Embed Size (px)
Citation preview

Research Article Open Access
Volume 5 • Issue 1 • 1000147
Open AccessCase Report
Journal of Patient CareJo
urnal of Patient Care
ISSN: 2573-4598
Tesemma, J Pat Care 2019, 5:1DOI: 10.4172/2573-4598.1000147
J Pat Care, an open access journalISSN: 2573-4598
*Corresponding author: Melese Gezahegn T, Department of Obstetrics & Gynecology, Jimma University Medical Center, Jimma, Ethiopia, Tel: +251919209714; E-mail: [email protected]
Received December 13, 2018; Accepted April 15, 2019; Published April 24, 2019
Citation: Tesemma MG (2019) Singleton Partial Molar Pregnancy Delivered in Third Trimester: A Case Report. J Pat Care 5: 147. doi: 10.4172/2573-4598.1000147
Copyright: © 2019 Tesemma MG. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords: β-hCG; Fetal karyotype; Partial mole; Eclampsia; Case report
Abbreviations: JUMC: Jimma University Medical Center; GTD: Gestational Trophoblastic Diseases; PM: Partial Mole; IUGR: Intra Uterine Growth Restriction; IUFD: Intra Uterine Fetal Death; GTCS: Generalized Tonic Clonic Seizure; NICU: Neonatal Intensive Care Unit; GCS: Glowsco Comma Scale; PTD: Persistent Trophoblastic Disease; PROM: Premature Rupture of Membrane; ENND: Early Neonatal Death
Background Gestational Trophoblastic diseases (GTD) consist of a broad
spectrum of conditions ranging from an uncomplicated partial hydatidiform molar pregnancy to choriocarcinoma with cerebral metastasis. Molar pregnancy is significantly more common in extremes of age [1,2]. Partial molar (PM) pregnancy is a rare entity in which there is a triple abnormal fetus associated with a large placenta with cystic changes [3]. Pregnancies with normal live fetus coexistent in with partial molar placenta are extremely rare because of numerous maternal and fetal complications. The incidence of hydatidiform mole with a co-existing live fetus varies between 0.005 to 0.01 % of all pregnancies [2].
Partial moles are characteristically triploid with 46 chromosomes coming from the father. The pathogenesis are explained by the dispermic fertilization of an ovum or monospermic fertilization with duplication of the paternal haploid chromosome. Exceptionally, there are also diploid cases with bi-parental contribution [4,5]. Occurrence of PM pregnancy and a coexisting normal fetus presumably follows mitotic abnormalities in the early post-fertilization period and represents placental mosaicism. Survival of a fetus to term in the presence of partial mole remains an extremely uncommon occurrence and such cases represent an extremely rare outcome of molar pregnancy [6]. Here we report one of the rarest presentations of singleton PM pregnancy associated with eclampsia and preterm birth.
Singleton Partial Molar Pregnancy Delivered in Third Trimester: A Case Report Melese Gezahegn Tesemma*Department of Obstetrics & Gynecology, Jimma University Medical Center, Jimma, Ethiopia
AbstractBackground: A partial mole is the result of fertilization of a haploid ovum by two sperms or duplication of one sperm,
resulting in a triploid karyotype (69 XXY, 69 XXX, 69 XYY). To date, there are very few cases of histo-pathologically confirmed partial moles with diploid karyotypes which survived. This case is reported to highlight the rarest variant of partial molar pregnancy.
Case presentation: Here we present a case of singleton partial molar pregnancy co-existing with a live fetus delivered to an 18 years old primigravida lady at Jimma university medical center (JUMC) after amenorrhea of 8 months. She presented with eclamptic seizure for which she was admitted with a diagnosis of Eclampsia in 3rd trimester pregnancy. Malpresentation (breech) with? Abruptio placenta to rule out partial mole was considered initially. Cesarean section (C/S) was done to effect delivery of an alive female neonate weighing 1100 gm with an APGAR score of 4, 6 & 7 at 1st, 5th & the 10th minute of life. The neonate is admitted to neonatal intensive care unit (NICU) where she is complicated by early neonatal death after 65 hours of stay despite many efforts, the possible cause of death being respiratory failure secondary to underlying prematurity. Grossly placenta was single, weighing 1200 gm and invaded by vesicles except its membrane. Histo-pathological finding of placenta was consistent with partial mole.
Conclusion: The optimal management of hydatidiform mole with coexistent live fetus is currently uncertain. Clinicians are recommended to present their individual cases for the establishment of guidelines for the management and prenatal counseling for pregnancies with partial mole with coexistent fetuses.
Case PresentationAn 18 years old primigravida lady who doesn’t remember her last
normal menstrual period, but who claimed amenorrhea of 8 months presented to JUMC after referred from the local health center, where she was having antenatal care (ANC). She was referred with a diagnosis Eclampsia after providing a loading dose of MgSO4 and oral Nifedipine. The presenting complaint was abnormal body movement that was generalized tonic clonic seizure (GTCS) of 3 episodes, one at the health center and the other two on the way to the hospital. Associated with GTCS, she had up rolling of eyes and drooling of saliva. She also had minimal vaginal bleeding of 1 hour duration. Prior to this seizure she was having global headache and blurring of vision of 5 days duration and was told to have raised blood pressure (BP) for which she was given Nifedipine 20 mg per OS twice daily during the last five days before arrival in hospital. She had excessive vomiting at third month of pregnancy, which was managed by antiemetic drugs that she doesn’t know specifically. Her personal, familial, medical and obstetric histories are unremarkable. Specifically, she had neither personal history of hypertension and epilepsy nor familial history of molar pregnancy. Only her age, primigravidity and molar pregnancy were identified to be a risk factors for development of eclampsia.

J Pat Care, an open access journalISSN: 2573-4598
Citation: Tesemma MG (2019) Singleton Partial Molar Pregnancy Delivered in Third Trimester: A Case Report. J Pat Care 5: 147. doi: 10.4172/2573-4598.1000147
Page 2 of 4
Volume 5 • Issue 1 • 1000147
On arrival she was confused with GCS of 14/15 and her vital signs were BP = 170/100 mmHg, PR=96 bpm, RR= 24 Br/min, T=37°C. Her Chest was clear and resonant. Abdominal finding was 36 weeks sized gravid uterus with breech presentation. Fetal heart beat was positive. After placenta previa ruled out by sonography, pelvic examination performed. There was minimal dark red blood on examining finger and Bishop Score was 4. Obstetric Ultrasound showed singleton intrauterine pregnancy with positive fetal heartbeat, breech presentation, fundal thick placenta measuring about 11 cm with areas of multiple cystic spaces. Aggregate gestational age was 32 weeks & 2 days and estimated fetal weight was 1190 g, biophysical profile was 8/8.
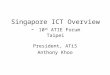
With the impression of Eclampsia in 3rd trimester pregnancy with Breech presentation +? Abruptio placentae to rule out partial mole, she was investigated with blood group & Rh (A+), Urinalysis (protein +3), Blood film (No hemo-parasite seen), RBS (112 gm/dl), CBC, RFT, LFT & TFT were in the normal limit. Abruption was initially considered due to the presence of vaginal bleeding, increased placental thickness (11 cm) & eclampsia while the diagnosis of molar pregnancy was not made prior to her current presentation. Anticonvulsant (MgSO4) and antihypertensive (hydralazine) were given to stabilize her. Once BP and convulsion was controlled the patient was taken to operation theatre for emergency caesarean section (C/S) within two hours of arrival. Transverse, lower uterine segment C/S done under general anesthesia to effect the delivery of an olive female neonate weighing 1100 g with an APGAR score of 4, 6 & 7 at 1st, 5th and 10th minutes of life. The neonate was grossly normal and neither visible congenital anomaly nor feature of hydrops was witnessed. The patient’s intraoperative condition was smooth. Grossly placenta was invaded by vesicles except its membrane and weighed 1200 gm. The placenta had one cord with its 3 vessels attached to it. But there was no evidence for abruption intra-operatively. The placenta is sent for histo-pathologic examination (Figure 1).
The neonate was referred to NICU with a diagnosis of Preterm + Very low birth weight + Hyaline membrane disease + hypothermia. The neonate has been on CPAP, radiant warmer, maintenance fluid, and antibiotics. Despite the above efforts the neonate was persistently hypothermic and later complicated by early neonatal death after 65 hours of stay at NICU, the possible cause of death being respiratory failure secondary to underlying prematurity. Blood pressure of the mother was dropped to 150/90 soon after birth and she continued
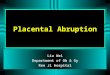
MgSO4 5 mg IM every 4 hours for first 24 hours after delivery, and overall clinical condition and urine output of the patient was good during postoperative period and discharged on her 7th post-op day with an advice to come for weekly surveillance follow up after provided with Depo-Provera Medroxy Progestrone Acetate injection for contraception as per her choice. Histo- pathologic examination showed mixture of small and large scalloped hydropic villi with central cisternae, mild irregular trophoblastic proliferation, and normal histology of umbilical cord. There are no atypical malignant cells seen. The finding is consistent with partial molar pregnancy (Figures 2 and 3). Serum B-hcG sent 48 hours after operation showed 162.3 mu/ml and her chest X-Ray is normal. During her weekly follow up, her serum B-Hcg level become normal at third week and become undetectable after three months following delivery. No evidence for persistent disease during her surveillance follow up
Discussion Although triploidy is the most frequent association, a fetus with
normal karyotype (diploidy) can survive in cases of partial molar
Figure 1: Placental tissue with its vesicle at delivery.
A) Medium power view A2. B) High power viewFigure 2: Chorionic villus taken from normal part of placental tissue.

J Pat Care, an open access journalISSN: 2573-4598
Citation: Tesemma MG (2019) Singleton Partial Molar Pregnancy Delivered in Third Trimester: A Case Report. J Pat Care 5: 147. doi: 10.4172/2573-4598.1000147
Page 3 of 4
Volume 5 • Issue 1 • 1000147
pregnancy. Singleton Partial mole with a live fetus may occasionally survive into full term [1,2,7] and even to the school age [8,9]. Fetuses with triploidy cannot survive after birth because of multiple malformations and severe intrauterine fetal growth retardation (IUGR) secondary to affected placental circulation. In PM there is partial replacement with hydropic villi and visible abnormal fetal parts mostly leading to termination of pregnancy in the first trimester. It presents with several dilemmas in management during pregnancy and the woman must be counseled regarding the maternal and fetal complications and the risk of persistent trophoblastic disease in later life [10-13].
Hydatidiform mole with coexistent normal fetus is not necessarily considered a partial mole. Cases of such association can be classified into three types. The first and most common is twin pregnancy with one normal fetus having a normal placenta and another complete mole. There have been so far, about 200 such cases fully documented in literature of which only 56 resulted in a term live birth, second type is a twin pregnancy with normal fetus with normal placenta and another partial mole. The third and most uncommon occurrence is a singleton normal fetus with partial molar placenta similar to our case [5,11]. Sometimes the third variant is difficult to diagnose especially when the patient come at third trimester or in labor for the first time as sonography alone can’t tell us everything. In our case the fact that the patient presented with eclampsia and alive fetus with single large placenta (11 cm thick with multiple hypo echoic area) leads us to consider abruptio placentae while the reality is not. We were in doubt to consider partial mole due to the extreme rarity of this case although there were clues in favor of partial mole.
In the past most molar pregnancies associated with live fetus were terminated in view of adverse maternal and fetal outcome in advanced gestations. Close maternal and fetal surveillance may help in achieving a favorable outcome though termination is required only in cases of gross fetal anomalies or deteriorating maternal condition [9]. Several factors may affect the outcome of the fetus in cases of partial molar pregnancy. These include karyotype of the fetus, the size of the abnormal molar placenta, the speed of molar degeneration, and the occurrence of fetal anemia or other obstetric complications [11].
Molar pregnancy with coexisting fetus carries a significant risk to the mother and the fetus. Maternal risks include abnormal bleeding, hyper emesis gravidarum, preeclampsia, eclampsia, hyperthyroidism, anemia, preterm labor, mal-presentation like transverse lie, Preterm premature rupture of membrane (PROM), persistent trophoblastic disease and abruption. Fetal complications include abortion, congenital anomalies, preterm, severe anemia due to limited placental circulation, IUGR and intra uterine fetal death (IUFD) [6,11-15]. In our case, hyper emesis gravidarum, preeclampsia, eclampsia, preterm delivery, mal-presentation (breech) and fetal anemia were seen Table 1. The serum B-hcG will drop immediately after delivery when compared to the one sent immediately before delivery. This is witnessed in one case report where serum B-Hcg sent before delivery was as high as 16,000 mIU, while sent once again 48 hours of delivery; it was 247 mIU [12]. Immediate post-delivery serum B-hCG value of our case is consistent with this report although difficult to comment on pre-delivery value.
After delivery serial follow up of mother for early detection of persistent trophoblastic disease (PTD) should be done as it is done in our case. Fetal karyotype is mandatory to know whether the partial mole is of normal or abnormal karyotype. Immuno-histochemical evaluation for p57 protein is occasionally needed to differentiate between complete or partial molar pregnancy. Early target scanning and early prophylactic antenatal steroids are recommended [15]. In our case emergent presentation of patient necessitating immediate delivery hinders us not to have targeted sonography and to provide corticosteroids for fetal lung maturity. Unfortunately, we don’t have karyotyping and Immuno-histochemical evaluation for p57 protein services in our medical center. From review of literatures all partial moles survived beyond late 2nd trimester were all having normal karyotype.
Although we don’t have karyotype and Immuno-histochemical evaluation for p57 protein, the fact that the fetus is apparently normal and alive with single placenta and histo-pathologic finding consistent with partial mole favors diagnosis of singleton partial molar pregnancy likely of normal karyotype than diagnosing complete molar pregnancy with co-twin fetus.
Figure 3: Hydropic villi taken from vesicle part of the same placenta. A) Medium power view A3, B) High power view, A3.

J Pat Care, an open access journalISSN: 2573-4598
Citation: Tesemma MG (2019) Singleton Partial Molar Pregnancy Delivered in Third Trimester: A Case Report. J Pat Care 5: 147. doi: 10.4172/2573-4598.1000147
Page 4 of 4
Volume 5 • Issue 1 • 1000147
ConclusionThe optimal management of Hydatidiform mole with coexistent
alive fetus is currently uncertain. Clinicians are recommended to present their individual cases for the establishment of guidelines for the management and prenatal counseling for pregnancies with partial mole with coexistent fetuses. From review of the literatures only partial molar pregnancies with normal karyotype (diploidy) have survived beyond late 2nd trimester and even to postnatal life.
References
1. Parveen Z, Bashir R, Jadoon T, Qayum I (2004) Partial hydatidiform mole along with term gestation and alive baby. J Ayub Med Coll Abbottabad 16: 84-85.
2. Ara R, Begum J, Kasem SB, Hoque S, Nargis SF (2016) Partial Hydatidiform Mole with Alive Term IUGR Foetus. J Bangladesh Coll Phys Surg 34: 3.
3. Singh S, Swain S, Das L, Das PC (2017) Partial molar pregnancy associated with a normal appearing fetus: A case report and review of the literature. Int J Reprod Contracept Obstet Gynecol 6: 2681-2683.
4. Yanik A, Yanik FF, Urman B (2006) Partial hydatidiform mole in a triplet pregnancy following intracytoplasmic sperm injection: Case Report and Review of the Literature. SAYFA: 70-72.
5. Dolapcioglu K, Gungoren A, Hakverdi S, Hakverdi AU, Egilmez E (2009) Twin pregnancy with complete hydatidiform mole and co-existent live fetus: Two case reports and review of the literature. Arch Gynecol Obstet 279: 431-436.
6. Dhingra KK, Gupta P`, Saroha V, Akhila L, Khurana N (2009) Partial hydatidiform mole with a full term infant. Indian J Pathol Microbiol 52: 590-591.
7. Deveer R, Ustun YE, Eryilmaz OG, Akbaba E, Deveer M (2015) Molar pregnancy with a live fetus. J Clin Anal Med 6: 88-90.
8. Rathod AD, Pajai SP, Gaddikeri A (2014) A partial mole with co-existing viable fetus-a clinical dilemma: a case report with review of literatures. J South Asian Feder Obste Gynae 6: 51-55.
9. Ramani B, Patel O, Behera SK, Pradhan S, Panda SR (2014) Living fetus without congenital malformation in a singleton partial hydatidiform molar pregnancy: A case report and review of the literature. Int J Reprod Contracept Obstet Gynecol 3: 1130-1133.
10. Rathod S, Rani R, John LB, Samal SK (2015) Successful outcome of twin gestation with partial mole and co-existing live fetus: A Case Report. J Clin Diag Res 9: QD01-QD02.
11. Hsieh CC, Hsieh TT, Hsueh C, Kuo DM, Lo LM, et al. (1999) Delivery of a severely anemic fetus after partial molar pregnancy: Clinical and ultrasonographic findings. Hum Reprod 14: 1122-1126.
12. Shobha UN, Dhananjaya BS, Nanda SK, Gopal N, Tejeswini KK, et al. (2011) A Term Pregnancy with Partial Molar Changes – A Case Report. Int J Biol Med Res 2: 1191-1192.
13. Koregol M, Bellad M, Malapati C (2009) Partial hydatidiform mole with a live fetus- A rare entity. J South Asian Feder Obste Gynae 1: 77-79.
14. Rahamni M, Parviz S (2016) A case report of partial molar pregnancy associated with a normal appearing dizygotic fetus. Asian Pacific J Reprod 5: 171-173.
15. Vikraman SK, Chandra V, Balakrishanan B, Batra M, Kuriakose R, et al. (2015) A case of viable fetus co-existing with a complete hydatidiform mole in a twin pregnancy with successful outcome. Int J Reprod Contracept Obstet Gynecol 4: 266-268.
References Maternal age (years)
Reproductive GA at Dx/Delivery
Fetal karyotype Serum B-Hcg Outcome Maternal & fetal complications
History
Parveen et al. [1] 23 G4P1A2 18/39 NA NAF=2700 g, Alive -Bleeding, anemia, IUGRPlacenta=800 g - No PTD
Ara et al. [2] 26 G2P1 28/40 46XY300 miu/ml M=1500 g, alive - IUGR
48 hrs p/partum Placenta=600 g - No PTD
Singh et al. [3] 24 G1 20.4/20.4 Trisomy 21 4, 24, 249 mIU/mlAlive, 200 g -Vaginal bleeding, anemia, IUGR
Placenta =700 g -pre eclampsia, but No PTD
Deveer et al. [5] 35 G5P4 14/39 46XY Not mentionedM=3100 g, -Hyperemesis gravidarum
Alive -Hyperthyroidism, but no PTD
Rathod et al. [8] 23 G1 22/34 46XX 23500 miu/mlF=1400 g, alive -Pre eclampsia, anemia, PROM,
Placenta=1700 g - preterm labor, IUGR, breech, -microcephaly but no PTD
Ramani B et al. [9] 36 G2P1 29.5/34 NA 315 miu/mlM=960 g, alive -Vaginal bleeding, anemia,
pretermPlacenta =1800 g -but no PTD
Hsieh CC et al. [11] 30 G1 18/32.6 46XX 167, 596 mIU/ml F=1551 g alive-maternal anemia, fetal anemia
- but no PTD
Shobha et al. [12] 21 G1 20/37 NA 16,000, 247 miu/mlM=1500 g, dead - IUGR, IUFDPlacenta =600 g -No PTD
Rahamni M, Parviz S [14] 23 G2P1 11.5/26 46XY 64750 mIU/mL
M, dead-PROM, IUFD
Placenta =1100 g
Koregol M et al. [13] 22 G2P1 31/31 NA NA
M=2000 g, alive Pretertm labor, PROM Hydrocephalus, spina bifida
Placenta =700 g -bilateral Tallipes eqinovarus, -ENND, No PTD
This case 18 G1 32.3/32.3 NA
162.3 F=1100 g, alive -Preeclampsia, eclampsia, preterm delivery, mal-
presentation(breech) and fetal anemia, ENND, No PTD
miu/ml Placenta =1200 g
Table 1: Review of cases of partial mole co-existing with live fetus in case of singleton pregnancy. G-P-A=Gravida Para Abortion, GA=Gestational age, NA=Not Available, PTD=Persistent trophoblastic disease, PROM= Premature rupture of membrane, ENND= Early Neonatal death, M=Male, F=Female, Dx=Diagnosis