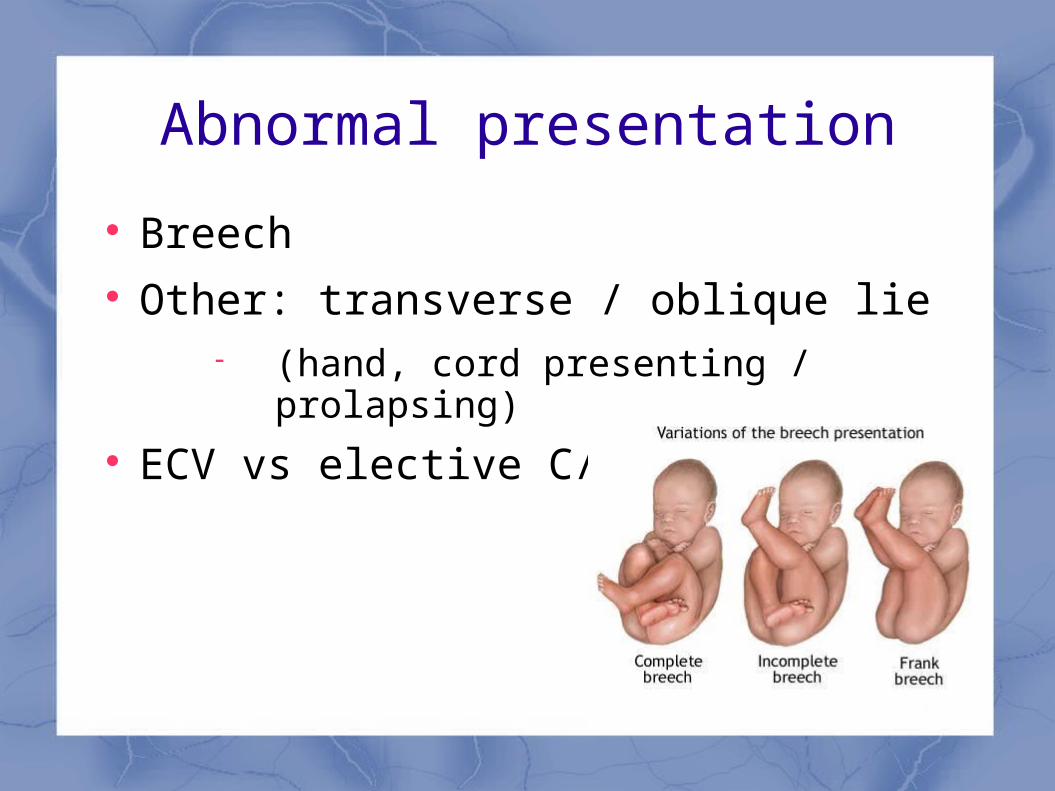
Abnormal presentation
Breech Other: transverse / oblique lie
(hand, cord presenting / prolapsing) ECV vs elective C/S
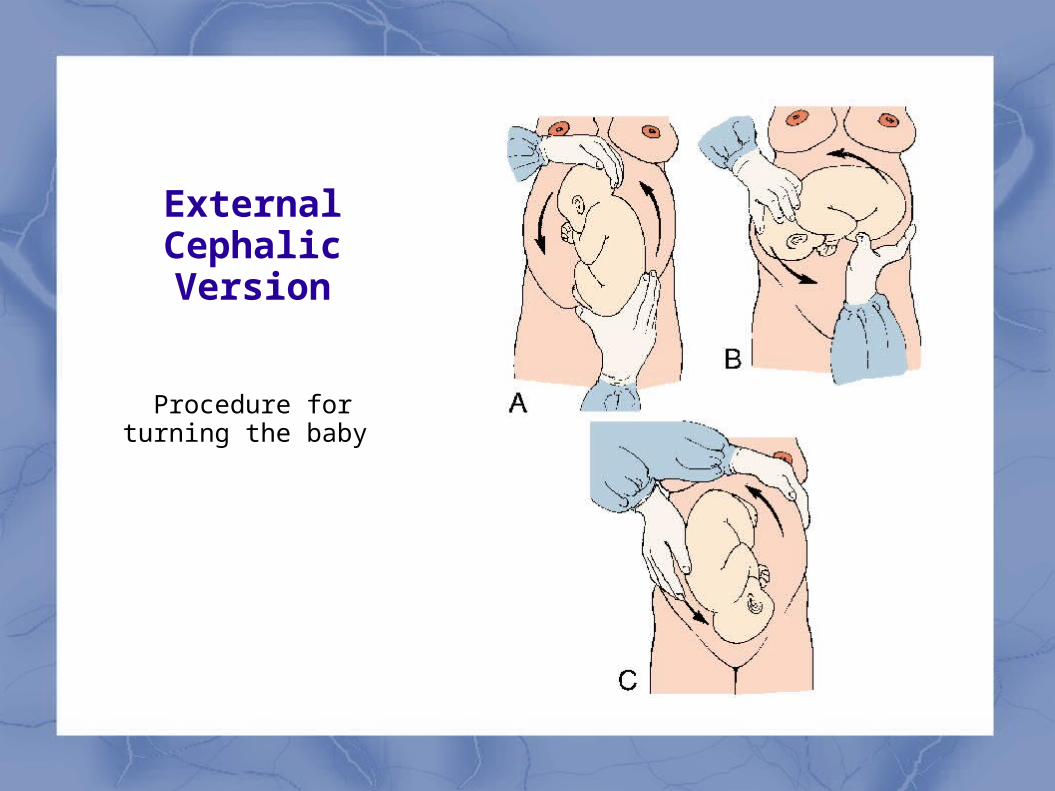
External Cephalic Version
Procedure for turning the baby
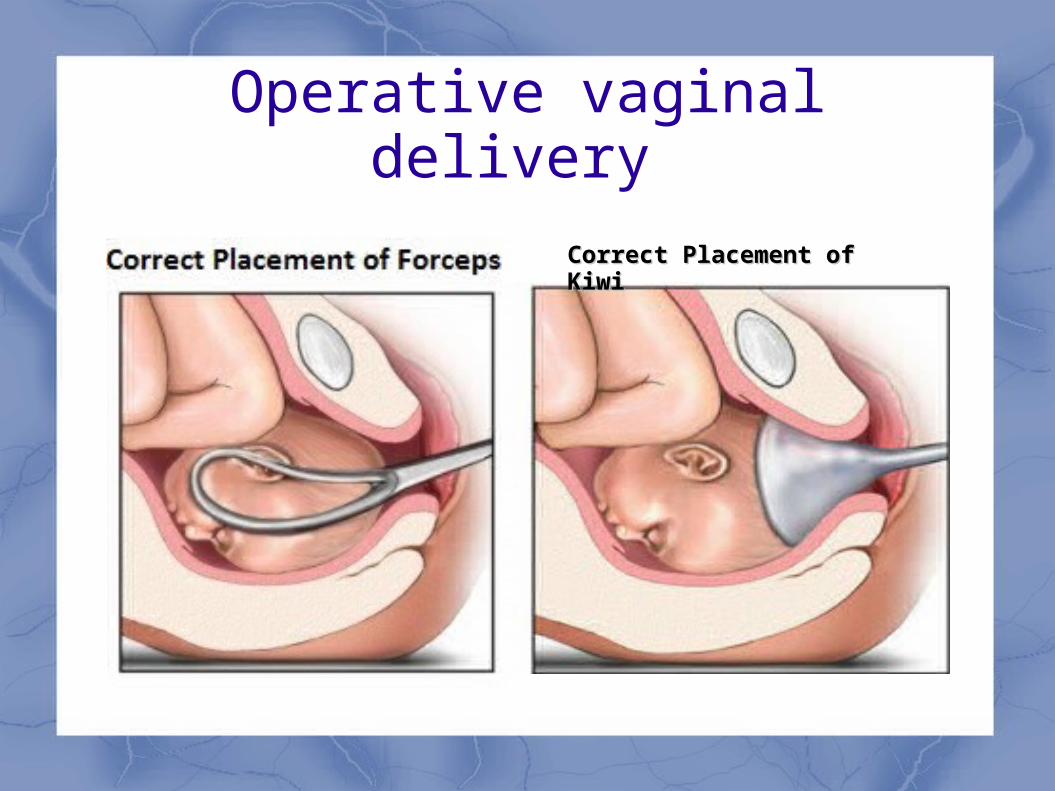
Operative vaginal delivery
Correct Placement of KiwiCorrect Placement of Kiwi
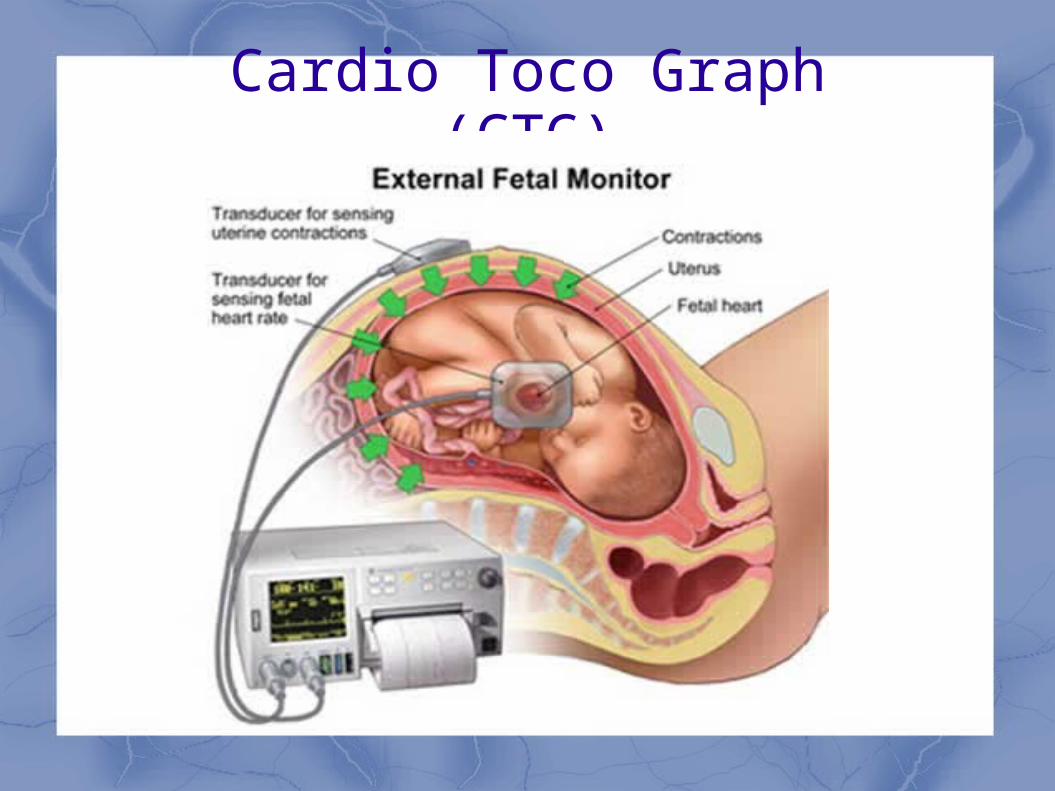
Cardio Toco Graph (CTG)
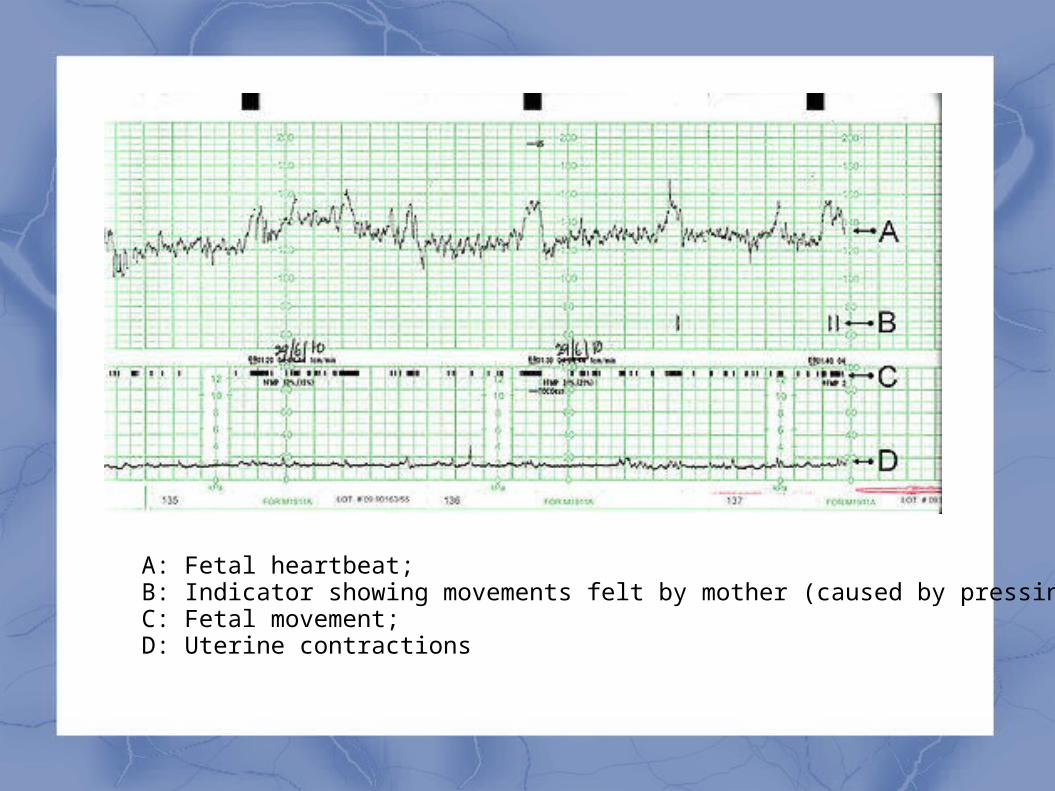
A: Fetal heartbeat; B: Indicator showing movements felt by mother (caused by pressing a button); C: Fetal movement; D: Uterine contractions
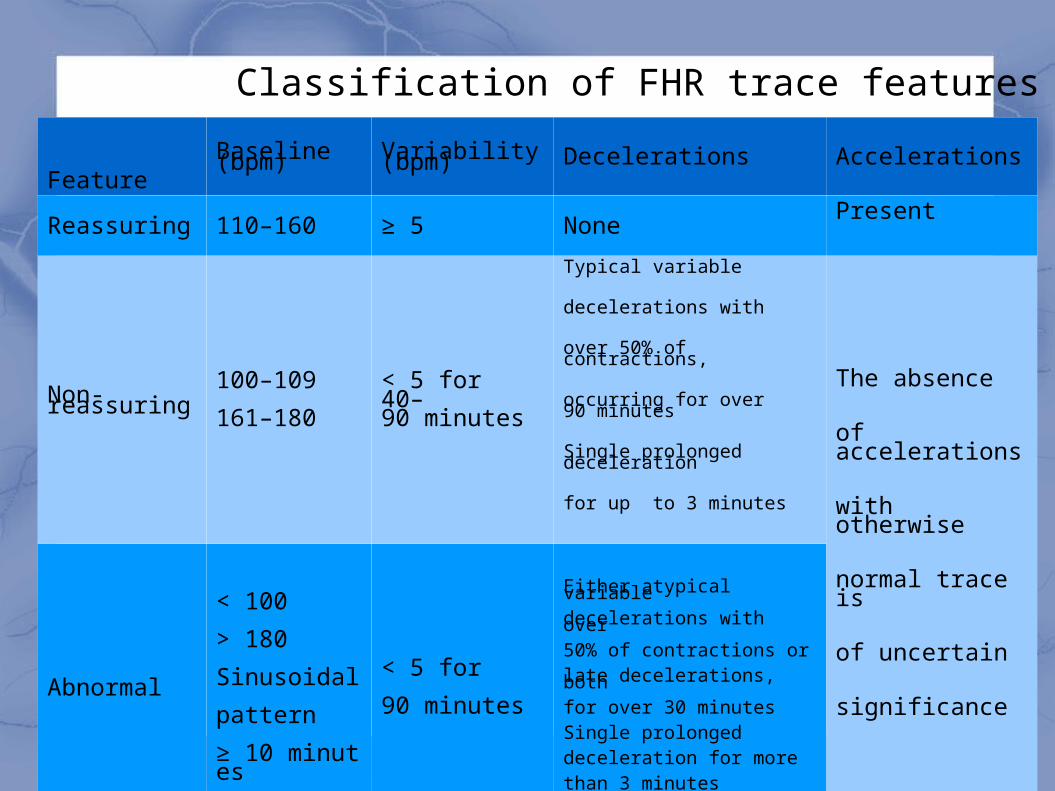
FeatureBaseline (bpm) Variability (bpm) Decelerations Accelerations
Reassuring 110–160 ≥ 5 NonePresent
Non-reassuring100–109
161–180< 5 for 40–90 minutes
Typical variable
decelerations with
over 50% of contractions,
occurring for over 90 minutes
Single prolonged deceleration
for up to 3 minutes
The absence
of accelerations
with otherwise
normal trace is
of uncertain
significanceAbnormal
< 100
> 180
Sinusoidal
pattern
≥ 10 minutes
< 5 for
90 minutes
Either atypical variable decelerations with over 50% of contractions or late decelerations, both for over 30 minutesSingle prolonged deceleration for more than 3 minutes
Classification of FHR trace features
Fetal Blood Sampling
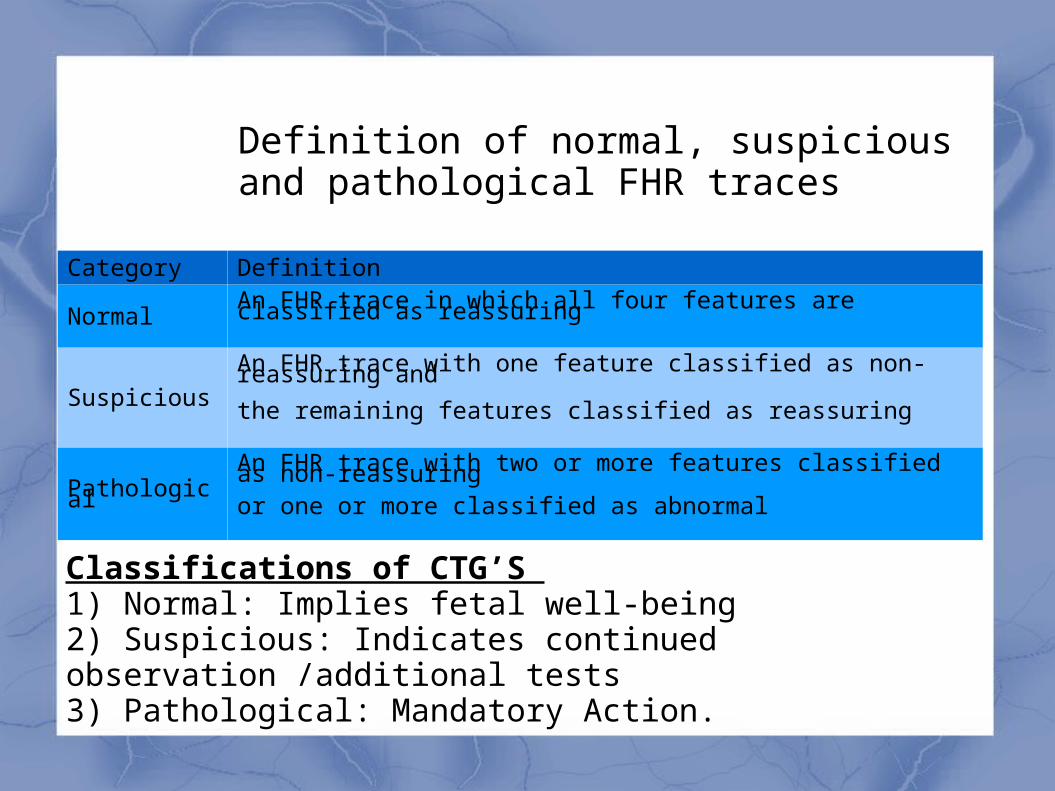
Category Definition
Normal An FHR trace in which all four features are classified as reassuring
SuspiciousAn FHR trace with one feature classified as non-reassuring and
the remaining features classified as reassuring
PathologicalAn FHR trace with two or more features classified as non-reassuring or one or more classified as abnormal
Definition of normal, suspicious and pathological FHR traces
Classifications of CTG’S 1) Normal: Implies fetal well-being 2) Suspicious: Indicates continued observation /additional tests 3) Pathological: Mandatory Action.
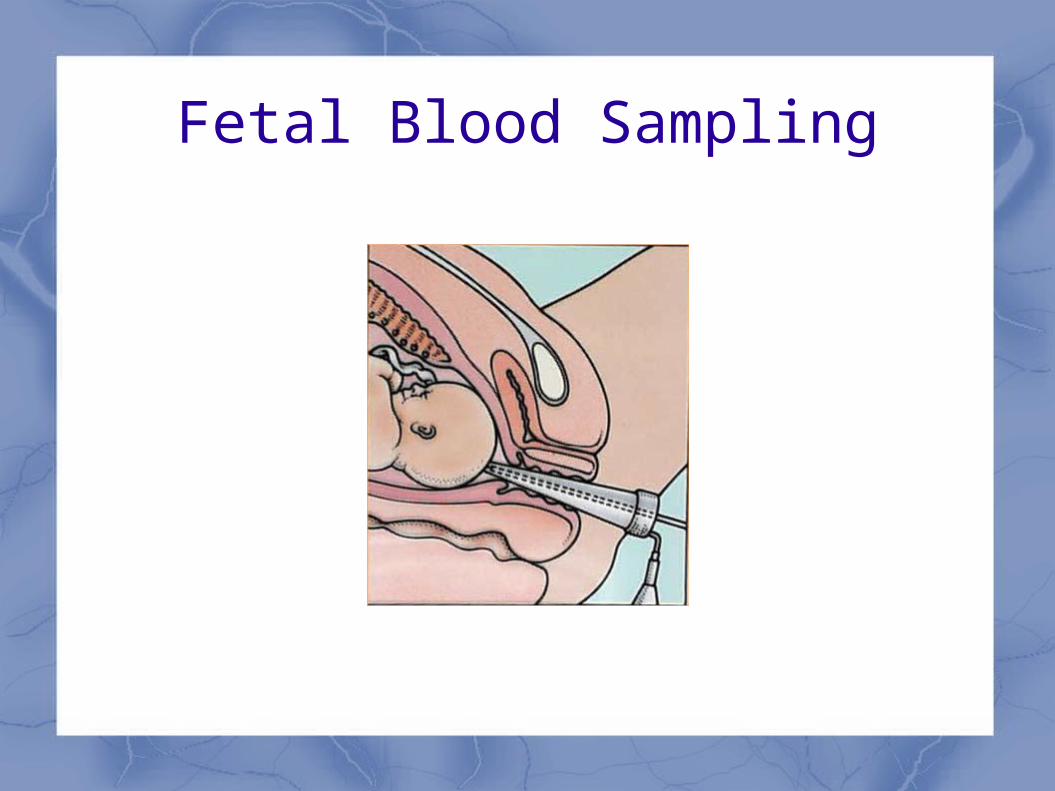
Fetal Blood Sampling
Fetal Blood Sampling
For pathological trace
Must be at least 3-4 cm dilated
pH>7.25: reassuring, but if CTG deteriorates then repeat
pH:7.20-7.25: repeat in 30 minutes or deliver
pH<7.20: deliver
Caesarean Section
• A Caesarean section is a surgical procedure in which an incisions is made in the uterus to deliver one or more babies
• The first modern Caesarean section was performed by German gynaecologist Ferdinand Adolf Kehrer in 1881.