Embed Size (px)
Citation preview

Advantages and disadvantages of different Advantages and disadvantages of different left atrial appendage closure systems.left atrial appendage closure systems.
Chair and 1st Department of Cardiology, Chair and 1st Department of Cardiology,
Poznan University of Medical Sciences, PolandPoznan University of Medical Sciences, Poland
Marek Grygier MD, PhD

www.escardio.org/guidelines European Heart Journal (2010) 31, 2369-2429
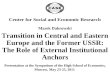
Approach to thromboprophylaxis in AF
AF = atrial fibrillation; CHA2DS2-VASc = cardiac failure, hypertension, age ≥ 75 (doubled), diabetes, stroke (doubled)-vascular disease, age 65–74 and sex category (female); INR = international normalized ratio; OAC = oral anticoagulation, such as a vitamin K antagonist (VKA) adjusted to an intensity range of INR 2.0–3.0 (target 2.5).

1-year bleeding risk assocciated with antithrombotic treatment
0
2
4
6
8
10
12
14
0 1 2 3 4 5 6 7 8 9
Euro Heart Survey
HAS-BLED score
Number of patients 798 1286 744 187 46 8 2 0 0 0
Number of bleeding episodes
9 13 14 7 4 1 0 0 0 0
Charakterystyka kliniczna Punkty
Nadciśnienie tętnicze (ciśnienie skurczowe >160 mm Hg)
1
Zaburzenia funkcji nerek lub wątroby 1 + 1
Udar mózgu 1
Krwawienie 1
Labilne wartości INR 1
Osoby w podeszłym wieku, >65 roku życia 1
Leki lub alkohol 1 + 1
Wynik całkowity Zakres 0-9
Pisters R et al. Chest 2010;138:1093–1100.

Mechanism of stroke in patients with AF.
blood flow in the LAA is slowed and can become
turbulent in the case of AF
a clot can form in the LAA which can embolize and cause a
stroke

Published reports of patients with non-rheumatic AF found thrombus present
in 12.6% of patients
90% of the thrombus was found in the LAA


7 SH-159501-AA MAY 2013
The Wind Sock Type LAA is an anatomy in which one dominant lobe of sufficient length is the primary structure.
The Chicken Wing Type LAA is an anatomy whose main feature is a sharp bend in the dominant lobe of the LAA anatomy at some distance from the perceived LAA ostium.
The Broccoli Type LAA is an anatomy whose main feature is an LAA that has limited overall length with more complex internal characteristics.
Major left atrial appendage types

8 SH-159501-AA MAY 2013
3. Assessment of LAA Dimensions
Assessment of LAA Dimensions

Surgical closure of the LAA.

Surgical closure of the LAA.

Percutaneous closure of the LAA

Percutaneous closure of the LAA- history …

What did the PLAATO data say ?
mean CHADS SCORE 2.5±1.3 expected annual risk of stroke: 6.5% follow-up: 3.2% stroke stroke risk reduction: 51%

Percutaneous closure of the LAA- what about tooday …

WATCHMAN LAA Closure Technology
The WATCHMAN device reduces the risk of stroke by closing off the left atrial appendage, which is known to be the main source of blood clots in patients with atrial fibrillation
Johnson, Eur J Cardiothoracic Surg 2000:17

16 SH-159501-AA MAY 2013
Frame: Nitinol structure• Available sizes:
– 21, 24, 27, 30, 33 mm (diameter)
– 10 Fixation anchors around device perimeter engage LAA tissue
– Contour shape accommodates most LAA anatomy
Fabric Cap: (PET) Fabric Polyethyl terephthalate
• Prevents harmful emboli from exiting during the healing process
• 160 micron filter
Anchors
PET fabric
WATCHMAN® LAA Closure System ComponentsWATCHMAN® LAA Closure System ComponentsWATCHMAN Device

17 SH-159501-AA MAY 2013
Double Curve
Single Curve
Transseptal Access System
• Double, Single, Anterior Curves
• 14F O.D. (4.7 mm), 12F I.D.
• 75 cm working length
Preformed curve shapes guide position in LAA
WATCHMAN® LAA Closure System ComponentsWATCHMAN Access System

18 SH-159501-AA MAY 2013
Constrained Device
Distal Marker Band
Hemostasis Valve
Core Wire
Deployment Knob
12F O.D. (compatible with all 5 device sizes)
WATCHMAN® LAA Closure System ComponentsWATCHMAN Delivery System

19 SH-159501-AA MAY 2013
All criteria must be met prior to device release
Position – device is distal to or at the ostium of the LAA
Anchor – (stability) fixation barbs engaged / device is stable
Size – device is compressed at least 8-20% of original size
Seal - device spans ostium, all lobes of LAA are covered
• If necessary, device can be recaptured (partial or full)
Device Release Criteria (PASS)

20 SH-159501-AA MAY 2013
Device Release Criteria – OPTIMAL POSITION
Fixation anchors engage LAA wall

PROTECT AF1,6 CAP2 ASAP3,4 PREVAIL5
Trial Design
Prospective RCT with patients able to
take warfarin
Prospective registry with patients able to take
warfarin
Prospective registry with patients contraindicated for
warfarin
Prospective RCT with patients able to take
warfarin
Outcome
WATCHMAN was non-inferior to
warfarin in patients at high-risk of
thromboembolism
Significantly improved safety results from early
PROTECT AF experience
Ischemic stroke rate significantly reduced in
warfarin contra-indicated patients
WATCHMAN device was safely implanted
by new operators
Mean age /CHADS2 72/2.2 74/2.4 72.4/2.8 74/2.6
Total Enrolled Subjects 707 randomized1 93 pts rolled in2 460 150 461
Total Patients Implanted 5422 437 142 269
Implantation Success 89.5%2 95.0% 94.7% 95.1%
Primary Efficacy (all-stroke, CV/unexplained
death, and systemic embolism)
40% reduction vs. warfarin6
29% reduction vs. warfarin N/A
0.064Identical 18-month rates
for WATCHMAN and warfarin
All-Stroke 32% reduction vs. warfarin6
23% reduction vs. warfarin
77% reduction vs. expected rate per CHADS₂ score
Data not yet available
Safety(7 day procedure-related*)
8.7%5
4.1%5
53% reduction vs. PROTECT AF
Pericardial effusion with tamponade=1.3%
Major bleeding=2.7%
4.4%49% reduction vs.
PROTECT AF
*Composite of vascular complications includes cardiac perforation, pericardial effusion with tamponade, ischemic stroke, device embolization, and Includes observed PE not necessitating intervention, AV fistula, major bleeding requiring transfusion, pseudoaneurysm, hematoma and groin bleeding
1 Holmes DR et al. Lancet 2009;374:534–42; 2 Reddy VY et al. Circulation. 2013; 127:720-729; 3 Sievert H. TCT 2011; 4 Reddy, JACC 2013; 5 Homes DR PREVAIL Mar 2016 Reddy, et al. HRS LBCT 2013
WATCHMAN™ Clinical ProgramAt 4yrs WATCHMAN was superior to warfarin in primary efficacy, all-cause mortality, & cardiovascular death
SH
-AA
-15
990
1-M
AY
20
13

PROTECT AF
SH
-AA
-15
990
1-M
AY
20
13

Patient Study Timeline:
Device subject takes Device subject takes warfarinwarfarinPreimplant intervalPreimplant interval
Day 0Day 0
Control subject takes warfarinControl subject takes warfarin
Device subject gets implantDevice subject gets implant
Device subject has ceased Device subject has ceased warfarinwarfarin
Ongoing to 5 yearsOngoing to 5 years
RandomizeRandomize
Day 0Day 0Day 45Day 45postimplantpostimplantDay 2-14Day 2-14 Ongoing to 5 yearsOngoing to 5 years
Dev
ice
Dev
ice
Control
Control
3000838-60

PROTECT AF Trial Endpoints
• Primary Efficacy EndpointPrimary Efficacy Endpoint• All stroke: ischemic or hemorrhagic All stroke: ischemic or hemorrhagic
• deficit with symptoms persisting more than 24 hours or deficit with symptoms persisting more than 24 hours or • symptoms less than 24 hours confirmed by CT or MRIsymptoms less than 24 hours confirmed by CT or MRI
• Cardiovascular and unexplained death: includes sudden death, Cardiovascular and unexplained death: includes sudden death, MI, CVA, cardiac arrhythmia and heart failure MI, CVA, cardiac arrhythmia and heart failure
• Systemic embolizationSystemic embolization
• Primary Safety Endpoint Primary Safety Endpoint • Device embolization requiring retrievalDevice embolization requiring retrieval• Pericardial effusion requiring interventionPericardial effusion requiring intervention• Cranial bleeds and gastrointestinal bleedsCranial bleeds and gastrointestinal bleeds• Any bleed that requires ≥ 2uPRBCAny bleed that requires ≥ 2uPRBC
• NB: Primary effectiveness endpoint contains safety eventsNB: Primary effectiveness endpoint contains safety events

Inci
denc
e R
ate
(%)
Warfarin GroupN=244
WATCHMAN Group
N=463
PNI = >99.9% PNI = >99.9%PNI = 99.3% PNI = >99.9%
PNI = Posterior non inferiority ProbabilitiesUnexplained Death
38% lower 29% lower
PROTECT AF – Primary Efficacy Endpoint – 1065 pt yrs
38% Reduction
David R Holmes, Lancet Vol 374 August 15, 2009


CAP
SH
-AA
-15
990
1-M
AY
20
13

WATCHMAN™ PROTECT-AF & Continued Access Protocol (CAP)
Reddy VY et al. Circulation. 2011;123:417-424
SH
-AA
-15
990
1-M
AY
20
13

WATCHMAN™ PROTECT-AF & Continued Access Protocol (CAP)
Reddy VY et al. Circulation. 2011;123:417-424
67
58
50
40455055606570
PROTECT AF Early PROTECT AFLate
CAP
Average Time (Minutes)
Procedure Time
8891
95
80
85
90
95
100
PROTECT AFEarly
PROTECT AFLate
CAP
Success %
Implant Success
83
9195
70
80
90
100
PROTECT AFEarly
PROTECT AFLate
CAP
Discontinuation %
45 Day Discontinuation Rate Among Implanted
With experience procedure time decreased by 30% Implant success improved to 95%
Warfarin cessation increased to 95%
With increased operator experience
The average procedure time reduced from 67 minutes to 50 minutes
Implant success improved from 88% to 95%
Discontinuation of Warfarin improved from 83% to 95% of patients
SH
-AA
-15
390
2-A
PR
201
3

WATCHMAN™ PROTECT-AF & Continued Access Protocol (CAP)
Reddy VY et al. Circulation. 2011;123:417-424
10
5,53,7
0
5
10
15
PROTECT AF Early PROTECT AF Late CAP
Incidence %
Procedure/Device Related Safety Adverse Event Within 7 Days
6,3
3,7
2,2
0
2
4
6
8
10
PROTECT AF Early PROTECT AF Late CAP
Incidence %
Serious Pericardial Effusion Within 7 Days
With increased operator experience
Procedure related adverse events and serious pericardial effusions were reduced significantly
Peri-procedural strokes were eliminated
1,10,7
00
1
2
3
4
5
PROTECT AF Early PROTECT AF Late CAP
Incidence %
Procedure Related Stroke
SH
-AA
-15
390
2-A
PR
201
3

PREVAIL
SH
-AA
-15
390
2-A
PR
201
3

PREVAIL Vascular Complications7 Day Serious Procedure/Device Related
Holmes TCTMD 2013PROTECT-AF and CAP data: Reddy, VY et al. Circulation. 2011;123:417-424.
n=39 n=23 n=12
p = 0.005
No procedure-related deaths reported in any of the trials
1 Includes observed PE not necessitating intervention, AV fistula, major bleeding requiring transfusion, pseudoaneurysm, hematoma and groin bleeding
Composite of vascular complications includes cardiac perforation, pericardial effusion with tamponade, ischemic stroke, device embolization, and other vascular complications1
49% reduction
SH
-AA
-15
390
2-A
PR
201
3

PREVAIL Implant Success
PROTECT AF Implant Success
90.9%
CAP Implant Success
94.3%
PREVAIL Implant Success
95.0%
p = 0.01
p = 0.282
N= 26N= 26
N= 24N= 24
Implant success defined as deployment and release of the device into the left atrial appendageHolmes TCTMD 2013
PROTECT-AF and CAP data: Reddy, VY et al. Circulation. 2011;123:417-424.
SH
-AA
-15
390
2-A
PR
201
3

ASAP
SH
-AA
-15
390
2-A
PR
201
3

WATCHMAN™ Preliminary Results ASA Plavix Feasibility Study
WATCHMAN Implantation for contra-indicated AF warfarin patients is: Feasible Low, but manageable, rate of device
thrombus Decreases the rate of stroke by 77%
5.0%
64%
Reddy, et al. JACC. 2013; In Press.
SH
-AA
-15
990
1-M
AY
20
13


Design components of Amplatzer Cardiac PlugDesign components of Amplatzer Cardiac Plug(St. Jude Medical)(St. Jude Medical)




ACPInitial European Registry1
ACPItalian registry2
Dual Center experience3
Initial single centre experience4
ACP Post-Market Observational study5
Initial Asia Pacific experience 6
Belgian Registry 7
Single centre experience 8
Total
N = 143 N = 100 N = 135 N = 34 N = 204 N = 20 N = 82 N = 86 804
Enrollment period
12/2008-12/2009
12/ 2008-2/2010
2010-2011 NR 8/2009 – 9/2011 NR 6/2009 – 4/2012
1/2009 – 9/2011
SuccessfulDevice implant
132(96.4%)
99(99%)
131(98.5%)
34(100%)
197(96.6%)
19(95%)
81(98.8%)
85(98.8%)
Serious Pericardial Effusion
5 1 0 1 3 0 1 1 12
Device Embolization
2 0 0 0 3 0 0 1 6
Stroke / TIA 3 0 0 0 0 0 0 2 5
MyocardialInfarction
0 0 0 0 0 0 2 0 2
Total Major complication
10 (7.3%)
1 (1%)
0 (0%)
1 (2.9%)
6 (2.9%)
0 3 (3.6%)
4 (4.7%)
25 (3.1%)
Total Minor complication
7(5.1%)
3(3%)
3(2.3%)
0(0%)
NR 2 (10%)
4(4.9%)
2(2.3%)
21(2.6%)
ACP Results Across Series
1. Park, J.-W. et al., Left atrial appendage closure with AMPLATZER Cardiac Plug in Atrial Fibrillation: Initial European experience. Cath and Cardiovasc Interv., 2011 77: 700–706.2. G. Santoro, Italian Experience with AMPLATZER Cardiac Plug , Presented at the Progress In Clinical Pacing Congress in December 2010 (Rome).3. Park, J.W, et al. Dual Center Experience with Different Strategies of Left Atrial Appendage Closure with AMPLATZER Cardiac Plug for Prevention of Stroke in Atrial Fibrillation. Presented at UHK Mayo Clinic Asia
cardiovascular summit. 2011 26-7 March (Hong Kong)4. Meerkin, D., Butnaru, A., Dratva, D. and Tzivoni, D. (2011) Initial experience with the Amplatzer Cardiac Plug for left atrial appendage occlusion. Journal of American College of Cardiology. 57(14):E1684. 5. Walsh, K. (2012) left atrial appendage closure with the AMPLATZER Cardiac Plug: Results of the European Prospective Observational Study. Presented at EuroPCR. Paris May 17 th.France6. Lam Y.Y,, Yip, G.W., Yu, C.M., Chan, W.W., Cheng, B.C., Yan, B.P., Clugston, R., Yong, G., Gattoma, T., and Paul, V. (2011) left Atrial Appendage closure with Amplatzer cardiac plug for stroke prevention in atrial
fibrillation: initial Asia-Pacific experience. Catheter Cardiovascular Interventions. May 3. doi:10.1002/ccd.23136 (Epub ahead of print) Catheter Cardiovasc Interv. 2012 Apr 1;79(5):794-8007. Kefer, J., Vermeersch,P., Budts, W., et al. (2012) Transcatheter percutaneous left atrial appendage closure for stroke prevention in atrial fibrillation: the Belgian Registry. Paper presented at : euroPCR: May 15-18 th. Paris
France. 8. Guérios, E.E., Schmid, M., Gloekler, S., Khattab, A.A., Wenaweser, P.M., Windecker, S., Meier, B. (2012) Left atrial appendage closure with the Amplatzer Cardiac Plug in patients with atrial fibrillation Arq Bras Cardiol.
2012 http://www.arquivosonline.com.br/english/2012/AOP/aop04012_ing.pdf (accessed 1st May 2012)



Key Differentiators During LAAC Implant Procedure
Key Differentiators During LAAC Implant Procedure
ACP2
s
s CX
• Design based on familiar ASD/PFO closure
1 WATCHMAN IFU 2 ACP IFU
This document is intended for internal educational use only and shall not be distributed outside of Boston Scientific. Indications, contraindications, warnings and instructions for use can be found in the product labeling supplied with each device. Information for the use only in countries with applicable health authority product registrations
SH-AA
-188301-SEP
2013
Device Placement
Ostium
Landing Zone LAA Neck Orifice
LAA Body
Key Differentiators
• 1 size access sheath for ease of use • Radiopaque markers on access sheath and
delivery catheter • Designed specifically for LAA • Pre-loaded • Accommodates very large LAA>28mm (33mm
device) • More positional forgiveness (angle b/ delivery
system and LAA) • Placement of only 1 part system
• Disk may form a seal of the LAA (multiple lobes)
• May be implanted in more shallow anatomies than WATCHMAN (but not <10mm)
devices
WATCHMAN™1
Key differentiators during LAAC implant procedure

Combined (surgical and percutaneous) closure of the LAA.

LARIAT device:LARIAT device:


Lariat device – contraindications:Lariat device – contraindications: Absolute contraindication: Absolute contraindication: prior open heart surgery prior open heart surgery
Relative contrindications: Relative contrindications: clinical history of severe pericarditis, epicardial VT clinical history of severe pericarditis, epicardial VT
ablation, uraemia, severe obesityablation, uraemia, severe obesity
Based on anatomy:Based on anatomy: LAA width >40mmLAA width >40mm superiorly oriented LAA with thesuperiorly oriented LAA with the LAA apex directed LAA apex directed
behind the pulmonary vascular trunkbehind the pulmonary vascular trunk bilobed LAA or multilobed LAA in which lobes are bilobed LAA or multilobed LAA in which lobes are
orientedoriented in different angles in different angles




LAA occluder

Kryteria kwalifikacji do przezskórnego zamknięcia Kryteria kwalifikacji do przezskórnego zamknięcia uszka lewego przedsionka w prewencji powikłań uszka lewego przedsionka w prewencji powikłań
zakrzepowo-zatorowych u pacjentów z migotaniem zakrzepowo-zatorowych u pacjentów z migotaniem przedsionków: przedsionków:
wysokie ryzyko epizodów zakrzepowo-zatorowych wysokie ryzyko epizodów zakrzepowo-zatorowych (CHA2DS2VASc≥3) oraz przeciwwskazania do przewlekłego (CHA2DS2VASc≥3) oraz przeciwwskazania do przewlekłego leczenia antagonistami witaminy K;leczenia antagonistami witaminy K;
pozytywna opinia zespołu ekspertów (HEART TEAM) w pozytywna opinia zespołu ekspertów (HEART TEAM) w składzie: kardiolog inwazyjny, elektrofizjolog, kardiolog oraz składzie: kardiolog inwazyjny, elektrofizjolog, kardiolog oraz kardiochirurg. kardiochirurg.