Embed Size (px)
Citation preview


Laboratory Diagnosis y gof toxoplasmosisof toxoplasmosis
Dr. M SaraeiQazvin University of Medical SciencesQazvin University of Medical Sciences

ToxoplasmosisToxoplasmosisToxoplasmosis is caused byToxoplasmosis is caused by Toxoplasma gondii, an obligate intracellular protozoan parasite that infects mostparasite that infects mostspecies of warm-bloodedanimals

Definitive HostDefinitive Host

Intermediate HostIntermediate Host

Intermediate HostIntermediate Host


FecalFecal--Oral TransmissionOral Transmission
OocystOocyst

CarnivorismCarnivorismCarnivorismCarnivorism

TransplacentalTransplacentalTransplacentalTransplacental
Tachyzoite


Tissue cyst in meat
Oocysts
Tissue cystTissue cyst
Acute Phase
Chronic Phase

Acute Phase

Chronic Phase

ToxoplasmosisToxoplasmosisA i d t l iAquired toxoplasmosisCongenital toxoplasmosisCongenital toxoplasmosis

Aquired toxoplasmosisAquired toxoplasmosisIn immunocompetent individuals acuteIn immunocompetent individuals, acute infection is usually asymptomatic and
t i th lspontaneous recovery is the rule.
Most often, toxoplasmosis manifests as asymptomatic cervical lymphadenopathyasymptomatic cervical lymphadenopathy, but any or all lymph node groups may be enlargedenlarged.

ToxoplasmicToxoplasmic encephalitisencephalitispp ppin immunocompromised patientsin immunocompromised patients

Congenital toxoplasmosisCongenital toxoplasmosisCongenital toxoplasmosisCongenital toxoplasmosis

Congenital toxoplasmosisp
Chorioretinitis is the most common manifestation of congenital toxoplasmosis

L b Di iLaboratory Diagnosisof
toxoplasmosisp

The laboratory diagnosis of The laboratory diagnosis of toxoplasmosis may be established by:toxoplasmosis may be established by:toxoplasmosis may be established by: toxoplasmosis may be established by:
Serological testsSerological testsHistological demonstration of the parasite
and/or its antigens (i e immunoperoxidaseand/or its antigens (i.e. immunoperoxidase stain)I l ti f th iIsolation of the organism. Molecular diagnosis (PCR/ Real Time PCR)

Diagnostic method may differ considerably with the clinical entity:considerably with the clinical entity:Immunocompetent patientImmunodeficient patientOcular toxoplasmosisOcular toxoplasmosisToxoplasmosis in pregnancyCongenital toxoplasmosis.

Main challenge for diagnosis of g f g ftoxoplasmosis is differentiation of
acute and chronic infectionsacute and chronic infections

Acute infection is diagnosed by:Acute infection is diagnosed by:• Isolation of T. gondii from blood or body fluids
PCR bl d b d fl id• PCR blood or body fluids• Demonstration of tachyzoites in histologic sections of tissue or in cytologic preparations ofsections of tissue or in cytologic preparations of body fluids• Demonstration of a characteristic lymph node• Demonstration of a characteristic lymph node histologic appearance• Serologic test resultsSerologic test results• Demonstration of T. gondii tissue cysts in the placenta, fetus, or neonate. p , f ,

Serodiagnosis of Toxoplasmosis
• Serologic tests for the demonstration of specific antibody to T. gondii is the primary method of diagnosis.

Serodiagnosis of Toxoplasmosis
• IgG, IgM, IgA, and IgE antibodies produce to T. gondii
• Initial serologic testing can be accomplished by simultaneouslyaccomplished by simultaneously requesting IgG and IgM antibody t ttests.

Pattern of IgG & IgM antibodies g gin acute and chronic infection

Serodiagnosis of Toxoplasmosis
ELISA, IFA, Chemiluminescent tests use for detection of specific IgG and IgM antibodies to T. gondii

SerodiagnosisSerodiagnosis of Toxoplasmosisof ToxoplasmosisSerodiagnosisSerodiagnosis of Toxoplasmosisof Toxoplasmosis
Sabin Feldman Dye TestSabin-Feldman Dye TestImmunosorbent Agglutination Assay (ISAGA)Differential agglutination (AC/HS)gg ( )IgG avidity Test

Serodiagnosis of Toxoplasmosis
• Commercial or nonreference laboratories can easily perform this task.

Serodiagnosis of Toxoplasmosis
• Only positive results in IgM antibody tests need to be sent for confirmatory testing to referenceconfirmatory testing to reference laboratories

IgM test is used to help d t i i h th ti tdeterminie whether a patient has been infected recently orhas been infected recently or
in the distant past

Defect of IgM test for serodiagnosis of to oplasmosisserodiagnosis of toxoplasmosis
I M tib diIgM antibodies can i t f th tpersist for months to
thmore than one year

IgG avidity test have been introduced to h l di i i t b thelp discriminate between recently acquired andrecently acquired and distant infection.distant infection.

IgG avidity testIgG avidity testStudies of the kinetics of the avidity ofStudies of the kinetics of the avidity of IgG in pregnant women who have
t d d i t ti hseroconverted during gestation have shown that women with high avidity test results were infected with T. gondii at least 3 to 5 months earlier (time to (conversion from low to high avidity antibodies varies with the method used).antibodies varies with the method used).

Defect of IgG avidity testg y
low avidity antibodies may persistlow avidity antibodies may persist for many months.
Therefore low avidity antibodiesTherefore, low avidity antibodies does not necessarily indicate recently acquired infection.

What is solutionWhat is solutionWhat is solutionWhat is solutionBecause of the significantBecause of the significant potential of misinterpreting apotential of misinterpreting a positive IgM test result, confirmatory testing should be performedshould be performed

Confirmatory test for toxoplasmosisConfirmatory test for toxoplasmosis
A combination of serologicalA combination of serological tests is frequently required to q y qestablish whether an individual has been more likel infected inhas been more likely infected in the distant past or has been precently infected.

The TSP has been clinically helpful in th tti fthe setting of:
LymphadenitisLymphadenitisMyocarditisPolymyositisCh i ti itiChorioretinitisDuring pregnancyg p g y

For confirmatory testing, TSL-PAMFRI* ff l f t toffers a panel of tests
Sabin-Feldman Dye Test (DT)Sabin-Feldman Dye Test (DT)Double sandwich IgM ELISAIgA ELISAIgE ELISAIgE ELISAAC/HS testI G A idiIgG Avidity test
* Toxoplasma Serology Laboratory of the Palo Alto Medical F d i R h I i (TSL PAMFRI)Foundation Research Institute (TSL-PAMFRI)

Sabin-Feldman Dye Test (DT)Sabin Feldman Dye Test (DT)
◦Available mainly in reference◦Available mainly in reference laboratories◦Requires use of live organisms◦Considered the “gold standard”Considered the gold standard

Sabin-Feldman Dye Test (DT)Sabin Feldman Dye Test (DT)
A positive DT establishes that the patientA positive DT establishes that the patient has been exposed to the parasite. A negative DT essentially rules out priorA negative DT essentially rules out prior exposure to T. gondii (unless the patient is hypogammaglobulinemic)is hypogammaglobulinemic).However, in a small number of patients, I G tib di i ht t b d t t dIgG antibodies might not be detected within 2 to 3 weeks after the initial
t th itexposure to the parasite.

Sabin-Feldman Dye Test (DT)Sabin Feldman Dye Test (DT)
In addition rare cases ofIn addition, rare cases of toxoplasmic chorioretinitis and t l i h liti (TE) itoxoplasmic encephalitis (TE) in immunocompromised patients have been documented in patients negative for T. gondii-specific IgG g g p gantibodies.

IFAIFA◦Easier safer and more economical◦Easier, safer and more economical
than the Sabin–Feldman dye test and i ld ll l ltyields parallel results.
◦False positives obtained in patients with ANAwith ANA.

Differential agglutination (AC/HS)Differential agglutination (AC/HS)
The differential agglutination test (alsoThe differential agglutination test (also known as the "AC/HS test") uses two
ti ti th tantigen preparations that express antigenic determinants found early following acute infection (AC antigen) or in the later stages of infection (HS). g ( )

Differential agglutination (AC/HS)Differential agglutination (AC/HS)Differential agglutination (AC/HS)Differential agglutination (AC/HS)
This test has proved useful inThis test has proved useful in helping differentiate acute from chronic infections but is best used in combination with a panel ofin combination with a panel of other tests (e.g.: the TSP).

IgG Avidity TestIgG Avidity TestThe functional affinity of specificThe functional affinity of specific IgG antibodies is initially low after primary antigenic challenge and increases during subsequentand increases during subsequent weeks and months.

IgG Avidity TestIgG Avidity TestProtein denaturing reagentsProtein-denaturing reagents including urea are used to dissociate th tib d ti lthe antibody-antigen complex.
The avidity result is determined using the ratios of antibody titrationusing the ratios of antibody titration curves of urea-treated and untreated serumuntreated serum

IgG Avidity TestIgG Avidity TestClinical laboratories involved in theClinical laboratories involved in the care of pregnant women should be
th t idit t ti iaware that avidity testing is a confirmatory test and not the ultimate test for decision-making.

IgM-ELISAIgM-ELISADoes not differentiate between acuteDoes not differentiate between acute and chronic infection.FDA warns against use as the sole method of determining infection during pregnancy.

Double-Sandwich IgM-ELISADouble Sandwich IgM ELISA
This method avoids falseThis method avoids false positive results due to the ppresence of RF and ANA

IgA- ELISAIgA ELISA
IgA antibodies may be detected in sera ofIgA antibodies may be detected in sera of acutely infected adults and congenitally infected infants using ELISA or ISAGA methods.
A i t f I M tib di t th itAs is true for IgM antibodies to the parasite, IgA antibodies may persist for many months to more than one yearto more than one year

IgA- ELISAIgA ELISAThe increased sensitivity of IgA assays over y g yIgM assays for diagnosis of congenital toxoplasmosis represents an advance in diagnosis of the infection in the fetus anddiagnosis of the infection in the fetus and newborn

IgA-ELISAIgA ELISA
In a number of newborns withIn a number of newborns with congenital toxoplasmosis and
ti I M tib di thnegative IgM antibodies, the serological diagnosis has been established by the presence of IgA and IgG antibodies.g

IgE-ELISAIgE ELISA
IgE antibodies are detectable byIgE antibodies are detectable by ELISA in sera of acutely infected adults, congenitally infected infants, and childreninfected infants, and children with congenital toxoplasmic h i ti itichorioretinitis

IgE-ELISAIgE ELISA
The duration of IgE seropositivityThe duration of IgE seropositivity is less than with IgM or IgA antibodies and hence appears useful as an adjunctive method foruseful as an adjunctive method for identifying recently acquired i f tiinfections.

PanelPanelToxoplasma Pregnancy Panel (16 weeks gestation or earlier):I G (D T t) I M ELISA I G A iditIgG (Dye Test), IgM-ELISA, IgG AvidityToxoplasma Pregnancy Panel (more than 16 weeks gestation):IgG (Dye Test), IgM-ELISA, AC/HSIgG (Dye Test), IgM ELISA, AC/HS
Toxoplasma Infant Panel (less than 6 months of age):IgG (Dye Test), IgM-ISAGA, IgA-ELISA
Toxoplasma Panel (6 months of age or older):IgG (Dye Test), IgM-ELISA, IgA-ELISA, IgE-ELISA, AC/HSAC/HS

IgM -ISAGAThe test is simple to perform, does not require the use of enzyme conjugate and is read in the sameuse of enzyme conjugate, and is read in the same manner as the agglutination test.
Overall, it is more sensitive and specific than the IgM-IFA test.IgM IFA test.
The presence of RF or ANA does not cause false-The presence of RF or ANA does not cause falsepositive results in the IgM-ISAGA.

IgM -ISAGAIn adults, it is more sensitive but much less
ifi th th d bl d i h I Mspecific than the double-sandwich IgM-ELISA method.
In infants, the IgM-ISAGA is the most sensitive method and is used effectively for the diagnosis of congenital infection in infants 6 months of age or younger.

IgM -ISAGAA positive IgM-ISAGA test result in the first 10 d f lif h ld b t d ft 1010 days of life should be repeated after 10 days to rule out the possibility of maternal
t i ti f I M tib dicontamination of IgM antibodies.
The ISAGA method has also been used to detect IgA and IgE antibodies.


Molecular diagnosis of toxoplasmosisMolecular diagnosis of toxoplasmosis
Serological diagnosis can be difficult in g gprenatal cases or in patients with immunodeficiency.y
The use of molecular diagnosticThe use of molecular diagnostic techniques is particularly appropriate for such patientssuch patients

Molecular diagnosis of toxoplasmosisMolecular diagnosis of toxoplasmosisMolecular diagnosis of toxoplasmosisMolecular diagnosis of toxoplasmosis
It is generally accepted thatIt is generally accepted that fetuses or immunocompromissed ppatients with toxoplasmosis must be treated as earl as possiblebe treated as early as possible

Molecular diagnosis of toxoplasmosisg p
Appropriate treatment can thus beAppropriate treatment can thus be started earlier and serious
li i i h fcomplications in the foetus or immunocompromissed patients can p pbe prevented.

Molecular diagnosis of toxoplasmosisg p
It was proven that prenatal p ptreatment within 4 weeks of
i d d h i kseroconversion reduced the risk of intracranial lesions comparedof intracranial lesions compared with no treatment

Brain biopsy in Brain biopsy in toxoplasmic encephalitisp yp y p p
Although brain biopsy can establish aAlthough brain biopsy can establish a definitive diagnosis of TE, it is an i i d i k dinvasive and risky procedure associated with significant morbidity and mortality, while only half of the TE cases are confirmedTE cases are confirmed

Prenatal diagnosis of toxoplasmosisPrenatal diagnosis of toxoplasmosis
PCR performed on amnioticPCR performed on amniotic fluid has revolutionized the diagnosis of fetal T. gondiiinfectioninfection

Prenatal diagnosis of toxoplasmosisPrenatal diagnosis of toxoplasmosisPrenatal diagnosis of toxoplasmosisPrenatal diagnosis of toxoplasmosis
A negative result from PCRA negative result from PCR performed on amniotic fluid pcannot rule out congenital i f iinfection.

Prenatal diagnosis of toxoplasmosisPrenatal diagnosis of toxoplasmosisg pg p
The rate of false negatives isThe rate of false negatives is variable according to the centres

Sequence targets & Protocoles in l l di i f l imolecular diagnosis of toxoplasmosis
V i dVarious sequence targets and PCR protocols have beenPCR protocols have been developed for molecular pdiagnosis of toxoplasmosis

B1 geneB1 geneFor detection of T gondii theFor detection of T. gondii, the sequence used most frequently is the B1 gene, which there are 35 copies in the genomecopies in the genome
Its high specificity is now well-establishedestablished

529-bp sequence529 bp sequence
Th i ifi fThe sequence is specific for T gondii which has overT. gondii, which has over 300 copies in the genome300 copies in the genome

Real-time PCRReal time PCRReal-time PCR is very sensitive yand is a promising technique that i bl f idiis capable of providing a quantitative result.quantitative result.

ComparisionComparision REPREP--529529 and Band B11 genegeneComparisionComparision REPREP 529 529 and Band B1 1 genegene
Real-time PCR using the REP-529 gTaqman probes was more efficient than B1 gene amplification for thethan B1 gene amplification for the diagnosis of congenital toxoplasmosis

Comparison REPComparison REP--529529 and Band B11 genegeneComparison REPComparison REP 529 529 and Band B1 1 genegene
In a study REP 529 sequenceIn a study REP-529 sequence was detected in all 20 samples pfrom patients with congenital
l i htoxoplasmosis, whereas B1 gene sequence was detected ingene sequence was detected in only 16 of the 20 specimens y p

Comparison REPComparison REP--529529 and Band B11 genegeneComparison REPComparison REP 529 529 and Band B1 1 genegene
A comparison of methods using theA comparison of methods using the B1 and 529-bp sequences with real-time PCR revealed a ten-fold improvement in sensitivity when theimprovement in sensitivity when the 529-bp sequence was used

Comparison REPComparison REP--529529 and Band B11 genegeneComparison REPComparison REP 529 529 and Band B1 1 genegene
Under specific conditions theUnder specific conditions, the detection limit for T. gondiiggenomic DNA was 200 fg for the B1 gene compared to 20 fg forB1 gene, compared to 20 fg for the 529-bp sequence p q

Interlaboratory EvaluationInterlaboratory Evaluation In an attempt to establish standardisedIn an attempt to establish standardised methodology, the EU BioMed 2 Programme performed an anonymous test of protocols used in 15 European laboratories.
The participating laboratories were required to p p g qdetect T. gondii in 12 'artificial samples' of amniotic fluid (four negative, eight positive)

Interlaboratory EvaluationInterlaboratory Evaluation Two laboratories identified all samples correctlyThree laboratories failed to detect the sample containing T. gondii at the lowest concentration (one tachyzoite/mL), without any false-positive results. There were also laboratories that failed to detect T. gondii in any of the samplesFour laboratories reported at least oneFour laboratories reported at least one negative control as positive.

PerspectivePerspectiveReal-Time PCR:short-term quantitative resultquantitative result fewer handling steps.
Application of this technique is limited at b f h l i l hi h fpresent because of the relatively high costs of
the necessary equipment.


TOXOPLASMOSIS IN THEIMMUNOCOMPETENT PATIENT
IgG and IgM antibodies should be used for initial evaluation of immunocompetentpatients.
Testing of serial specimens obtained 3 weeks apart (in parallel) provides the best p ( p e ) p ov des e besdiscriminatory power if the results in the initial specimen are equivocalp q

TOXOPLASMOSIS IN THEIMMUNOCOMPETENT PATIENT
Histologic diagnosis can be useful in some cases of suspected toxoplasmosis
Endomyocardial biopsy and biopsy of skeletal l h b f ll d t t bli h Tmuscle have been successfully used to establish T.
gondii as the etiologic agent of myocarditis and polymyositis in the rare casespolymyositis in the rare cases
Isolation studies and PCR have rarely proved usefulIsolation studies and PCR have rarely proved useful in immunocompetent patients.

TOXOPLASMOSIS IN THEIMMUNODEFICIENT PATIENT
In patients with AIDS and toxoplasmosis, the IgGtiter may be relatively low, and tests for IgM, IgA,
d I E tib di b tiand IgE antibodies may be negative.
A d fi iti di i f t l i i thA definitive diagnosis of toxoplasmosis in the immunodeficient patient relies on:
Histologic demonstration of the parasite• Histologic demonstration of the parasite• Detection of T.gondii DNA
I l ti f th it• Isolation of the parasite

TOXOPLASMOSIS IN THEIMMUNODEFICIENT PATIENT
The presence of tachyzoites is diagnostic of active infection.
The presence of a solitary T. gondii tissue cyst e p ese ce o a so ta y . gondii t ssue cystmay only reflect chronic infection unless it is associated with an area of inflammationssoc ed w e o o
Visualization of several tissue cysts virtuallyVisualization of several tissue cysts virtually always means that active infection is present.

TOXOPLASMOSIS IN THEIMMUNODEFICIENT PATIENT
Brain biopsy should be considered in immunodeficient patients with presumed f p pTE if:• A single lesion is seen on MRI• A single lesion is seen on MRI• An IgG antibody test result is negative• An inadequate clinical response

TOXOPLASMOSIS IN THEIMMUNODEFICIENT PATIENT
An impression smear of the brain biopsy specimen can be made and immediately examined for the presence of tachyzoites using the conventional staining

TOXOPLASMOSIS IN THEIMMUNODEFICIENT PATIENT
In addition to H&E staining, T. gondii-specific immunoperoxidase staining p f p gshould be performed.

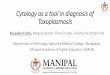
Toxoplasma gondii, purulent meningitispurulent meningitis
Oil immersion observation discloses that banana-shaped or crescentic tachyzoites (a proliferative form) possess a single nucleus (HE).
Image Source Page: http://pathy.fujita-hu.ac.jp/~tsutsumi/case/case105.htm

Toxoplasma gondii, purulent meningitispurulent meningitis
Indirect immunoperoxidase staining using a 1:500Indirect immunoperoxidase staining using a 1:500 diluted human serum with high Toxoplasma antibody titer demonstrates positive membrane signals on the disseminated tachyzoites
Image Source Page: http://pathy.fujita-hu.ac.jp/~tsutsumi/case/case105.htm

TOXOPLASMOSIS IN THEIMMUNODEFICIENT PATIENT
Because the amount of brain tissue obtained at aspiration or biopsy is usually p p y ysmall, sufficient tissue for mouse inoculation may not be available;inoculation may not be available; however, this should be performed whenever feasiblewhenever feasible

TOXOPLASMOSIS IN THEIMMUNODEFICIENT PATIENT
PCR has been used successfully in brain tissue to diagnose TE, but a positive result should be i t t d ith ti b it tinterpreted with caution because it may not distinguish a patient with TE from one withlatent infection (asymptomatic carrier of brain tissuelatent infection (asymptomatic carrier of brain tissue cysts) who has CNS pathology due to a process other than toxoplasmosis.p

TOXOPLASMOSIS IN THEIMMUNODEFICIENT PATIENT
In the appropriate clinical setting, it is important to include toxoplasmosis in the differential diagnosis of pulmonary symptoms, particularly in those individuals with interstitial infiltrates.
Wright-Giemsa stain and PCR of BALWright Giemsa stain and PCR of BAL specimens are useful for the diagnosis of pulmonary toxoplasmosispulmonary toxoplasmosis

TOXOPLASMOSIS IN THEIMMUNODEFICIENT PATIENT
In patients with visual symptoms in whom toxoplasmic chorioretinitis is a possibility, PCR examination of vitreous or aqueous fluid can be considered and is particularly helpful in patients with atypical clinical features of toxoplasmic chorioretinitis.'

OCULAR TOXOPLASMOSIS
Low titers of IgG antibody are usual in patients with active chorioretinitis due to reactivation of congenital gondii infection; IgM antibodies are not usually detected.
When sera from such patients are examinedpin the dye test, they should be titered beginning with undiluted serum because, inbeginning with undiluted serum because, in some cases, the conventional initial dilution of 1: 16 may be negative.1: 16 may be negative.

OCULAR TOXOPLASMOSIS
In most cases, toxoplasmicchorioretinitis is diagnosed bychorioretinitis is diagnosed by ophthalmologic examination, and
i i l h di d iempirical therapy directed against the organism is often instituted based gon clinical findings and serologic test resultsresults.

OCULAR TOXOPLASMOSIS
In a number of patients, the morphology of the retinal lesion or lesions may be nondiagnostic or, the
t t t t b b ti l b thresponse to treatment may be suboptimal or both.
I h th d t ti f b l T diiIn such cases, the detection of an abnormal T. gondii-antibody response in ocular fluids or PCR has been used successfully to establish the diagnosis orused successfully to establish the diagnosis or demonstration of the parasite by isolation, histopathology.p gy

CONGENITAL INFECTION IN THEFETUS AND NEWBORN
Prenatal diagnosis of congenital toxoplasmosis is currently based on ultrasonography and amniocentesis.
PCR on amniotic fluid for the detection of T. gondii-specific DNA performed at 18 weeks of gondii specific N pe fo med at 8 weeks ofgestation or later is more sensitive, more rapid, and safer than conventional diagnostic p , gprocedures involving fetal blood sampling.

CONGENITAL INFECTION IN THEFETUS AND NEWBORN
Amniotic fluid should be tested by PCR in all cases with serologic test results diagnostic of or highly
ti f t i d i f ti d isuggestive of acute acquired infection during pregnancy and also if there is evidence of fetal damage on ultrasound examination (e gdamage on ultrasound examination (e.g., hydrocephalus and/or calcifications).
PCR on amniotic f1uid had a sensitivity of 64%, specificity of 100%, positive predictive value of p y , p p100%, and negative predictive value of88%.

CONGENITAL INFECTION IN THEFETUS AND NEWBORN
Maternal IgG antibodies present in the newborn may reflect either past or recent infection in the
thmother.
F thi t t f th d t ti f I A dFor this reason, tests for the detection of IgA and IgM antibodies are commonly used for the diagnosis of infection in the newbornof infection in the newborn.
The demonstration of IgA antibodies seems to beThe demonstration of IgA antibodies seems to be more sensitive than the detection of IgM antibodies for establishing infection in the newborn.g

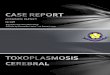
IgG/lgMIdeally, requested at first prenatal visit or preconception
IgG-/lgM- IgG+/lgM- IgG-/lgM+ IgG+/lgM+
Woman has not been infected with T. gondii; risk for CTonly if primary i f i i i
<18 weeksInfection acquired prior to
i k f C T i
Repeat IgG/lgMin 2 to 3 weeksor send to areferencelaboratory
Serum should be sent to reference laboratory
Confirmatory serologic infection is acquired during gestation. IgG/lgM should be tested throughout pregnancy in order
pregnancy; risk for C.T. is essentially non-existent unless patient is immunocompromisedNo further action required
IgG-/lgM+
y gtests are performed at reference lab. Results are consistent with
an acute infection acquired to detect seroconversion. In some countries (e.g., France) IgG (-) women are tested
f q>18 weeksIt is difficult to distinguish between infection acquired during pregnancy vsacquired in the distant past
IgM positive result has no
during gestation Risk for CT. Treatment should be initiated Amniotic fluid PCR and monthly U/S shouldbe performed.
every month acquired in the distant past (e.g., patient may have been infected early in pregnancy and become IgM negative) Consultation with a reference
clinical relevance.Manage asIgG ( )/lgM
an infection acquired prior to gestationNo risk for CT unless patient is immunocompromised
laboratory is recommended IgG (-)/lgM(-) patient equivocal interpretation:
usually requires follow-up serum and consultation withmedical experts in toxoplasmosis

Detection of cases depends h li i i d hon the clinician and the
laboratorylaboratory
i il !Be vigilant!

ش شف ش ش گل و چون گل خوشرو و شادی بخشموفق باشيد

Laboratory diagnosis of amebiasis
Dr Mehrzad SaraeiDr Mehrzad Saraei
Qazvin University of Medical Sciences

EntamoebaEntamoeba histolyticahistolyticayyEntamoeba histolytica is well recognized as a pathogenic ameba associated witha pathogenic ameba, associated with intestinal and extraintestinal infections.
The other species are important because they b imay be confused with E. histolytica in
diagnostic investigations


Cysts are typically found Trophozoites are typically y yp yin formed stool.
p yp yfound in diarrheal stool

Clinical FeaturesClinical Features• Asymptomatic infection•Intestinal amebiasis (dysentery, colitis, appendicitis, toxic megacolon, amebomas)• Extraintestinal amebiasis (liver• Extraintestinal amebiasis (liver abscess, peritonitis, pleuropulmonaryabscess cutaneous and genital amebicabscess, cutaneous and genital amebic lesions).

Flask-shaped ulcer of invasiveulcer of invasive
intestinal amebiasis

dysentery showing diffuse ulceration ofulceration of mucosa
/A2006http://www.stanford.edu/group/parasites/ParaSitesmoebiasis/clinicalpresentations.html

Gross PathologyGross Pathology of amoebic liver abscess
/A2006http://www.stanford.edu/group/parasites/ParaSitesmoebiasis/clinicalpresentations.html

Abscesses on the skin
d/kenyan/ameobaisis.html4http://www.gg.rhul.ac.uk/ict

This amebiasis patient ppresented with tissue destruction, and
l i f hgranulation of the anoperineal region due to an Entamoebato an Entamoeba histolytica infection.
.html6635http://www.rightdiagnosis.com/phil/html/amebiasis/

Patient with amoebiasis liver absess, withabsess, with perforation of abscess through abdominal skinskin
/A2006http://www.stanford.edu/group/parasites/ParaSitesmoebiasis/clinicalpresentations.html

Laboratory Diagnosis of Laboratory Diagnosis of amoebiasisamoebiasisabo ato y iagnosis ofabo ato y iagnosis of amoebiasisamoebiasis
MicroscopyMicroscopyImmunodiagnosisMolecular Methods

MicroscopyMicroscopy• Inadequacies of the stool examination qhave been appreciated since at least 1978
• Surprisingly 30 years later the stool• Surprisingly, 30 years later, the stool examination remained the most common test ordered by United States physicianstest ordered by United States physicians when intestinal amebiasis was suspectedsuspected.

Stool Examination•Fresh stool or Concentrates from fresh stool: •wet mounts, with or without iodine stain•permanently stained preparations (e.g., p y p p ( g ,trichrome).
Concentration procedures are not useful for demonstrating trophozoitesfor demonstrating trophozoites

MicroscopyEntamoeba histolytica must be differentiated from other intestinal ff fprotozoa including:E coliE. coliE. hartmanniE d liEndolimax nanaIodamoeba buetschliiDientamoeba fragilisEntamoeba polecki.p

15 to 20 µm (range 10 to 60 µm)
Entamoeba histolytica Trophozoite inEntamoeba histolytica. Trophozoite in fecal smear (saline wet mount, high power). Numerous ingested erythrocytes are present in the cytoplasm, but the nucleus is not visible.
.htm4/web/ehisto50249http://ruby.fgcu.edu/courses/davidb/

Direct Wet mount stained
with iodinewith iodine
Trophozoites of E. histolytica/E. dispar in a direct wet mount stained with iodine

Direct Wet mount stainedmount stained
with iodine
T h it f E hi t l ti /E diTrophozoites of E. histolytica/E. disparin a direct wet mount stained with iodine

Trophozoites of E. histolytica/E. disparstained with trichrome

Permanent smear stainedsmear stained
with T i hTrichrome
Trophozoite of E. histolytica/E. dispar,Trophozoite of E. histolytica/E. dispar, measuring approximately 16.7 µm, stained with trichrome

Permanent smear stained
withwith Trichrome
Erythrophagocytosis is the only characteristic that can be used to differentiate morphologically E. histolyticafrom the nonpathogenic E. dispar

Trophozoites of E. histolytica with ingested erythrocytes stained
ith t i hwith trichrome

Cyst of E. histolytica/E. dispar in an unstained concentrated wet mount of stool
Mature E. histolytica/ E. dispar cysts :• 1-4 nuclei have centrally located kar osomes and finekaryosomes and fine, uniformly distributed peripheral chromatin.peripheral chromatin.• usually measure 12 to 15 µm.
Notice the chromatoid body with blunt, rounded ends (arrow).

E. histolytica/E. dispar cyst with three visible nuclei

Cyst of E. histolytica/E. dispar in a Cys o . istolytica/ . dispaconcentrated wet mount stained with iodine

E. histolytica/E. dispar cyst in iodine with one visible nucleus and a glycogen vacuole
E. histolytica/E. dispar cyst

Cyst of E. histolytica/E. dispar in a concentrated wet mount stained with iodine
Cyst of E. histolytica/E. dispar

Cyst of E. histolytica/E. dispar stained with Trichrome
Th l i i ibl i th f l l (bl kThree nuclei are visible in the focal plane (black arrows), and the cyst contains a chromatoid body with typically blunted ends (red arrow).

Cyst of E. histolytica/E. dispar stained with Trichrome
Notice the chromatoid body with blunt, rounded ends (arrow).


Other intestinal amebae that may be mistaken for E histolytica/E disparE. histolytica/E.dispar



Cyst of E. nanain a direct wetin a direct wet mount stained with iodine

Cysts of E. nana stained with trichrome

Trophozoites of E. nana stained with trichrome

Trophozoites of E. nana stained with trichrome

Cyst of E. coli in a concentrated wet mount stained with iodine. Five nuclei are visible in this focal plane

Cyst of E. coli in a concentrated wet mount stained with iodine. Seven nuclei are visible in this focal planep

Mature cyst of E. coli, stained with trichrome
a trophozoite of Endolimax nana can be se

Mature cyst of E. coli, stained with trichrome

Immature cyst of E. coli, stained with trichrome
Notice the presence of only two nuclei, and a large glycogen vacuole

Mature cyst of E. coli, stained with trichromey
five nuclei are visible in the shown focal plane

Trophozoites of E. coli stained with trichrome

Trophozoites of E. coli stained with trichrome

Cyst of an E. hartmanni in a wet mount, stained with iodine

Cyst of E. hartmanni stained with trichrome
Notice the bluntly-ended chromatoid bodies

Trophozoite of E. hartmannistained with trichrome

Trophozoite of E. hartmanni stained with trichrome.
In the upper-right of the image is a cyst-like body of Blastocystis hominis

Entamoebahistolytica/dispar
Entamoebahartmanni
Entamoeba coli Entamoebapolecki
Endolimaxnana
Iodamoebabeutschlii
Amoebae
____10 µm

What is main problem?The main problem for microscopy detection is defferentiation of Edetection is defferentiation of E. histolytica from E. dispar and E. moshkovskii.

Why?Because it is not possible with a stool examination to distinguishstool examination to distinguish morphologically the three closely related and common amebae: pathogenic E histolytica andpathogenic E. histolytica and commensal E. dispar and E.
hk kiimoshkovskii.

MicroscopyThe presence of ingested erythrocyteswas the sole morphologicwas the sole morphologic characteristic that was of some use in identifying E. histolytica

MicroscopyIn one study, erythrocytes were present in only 68% of cases of Epresent in only 68% of cases of E. histolytica but also present in 16% of cases of E. dispar.

MicroscopyThe problems with stool examination were magnified by the fact that onlywere magnified by the fact that only 5% (3) of the 65 positive results for E. histolytica/E.dispar complex were in fact E. histolyticay

In most industrialized countries, E. dispar is 10 times more commondispar is 10 times more common than E. histolytica and even in a developing country, E. histolyticaand E dispar can be equallyand E. dispar can be equally prevalent.

In a study of preschool children from an urban slum in Bangladesh:from an urban slum in Bangladesh:E. moshkovskii: 21 %E. histolytica: 16%E di 36%E. dispar: 36%

MicroscopyIn a study from Tanzania of approximately 100 HIV infectedapproximately 100 HIV-infected individuals with diarrhea:E. moshkovskii: 13%E hi l i 4%E. histolytica: 4%E dispar: 5%E. dispar: 5%

MicroscopyIn Sydney, Australia, 50% of E b i id tifi dEntamoeba organisms identified by stool O&P examination wereby stool O&P examination were E. moshkovskii

MicroscopyConclusion
stool O&P examination suffers from insensitivity and thefrom insensitivity and the inability to distinguish E. histolytica from E. dispar and E moshkovskiiE. moshkovskii

Culture of Culture of E. E. histolyticahistolyticayyIs available in only a few research laboratories
id idworidwide Sensitivity: stool exam< Culture<antigen detection
PCRor PCRNot specific for E. histolytica
Thus an E. histolytica-specific antigen detection or PCR test must be used on the cultured material.

Colonoscopy & Biopsy•helpful in the diagnosis of intestinal amebiasis. • Amebas can be difficult to visualize in the biopsy samples•PAS or, ideally, immunoperoxidase with anti-, y, pE. histolytica antibodies, can help to identify the parasites.p• A limitation of colonoscopy is that it is an invasive procedure and not widely availableinvasive procedure and not widely available in developing nations.

Trophozoites of E. histolytica in a colon biopsy specimen, stained with hematoxylin and eosin (H&E).

Trophozoites of E. histolytica in a perianal biopsy specimens, stained with H&E.

ImmunodiagnosisgAntibody DetectionyAntibody detection is most useful in patients with extraintestinal amoebiasispatients with extraintestinal amoebiasis(i.e., amebic liver abscess) when organisms are not generally found onorganisms are not generally found on stool examination.

Antibody DetectionctionyELISA test detects antibody specific for E. histolytica in approximately :• 95% of patients with extraintestinal amebiasis• 70% of patients with active intestinal infection• 10% of asymptomatic persons who are passing y p p p gcysts of E. histolytica.

Antibody DetectionyIf antibodies are not detectable in patients with an acute presentation of suspected amebic liver abscess, a second specimen should be drawn 7-10 days later.

Antibody Detectiony
If the second specimen does not show seroconversion, other agents should be , gconsidered.

Limitation of Antibody Detectiontat o o t body etect o
Detectable E. histolytica-specific antibodies may persist for years after successful treatment, so the presence of antibodies does not necessarily indicate acute or current infection.

Antibody DetectionyThe IHA and EIA tests are more suitable for laboratories that have frequent requests for amebiasisfrequent requests for amebiasisserology.

Antibody DetectionyMicrotiter ELISA ,ImmunoTab and IHA were compared in one study of amebic liver abscess patients from Kuwait.
All three tests had equal sensitivities of 98%All three tests had equal sensitivities of 98% to 99%. The ImmunoTab and Microtiter ELISA specificities were 95%, less than theELISA specificities were 95%, less than the 99.8% calculated specificity of the IHA.

Antibody DetectionyIn a study in Egypt, IgG antibodies to the Gal/GalNAc lectin were found in the sera of:89% of patients with amebic colitis 86% ( i ) f ti t ith86% (six) of seven patients with intestinal amebiasisGal/GalNAc lectin is a novel multifunctional virulence factor of the human parasite Entamoeba histolyticahuman parasite Entamoeba histolyticagalactose (Gal) and N-acetyl-D-galactosamine (GalNAc) inhibitable lectin

Antibody DetectionyAlthough detection of IgM antibodies g gspecific for E. histolytica has been reported, sensitivity is only about 64%reported, sensitivity is only about 64% in patients with current invasive diseasedisease.

Antibody Detectiony
Although the immunodiffusion test is as specific, it is slightly less sensitive than the IHA d EIA d i i i f 24IHA and EIA and requires a minimum of 24 hours to obtain a result, in contrast to 2 hours required for the IHA or EIA testshours required for the IHA or EIA tests.
H h i li i f h dHowever, the simplicity of the procedure makes it ideal for the laboratory that has only an occasional specimen to testonly an occasional specimen to test.

Antibody DetectionyConclusionConclusion
Antibody detection is an important f h di i f i i l dpart of the diagnosis of intestinal and
extra intestinal amebiasis.

Antibody DetectionyConclusionConclusion
Antibody detection can be particularly h l f l h E hi t l ti ifi t lhelpful when E. histolytica-specific stool diagnostic techniques (antigen detection or PCR) are not available

Antigen detectiongAntigen detection may be useful as g yan adjunct to microscopic diagnosis in detecting parasites and canin detecting parasites and can distinguish between pathogenic and nonpathogenic infections.

Antigen Detectiong
Recent studies indicate improved sensitivity and specificity of fecal y p yantigen assays with the use of monoclonal antibodies which canmonoclonal antibodies which can distinguish between E. histolytica and E. dispar infectionsdispar infections.

Antigen DetectiongThe only fecal antigen test that disting ishes E hi t l ti from E didistinguishes E. histolytica from E. disparand E. moshkovskii is the TechLab E. histolytica II enzyme-linkedhistolytica II enzyme linked immunosorbent assay (ELISA).
This microwell ELISA,which detects the Gal/GalNAc adherence lectin of E. histolytica, is more sensitive than stool O&P examination or culture, and it is rapid (<2 hours)(<2 hours).

Antigen DetectiongIn one study, the TechLab E. histolytica II assay detected Gal/GalNAc lectin in the sera of 96% (22) of 23 patients with amebic liver abscess before they underwent treatment with the antiamebic drug metronidazole.g

Antigen DetectiongFor liver abscess pus, it was 41% to 74% psensitive for detection of the parasite.
Furthermore, for stool specimens ll d h i f di i fcollected at the time of diagnosis of
amebic liver abscess (and before metronidazole treatment), it detected the parasite in 43% (3 of 7).p % ( )

Molecular diagnosisReal-time PCR is superior in sensitivity to stool antigen detection but gunfortunately is still a technically complex means for the diagnosis ofcomplex means for the diagnosis of amebiasis.
Real-time PCR is more sensitive than conventional PCR.

Molecular diagnosisReal-time PCR is also a sensitive test for detection of E. histolytica in liver abscess pus.
In one study, Real-Time PCR yielded positive o e study, eal ime C y e ded pos t veresults in 20 of 23 liver abscess pus specimens; the 3 specimens with negative spec e s; e 3 spec e s w eg vefindings had been collected from patients who had already received antiamebic therapy (8 y py (days for one patient and 30 days for two patients).p )

Molecular diagnosisgIn reference diagnosis laboratories, g ,molecular analysis by PCR-basedassays is the method of choice forassays is the method of choice for discriminating between the pathogenic species (E. histolytica) and the nonpathogenic species (Eand the nonpathogenic species (E. dispar).

ConclusionTechLab E histolytica II ELISAantigenTechLab E. histolytica II ELISAantigen detection test has sensitivity and
ifi it i t th f t l O&Pspecificity superior to those of stool O&P examination, and its sensitivity inferior but its specificity comparable with those of PCR, but it is technically simpler to y pperform.