Embed Size (px)
Citation preview

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Note: This article will be published in a forthcoming issue of
the Journal of Aging and Physical Activity. This article
appears here in its accepted, peer-reviewed form; it has not
been copy edited, proofed, or formatted by the publisher.
Section: Original Research
Article Title: Physical Activity in the Acute Ward Following Hip Fracture Surgery is
Associated With Less Fear of Falling
Authors: Lise Kronborg1, Thomas Bandholm1, 2, 3, Henrik Palm3, Henrik Kehlet4, and
Morten Tange Kristensen1, 3
Affiliations: 1Physical Medicine and Rehabilitation Research – Copenhagen (PMR-C),
Department of Physical Therapy, Copenhagen University Hospital, Hvidovre, Denmark. 2Clinical Research Centre, Copenhagen University Hospital, Hvidovre, Denmark. 3Department of Orthopedic Surgery, Copenhagen University Hospital, Hvidovre, Denmark. 4Section for Surgical Pathophysiology, Rigshospitalet, Copenhagen University, Denmark.
Running Head: Physical activity in the acute ward after hip fracture surgery
Journal: Journal of Aging and Physical Activity
Acceptance Date: January 13, 2016
©2016 Human Kinetics, Inc.
DOI: http://dx.doi.org/10.1123/japa.2015-0071

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Title: Physical activity in the acute ward following hip fracture surgery is associated with
less fear of falling
Section: Original Research
Authors: Lise Kronborg, Msc1, Thomas Bandholm, PhD1, 2, 3, Henrik Palm, MD3, Henrik
Kehlet, PhD4, Morten Tange Kristensen, PhD1, 3
Affiliations:
1) Physical Medicine and Rehabilitation Research – Copenhagen (PMR-C), Department of
Physical Therapy, Copenhagen University Hospital, Hvidovre, Denmark
2) Clinical Research Centre, Copenhagen University Hospital, Hvidovre, Denmark
3) Department of Orthopedic Surgery, Copenhagen University Hospital, Hvidovre, Denmark
4) Section for Surgical Pathophysiology, Rigshospitalet, Copenhagen University, Denmark.
Running head: Physical activity in the acute ward after hip fracture surgery
Corresponding author: Lise Kronborg, Department of Physical Therapy 236, Hvidovre
Hospital, Kettegaard Alle 30, DK-2650 Hvidovre, Denmark. Phone: work: +45 3862 6634.
Mobile: +45 4051 1710. E-mail: [email protected]
Reprints can be obtained from the corresponding author.
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Abstract
Early mobilization following hip fracture surgery reduces medical complications and
mortality, but may increase the risk of falling. The aim was to measure objectively the
physical activity (time spent upright) the first week after hip fracture surgery, and relate it to
functional performance and fear of falling at discharge. The 24-hour upright time was
measured for a median of 6 days using a thigh-worn accelerometer in 37 patients (mean 80
years 8.4) and increased from median 13 (IQR 6-31) minutes to 46 (11-107) minutes at day
7. More upright time at discharge was associated with less fear of falling (r=-0.48, p=0.01,
n=27), which also was associated with fast gait speed (r=-0.50, p=0.02, n=23) and a faster
Timed Up and Go test time (r=0.54, p < 0.01, n=22), indicating a need for further studies on
motivation and limitations for more physical activity following hip fracture surgery.
Keywords: physical activity, accelerometers, hip fracture, basic mobility, fear of falling
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Introduction
Immobilization following hip fracture surgery is associated with slow recovery, long-
term loss of function, change of residence, medical complications and long-term mortality
(Kristensen, 2011; Gill, Murphy, Gahbauer, & Allore, 2013; Rosell & Parker, 2003; Ariza-
Vega, Kristensen, Martin-Martin, & Jimenez-Moleon, 2015; Resnick et al., 2011). Early
ambulation involving weight bearing and walking has been found efficient to improve short-
term outcomes after hip fracture surgery and is therefore recommended (Foss, Kristensen, &
Kehlet, 2006; Sherrington, Lord, & Herbert, 2003; Oldmeadow et al., 2006; Siu et al., 2006).
The beneficial effects of physical activity (PA) are undisputable, especially in frail older
adults where days of bed rest can have a huge impact on functional capacity (Kortebein et al.,
2008; Zisberg et al., 2011). Still, for hip-fracture patients in the acute ward, potentially
affected by pain (Foss, Kristensen, Palm, & Kehlet, 2009), pain medication (Foss, Kristensen,
Kristensen, Jensen, & Kehlet, 2005) and postoperative delirium after surgery (Robertson &
Robertson, 2006), PA such as standing or walking is also associated with a potentially greater
risk of falling and compromising the newly acquired orthopedic treatment. This presents a
dilemma of patient safety to the ward staff and may affect staff behavior and perspective on
promotion of PA to the patients (Grant, Granat, Thow, & Maclaren, 2010; Doherty-King,
Yoon, Pecanac, Brown, & Mahoney, 2014; Brown, Williams, Woodby, Davis, & Allman,
2007). Overcoming perceived barriers to mobility for the older patient such as fear of falling,
pain and perspectives towards exercise and PA as a way to recover as opposed to bed rest
may require behavior change and be associated with the motivation for PA immediately after
surgery (Franco et al., 2015; Visschedijk, van, Hertogh, & Achterberg, 2013; Schiller et al.,
2015; Schwarzer, Lippke, & Luszczynska, 2011; Bandura, 1977). Fear of falling has been
recognized as a common problem among elderly, especially those with a history of falls, as it
can activate a negative trajectory of avoiding activities that lead to a subsequent negative
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
impact on the level of physical function and quality of life in patients with a hip fracture
(Visschedijk et al., 2013). Thus, fear of falling is considered important to target at an early
stage in the rehabilitation after hip fracture (Jellesmark, Herling, Egerod, & Beyer, 2012).
Studies of medical (Brown, Redden, Flood, & Allman, 2009; Doherty-King &
Bowers, 2011; Pedersen et al., 2013) or geriatric in-hospital, non-surgical patients (Brown et
al., 2009; Villumsen, Jorgensen, Andreasen, Rathleff, & Molgaard, 2014) have found low
amounts of time spent standing or walking (upright time), down to a median of 43 minutes
per day during admission. Some of these results in non-surgical patients suggest that an
increase in upright time is associated with achieved independent basic mobility skills
(Pedersen et al., 2013; Villumsen et al., 2014). In hip fracture patients hospitalized in the
acute orthopedic ward, even lower levels of activity - down to an average of 16 minutes of
standing and walking per day - have recently been reported (Davenport et al., 2014). This
emphasizes the relevance of an early, targeted rehabilitation towards independent mobility
and walking skills for the hip-fracture patient to prevent excessive functional decline.
A usual gait speed below 0.6 m/s has been associated with an increased risk of
mobility disability in a general population (Cummings, Studenski, & Ferrucci, 2014).
Furthermore, risk thresholds of maintaining in-hospital walking independence in acutely ill
older adults has been identified to be usual gait speeds down to 0.30 to 0.35 m/s, which may
serve as a relevant target value of independent mobility in a population of hip-fracture
patients (Graham, Fisher, Berges, Kuo, & Ostir, 2010; Kronborg, Bandholm, Palm, Kehlet, &
Kristensen, 2014). Thus, the physical function even at the very early stage after hip-fracture
surgery seems vital to future perspectives for the individual patient.
Objective measurement of 24-hour PA together with functional tests during admission
will provide useful knowledge of the relation between the level of basic mobility skills and
the actual time spent upright by the individual throughout the day (Grant et al., 2010; Ostir et
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
al., 2013). Combined with fall-related self-efficacy data we aimfor a better understanding of
factors affecting PA in hip fracture patients right after surgery. Consequently, in this study we
measured the 24-hour PA (upright time) and associations with physical function and fear of
falling in older adults ( 65 years old) the first week in the acute orthopedic ward after hip-
fracture surgery, in order to generate knowledge towards planning of optimal recovery
programs for hip-fracture patients in the acute ward.
Method
Study Design and Population
In this observational study, a sample of 38 older adults ( 65 years old) admitted to
the acute orthopedic hip fracture unit at a university hospital was recruited from 40 patients
enrolled in another study concerning feasibility of strength training (Kronborg et al., 2014)
(Figure 1. For original, detailed enrollment, see Kronborg et al.). No compensation for
participation was given, but patients were instructed that mobilization was considered
beneficial for the recovery. All patients were home residing with an independent pre-fracture
ability to walk indoor, according to a modified and reliable (Kristensen, Bandholm, Foss,
Ekdahl, & Kehlet, 2008; Kristensen & Kehlet, 2012) indoor New Mobility Score (NMS)
(Parker & Palmer, 1993) of 2 or more. The NMS evaluates the pre-fracture functional level
with a score from 0 (no walking ability) to 9 (fully independent) consisting of sub-scores
within 3 activities; indoor walking, outdoor walking and walking during shopping. Each
activity provides a score from 0 to 3 (0: not at all, 1: with help from another person, 2: with a
walking aid or 3: no difficulty and no aid) (Kristensen & Kehlet, 2012). All patients were
allowed full weight-bearing immediately after surgery and followed an optimized,
multimodal, in-hospital treatment program (Kehlet, 2011) that included a daily regular
physical therapy program at postoperative day 1-3 and most often daily on weekdays
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
hereafter. A previous study evaluating the physical activity level (monitored with an ActivPal
body-worn sensor) in older people with impaired function reported difficulties in registration
of walking activity, and especially at slow gait speeds (Taraldsen et al., 2011). Physical
activity (ActivPal) data evaluated in the present study were therefore collected as an
amendment to the feasibility study (Kronborg et al., 2014). The study was approved by the
Capital Region’s Research Ethics Committee (H-A-2007-0127) and conducted according to
the Declaration of Helsinki. The reporting of the study adheres to the Strengthening the
Reporting of Observational Studies in Epidemiology (STROBE) guidelines, using the
checklist for cohort studies (Vandenbroucke et al., 2007) (Checklist S1).
Data Collection and Outcomes
One trained physical therapist from the Department of Physical Therapy with more
than 10 years of clinical experience handled the data collection. Patients were included at the
first day or no later than the 3rd day after surgery. The primary outcomes were the time spent
standing and walking (upright time) and the number of daily up right events (sitting to
standing) per 24 hoursand measured by one thigh-worn, accelerometer-based, activity
monitor (ActivPal3TM, PAL Technologies Ltd., Glasgow, UK). Corresponding with the day
of patient inclusion the monitor was set to record for 10 days non-stop, wrapped waterproof
and attached by an adhesive pad (PALstickie) mid-line on the quadriceps region of the non-
fractured limb and 1/3 of the way from the hip to the knee.
The ActivPal3TM accelerometer, measuring physical activity as time spent in the sit/lie
position (X-axis), standing (Y-axis) and walking (Z-axis), has been validated in several
studies in healthy adults (Godfrey, Culhane, & Lyons, 2007) and in older adults with a hip
fracture (Taraldsen, Vereijken, Thingstad, Sletvold, & Helbostad, 2013; Taraldsen et al.,
2011). Still, the default setting of the monitor for registration of walking is a limitation to our
sample, since walking is defined as an activity in the Z-axis with a cadence of more than 20
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
steps per minute. For an older adult right after hip fracture surgery, this level of gait speed is
most often not possible to achieve. This means that some of the time actually spent walking is
not registered as walking or step count, but as time spent standing. We performed several
tests to determine the accuracy of registrations of step count and time spent walking in
conditions similar to the sample of older adults with impaired walking ability. The tests
showed a huge discrepancy between the monitor’s registration of step count and walking time
and the actual performance with a loss of counts up to 60% in a single bout of non-stop slow
walking. Based on this and related findings by others (Taraldsen et al., 2011; Grant et al.,
2010), we chose not to analyze data on step count and the time spent walking as single
outcomes. Instead, we analysed data from time spent standing and walking as one outcome –
upright time – as done in related studies (Taraldsen et al., 2013; Taraldsen et al., 2013).
The ActivPal3TM software (v.7.2.29) was used to reduce data from the ActivPal
monitor having visually inspected all data for irregularities. The summary results of complete
days of data were exported to SPSS statistical software and filed as upright time (minutes
spent standing and walking) and number of upright events (sitting to standing) during 24
hours each day, between days 2 and 7 postoperatively, and used in the data analysis of
upright time and upright events per day, respectively.
Secondary outcomes included the Cumulated Ambulation Score (CAS) assessing the
basic mobility skills (getting in and out of bed, sit-to-stand-to-sit from a chair and walking,
with a maximum score of 6 = independent mobility) on a daily basis (Kristensen et al.,
2009). The day of independent mobility was determined as the first day postoperatively that
the participant achieved the maximum score of CAS = 6 and used in the data analysis
(Kristensen, Foss, Ekdahl, & Kehlet, 2010). Functional performance was measured by the
Timed Up-and-Go (TUG) test (fastest of 3 attempts used) and the 10 Meter fast speed
Walking Test (10MWT) 1 time, using a rollator as the standardized walking aid the day

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
before discharge as described in Kronborg et al. (Kronborg et al., 2014). Hip fracture-related
pain was assessed once before (at rest) and once during functional performance tests using a
five-point Verbal Ranking Scale (VRS 0–4 points; 0 = none, 1 = light, 2 = moderate, 3=
severe and 4= intolerable pain) (Bech, Lauritsen, Ovesen, & Overgaard, 2015). Fear of falling
at discharge was assessed by the Short Falls Efficacy Scale International (Short FES-I, 7-28
points, high scores indicating a high degree of fear of falling) and used in the data analysis
(Kempen et al., 2008). The Short FES-I questionnaire was administered as interviewer-
assisted, completed by paper and pencil. Demographic data included age, gender, type of
fracture, cognitive function measured in the emergency room by Hindsoe’s Test (Kristensen
M T, 2010) and postoperatively by the Mini Mental State Examination (MMSE) (Folstein,
Folstein, & McHugh, 1975), the postoperative day of discharge and discharge destination.
Data Analysis
All data were examined for normality of distribution (Kolmogorov-Smirnov and Q-Q
plots). Descriptive statistics was used to report characteristics of the study sample and the
differences were presented as mean SD when normally distributed, otherwise as medians
(first-third quartile, (IQR)) values, or as numbers with percentages. Subgroups of participants
with and without complete activity data samples – but with independent mobility at discharge
- were examined for differences using the Student t-test, Mann-Whitney U Test, Chi-square
test or the Fischer’s exact test, as appropriate. Changes in upright time and upright events
before and after achievement of independent mobility were examined using the Wilcoxon
Signed-Rank test. Correlations between upright time, the number of upright events, day
achieving independent mobility, TUG time, Fast gait speed and Short FES-I at discharge
were examined by the Spearman rho Correlation test. According to Portney & Watkins’
classification of relationship, correlation coefficients from 0 - 0.25 indicates little or no
relationship, 0.26 - 0.50 a fair degree of relationship, 0.51 - 0.75 a moderate to good degree

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
and 0.76 – 1.0 a good to excellent degree of relationship (Portney & Watkins, 2009). The
level of significance was set at p < 0.05. No formal sample size calculation was made, as the
study was considered explorative. All statistical analyses were conducted with the SPSS
statistical software (version 19; SPSS inc. Chicago, Illinois, USA).
Results
Thirty-eight patients agreed to participate and were included in the study. One
participant who lost the monitor due to detachment during an early postoperative stage of
confusion and delirium was excluded from further analysis. Otherwise, no episodes of
postoperative delirium were noted in the study sample. Characteristics of the remaining 37
participants; mean age of 80 8.4 years, 19 with a cervical hip fracture and 29 (78%) women
are presented in Table 1. These participants wore an activity monitor continuously the first
week after surgery for a median of 6 (5-6) days (Table 2). The majority of participants (n =
22) used no walking aid before hospitalization. Out of the remaining 15 participants, 11 used
a rollator or crutches for indoor activity, 7 used a walking aid or personal assistance for
outdoor activities, while 5 participants needed a walking aid or assistance for shopping.
Thirty participants (81%) achieved independent basic mobility before discharge using a
walking aid (walker or crutches). Of these, complete activity data was available for 20 (54%)
participants at the day before and after independent mobility was achieved (mean of 6.7 2.4
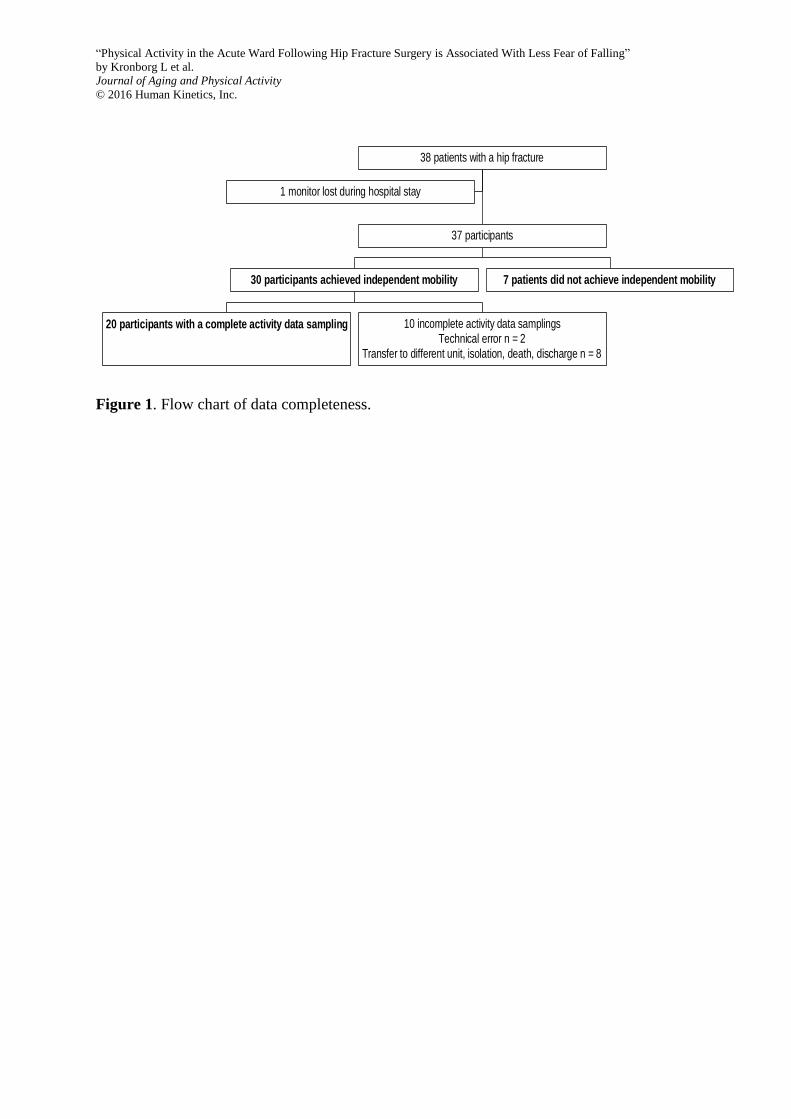
days postoperatively) (Table 3). Incomplete samplings occurred in 10 participants as 2
monitors had technical errors, 2 samplings were stopped due to transfer to a different ward, 1
monitor was removed due to isolation of the patient, 1 patient died during hospitalization and
4 samplings were incomplete (< 24 hours) due to discharge on the day of achieving
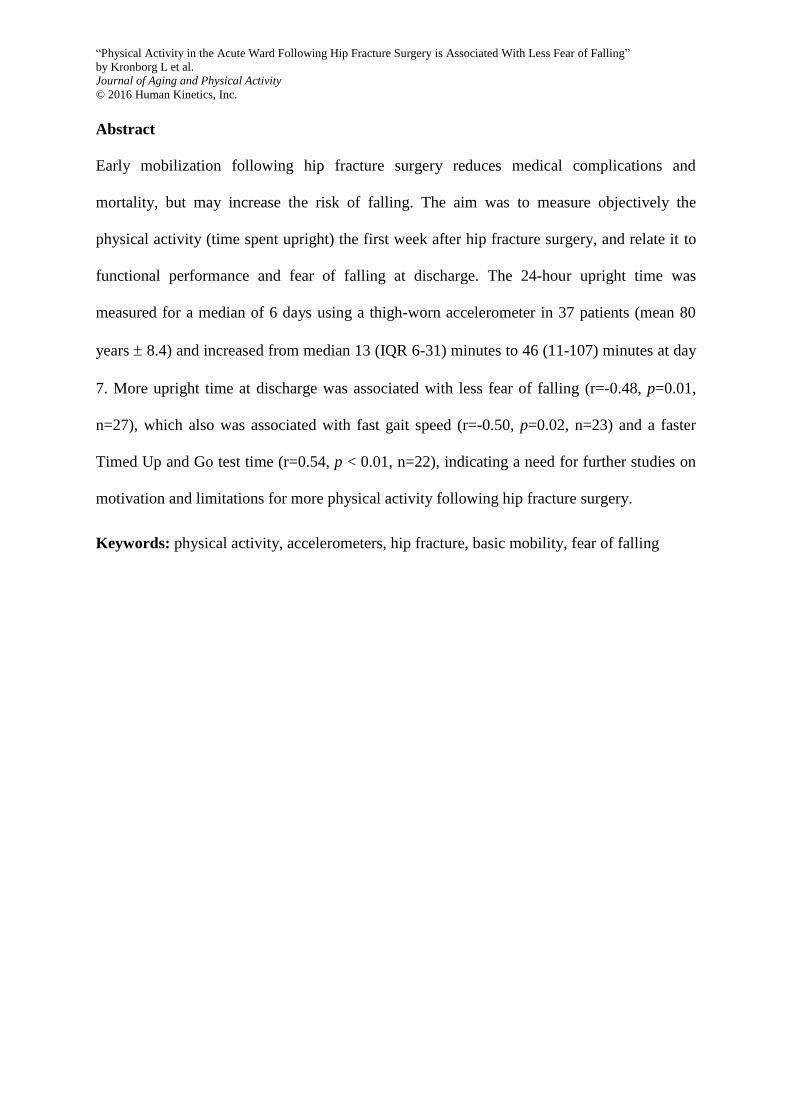
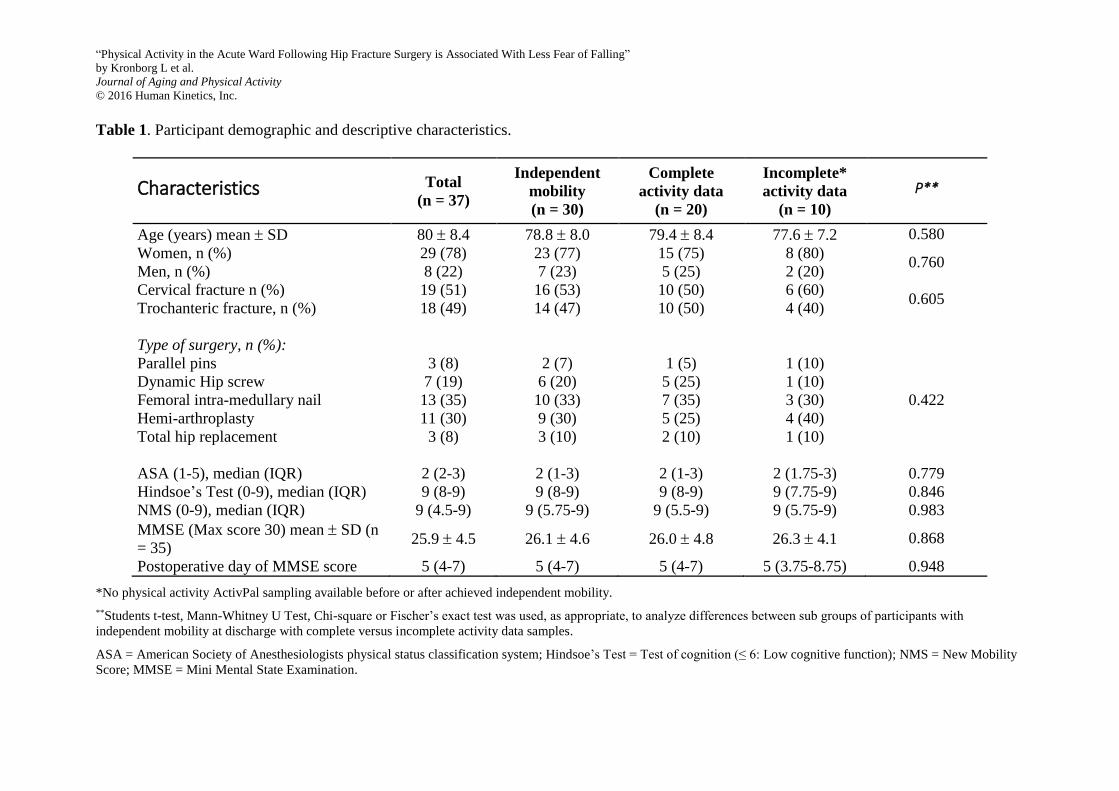
independent mobility (Figure 1). There were no significant differences in the characteristics
between subgroups of participants who achieved independent mobility and had complete
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
activity data (n = 20) or incomplete activity data sampling (n = 10) (Table 1). Twenty-nine
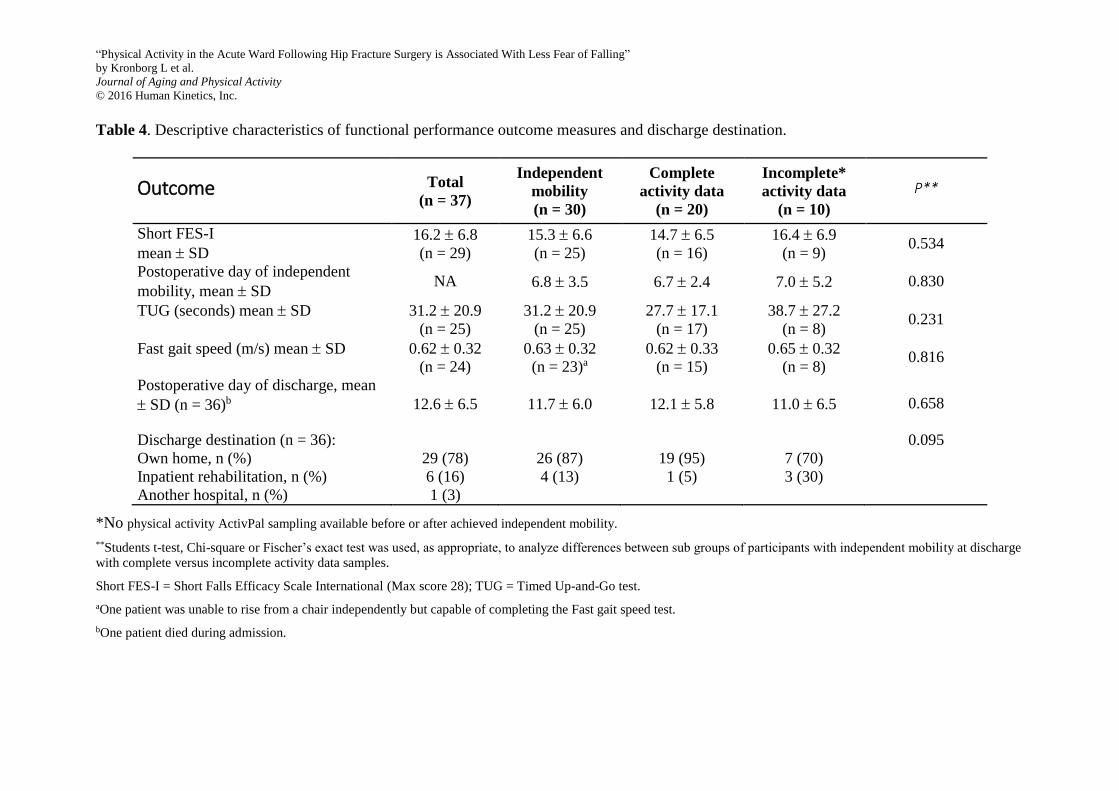
participants (78%) were discharged to their home, 6 (16%) to inpatient rehabilitation and 1
(3%) to another hospital while 1 participant died during admission (Table 4).
Primary Analyses
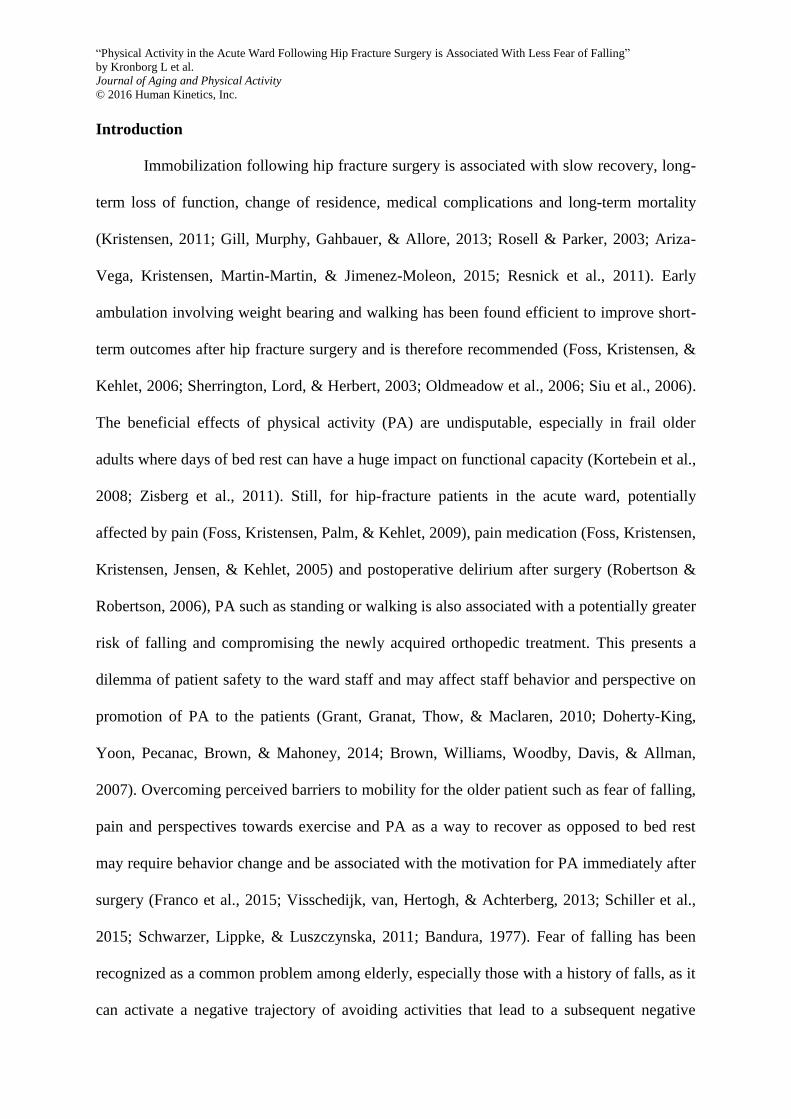
Upright time for all participants, irrespective of whether they achieved independent
mobility or not during the hospital stay, increased from a median of 13 (6;31) min/day in
patients monitored at day 2 (n = 26) to 46 (11;107) min/day at day 7 (n = 29). Likewise, the
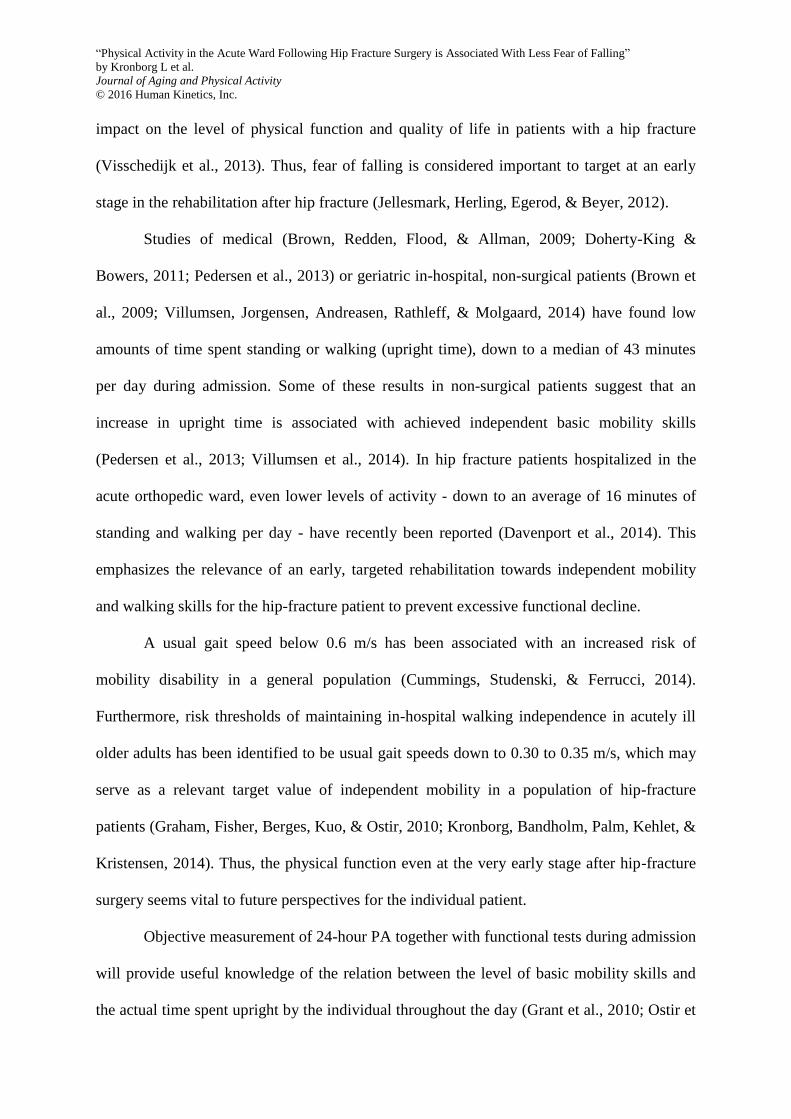
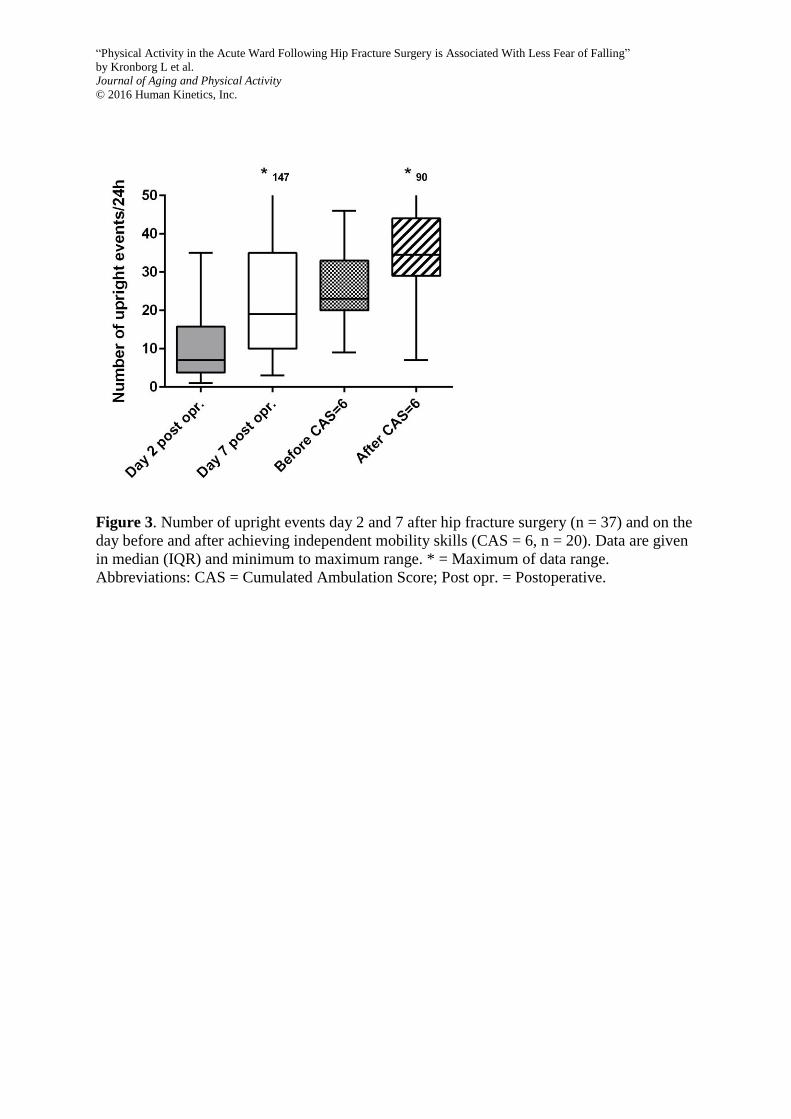
median number of upright events per day increased from 7 (4;16) at day 2 to 18 (8;34)
upright events at day 7 (Table 2, Figure 2-3).
In the subgroup of participants with complete activity data (n = 20), the median time
spent upright increased from 60 (39;112) to 91 (72;119) min/day (z = -2.315, p = 0.021) from
the day before compared to the day after achieving independent mobility, and with a variation
from 14 to 205 minutes upright on day 7. The median number of upright events increased
from 23 (20;33) at the day before to 35 (29;44) upright events at the day after achieving
independent mobility (z = -2.708, p = 0.007) (Figure 2-3, Table 3).
Secondary Analyses
The mean TUG time was 31.2 (20.9) seconds (n = 25) while the mean fast gait speed
was 0.63 (0.32) m/s (n = 23) at discharge in the subgroup of participants who achieved
independent mobility (Table 4). There was no significant difference in results on TUG
performance (p = 0.231) and fast gait speed (p = 0.816) between subgroups of participants
who achieved independent mobility and had complete activity data or not (Table 4). Hip
fracture-related pain at rest was reported to none or light pain while 4 patients reported more
than light pain during functional performance tests. No significant differences were found
between subgroups of complete or incomplete data (pain at TUG, p = .057 and pain at
10MWT, p = 1.00). Significant differences (p = 0.001) were found in pre-fracture level of
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
function (NMS) between participants that did and did not achieve independent mobility. No
significant differences were found between these subgroups in any other outcome.
Correlation analyses revealed that earlier achievement of independent mobility after surgery
was associated with more upright time before (r = -0.451, p < 0.05) and after (r = -0.574, p <
0.01) achieving independent mobility, as well as on the day before discharge (r = -0.596, p <
0.01). More upright time at discharge was associated with less fear of falling (r = -0.48, p =
0.01, n = 27), which also was associated with fast gait speed (r = -0.50, p = 0.02, n = 23) and
a faster Timed Up and Go test time (r = 0.54, p < 0.01, n = 22.
Discussion
The primary aim of this study was to report the 24-hour PA and associations with
physical function and fear of falling in older adults one week after hip fracture surgery.
Improvements in PA were mainly observed in patients achieving independent mobility skills
and with fair to moderate associations connecting more PA with a lower degree of fear of
falling. Large variations between subjects were seen in the upright time, differing from 14 to
205 minutes in 24hours, measured 7 days after surgery.
A large variation is common to find in studies of PA in older adults, which might also
relate to differences in early recovery programs (e.g., comprehensive geriatric care compared
to orthopaedic care), as found in a Norwegian study (Taraldsen et al., 2013). Thus, the
upright time at postoperative day 4 reached a mean of 52 (63.7) minutes and 21.8 (19.9)
upright events for the sample of patients receiving comprehensive geriatric care as compared
to 45.1 (57.7) minutes upright time and 19 (16.5) upright events in the orthopedic care sample
(Taraldsen et al., 2013). In comparison, the mean upright time at postoperative day 4 in our
sample (n = 35) was 52.1 (52.5) minutes per day and number of upright events 18.5 (15.7),
placing the sample in the present study in alignment with these care-modalities.

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
The significant association between the physical performances (TUG and 10MWT),
upright time at discharge and fear of falling (Short FES-I) is interesting. This underlines the
importance that adequate attention is given to inform, motivate and empower, the patient as
well as the ward staff, to maximize the patients’ confidence to engage in PA shortly after hip
fracture surgery. A potential action to this could be an increased mutual recognition of
Bandura’s social cognitive theory of behaviour change (Bandura, 1977). In this terminology,
such a behavior change could for our patients begin with verbal encouragement from the
health professionals to facilitate motivation and strategies to challenge possible pain and fear
of falling and engage in physical activity. To the patient, this will be the potential way to an
experience of success (i.e. mastery experience) and regain of further physical function by
addressing the different sources of self-efficacy (Bandura, 1977; Schwarzer et al., 2011;
Warner et al., 2014). Corresponding with this, the understanding of factors affecting PA in
hospitalized older adults have been studied and explained as highly multifactorial including
complications, lack of resources, unit expectations to ambulate patients as well as the
decisions made by the nurses and the patient’s relatives (Doherty-King & Bowers, 2011). The
patterns of sedentary behavior during hospitalization have been found to continue the patterns
of PA in community-dwelling hip fracture patients the first year after surgery (Fleig et al.,
2015; Resnick et al., 2011). The limitations, as well as the possibilities for PA in the acute
setting, are many, as illustrated by Zisberg et. al (Zisberg, Shadmi, Gur-Yaish, Tonkikh, &
Sinoff, 2015). The findings from these studies add to the understanding of the low levels of
PA recorded in our study and underline the need for tailored recovery programs for older
adults after hip fracture surgery.
The achievement of independent mobility at an early stage after surgery was found to
have a positive association withupright time in the present study. Thus, patients that achieved
independent mobility later after surgery spent significantly less time upright and had more
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
fear of falling at discharge, compared to those who achieved independent mobility at an
earlier day after surgery. Since the importance of PA as a way to prevent complications for
older adults during hospital stay has been established, these findings are considered important
to address specifically as a part of the early recovery program after a hip fracture as
highlighted in recent studies (Davenport et al., 2014; Jellesmark et al., 2012).
The very low levels of hip fracture-related pain reported during functional
performance tests indicate that pain as such was no limitation to PA in the present study.
However, these tests were performed on the day before discharge and may not reflect the
levels of pain experienced before this day. Cummings et al. found that usual gait speed below
0.6 m/s is equal to increased risk of mobility disability (Cummings et al., 2014). These results
show how disposed our sample of older adults with a low mean fast speed gait of 0.63 0.32
m/s are to the risk of further mobility disability and loss of vital physical function.with This is
further underlined by the no-falls cut-point of 24 seconds to perform the TUG test at
discharge as identified by Kristensen et al. (Kristensen, Foss, & Kehlet, 2007), categorizing
the majority of participants in the present study at increased risk of new falls within the
following 6 months. Thus, continuous rehabilitation and fall prevention is still highly
necessary post-discharge, despite an optimized in-hospital treatment program (Kehlet, 2009).
Strength and Limitations
The ActivPal monitor was well tolerated by the participants in the present study, and
no adverse events were reported. However, the monitor had a tendency to detach during the
up to 10 days of non-stop wear either due to wear-out of the adhesive tape or to removal by
staff during treatment or personal care. The monitor that was lost during our study
disappeared due to detachment by the participant during a stage of confusion and delirium.
Our study sample was small and was minimized further by some incomplete activity
data samples. Nevertheless, no significant difference was found in characteristics between the
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
subgroups of participants who achieved independent mobility but had complete or incomplete
activity data sampling (Table 1). Still, the interpretation of our findings are limited to a
population treated in an optimized in-hospital treatment program (Kehlet, 2009).
The data collection was performed in the acute ward, providing important knowledge on the
actual in-hospital PA and the associations with mobility skills and fear of falling in hip
fracture patients at this early time point after surgery. To our knowledge, this is the first study
on this topic and, thus, adds to the understanding of how to further optimize future recovery
programs for older adults after hip fracture surgery.
Conclusion
In this study, patients with a hip fracture increased the upright time during the first
week postoperatively, while following an enhanced recovery program in an acute orthopedic
ward. More time spent upright was significantly associated with less fear of falling and
mainly observed in patients achieving independent mobility skills during their admission. The
low amount of physical activity and the associations between the time spent upright,
independent mobility skills and fear of falling at discharge indicate a need of actions to
further motivate both patients and health professionals towards behavior changes that
facilitate increased physical activity immediately after hip fracture surgery.
ACKNOWLEDGMENTS
Additional contribution: We thank all the patients in this study for their valuable
contribution. A special thank to the participating physical therapists, Maria Svennergren (B.
Pt.), Kirsten Aunskjær Pedersen (Pt.), Kirsten Juel Nielsen (Pt.), Maria StokholmVan (B. Pt.)
and Sanne Busk Stie (B. Pt.), nurse staff and doctors from the Hip Fracture Unit and the
Department of Orthopedic Surgery at Hvidovre Hospital, whom provided essential
cooperative assistance with the study without any compensation.

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Funding
The study was supported by grants from The IMK Foundation, The Research Foundation of
the Capital Region, The Research Foundation of the Danish Physical Therapy Organization,
The Research Foundation of Hvidovre Hospital and The UCSF Lundbeck Foundation. The
funding agencies had no influence on the study design, methods, subjects, data collection,
analyses or manuscript.
Disclosures
The authors have declared that no competing interests exist.
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Reference List
Ariza-Vega, P., Kristensen, M. T., Martin-Martin, L., & Jimenez-Moleon, J. J. (2015).
Predictors of long-term mortality in older people with hip fracture. Archives of
Physical Medicine and Rehabilitation, 96(7), 1215-1221. S0003-9993(15)00138-0
[pii];10.1016/j.apmr.2015.01.023 [doi].
Bandura, A. (1977). Self-efficacy: toward a unifying theory of behavioral change.
Psychological Review, 84(2), 191-215.
Bech, R. D., Lauritsen, J., Ovesen, O., & Overgaard, S. (2015). The Verbal Rating Scale is
reliable for assessment of postoperative pain in hip fracture patients. Pain Research
and Treatment, 2015 676212. 10.1155/2015/676212 [doi].
Brown, C. J., Redden, D. T., Flood, K. L., & Allman, R. M. (2009). The underrecognized
epidemic of low mobility during hospitalization of older adults. Journal of the
American Geriatrics Society, 57(9), 1660-1665.
Brown, C. J., Williams, B. R., Woodby, L. L., Davis, L. L., & Allman, R. M. (2007). Barriers
to mobility during hospitalization from the perspectives of older patients and their
nurses and physicians. Journal of Hospital Medicine, 2(5), 305-313. 10.1002/jhm.209
[doi].
Cummings, S. R., Studenski, S., & Ferrucci, L. (2014). A diagnosis of dismobility--giving
mobility clinical visibility: a Mobility Working Group recommendation. JAMA,
311(20), 2061-2062. 1865472 [pii];10.1001/jama.2014.3033 [doi].
Davenport, S. J., Arnold, M., Hua, C., Schenck, A., Batten, S., & Taylor, N. F. (2014).
Physical activity levels during acute inpatient admission after hip fracture are very
low. Physiotherapy Research International, 10.1002/pri.1616 [doi].
Doherty-King, B. & Bowers, B. (2011). How nurses decide to ambulate hospitalized older
adults: development of a conceptual model. Gerontologist, 51(6), 786-797. gnr044
[pii];10.1093/geront/gnr044 [doi].
Doherty-King, B., Yoon, J. Y., Pecanac, K., Brown, R., & Mahoney, J. (2014). Frequency
and duration of nursing care related to older patient mobility. Journal of Nursing
Scholarship, 46(1), 20-27. 10.1111/jnu.12047 [doi].
Fleig, L., McAllister, M. M., Brasher, P., Cook, W. L., Guy, P., Puyat, J. et al. (2015).
Sedentary behaviour and physical activity patterns in older adults after hip fracture: A
call to action. Journal of Aging and Physical Activity, 2015-0013
[pii];10.1123/japa.2015-0013 [doi].
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). "Mini-mental state". A practical
method for grading the cognitive state of patients for the clinician. Journal of
Psychiatric Research, 12(3), 189-198. 0022-3956(75)90026-6 [pii].
Foss, N. B., Kristensen, M. T., & Kehlet, H. (2006). Prediction of postoperative morbidity,
mortality and rehabilitation in hip fracture patients: the cumulated ambulation score.
Clinical Rehabilitation, 20(8), 701-708.

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Foss, N. B., Kristensen, M. T., Kristensen, B. B., Jensen, P. S., & Kehlet, H. (2005). Effect of
postoperative epidural analgesia on rehabilitation and pain after hip fracture surgery: a
randomized, double-blind, placebo-controlled trial. Anesthesiology, 102(6), 1197-
1204. 00000542-200506000-00020 [pii].
Foss, N. B., Kristensen, M. T., Palm, H., & Kehlet, H. (2009). Postoperative pain after hip
fracture is procedure specific. British Journal of Anaesthesia, 102(1), 111-116.
aen345 [pii];10.1093/bja/aen345 [doi].
Franco, M. R., Tong, A., Howard, K., Sherrington, C., Ferreira, P. H., Pinto, R. Z. et al.
(2015). Older people's perspectives on participation in physical activity: a systematic
review and thematic synthesis of qualitative literature. British Journal of Sports
Medicine, bjsports-2014-094015 [pii];10.1136/bjsports-2014-094015 [doi].
Gill, T. M., Murphy, T. E., Gahbauer, E. A., & Allore, H. G. (2013). The course of disability
before and after a serious fall injury. JAMA Internal Medicine, 173(19), 1780-1786.
1729533 [pii];10.1001/jamainternmed.2013.9063 [doi].
Godfrey, A., Culhane, K. M., & Lyons, G. M. (2007). Comparison of the performance of the
activPAL Professional physical activity logger to a discrete accelerometer-based
activity monitor. Medical Engineering and Physics, 29(8), 930-934. S1350-
4533(06)00204-9 [pii];10.1016/j.medengphy.2006.10.001 [doi].
Graham, J. E., Fisher, S. R., Berges, I. M., Kuo, Y. F., & Ostir, G. V. (2010). Walking speed
threshold for classifying walking independence in hospitalized older adults. Physical
Therapy, 90(11), 1591-1597. ptj.20100018 [pii];10.2522/ptj.20100018 [doi].
Grant, P. M., Granat, M. H., Thow, M. K., & Maclaren, W. M. (2010). Analyzing free-living
physical activity of older adults in different environments using body-worn activity
monitors. Journal of Aging and Physical Activity, 18(2), 171-184.
Jellesmark, A., Herling, S. F., Egerod, I., & Beyer, N. (2012). Fear of falling and changed
functional ability following hip fracture among community-dwelling elderly people:
an explanatory sequential mixed method study. Disability and Rehabilitation, 34(25),
2124-2131. 10.3109/09638288.2012.673685 [doi].
Kehlet, H. (2009). Multimodal approach to postoperative recovery. Current Opinion in
Crititcal Care, 15(4), 355-358.
Kehlet, H. (2011). Fast-track surgery-an update on physiological care principles to enhance
recovery. Langenbeck's Archives of Surgery, 396(5), 585-590.
Kempen, G. I., Yardley, L., van Haastregt, J. C., Zijlstra, G. A., Beyer, N., Hauer, K. et al.
(2008). The Short FES-I: a shortened version of the falls efficacy scale-international
to assess fear of falling. Age and Ageing, 37(1), 45-50. afm157
[pii];10.1093/ageing/afm157 [doi].
Kortebein, P., Symons, T. B., Ferrando, A., Paddon-Jones, D., Ronsen, O., Protas, E. et al.
(2008). Functional impact of 10 days of bed rest in healthy older adults. Journals of
Gerontology Series A: Biological Sciences and Medical Sciences, 63(10), 1076-1081.
63/10/1076 [pii].

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Kristensen M T (2010). Thesis. Hip fractures, functional assessments and factors influencing
in-hospital outcome, a physiotherapeutic perspective. Department of Health Sciences,
Division of Physiotherapy, Faculty of Medicine, Lund University, Sweden.
Kristensen, M. T. (2011). Factors affecting functional prognosis of patients with hip fracture.
European Journal of Physical and Rehabilitation Medicine, 47(2), 257-264.
R33112514 [pii].
Kristensen, M. T., Andersen, L., Bech-Jensen, R., Moos, M., Hovmand, B., Ekdahl, C. et al.
(2009). High intertester reliability of the cumulated ambulation score for the
evaluation of basic mobility in patients with hip fracture. Clinical Rehabilitation,
23(12), 1116-1123. 0269215509342330 [pii];10.1177/0269215509342330 [doi].
Kristensen, M. T., Bandholm, T., Foss, N. B., Ekdahl, C., & Kehlet, H. (2008). High inter-
tester reliability of the new mobility score in patients with hip fracture. Journal of
Rehabilitation Medicine, 40(7), 589-591. 10.2340/16501977-0217 [doi].
Kristensen, M. T., Foss, N. B., Ekdahl, C., & Kehlet, H. (2010). Prefracture functional level
evaluated by the New Mobility Score predicts in-hospital outcome after hip fracture
surgery. Acta Orthopaedica, 81(3), 296-302. 10.3109/17453674.2010.487240 [doi].
Kristensen, M. T., Foss, N. B., & Kehlet, H. (2007). Timed "up & go" test as a predictor of
falls within 6 months after hip fracture surgery. Physical Therapy, 87(1), 24-30.
ptj.20050271 [pii];10.2522/ptj.20050271 [doi].
Kristensen, M. T. & Kehlet, H. (2012). Most patients regain prefracture basic mobility after
hip fracture surgery in a fast-track programme. Danish Medical Journal, 59(6),
A4447. A4447 [pii].
Kronborg, L., Bandholm, T., Palm, H., Kehlet, H., & Kristensen, M. T. (2014). Feasibility of
progressive strength training implemented in the acute ward after hip fracture surgery.
PLOS ONE, 9(4), e93332. 10.1371/journal.pone.0093332 [doi];PONE-D-13-39133
[pii].
Oldmeadow, L. B., Edwards, E. R., Kimmel, L. A., Kipen, E., Robertson, V. J., & Bailey, M.
J. (2006). No rest for the wounded: early ambulation after hip surgery accelerates
recovery. ANZ Journal of Surgery, 76(7), 607-611. ANS3786 [pii];10.1111/j.1445-
2197.2006.03786.x [doi].
Ostir, G. V., Berges, I. M., Kuo, Y. F., Goodwin, J. S., Fisher, S. R., & Guralnik, J. M.
(2013). Mobility activity and its value as a prognostic indicator of survival in
hospitalized older adults. Journal of the American Geriatrics Society, 61(4), 551-557.
10.1111/jgs.12170 [doi].
Parker, M. J. & Palmer, C. R. (1993). A new mobility score for predicting mortality after hip
fracture. Journal of Bone and Joint Surgery.British Volume, 75(5), 797-798.
Pedersen, M. M., Bodilsen, A. C., Petersen, J., Beyer, N., Andersen, O., Lawson-Smith, L. et
al. (2013). Twenty-four-hour mobility during acute hospitalization in older medical
patients. Journals of Gerontology Series A: Biological Sciences and Medical
Sciences, 68(3), 331-337. gls165 [pii];10.1093/gerona/gls165 [doi].

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Portney, L. G. & Watkins, M. P. (2009). Foundations of clinical research: Applications to
practice. Upper Saddle River: N.J.: Pearson/prentice Hall.
Resnick, B., Galik, E., Boltz, M., Hawkes, W., Shardell, M., Orwig, D. et al. (2011). Physical
activity in the post-hip-fracture period. Journal of Aging and Physical Activity, 19(4),
373-387.
Robertson, B. D. & Robertson, T. J. (2006). Postoperative delirium after hip fracture. Journal
of Bone and Joint Surgery, 88(9), 2060-2068. 88/9/2060 [pii];10.2106/JBJS.F.00049
[doi].
Rosell, P. A. & Parker, M. J. (2003). Functional outcome after hip fracture. A 1-year
prospective outcome study of 275 patients. Injury, 34(7), 529-532.
Schiller, C., Franke, T., Belle, J., Sims-Gould, J., Sale, J., & Ashe, M. C. (2015). Words of
wisdom - patient perspectives to guide recovery for older adults after hip fracture: a
qualitative study. Journal of Patient Preference and Adherence, 9 57-64.
10.2147/PPA.S75657 [doi];ppa-9-057 [pii].
Schwarzer, R., Lippke, S., & Luszczynska, A. (2011). Mechanisms of health behavior change
in persons with chronic illness or disability: the Health Action Process Approach
(HAPA). Rehabilitation Psychology, 56(3), 161-170. 2011-14571-001
[pii];10.1037/a0024509 [doi].
Sherrington, C., Lord, S. R., & Herbert, R. D. (2003). A randomised trial of weight-bearing
versus non-weight-bearing exercise for improving physical ability in inpatients after
hip fracture. Australian Journal of Physiotherapy, 49(1), 15-22.
Siu, A. L., Penrod, J. D., Boockvar, K. S., Koval, K., Strauss, E., & Morrison, R. S. (2006).
Early ambulation after hip fracture: effects on function and mortality. Archives of
Internal Medicine, 166(7), 766-771. 166/7/766 [pii];10.1001/archinte.166.7.766 [doi].
Taraldsen, K., Askim, T., Sletvold, O., Einarsen, E. K., Bjastad, K. G., Indredavik, B. et al.
(2011). Evaluation of a body-worn sensor system to measure physical activity in older
people with impaired function. Physical Therapy, 91(2), 277-285. ptj.20100159
[pii];10.2522/ptj.20100159 [doi].
Taraldsen, K., Sletvold, O., Thingstad, P., Saltvedt, I., Granat, M. H., Lydersen, S. et al.
(2013). Physical behavior and function early after hip fracture surgery in patients
receiving comprehensive geriatric care or orthopedic care--A randomized controlled
trial. Journals of Gerontology Series A: Biological Sciences and Medical Sciences,
glt097 [pii];10.1093/gerona/glt097 [doi].
Taraldsen, K., Vereijken, B., Thingstad, P., Sletvold, O., & Helbostad, J. L. (2013). Multiple
days of monitoring are needed to obtain a reliable estimate of physical activity in hip
fracture patients. Journal of Aging and Physical Activity, 2012-0130 [pii].
Vandenbroucke, J. P., von, E. E., Altman, D. G., Gotzsche, P. C., Mulrow, C. D., Pocock, S.
J. et al. (2007). Strengthening the Reporting of Observational Studies in
Epidemiology (STROBE): explanation and elaboration. Epidemiology, 18(6), 805-
835. 10.1097/EDE.0b013e3181577511 [doi];00001648-200711000-00028 [pii].
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Villumsen, M., Jorgensen, M. G., Andreasen, J., Rathleff, M. S., & Molgaard, C. M. (2014).
Very low levels of physical activity in older patients during hospitalization at an acute
geriatric ward - A Prospective Cohort Study. Journal of Aging and Physical Activity,
2014-0115 [pii];10.1123/japa.2014-0115 [doi].
Visschedijk, J., van, B. R., Hertogh, C., & Achterberg, W. (2013). Fear of falling in patients
with hip fractures: prevalence and related psychological factors. Journal of the
American Medical Directors Association, 14(3), 218-220. S1525-8610(12)00402-1
[pii];10.1016/j.jamda.2012.10.013 [doi].
Warner, L. M., Schuz, B., Wolff, J. K., Parschau, L., Wurm, S., & Schwarzer, R. (2014).
Sources of self-efficacy for physical activity. Health Psychology, 33(11), 1298-1308.
2014-12178-001 [pii];10.1037/hea0000085 [doi].
Zisberg, A., Shadmi, E., Gur-Yaish, N., Tonkikh, O., & Sinoff, G. (2015). Hospital-
associated functional decline: the role of hospitalization processes beyond individual
risk factors. Journal of the American Geriatrics Society, 63(1), 55-62.
10.1111/jgs.13193 [doi].
Zisberg, A., Shadmi, E., Sinoff, G., Gur-Yaish, N., Srulovici, E., & Admi, H. (2011). Low
mobility during hospitalization and functional decline in older adults. Journal of the
American Geriatrics Society, 59(2), 266-273. 10.1111/j.1532-5415.2010.03276.x
[doi].
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Figure 1. Flow chart of data completeness.
1 monitor lost during hospital stay
20 participants with a complete activity data sampling 10 incomplete activity data samplings
Technical error n = 2
Transfer to different unit, isolation, death, discharge n = 8
30 participants achieved independent mobility 7 patients did not achieve independent mobility
37 participants
38 patients with a hip fracture

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Figure 2. Time spent upright day 2 and 7 after hip fracture surgery (n = 37) and on the day
before and after achieving independent mobility skills (CAS = 6, n = 20). Data are given in
median (IQR) and minimum to maximum range. * = Maximum of data range.
Abbreviations: CAS = Cumulated Ambulation Score; Post opr. = Postoperative.
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Figure 3. Number of upright events day 2 and 7 after hip fracture surgery (n = 37) and on the
day before and after achieving independent mobility skills (CAS = 6, n = 20). Data are given
in median (IQR) and minimum to maximum range. * = Maximum of data range.
Abbreviations: CAS = Cumulated Ambulation Score; Post opr. = Postoperative.
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Table 1. Participant demographic and descriptive characteristics.
Characteristics
Total
(n = 37)
Independent
mobility
(n = 30)
Complete
activity data
(n = 20)
Incomplete*
activity data
(n = 10)
P**
Age (years) mean SD 80 8.4 78.8 8.0 79.4 8.4 77.6 7.2 0.580
Women, n (%) 29 (78) 23 (77) 15 (75) 8 (80) 0.760
Men, n (%) 8 (22) 7 (23) 5 (25) 2 (20)
Cervical fracture n (%) 19 (51) 16 (53) 10 (50) 6 (60) 0.605
Trochanteric fracture, n (%) 18 (49) 14 (47) 10 (50) 4 (40)
Type of surgery, n (%):
0.422
Parallel pins 3 (8) 2 (7) 1 (5) 1 (10)
Dynamic Hip screw 7 (19) 6 (20) 5 (25) 1 (10)
Femoral intra-medullary nail 13 (35) 10 (33) 7 (35) 3 (30)
Hemi-arthroplasty 11 (30) 9 (30) 5 (25) 4 (40)
Total hip replacement 3 (8) 3 (10) 2 (10) 1 (10)
ASA (1-5), median (IQR) 2 (2-3) 2 (1-3) 2 (1-3) 2 (1.75-3) 0.779
Hindsoe’s Test (0-9), median (IQR) 9 (8-9) 9 (8-9) 9 (8-9) 9 (7.75-9) 0.846
NMS (0-9), median (IQR) 9 (4.5-9) 9 (5.75-9) 9 (5.5-9) 9 (5.75-9) 0.983
MMSE (Max score 30) mean SD (n
= 35) 25.9 4.5 26.1 4.6 26.0 4.8 26.3 4.1 0.868
Postoperative day of MMSE score 5 (4-7) 5 (4-7) 5 (4-7) 5 (3.75-8.75) 0.948
*No physical activity ActivPal sampling available before or after achieved independent mobility.
**Students t-test, Mann-Whitney U Test, Chi-square or Fischer’s exact test was used, as appropriate, to analyze differences between sub groups of participants with
independent mobility at discharge with complete versus incomplete activity data samples.
ASA = American Society of Anesthesiologists physical status classification system; Hindsoe’s Test = Test of cognition (≤ 6: Low cognitive function); NMS = New Mobility
Score; MMSE = Mini Mental State Examination.

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Table 2. Physical Activity data for participants (n = 37).
Day after surgery
Variable 2
(n = 26)
3
(n = 34)
4
(n = 35)
5
(n = 35)
6
(n = 31)
7
(n = 29)
24h Upright time
(minutes)
median (IQR) 13 (6-31) 21 (8-47) 42 (9-79) 48 (16-102) 46 (7-103) 46 (11-107)
24h upright events
(n) median (IQR) 7 (4-16) 11 (5-22) 14 (6-30) 20 (8-32) 20 (6-33) 18 (8-34)
Participants with
incomplete 24h
activity data (n)
11 3 2 2 6 8
Reason for incomplete data:
Day of monitor
appliance (n) 11 2
Technical error (n) 1 1
Participant
discharged (n) 1 2 6 8

“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Table 3. Physical Activity data for participants with independent mobility achieved and
complete data sampling (n = 20).
Participants with independent
mobility achieved and complete
data sampling (n = 20)
Day after surgery
Variable 2
(n = 14)
3
(n = 20)
4
(n = 20)
5
(n = 20)
6
(n = 18)
7
(n = 18)
Upright time,
median (IQR)
(min/day) 11 (5-29) 24 (9-44) 54 (17-85) 79 (33-113) 81 (37-124) 80 (39-121)
24h upright events
(n) median (IQR) 8 (3-16) 12 (8-23) 19 (12-29) 24 (20-35) 28 (22-35) 30 (17-45)
Reason for incomplete data:
Day of monitor
appliance (n) 6
Participant
discharged (n) 2 2
“Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated With Less Fear of Falling”
by Kronborg L et al.
Journal of Aging and Physical Activity
© 2016 Human Kinetics, Inc.
Table 4. Descriptive characteristics of functional performance outcome measures and discharge destination.
Outcome
Total
(n = 37)
Independent
mobility
(n = 30)
Complete
activity data
(n = 20)
Incomplete*
activity data
(n = 10)
P**
Short FES-I
mean SD
16.2 6.8
(n = 29)
15.3 6.6
(n = 25)
14.7 6.5
(n = 16)
16.4 6.9
(n = 9) 0.534
Postoperative day of independent
mobility, mean SD NA 6.8 3.5 6.7 2.4 7.0 5.2 0.830
TUG (seconds) mean SD 31.2 20.9
(n = 25)
31.2 20.9
(n = 25)
27.7 17.1
(n = 17)
38.7 27.2
(n = 8) 0.231
Fast gait speed (m/s) mean SD 0.62 0.32
(n = 24)
0.63 0.32
(n = 23)a 0.62 0.33
(n = 15)
0.65 0.32
(n = 8) 0.816
Postoperative day of discharge, mean
SD (n = 36)b 12.6 6.5 11.7 6.0 12.1 5.8 11.0 6.5 0.658
Discharge destination (n = 36): 0.095
Own home, n (%) 29 (78) 26 (87) 19 (95) 7 (70)
Inpatient rehabilitation, n (%) 6 (16) 4 (13) 1 (5) 3 (30)
Another hospital, n (%) 1 (3)
*No physical activity ActivPal sampling available before or after achieved independent mobility.
**Students t-test, Chi-square or Fischer’s exact test was used, as appropriate, to analyze differences between sub groups of participants with independent mobility at discharge
with complete versus incomplete activity data samples.
Short FES-I = Short Falls Efficacy Scale International (Max score 28); TUG = Timed Up-and-Go test.
aOne patient was unable to rise from a chair independently but capable of completing the Fast gait speed test.
bOne patient died during admission.





























