Embed Size (px)
Citation preview
1
MINISTRY OF NATIONAL GUARD
HEALTH AFFAIRS
DEPARTMENT OF PATHOLOGY AND LABORATORY MEDICINE
RECEIVING AND ACC LABORATORY
“Accurate and Precise Laboratory Data Depends on Properly Performed
Phlebotomy to Obtain a High Quality Specimen”
FEBRUARY 2015
Laboratory Specimen
Collection Guidelines
2
TABLE OF CONTENTS
1. INRODUCTION 3
2. OBJECTIVES 3
3 ORDERING OF LABORATORY TEST IN THE HIS (QCPR) 3
4. PATIENT IDENTIFICATION 4
5. PATIENT PREPARATION 5
6. COLLECTION ORDER OF DRAW 8 Figure 1 8
Figure 2 9
7. TYPES OF CONTAINERS 10
8. SPECIMEN COLLECTION POLICIES 11
9. PREPARATION OF PHLEBOTOMY SUPPLIES 12
10. SAFETY PRECAUTIONS AND INFECTION CONTROL PRACTICES 12
11. BLOOD COLLECTION PROCEDURE 13 Figure 1 10
Figure 2 10
Figure 3 10
Figure 4 10
Figure 5 14
Figure 6 14
Figure 7 14
Figure 8 15
Figure 9 15
Figure 10 15
Figure 11 16
12. SPECIAL HANDLING OF SPECIMEN BETWEEN TIME OF COLLECTION
AND TIME RECEIVED BY THE LABORATORY 16
13. PROPER SPECIMEN LABELING 17
14. SAMPLE TRANSPORTATION 18
15. REASONS FOR SPECIMEN REJECTION 19
16. IRRETRIEVABLE SAMPLES 20
17. BODY FLUIDS 20
18. HISTOPATHOLOGY AND CYTOLOGY SAMPLES 21
19. SAMPLE INTEGRITY 22
20. SPECIMEN COLLECTION PRIORITIES AND TURN AROUND TIME 22
21. URINE COLLECTION 22
22. LIST OF URINARY TESTS PERFORMED IN THE LABORATORY 23
23. LABORATORY TEST LIST
IN-HOUSE TESTS 24
Table 1 24
Table 2 27
Table 3 28
Table 4 30
Table 5 30
Table 6 33
Table 7 34
SEND-OUT/REFERRED TESTS 38
24. DEPARTMENT OF PATHOLOGY AND LABORATORY CONTACT
NUMBERS 39
3
1. INTRODUCTION
These guidelines are provided to ensure correct, error-free and safe blood collection. By
understanding and following these instructions, you will be adhering to best practices and
policies of the King Abdulaziz Medical City- Ministry of National Guard Health Affairs.
2. OBJECTIVES
To provide an overview of Phlebotomy in general:
Patient Identification
Specimen Collection Policies
Blood Collection Procedures
Order of Draw
To provide an overview on proper urine collection and storage.
To provide a list of different tests available in the laboratory.
To provide guidelines on the minimum volumes required, tube to be used and
sample requirements for the different tests available in the laboratory.
3. ORDERING OF LABORATORY TESTS IN THE
HOSPITAL INFORMATION SYSTEM (HIS) Physicians are the one’s ordering the laboratory tests of each patient in the
Quadramed (QCPR). All the special areas (ICU’s, ER, CCU, Liver Step-down, Pediatric
Cardiac Step-down) which are NURSE DRAW should be entered as NON-LAB
COLLECT while the regular wards in the hospital (WARDS 1-5, 12-16, 18-25, 29-30,
33-34, 36-16C) which are LAB DRAW should be entered as LAB COLLECT.
***All Laboratory specimens that are sent to the laboratory should have an
entry in the computer system. All nurses should collect in the system all the ordered
tests of the doctor before sending the samples to avoid delay in the processing of the
samples.
4
SAMPLES WITH ACCOMPANYING REQUISITION FORMS
3.1 Specimens to be analyzed for the following test should
have an accompanied requisition form:
3.1.1 All referred tests
*NOTE: List of tests sent to other
laboratories is available on the
Online Help System in the intranet.
3.1.2 Molecular laboratory test
3.1.2.1 Genetic disease tests
3.1.2.2 DNA banking
*NOTE: DNA banking and Genetic tests
should be accompanied by a consent
form signed by the patient or the
patient’s immediate relative and the
requesting Physician.
3.1.3 Virology tests
3.1.3.1 CMV PP65
3.1.3.2 PCR and viral load test
3.1.4 Blood bank tests
3.1.4.1 Type and screen
3.1.4.2 Transfusion reaction
3.1.4.3 Cord blood typing
3.1.4.4 ABO Rh typing
3.1.4.5 DAT blank test
3.1.5 Serology tests
3.1.5.1 Allergy test
3.1.5.2 Aspergillus test
3.1.6 Cytogenetic tests
3.1.6.1 Chromosomal analysis
3.1.6.2 Amniotic fluid analysis
3.1.7 All HLA and Flowcytometry tests
3.1.8 All Histopathology and Cytology tests
NOTE: appropriate clinical date is mandatory for the following
section of the Laboratory - Cytology, Histology, Molecular,
Metabolic Laboratory and Referral-Send out.
5
4. PATIENT IDENTIFICATION
. *NOTE: All patients must be positively identified
before the specimen collection is
performed. 4.3.1 For Inpatients:
4.3.1.1 The two patient identifiers must be present (patient’s name
and patient’s medical record number) on the patient’s wrist band.
4.3.1.2 The patient’s room and bed number may not be used as an
identifier.
4.3.1.3 While checking the wrist band, ask the patient to state his/
her full name or if not possible, the relative of the patient.
4.3.1.4 The patient’s wrist band must match exactly the full name
and the medical record number of the patient on the requisition
forms and all specimen labels.
4.3.2 For Outpatient:
4.3.2.1 While checking the hospital medical card, appointment slip
or Saudi ID and the laboratory requisition form, ask the patient to
state his/ her full name or if not possible, the relative of the patient.
4.3.2.2 The patient’s medical record card, appointment slip or Saudi
D must match exactly the full name and the medical record number
of the patient on the requisition forms and all specimen labels.
4.3.3 Patient Identification for Blood Bank Compatibility Testing
4.3.3.1 For Inpatients:
4.3.3.1.1 The patient identification and sample collection
should be witnessed by a nurse and the badge numbers of the
phlebotomist and the nurse must be documented on the Blood and
Blood Components Requisition Form.
4.3.3.2 For Outpatients:
4.3.3.2.1 The patient identification and sample collection
should be witnessed by another phlebotomist or the team leader
and their badge numbers must be documented on the Blood and
Blood Components Requisition Form.
4.3.3.3 For Clinic 101 patients:
4.3.3.3.1 The patient identification and sample collection
should be witnessed by a nurse and the badge numbers of the
phlebotomist and the nurse must be documented on the Blood and
Blood Components Requisition Form.
5. PATIENT PREPARATION
The phlebotomist should ask the patient if there is any
preparation observed before undergoing a specific laboratory
test such as fasting, diet restrictions and avoidance of certain
6
activities (smoking, strenuous exercise, etc.) that may
compromise the result.
*NOTE: Fasting for blood sugar test should be 8 to 10 hours
while lipid test should be 10 to 12 hours.
The phlebotomist should ask the patient for any allergy to
latex supplies or iodine disinfectants which will be use
during the sample collection.
*NOTE: Use non-latex tourniquet and gloves to patients with
allergy to latex. Use Chlorhexidine swabs as disinfectants for
patients with allergy to iodine for blood culture collection.
Patients should be clearly informed about the proper collection
of 24 hour urine samples. Improperly collected samples yield
inaccurate results.
Instruct the patient to maintain usual amount of liquid intake.
During the collection inform the patient that the urine container
must be placed in a cool environment or in the refrigerator if
possible, to prevent growth of microorganisms and possible
decomposition of urine constituents.
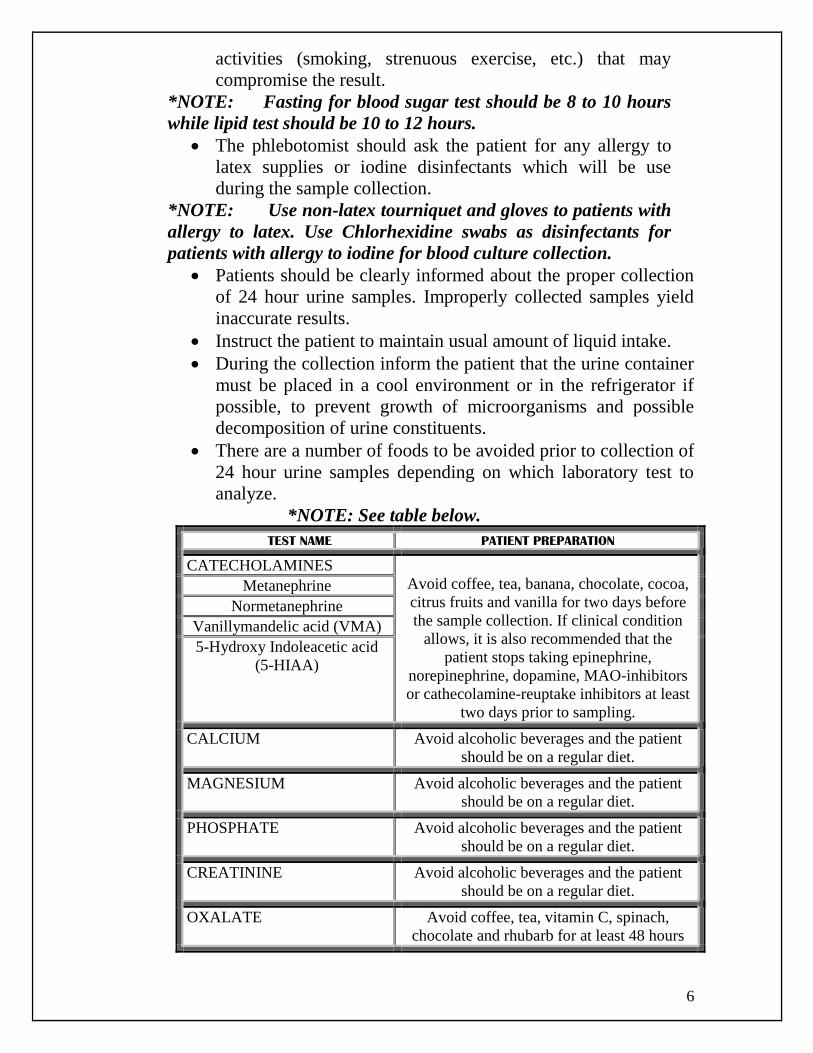
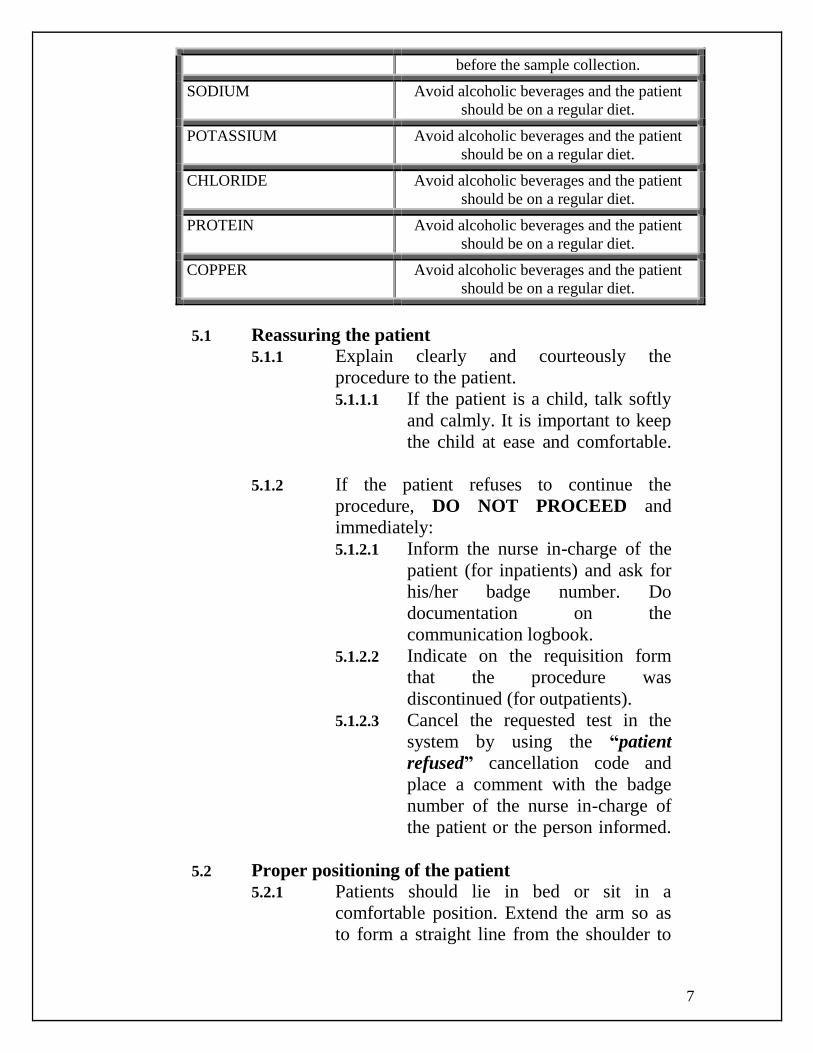
There are a number of foods to be avoided prior to collection of
24 hour urine samples depending on which laboratory test to
analyze.
*NOTE: See table below.
TEST NAME PATIENT PREPARATION
CATECHOLAMINES
Avoid coffee, tea, banana, chocolate, cocoa,
citrus fruits and vanilla for two days before
the sample collection. If clinical condition
allows, it is also recommended that the
patient stops taking epinephrine,
norepinephrine, dopamine, MAO-inhibitors
or cathecolamine-reuptake inhibitors at least
two days prior to sampling.
Metanephrine
Normetanephrine
Vanillymandelic acid (VMA)
5-Hydroxy Indoleacetic acid
(5-HIAA)
CALCIUM Avoid alcoholic beverages and the patient
should be on a regular diet.
MAGNESIUM Avoid alcoholic beverages and the patient
should be on a regular diet.
PHOSPHATE Avoid alcoholic beverages and the patient
should be on a regular diet.
CREATININE Avoid alcoholic beverages and the patient
should be on a regular diet.
OXALATE Avoid coffee, tea, vitamin C, spinach,
chocolate and rhubarb for at least 48 hours
7
before the sample collection.
SODIUM Avoid alcoholic beverages and the patient
should be on a regular diet.
POTASSIUM Avoid alcoholic beverages and the patient
should be on a regular diet.
CHLORIDE Avoid alcoholic beverages and the patient
should be on a regular diet.
PROTEIN Avoid alcoholic beverages and the patient
should be on a regular diet.
COPPER Avoid alcoholic beverages and the patient
should be on a regular diet.
5.1 Reassuring the patient
5.1.1 Explain clearly and courteously the
procedure to the patient.
5.1.1.1 If the patient is a child, talk softly
and calmly. It is important to keep
the child at ease and comfortable.
5.1.2 If the patient refuses to continue the
procedure, DO NOT PROCEED and
immediately:
5.1.2.1 Inform the nurse in-charge of the
patient (for inpatients) and ask for
his/her badge number. Do
documentation on the
communication logbook.
5.1.2.2 Indicate on the requisition form
that the procedure was
discontinued (for outpatients).
5.1.2.3 Cancel the requested test in the
system by using the “patient
refused” cancellation code and
place a comment with the badge
number of the nurse in-charge of
the patient or the person informed.
5.2 Proper positioning of the patient
5.2.1 Patients should lie in bed or sit in a
comfortable position. Extend the arm so as
to form a straight line from the shoulder to
8
wrist. Add support under the arm if
necessary.
5.2.2 Ambulatory or outpatients should sit in a chair
with armrest to protect fainting patients from
fall. Place arm on the table or on the armrest in
a straight line from the shoulder to wrist. The
arm should be slightly bent at the elbow. If
support is needed, ask the patient to form a fist
with the other hand and place it under the
elbow.
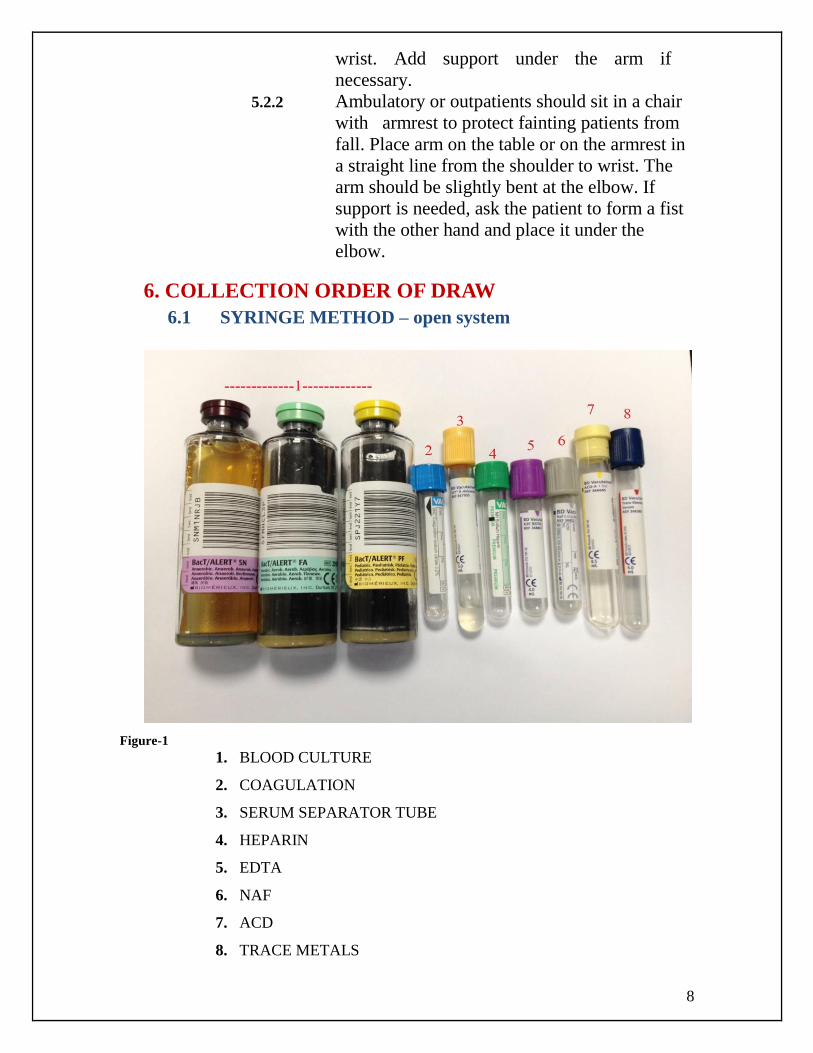
6. COLLECTION ORDER OF DRAW
6.1 SYRINGE METHOD – open system
Figure-1
1. BLOOD CULTURE
2. COAGULATION
3. SERUM SEPARATOR TUBE
4. HEPARIN
5. EDTA
6. NAF
7. ACD
8. TRACE METALS
9
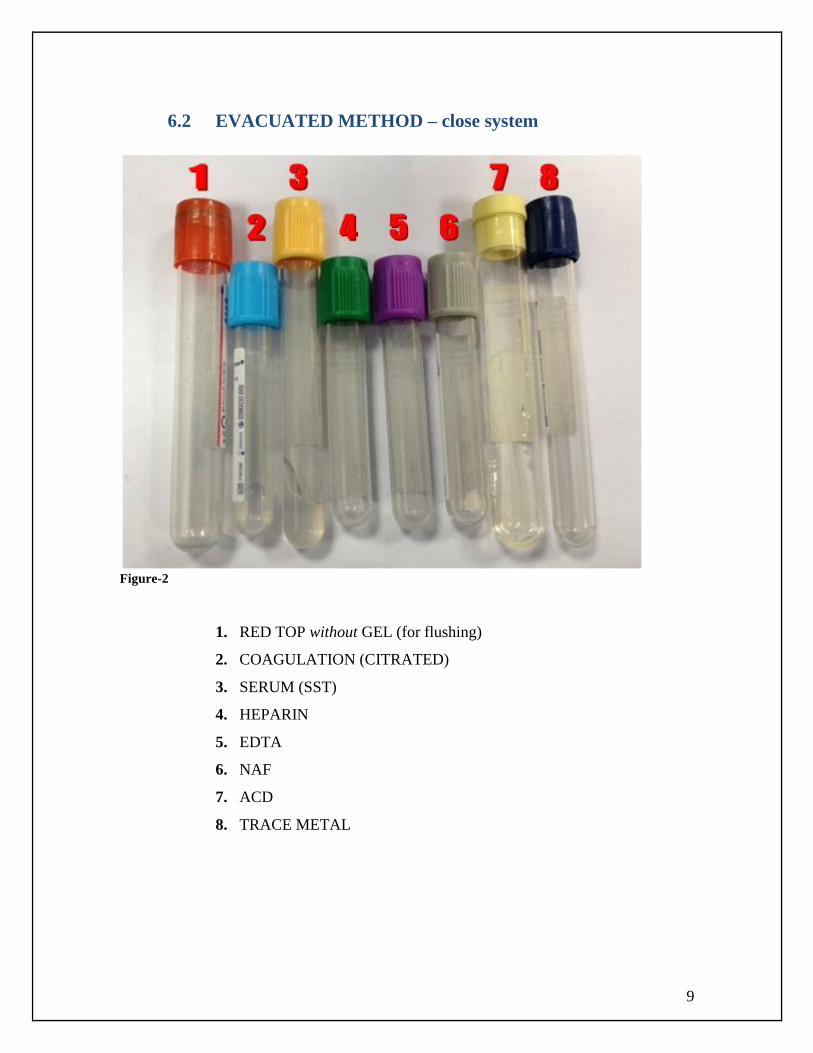
6.2 EVACUATED METHOD – close system
Figure-2
1. RED TOP without GEL (for flushing)
2. COAGULATION (CITRATED)
3. SERUM (SST)
4. HEPARIN
5. EDTA
6. NAF
7. ACD
8. TRACE METAL
10
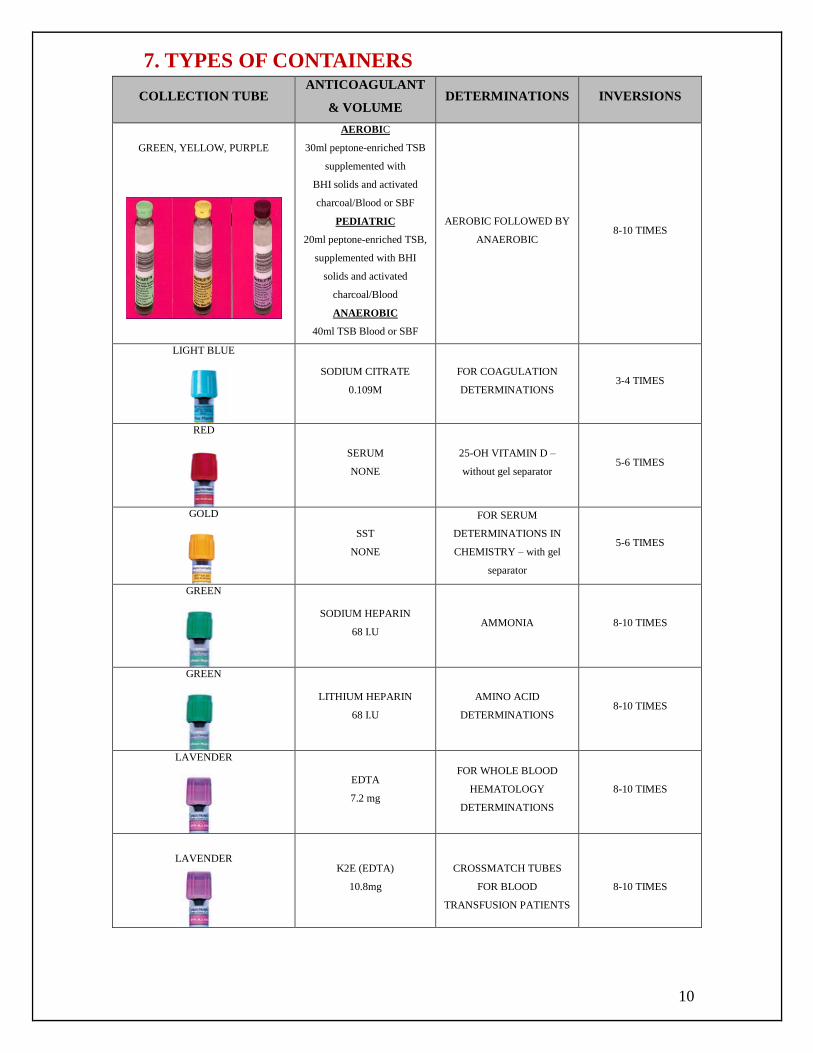
7. TYPES OF CONTAINERS
COLLECTION TUBE ANTICOAGULANT
& VOLUME DETERMINATIONS INVERSIONS
GREEN, YELLOW, PURPLE
AEROBIC
30ml peptone-enriched TSB
supplemented with
BHI solids and activated
charcoal/Blood or SBF
PEDIATRIC
20ml peptone-enriched TSB,
supplemented with BHI
solids and activated
charcoal/Blood
ANAEROBIC
40ml TSB Blood or SBF
AEROBIC FOLLOWED BY
ANAEROBIC 8-10 TIMES
LIGHT BLUE
SODIUM CITRATE
0.109M
FOR COAGULATION
DETERMINATIONS 3-4 TIMES
RED
SERUM
NONE
25-OH VITAMIN D –
without gel separator 5-6 TIMES
GOLD
SST
NONE
FOR SERUM
DETERMINATIONS IN
CHEMISTRY – with gel
separator
5-6 TIMES
GREEN
SODIUM HEPARIN
68 I.U AMMONIA 8-10 TIMES
GREEN
LITHIUM HEPARIN
68 I.U
AMINO ACID
DETERMINATIONS 8-10 TIMES
LAVENDER
EDTA
7.2 mg
FOR WHOLE BLOOD
HEMATOLOGY
DETERMINATIONS
8-10 TIMES
LAVENDER
K2E (EDTA)
10.8mg
CROSSMATCH TUBES
FOR BLOOD
TRANSFUSION PATIENTS
8-10 TIMES
11
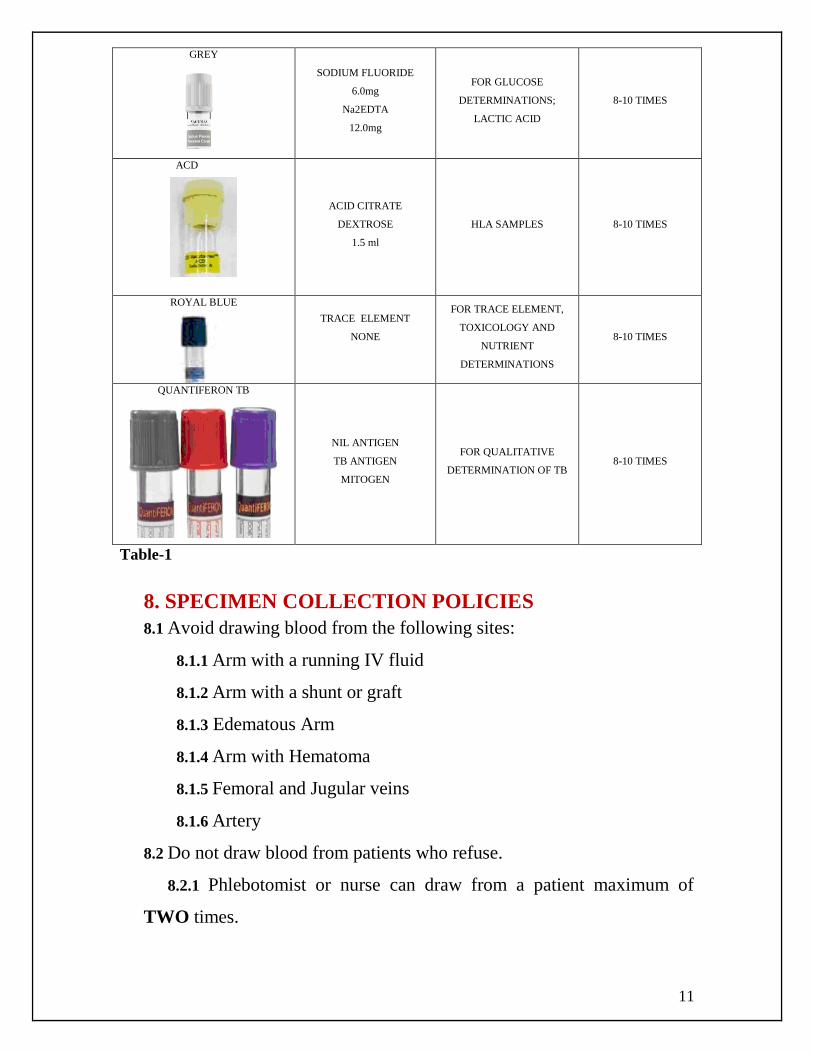
GREY
SODIUM FLUORIDE
6.0mg
Na2EDTA
12.0mg
FOR GLUCOSE
DETERMINATIONS;
LACTIC ACID
8-10 TIMES
ACD
ACID CITRATE
DEXTROSE
1.5 ml
HLA SAMPLES 8-10 TIMES
ROYAL BLUE
TRACE ELEMENT
NONE
FOR TRACE ELEMENT,
TOXICOLOGY AND
NUTRIENT
DETERMINATIONS
8-10 TIMES
QUANTIFERON TB
NIL ANTIGEN
TB ANTIGEN
MITOGEN
FOR QUALITATIVE
DETERMINATION OF TB 8-10 TIMES
Table-1
8. SPECIMEN COLLECTION POLICIES
8.1 Avoid drawing blood from the following sites:
8.1.1 Arm with a running IV fluid
8.1.2 Arm with a shunt or graft
8.1.3 Edematous Arm
8.1.4 Arm with Hematoma
8.1.5 Femoral and Jugular veins
8.1.6 Artery
8.2 Do not draw blood from patients who refuse.
8.2.1 Phlebotomist or nurse can draw from a patient maximum of
TWO times.
12
8.3 Phlebotomist or nurse may draw patients from an on-going blood
transfusion if the doctor/nurse insists due to a necessary blood test. In this
case, get the badge number of the doctor and the nurse in-charge. Inform
also the Receiving Supervisor and the Section that the blood was taken
during the blood transfusion or just indicate in the barcode label.
8.4 All Phlebotomist are only allowed to draw blood from Hardstick
patients in the special areas of the hospital (e. g. ICU's, ER, CCU,
Liver Stepdown, Pediatric Cardiac Stepdown)
AS PER APP: All Employees are not allowed to arrange their own
blood extractions. They should go to Ambulatory Care Center (ACC)
to have their blood draw with the valid hospital card and request
form from the Employee Health Clinic or from the other clinics.
9. PREPARATION OF PHLEBOTOMY SUPPLIES
9.1 Non-sterile gloves
9.2 Chlorhexidine Gluconate scrub or Povidone
Prep (2 months old), for blood culture
collection.
9.3 Alcohol Prep pad
9.4 Gauze
9.5 Disposable Tourniquet
9.6 Evacuated collection tubes
9.7 Evacuated tube holder
9.8 Band aids, tapes or pressure bandages
10. SAFETY PRECAUTIONS AND INFECTION
CONTROL PRACTICES
10.1 Treat all samples as potentially infectious
10.2 Perform hand hygiene (hand washing or using hand sanitizer)
before and after patient contact.
10.3 Change gloves between each patient.
10.4 Discard the disposable tourniquet after each blood collection.
10.5 Never take venipuncture trays inside the isolation rooms.
10.6 Do not use latex gloves and tourniquets to patients with allergy
to latex.

13
11. BLOOD COLLECTION PROCEDURE
11.1 Perform Hand Hygiene (Figure-1) & (Figure-2).
Figure-2
11.2 Put on gloves (Figure-3).
Figure-3
11.3 Apply tourniquet 3-4 inches above venipuncture site (Figure-4).
* Never leave the tourniquet longer than 1 minute.
Figure-4
Figure-1
14
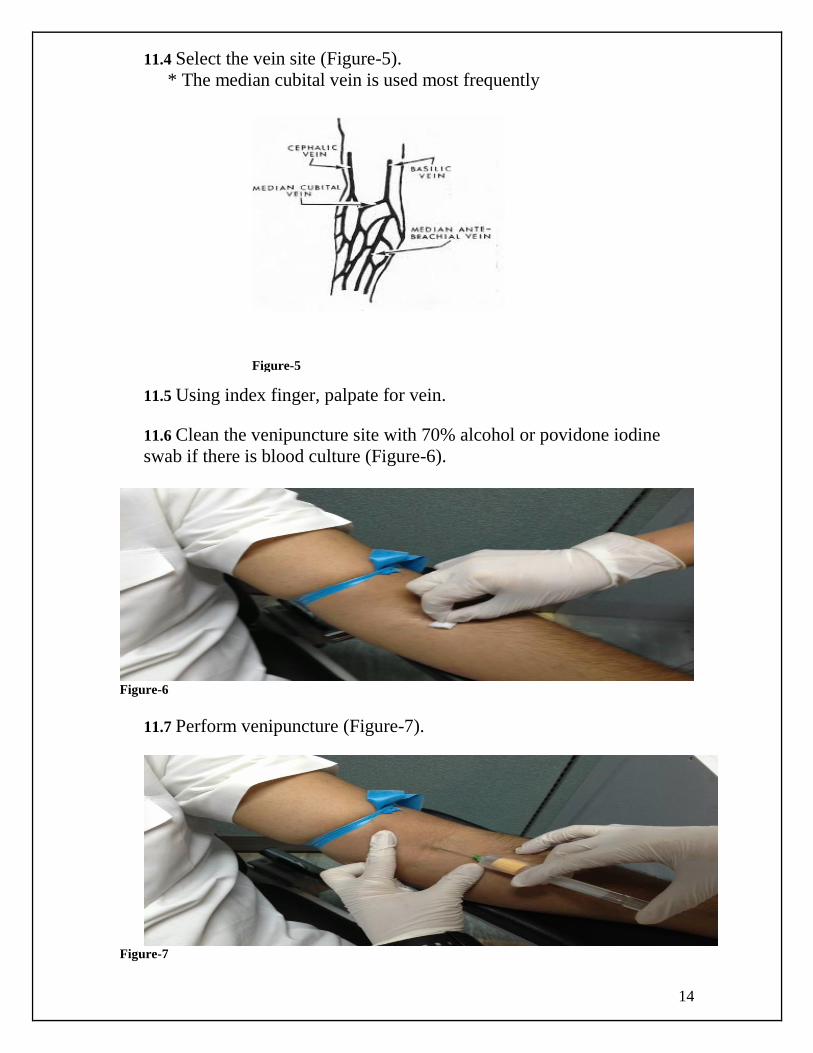
11.4 Select the vein site (Figure-5).
* The median cubital vein is used most frequently
11.5 Using index finger, palpate for vein.
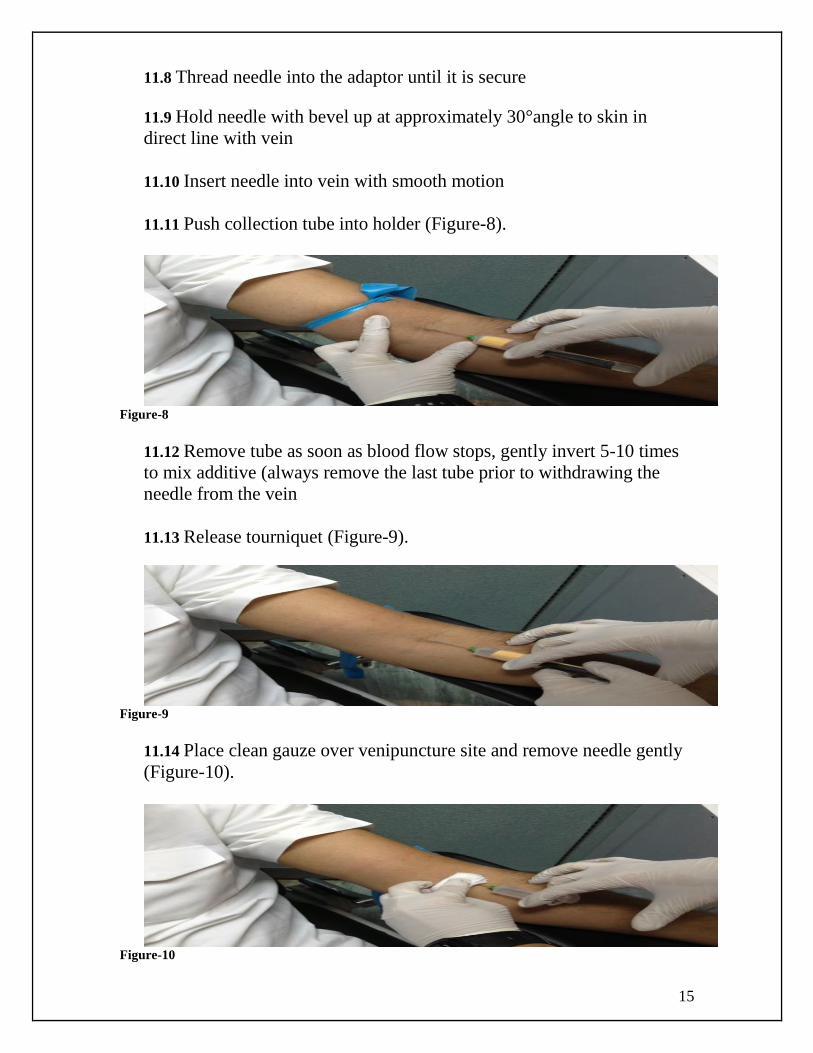
11.6 Clean the venipuncture site with 70% alcohol or povidone iodine
swab if there is blood culture (Figure-6).
Figure-6
11.7 Perform venipuncture (Figure-7).
Figure-7
Figure-5
15
11.8 Thread needle into the adaptor until it is secure
11.9 Hold needle with bevel up at approximately 30°angle to skin in
direct line with vein
11.10 Insert needle into vein with smooth motion
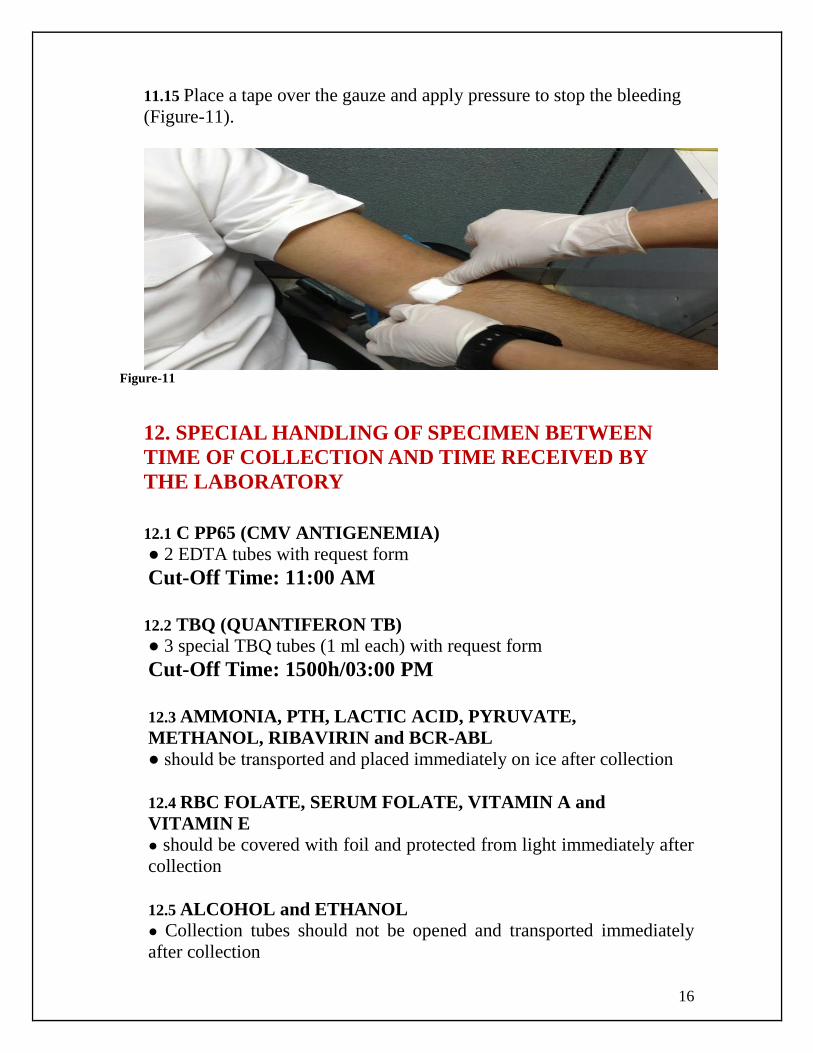
11.11 Push collection tube into holder (Figure-8).
Figure-8
11.12 Remove tube as soon as blood flow stops, gently invert 5-10 times
to mix additive (always remove the last tube prior to withdrawing the
needle from the vein
11.13 Release tourniquet (Figure-9).
Figure-9
11.14 Place clean gauze over venipuncture site and remove needle gently
(Figure-10).
Figure-10
16
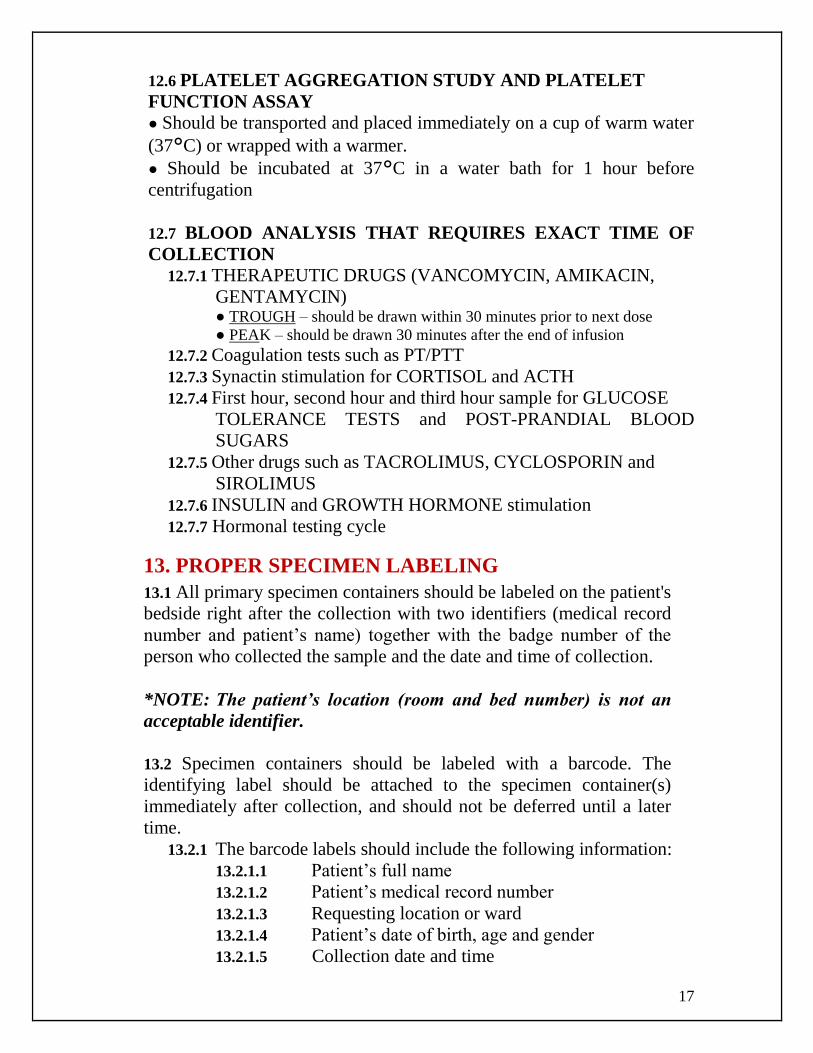
11.15 Place a tape over the gauze and apply pressure to stop the bleeding
(Figure-11).
Figure-11
12. SPECIAL HANDLING OF SPECIMEN BETWEEN
TIME OF COLLECTION AND TIME RECEIVED BY
THE LABORATORY
12.1 C PP65 (CMV ANTIGENEMIA)
● 2 EDTA tubes with request form
Cut-Off Time: 11:00 AM
12.2 TBQ (QUANTIFERON TB)
● 3 special TBQ tubes (1 ml each) with request form
Cut-Off Time: 1500h/03:00 PM
12.3 AMMONIA, PTH, LACTIC ACID, PYRUVATE,
METHANOL, RIBAVIRIN and BCR-ABL
● should be transported and placed immediately on ice after collection
12.4 RBC FOLATE, SERUM FOLATE, VITAMIN A and
VITAMIN E
● should be covered with foil and protected from light immediately after
collection
12.5 ALCOHOL and ETHANOL
● Collection tubes should not be opened and transported immediately
after collection
17
12.6 PLATELET AGGREGATION STUDY AND PLATELET
FUNCTION ASSAY
● Should be transported and placed immediately on a cup of warm water
(37°C) or wrapped with a warmer.
● Should be incubated at 37°C in a water bath for 1 hour before
centrifugation
12.7 BLOOD ANALYSIS THAT REQUIRES EXACT TIME OF
COLLECTION
12.7.1 THERAPEUTIC DRUGS (VANCOMYCIN, AMIKACIN,
GENTAMYCIN) ● TROUGH – should be drawn within 30 minutes prior to next dose
● PEAK – should be drawn 30 minutes after the end of infusion
12.7.2 Coagulation tests such as PT/PTT
12.7.3 Synactin stimulation for CORTISOL and ACTH
12.7.4 First hour, second hour and third hour sample for GLUCOSE
TOLERANCE TESTS and POST-PRANDIAL BLOOD
SUGARS
12.7.5 Other drugs such as TACROLIMUS, CYCLOSPORIN and
SIROLIMUS
12.7.6 INSULIN and GROWTH HORMONE stimulation
12.7.7 Hormonal testing cycle
13. PROPER SPECIMEN LABELING
13.1 All primary specimen containers should be labeled on the patient's
bedside right after the collection with two identifiers (medical record
number and patient’s name) together with the badge number of the
person who collected the sample and the date and time of collection.
*NOTE: The patient’s location (room and bed number) is not an
acceptable identifier.
13.2 Specimen containers should be labeled with a barcode. The
identifying label should be attached to the specimen container(s)
immediately after collection, and should not be deferred until a later
time.
13.2.1 The barcode labels should include the following information:
13.2.1.1 Patient’s full name
13.2.1.2 Patient’s medical record number
13.2.1.3 Requesting location or ward
13.2.1.4 Patient’s date of birth, age and gender
13.2.1.5 Collection date and time
18
13.2.1.6 Collection priority status
13.2.1.7 Sample’s accession number
13.2.1.8 Test name
13.3 Check the name on each label to verify again that the name on the
tube matches the barcode label.
13.4 The badge number of the person labeling the sample should be
written on the barcode label.
13.5 Labeling of samples for Blood bank Compatibility Testing
13.5.1 The specimen container should be labeled handwritten on the
patient's bedside right after the collection with two identifiers
(medical record number and patient’s full name) together with the
badge number of the person who collected the sample and the date
and time of collection.
13.5.2 A barcode label containing the same patient information with
the badge number of the person labeling the sample is then affixed
to the specimen container.
13.5.3 Cord blood samples submitted to the laboratory should be
labeled with an addressograph on the patient's bedside right after
the collection containing the two identifiers (medical record
number and patient’s name) together with the mother’s medical
record number and name, badge number of the person who
collected the sample and the date and time of collection.
13.6 Labeling of samples for HLA Compatibility testing
13.6.1 The specimen container should be labeled handwritten on the
patient's bedside right after the collection with two identifiers
(medical record number and the patient’s three names) together
with the badge number of the person who collected the sample and
the date and time of collection.
13.6.2 A barcode label containing the same patient information with
the badge number of the person labeling the sample is then affixed
to the specimen container.
14. SAMPLE TRANSPORTATION
There are TWO ways of sample transportation in the hospital:
Handheld
Pneumatic System
WHAT ARE THE SAMPLES THAT CAN BE SENT THRU THE
CAPSULE (PNEUMATIC SYSTEM)?
14.1 The following are laboratory specimens that CAN be sent via the
pneumatic tube system:
19
14.1.1 Blood specimens in evacuated containers
14.1.2 Urine and stool specimens in small plastic containers
14.1.3 All culture swabs for Microbiology
14.1.4 Blood culture bottles
14.2 The following are laboratory specimens that CANNOT be sent via
the pneumatic tube system:
14.2.1 H1N1 swabs and other highly infectious samples
14.2.2 Blood specimens for TYPE and SCREEN (ABORH), DAT
BLANK and TRANSFUSION REACTION
14.2.3 Histopathology samples
14.2.4 Pap’s smear
14.2.5 Body Fluids (CSF, Ascitic, Pleural, Peritoneal, Synovial)
14.2.6 MERS-COV samples (swab, sputum, tracheal aspirate, blood)
14.2.7 Blood samples for platelet aggregation and platelet function test
15. REASONS FOR SPECIMEN REJECTION
15.1 Unlabeled specimens
15.2 Mislabeled specimens
15.3 Clotted sample
15.4 QNS (Quantity not sufficient)
15.5 Wrong transportation (ex. not transported with ice)
15.6 Spilled sample
15.7 Wrong sample
15.8 Wrong tube/container
15.9 Improperly filled request form
Note: All submitted request form should be properly filled up by the
nurses/physicians. It should contain the following:
15.9.1 Physicians badge and beeper number
15.9.2 Date and Time of collection
15.9.3 Collector’s Badge number
20
15.9.4 Diagnosis
15.9.5 Type of Specimen
16. IRRETRIEVABLE SAMPLES
These are samples that are difficult to re-collect, hence should be
taken carefully before sending to the laboratory.
1. BODY FLUIDS (CSF, ASCITIC, PLEURAL, SYNOVIAL, PERITONEAL, etc.)
2. HISTOPATHOLOGY SAMPLES (TISSUES)
3. PAP’S SMEAR
4. CORD BLOOD
A Corrective Sample Form (for IRRETRIEVABLE samples)
should be filled in by the nurse-in-charge before re-labeling any
unlabeled or mislabeled irretrievable samples.
17. BODY FLUIDS
Body Fluids are pleural, pericardial, ascitic, peritoneal cavities and
synovial joints. Samples are obtained by authorized physician of the
patient.
COLLECTION CONTAINERS:
Sterile containers or sterile plain tubes for CSF and other fluid
examinations except synovial fluid cell count.
Synovial fluids for cell count should be anticoagulated in EDTA tube
or HEPARIN tube.
NOTE: In order to avoid delaying the process and/ or contaminating
the specimens please submit 3 separate samples containing 2-3ml of
each fluid.
21
18. HISTOPATHOLOGY AND CYTOLOGY SAMPLES
● REQUIRED LABORATORY REQUISITION FORMS
18.1 Surgical Pathology Request Form
18.1.1 Fresh tissue samples for frozen sections
18.1.2 Tissue samples for biopsy
18.2 Non-Gynecological Cytology Request Form
18.2.1 Fluid cytology
18.3 Gynecological Cytology Request Form
18.3.1 Pap smear
● COLLECTION OF SPECIMENS
18.4 Samples are obtained by authorized physician of the
patient.
18.5 Specimens collected from multiple sites should be collected in
separate vials/slides with the specimen source identified.
● COLLECTION CONTAINERS
18.6 Fluid samples for non-gynecological cytology are collected in
sterile containers.
18.7 Gynecological samples are collected in Pap smear containers
with prepared fixatives.
18.8 Fresh tissue samples for frozen sections are collected in a
sterile container.
18.9 Tissue samples for biopsy are collected in sterile containers
with prepared concentration of formalin.
● SPECIMEN LABELING GUIDELINES
18.10 Specimen containers should be labeled immediately after
collection with the two identifiers (medical record number and
patient’s name) together with the badge number of the physician
who collected the sample, date and time of collection and the type of
specimen collected
All samples for Histopathology and Cytology must be submitted directly to
the reception area of Histopathology and Cytology during working hours
0800-1700 weekdays (Sunday- Thursday). After 1700 and during
weekends (Friday – Saturday), samples must be submitted to the Receiving
Laboratory.
22
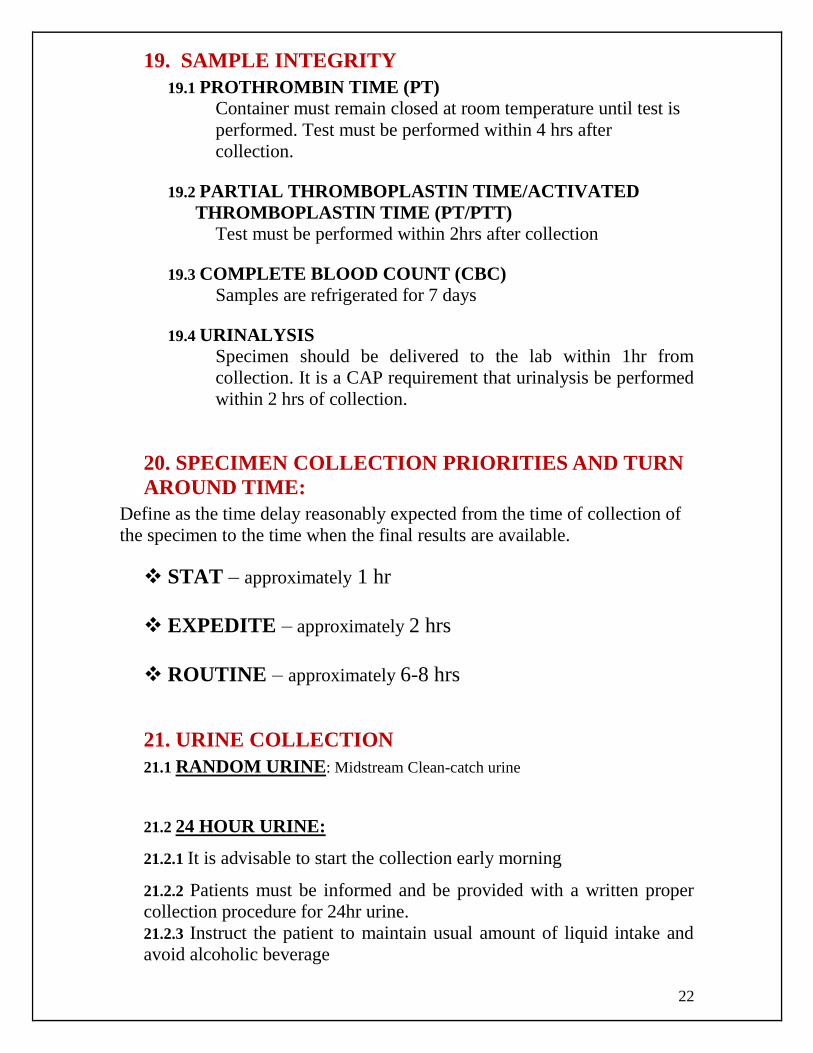
19. SAMPLE INTEGRITY
19.1 PROTHROMBIN TIME (PT)
Container must remain closed at room temperature until test is
performed. Test must be performed within 4 hrs after
collection.
19.2 PARTIAL THROMBOPLASTIN TIME/ACTIVATED
THROMBOPLASTIN TIME (PT/PTT)
Test must be performed within 2hrs after collection
19.3 COMPLETE BLOOD COUNT (CBC)
Samples are refrigerated for 7 days
19.4 URINALYSIS Specimen should be delivered to the lab within 1hr from
collection. It is a CAP requirement that urinalysis be performed
within 2 hrs of collection.
20. SPECIMEN COLLECTION PRIORITIES AND TURN
AROUND TIME:
Define as the time delay reasonably expected from the time of collection of
the specimen to the time when the final results are available.
STAT – approximately 1 hr
EXPEDITE – approximately 2 hrs
ROUTINE – approximately 6-8 hrs
21. URINE COLLECTION
21.1 RANDOM URINE: Midstream Clean-catch urine
21.2 24 HOUR URINE:
21.2.1 It is advisable to start the collection early morning
21.2.2 Patients must be informed and be provided with a written proper
collection procedure for 24hr urine.
21.2.3 Instruct the patient to maintain usual amount of liquid intake and
avoid alcoholic beverage
23
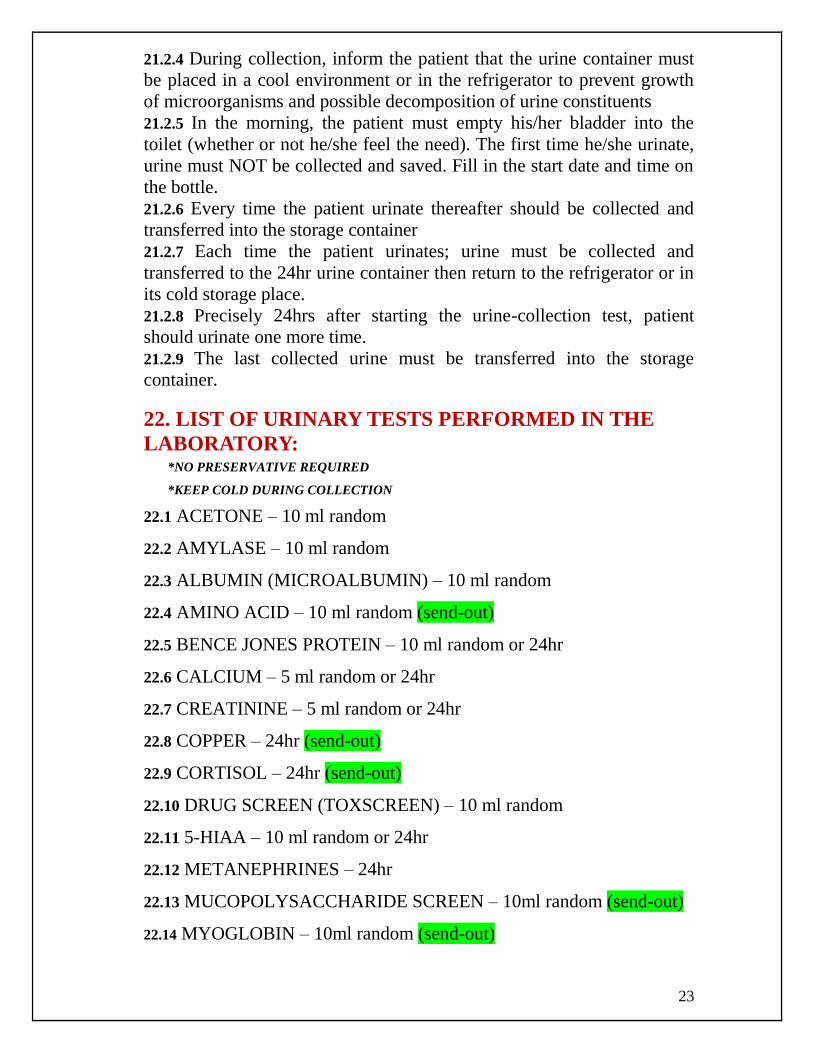
21.2.4 During collection, inform the patient that the urine container must
be placed in a cool environment or in the refrigerator to prevent growth
of microorganisms and possible decomposition of urine constituents
21.2.5 In the morning, the patient must empty his/her bladder into the
toilet (whether or not he/she feel the need). The first time he/she urinate,
urine must NOT be collected and saved. Fill in the start date and time on
the bottle.
21.2.6 Every time the patient urinate thereafter should be collected and
transferred into the storage container
21.2.7 Each time the patient urinates; urine must be collected and
transferred to the 24hr urine container then return to the refrigerator or in
its cold storage place.
21.2.8 Precisely 24hrs after starting the urine-collection test, patient
should urinate one more time.
21.2.9 The last collected urine must be transferred into the storage
container.
22. LIST OF URINARY TESTS PERFORMED IN THE
LABORATORY: *NO PRESERVATIVE REQUIRED
*KEEP COLD DURING COLLECTION
22.1 ACETONE – 10 ml random
22.2 AMYLASE – 10 ml random
22.3 ALBUMIN (MICROALBUMIN) – 10 ml random
22.4 AMINO ACID – 10 ml random (send-out)
22.5 BENCE JONES PROTEIN – 10 ml random or 24hr
22.6 CALCIUM – 5 ml random or 24hr
22.7 CREATININE – 5 ml random or 24hr
22.8 COPPER – 24hr (send-out)
22.9 CORTISOL – 24hr (send-out)
22.10 DRUG SCREEN (TOXSCREEN) – 10 ml random
22.11 5-HIAA – 10 ml random or 24hr
22.12 METANEPHRINES – 24hr
22.13 MUCOPOLYSACCHARIDE SCREEN – 10ml random (send-out)
22.14 MYOGLOBIN – 10ml random (send-out)
24
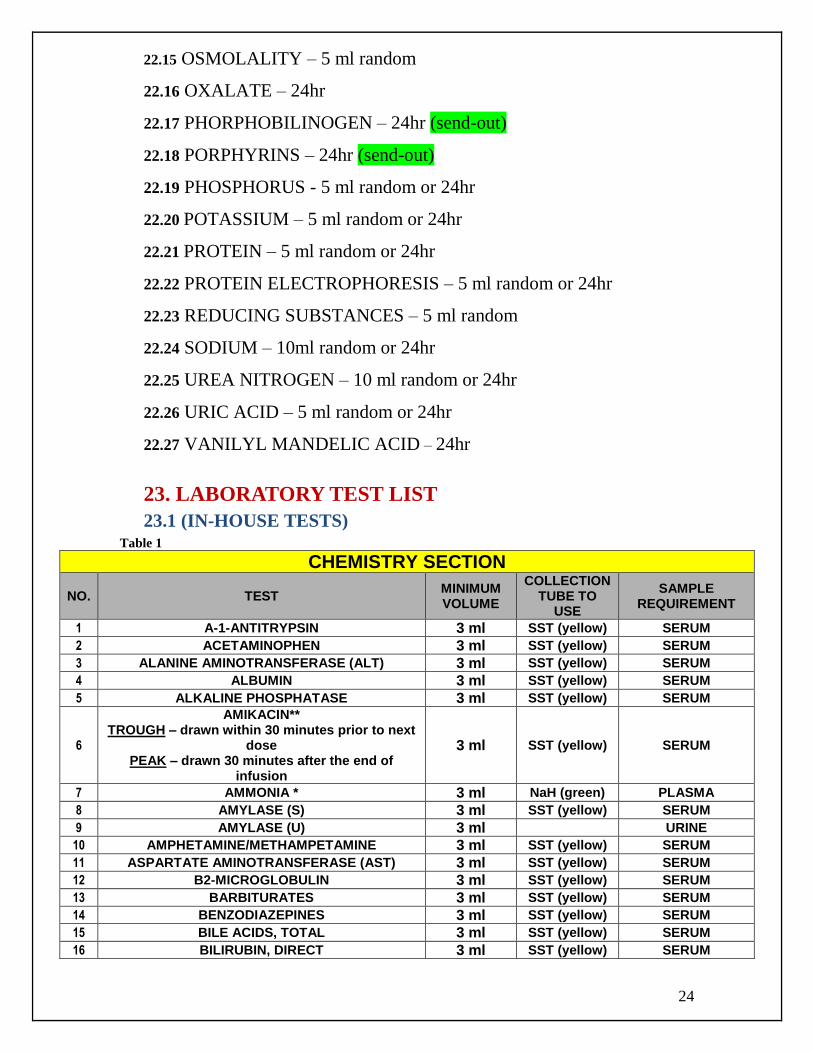
22.15 OSMOLALITY – 5 ml random
22.16 OXALATE – 24hr
22.17 PHORPHOBILINOGEN – 24hr (send-out)
22.18 PORPHYRINS – 24hr (send-out)
22.19 PHOSPHORUS - 5 ml random or 24hr
22.20 POTASSIUM – 5 ml random or 24hr
22.21 PROTEIN – 5 ml random or 24hr
22.22 PROTEIN ELECTROPHORESIS – 5 ml random or 24hr
22.23 REDUCING SUBSTANCES – 5 ml random
22.24 SODIUM – 10ml random or 24hr
22.25 UREA NITROGEN – 10 ml random or 24hr
22.26 URIC ACID – 5 ml random or 24hr
22.27 VANILYL MANDELIC ACID – 24hr
23. LABORATORY TEST LIST
23.1 (IN-HOUSE TESTS) Table 1
CHEMISTRY SECTION
NO. TEST MINIMUM VOLUME
COLLECTION TUBE TO
USE
SAMPLE REQUIREMENT
1 A-1-ANTITRYPSIN 3 ml SST (yellow) SERUM
2 ACETAMINOPHEN 3 ml SST (yellow) SERUM
3 ALANINE AMINOTRANSFERASE (ALT) 3 ml SST (yellow) SERUM
4 ALBUMIN 3 ml SST (yellow) SERUM
5 ALKALINE PHOSPHATASE 3 ml SST (yellow) SERUM
6
AMIKACIN** TROUGH – drawn within 30 minutes prior to next
dose PEAK – drawn 30 minutes after the end of
infusion
3 ml SST (yellow) SERUM
7 AMMONIA * 3 ml NaH (green) PLASMA
8 AMYLASE (S) 3 ml SST (yellow) SERUM
9 AMYLASE (U) 3 ml URINE
10 AMPHETAMINE/METHAMPETAMINE 3 ml SST (yellow) SERUM
11 ASPARTATE AMINOTRANSFERASE (AST) 3 ml SST (yellow) SERUM
12 B2-MICROGLOBULIN 3 ml SST (yellow) SERUM
13 BARBITURATES 3 ml SST (yellow) SERUM
14 BENZODIAZEPINES 3 ml SST (yellow) SERUM
15 BILE ACIDS, TOTAL 3 ml SST (yellow) SERUM
16 BILIRUBIN, DIRECT 3 ml SST (yellow) SERUM
25
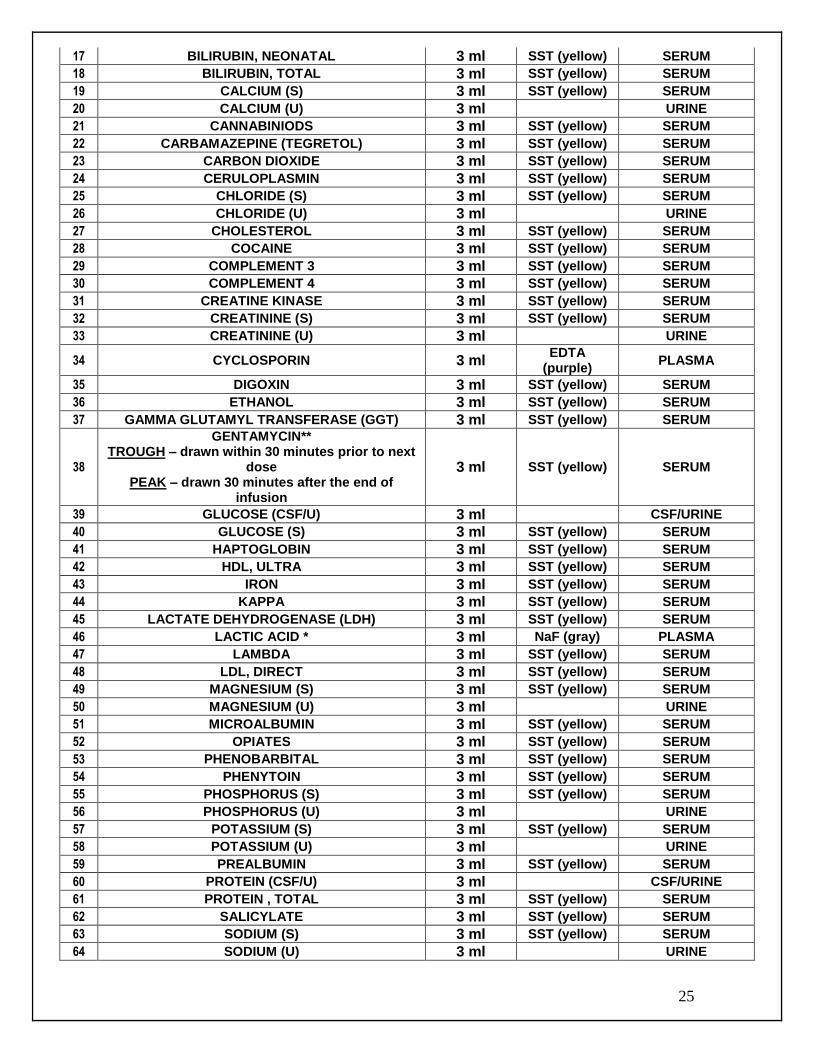
17 BILIRUBIN, NEONATAL 3 ml SST (yellow) SERUM
18 BILIRUBIN, TOTAL 3 ml SST (yellow) SERUM
19 CALCIUM (S) 3 ml SST (yellow) SERUM
20 CALCIUM (U) 3 ml URINE
21 CANNABINIODS 3 ml SST (yellow) SERUM
22 CARBAMAZEPINE (TEGRETOL) 3 ml SST (yellow) SERUM
23 CARBON DIOXIDE 3 ml SST (yellow) SERUM
24 CERULOPLASMIN 3 ml SST (yellow) SERUM
25 CHLORIDE (S) 3 ml SST (yellow) SERUM
26 CHLORIDE (U) 3 ml URINE
27 CHOLESTEROL 3 ml SST (yellow) SERUM
28 COCAINE 3 ml SST (yellow) SERUM
29 COMPLEMENT 3 3 ml SST (yellow) SERUM
30 COMPLEMENT 4 3 ml SST (yellow) SERUM
31 CREATINE KINASE 3 ml SST (yellow) SERUM
32 CREATININE (S) 3 ml SST (yellow) SERUM
33 CREATININE (U) 3 ml URINE
34 CYCLOSPORIN 3 ml EDTA
(purple) PLASMA
35 DIGOXIN 3 ml SST (yellow) SERUM
36 ETHANOL 3 ml SST (yellow) SERUM
37 GAMMA GLUTAMYL TRANSFERASE (GGT) 3 ml SST (yellow) SERUM
38
GENTAMYCIN** TROUGH – drawn within 30 minutes prior to next
dose PEAK – drawn 30 minutes after the end of
infusion
3 ml SST (yellow) SERUM
39 GLUCOSE (CSF/U) 3 ml CSF/URINE
40 GLUCOSE (S) 3 ml SST (yellow) SERUM
41 HAPTOGLOBIN 3 ml SST (yellow) SERUM
42 HDL, ULTRA 3 ml SST (yellow) SERUM
43 IRON 3 ml SST (yellow) SERUM
44 KAPPA 3 ml SST (yellow) SERUM
45 LACTATE DEHYDROGENASE (LDH) 3 ml SST (yellow) SERUM
46 LACTIC ACID * 3 ml NaF (gray) PLASMA
47 LAMBDA 3 ml SST (yellow) SERUM
48 LDL, DIRECT 3 ml SST (yellow) SERUM
49 MAGNESIUM (S) 3 ml SST (yellow) SERUM
50 MAGNESIUM (U) 3 ml URINE
51 MICROALBUMIN 3 ml SST (yellow) SERUM
52 OPIATES 3 ml SST (yellow) SERUM
53 PHENOBARBITAL 3 ml SST (yellow) SERUM
54 PHENYTOIN 3 ml SST (yellow) SERUM
55 PHOSPHORUS (S) 3 ml SST (yellow) SERUM
56 PHOSPHORUS (U) 3 ml URINE
57 POTASSIUM (S) 3 ml SST (yellow) SERUM
58 POTASSIUM (U) 3 ml URINE
59 PREALBUMIN 3 ml SST (yellow) SERUM
60 PROTEIN (CSF/U) 3 ml CSF/URINE
61 PROTEIN , TOTAL 3 ml SST (yellow) SERUM
62 SALICYLATE 3 ml SST (yellow) SERUM
63 SODIUM (S) 3 ml SST (yellow) SERUM
64 SODIUM (U) 3 ml URINE
26
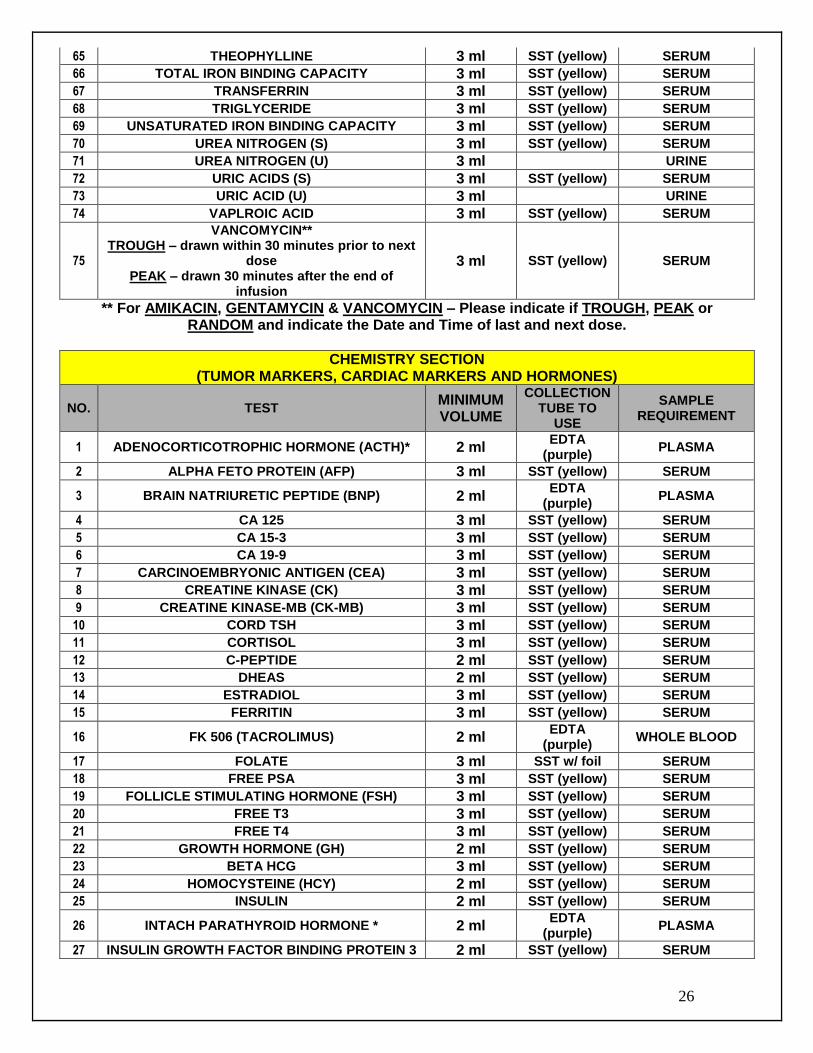
65 THEOPHYLLINE 3 ml SST (yellow) SERUM
66 TOTAL IRON BINDING CAPACITY 3 ml SST (yellow) SERUM
67 TRANSFERRIN 3 ml SST (yellow) SERUM
68 TRIGLYCERIDE 3 ml SST (yellow) SERUM
69 UNSATURATED IRON BINDING CAPACITY 3 ml SST (yellow) SERUM
70 UREA NITROGEN (S) 3 ml SST (yellow) SERUM
71 UREA NITROGEN (U) 3 ml URINE
72 URIC ACIDS (S) 3 ml SST (yellow) SERUM
73 URIC ACID (U) 3 ml URINE
74 VAPLROIC ACID 3 ml SST (yellow) SERUM
75
VANCOMYCIN** TROUGH – drawn within 30 minutes prior to next
dose PEAK – drawn 30 minutes after the end of
infusion
3 ml SST (yellow) SERUM
** For AMIKACIN, GENTAMYCIN & VANCOMYCIN – Please indicate if TROUGH, PEAK or RANDOM and indicate the Date and Time of last and next dose.
CHEMISTRY SECTION (TUMOR MARKERS, CARDIAC MARKERS AND HORMONES)
NO. TEST MINIMUM VOLUME
COLLECTION TUBE TO
USE
SAMPLE REQUIREMENT
1 ADENOCORTICOTROPHIC HORMONE (ACTH)* 2 ml EDTA
(purple) PLASMA
2 ALPHA FETO PROTEIN (AFP) 3 ml SST (yellow) SERUM
3 BRAIN NATRIURETIC PEPTIDE (BNP) 2 ml EDTA
(purple) PLASMA
4 CA 125 3 ml SST (yellow) SERUM
5 CA 15-3 3 ml SST (yellow) SERUM
6 CA 19-9 3 ml SST (yellow) SERUM
7 CARCINOEMBRYONIC ANTIGEN (CEA) 3 ml SST (yellow) SERUM
8 CREATINE KINASE (CK) 3 ml SST (yellow) SERUM
9 CREATINE KINASE-MB (CK-MB) 3 ml SST (yellow) SERUM
10 CORD TSH 3 ml SST (yellow) SERUM
11 CORTISOL 3 ml SST (yellow) SERUM
12 C-PEPTIDE 2 ml SST (yellow) SERUM
13 DHEAS 2 ml SST (yellow) SERUM
14 ESTRADIOL 3 ml SST (yellow) SERUM
15 FERRITIN 3 ml SST (yellow) SERUM
16 FK 506 (TACROLIMUS) 2 ml EDTA
(purple) WHOLE BLOOD
17 FOLATE 3 ml SST w/ foil SERUM
18 FREE PSA 3 ml SST (yellow) SERUM
19 FOLLICLE STIMULATING HORMONE (FSH) 3 ml SST (yellow) SERUM
20 FREE T3 3 ml SST (yellow) SERUM
21 FREE T4 3 ml SST (yellow) SERUM
22 GROWTH HORMONE (GH) 2 ml SST (yellow) SERUM
23 BETA HCG 3 ml SST (yellow) SERUM
24 HOMOCYSTEINE (HCY) 2 ml SST (yellow) SERUM
25 INSULIN 2 ml SST (yellow) SERUM
26 INTACH PARATHYROID HORMONE * 2 ml EDTA
(purple) PLASMA
27 INSULIN GROWTH FACTOR BINDING PROTEIN 3 2 ml SST (yellow) SERUM
27
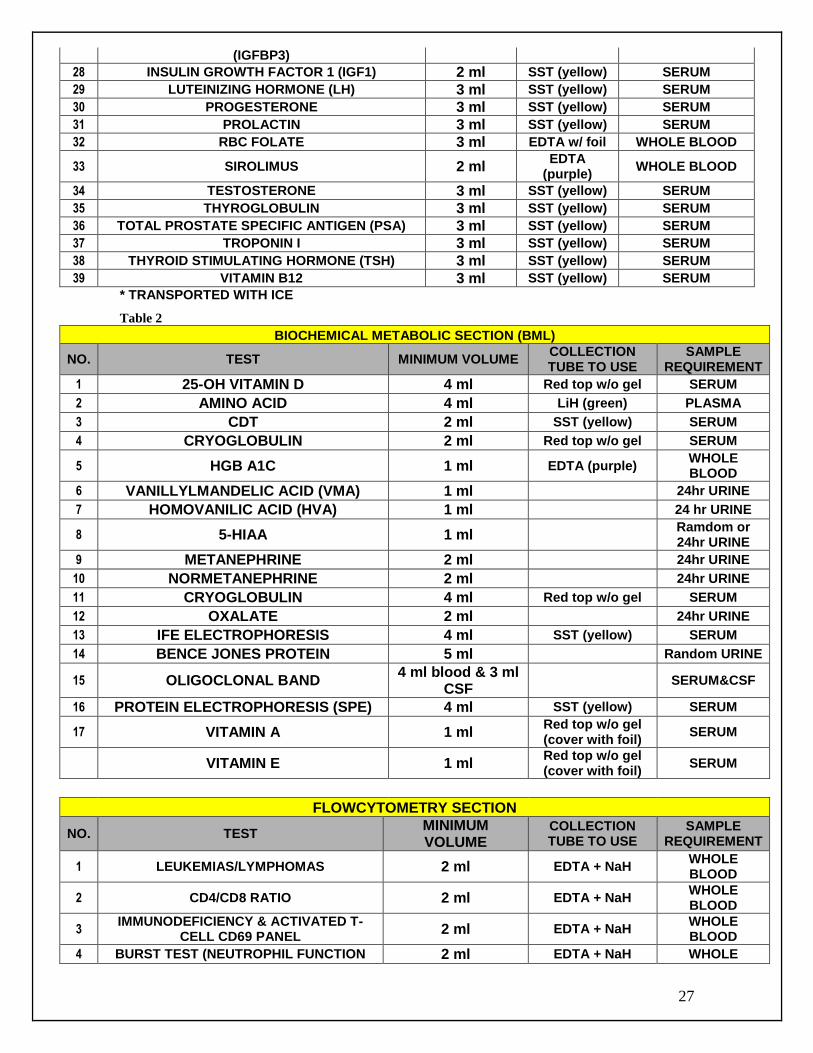
(IGFBP3)
28 INSULIN GROWTH FACTOR 1 (IGF1) 2 ml SST (yellow) SERUM
29 LUTEINIZING HORMONE (LH) 3 ml SST (yellow) SERUM
30 PROGESTERONE 3 ml SST (yellow) SERUM
31 PROLACTIN 3 ml SST (yellow) SERUM
32 RBC FOLATE 3 ml EDTA w/ foil WHOLE BLOOD
33 SIROLIMUS 2 ml EDTA
(purple) WHOLE BLOOD
34 TESTOSTERONE 3 ml SST (yellow) SERUM
35 THYROGLOBULIN 3 ml SST (yellow) SERUM
36 TOTAL PROSTATE SPECIFIC ANTIGEN (PSA) 3 ml SST (yellow) SERUM
37 TROPONIN I 3 ml SST (yellow) SERUM
38 THYROID STIMULATING HORMONE (TSH) 3 ml SST (yellow) SERUM
39 VITAMIN B12 3 ml SST (yellow) SERUM
* TRANSPORTED WITH ICE
Table 2
BIOCHEMICAL METABOLIC SECTION (BML)
NO. TEST MINIMUM VOLUME COLLECTION TUBE TO USE
SAMPLE REQUIREMENT
1 25-OH VITAMIN D 4 ml Red top w/o gel SERUM
2 AMINO ACID 4 ml LiH (green) PLASMA
3 CDT 2 ml SST (yellow) SERUM
4 CRYOGLOBULIN 2 ml Red top w/o gel SERUM
5 HGB A1C 1 ml EDTA (purple) WHOLE BLOOD
6 VANILLYLMANDELIC ACID (VMA) 1 ml 24hr URINE
7 HOMOVANILIC ACID (HVA) 1 ml 24 hr URINE
8 5-HIAA 1 ml Ramdom or 24hr URINE
9 METANEPHRINE 2 ml 24hr URINE
10 NORMETANEPHRINE 2 ml 24hr URINE
11 CRYOGLOBULIN 4 ml Red top w/o gel SERUM
12 OXALATE 2 ml 24hr URINE
13 IFE ELECTROPHORESIS 4 ml SST (yellow) SERUM
14 BENCE JONES PROTEIN 5 ml Random URINE
15 OLIGOCLONAL BAND 4 ml blood & 3 ml
CSF SERUM&CSF
16 PROTEIN ELECTROPHORESIS (SPE) 4 ml SST (yellow) SERUM
17 VITAMIN A 1 ml Red top w/o gel (cover with foil)
SERUM
VITAMIN E 1 ml Red top w/o gel (cover with foil)
SERUM
FLOWCYTOMETRY SECTION
NO. TEST MINIMUM VOLUME
COLLECTION TUBE TO USE
SAMPLE REQUIREMENT
1 LEUKEMIAS/LYMPHOMAS 2 ml EDTA + NaH WHOLE BLOOD
2 CD4/CD8 RATIO 2 ml EDTA + NaH WHOLE BLOOD
3 IMMUNODEFICIENCY & ACTIVATED T-
CELL CD69 PANEL 2 ml EDTA + NaH
WHOLE BLOOD
4 BURST TEST (NEUTROPHIL FUNCTION 2 ml EDTA + NaH WHOLE
28
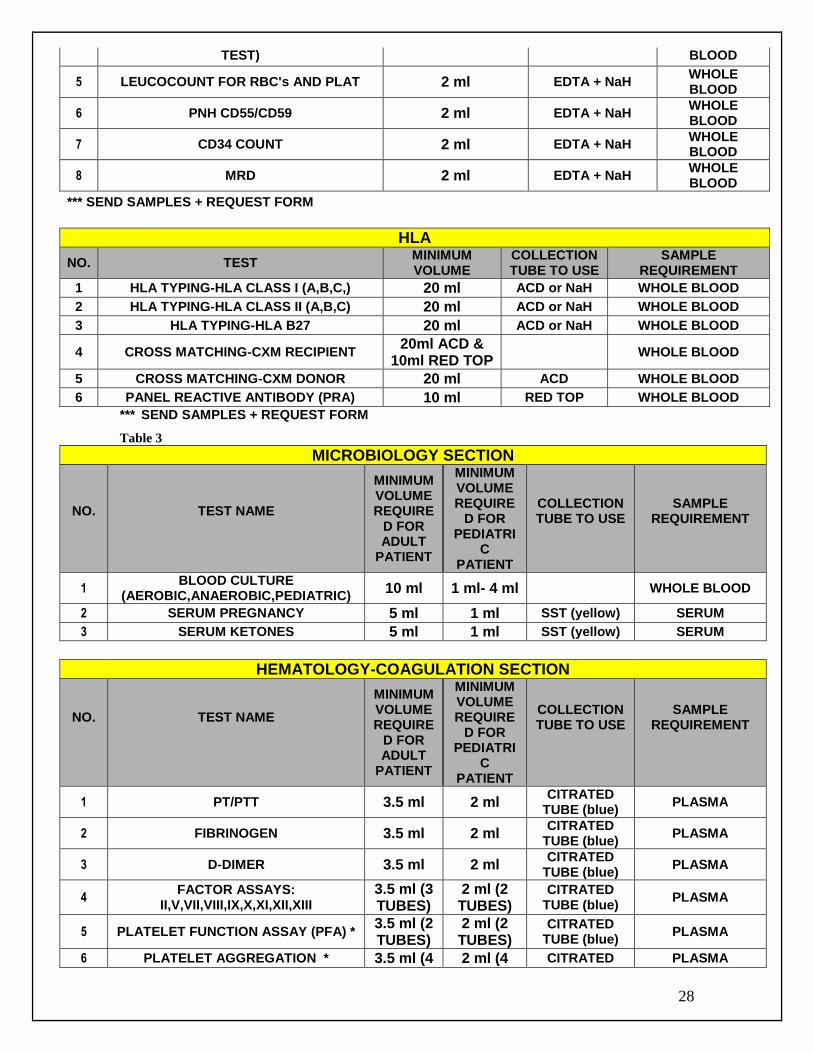
TEST) BLOOD
5 LEUCOCOUNT FOR RBC's AND PLAT 2 ml EDTA + NaH WHOLE BLOOD
6 PNH CD55/CD59 2 ml EDTA + NaH WHOLE BLOOD
7 CD34 COUNT 2 ml EDTA + NaH WHOLE BLOOD
8 MRD 2 ml EDTA + NaH WHOLE BLOOD
*** SEND SAMPLES + REQUEST FORM
HLA
NO. TEST MINIMUM VOLUME
COLLECTION TUBE TO USE
SAMPLE REQUIREMENT
1 HLA TYPING-HLA CLASS I (A,B,C,) 20 ml ACD or NaH WHOLE BLOOD
2 HLA TYPING-HLA CLASS II (A,B,C) 20 ml ACD or NaH WHOLE BLOOD
3 HLA TYPING-HLA B27 20 ml ACD or NaH WHOLE BLOOD
4 CROSS MATCHING-CXM RECIPIENT 20ml ACD &
10ml RED TOP WHOLE BLOOD
5 CROSS MATCHING-CXM DONOR 20 ml ACD WHOLE BLOOD
6 PANEL REACTIVE ANTIBODY (PRA) 10 ml RED TOP WHOLE BLOOD
*** SEND SAMPLES + REQUEST FORM
Table 3
MICROBIOLOGY SECTION
NO.
TEST NAME
MINIMUM VOLUME REQUIRE
D FOR ADULT
PATIENT
MINIMUM VOLUME REQUIRE
D FOR PEDIATRI
C PATIENT
COLLECTION TUBE TO USE
SAMPLE REQUIREMENT
1 BLOOD CULTURE
(AEROBIC,ANAEROBIC,PEDIATRIC) 10 ml 1 ml- 4 ml WHOLE BLOOD
2 SERUM PREGNANCY 5 ml 1 ml SST (yellow) SERUM
3 SERUM KETONES 5 ml 1 ml SST (yellow) SERUM
HEMATOLOGY-COAGULATION SECTION
NO.
TEST NAME
MINIMUM VOLUME REQUIRE
D FOR ADULT
PATIENT
MINIMUM VOLUME REQUIRE
D FOR PEDIATRI
C PATIENT
COLLECTION TUBE TO USE
SAMPLE REQUIREMENT
1 PT/PTT 3.5 ml 2 ml CITRATED
TUBE (blue) PLASMA
2 FIBRINOGEN 3.5 ml 2 ml CITRATED
TUBE (blue) PLASMA
3 D-DIMER 3.5 ml 2 ml CITRATED
TUBE (blue) PLASMA
4 FACTOR ASSAYS:
II,V,VII,VIII,IX,X,XI,XII,XIII 3.5 ml (3 TUBES)
2 ml (2 TUBES)
CITRATED TUBE (blue)
PLASMA
5 PLATELET FUNCTION ASSAY (PFA) * 3.5 ml (2 TUBES)
2 ml (2 TUBES)
CITRATED TUBE (blue)
PLASMA
6 PLATELET AGGREGATION * 3.5 ml (4 2 ml (4 CITRATED PLASMA
29
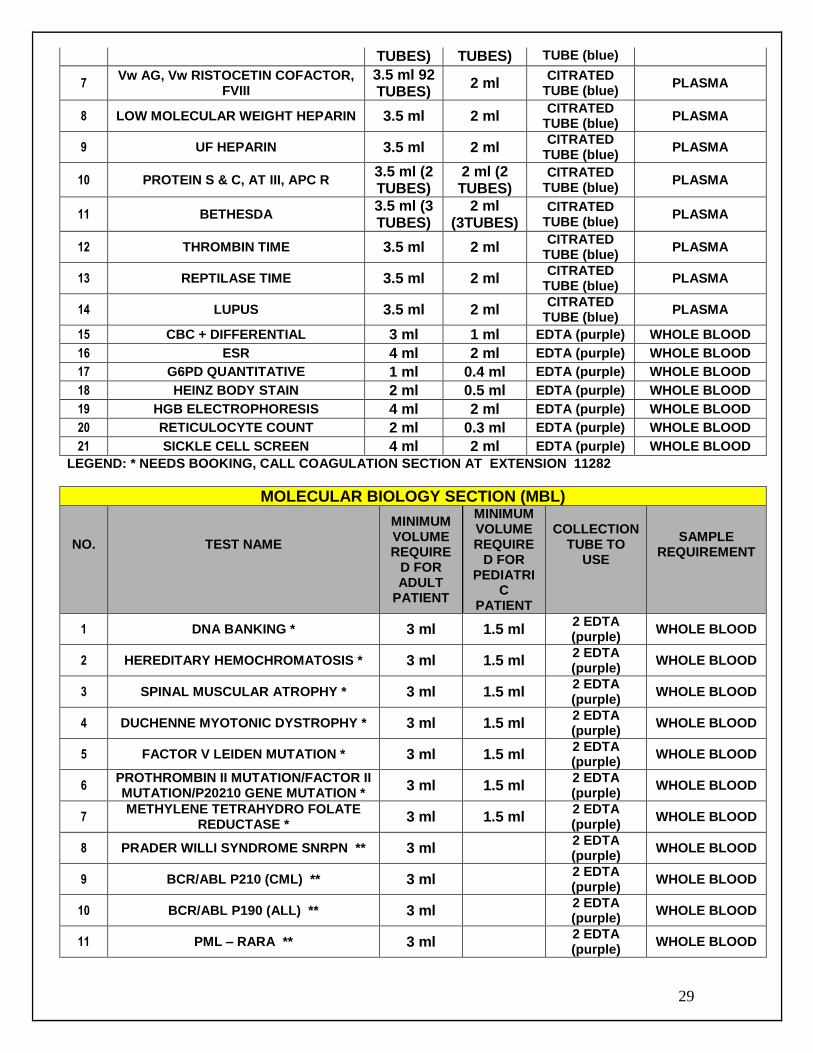
TUBES) TUBES) TUBE (blue)
7 Vw AG, Vw RISTOCETIN COFACTOR,
FVIII 3.5 ml 92 TUBES)
2 ml CITRATED
TUBE (blue) PLASMA
8 LOW MOLECULAR WEIGHT HEPARIN 3.5 ml 2 ml CITRATED
TUBE (blue) PLASMA
9 UF HEPARIN 3.5 ml 2 ml CITRATED
TUBE (blue) PLASMA
10 PROTEIN S & C, AT III, APC R 3.5 ml (2 TUBES)
2 ml (2 TUBES)
CITRATED TUBE (blue)
PLASMA
11 BETHESDA 3.5 ml (3 TUBES)
2 ml (3TUBES)
CITRATED TUBE (blue)
PLASMA
12 THROMBIN TIME 3.5 ml 2 ml CITRATED
TUBE (blue) PLASMA
13 REPTILASE TIME 3.5 ml 2 ml CITRATED
TUBE (blue) PLASMA
14 LUPUS 3.5 ml 2 ml CITRATED
TUBE (blue) PLASMA
15 CBC + DIFFERENTIAL 3 ml 1 ml EDTA (purple) WHOLE BLOOD
16 ESR 4 ml 2 ml EDTA (purple) WHOLE BLOOD
17 G6PD QUANTITATIVE 1 ml 0.4 ml EDTA (purple) WHOLE BLOOD
18 HEINZ BODY STAIN 2 ml 0.5 ml EDTA (purple) WHOLE BLOOD
19 HGB ELECTROPHORESIS 4 ml 2 ml EDTA (purple) WHOLE BLOOD
20 RETICULOCYTE COUNT 2 ml 0.3 ml EDTA (purple) WHOLE BLOOD
21 SICKLE CELL SCREEN 4 ml 2 ml EDTA (purple) WHOLE BLOOD
LEGEND: * NEEDS BOOKING, CALL COAGULATION SECTION AT EXTENSION 11282
MOLECULAR BIOLOGY SECTION (MBL)
NO.
TEST NAME
MINIMUM VOLUME REQUIRE
D FOR ADULT
PATIENT
MINIMUM VOLUME REQUIRE
D FOR PEDIATRI
C PATIENT
COLLECTION TUBE TO
USE
SAMPLE REQUIREMENT
1 DNA BANKING * 3 ml 1.5 ml 2 EDTA (purple)
WHOLE BLOOD
2 HEREDITARY HEMOCHROMATOSIS * 3 ml 1.5 ml 2 EDTA (purple)
WHOLE BLOOD
3 SPINAL MUSCULAR ATROPHY * 3 ml 1.5 ml 2 EDTA (purple)
WHOLE BLOOD
4 DUCHENNE MYOTONIC DYSTROPHY * 3 ml 1.5 ml 2 EDTA (purple)
WHOLE BLOOD
5 FACTOR V LEIDEN MUTATION * 3 ml 1.5 ml 2 EDTA (purple)
WHOLE BLOOD
6 PROTHROMBIN II MUTATION/FACTOR II MUTATION/P20210 GENE MUTATION *
3 ml 1.5 ml 2 EDTA (purple)
WHOLE BLOOD
7 METHYLENE TETRAHYDRO FOLATE
REDUCTASE * 3 ml 1.5 ml
2 EDTA (purple)
WHOLE BLOOD
8 PRADER WILLI SYNDROME SNRPN ** 3 ml 2 EDTA (purple)
WHOLE BLOOD
9 BCR/ABL P210 (CML) ** 3 ml 2 EDTA (purple)
WHOLE BLOOD
10 BCR/ABL P190 (ALL) ** 3 ml 2 EDTA (purple)
WHOLE BLOOD
11 PML – RARA ** 3 ml 2 EDTA (purple)
WHOLE BLOOD
30
* NEEDS CONSENT FORM ** SAMPLES TRANSPORTED WITH ICE
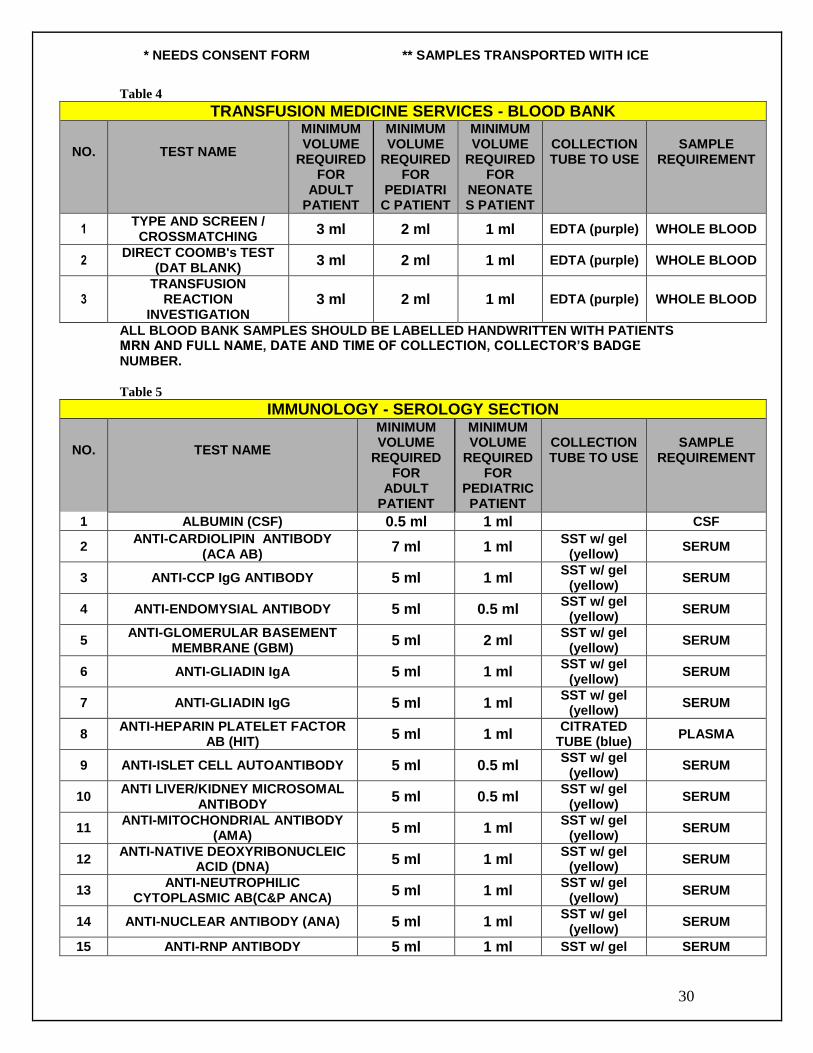
Table 4
TRANSFUSION MEDICINE SERVICES - BLOOD BANK
NO.
TEST NAME
MINIMUM VOLUME
REQUIRED FOR
ADULT PATIENT
MINIMUM VOLUME
REQUIRED FOR
PEDIATRIC PATIENT
MINIMUM VOLUME
REQUIRED FOR
NEONATES PATIENT
COLLECTION TUBE TO USE
SAMPLE REQUIREMENT
1 TYPE AND SCREEN / CROSSMATCHING
3 ml 2 ml 1 ml EDTA (purple) WHOLE BLOOD
2 DIRECT COOMB's TEST
(DAT BLANK) 3 ml 2 ml 1 ml EDTA (purple) WHOLE BLOOD
3 TRANSFUSION
REACTION INVESTIGATION
3 ml 2 ml 1 ml EDTA (purple) WHOLE BLOOD
ALL BLOOD BANK SAMPLES SHOULD BE LABELLED HANDWRITTEN WITH PATIENTS MRN AND FULL NAME, DATE AND TIME OF COLLECTION, COLLECTOR’S BADGE NUMBER.
Table 5
IMMUNOLOGY - SEROLOGY SECTION
NO.
TEST NAME
MINIMUM VOLUME
REQUIRED FOR
ADULT PATIENT
MINIMUM VOLUME
REQUIRED FOR
PEDIATRIC PATIENT
COLLECTION TUBE TO USE
SAMPLE REQUIREMENT
1 ALBUMIN (CSF) 0.5 ml 1 ml CSF
2 ANTI-CARDIOLIPIN ANTIBODY
(ACA AB) 7 ml 1 ml
SST w/ gel (yellow)
SERUM
3 ANTI-CCP IgG ANTIBODY 5 ml 1 ml SST w/ gel
(yellow) SERUM
4 ANTI-ENDOMYSIAL ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
5 ANTI-GLOMERULAR BASEMENT
MEMBRANE (GBM) 5 ml 2 ml
SST w/ gel (yellow)
SERUM
6 ANTI-GLIADIN IgA 5 ml 1 ml SST w/ gel
(yellow) SERUM
7 ANTI-GLIADIN IgG 5 ml 1 ml SST w/ gel
(yellow) SERUM
8 ANTI-HEPARIN PLATELET FACTOR
AB (HIT) 5 ml 1 ml
CITRATED TUBE (blue)
PLASMA
9 ANTI-ISLET CELL AUTOANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
10 ANTI LIVER/KIDNEY MICROSOMAL
ANTIBODY 5 ml 0.5 ml
SST w/ gel (yellow)
SERUM
11 ANTI-MITOCHONDRIAL ANTIBODY
(AMA) 5 ml 1 ml
SST w/ gel (yellow)
SERUM
12 ANTI-NATIVE DEOXYRIBONUCLEIC
ACID (DNA) 5 ml 1 ml
SST w/ gel (yellow)
SERUM
13 ANTI-NEUTROPHILIC
CYTOPLASMIC AB(C&P ANCA) 5 ml 1 ml
SST w/ gel (yellow)
SERUM
14 ANTI-NUCLEAR ANTIBODY (ANA) 5 ml 1 ml SST w/ gel
(yellow) SERUM
15 ANTI-RNP ANTIBODY 5 ml 1 ml SST w/ gel SERUM

31
(yellow)
16 ANTI-SCL 70 ANTIBODY 5 ml 1 ml SST w/ gel
(yellow) SERUM
17 ANTI-SMITH ANTIBODY 5 ml 1 ml SST w/ gel
(yellow) SERUM
18 ANTI-SMOOTH MUSCLE ANTIBODY
(ASMA) 5 ml 1 ml
SST w/ gel (yellow)
SERUM
19 ANTI-SS-A ANTIBODY (ANTI-RO) 5 ml 1 ml SST w/ gel
(yellow) SERUM
20 ANTI-SS-B ANTIBODY (ANTI-LA) 5 ml 1 ml SST w/ gel
(yellow) SERUM
21 ANTI-STREPTOLYSIN O (ASOT) 5 ml 1 ml SST w/ gel
(yellow) SERUM
22 ANTI-STREPTOZYME ANTIBODY 5 ml 1 ml SST w/ gel
(yellow) SERUM
23 ANTI-THYROGLOBULIN AB (htg) 5 ml 1 ml SST w/ gel
(yellow) SERUM
24 ANTI-THYROID PEROXIDASE AB
(TPO) 5 ml 1 ml
SST w/ gel (yellow)
SERUM
25 BETA 2 GLYCOPROTEIN IgA, IgM,
IgG 5 ml 1 ml
SST w/ gel (yellow)
SERUM
26 BRUCELLA ANTIBODY 5 ml 1 ml SST w/ gel
(yellow) SERUM/
CSF
27 CHLAMYDIA ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
28 CMV IgG 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
29 CMV IgM 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
30 COLD AGGLUTININS 5 ml 1 ml SST w/ gel
(yellow) SERUM
31 CONFIRMATORY TEST FOR
HEPATITIS B SURFACE ANTIGEN 10 ml 0.5 ml
SST w/ gel (yellow)
SERUM
32 CONFIRMATORY TEST FOR
HEPATITIS C VIRUS 5 ml 0.3 ml
SST w/ gel (yellow)
SERUM
33 C-REACTIVE PROTEIN (CRP) 5 ml 1 ml SST w/ gel
(yellow) SERUM
34 CRYPTOCOCCAL ANTIGEN
DETECTION 5 ml 1 ml
SST w/ gel (yellow)
SERUM
35 DENGUE IgG & IgM 5 ml 1 ml SST w/ gel
(yellow) SERUM
36 EBNA-G 5 ml 1 ml SST w/ gel
(yellow) SERUM
37 EBV-EA 5 ml 1 ml SST w/ gel
(yellow) SERUM
38 EBV-IgG 5 ml 1 ml SST w/ gel
(yellow) SERUM
39 EBV-IgM 5 ml 1 ml SST w/ gel
(yellow) SERUM
40 FEBRILE AGGLUTININS 10 ml 1 ml SST w/ gel
(yellow) SERUM
41 FTA-ABSORBTION 5 ml 1 ml SST w/ gel
(yellow) SERUM
42 FUNGAL SEROLOGY 5 ml 1 ml SST w/ gel
(yellow) SERUM
43 GASTRIC PARIETAL CELL
ANTIBODY (GPA) 5 ml 1 ml
SST w/ gel (yellow)
SERUM
44 GLUTAMATE DECARBOXYLASE 2 ml 1 ml SST w/ gel SERUM
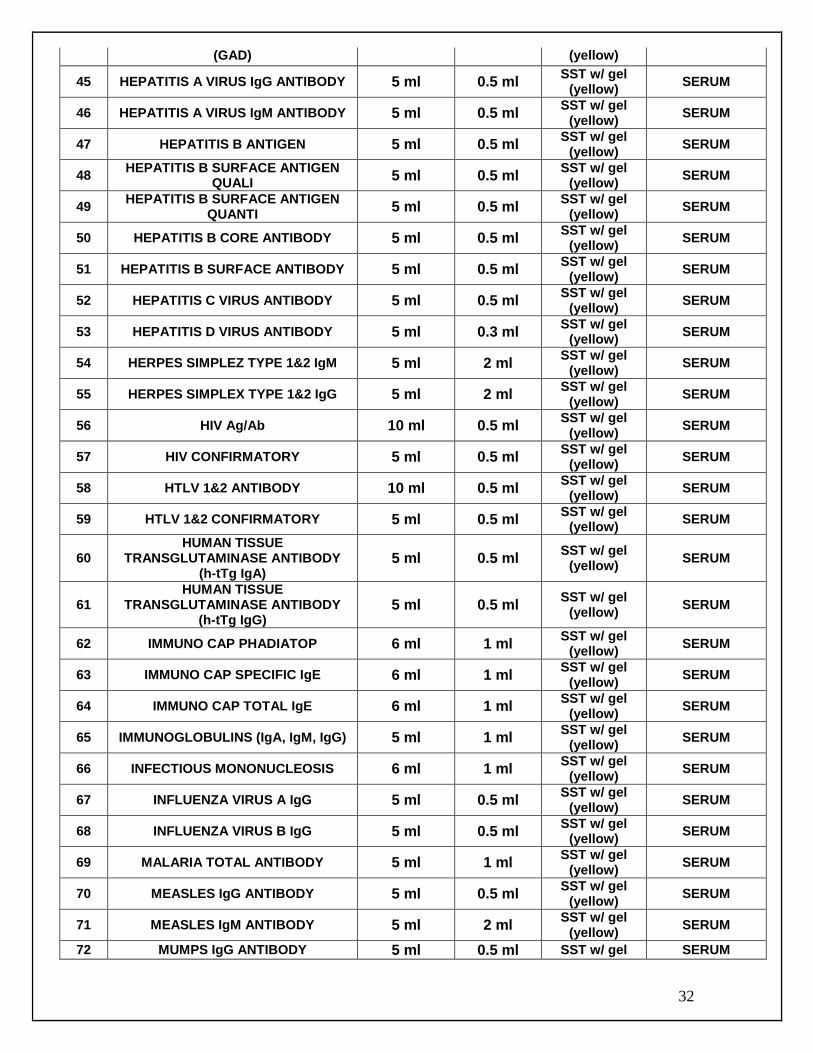
32
(GAD) (yellow)
45 HEPATITIS A VIRUS IgG ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
46 HEPATITIS A VIRUS IgM ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
47 HEPATITIS B ANTIGEN 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
48 HEPATITIS B SURFACE ANTIGEN
QUALI 5 ml 0.5 ml
SST w/ gel (yellow)
SERUM
49 HEPATITIS B SURFACE ANTIGEN
QUANTI 5 ml 0.5 ml
SST w/ gel (yellow)
SERUM
50 HEPATITIS B CORE ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
51 HEPATITIS B SURFACE ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
52 HEPATITIS C VIRUS ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
53 HEPATITIS D VIRUS ANTIBODY 5 ml 0.3 ml SST w/ gel
(yellow) SERUM
54 HERPES SIMPLEZ TYPE 1&2 IgM 5 ml 2 ml SST w/ gel
(yellow) SERUM
55 HERPES SIMPLEX TYPE 1&2 IgG 5 ml 2 ml SST w/ gel
(yellow) SERUM
56 HIV Ag/Ab 10 ml 0.5 ml SST w/ gel
(yellow) SERUM
57 HIV CONFIRMATORY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
58 HTLV 1&2 ANTIBODY 10 ml 0.5 ml SST w/ gel
(yellow) SERUM
59 HTLV 1&2 CONFIRMATORY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
60 HUMAN TISSUE
TRANSGLUTAMINASE ANTIBODY (h-tTg IgA)
5 ml 0.5 ml SST w/ gel
(yellow) SERUM
61 HUMAN TISSUE
TRANSGLUTAMINASE ANTIBODY (h-tTg IgG)
5 ml 0.5 ml SST w/ gel
(yellow) SERUM
62 IMMUNO CAP PHADIATOP 6 ml 1 ml SST w/ gel
(yellow) SERUM
63 IMMUNO CAP SPECIFIC IgE 6 ml 1 ml SST w/ gel
(yellow) SERUM
64 IMMUNO CAP TOTAL IgE 6 ml 1 ml SST w/ gel
(yellow) SERUM
65 IMMUNOGLOBULINS (IgA, IgM, IgG) 5 ml 1 ml SST w/ gel
(yellow) SERUM
66 INFECTIOUS MONONUCLEOSIS 6 ml 1 ml SST w/ gel
(yellow) SERUM
67 INFLUENZA VIRUS A IgG 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
68 INFLUENZA VIRUS B IgG 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
69 MALARIA TOTAL ANTIBODY 5 ml 1 ml SST w/ gel
(yellow) SERUM
70 MEASLES IgG ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
71 MEASLES IgM ANTIBODY 5 ml 2 ml SST w/ gel
(yellow) SERUM
72 MUMPS IgG ANTIBODY 5 ml 0.5 ml SST w/ gel SERUM
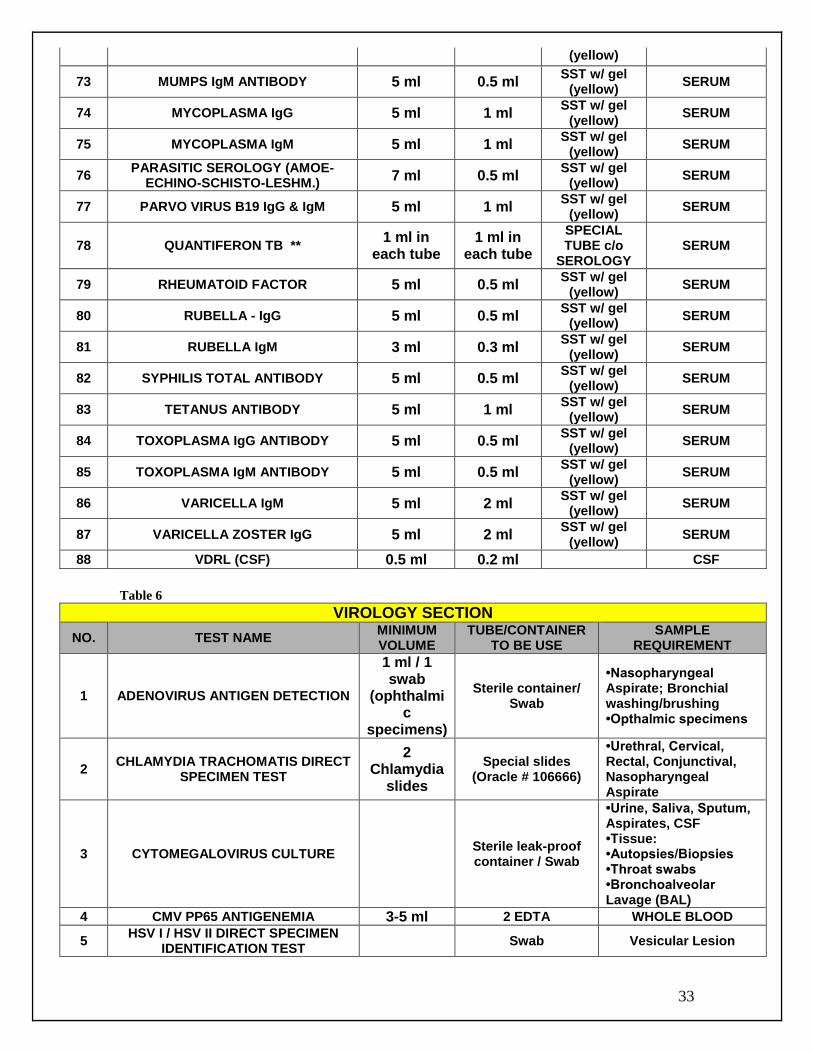
33
(yellow)
73 MUMPS IgM ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
74 MYCOPLASMA IgG 5 ml 1 ml SST w/ gel
(yellow) SERUM
75 MYCOPLASMA IgM 5 ml 1 ml SST w/ gel
(yellow) SERUM
76 PARASITIC SEROLOGY (AMOE-
ECHINO-SCHISTO-LESHM.) 7 ml 0.5 ml
SST w/ gel (yellow)
SERUM
77 PARVO VIRUS B19 IgG & IgM 5 ml 1 ml SST w/ gel
(yellow) SERUM
78 QUANTIFERON TB ** 1 ml in
each tube 1 ml in
each tube
SPECIAL TUBE c/o
SEROLOGY SERUM
79 RHEUMATOID FACTOR 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
80 RUBELLA - IgG 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
81 RUBELLA IgM 3 ml 0.3 ml SST w/ gel
(yellow) SERUM
82 SYPHILIS TOTAL ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
83 TETANUS ANTIBODY 5 ml 1 ml SST w/ gel
(yellow) SERUM
84 TOXOPLASMA IgG ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
85 TOXOPLASMA IgM ANTIBODY 5 ml 0.5 ml SST w/ gel
(yellow) SERUM
86 VARICELLA IgM 5 ml 2 ml SST w/ gel
(yellow) SERUM
87 VARICELLA ZOSTER IgG 5 ml 2 ml SST w/ gel
(yellow) SERUM
88 VDRL (CSF) 0.5 ml 0.2 ml CSF
Table 6
VIROLOGY SECTION
NO. TEST NAME MINIMUM VOLUME
TUBE/CONTAINER TO BE USE
SAMPLE REQUIREMENT
1 ADENOVIRUS ANTIGEN DETECTION
1 ml / 1 swab
(ophthalmic
specimens)
Sterile container/ Swab
•Nasopharyngeal Aspirate; Bronchial washing/brushing •Opthalmic specimens
2 CHLAMYDIA TRACHOMATIS DIRECT
SPECIMEN TEST
2 Chlamydia
slides
Special slides (Oracle # 106666)
•Urethral, Cervical, Rectal, Conjunctival, Nasopharyngeal Aspirate
3 CYTOMEGALOVIRUS CULTURE Sterile leak-proof container / Swab
•Urine, Saliva, Sputum, Aspirates, CSF •Tissue: •Autopsies/Biopsies •Throat swabs •Bronchoalveolar Lavage (BAL)
4 CMV PP65 ANTIGENEMIA 3-5 ml 2 EDTA WHOLE BLOOD
5 HSV I / HSV II DIRECT SPECIMEN
IDENTIFICATION TEST Swab Vesicular Lesion
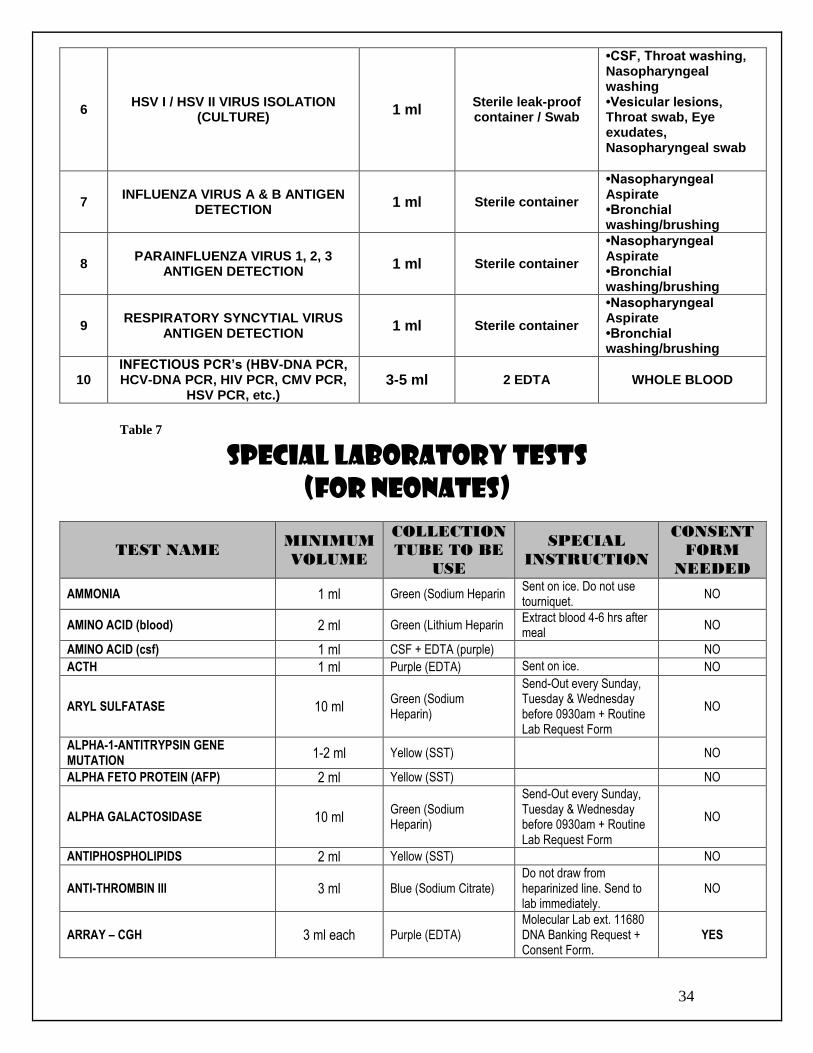
34
6 HSV I / HSV II VIRUS ISOLATION
(CULTURE) 1 ml
Sterile leak-proof container / Swab
•CSF, Throat washing, Nasopharyngeal washing •Vesicular lesions, Throat swab, Eye exudates, Nasopharyngeal swab
7 INFLUENZA VIRUS A & B ANTIGEN
DETECTION 1 ml Sterile container
•Nasopharyngeal Aspirate •Bronchial washing/brushing
8 PARAINFLUENZA VIRUS 1, 2, 3
ANTIGEN DETECTION 1 ml Sterile container
•Nasopharyngeal Aspirate •Bronchial washing/brushing
9 RESPIRATORY SYNCYTIAL VIRUS
ANTIGEN DETECTION 1 ml Sterile container
•Nasopharyngeal Aspirate •Bronchial washing/brushing
10 INFECTIOUS PCR’s (HBV-DNA PCR, HCV-DNA PCR, HIV PCR, CMV PCR,
HSV PCR, etc.) 3-5 ml 2 EDTA WHOLE BLOOD
Table 7
SPECIAL LABORATORY TESTS (FOR NEONATES)
TEST NAME MINIMUM
VOLUME
COLLECTION
TUBE TO BE
USE
SPECIAL
INSTRUCTION
CONSENT
FORM
NEEDED
AMMONIA 1 ml Green (Sodium Heparin Sent on ice. Do not use tourniquet.
NO
AMINO ACID (blood) 2 ml Green (Lithium Heparin Extract blood 4-6 hrs after meal
NO
AMINO ACID (csf) 1 ml CSF + EDTA (purple) NO ACTH 1 ml Purple (EDTA) Sent on ice. NO
ARYL SULFATASE 10 ml Green (Sodium Heparin)
Send-Out every Sunday, Tuesday & Wednesday before 0930am + Routine Lab Request Form
NO
ALPHA-1-ANTITRYPSIN GENE MUTATION
1-2 ml Yellow (SST)
NO
ALPHA FETO PROTEIN (AFP) 2 ml Yellow (SST) NO
ALPHA GALACTOSIDASE 10 ml Green (Sodium Heparin)
Send-Out every Sunday, Tuesday & Wednesday before 0930am + Routine Lab Request Form
NO
ANTIPHOSPHOLIPIDS 2 ml Yellow (SST) NO
ANTI-THROMBIN III 3 ml Blue (Sodium Citrate) Do not draw from heparinized line. Send to lab immediately.
NO
ARRAY – CGH 3 ml each Purple (EDTA) Molecular Lab ext. 11680 DNA Banking Request + Consent Form.
YES
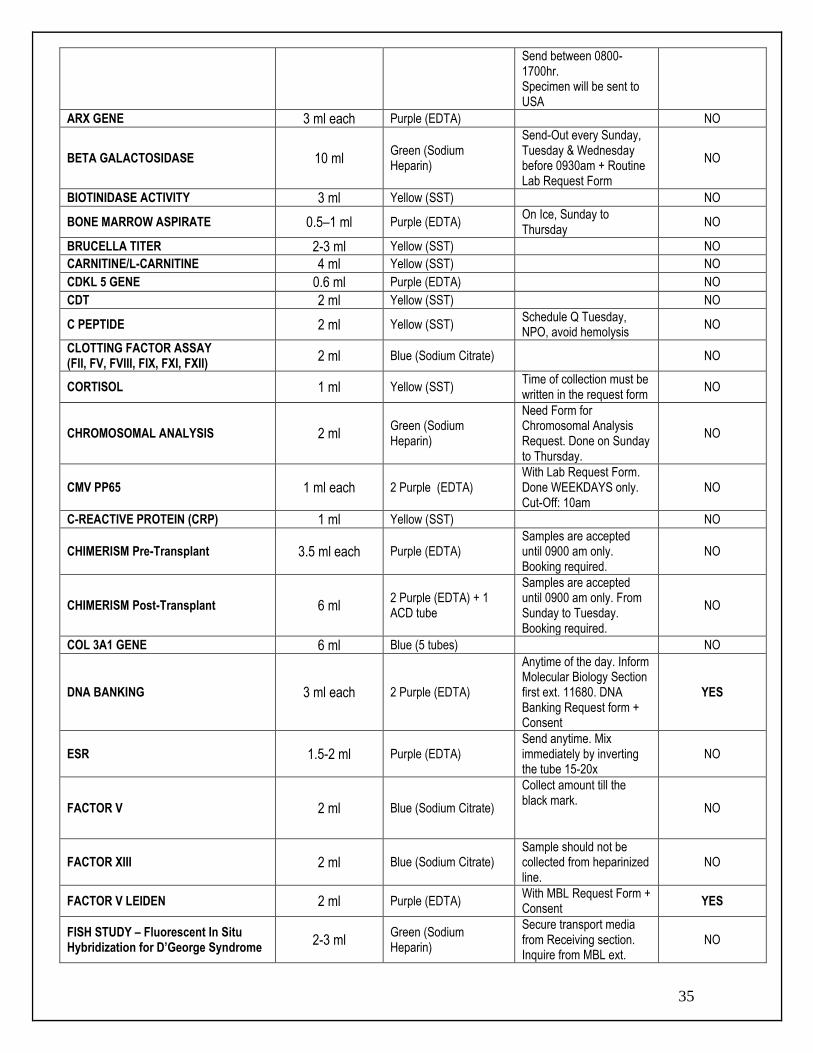
35
Send between 0800-1700hr. Specimen will be sent to USA
ARX GENE 3 ml each Purple (EDTA) NO
BETA GALACTOSIDASE 10 ml Green (Sodium Heparin)
Send-Out every Sunday, Tuesday & Wednesday before 0930am + Routine Lab Request Form
NO
BIOTINIDASE ACTIVITY 3 ml Yellow (SST) NO
BONE MARROW ASPIRATE 0.5–1 ml Purple (EDTA) On Ice, Sunday to Thursday
NO
BRUCELLA TITER 2-3 ml Yellow (SST) NO CARNITINE/L-CARNITINE 4 ml Yellow (SST) NO
CDKL 5 GENE 0.6 ml Purple (EDTA) NO
CDT 2 ml Yellow (SST) NO
C PEPTIDE 2 ml Yellow (SST) Schedule Q Tuesday, NPO, avoid hemolysis
NO
CLOTTING FACTOR ASSAY (FII, FV, FVIII, FIX, FXI, FXII)
2 ml Blue (Sodium Citrate)
NO
CORTISOL 1 ml Yellow (SST) Time of collection must be written in the request form
NO
CHROMOSOMAL ANALYSIS 2 ml Green (Sodium Heparin)
Need Form for Chromosomal Analysis Request. Done on Sunday to Thursday.
NO
CMV PP65 1 ml each 2 Purple (EDTA) With Lab Request Form. Done WEEKDAYS only. Cut-Off: 10am
NO
C-REACTIVE PROTEIN (CRP) 1 ml Yellow (SST) NO
CHIMERISM Pre-Transplant 3.5 ml each Purple (EDTA) Samples are accepted until 0900 am only. Booking required.
NO
CHIMERISM Post-Transplant 6 ml 2 Purple (EDTA) + 1 ACD tube
Samples are accepted until 0900 am only. From Sunday to Tuesday. Booking required.
NO
COL 3A1 GENE 6 ml Blue (5 tubes) NO
DNA BANKING 3 ml each 2 Purple (EDTA)
Anytime of the day. Inform Molecular Biology Section first ext. 11680. DNA Banking Request form + Consent
YES
ESR 1.5-2 ml Purple (EDTA) Send anytime. Mix immediately by inverting the tube 15-20x
NO
FACTOR V 2 ml Blue (Sodium Citrate)
Collect amount till the black mark.
NO
FACTOR XIII 2 ml Blue (Sodium Citrate) Sample should not be collected from heparinized line.
NO
FACTOR V LEIDEN 2 ml Purple (EDTA) With MBL Request Form + Consent
YES
FISH STUDY – Fluorescent In Situ Hybridization for D’George Syndrome
2-3 ml Green (Sodium Heparin)
Secure transport media from Receiving section. Inquire from MBL ext.
NO
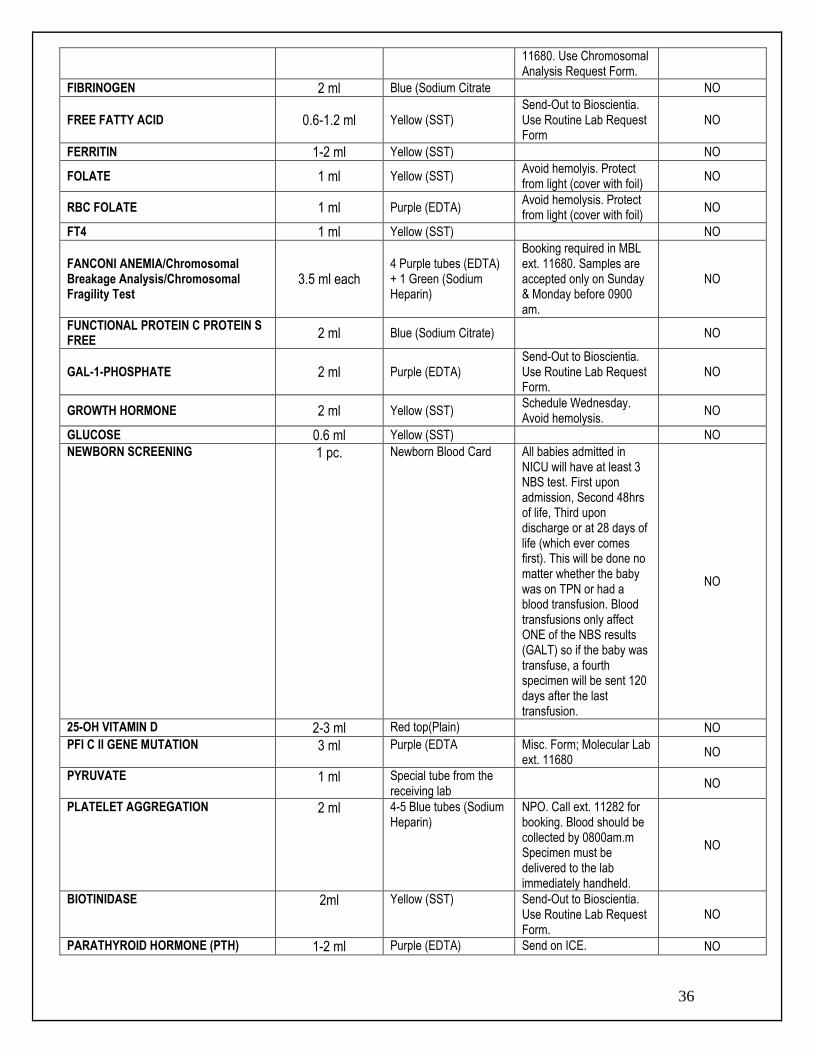
36
11680. Use Chromosomal Analysis Request Form.
FIBRINOGEN 2 ml Blue (Sodium Citrate NO
FREE FATTY ACID 0.6-1.2 ml Yellow (SST) Send-Out to Bioscientia. Use Routine Lab Request Form
NO
FERRITIN 1-2 ml Yellow (SST) NO
FOLATE 1 ml Yellow (SST) Avoid hemolyis. Protect from light (cover with foil)
NO
RBC FOLATE 1 ml Purple (EDTA) Avoid hemolysis. Protect from light (cover with foil)
NO
FT4 1 ml Yellow (SST) NO
FANCONI ANEMIA/Chromosomal Breakage Analysis/Chromosomal Fragility Test
3.5 ml each 4 Purple tubes (EDTA) + 1 Green (Sodium Heparin)
Booking required in MBL ext. 11680. Samples are accepted only on Sunday & Monday before 0900 am.
NO
FUNCTIONAL PROTEIN C PROTEIN S FREE
2 ml Blue (Sodium Citrate)
NO
GAL-1-PHOSPHATE 2 ml Purple (EDTA) Send-Out to Bioscientia. Use Routine Lab Request Form.
NO
GROWTH HORMONE 2 ml Yellow (SST) Schedule Wednesday. Avoid hemolysis.
NO
GLUCOSE 0.6 ml Yellow (SST) NO NEWBORN SCREENING 1 pc. Newborn Blood Card All babies admitted in
NICU will have at least 3 NBS test. First upon admission, Second 48hrs of life, Third upon discharge or at 28 days of life (which ever comes first). This will be done no matter whether the baby was on TPN or had a blood transfusion. Blood transfusions only affect ONE of the NBS results (GALT) so if the baby was transfuse, a fourth specimen will be sent 120 days after the last transfusion.
NO
25-OH VITAMIN D 2-3 ml Red top(Plain) NO PFI C II GENE MUTATION 3 ml Purple (EDTA Misc. Form; Molecular Lab
ext. 11680 NO
PYRUVATE 1 ml Special tube from the receiving lab
NO
PLATELET AGGREGATION 2 ml 4-5 Blue tubes (Sodium Heparin)
NPO. Call ext. 11282 for booking. Blood should be collected by 0800am.m Specimen must be delivered to the lab immediately handheld.
NO
BIOTINIDASE 2ml Yellow (SST) Send-Out to Bioscientia. Use Routine Lab Request Form.
NO
PARATHYROID HORMONE (PTH) 1-2 ml Purple (EDTA) Send on ICE. NO
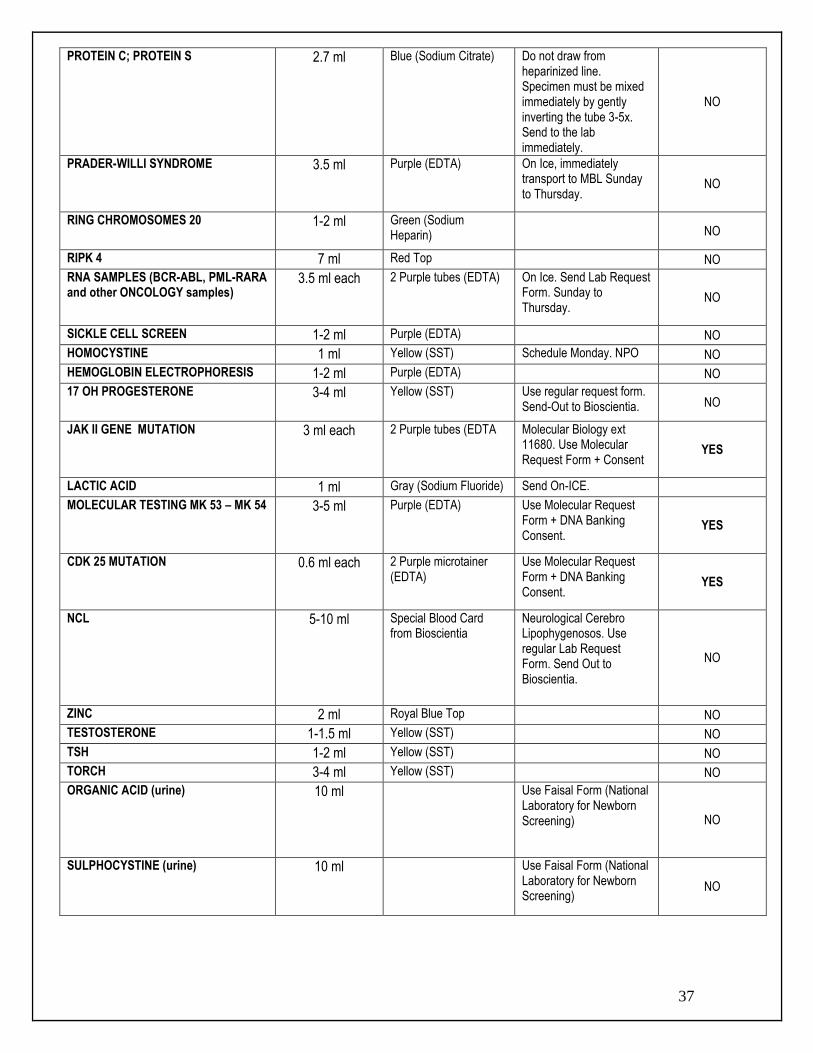
37
PROTEIN C; PROTEIN S 2.7 ml Blue (Sodium Citrate) Do not draw from heparinized line. Specimen must be mixed immediately by gently inverting the tube 3-5x. Send to the lab immediately.
NO
PRADER-WILLI SYNDROME 3.5 ml Purple (EDTA) On Ice, immediately transport to MBL Sunday to Thursday.
NO
RING CHROMOSOMES 20 1-2 ml Green (Sodium Heparin)
NO
RIPK 4 7 ml Red Top NO
RNA SAMPLES (BCR-ABL, PML-RARA and other ONCOLOGY samples)
3.5 ml each 2 Purple tubes (EDTA) On Ice. Send Lab Request Form. Sunday to Thursday.
NO
SICKLE CELL SCREEN 1-2 ml Purple (EDTA) NO
HOMOCYSTINE 1 ml Yellow (SST) Schedule Monday. NPO NO
HEMOGLOBIN ELECTROPHORESIS 1-2 ml Purple (EDTA) NO
17 OH PROGESTERONE 3-4 ml Yellow (SST) Use regular request form. Send-Out to Bioscientia. NO
JAK II GENE MUTATION 3 ml each 2 Purple tubes (EDTA Molecular Biology ext 11680. Use Molecular Request Form + Consent
YES
LACTIC ACID 1 ml Gray (Sodium Fluoride) Send On-ICE.
MOLECULAR TESTING MK 53 – MK 54 3-5 ml Purple (EDTA) Use Molecular Request Form + DNA Banking Consent.
YES
CDK 25 MUTATION 0.6 ml each 2 Purple microtainer (EDTA)
Use Molecular Request Form + DNA Banking Consent.
YES
NCL 5-10 ml Special Blood Card from Bioscientia
Neurological Cerebro Lipophygenosos. Use regular Lab Request Form. Send Out to Bioscientia.
NO
ZINC 2 ml Royal Blue Top NO TESTOSTERONE 1-1.5 ml Yellow (SST) NO TSH 1-2 ml Yellow (SST) NO TORCH 3-4 ml Yellow (SST) NO ORGANIC ACID (urine) 10 ml Use Faisal Form (National
Laboratory for Newborn Screening)
NO
SULPHOCYSTINE (urine) 10 ml Use Faisal Form (National Laboratory for Newborn Screening)
NO
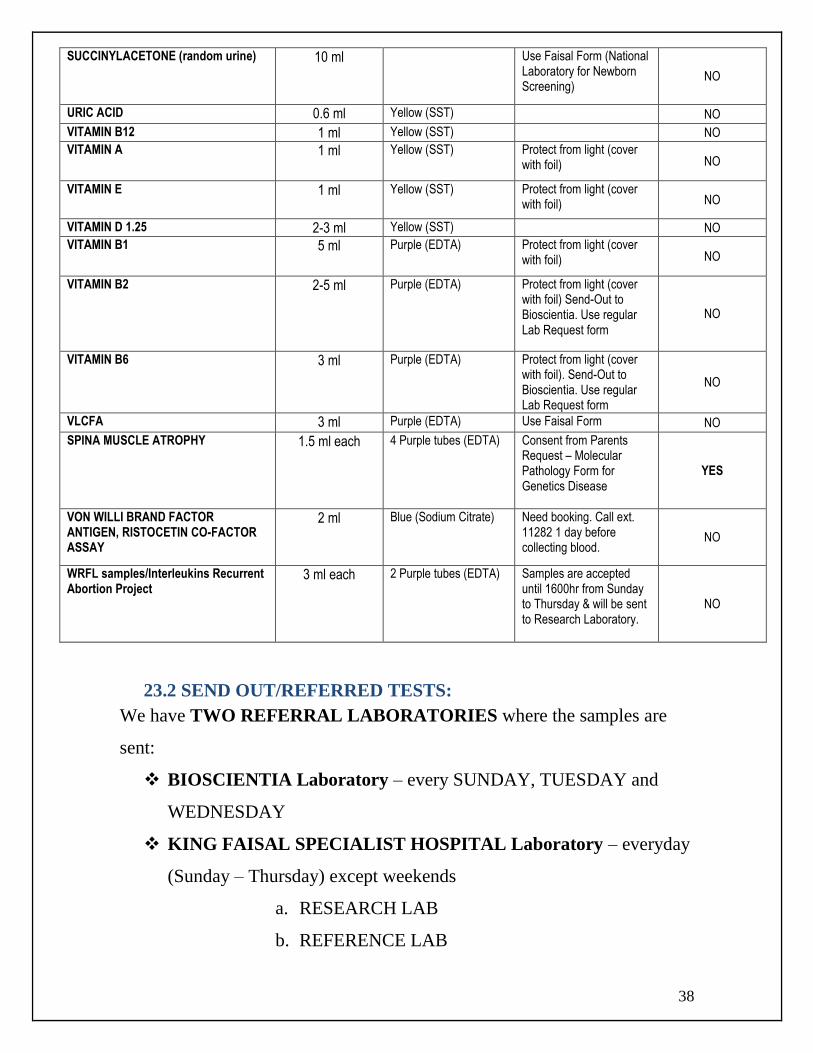
38
SUCCINYLACETONE (random urine) 10 ml Use Faisal Form (National Laboratory for Newborn Screening)
NO
URIC ACID 0.6 ml Yellow (SST) NO VITAMIN B12 1 ml Yellow (SST) NO VITAMIN A 1 ml Yellow (SST) Protect from light (cover
with foil) NO
VITAMIN E 1 ml Yellow (SST) Protect from light (cover with foil) NO
VITAMIN D 1.25 2-3 ml Yellow (SST) NO
VITAMIN B1 5 ml Purple (EDTA) Protect from light (cover with foil) NO
VITAMIN B2 2-5 ml Purple (EDTA) Protect from light (cover with foil) Send-Out to Bioscientia. Use regular Lab Request form
NO
VITAMIN B6 3 ml Purple (EDTA) Protect from light (cover with foil). Send-Out to Bioscientia. Use regular Lab Request form
NO
VLCFA 3 ml Purple (EDTA) Use Faisal Form NO
SPINA MUSCLE ATROPHY 1.5 ml each 4 Purple tubes (EDTA) Consent from Parents Request – Molecular Pathology Form for Genetics Disease
YES
VON WILLI BRAND FACTOR ANTIGEN, RISTOCETIN CO-FACTOR ASSAY
2 ml Blue (Sodium Citrate) Need booking. Call ext. 11282 1 day before collecting blood.
NO
WRFL samples/Interleukins Recurrent Abortion Project
3 ml each 2 Purple tubes (EDTA) Samples are accepted until 1600hr from Sunday to Thursday & will be sent to Research Laboratory.
NO
23.2 SEND OUT/REFERRED TESTS:
We have TWO REFERRAL LABORATORIES where the samples are
sent:
BIOSCIENTIA Laboratory – every SUNDAY, TUESDAY and
WEDNESDAY
KING FAISAL SPECIALIST HOSPITAL Laboratory – everyday
(Sunday – Thursday) except weekends
a. RESEARCH LAB
b. REFERENCE LAB
39
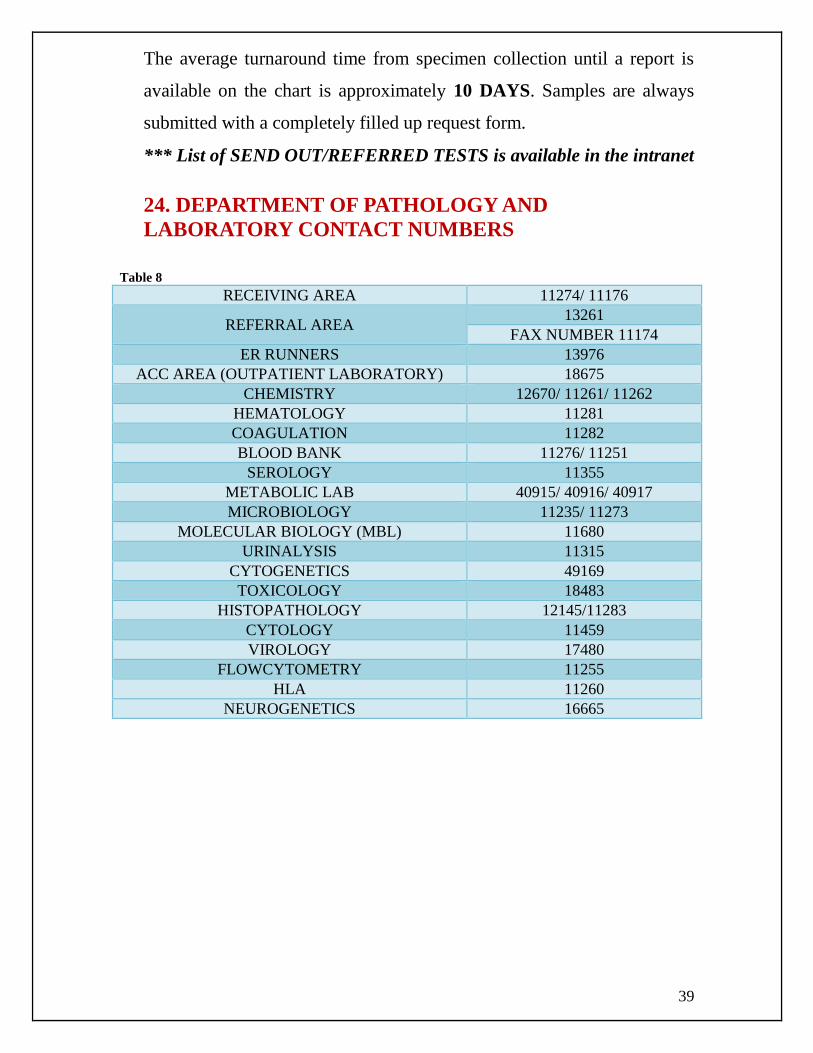
The average turnaround time from specimen collection until a report is
available on the chart is approximately 10 DAYS. Samples are always
submitted with a completely filled up request form.
*** List of SEND OUT/REFERRED TESTS is available in the intranet
24. DEPARTMENT OF PATHOLOGY AND
LABORATORY CONTACT NUMBERS
Table 8
RECEIVING AREA 11274/ 11176
REFERRAL AREA 13261
FAX NUMBER 11174
ER RUNNERS 13976
ACC AREA (OUTPATIENT LABORATORY) 18675
CHEMISTRY 12670/ 11261/ 11262
HEMATOLOGY 11281
COAGULATION 11282
BLOOD BANK 11276/ 11251
SEROLOGY 11355
METABOLIC LAB 40915/ 40916/ 40917
MICROBIOLOGY 11235/ 11273
MOLECULAR BIOLOGY (MBL) 11680
URINALYSIS 11315
CYTOGENETICS 49169
TOXICOLOGY 18483
HISTOPATHOLOGY 12145/11283
CYTOLOGY 11459
VIROLOGY 17480
FLOWCYTOMETRY 11255
HLA 11260
NEUROGENETICS 16665

40
For Further Information Please Contact:
MS. RAMOU SARR
Receiving and ACC Supervisor
Department of Pathology & Laboratory Medicine
King Abdulaziz Medical City
Ministry of National Guard Health Affairs
Extension 13353 / Pager 5261
















![Specimen Collection[1]](https://img.pdfslide.us/doc/110x75/54677775af795932578b4f14/specimen-collection1.jpg)












