Embed Size (px)
DESCRIPTION
PETITION FOR INTER PARTES REVIEWOF U.S. PATENT NO. 6,315,720
Citation preview
Paper No. ______ Filed: April 23, 2015
UNITED STATES PATENT AND TRADEMARK OFFICE ____________________
BEFORE THE PATENT TRIAL AND APPEAL BOARD ___________________
COALITION FOR AFFORDABLE DRUGS VI LLC
PETITIONER
V.
CELGENE
PATENT OWNER
___________________
CASE NO.: UNASSIGNED PATENT NO. 6,315,720
FILED: OCTOBER 23, 2000 ISSUED: NOVEMBER 13, 2001
INVENTORS: BRUCE A. WILLIAMS AND JOSEPH K. KAMINSKI
TITLE: METHODS FOR DELIVERING A DRUG TO A PATIENT WHILE AVOIDING THE OCCURRENCE OF AN ADVERSE SIDE EFFECT KNOWN
OR SUSPECTED OF BEING CAUSED BY THE DRUG ___________________
PETITION FOR INTER PARTES REVIEW OF U.S. PATENT NO. 6,315,720
Patent No. 6,315,720
TABLE OF CONTENTS
I. INTRODUCTION ..................................................................................................... 1
II. GROUNDS FOR STANDING (37 C.F.R. § 42.104(a)) ........................................ 1
III. MANDATORY NOTICES (37 C.F.R. § 42.8) ........................................................ 1
A. Real Parties-in-Interest (37 C.F.R. § 42.8(b)(1)) .................................................... 1
B. Related Judicial and Administrative Matters (37 C.F.R. § 42.8(b)(2)) ................. 2
C. Lead and Back-Up Counsel (37 C.F.R. § 42.8(b)(3)) and Service Information (37 C.F.R. § 42.8(b)(4)) ....................................................................... 3
IV. PAYMENT OF FEES (37 C.F.R. § 42.15(a) and § 42.103) ................................... 3
V. IDENTIFICATION OF CHALLENGE ................................................................ 3
A. Overview of U.S. Patent No. 6,315,720 ................................................................. 3
The ’720 Patent Specification ............................................................................. 4 1.
The ’720 Claims .................................................................................................... 5 2.
The ’720 Prosecution History ............................................................................. 6 3.
B. Claim Construction of Challenged Claims ............................................................. 9
“Consulted” ......................................................................................................... 10 1.
“Teratogenic effect” ........................................................................................... 10 2.
“Adverse side effect” ......................................................................................... 11 3.
C. Statement of Precise Relief Requested for Each Claim Challenged ................. 11
Claims for Which Review is Requested ........................................................... 11 1.
Statutory Grounds of Challenge ....................................................................... 11 2.
D. Overview of the State of the Art ........................................................................... 12
VI. DETAILED EXPLANATION OF THE CHALLENGE ................................. 14
A. Ground 1: THALOMID™ (thalidomide) Capsules Revised Package Insert anticipates Claims 1–32 of U.S. Patent No. 6,315,720 under 35 U.S.C. § 102(b). ...................................................................... 14
Thalomid PI anticipates Claim 1. ........................................................................ 17 1.
i
Patent No. 6,315,720
Thalomid PI anticipates Claims 2–6. .................................................................. 22 2.
Thalomid PI anticipates Claims 7–10. ................................................................ 25 3.
Thalomid PI anticipates Claims 11–14 and 20–25. ........................................... 28 4.
Thalomid PI anticipates Claim 15. ...................................................................... 30 5.
Thalomid PI anticipates Claims 16–17. .............................................................. 31 6.
Thalomid PI anticipates Claims 18–19 and 26–27. ........................................... 33 7.
Thalomid PI anticipates Claims 28–32. .............................................................. 34 8.
Claim chart for Ground 1 showing exemplary citations in 9.Thalomid PI. ......................................................................................................... 36
B. Ground 2: Claims 1–32 of U.S. Patent No. 6,315,720 are obvious under 35 U.S.C. § 103(a) over Thalomid PI in view of Cunningham, and in further view of the knowledge of one of ordinary skill in the art. ........ 51
Claims 1(e) and 28(e) are obvious over Thalomid PI in view 1.of Cunningham. .................................................................................................... 52
Claims 5 and 6 are obvious over Thalomid PI in view of the 2.knowledge of one of ordinary skill in the art. ................................................ 54
Claims 9 and 10 are obvious over Thalomid PI in view of the 3.knowledge of one of ordinary skill in the art. ................................................ 57
Claim 17 is obvious over Thalomid PI in view of the knowledge 4.of one of ordinary skill in the art. .................................................................... 59
Claim Chart for Ground 2 showing exemplary citations in 5.Cunningham. ......................................................................................................... 59
VII. CONCLUSION ......................................................................................................... 60
ii
Patent No. 6,315,720
TABLE OF AUTHORITIES Cases Abbott Labs v. Andrx Pharms., Inc.,
452 F.3d 1331 (Fed. Cir. 2006) ....................................................................................... 54 Atlas Powder Co. v. IRECO, Inc.,
190 F.3d 1342 (Fed. Cir. 1999) ....................................................................................... 16 Bayer Schering Pharma AG v. Barr Labs., Inc.,
575 F.3d 1341 (Fed. Cir. 2009) ....................................................................................... 56 Continental Can Co. USA, Inc. v. Monsanto Co.,
948 F.2d 1264 (Fed. Cir. 1991) ................................................................................. 17, 21 Dow Chem. Co. v. Sumitomo Chem. Co.,
257 F.3d 1364 (Fed. Cir. 2001) ....................................................................................... 17 Dystar Textilfarben GmbH v. C.H. Patrick Co.,
464 F.3d 1356 (Fed. Cir. 2006) ....................................................................................... 54 In re Am. Acad. of Sci. Tech. Ctr.,
367 F.3d 1359 (Fed. Cir. 2004) ....................................................................................... 10 In re Baxter Travenol Labs,
952 F.2d 388 (Fed. Cir. 1991) ......................................................................................... 17 In re Cruciferous Sprout Litigation,
301 F.3d 1343 (Fed. Cir. 2002) ....................................................................................... 27 In re Cuozzo Speed Techs., LLC,
778 F.3d 1271 (Fed. Cir. 2015) ......................................................................................... 9 In re Glatt Air Techniques, Inc.,
630 F.3d 1026 (Fed. Cir. 2011) ....................................................................................... 18 In re Graves,
69 F.3d 1147 (Fed. Cir. 1995) ............................................................................. 21, 25, 27 In re LeGrice,
301 F.2d 929 (CCPA 1962) ....................................................................................... 21, 27 In re Venner,
262 F.2d 91 (C.C.P.A. 1958) ........................................................................................... 59 KSR Int'l Co. v. Teleflex Inc.,
550 U.S. 398 (2007) .......................................................................................................... 53 Pacing Techs., LLC v. Garmin Int’l, Inc.,
778 F.3d 1021 (Fed. Cir. 2015) ....................................................................................... 10
iii
Patent No. 6,315,720
Pentec, Inc. v. Graphic Controls Corp., 776 F.2d 309 (Fed. Cir. 1985) ......................................................................................... 18
Perfect Web Techs., Inc. v. InfoUSA, Inc., 587 F.3d 1324 (Fed. Cir. 2009) ....................................................................................... 56
Schering Corp. v. Geneva Pharms., Inc., 339 F.3d 1373 (Fed. Cir. 2003) .............................................................. 21, 24, 31, 27, 33
SmithKline Beecham Corp. v. Apotex Corp., 403 F.3d 1331 (Fed. Cir. 2005) ....................................................................................... 33
Titanium Metals Corp. v. Banner, 778 F.2d 775 (Fed. Cir. 1985) ......................................................................................... 16
Tyco Healthcare Grp. LP v. Ethicon Endo-Surgery, Inc., 774 F.3d 968 (Fed. Cir. 2014) ......................................................................................... 58
Unigene Labs., Inc. v. Apotex, Inc., 655 F.3d 1352 (Fed. Cir. 2011) ....................................................................................... 58
Verdegaal Bros. v. Union Oil Co. of California, 814 F.2d 628 (Fed. Cir. 1987) ......................................................................................... 16
Rules 37 C.F.R. § 42.103 .................................................................................................................. 3 37 C.F.R. § 42.15(a) ................................................................................................................ 3 37 C.F.R. § 42.8(b)(1) ............................................................................................................. 1
iv
Patent No. 6,315,720
TABLE OF EXHIBITS
Exhibit No. Description Exhibit 1001 U.S. Patent No. 6,315,720 to Bruce A. Williams and Joseph K.
Kaminski, filed on Oct. 23, 2003, and issued on Nov. 13, 2001 (the “’720 Patent”)
Exhibit 1002 U.S. Patent No. 6,315,720 Prosecution History (“’720 prosecution history”)
Exhibit 1003 U.S. Patent No. 6,045,501 to Marc Elsayed and Bruce Williams, filed on Aug. 28, 1998, and issued on Apr. 4, 2000 (“Elsayed”)
Exhibit 1004 U.S. Patent No. 6,063,026 to Mark A. Schauss and Patricia Kane, filed on Mar. 22, 1996, and issued on May 16, 2000 (“Schauss”)
Exhibit 1005 U.S. Patent No. 6,202,923 to Joseph H. Boyer et al., filed on Aug. 23, 1999, and issued on Mar. 20, 2001 (“Boyer”)
Exhibit 1006 “THALOMID™ (thalidomide) Capsules Revised Package Insert” (Jul. 15, 1998) (“Thalomid PI”)
Exhibit 1007 “Guideline for the clinical use and dispensing of thalidomide,” R.J. Powell and J.M.M Gardner-Medwin, Postgrad Med. J. (1994) 79, 901–904 (“Powell”)
Exhibit 1008 “Pharmacists’ role in clozapine therapy at a Veterans Affairs medical center,” Benjamin R. Dishman et al., Am. J. Hosp. Pharm. (Apr. 1, 1994) 51, 899–901 (“Dishman”)
Exhibit 1009 U.S. Patent No. 5,832,449 to David W. Cunningham, filed on Nov. 13, 1995, and issued on Nov. 3, 1998 (“Cunningham”)
Exhibit 1010 U.S. Patent No. 6,055,507 to David W. Cunningham, filed on Aug. 20, 1998, and issued on Apr. 25, 2000 (“Cunningham Divisional”)
Exhibit 1011 “A Pregnancy-Prevention Program in Women of Childbearing Age Receiving Isotretinoin,” Allen A. Mitchell et al., New Eng. J. Med. (Jul. 13, 1995) 333:2, 101–06 (“Mitchell”)
Exhibit 1012 “S.T.E.P.S.TM: A Comprehensive Program for Controlling and Monitoring Access to Thalidomide,” Jerome B. Zeldis et al., Clinical Therapeutics (1999) 21:2, 319–30 (“Zeldis”)
Exhibit 1013 Transcript of the FDA’s “Forty-Seventh Meeting of the Dermatologic and Opthalmic Drugs Advisory Committee,” Sept. 4, 1997 (“FDA Meeting Part 1”)
v
Patent No. 6,315,720
Exhibit No. Description Exhibit 1014 Transcript of the FDA’s “Forty-Seventh Meeting of the
Dermatologic and Opthalmic Drugs Advisory Committee,” Sept. 5, 1997 (“FDA Meeting Part 2”)
Exhibit 1015 “CDC Meeting: 03/26/1997 Minutes and Agenda Regarding Thalidomide” (“CDC Meeting”)
Exhibit 1016 “Assessing the Effectiveness of a Computerized Pharmacy System,” Reed M. Gardner et al., Decision Support Systems in Critical Care, 1994, M.M. Schabot et al., eds. (“Gardner”)
Exhibit 1017 “Review of computer applications in institutional pharmacy—1975–1981,” Ken W. Burleson, Am. J. Hosp. Pharm. (1982) 39:53–70 (“Burleson”)
Exhibit 1018 “Challenges of thalidomide distribution in a hospital setting,” Daniel P. Keravich and Charles E. Daniels, Am. J. Health-Syst. Pharm. (Sept. 1, 1999) 56:1721–75 (“Keravich”)
Exhibit 1019 “The Assessment of Refill Compliance Using Pharmacy Records: Methods, Validity, and Applications,” John F. Steiner and Allan V. Prochazka, J. Clin. Epidemiol. (1997) 50:1, 105–16 (“Steiner”)
Exhibit 1020 “Therapeutic Antibiotic Monitoring: Surveillance Using a Computerized Expert System,” Stanley L. Pestotnik et al., Am. J. Med. (Jan. 1990) 88:43–48 (“Pestotnik”)
Exhibit 1021 Declaration of Jeffrey Fudin, R.Ph., B.S., Pharm.D., DAAPM, FCCP, FASHP (“Fudin Decl.”)
Exhibit 1022 Curriculum Vitae for Jeffrey Fudin, R.Ph., B.S., Pharm.D., DAAPM, FCCP, FASHP (“Fudin CV”)
Exhibit 1023 “Joint Claim Construction and Prehearing Statement,” Celgene Corp. v. Natco Pharma Ltd., NJD-2-10-cv-05197, Jul. 18, 2011 (“Celgene Claim Construction Brief”)
Exhibit 1024 “Interactive Voice Response Systems in Clinical Research and Treatment,” James C. Mundt, Psychiatric Services (May 1997) 48:5, 611–12, 623 (“Mundt”)
Exhibit 1025 “Center for Drug Evaluation and Research Approval Package for: Application Number NDA 20-785 Approval Letter(s),” Sept. 19, 1997, and Jul. 16, 1998 (“FDA Thalomid Approval Letters”)
vi
Patent No. 6,315,720
I. INTRODUCTION
Petitioner Coalition For Affordable Drugs VI LLC (“CFAD”), requests an Inter
Partes Review (“IPR”) of Claims 1–32 (collectively, the “Challenged Claims”) of U.S.
Patent No. 6,315,720 (the “’720 Patent”) (Ex. 1001) in accordance with 35 U.S.C.
§§ 311–19 and 37 C.F.R. §§ 42.100 et seq.
II. GROUNDS FOR STANDING (37 C.F.R. § 42.104(A))
Pursuant to 37 C.F.R. § 42.104(a), Petitioner certifies that the ’720 patent is
available for IPR and that Petitioner is not barred or estopped from requesting IPR
challenging the claims of the ’720 patent on the grounds identified in this Petition.
III. MANDATORY NOTICES (37 C.F.R. § 42.8)
A. Real Parties-in-Interest (37 C.F.R. § 42.8(b)(1))
Pursuant to 37 C.F.R. § 42.8(b)(1), Petitioner certifies that Coalition For
Affordable Drugs VI LLC (“CFAD VI”), Hayman Credes Master Fund, L.P.
(“Credes”), Hayman Orange Fund SPC – Portfolio A (“HOF”), Hayman Capital
Master Fund, L.P. (“HCMF”), Hayman Capital Management, L.P. (“HCM”), Hayman
Offshore Management, Inc. (“HOM”), Hayman Investments, L.L.C. (“HI”), nXn
Partners, LLC (“nXnP”), IP Navigation Group, LLC (“IPNav”), J. Kyle Bass, and
Erich Spangenberg are the real parties in interest (collectively, “RPI”). The RPI
hereby certify the following information: CFAD VI is a wholly owned subsidiary of
Credes. Credes is a limited partnership. HOF is a segregated portfolio company.
HCMF is a limited partnership. HCM is the general partner and investment manager
1
Patent No. 6,315,720
of Credes and HCMF. HCM is the investment manager of HOF. HOM is the
administrative general partner of Credes and HCMF. HI is the general partner of
HCM. J. Kyle Bass is the sole member of HI and sole shareholder of HOM. CFAD
VI, Credes, HOF and HCMF act, directly or indirectly, through HCM as the general
partner and/or investment manager of Credes, HOF and HCMF. nXnP is a paid
consultant to HCM. Erich Spangenberg is the 98.5% member of nXnP. IPNav is a
paid consultant to nXnP. Erich Spangenberg is the 98.5% member of IPNav. Other
than HCM and J. Kyle Bass in his capacity as the Chief Investment Officer of HCM
and nXnP and Erich Spangenberg in his capacity as the Manager/CEO of nXnP, no
other person (including any investor, limited partner, or member or any other person
in any of CFAD VI, Credes, HOF, HCMF, HCM, HOM, HI, nXnP or IPNav) has
authority to direct or control (i) the timing of, filing of, content of, or any decisions or
other activities relating to this Petition or (ii) any timing, future filings, content of, or
any decisions or other activities relating to the future proceedings related to this
Petition. All of the costs associated with this Petition will be borne by HCM, CFAD
VI, Credes, HOF and/or HCMF.
B. Related Judicial and Administrative Matters (37 C.F.R. § 42.8(b)(2))
Pursuant to 37 C.F.R. § 42.8(b)(2), Petitioner states that the ’720 Patent has
been the subject of the following lawsuits: Celgene Corp. et al. v. Lannett Holdings, Inc. et
al., NJD-2-15-00697 (filed Jan. 30, 2015); Celgene Corp. v. Natco Pharma Ltd., NJD-2-10-
cv-05197 (filed Oct. 8, 2010); Celgene Corp. et al. v. Barr Laboratories, Inc. et al., NJD-2-
2
Patent No. 6,315,720
08-cv-03357 (filed July 3, 2008); Celgene Corp. et al. v. Barr Laboratories, Inc. et al., NJD-2-
07-cv-05485 (filed Nov. 14, 2007); Celgene Corp. et al. v. Barr Laboratories, Inc. et al., NJD-
2-07-cv-04050 (filed Aug. 23, 2007); Celgene Corp. et al. v. Barr Laboratories, Inc. et al.,
NJD-2-07-cv-00286 (filed Jan. 18, 2007).
C. Lead and Back-Up Counsel (37 C.F.R. § 42.8(b)(3)) and Service Information (37 C.F.R. § 42.8(b)(4))
Lead counsel is Sarah E. Spires, Reg. No. 61,501,
[email protected]. Back-up counsel are Ki O, Reg. No. 68,952,
[email protected]; Dr. Parvathi Kota, Reg. No. 65,122,
[email protected]; and Paul J. Skiermont (pro hac vice requested),
[email protected]—all of Skiermont Puckett LLP, 2200 Ross
Ave. Ste. 4800W, Dallas, Texas 75201, P: 214-978-6600/F: 214-978-6601. Petitioner
consents to electronic service.
IV. PAYMENT OF FEES (37 C.F.R. § 42.15(A) AND § 42.103)
The required fees are submitted herewith in accordance with 37 C.F.R.
§§ 42.103(a) and 42.15(a). If any additional fees are due during this proceeding, the
Office is authorized to charge such fees to Deposit Account No. 506293. Any
overpayment or refund of fees may also be deposited in this Deposit Account.
V. IDENTIFICATION OF CHALLENGE
A. Overview of U.S. Patent No. 6,315,720
The ’720 Patent is titled “Methods for Delivering a Drug To A Patient While
Avoiding The Occurrence Of An Adverse Side Effect Known Or Suspected Of Being 3
Patent No. 6,315,720
Caused By The Drug.” (Ex. 1001 at Front Cover.) The underlying application, U.S.
Patent Application Serial No. 09/694,217, was filed on October 23, 2000. The ’720
Patent issued to Bruce Williams and Joseph K. Kaminski on November 13, 2001. (Id.)
The ’720 Patent Specification 1.
The ’720 Patent claims methods for delivering a drug to a patient, while
avoiding the occurrence of adverse side effects. (Id. at Abstract.) The ’720 Patent
generally describes methods for “the distribution to patients of drugs, particularly
teratogenic drugs, in ways wherein such distribution can be carefully monitored and
controlled.” (Id. at 1:13–16.) A teratogenic drug can cause severe birth defects when
administered to a pregnant woman. (Id. at 1:27–29.) The ’720 specification
acknowledges that prior “[m]ethods for monitoring and educating patients to whom a
drug is distributed have been developed in connection with” a known teratogenic
drug (isotretinoin), including a “pregnancy prevention program.” (Id. at 2:13–20.)
The invention of the ’720 Patent was allegedly conceived in the context of the
FDA approval of thalidomide—a teratogenic drug effective in treating a variety of
diseases—when the inventors were seeking methods “to control the distribution of
[thalidomide] so as to preclude administration to foetuses.” (Id. at 1:46–64.)
The ’720 Patent’s invention can be summarized as: (1) filling prescriptions only
after consulting a computer readable storage medium to confirm that the prescribers,
pharmacies, and patients are registered in a computer database; (2) assigning patients
to risk groups based on the risk that the drug will cause adverse side effects and
4
Patent No. 6,315,720
entering the risk group assignment in the storage medium; (3) determining the
acceptability of the likely adverse effect; and (4) “generating a prescription approval
code to … said pharmacy before said prescription is filled.” (Id. at 2:49–3:4.) The ’720
Patent specification also teaches that “[t]he invention is not limited to the distribution
of teratogenic drugs; other potentially hazardous drugs may also be distributed in
accordance with embodiments of this invention … in such a fashion that persons for
whom such drugs are contraindicated will not receive them.” (Id. at 3:21–26.)
The patent also discloses that when a patient is registered in the computer
readable storage medium, information probative of the risk of a drug’s side effects is
also collected from the patient. (Id. at 6:30–33.) This information can then be
compared with a defined set of risk parameters for the drug, allowing for assignment
of the patient to a particular risk group. (Id. at 6:33–36.) If the risk of adverse side
effects is deemed acceptable, the patient may receive the drug from a registered
pharmacy, subject to conditions such as a negative pregnancy test, but may not receive
refills without a renewal prescription from the prescriber. (Id. at 11:62–12:8.)
The ’720 Claims 2.
The ’720 Patent has two independent claims and 30 dependent claims. Claim 1
is representative and is reproduced below.
In a method for delivering a drug to a patient in need of the drug, while
avoiding the occurrence of an adverse side effect known or suspected of
being caused by said drug, wherein said method is of the type in which
5
Patent No. 6,315,720
prescriptions for said drug are filled only after a computer readable
storage medium has been consulted to assure that the prescriber is
registered in said medium and qualified to prescribe said drug, that the
pharmacy is registered in said medium and qualified to fill the
prescription for said drug, and the patient is registered in said medium
and approved to receive said drug, the improvement comprising:
a. defining a plurality of patient risk groups based upon a
predefined set of risk parameters for said drug;
b. defining a set of information to be obtained from said patient,
which information is probative of the risk that said adverse side effect is
likely to occur if said drug is taken by said patient;
c. in response to said information set, assigning said patient to at
least one of said risk groups and entering said risk group assignment in
said medium;
d. based upon said information and said risk group assignment,
determining whether the risk that said adverse side effect is likely to
occur is acceptable; and
e. upon a determination that said risk is acceptable, generating a
prescription approval code to be retrieved by said pharmacy before said
prescription is filled.
(Ex. 1001 at 18:17–42.) All other claim limitations are listed within Ground 1 below.
The ’720 Prosecution History 3.
During prosecution of U.S. Patent Application No. 09/694,217 (filed October
23, 2000), which led to the ’720 Patent, the Examiner initially rejected Claims 1–27 as
obvious under 35 U.S.C. § 103(a) over U.S. Patent No. 6,045,501 (Ex. 1003, “Elsayed”)
6
Patent No. 6,315,720
in view of U.S. Patent No. 6,063,026 (Ex. 1004, “Schauss”). (See Ex. 1002 at 57–58.1)
At this time, Claims 1–32 were pending. (Id. at 56.) Claim 1, the only independent
claim, recited “a method for delivering a drug to a patient in need of the drug while
avoiding the occurrence of an adverse side effect known or suspected of being caused
by said drug.” (Id. at 44.)
The Examiner rejected Claims 1–27, stating that Elsayed suggested the “use of
the information to evaluate risk levels,” while Schauss taught “a medical diagnostic
analysis system that evaluates patient data obtained from medical testing or patient
questioning for drugs contraindications.” (Id. at 58.) The Examiner concluded that “it
would have been obvious to one of ordinary skill in the art at the time of the invention
to implement the screening for drug contraindications suggested in Elsayed et al. with
the method of Schauss et al., since Schauss et al. teach the particular steps for
performing the analysis.” (Id. at 58.) Regarding Claim 6, the Examiner stated that
although Elsayed “does not specifically teach that data received by facsimile
transmission is entered by an OCR software, it is inherent that this data must be
entered into database.” (Id. at 58.) The Examiner objected to Claims 28–32 “as being
dependent upon a rejected base claim, but would be allowable if rewritten in
independent form.” (Id. at 59.)
1 Except for the prosecution history, exhibit cites herein are directed to the internal
page numbers of the exhibit, rather than to the Exhibit’s Bates numbers.
7
Patent No. 6,315,720
In response, applicants amended Claim 1 by adding, among other limitations,
“upon a determination that said risk is acceptable, generating a prescription approval
code to be retrieved by said pharmacy before said prescription is filled.” (Id. at 87.)
Based on this amendment, applicants argued that “Elsayed, although teaching a
method which contains many of the steps of the present invention, contains no
disclosure of the generation of a prescription approval code as recited in amended
Claim 1.” (Id. at 85.) Applicants further argued that “[a]lthough Schauss may describe
a medical diagnostic analysis system that evaluates patient data obtained from
questioning a patient or medical testing, Schauss contains no disclosure remotely
related to the generation of a prescription approval code, this being the subject of
Applicants’ claims.” (Id. at 86.)
In response, the Examiner rejected the claims as obvious over Elsayed in view of
Schauss and Boyer, U.S. Patent No. 6,202,923 (Ex. 1005, “Boyer”), which “includes a step
for generating a prescription number or code associated with said prescription by a
computer workstation.” (Id. at 91–92.)
In response, applicants argued:
As amended on March 23, 2001, Claim 1 further requires an assessment,
based upon the risk group assignment and the information collected
from the patient, as to whether the risk of the side effect occurring is
acceptable. Upon a determination that the risk is acceptable, and only upon
such a determination, a prescription approval code is generated, which must
be retrieved by the pharmacy before the prescription may be filled. Thus,
8

Patent No. 6,315,720
the prescription approval code is not merely a number that is associated
with the prescription, but instead represents the fact that a determination
has been made that the risk of the side effect occurring is acceptable, and
that approval—an affirmative decision—has been made for the
prescription to be filled. Boyer does not disclose or suggest such an
approval code.
(Id. at 106–07.) Applicants further argued that in Boyer, the prescription number “is
simply an identifier for the prescription, and is not an approval code, as recited in
Applicants’ claims,” and that Boyer provides “no indication that a prescription approval
code, as described and claimed in the instant application, must be generated and
retrieved by the pharmacist before the prescription may be filled.” (Id. at 107.)
The applicants amended Claim 28 to be an independent claim, and then argued
that because “[a]ny proper combination of the disclosure of Boyer with that of
Elsayed and Schauss does not teach or suggest the invention defined by Applicants’
claims,” the Examiner should withdraw the 103 rejection. (Id. at 106–07.)
After this response, all of the ’720 Patent claims were allowed. (Id. at 111.)
B. Claim Construction of Challenged Claims
A claim subject to IPR receives the “broadest reasonable construction in light
of the specification of the patent in which it appears.” 37 C.F.R. § 42.100(b); see In re
Cuozzo Speed Techs., LLC, 778 F.3d 1271, 1279 (Fed. Cir. 2015). In applying such a
standard, the broadest reasonable construction of claim language is not one that
permits any reading, but instead is one that must be made “in light of the specification
9
Patent No. 6,315,720
as it would be interpreted by one of ordinary skill in the art.” In re Am. Acad. of Sci.
Tech. Ctr., 367 F.3d 1359, 1364 (Fed. Cir. 2004) (citation omitted).
Unless otherwise noted, Petitioner accepts, for purposes of IPR only, that the
claim terms of the ’720 Patent are presumed to take on the ordinary and customary
meaning that they would have to one of ordinary skill in the art.2
“Consulted” 1.
“Consulted” means “accessed and considered.” (Ex. 1023 at 3; Ex. 1021 ¶ 39.)
“Teratogenic effect” 2.
“Teratogenic effect” means “any effect that disturbs the normal growth and
development of an embryo or fetus.” (Ex. 1023 at 3; Ex. 1021 ¶ 40.)
2 Petitioner notes that, in some instances, the patentee has defined claim terms apart
from their plain meaning. See Pacing Techs., LLC v. Garmin Int’l, Inc., 778 F.3d 1021,
1024 (Fed. Cir. 2015). These terms include “drug,” “computer readable storage
medium,” “patient risk groups,” “risk parameters,” “risk group assignment,” “likely to
occur,” “prescription approval code,” “counseled,” “risk avoidance measures,” and
“informed consent.” (Ex. 1001 at 3:35–38, 3:45–48, 4:54–56, 5:29–33, 6:30–7:19,
8:45–57, 9:8–26, 10:41–46, 13:44–64.)
10
Patent No. 6,315,720
“Adverse side effect” 3.
“Adverse side effect” means “any unfavorable abnormality, defect, mutation,
lesion, degeneration or injury which may be caused by taking the drug.” (Ex. 1023 at
6; Ex. 1021 ¶ 41; see Ex. 1001 at 3:38–44.)
C. Statement of Precise Relief Requested for Each Claim Challenged
Claims for Which Review is Requested 1.
Petitioner requests IPR under 35 U.S.C. § 311 of Claims 1–32 of the ’720
Patent, and cancellation of these 32 claims as unpatentable.
Statutory Grounds of Challenge 2.
Petitioner requests IPR of Claims 1–32 of the ’720 Patent in view of the
following references, each of which is prior art to the ’720 Patent under 35 U.S.C.
§§ 102(a) and (b) or 103. The Examiner did not reference any of the prior art listed in
the following chart in any Office Action. (See generally, Ex. 1002.) Claims 1–32 are
unpatentable under 35 U.S.C. §§ 102(b) and 103(a):
Ground Proposed Rejections for the ’720 Patent Exhibit Number(s) 1 Claims 1–32 are anticipated under 35 U.S.C. §
102(b) by the Thalidomide Package Insert (Ex. 1006,
“Thalomid PI”).
1006
2 Claims 1–32 are obvious under 35 U.S.C. § 103(a) in
view of Thalomid PI (Ex. 1006) and Cunningham (Ex.
1009).
1006 and 1009
11
Patent No. 6,315,720
D. Overview of the State of the Art
By October of 2000, it was well recognized in the art that teratogenic drugs—
which can cause birth defects—needed to be regulated. (See, e.g., Ex. 1007 at 901–04;
Ex. 1011 at 101–05.) The central regulatory goal was to avoid pregnancy in patients
treated with the drug. (See, e.g., Ex. 1011 at 101.) One notable case of a drug marketed
through methods to prevent its use in pregnant patients is isotretinoin, marketed
under the trade name Accutane®. (See id. at 101.) Rather than remove this drug from
the market once its teratogenicity was realized, isotretinoin became part of a
manufacturer-sponsored Pregnancy Prevention Program (“PPP”). (Id. at 101.) The
program, among other features, included the distribution to physicians of a kit that
included informed consent documents and patient counseling information. (Id. at
101.) In particular, patients were warned against the teratogenic risk of isotretinoin
and the need to prevent pregnancy while taking the drug. (Id. at 105.) Patients were
also advised as to the proper methods of birth control available. (See id. at 103.)
Thalidomide is a drug that originated in Germany in 1957. (Ex. 1001 at 1:40–
41.) Doctors initially prescribed the drug as a sedative, but quickly noticed its
effectiveness in treating a form of leprosy, erythema nodosum leprosum (ENL), as
well. (Ex. 1012 at 320–21.) However, shortly after thalidomide came on the market,
doctors realized that the drug caused severe birth defects in infants whose mothers
took the drug while pregnant. (Ex. 1012 at 320.) As a result, thalidomide was generally
12
Patent No. 6,315,720
taken off of most markets by 1962. (Ex. 1001 at 1:44–45.) Due to thalidomide’s
therapeutic effects, the drug was reintroduced in the United States in the 1990s with
the understanding that it could be marketed only with strict controls, and gained FDA
approval for treatment of ENL in 1998. (See Ex. 1007 at 901; Ex. 1012 at 320.)
Doctors and pharmacists interested in bringing thalidomide to the market with
restrictions to protect from its teratogenic effects considered the Accutane PPP, with
its focus on counseling, as a starting point. (Ex. 1013 at 110–11; see Ex. 1015 at 1.)
They also considered modeling a thalidomide program on experiences with other
hazardous drugs, including clozapine (trade name Clozaril®). (Ex. 1013 at 111–12.)
As early as 1997, medical professionals observed that the prescription control
methods for clozapine, an anti-depressant with potential adverse effects indicated by
white blood cell counts (“WBCs”), could be copied for thalidomide. (Ex. 1013 at
112.) In particular, these prescription control methods included keeping records of
patients taking the drug, as well as physicians and pharmacists pre-approved to
prescribe and dispense the drug. (Ex. 1008 at 899–900; see Ex. 1013 at 115–19;
Ex. 1015 at 9, 24.) The clozapine patients were also required to submit to weekly
WBC testing and could only have a prescription for clozapine filled if the test results
fell within a pre-designated range. (Ex. 1008 at 899; see Ex. 1013 at 112; Ex. 1015 at 8.)
“It was also well known in the art prior to 2000 to keep prescription records in
a computerized system.” (See, e.g., Ex. 1016 at 174; Ex. 1017 at 56, 60–63, 68; Ex. 1021
¶ 56.) Such records would include information such as the patient’s sex, allergies,
13
Patent No. 6,315,720
height, weight, and other health-related measures. (See Ex. 1017 at 59; Ex. 1021 ¶ 56.)
Physicians and pharmacists had used computerized systems to track their patients
since at least 1975. (See, e.g., Ex. 1017 at 53; Ex. 1016 at 174, 182–83.) Practitioners
then used this data to determine (1) whether to prescribe a drug to a patient, and (2)
the duration of the prescription. (See Ex. 1017 at 53, 63–67.)
Thus, in the case of thalidomide or any other teratogenic drug, those of
ordinary skill in the art would have been—and indeed were—motivated to combine
the method for avoiding pregnancy with a computerized tracking system that only
permits filling prescriptions for the drug when certain conditions (e.g., non-pregnancy)
are met. (See Ex.1013 at 111–12; Ex. 1021, ¶ 59.) An example of this combination,
discussed in detail below, is the System for Thalidomide Education and Prescribing
Safety (S.T.E.P.S.)—“a comprehensive program to control prescribing, dispensing,
and use of” thalidomide to ensure that fetal exposure to thalidomide does not occur.
(Ex. 1006 at 1, 2, 3; Ex. 1012 at Abstract; see Ex. 1021 ¶ 59.)
VI. DETAILED EXPLANATION OF THE CHALLENGE
A. Ground 1: THALOMID™ (thalidomide) Capsules Revised Package Insert anticipates Claims 1–32 of U.S. Patent No. 6,315,720 under 35 U.S.C. § 102(b).
The ’720 Patent’s method for delivering a drug to a patient while avoiding the
occurrence of an adverse side effect was known before October 23, 2000—the earliest
possible priority date for the ’720 Patent—as evidenced by the THALOMID™
(thalidomide) Capsules Revised Package Insert (15 July 1998) (“Thalomid PI”). (See
14
Patent No. 6,315,720
Ex. 1006 at 1.) Thalomid PI was published on July 15, 1998, and is prior art under 35
U.S.C. § 102(b). (Ex. 1006 at 1.) Thalomid PI was not considered by the USPTO during
prosecution of the ’720 Patent. (Ex. 1001 at Cover.)
Thalomid PI describes a method for delivering thalidomide to a patient in need
of the drug, while avoiding the occurrence of severe, life-threatening birth defects.
(Ex. 1006 at 1.) Specifically, Thalomid PI recites:
BECAUSE OF THIS TOXICITY AND IN AN EFFORT TO MAKE
THE CHANCE OF FETAL EXPOSURE TO THALOMID AS
NEGLIGIBLE AS POSSIBLE, THALOMID IS APPROVED FOR
MARKETING ONLY UNDER A SPECIAL RESTRICTED
DISTRIBUTION PROGRAM APPROVED BY THE FOOD AND
DRUG ADMINISTRATION. THIS PROGRAM IS CALLED THE
“SYSTEM FOR THALIDOMIDE EDUCATION AND
PRESCRIBING SAFETY (S.T.E.P.S.).”
(Ex. 1006 at 1.) Thalomid PI also states:
UNDER THIS RESTRICTED DISTRIBUTION PROGRAM, ONLY
PRESCRIBERS AND PHARMACISTS REGISTERED WITH THE
PROGRAM ARE ALLOWED TO PRESCRIBE AND DISPENSE
THE PRODUCT. IN ADDITION, PATIENTS MUST BE ADVISED
OF, AGREE TO, AND COMPLY WITH THE REQUIREMENTS
OF THE S.T.E.P.S. PROGRAM IN ORDER TO RECEIVE
PRODUCT.
(Ex. 1006 at 1.)
15

Patent No. 6,315,720
Thalomid PI further teaches that “a prescription for thalidomide for a woman of
childbearing potential must not be issued by the prescriber until a written report of a
negative pregnancy test has been obtained by the prescriber.” (Id at 2.) Further,
Thalomid PI requires that, for these women to receive the drug, “[t]wo reliable forms
of contraception must be used simultaneously. … Women of childbearing potential
should be referred to a qualified provider of contraceptive methods, if needed.” (Id. at
2.) Thalomid PI further discloses that “[t]halidomide is contraindicated in sexually
mature MALES.…” (Id. at 4.) Based on these disclosures, Thalomid PI teaches the
subject matter claimed in the ’720 Patent – a method of delivering drug to a patient in
need of the drug while avoiding the occurrence of a known adverse side effect. (Id. at
1–4; Ex. 1021 ¶ 76.)
To anticipate a claim, a prior art reference must disclose each claim limitation,
either expressly or inherently. Verdegaal Bros. v. Union Oil Co. of California, 814 F.2d 628,
631 (Fed. Cir. 1987). “[I]f granting patent protection on the disputed claim would
allow the patentee to exclude the public from practicing the prior art, then that claim
is anticipated, regardless of whether [the claim] also covers subject matter not in the
prior art.” Atlas Powder Co. v. IRECO, Inc., 190 F.3d 1342, 1349 (Fed. Cir. 1999) (citing
Titanium Metals Corp. v. Banner, 778 F.2d 775, 781 (Fed. Cir. 1985)). The patent
protection previously granted to Claims 1–32 of the ’720 Patent excludes the public
from practicing Thalomid PI, so the ’720 Patent claims should be canceled.
16
Patent No. 6,315,720
To explain the meaning of an anticipatory prior art reference or to describe the
technical knowledge available to persons skilled in the art, extrinsic evidence may be
used; however, extrinsic evidence may not be used to expand on, or fill in gaps in an
anticipation prior art reference. In re Baxter Travenol Labs, 952 F.2d 388, 390 (Fed. Cir.
1991); Continental Can Co. USA, Inc. v. Monsanto Co., 948 F.2d 1264 (Fed. Cir. 1991).
Here, the Keravich reference and the Fudin Declaration are used to explain the
meaning of Thalomid PI and to explain the technical facts known in the medical
community more than one year before the ’720 Patent filing, but they are not used to
expand on or fill in any gaps in Thalomid PI—which by itself, as understood by a
POSA—contains every claim limitation of the ’720 Patent. (See generally, Ex. 1018; Ex.
1021.)
Thalomid PI anticipates Claim 1. 1.
Claim 1 of the ’720 Patent “is written in Jepson format, meaning that the claim
first describes the scope of the prior art and then claims an improvement over the
prior art.” Dow Chem. Co. v. Sumitomo Chem. Co., 257 F.3d 1364, 1368 (Fed. Cir. 2001).
Specifically, the Claim 1 preamble recites:
In a method for delivering a drug to a patient in need of the drug, while
avoiding the occurrence of an adverse side effect known or suspected of
being caused by said drug, wherein said method is of the type in which
prescriptions for said drug are filled only after a computer readable
storage medium has been consulted to assure that the prescriber is
registered in said medium and qualified to prescribe said drug, that the
17
Patent No. 6,315,720
pharmacy is registered in said medium and qualified to fill the
prescription for said drug, and the patient is registered in said medium
and approved to receive said drug, the improvement comprising:
(Ex. 1001 at 18:17–27.) (emphasis added) Because “a preamble is impliedly admitted
to be prior art when a Jepson claim is used,” the patentee has admitted that the Claim
1 preamble is prior art, rather than a point of novelty. Pentec, Inc. v. Graphic Controls
Corp., 776 F.2d 309, 315 (Fed. Cir. 1985); see In re Glatt Air Techniques, Inc., 630 F.3d
1026, 1028 (Fed. Cir. 2011) (rejecting a claim “as obvious in view of the admitted
prior art from the claim preamble and a single cited reference”).
Thalomid PI teaches every element of Claim 1 of the ’720 Patent, including
“defining a plurality of patient risk groups based upon a predefined set of risk
parameters for said drug” as required by Claim 1(a), “defining a set of information to
be obtained from said patient, which information is probative of the risk that said
adverse side effect is likely to occur if said drug is taken by said patient” as required by
Claim 1(b), “in response to said information set, assigning said patient to at least one
of said risk groups” as required by the first portion of Claim 1(c), “based upon said
information and said risk group assignment, determining whether the risk that said
adverse side effect is likely to occur is acceptable” as required by Claim 1(d), and
“upon a determination that said risk is acceptable, generating a prescription approval
code to be retrieved by said pharmacy before said prescription is filled” as required by
Claim 1(e). (See Ex. 1001 at 28–42; Ex. 1006 at 1, 3–4, 18; Ex. 1021 ¶ 76.)
18
Patent No. 6,315,720
Specifically, Thalomid PI teaches the risk groups to which a drug with
teratogenic side effects, such as thalidomide, cannot be administered, as in Claim
1(a), because of an unacceptable risk of teratogenic side effects to a fetus, as in Claim
1(d). (See Ex. 1006 at 3–4; Ex. 1021 ¶¶ 83–84, 97–99.) Thalomid PI’s risk group list
includes, for example, “WOMEN of childbearing potential,” further differentiated by
those who do and do not meet a listed set of conditions, as well as “sexually mature
“MALES,” also further differentiated by those who do and do not meet a listed set of
conditions. (Ex. 1006 at 3–4.) One of ordinary skill in the art would understand that a
prescriber would assign a patient to these various risk groups, as in the first portion of
Claim 1(c), by obtaining information from the patient such as their gender,
“childbearing potential” and whether they meet the listed set of conditions for their
gender, which are “probative of the risk that said adverse side effect is likely to occur
if said drug is taken by said patient,” as in Claim 1(b). (Ex. 1006 at 3–4; Ex. 1021
¶¶ 85–90.)
With respect to the second portion of Claim 1(c)—“entering said risk group in
said medium”—Thalomid PI discloses entering the patient’s information in a computer
readable medium. (Ex. 1006 at 3–4.) For example, Thalomid PI requires that the patient
“is capable of complying with the mandatory contraceptive measures, pregnancy
testing, patient registration, and patient survey as described in the System for
Thalidomide Education and Prescribing Safety (S.T.E.P.S.) program.” (Id. at 3–4.)
Thalomid PI further requires:
19
Patent No. 6,315,720
UNDER THIS RESTRICTED DISTRIBUTION PROGRAM, ONLY
PRESCRIBERS AND PHARMACISTS REGISTERED WITH THE
PROGRAM ARE ALLOWED TO PRESCRIBE AND DISPENSE
THE PRODUCT. IN ADDITION, PATIENTS MUST BE ADVISED
OF, AGREE TO, AND COMPLY WITH THE REQUIREMENTS
OF THE S.T.E.P.S. PROGRAM IN ORDER TO RECEIVE
PRODUCT.
(Id. at 1.) An ordinarily skilled artisan would have understood from Thalomid PI “that
the S.T.E.P.S. program must include the patient’s risk group assignment data in a
computer database” for “prescribers and pharmacists to access the patient’s
information before they prescribe and fill prescriptions for thalidomide.” (Ex. 1021 ¶
95.)
The final portion of Claim 1—Claim 1(e)—requires that, “upon a
determination that said risk is acceptable, generating a prescription approval code to
be retrieved by said pharmacy before said prescription is filled.” (Ex. 1001 at 18:40–
42.) This mechanism would have been recognized by an ordinarily skilled artisan as
inherent in the system disclosed by Thalomid PI. (Ex. 1021 ¶¶ 105–06.) Specifically,
Thalomid PI discloses the following details about Celgene’s S.T.E.P.S. program:
UNDER THIS RESTRICTED DISTRIBUTION PROGRAM, ONLY
PRESCRIBERS AND PHARMACISTS REGISTERED WITH THE
PROGRAM ARE ALLOWED TO PRESCRIBE AND DISPENSE
THE PRODUCT. IN ADDITION, PATIENTS MUST BE ADVISED
OF, AGREE TO, AND COMPLY WITH THE REQUIREMENTS
20
Patent No. 6,315,720
OF THE S.T.E.P.S. PROGRAM IN ORDER TO RECEIVE
PRODUCT.
(Ex. 1006 at 1.) Thalomid PI further explains:
THALOMID MUST ONLY BE ADMINISTERED IN
COMPLIANCE WITH ALL OF THE TERMS OUTLINED IN THE
S.T.E.P.S. PROGRAM. THALOMID MAY ONLY BE PRESCRIBED
BY PRESCRIBERS REGISTERED WITH THE S.T.E.P.S.
PROGRAM AND MAY ONLY BE DISPENSED BY
PHARMACISTS REGISTERED WITH THE S.T.E.P.S. PROGRAM.
(Ex. 1006 at 18.) One of ordinary skill in the art would have known that an approval
code system—such as that required by Claim 1(e)—was one of the mechanisms
“outlined in the S.T.E.P.S. program,” and inherent in Thalomid PI’s requirement that
“THALOMID MUST ONLY BE ADMINISTERED IN COMPLIANCE WITH
ALL OF THE TERMS OUTLINED IN THE S.T.E.P.S. PROGRAM.” (Ex. 1006 at
18; Ex. 1021 ¶¶ 104–05.) See Schering Corp. v. Geneva Pharms., Inc., 339 F.3d 1373, 1377
(Fed. Cir. 2003) (“[A] prior art reference may anticipate without disclosing a feature of
the claimed invention if that missing characteristic is necessarily present, or inherent,
in the single anticipating reference (quoting Continental Can Co. U.S.A. Inc. v. Monsanto
Co., 948 F.2d 1264, 1268 (Fed. Cir. 1991))” (emphasis added).); see also In re Graves, 69
F.3d 1147, 1152 (Fed. Cir. 1995) (“A reference anticipates a claim if it discloses the
claimed invention ‘such that a skilled artisan could take its teachings in combination
with his own knowledge of the particular art and be in possession of the invention.’”)
(quoting In re LeGrice, 301 F.2d 929, 936 (CCPA 1962).
21
Patent No. 6,315,720
Thalomid PI anticipates Claims 2–6. 2.
Each of Claims 2 through 6 of the ’720 Patent directly or indirectly depends
from Claim 1, and merely add limitations anticipated by Thalomid PI. Claim 2 requires
that “in response to said risk group assignment, said patient is counseled as to the
risks of taking said drug and advised as to risk avoidance measures,” while Claim 3
requires that the Claim 2 “counseling comprises full disclosure of said risks,” Claim 4
requires that “said prescription is filled only following [the Claim 3] full disclosure and
informed consent of said patient,” Claim 5 requires that “said risk group assignment
and [Claim 4] informed consent is verified by said prescriber at the time that said
patient is registered in said computer readable storage medium,” and Claim 6 requires
that “said risk group assignment and said informed consent is transmitted to [the
Claim 5] computer readable storage medium by facsimile and interpreted by optical
character recognition software.” (Ex. 1001 at 18:43–58 (emphasis added).)
“Thalomid PI requires counseling patients regarding thalidomide risks and risk
avoidance measures.” (Ex. 1006 at 2, 9, 10, 13; Ex. 1021 ¶ 108.) For example, Thalomid
PI teaches that “Thalidomide is contraindicated in WOMEN of childbearing potential
unless” “she has received both oral and written warnings of the hazards of taking
thalidomide during pregnancy and of exposing a fetus to the drug,” and “she has
received both oral and written warnings of the risk of possible contraception failure
and of the need to use two reliable forms of contraception simultaneously.” (Ex. 1006
22

Patent No. 6,315,720
at 3.) Therefore, Thalomid PI’s disclosure anticipates the counseling requirements of
Claims 2 and 3. (Ex. 1021 ¶ 110.)
Further, the second portion of Claim 3 requires that “counseling comprises
full disclosure of said risks.” (Ex. 1001 at 18:46–47.) Thalomid PI requires that
“[p]atients should be instructed” of all thalidomide risks including, for example,
“potential teratogenicity,” “drowsiness and somnolence,” “peripheral neuropathies,”
and “orthostatic hypotension.” (Ex. 1006 at 11.) Thalomid PI further requires that the
physician has “fully explained to the patient the nature, purpose, and risks of the
treatment,” as required by the ’720 Patent’s Claim 3. (Ex. 1006 at 21.) Thus, Thalomid
PI anticipates the full disclosure requirement of Claim 3. (Ex. 1021 ¶ 113.)
With respect to Claims 4 and 5 of the ’720 Patent, Thalomid PI’s
“Authorization” form teaches that the physician has “fully explained to the patient the
nature, purpose, and risks of the treatment … [and] will ensure that the appropriate
components of the patient consent form are completed. In addition, I will comply
with all of my obligations and responsibilities as a prescriber registered under the
S.T.E.P.S. restricted distribution program.” (Ex. 1006 at 21.) These teachings
anticipate the disclosure and informed consent prerequisites of Claim 4, as well as the
consent verification of Claim 5. The Claim 5 consent and risk group verification at
the time of patient registration is inherently anticipated by Thalomid PI’s warning:
PATIENTS MUST BE ADVISED OF, AGREE TO, AND COMPLY
WITH THE REQUIREMENTS OF THE S.T.E.P.S. PROGRAM IN
23
Patent No. 6,315,720
ORDER TO RECEIVE PRODUCT. … THALOMID MUST ONLY
BE ADMINISTERED IN COMPLIANCE WITH ALL OF THE
TERMS OUTLINED IN THE S.T.E.P.S. PROGRAM.
(Id. at 1, 18.)
One of ordinary skill in the art would have known that, as part of the
physician’s requirements under “THE TERMS OUTLINED IN THE S.T.E.P.S.
PROGRAM” to ensure that the patient was “ADVISED OF, AGREE[S] TO, AND
COMPL[IES] WITH THE REQUIREMENTS OF THE S.T.E.P.S. PROGRAM,”
“the physician was required to verify the patient’s risk group and informed consent” at
the time of “registering the patient in the database,” as Claim 5 requires. (Ex. 1021 ¶ 119
(emphasis added.) See Schering Corp. v. Geneva Pharms., Inc., 339 F.3d at 1377. For
example, Keravich—published more than one year before the earliest priority date of
the ’720 Patent—explains that the S.T.E.P.S. program “patient database provides
critical patient-related information that is found on the consent form.” (Ex. 1018 at
1723.) Indeed, the prescriber must use information from the patient’s informed
consent form—which Thalomid PI discloses is a different form for male and female
patients and so indicative of the patient’s risk group—when registering the patient in
the database. (See Ex. 1006 at 20–21.) Therefore, Thalomid PI also anticipates Claim 5
of the ’720 Patent. (Ex. 1006 at 3, 4, 21; Ex. 1021 ¶ 120.)
Thalomid PI discloses that the informed consent and risk group assignment are
transmitted to the S.T.E.P.S. program database described above with respect to Claim
24
Patent No. 6,315,720
1(c), and as required by the first portion of Claim 6. (Ex. 1021 ¶ 121.) As with Claim
5, Thalomid PI’s disclosure that the S.T.E.P.S program must be followed would
inherently disclose to one of ordinary skill in the art that one way that a patient’s
informed consent and risk group assignment are transmitted to the S.T.E.P.S.
database is through fax, which is then interpreted by optical character recognition
(OCR) software. (Ex. 1021 ¶¶ 127–29.) For example, Keravich explains that “Celgene
provides telephone and fax services for patient registration, patient approval, and
prescriber verification.” (Ex. 1018 at 1723–24.) Keravich further explains that the
S.T.E.P.S. program “patient database provides critical patient-related information that
is found on the consent form,” thus making clear that the S.T.E.P.S. program
disclosed in Thalomid PI inherently requires that the faxed informed consent
information make it into the database, which one of ordinary skill in the art would
have known to be interpreted through OCR means as Claim 6 requires. (Ex. 1018 at
1723; Ex. 1021 ¶ 129.) See In re Graves, 69 F.3d 1147, 1152 (Fed. Cir. 1995) (“A
reference anticipates a claim if it discloses the claimed invention ‘such that a skilled
artisan could take its teachings in combination with his own knowledge of the
particular art and be in possession of the invention.’”) (quoting In re LeGrice, 301 F.2d
929, 936 (CCPA 1962)).
Thalomid PI anticipates Claims 7–10. 3.
Claims 7–10 depend from Claim 1, and merely add limitations anticipated by
Thalomid PI. Claim 7 requires that the “information to be obtained from said patient,”
25
Patent No. 6,315,720
prior to treatment, “includes the results of diagnostic testing,” while Claims 8, 9, and
10 respectively require that the diagnostic testing “is probative of the onset of said
adverse side effect,” “is probative of the concentration of said drug in a tissue of said
patient,” and “comprises genetic testing.” (Ex. 1001 at 18:59–67.)
Thalomid PI discloses diagnostic testing, including testing “probative of the
onset of said adverse side effect,” anticipating the additional limitations of Claims 7
and 8. Specifically, Thalomid PI teaches that “[b]efore starting treatment, women of
childbearing potential should have a pregnancy test … within the 24 hours prior to
beginning therapy” because “IF THALIDOMIDE IS TAKEN DURING
PREGNANCY, IT CAN CAUSE SEVERE BIRTH DEFECTS OR DEATH TO
AN UNBORN BABY.” (Ex. 1006 at 1–2.)
With respect to Claim 9, Thalomid PI teaches that “[d]ecreased white blood cell
counts, including neutropenia, have been reported in association with the clinical use
of thalidomide. … White blood cell count and differential should be monitored on an
on-going basis.” (Ex. 1006 at 10.) From this teaching, a person of ordinary skill in the
art “would have recognized the need to conduct diagnostic testing probative of the
concentration of the drug remaining in the patient’s body.” (Ex. 1021 ¶ 136.)
However, because many drugs do not generally distribute uniformly in the body, but
instead are preferentially absorbed by certain body tissues, one of ordinary skill in the
art would have further recognized the importance of performing diagnostic testing
that would be probative of the concentration of such a non-uniformly distributed
26
Patent No. 6,315,720
drug in the drug’s target tissues. (Ex. 1021 ¶ 138–39.) See In re Cruciferous Sprout
Litigation, 301 F.3d 1343, 1345 (Fed. Cir. 2002) (“The patent owners had not done
anything more than recognize properties inherent in certain prior art sprouts, and had
not invented anything new, and therefore, their claims were invalid.”).
With respect to Claim 10, a person of ordinary skill in the art “would have
recognized genetic testing as one of the tests” in “the extensive diagnostic testing
taught by Thalomid PI.” (Ex. 1021 ¶ 142.) Specifically, it was common in the art at the
time of the ’720 Patent “to conduct genetic testing at the same time as the pregnancy
testing taught in Thalomid PI.” (Ex. 1021 ¶ 141.) Because thalidomide was known to
cause birth defects at the time of the ’720 Patent, a person of ordinary skill in the art
would have recognized that the extensive diagnostic testing in Thalomid PI would
include genetic testing. (Ex. 1021 ¶ 143.) More generally, because genetic testing was a
well-known diagnostic procedure at the time of the ’720 Patent, one of ordinary skill
in the art would have included genetic testing as one of the methods in the diagnostic
testing for thalidomide therapy. (Ex. 1021 ¶ 141.) See Schering Corp., 339 F.3d at 1377;
see also In re Graves, 69 F.3d 1147, 1152 (Fed. Cir. 1995) (“A reference anticipates a
claim if it discloses the claimed invention ‘such that a skilled artisan could take its
teachings in combination with his own knowledge of the particular art and be in
possession of the invention.’”) (quoting In re LeGrice, 301 F.2d 929, 936 (CCPA 1962).
27
Patent No. 6,315,720
Thalomid PI anticipates Claims 11–14 and 20–25. 4.
Claims 11–14, and 21–25 depend from Claim 1, and merely add limitations
anticipated by Thalomid PI. Claims 11, 12, and 13 respectively require that the drug’s
associated side effect “is likely to arise in said patient,” “is likely to arise in a foetus
carried by said patient,” and “is likely to arise in a recipient or a foetus carried by a
recipient of the bodily fluid of said patient,” while Claim 14 requires that the Claim
12 “recipient is a sexual partner of said patient.” (Ex. 1001 at 19:1–9.) Claim 22
requires that the “drug is thalidomide.” (Ex. 1001 at 19:34–35.) Claim 21 requires that
the drug’s associated side effect “comprises a teratogenic effect,” while Claims 23
and 24 respectively require that the Claim 21 teratogenic effect “is likely to arise in a
foetus carried by said patient,” and “is likely to arise in a foetus carried by a recipient
of the bodily fluid of said patient.” Claim 25 requires that the Claim 24 “recipient of
the bodily fluid of said patient is a sexual partner of said patient.” (Ex. 1001 at 19:32–
33, 36–42.) Claim 20 requires “providing said patient with a contraceptive device or
formulation.” (Ex. 1001 at 19:30–31.)
“Thalomid PI explicitly discloses that thalidomide’s side effects arise in the
patient taking the drug”—in the case of “peripheral neuropathy,” “and also in a fetus
carried by the patient taking the drug”—in the case of “teratogenicity,” anticipating
Claims 11, 12, 21, 22 and 23. (Ex. 1006 at 1, 2, 8, 9, 10; Ex. 1021 ¶ 149–50.)
Thalomid PI also explicitly discloses that thalidomide side effects likely arise in a
sexual partner and recipient of bodily fluid of a male treated with the drug,
28
Patent No. 6,315,720
anticipating Claims 13, 14, and 25, or in the fetus of this sexual partner, anticipating
in Claims 13 and 24.For example, Thalomid PI discloses that “[b]ecause it is not
known whether or not thalidomide is present in the ejaculate of males receiving the
drug, males receiving thalidomide must always use a latex condom when engaging in
sexual activity with women of childbearing potential.” (Ex. 1006 at 9.) Thalomid PI
further discloses that “male patients should be instructed that they are not permitted
to donate sperm while taking thalidomide;” and that male patients “must NEVER
have unprotected sex with a woman because it is not known if the drug is present in
semen or sperm.” (Ex. 1006 at 11, 21.)
Finally, with respect to Claim 20, Thalomid PI teaches informing patients that
“[e]ffective contraception … must be used for at least 1 month before beginning
thalidomide therapy, during thalidomide therapy, and for 1 month following
discontinuation of thalidomide therapy. … Women of childbearing potential should
be referred to a qualified provider of contraceptive methods, if needed.” (Ex. 1006 at
2 (emphasis added).) Thalomid PI further teaches:
Women must commit either to abstain continuously from heterosexual
sexual intercourse or to use two methods of reliable birth control,
including at least one highly effective method (e.g., IUD, hormonal
contraception, tubal ligation, or partner’s vasectomy) and one additional
effective method (e.g., latex condom, diaphragm, or cervical cap),
beginning 4 weeks prior to initiating treatment with thalidomide, during
29
Patent No. 6,315,720
therapy with thalidomide, and continuing for 4 weeks following
discontinuation of thalidomide therapy.
(Id. at 8–9.) In light of Thalomid PI’s teachings, a person of ordinary skill in the art
would have inherently understood that when a potential patient for whom
contraception was a prerequisite for taking thalidomide was referred to a “qualified
provider of contraceptive methods,” that doctor would provide the “patient with a
contraceptive device or formulation” as in Claim 20, in order to accomplish Thalomid
PI’s objective of ensuring that “[w]omen of childbearing potential” taking thalidomide
took “reliable contraceptive precautions.” (Ex. 1006 at 2; Ex. 1021 ¶ 159.) See In re
Graves, 69 F.3d at 1152.
Thalomid PI anticipates Claim 15. 5.
Claim 15 depends from Claim 1, and merely adds limitations anticipated by
Thalomid PI. Claim 15 requires “f. defining for each said risk group a second set of
information to be collected from said patient on a period basis; g. obtaining said
second set of information from said patient; and h. entering said second set of
information in said medium before said patient is approved to receive said drug.”
(Ex. 1001 at 19:10–18.)
Thalomid PI explicitly discloses defining information to be collected and
periodically obtaining that information from the patient as in Claim 15(f) and (g).
For example, Thalomid PI discloses, “Once treatment has started, pregnancy testing
should occur weekly during the first month of use, then monthly thereafter,” and that
30
Patent No. 6,315,720
the patient consents that “I understand that I must participate in a survey and patient
registry while I am on THALOMIDTM.” (Id. at 2, 20–21.) Further, as previously
discussed above with respect to the second portion of Claim 1(c)—Thalomid PI
discloses that the patient’s periodic evaluations are stored in the S.T.E.P.S. program.
(Id. at 10.) Thalomid PI additionally discloses that “Drug prescribing to women of
childbearing potential should be contingent upon initial and continued
confirmed negative results of pregnancy testing.” (Id. at 18.) From these teachings
requiring periodic test results and computer approval before drug distribution, one of
ordinary skill in the art would have recognized that, to make use of the computerized
tracking, the periodic test results inherently must be entered in the “medium before
said patient is approved to receive said drug,” as required by Claim 15(h). (Id. at 10;
Ex. 1021 ¶ 168–69.) See Schering Corp., 339 F.3d at 1377.
Thalomid PI anticipates Claims 16–17. 6.
Claims 16–17 depend from Claim 1, and merely add limitations anticipated by
Thalomid PI. Claim 16 requires that the Claim 15 second set of information
“comprises a survey regarding said patient’s behavior and compliance with said risk
avoidance measures,” while Claim 17 requires that the Claim 16 survey “is conducted
telephonically using an integrated voice response system.” (Ex. 1001 at 19:19–24.)
With respect to Claim 16’s requirement of “a survey regarding said patient’s
behavior and compliance with said risk avoidance measures,” Thalomid PI teaches the
importance of compliance with risk avoidance measures, as well as pre-treatment
31
Patent No. 6,315,720
interview surveys regarding the patient’s behavior and ability to comply with risk
avoidance measures. For example, Thalomid PI requires that the patient sign an
authorization stating “I understand that if I do not follow all of my doctor’s
instructions, I will not be able to receive THALOMIDTM” and “I understand that I
must participate in a survey and patient registry while I am on THALOMIDTM.”
(Ex. 1006 at 20–21.) Thalomid PI also requires that the patient “is capable of
complying with the mandatory contraceptive measures, pregnancy testing, patient
registration, and patient survey as described in the System for Thalidomide Education
and Prescribing Safety (S.T.E.P.S.) program.” (Id. at 3, 4.) Additionally, the required
survey for “continued confirmed negative results of pregnancy testing”—an
indicator of the patient’s behavior and compliance with the required risk avoidance
measures—anticipates the Claim 16 requirements. (Id. at 18; Ex. 1021 ¶ 176.)
Just as for Claims 5 and 6, Thalomid PI’s disclosure that the S.T.E.P.S program
must be followed would inherently disclose to one of ordinary skill in the art that one
way that a patient’s required survey may be conducted is via telephone, and
specifically utilizing a telephonic integrated voice response system as required by
Claim 17. (Ex. 1021 ¶ 178–79.) For example, Keravich explains that, under the
S.T.E.P.S. program, “[p]atients are eligible to continue to receive thalidomide if they
… [p]articipate in a mandatory and confidential patient survey every 30 days (women)
or every 90 days (men),” and that for subsequent prescriptions, “[o]nce patient
eligibility is confirmed, the prescription needs to be authorized through online
32
Patent No. 6,315,720
adjudication, fax submission, or telephone contact with Celgene.” (Ex. 1018 at 1722–
23 (emphasis added).) See Schering Corp., 339 F.3d at 1377; see also SmithKline Beecham
Corp. v. Apotex Corp., 403 F.3d 1331, 1343 (Fed. Cir. 2005).
Thalomid PI anticipates Claims 18–19 and 26–27. 7.
Claims 18–19 and 26–27 ultimately depend from Claim 1, and merely add
limitations anticipated by Thalomid PI. Claim 18 requires that, where the “patient is a
female of childbearing potential,” the Claim 15 second set of information collected on
a periodic basis “comprises the results of a pregnancy test,” while Claim 19 requires
that the periodic interval for the Claim 18 pregnancy test “comprises about 28 days.”
(Ex. 1001 at 19:25–29.) Claim 26 similarly requires that, where the drug has a
teratogenic effect, the “information to be obtained from said patient” “includes the
results of a pregnancy test,” while Claim 27 adds to the requirements of Claim 26 that
“said prescription is filled for no more than about 28 days.” (Ex. 1001 at 19:43–20:2.)
Thalomid PI explicitly discloses that, in light of thalidomide’s “teratogenicity,”
“[b]efore starting treatment, women of childbearing potential should have a
pregnancy test … within the 24 hours prior to beginning therapy,” as required by
Claim 26. (Ex. 1006 at 2; see also Id. at 9, 11–12, 20.)
Thalomid PI further anticipates the Claim 18 and 19 requirements for obtaining
periodic pregnancy test results every about 28 days by requiring that the patient
acknowledge “I know that I must have a pregnancy test done every week during the
first 4 weeks of THALOMID therapy. I will then have a pregnancy test every 4 weeks
33
Patent No. 6,315,720
if I have regular menstrual cycles, or every 2 weeks if my cycles are irregular while I
am taking THALOMID.” (Ex. 1006 at 20.)
Thalomid PI also explicitly discloses that prescriptions must be filled “for no
more than about 28 days,” as in Claim 27. For example, Thalomid PI discloses that
patients must “have a pregnancy test every 4 weeks … while I am taking
THALOMID,” that “[d]rug prescribing to women of childbearing potential
should be contingent upon initial and continued confirmed negative results of
pregnancy testing” occurring every 28 days, and that the “DRUG MUST ONLY
BE DISPENSED IN NO MORE THAN A 1-MONTH SUPPLY.” (Ex. 1006 at 18–
19 (emphasis added); Ex. 1021 ¶¶ 185–88.)
Thalomid PI anticipates Claims 28–32. 8.
Claim 28, although an independent claim, merely repeats the language of Claim
1 with a single added limitation anticipated by Thalomid PI. Claims 29–32 depend from
Claim 28, and similarly add limitations already known in the field and anticipated by
Thalomid PI. In addition to the exact requirements of Claim 1, Claim 28 requires that
“said adverse side effect is likely to arise in patients who take said drug in combination
with at least one other drug.” (Ex. 1001 at 20:3–31.) Claims 29 and 30 respectively
require that the “information to be obtained from said patient” “is also probative of
the likelihood that said patient may take said drug and said other drug in
combination,” and “includes the results of diagnostic testing,” while Claims 31 and
32 respectively require that the Claim 30 diagnostic testing “comprises testing for
34

Patent No. 6,315,720
evidence of the use of said other drug” and “comprises testing for evidence which is
indicative of the onset of said adverse event.” (Ex. 1001 at 20:32–42.)
Thalomid PI teaches that thalidomide in combination with other drugs would
cause adverse side effects in patients. (Ex. 1006 at 12.) For example, Thalomid PI
teaches, “Drug Interactions. Thalidomide has been reported to enhance the sedative
activity of barbiturates, alcohol, chlorpromazine, and reserpine.…” (Id. at 12.)
Thalomid PI further teaches that “[m]edications known to be associated with peripheral
neuropathy should be used with caution in patients receiving thalidomide.” (Id. at 12.)
Because these Thalomid PI teachings satisfy “adverse side effect is likely to arise in
patients who take said drug in combination with at least one other drug,” as required
by Claim 28, Thalomid PI anticipates Claim 28.
As previously discussed with respect to Claims 7 and 8, Thalomid PI discloses
extensive diagnostic testing, including testing “for evidence which is indicative of the
onset of said adverse side effect” prior to treatment, anticipating Claims 30 and 32.
Specifically, Thalomid PI teaches that “[b]efore starting treatment, women of
childbearing potential should have a pregnancy test. … The test should be performed
within the 24 hours prior to beginning therapy” because “IF THALIDOMIDE IS
TAKEN DURING PREGNANCY, IT CAN CAUSE SEVERE BIRTH DEFECTS
OR DEATH TO AN UNBORN BABY.” (Ex. 1006 at 1–2.)
Thalomid PI teaches “Drug Interactions. Thalidomide has been reported to
enhance the sedative activity of barbiturates, alcohol, chlorpromazine, and reserpine,”
35
Patent No. 6,315,720
which reports that patient data regarding taking Thalomid in combination with other
drugs has been collected, as required by Claim 29. (Id. at 12.) Thalomid PI further
teaches that “[m]edications known to be associated with peripheral neuropathy should
be used with caution in patients receiving thalidomide.” (Id. at 12.) In light of these
teachings, a person of ordinary skill in the art would have recognized that the
extensive patient consultations would have included questioning regarding other drugs
the patient may take along with Thalomid, as required by Claim 29. (Ex. 1021 ¶ 208.)
With respect to Claim 31, Thalomid PI discloses diagnostic “testing for evidence
of the use of said other drug.” For example, Thalomid PI discloses testing
pharmacokinetic profiles of patients on oral contraceptives—“[i]n 10 healthy women,
the pharmacokinetic profiles of norethindrone and ethinyl estradiol following
administration of a single dose containing 1.0 mg of norethindrone acetate and 75 μg
of ethinyl estradiol were studied. The results were similar with and without
coadministration of thalidomide 200 mg/day to steady-state levels.” (Id. at 12.)
Claim chart for Ground 1 showing exemplary citations in 9.Thalomid PI.
Element Prior Art 1pre. In a method for delivering a drug to a patient in need of the drug, while avoiding the occurrence of an adverse side effect known or suspected of being
Thalomid PI teaches a method for delivering thalidomide to a patient in need of the drug, while avoiding the occurrence of an adverse side effect: Ex. 1006 at 2 (“THALOMIDTM (thalidomide) may be prescribed only by licensed prescribers who are registered in the S.T.E.P.S. program and understand the risk of teratogenicity if thalidomide is used during pregnancy.”); Id. at 1 (“Thalidomide is contraindicated in WOMEN of
36
Patent No. 6,315,720
caused by said drug, wherein said method is of the type in which prescriptions for said drug are filled only after a computer readable storage medium has been consulted to assure that the prescriber is registered in said medium and qualified to prescribe said drug, that the pharmacy is registered in said medium and qualified to fill the prescription for said drug, and the patient is registered in said medium and approved to receive said drug, the improvement comprising:
childbearing potential unless alternative therapies are considered inappropriate AND the patient MEETS ALL OF THE FOLLOWING CONDITIONS (i.e., she is essentially unable to become pregnant while on thalidomide therapy).”); Id. at 4 (“Thalidomide is contraindicated in sexually mature MALES unless the PATIENT MEETS ALL OF THE FOLLOWING CONDITIONS: … he is capable of complying with the mandatory contraceptive measures that are appropriate for men, patient registration, and patient survey as described in the S.T.E.P.S. program.”); Id. at 3 (see “Female Patients” chart); Id. at 18 (“THALOMID MUST ONLY BE ADMINISTERED IN COMPLIANCE WITH ALL OF THE TERMS OUTLINED IN THE S.T.E.P.S. PROGRAM. THALOMID MAY ONLY BE PRESCRIBED BY PRESCRIBERS REGISTERED WITH THE S.T.E.P.S. PROGRAM AND MAY ONLY BE DISPENSED BY PHARMACISTS REGISTERED WITH THE S.T.E.P.S. PROGRAM.”); Id. at 19 (“THIS PRODUCT IS ONLY SUPPLIED TO PHARMACISTS REGISTERED WITH THE S.T.E.P.S. PROGRAM. … SPECIFIC INFORMED CONSENT … AND COMPLIANCE WITH THE MANDATORY PATIENT REGISTRY AND SURVEY ARE REQUIRED FOR ALL PATIENTS (MALE AND FEMALE) PRIOR TO DISPENSING BY THE PHARMACIST.”). Ex. 1021, Fudin Decl. ¶¶ 78–82.
a. defining a plurality of patient risk groups based upon a predefined set of risk parameters for said drug;
Thalomid PI defines a plurality of patient risk groups based on a predefined set of risk parameters: Ex. 1006 at 3 (“Thalidomide is contraindicated in WOMEN of childbearing potential unless alternative therapies are considered inappropriate.”); Id. at 4 (“Thalidomide is contraindicated in sexually mature MALES.”).
b. defining a set of information to be obtained from said patient, which
Thalomid PI provides guidelines on the information that is probative of the risk to the adverse side effect of the drug: Ex. 1006 at 20 (“WARNING: SERIOUS HUMAN BIRTH
37

Patent No. 6,315,720
information is probative of the risk that said adverse side effect is likely to occur if said drug is taken by said patient;
DEFECTS IF THALIDOMIDE IS TAKEN DURING PREGNANCY, IT CAN CAUSE SEVERE BIRTH DEFECTS OR DEATH TO AN UNBORN BABY. THALIDOMIDE SHOULD NEVER BE USED BY WOMEN WHO ARE PREGNANT OR WHO COULD BECOME PREGNANT WHILE TAKING THE DRUG. EVEN A SINGLE DOSE [1 CAPSULE (50 mg)] TAKEN BY A PREGNANT WOMAN CAN CAUSE SEVERE BIRTH DEFECTS.”); Id.
; Id. at 21
38
Patent No. 6,315,720
. c. in response to said information set, assigning said patient to at least one of said risk groups and entering said risk group assignment in said medium;
Thalomid PI discloses that the patient is assigned to one of the risk groups and this information is entered into the S.T.E.P.S. database: Ex. 1006 at 3 (“Thalidomide is contraindicated in WOMEN of childbearing potential unless alternative therapies are considered inappropriate AND the patient MEETS ALL OF THE FOLLOWING CONDITIONS (i.e., she is essentially unable to become pregnant while on thalidomide therapy).”); Id. at 4 (“Thalidomide is contraindicated in sexually mature MALES unless the PATIENT MEETS ALL OF THE FOLLOWING CONDITIONS: … he is capable of complying with the mandatory contraceptive measures that are appropriate for men, patient registration, and patient survey as described in the S.T.E.P.S. program.”); Id. at 1 (“UNDER THIS RESTRICTED DISTRIBUTION PROGRAM, ONLY PRESCRIBERS AND PHARMACISTS REGISTERED WITH THE PROGRAM ARE ALLOWED TO PRESCRIBE AND DISPENSE THE PRODUCT. IN ADDITION, PATIENTS MUST BE ADVISED OF, AGREE TO, AND COMPLY WITH THE REQUIREMENTS OF THE S.T.E.P.S. PROGRAM IN ORDER TO RECEIVE PRODUCT.”); Id. at 21
39
Patent No. 6,315,720
.
Ex. 1021, Fudin Decl. ¶¶ 89–96. d. based upon said information and said risk group assignment, determining whether the risk that said adverse side effect is likely to occur is acceptable; and
Thalomid PI discloses that the patient is assigned to one of the risk groups and the adverse side effect is likely to occur is acceptable: Ex. 1006 at 3 (“Thalidomide is contraindicated in WOMEN of childbearing potential unless alternative therapies are considered inappropriate AND the patient MEETS ALL OF THE FOLLOWING CONDITIONS (i.e., she is essentially unable to become pregnant while on thalidomide therapy).”); Id. at 4 (“Thalidomide is contraindicated in sexually mature MALES unless the PATIENT MEETS ALL OF THE FOLLOWING CONDITIONS: … he is capable of complying with the mandatory contraceptive measures that are appropriate for men, patient registration, and patient survey as described in the S.T.E.P.S. program.”); Id. at 21 (see Authorization form copied at Claim 1c.). Ex. 1021, Fudin Decl. ¶¶ 97–99.
e. upon a determination that said risk is acceptable, generating a prescription approval code to be retrieved by said
Thalomid PI teaches that upon information that the risk is acceptable, the patient’s information is entered into the S.T.E.P.S. program to generate a prescription approval code : Ex. 1006 at 20, 21 (“I have read the THALOMIDTM patient brochure and/or viewed the videotape, ‘Important Information for Men and Women Taking THALOMIDTM (thalidomide)’. I understand the contents, including other possible health
40
Patent No. 6,315,720
pharmacy before said prescription is filled.
problems from THALOMIDTM, so-called ‘side effects’. I know that I cannot donate blood while taking THALOMIDTM.”); Id. at 1 (“UNDER THIS RESTRICTED DISTRIBUTION PROGRAM, ONLY PRESCRIBERS AND PHARMACISTS REGISTERED WITH THE PROGRAM ARE ALLOWED TO PRESCRIBE AND DISPENSE THE PRODUCT. IN ADDITION, PATIENTS MUST BE ADVISED OF, AGREE TO, AND COMPLY WITH THE REQUIREMENTS OF THE S.T.E.P.S. PROGRAM IN ORDER TO RECEIVE PRODUCT.”); Id. at 21 (see Authorization form copied at Claim 1c.); Id. at 19 (“Rx only and only able to be prescribed and dispensed under the terms of the S.T.E.P.S. Restricted Distribution Program.”). Ex. 1021, Fudin Decl. ¶¶ 101–06.
2. The method of claim 1 wherein, in response to said risk group assignment, said patient is counseled as to the risks of taking said drug and advised as to risk avoidance measures.
Thalomid PI teaches counseling for patients regarding the risks of taking thalidomide and the risk avoidance measures: Ex. 1006 at 2, 9, 13 (“Pregnancy testing and counseling should be performed if a patient misses her period or if there is any abnormality in menstrual bleeding … [if a]ny suspected fetal exposure to THALOMID (thalidomide) … [t]he patient should be referred to an obstetrician/gynecologist experienced in reproductive toxicity for further evaluation and counseling.”); Id. at 10 (“Patients should be regularly counseled, questioned, and evaluated for signs or symptoms of peripheral neuropathy.”).
3. The method of claim 2 wherein said counseling comprises full disclosure of said risks.
Thalomid PI teaches counseling comprising full disclosure of risks of thalidomide treatment: Ex. 1006 at 21 (see Authorization form copied at Claim 1c.).
4. The method of claim 3 wherein said prescription is filled only following said full disclosure and
Thalomid PI teaches that the prescription is filled only after full disclosure of risks is given and informed consent is obtained: Ex. 1006 at 20 (“SPECIFIC INFORMED CONSENT … AND COMPLIANCE WITH THE MANDATORY PATIENT REGISTRY AND SURVEY ARE REQUIRED FOR ALL PATIENTS (MALE AND FEMALE) PRIOR TO
41
Patent No. 6,315,720
informed consent of said patient.
DISPENSING BY THE PHARMACIST.”); Id. at 21 (see Authorization form copied at Claim 1c.).
5. The method of claim 4 wherein said risk group assignment and said informed consent is verified by said prescriber at the time that said patient is registered in said computer readable storage medium.
Thalomid PI teaches that the prescriber screens patient’s risk group assignment and informed consent at the time the patient is registered in the S.T.E.P.S. program: Ex. 1006 at 1 (“UNDER THIS RESTRICTED DISTRIBUTION PROGRAM, ONLY PRESCRIBERS AND PHARMACISTS REGISTERED WITH THE PROGRAM ARE ALLOWED TO PRESCRIBE AND DISPENSE THE PRODUCT. IN ADDITION, PATIENTS MUST BE ADVISED OF, AGREE TO, AND COMPLY WITH THE REQUIREMENTS OF THE S.T.E.P.S. PROGRAM IN ORDER TO RECEIVE PRODUCT.”); Id. at 21 (see Authorization form copied at Claim 1c.). Ex. 1021, Fudin Decl. ¶¶ 118–20.
6. The method of claim 5 wherein said risk group assignment and said informed consent is transmitted to said computer readable storage medium by facsimile and interpreted by optical character recognition software.
Thalomid PI teaches risk group assignment and informed consent are transmitted to S.T.E.P.S. program: Ex. 1006 at 3, 4 (See supra Claim 1(c)); Id. at 10 (“Patients should be examined at monthly intervals for the first 3 months of thalidomide therapy to enable the clinician to detect early signs of neuropathy. … Patients should be evaluated periodically thereafter during treatment. Patients should be regularly counseled, questioned, and evaluated for signs or symptoms.”). Keravich teaches patient registration by fax: Ex. 1018 at 1722 (“The pharmacy is responsible for registering the patient with Celgene by one of three methods: online adjudication, submission of a manual patient-registration form by fax … or telephone.”). Ex. 1021, Fudin Decl. ¶¶ 121–29.
7. The method of claim 1 wherein said set of information includes the results of diagnostic testing.
Thalomid PI teaches diagnostic testing prior to treatment: Ex. 1006 at 2 (“Before starting treatment, women of childbearing potential should have a pregnancy test. … The test should be performed within the 24 hours prior to beginning therapy.”); Id. at 3 (“[S]he has had a negative pregnancy test with a
42
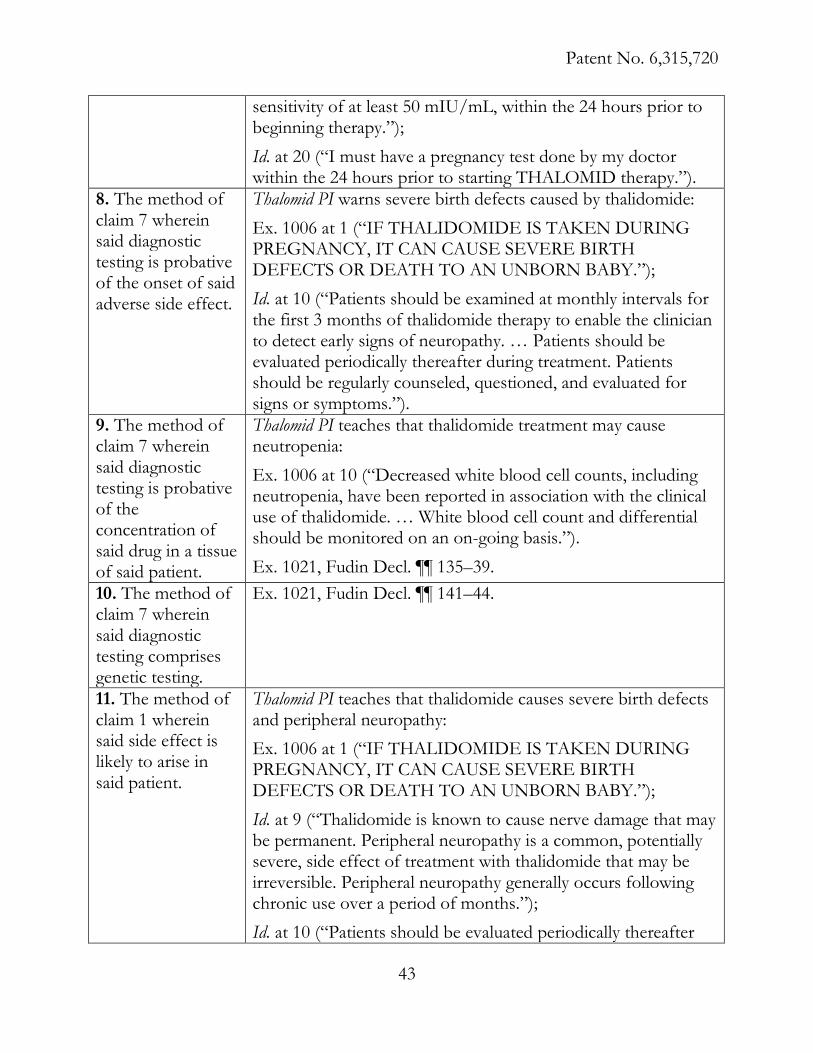
Patent No. 6,315,720
sensitivity of at least 50 mIU/mL, within the 24 hours prior to beginning therapy.”); Id. at 20 (“I must have a pregnancy test done by my doctor within the 24 hours prior to starting THALOMID therapy.”).
8. The method of claim 7 wherein said diagnostic testing is probative of the onset of said adverse side effect.
Thalomid PI warns severe birth defects caused by thalidomide: Ex. 1006 at 1 (“IF THALIDOMIDE IS TAKEN DURING PREGNANCY, IT CAN CAUSE SEVERE BIRTH DEFECTS OR DEATH TO AN UNBORN BABY.”); Id. at 10 (“Patients should be examined at monthly intervals for the first 3 months of thalidomide therapy to enable the clinician to detect early signs of neuropathy. … Patients should be evaluated periodically thereafter during treatment. Patients should be regularly counseled, questioned, and evaluated for signs or symptoms.”).
9. The method of claim 7 wherein said diagnostic testing is probative of the concentration of said drug in a tissue of said patient.
Thalomid PI teaches that thalidomide treatment may cause neutropenia: Ex. 1006 at 10 (“Decreased white blood cell counts, including neutropenia, have been reported in association with the clinical use of thalidomide. … White blood cell count and differential should be monitored on an on-going basis.”). Ex. 1021, Fudin Decl. ¶¶ 135–39.
10. The method of claim 7 wherein said diagnostic testing comprises genetic testing.
Ex. 1021, Fudin Decl. ¶¶ 141–44.
11. The method of claim 1 wherein said side effect is likely to arise in said patient.
Thalomid PI teaches that thalidomide causes severe birth defects and peripheral neuropathy: Ex. 1006 at 1 (“IF THALIDOMIDE IS TAKEN DURING PREGNANCY, IT CAN CAUSE SEVERE BIRTH DEFECTS OR DEATH TO AN UNBORN BABY.”); Id. at 9 (“Thalidomide is known to cause nerve damage that may be permanent. Peripheral neuropathy is a common, potentially severe, side effect of treatment with thalidomide that may be irreversible. Peripheral neuropathy generally occurs following chronic use over a period of months.”); Id. at 10 (“Patients should be evaluated periodically thereafter
43
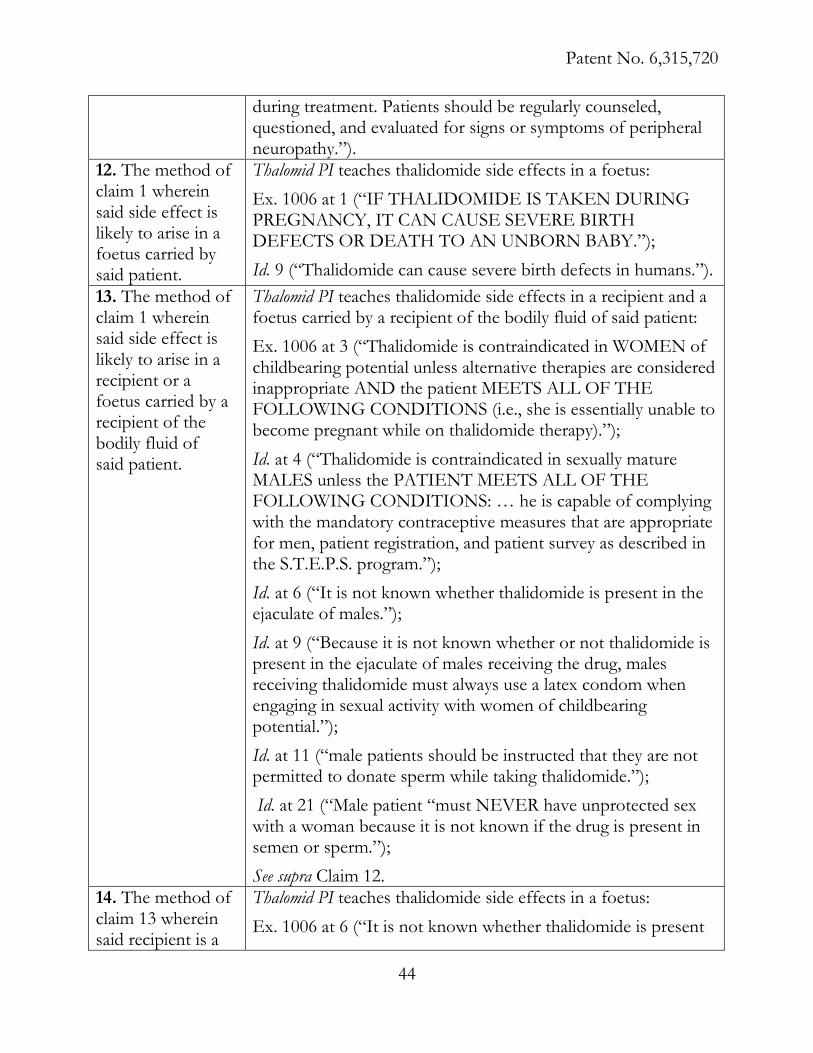
Patent No. 6,315,720
during treatment. Patients should be regularly counseled, questioned, and evaluated for signs or symptoms of peripheral neuropathy.”).
12. The method of claim 1 wherein said side effect is likely to arise in a foetus carried by said patient.
Thalomid PI teaches thalidomide side effects in a foetus: Ex. 1006 at 1 (“IF THALIDOMIDE IS TAKEN DURING PREGNANCY, IT CAN CAUSE SEVERE BIRTH DEFECTS OR DEATH TO AN UNBORN BABY.”); Id. 9 (“Thalidomide can cause severe birth defects in humans.”).
13. The method of claim 1 wherein said side effect is likely to arise in a recipient or a foetus carried by a recipient of the bodily fluid of said patient.
Thalomid PI teaches thalidomide side effects in a recipient and a foetus carried by a recipient of the bodily fluid of said patient: Ex. 1006 at 3 (“Thalidomide is contraindicated in WOMEN of childbearing potential unless alternative therapies are considered inappropriate AND the patient MEETS ALL OF THE FOLLOWING CONDITIONS (i.e., she is essentially unable to become pregnant while on thalidomide therapy).”); Id. at 4 (“Thalidomide is contraindicated in sexually mature MALES unless the PATIENT MEETS ALL OF THE FOLLOWING CONDITIONS: … he is capable of complying with the mandatory contraceptive measures that are appropriate for men, patient registration, and patient survey as described in the S.T.E.P.S. program.”); Id. at 6 (“It is not known whether thalidomide is present in the ejaculate of males.”); Id. at 9 (“Because it is not known whether or not thalidomide is present in the ejaculate of males receiving the drug, males receiving thalidomide must always use a latex condom when engaging in sexual activity with women of childbearing potential.”); Id. at 11 (“male patients should be instructed that they are not permitted to donate sperm while taking thalidomide.”); Id. at 21 (“Male patient “must NEVER have unprotected sex with a woman because it is not known if the drug is present in semen or sperm.”); See supra Claim 12.
14. The method of claim 13 wherein said recipient is a
Thalomid PI teaches thalidomide side effects in a foetus: Ex. 1006 at 6 (“It is not known whether thalidomide is present
44
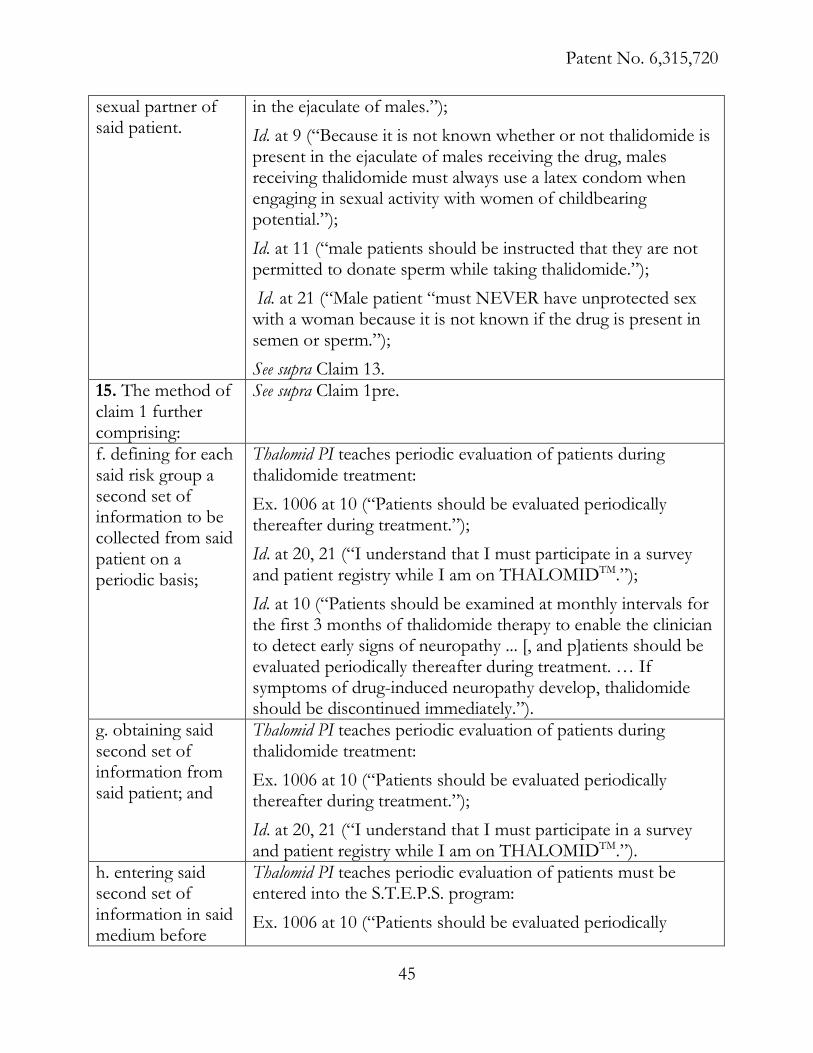
Patent No. 6,315,720
sexual partner of said patient.
in the ejaculate of males.”); Id. at 9 (“Because it is not known whether or not thalidomide is present in the ejaculate of males receiving the drug, males receiving thalidomide must always use a latex condom when engaging in sexual activity with women of childbearing potential.”); Id. at 11 (“male patients should be instructed that they are not permitted to donate sperm while taking thalidomide.”); Id. at 21 (“Male patient “must NEVER have unprotected sex with a woman because it is not known if the drug is present in semen or sperm.”); See supra Claim 13.
15. The method of claim 1 further comprising:
See supra Claim 1pre.
f. defining for each said risk group a second set of information to be collected from said patient on a periodic basis;
Thalomid PI teaches periodic evaluation of patients during thalidomide treatment: Ex. 1006 at 10 (“Patients should be evaluated periodically thereafter during treatment.”); Id. at 20, 21 (“I understand that I must participate in a survey and patient registry while I am on THALOMIDTM.”); Id. at 10 (“Patients should be examined at monthly intervals for the first 3 months of thalidomide therapy to enable the clinician to detect early signs of neuropathy ... [, and p]atients should be evaluated periodically thereafter during treatment. … If symptoms of drug-induced neuropathy develop, thalidomide should be discontinued immediately.”).
g. obtaining said second set of information from said patient; and
Thalomid PI teaches periodic evaluation of patients during thalidomide treatment: Ex. 1006 at 10 (“Patients should be evaluated periodically thereafter during treatment.”); Id. at 20, 21 (“I understand that I must participate in a survey and patient registry while I am on THALOMIDTM.”).
h. entering said second set of information in said medium before
Thalomid PI teaches periodic evaluation of patients must be entered into the S.T.E.P.S. program: Ex. 1006 at 10 (“Patients should be evaluated periodically
45
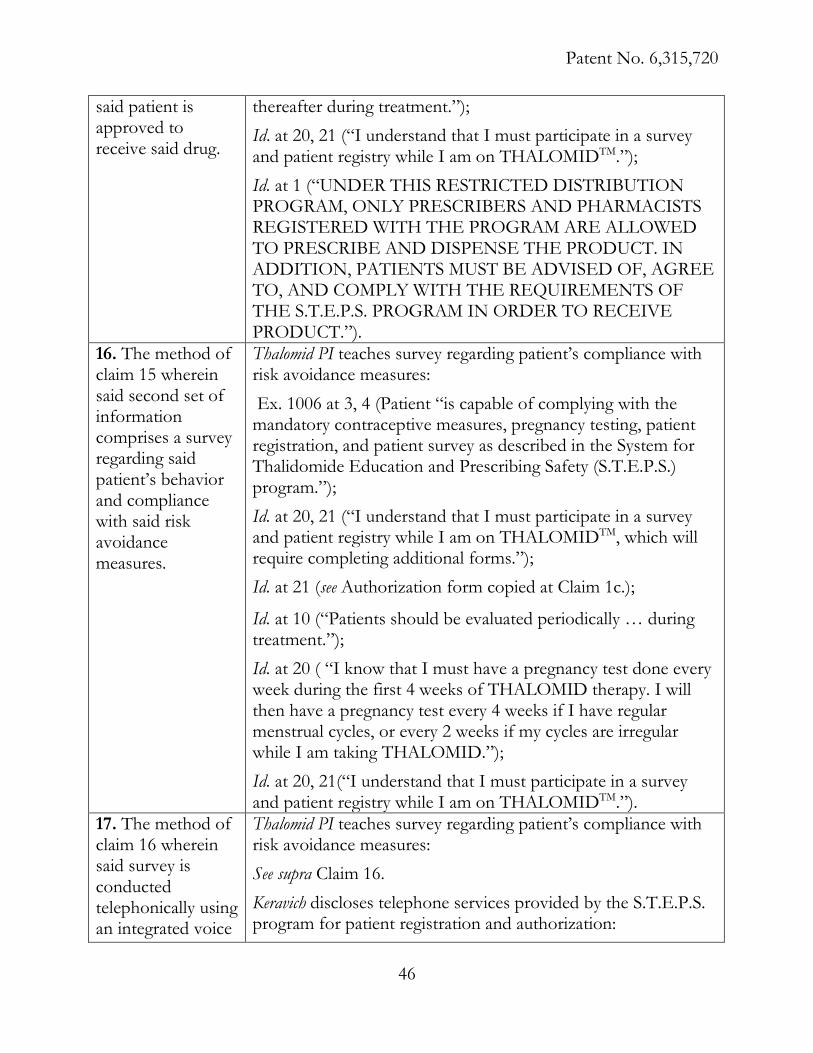
Patent No. 6,315,720
said patient is approved to receive said drug.
thereafter during treatment.”); Id. at 20, 21 (“I understand that I must participate in a survey and patient registry while I am on THALOMIDTM.”); Id. at 1 (“UNDER THIS RESTRICTED DISTRIBUTION PROGRAM, ONLY PRESCRIBERS AND PHARMACISTS REGISTERED WITH THE PROGRAM ARE ALLOWED TO PRESCRIBE AND DISPENSE THE PRODUCT. IN ADDITION, PATIENTS MUST BE ADVISED OF, AGREE TO, AND COMPLY WITH THE REQUIREMENTS OF THE S.T.E.P.S. PROGRAM IN ORDER TO RECEIVE PRODUCT.”).
16. The method of claim 15 wherein said second set of information comprises a survey regarding said patient’s behavior and compliance with said risk avoidance measures.
Thalomid PI teaches survey regarding patient’s compliance with risk avoidance measures: Ex. 1006 at 3, 4 (Patient “is capable of complying with the mandatory contraceptive measures, pregnancy testing, patient registration, and patient survey as described in the System for Thalidomide Education and Prescribing Safety (S.T.E.P.S.) program.”); Id. at 20, 21 (“I understand that I must participate in a survey and patient registry while I am on THALOMIDTM, which will require completing additional forms.”); Id. at 21 (see Authorization form copied at Claim 1c.);
Id. at 10 (“Patients should be evaluated periodically … during treatment.”); Id. at 20 ( “I know that I must have a pregnancy test done every week during the first 4 weeks of THALOMID therapy. I will then have a pregnancy test every 4 weeks if I have regular menstrual cycles, or every 2 weeks if my cycles are irregular while I am taking THALOMID.”); Id. at 20, 21(“I understand that I must participate in a survey and patient registry while I am on THALOMIDTM.”).
17. The method of claim 16 wherein said survey is conducted telephonically using an integrated voice
Thalomid PI teaches survey regarding patient’s compliance with risk avoidance measures: See supra Claim 16. Keravich discloses telephone services provided by the S.T.E.P.S. program for patient registration and authorization:
46

Patent No. 6,315,720
response system. Ex. 1018 at 1723 (“A pharmacist who registers a patient by telephone can provide the information required for prescription authorization at the same time.”); Id. at 1724 (“The binders also contain blank patient registration forms and prescription verification forms for use when registration and verification by telephone are not possible.”) Ex. 1021, Fudin Decl. ¶¶ 177–79.
18. The method of claim 16 wherein said patient is a female of childbearing potential and said second set of information comprises the results of a pregnancy test.
Thalomid PI teaches periodic pregnancy tests for a woman of childbearing potential on Thalomid: Ex. 1006 at 2 (“Once treatment has started, pregnancy testing should occur weekly during the first month of use, then monthly thereafter in women with regular menstrual cycles.”); Id. at 18 (“Drug prescribing to women of childbearing potential should be contingent upon initial and continued confirmed negative results of pregnancy testing.”); Id. at 20 (“I know that I must have a pregnancy test done every week during the first 4 weeks of THALOMID therapy. I will then have a pregnancy test every 4 weeks if I have regular menstrual cycles, or every 2 weeks if my cycles are irregular while I am taking THALOMID.”).
19. The method of claim 18 wherein said periodic interval comprises about 28 days.
Thalomid PI teaches periodic (about 28 days) pregnancy tests for a woman of childbearing potential on Thalomid: Ex. 1006 at 20 (“I know that I must have a pregnancy test done every week during the first 4 weeks of THALOMID therapy. I will then have a pregnancy test every 4 weeks if I have regular menstrual cycles, or every 2 weeks if my cycles are irregular while I am taking THALOMID.”).
20. The method of claim 1 further comprising providing said patient with a contraceptive device or formulation.
Thalomid PI discloses types of contraception that can be used by women on Thalomid: Ex. 1006 at 2 (“Effective contraception … must be used for at least 1 month before beginning thalidomide therapy, during thalidomide therapy, and for 1 month following discontinuation of thalidomide therapy. … Women of childbearing potential should be referred to a qualified provider of contraceptive methods, if needed.”) Ex. 1021, Fudin Decl. ¶¶ 156–60.
21. The method of Thalomid PI discloses teratogenic effect of Thalomid:
47
Patent No. 6,315,720
claim 1 wherein said adverse side effect comprises a teratogenic effect.
Ex. 1006 at 1 (“IF THALIDOMIDE IS TAKEN DURING PREGNANCY, IT CAN CAUSE SEVERE BIRTH DEFECTS OR DEATH TO AN UNBORN BABY.”); Id. at 2 (“THALOMIDTM (thalidomide) may be prescribed only by licensed prescribers who are registered in the S.T.E.P.S. program and understand the risk of teratogenicity if thalidomide is used during pregnancy.”); Id. at 8 (“Due to its known human teratogenicity, even following a single dose, thalidomide is contraindicated in pregnant women and women capable of becoming pregnant.”); Id. at 9 (“Patient should be instructed about the potential teratogenicity of thalidomide.”).
22. The method of claim 1 wherein said drug is thalidomide.
Thalomid PI discloses the drug THALOMIDTM (thalidomide): Ex. 1006 at 1 (“IF THALIDOMIDE IS TAKEN DURING PREGNANCY, IT CAN CAUSE SEVERE BIRTH DEFECTS OR DEATH TO AN UNBORN BABY.”); Id. at 2 (“THALOMIDTM (thalidomide) may be prescribed only by licensed prescribers who are registered in the S.T.E.P.S. program and understand the risk of teratogenicity if thalidomide is used during pregnancy.”).
23. The method of claim 21 wherein said teratogenic effect is likely to arise in a foetus carried by said patient.
Thalomid PI discloses that teratogenic effect of Thalomid is likely to arise in a foetus: Ex. 1006 at 1 (“IF THALIDOMIDE IS TAKEN DURING PREGNANCY, IT CAN CAUSE SEVERE BIRTH DEFECTS OR DEATH TO AN UNBORN BABY.”); Id. at 2 (“THALOMIDTM (thalidomide) may be prescribed only by licensed prescribers who are registered in the S.T.E.P.S. program and understand the risk of teratogenicity if thalidomide is used during pregnancy.”); Id. at 8 (“Due to its known human teratogenicity, even following a single dose, thalidomide is contraindicated in pregnant women and women capable of becoming pregnant.”); Id. at 9 (“Patient should be instructed about the potential teratogenicity of thalidomide.”).
24. The method of claim 21 wherein said teratogenic
Thalomid PI discloses that teratogenic effect of Thalomid is likely to arise in a foetus:
48
Patent No. 6,315,720
effect is likely to arise in a foetus carried by a recipient of the bodily fluid of said patient.
See supra Claims 12, 13, 14.
25. The method of claim 24 wherein said recipient of the bodily fluid of said patient is a sexual partner of said patient.
Thalomid PI explicitly discloses that thalidomide side effects likely arise in a sexual partner of a male treated with the drug: Ex. 1006 at 6 (“It is not known whether thalidomide is present in the ejaculate of males.”); Id. at 9 (“Because it is not known whether or not thalidomide is present in the ejaculate of males receiving the drug, males receiving thalidomide must always use a latex condom when engaging in sexual activity with women of childbearing potential.”); Id. at 11 (“male patients should be instructed that they are not permitted to donate sperm while taking thalidomide.”); Id. at 21 (“Male patient “must NEVER have unprotected sex with a woman because it is not known if the drug is present in semen or sperm.”).
26. The method of claim 21 wherein said set of information includes the results of a pregnancy test.
Thalomid PI teaches that information includes results of pregnancy tests: Ex. 1006 at 2 (“Before starting treatment, women of childbearing potential should have a pregnancy test … within the 24 hours prior to beginning therapy.”); Id. at 18 (“Drug prescribing to women of childbearing potential should be contingent upon initial and continued confirmed negative results of pregnancy testing.”); Id. at 20 (“I know that I must have a pregnancy test done every week during the first 4 weeks of THALOMID therapy. I will then have a pregnancy test every 4 weeks if I have regular menstrual cycles, or every 2 weeks if my cycles are irregular while I am taking THALOMID.”).
27. The method of claim 26 wherein said prescription is filled for no more than about 28 days.
Thalomid PI teaches that the prescription is filled for no more than about 28 days: Ex. 1006 at 19 (“DRUG MUST ONLY BE DISPENSED IN NO MORE THAN A 1-MONTH SUPPLY.”).
49
Patent No. 6,315,720
Keravich teaches that the prescription is filled for no more than about 28 days: Ex. 1018 at 1722 (“Prescribe no more than 28 days of therapy and not authorize refills.”). Ex. 1021, Fudin Decl. ¶¶ 188–90.
28pre and (a)–(e). See supra Claim 1pre and (a)–(e).
28. wherein said adverse side effect is likely to arise in patients who take said drug in combination with at least one other drug.
Thalomid PI teaches thalidomide drug interactions: Ex. 1006 at 12 (“Drug Interactions. Thalidomide has been reported to enhance the sedative activity of barbiturates, alcohol, chlorpromazine, and reserpine.…”); Id. (“Medications known to be associated with peripheral neuropathy should be used with caution in patients receiving thalidomide.”). Ex. 1021, Fudin Decl. ¶¶ 191–96.
29. The method of claim 28, wherein said set of information is also probative of the likelihood that said patient may take said drug and said other drug in combination.
Thalomid PI teaches thalidomide drug interactions: Ex. 1006 at 12 (“Drug Interactions. Thalidomide has been reported to enhance the sedative activity of barbiturates, alcohol, chlorpromazine, and reserpine.…”); Id. (“Medications known to be associated with peripheral neuropathy should be used with caution in patients receiving thalidomide.”). Ex. 1021, Fudin Decl. ¶¶ 205–09.
30. The method of claim 28 wherein said set of information includes the results of diagnostic testing.
Thalomid PI teaches that the patient information includes diagnostic test results: Ex. 1006 at 3 (“[S]he has had a negative pregnancy test with a sensitivity of at least 50 mIU/mL, within the 24 hours prior to beginning therapy.”); Id. at 20 (“I know that I must have a pregnancy test done by my doctor within the 24 hours prior to starting THALOMID therapy, then every week during the first 4 weeks of THALOMID therapy. I will then have a pregnancy test every 4 weeks if I have regular menstrual cycles, or every 2 weeks if my cycles are irregular while I am taking THALOMID.”); Id. at 10 (“Patients should be evaluated periodically thereafter during treatment. Patients should be regularly counseled,
50
Patent No. 6,315,720
questioned, and evaluated for signs or symptoms of peripheral neuropathy. Consideration should be given to electrophysiological testing.”). See also Ex. 1021, Fudin Decl. ¶¶ 197–204.
31. The method claim 30 wherein said diagnostic testing comprises testing for evidence of the use of said other drug.
Thalomid PI discloses testing women on other medications: Ex. 1006 at 12 (“In 10 healthy women, the pharmacokinetic profiles of norethindrone and ethinyl estradiol following administration of a single dose containing 1.0 mg of norethindrone acetate and 75 μg of ethinyl estradiol were studied. The results were similar with and without coadministration of thalidomide 200 mg/day to steady-state levels.”). See also Ex. 1021, Fudin Decl. ¶¶ 210–12.
32. The method of claim 30 wherein said diagnostic testing comprises for evidence which is indicative of the onset of said adverse side effect.
Thalomid PI teaches adverse side effects and laboratory tests to determine the evidence of adverse side effects in patients on thalidomide therapy: Ex. 1006 at 9–11 (“Birth defects … Drowsiness and somnolence … Peripheral neuropathy … Dizziness and orthostatic hypotension … Neutropenia … Increased HIV-viral load … Hypersensitivity … [and] Bradycardia.…”); Id. at 11–12 (“Pregnancy Testing … Neutropenia … [and] HIV viral load.”). Ex. 1021, Fudin Decl. ¶¶ 197–204.
B. Ground 2: Claims 1–323 of U.S. Patent No. 6,315,720 are obvious under 35 U.S.C. § 103(a) over Thalomid PI in view of Cunningham, and in further view of the knowledge of one of ordinary skill in the art.
The Cunningham patent constitutes prior art under 35 U.S.C. § 102(b) because it
was filed in 1995 and granted in 1998. (Ex. 1009 at Cover.) During the prosecution of
the ’720 Patent, the examiner did not consider this reference. (See Ex. 1001 at Cover.)
3 For all claim elements not specifically discussed under Ground 2, those claim
element disclosures are the same as discussed under Ground 1.
51
Patent No. 6,315,720
The examiner did consider, but did not cite, a divisional of this reference. (See id. at
Cover; Ex. 1010 at Cover.)
Cunningham discloses a method of dispensing pharmaceutical product samples
by linking prescribers and pharmacies to a central computing station. (Ex. 1009 at
Cover.) Specifically, before filling any prescription for a pharmaceutical trial product,
the pharmacy must upload defined information into the central computing station.
(See id. at 11:6–13.) Only if the central computing station establishes that the uploaded
information is valid can the central computing station issue a pharmacy approval code
for the pharmacy to then dispense the pharmaceutical product. (See id. at 11:13–23.)
Claims 1(e) and 28(e) are obvious over Thalomid PI in view of 1.Cunningham.
Claims 1(e) and 28(e)4 of the ’720 Patent require that, “upon a determination
that said risk is acceptable, generating a prescription approval code to be retrieved by
said pharmacy before said prescription is filled.” (Ex. 1001 at 18:40–42.) This
mechanism would have been obvious to a person of ordinary skill in the art, upon
reading Thalomid PI, which discloses that a prescription may not be filled until the
risks are deemed acceptable and the prescription has been approved:
THALOMIDTM (thalidomide) may be prescribed only by licensed
prescribers who … understand the risk of teratogenicity if thalidomide is
used during pregnancy. … A prescription for thalidomide for a woman
4 The other elements of Claims 1 and 28 are as described for Ground 1.
52
Patent No. 6,315,720
of childbearing potential must not be issued by the prescriber until a
written report of a negative pregnancy test has been obtained by the
prescriber.
(Ex. 1006 at 2; Ex. 1021 ¶¶ 213–14.)
As the ’720 Patent correctly states, “[s]uitable computer readable storage media
… will be apparent to one of ordinary skill in the art, once armed with the teachings
of the present application.” (Ex. 1001 at 5:11–16.) Indeed, it would have been
apparent and obvious to one of ordinary skill in the art to utilize the Claim 1(e) and
28(e) approval codes to implement the drug restriction required by Thalomid PI, in
light of Cunningham’s disclosure of an approval code lockout system for a pharmacy:
If authenticity is not established, it follows that the participating
pharmacy cannot dispense corresponding pharmaceutical product. …
However, if authenticity is established then the pharmac[y’s] terminal
dials the central computing station and data and information from the
pharmac[y’s] authorization media and personal identification is uploaded
to the database of the central computing station 12. … Assuming full
validation, the central computing station issues a pharmacy
approval code and the pharmacy records that approval code on the
actual presented product trial media 18. … Once validation is established
the pharmacy then dispenses pharmaceutical trial product …
(Ex. 1009 at 11:6–8, 17–23 (emphasis added); Ex. 1021 ¶ 214.) See KSR Int'l Co. v.
Teleflex Inc., 550 U.S. 398, 416–17 (2007) (where a combination of references “[s]imply
arranges old elements with each performing the same function it had been known to
53
Patent No. 6,315,720
perform and yields no more than one would expect from such an arrangement, the
combination is obvious.”) (internal quotations and citations omitted).
“In view of the guidelines for the avoidance of treating pregnant patients with
thalidomide taught by Thalomid PI, it would have been obvious to a” person of
ordinary skill in the art “to implement the methods disclosed in Cunningham to limit
dispensation of a drug associated with adverse effects to certain risk groups.” (Ex.
1021 ¶ 215.) See Abbott Labs v. Andrx Pharms., Inc., 452 F.3d 1331, 1345 (Fed. Cir.
2006) (finding substantial question of invalidity because the combination of references
for “the reduction of systemic side effects would not be surprising and would not be
unexpected.”). Therefore, an ordinarily skilled artisan “treating a patient with a
teratogenic or other risk-laden drug in accordance with Thalomid PI’s guidelines would
look to the approval code system taught by Cunningham—and would view Claims 1
and 28 of the ’720 Patent obvious in view of these references.” (Ex. 1021 ¶ 216.) See
Dystar Textilfarben GmbH v. C.H. Patrick Co., 464 F.3d 1356, 1361 (Fed. Cir. 2006)
(“The motivation need not be found in the references sought to be combined, but
may be found in any number of sources, including common knowledge, the prior art
as a whole, or the nature of the problem itself.”).
Claims 5 and 6 are obvious over Thalomid PI in view of the 2.knowledge of one of ordinary skill in the art.
Claim 5 requires that “said risk group assignment and informed consent is
verified by said prescriber at the time that said patient is registered in said computer
54
Patent No. 6,315,720
readable storage medium,” and Claim 6 requires that “said risk group assignment and
said informed consent is transmitted to [the Claim 5] computer readable storage
medium by facsimile and interpreted by optical character recognition software.”
(Ex. 1001 at 18:51–58.)
The Claim 5 consent and risk group verification at the time of patient
registration was obvious to one of ordinary skill in the art in light of Thalomid PI’s
requirement that the prescriber “ensure that the appropriate components of the
patient consent form are completed.” (Ex. 1006 at 21; Ex. 1021 ¶ 217.) Specifically,
“Thalomid PI sets forth different consent forms for male and female patients, thus
requiring that the prescriber verify the patient’s gender risk group by selecting the
consent form for completion.” (Id. at 20–21; Ex. 1021 ¶ 218.) Further, it was within
the knowledge of one of ordinary skill in the art “that, as part of the S.T.E.P.S.
Program, information from the consent form had to be entered into the patient
registration database.” (Ex. 1021 ¶ 219; see, e.g., Ex. 1018 at 1723 (“The patient
database provides critical patient-related information that is found on the consent
form”); Ex. 1012 at 325; Ex. 1015 at 8.) “Because Thalomid PI requires that the
prescriber is the one to ‘ensure that the appropriate components of the patient
consent form are completed,’ it would have been obvious to” one of ordinary skill in
the art “that, while verifying the patient consent and associated risk group assignment,
the prescriber could eliminate error and delay by also registering the patient into the
database at that time.” (Ex. 1006 at 21; Ex. 1021 ¶ 220.) See Bayer Schering Pharma AG
55
Patent No. 6,315,720
v. Barr Labs., Inc., 575 F.3d 1341, 1347 (Fed. Cir. 2009) (“When there is a design need
or market pressure to solve a problem and there are a finite number of identified,
predictable solutions, a person of ordinary skill has good reason to pursue the known
options within his or her technical grasp. If this leads to the anticipated success, it is
likely the product not of innovation but of ordinary skill and common sense.”)
(quotation omitted).
The previous disclosure also teaches an ordinarily skilled artisan that the
informed consent and risk group assignment are transmitted to the patient database
described in Ground 1’s Claim 1(c), and as required by the first portion of Claim 6.
(Ex. 1021 ¶ 221.) One of ordinary skill in the art “would understand that a prescriber
would typically print Thalomid PI’s consent forms.” (Ex. 1006 at 20–21; Ex. 1021
¶ 222; see Ex. 1018 at 1722 (“A packet of materials is mailed to each interested or
registered prescriber for use with each patient undergoing thalidomide treatment. The
packet contains an FDA-approved informed-consent form, an initial confidential
patient survey”).) Because it was within the knowledge of one of ordinary skill in the
art “to transfer paper data into a computer database by fax, which is then ‘interpreted
by optical character recognition [OCR] software,’ it would have been obvious to” an
ordinarily skilled artisan “that paper risk group assignments and informed consents
could similarly be transferred to the patient database through fax and OCR,” as the
last portion of Claim 6 requires. (Ex. 1021 ¶ 223.) See Perfect Web Techs., Inc. v.
InfoUSA, Inc., 587 F.3d 1324, 1329 (Fed. Cir. 2009) (“KSR expanded the sources of
56
Patent No. 6,315,720
information for a properly flexible obviousness inquiry to include … the background
knowledge, creativity, and common sense of the person of ordinary skill.”).
Claims 9 and 10 are obvious over Thalomid PI in view of the 3.knowledge of one of ordinary skill in the art.
Claims 9 and 10 include the Claim 7 requirement that the “information to be
obtained from said patient” prior to treatment “includes the results of diagnostic
testing,” with the further respective limitations that this diagnostic testing “is
probative of the concentration of said drug in a tissue of said patient,” and “comprises
genetic testing.” (Ex. 1001 at 18:59–60, 66–67.)
As explained in Ground 1, Thalomid PI anticipates the Claim 7 diagnostic
testing. (Ex. 1006 at 2 (“Before starting treatment, women of childbearing potential
should have a pregnancy test”).) With respect to Claim 9, it would have been obvious
to an ordinarily skilled artisan “to include, within the extensive diagnostic testing
taught by Thalomid PI, testing for the drug concentration in patient tissue.” (Ex. 1021
¶ 226.) Specifically, “[f]or a patient previously treated with the drug, it would have
been obvious to” one of ordinary skill in the art “to conduct diagnostic testing
probative of the concentration of the drug remaining in the patient’s body.” (Ex. 1021
¶ 227.) However, “[b]ecause many drugs do not generally distribute uniformly in the
body, but instead are preferentially absorbed by certain body tissues,” one of ordinary
skill in the art “would have further recognized the importance of performing
diagnostic testing that would be probative of the concentration of such a non-
57
Patent No. 6,315,720
uniformly distributing drug in the drug’s target tissues.” (Ex. 1021 ¶ 228.) See Tyco
Healthcare Grp. LP v. Ethicon Endo-Surgery, Inc., 774 F.3d 968, 977 (Fed. Cir. 2014)
(“Claims would have been obvious if they are nothing more than a combination of
familiar elements that yield predictable results.”).
With respect to Claim 10, it would have been further obvious to an ordinarily
skilled artisan “to include genetic testing in the extensive diagnostic testing taught by
Thalomid PI.” (Ex. 1021 ¶ 229.) Specifically, “[i]t was common in the art at the time of
the ’720 Patent to conduct genetic testing at the same time as the pregnancy testing
taught in Thalomid PI.” (Ex. 1021 ¶ 230.) More generally, “because genetic testing was
a well-known diagnostic procedure at the time of the ’720 Patent, it would have been
obvious” to one of ordinary skill in the art “to include genetic testing in the diagnostic
testing that preceded such last-resort treatments as that disclosed in Thalomid PI.” (Ex.
1021 ¶ 231.) See Unigene Labs., Inc. v. Apotex, Inc., 655 F.3d 1352, 1361 (Fed. Cir. 2011)
(“This court has observed that teachings from prior art, suggestions beyond the literal
teachings of those art references, or even motivations from the store of common
knowledge of one of ordinary skill in the art field (‘TSM’)—flexibly viewed and
applied—provide the sources of evidence that an ordinary skilled artisan might have
found and combined at the time of the invention.”).
58
Patent No. 6,315,720
Claim 17 is obvious over Thalomid PI in view of the knowledge of 4.one of ordinary skill in the art.
Claim 17 requires that the Claim 16 survey “is conducted telephonically using
an integrated voice response system.” (Ex. 1001 at 19:22–24.) As explained in Ground
1, Thalomid PI anticipates the Claim 16 patient survey requirement. Further, “[b]ecause
one method of conducting surveys well known” to those of ordinary skill in the art
“at the time of the ’720 Patent was via the telephone, using an integrated voice
response system—which was well known” to those of ordinary skill in the art at the
time—as required by Claim 17, “would have been obvious” to one of ordinary skill in
the art. (Ex. 1021 ¶ 233; see, e.g., Ex. 1024 at 611–12, 623.) See In re Venner, 262 F.2d
91, 95 (C.C.P.A. 1958) (“Furthermore, it is well settled that it is not ‘invention’ to
broadly provide a mechanical or automatic means to replace manual activity which has
accomplished the same result.”).
Claim Chart for Ground 2 showing exemplary citations in 5.Cunningham.
All Thalomid PI disclosures are listed in the Ground 1 claim chart above.
Element Prior Art 1e./28e. upon a determination that said risk is acceptable, generating a prescription approval code to be retrieved by said pharmacy before said prescription is
Cunningham discloses an approval code lockout system for a pharmacy: Ex. 1009 at 11:6–8, 17–23 (“If authenticity is not established, it follows that the participating pharmacy cannot dispense corresponding pharmaceutical product. … However, if authenticity is established then the pharmac[y’s] terminal dials the central computing station and data and information from the pharmac[y’s] authorization media and personal identification is uploaded to the database of the central computing station 12. … Assuming full validation, the central computing station
59
Patent No. 6,315,720
filled. issues a pharmacy approval code and the pharmacy records that approval code on the actual presented product trial media 18. … Once validation is established the pharmacy then dispenses pharmaceutical trial product….”). Ex. 1021, Fudin Decl. ¶¶ 214–16.
VII. CONCLUSION
Thus, Petitioners respectfully request inter partes review of Claims 1–32 of U.S.
Patent No. 6,315,720.
Respectfully Submitted, /Sarah E. Spires/ Sarah E. Spires (Reg. No. 61,501) SKIERMONT PUCKETT LLP 2200 Ross Ave. Ste. 4800W Dallas, Texas 75201 P: 214-978-6600/F: 214-978-6601 Lead Counsel for Petitioner
April 23, 2015 Ki O (Reg. No. 68,952) Dr. Parvathi Kota (Reg. No. 65,122) Paul J. Skiermont (pro hac vice requested) SKIERMONT PUCKETT LLP 2200 Ross Ave. Ste. 4800W Dallas, Texas 75201 P: 214-978-6600/F: 214-978-6621 Back-Up Counsel for Petitioner
60
Patent No. 6,315,720
CERTIFICATE OF SERVICE
I hereby certify that on April 23, 2015, a copy of this Petition for Inter Partes
Review of U.S. Patent No. 6,315,720, including all exhibits, was served via FedEx,
overnight delivery, upon the following:
Celgene Corporation 86 Morris Avenue Summit, New Jersey 07901 S. Maurice Valla BakerHostetler Cira Centre, 12th Floor 2929 Arch Street Philadelphia, Pennsylvania 19104-2891
Date: April 23, 2015 /Sarah E. Spires/





























