Embed Size (px)
Citation preview
PEDIATRIC AND NEONATAL RESUSCITATION
Kristen JohnsonAdam Oster
Objectives
Highlight differences between pediatric and adult cardiac arrest regarding Etiology Outcomes
Practice the basics of pediatric resuscitation through a variety of cases
Provide numbers and tips to help in a crunch
Review controversial areas of resuscitation
Not little adults?
Newly Born – in delivery room, including first few hours of life
Newborn – delivery until discharge from hospital/NICU
Infant – initial discharge from hospital until 12 months
Child – 1 year old until adolescence (signs of puberty)
Adult – adolescent (signs of puberty) and older
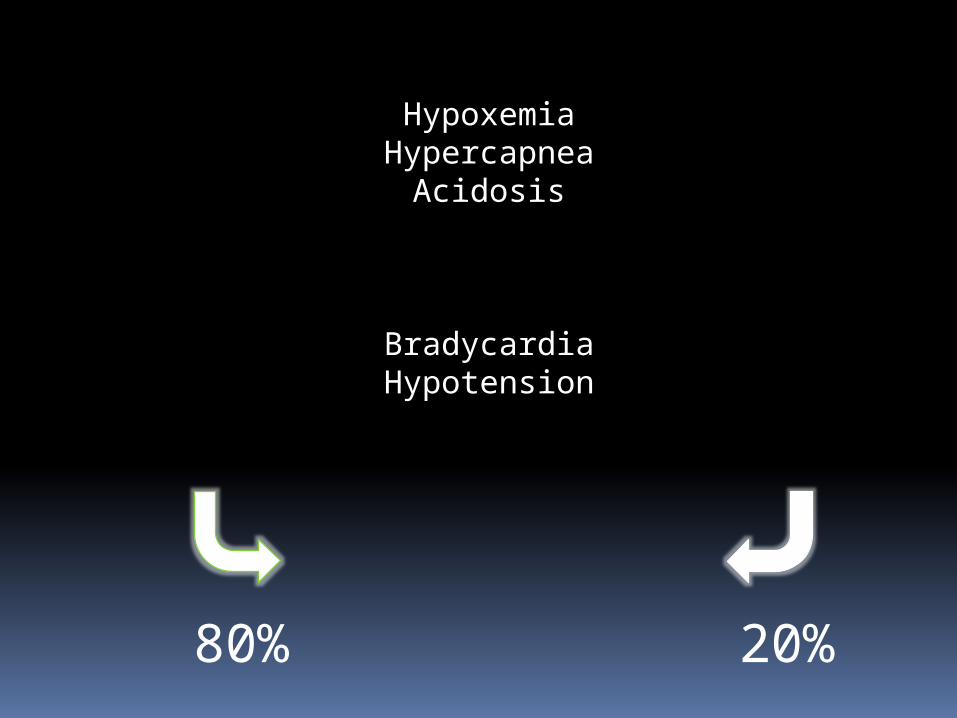
80% 20%
HypoxemiaHypercapnea
Acidosis
BradycardiaHypotension
Airway intervention saves 90%
IV access saves 9%
Drugs save 1%
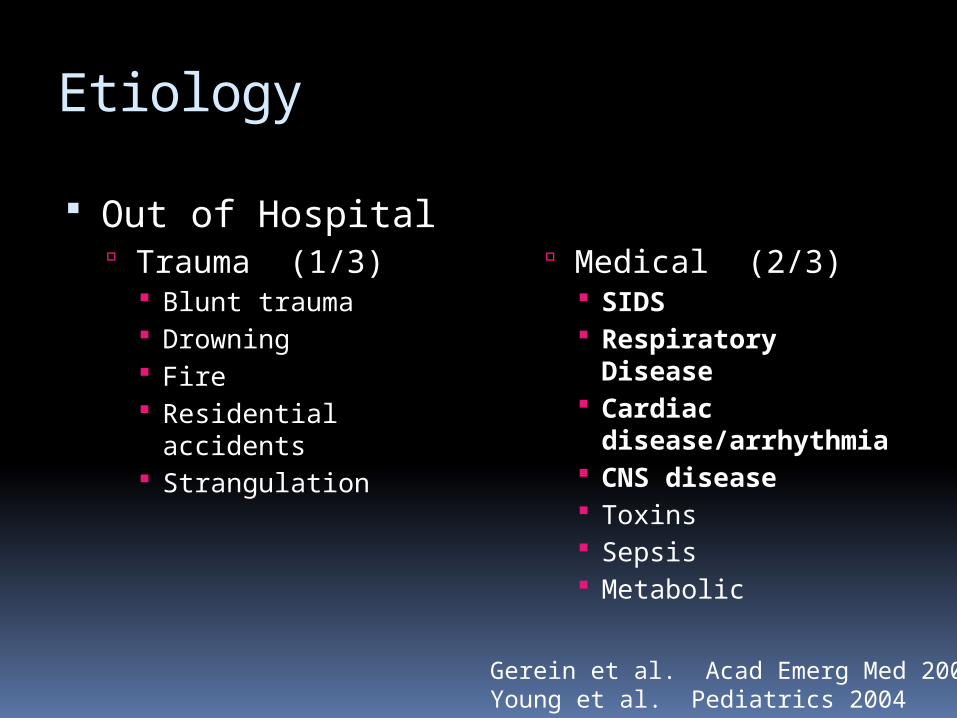
Etiology
Out of Hospital Trauma (1/3)
Blunt trauma Drowning Fire Residential accidents Strangulation
Medical (2/3) SIDS Respiratory
Disease Cardiac
disease/arrhythmia CNS disease Toxins Sepsis Metabolic
Gerein et al. Acad Emerg Med 2006Young et al. Pediatrics 2004
Incidence of Out of Hospital Cardiac Arrest
Atkins et al. Circulation 2009
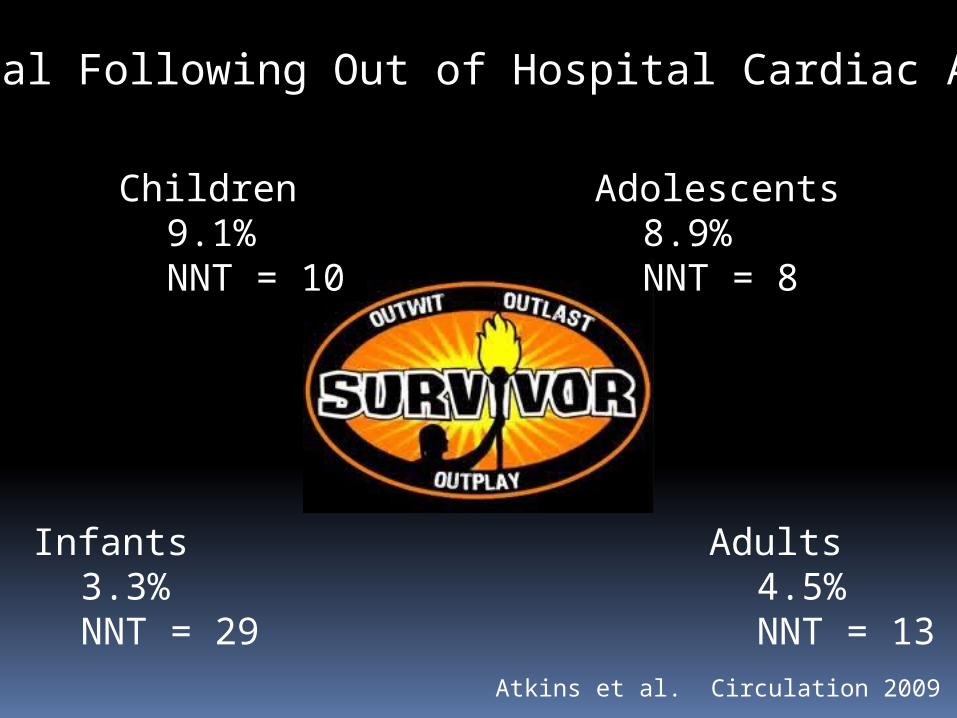
Survival Following Out of Hospital Cardiac Arrest
Infants3.3%NNT = 29
Children9.1%NNT = 10
Adolescents8.9%NNT = 8
Adults4.5%NNT = 13
Atkins et al. Circulation 2009
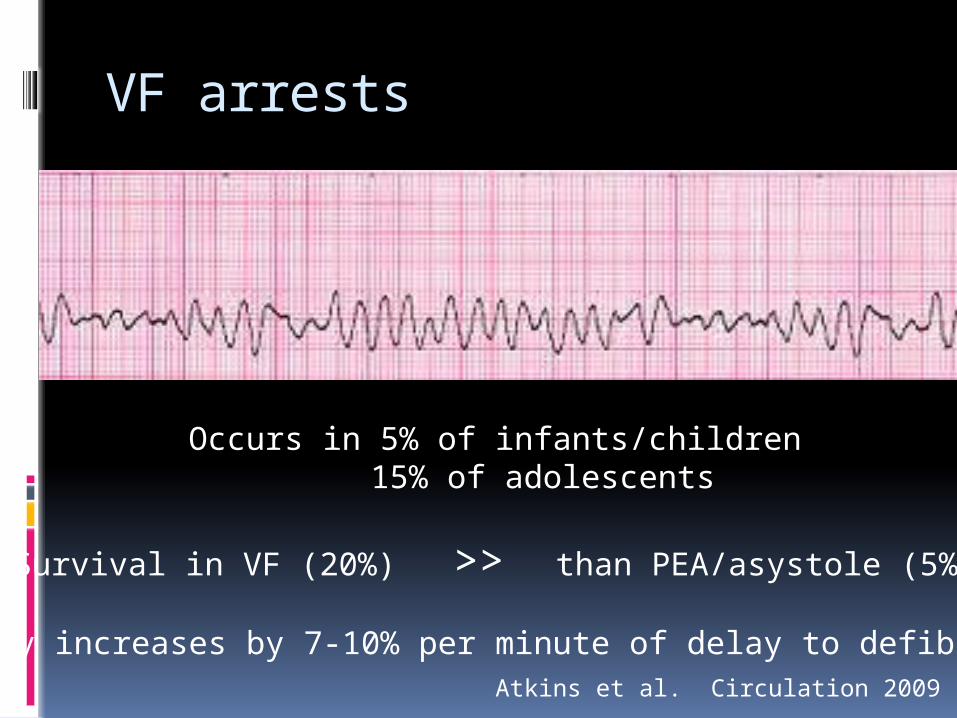
VF arrests
Occurs in 5% of infants/children15% of adolescents
Survival in VF (20%) >> than PEA/asystole (5%)
Mortality increases by 7-10% per minute of delay to defibrillationAtkins et al. Circulation 2009
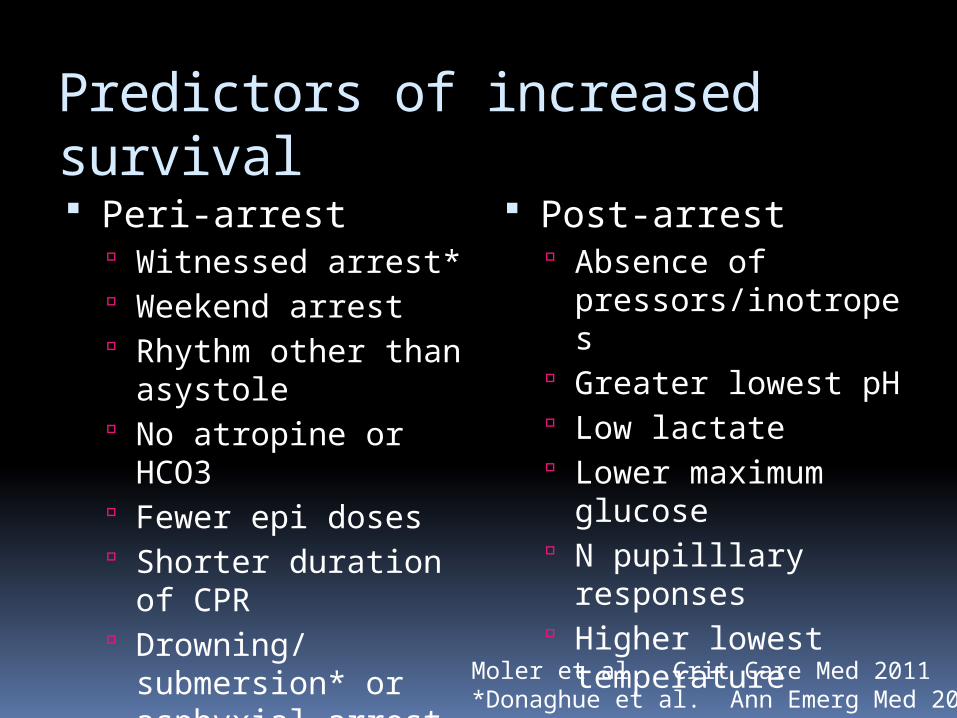
Predictors of increased survival Peri-arrest
Witnessed arrest* Weekend arrest Rhythm other than
asystole No atropine or
HCO3 Fewer epi doses Shorter duration of
CPR Drowning/
submersion* or asphyxial arrest
Post-arrest Absence of
pressors/inotropes Greater lowest pH Low lactate Lower maximum
glucose N pupilllary
responses Higher lowest
temperatureMoler et al. Crit Care Med 2011*Donaghue et al. Ann Emerg Med 2005

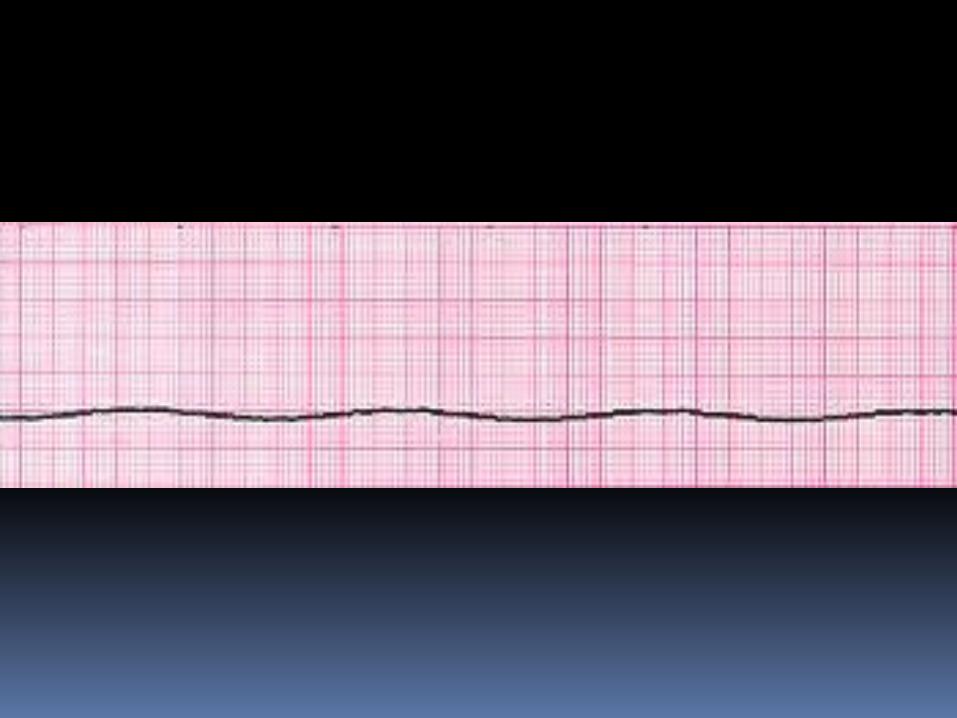
Unresponsive in crib this morning
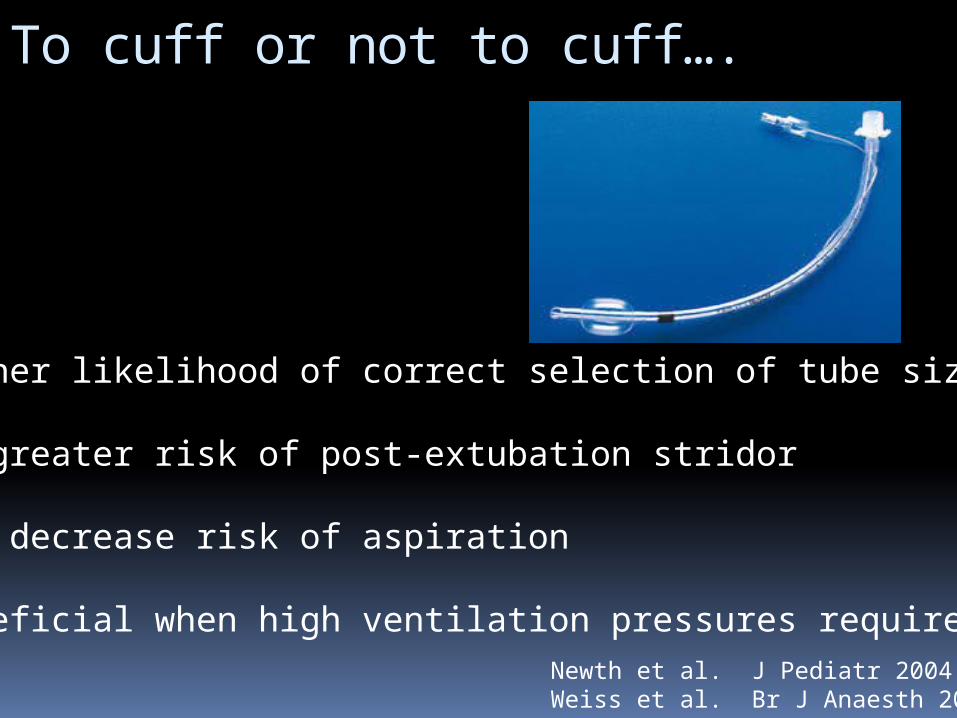
To cuff or not to cuff….
Higher likelihood of correct selection of tube size
No greater risk of post-extubation stridor
May decrease risk of aspiration
Beneficial when high ventilation pressures requiredNewth et al. J Pediatr 2004Weiss et al. Br J Anaesth 2009
Any role for intratracheal epi?Maybe Probably Not
Is there a role for high dose epinephrine?
“Less is more…”
“There is no survival benefit from high dose epinephrine, and it may be harmful, particularly
in asphyxia.”Dieckmann et al. Pediatrics 1995Carpenter et al. Pediatrics 1997Perondi et al. NEJM 2004Patterson et al. Pediatr Emerg Care 2005
Family presence during resuscitationPatient perspective• ???
Family perspective•overwhelmingly positive
Clinician perspective• mixed thoughts
Families should be allowed in the resuscitation room.Families Clinicians
Majority want to be present
Most do not regret their decision to be present
Positive trend in psychological health Less anxiety/depression Fewer disturbing
memories Eased grief
Family presence does not delay or interfere with care
Procedural performance is not affected Some have performance
anxiety Some have medical-legal
concerns
Nurses > Physicians > Trainees in willingness to include familiesTinsley et al. Pediatrics 2008
???When to call it???
Young et al. Pediatrics 2004Moler et al. Crit Care Med 2011Raymond et al. Pediatr Crit Care Med 2010Morris et al. Pediatr Crit Care Med 2004
>3 doses of epinephrine > 30 minutes of CPR in ED
Exceptions:Primary cardiac disease and
ECMO availableHypothermiaSuspected toxicologic cause

Called STAT overhead
18 month old Unwell for 3-4 days
FeverCough
resp distress
Should we cool our patient?
Adults
Neonates
Pediatrics ?
Fink et al. Pediatr Crit Care Med 2010Doherty et al. Circulation 2009
7 year old girl
Unwell for 1 weekFlu-like illness
Low grade fever
What is the best energy dose for defibrillation?
2 J/kg likely too low
3-5 J/kg may be better
No more than 10 J/kg
PALS = 2 - 4 J/kg with 4 J/kg for subsequent shocks
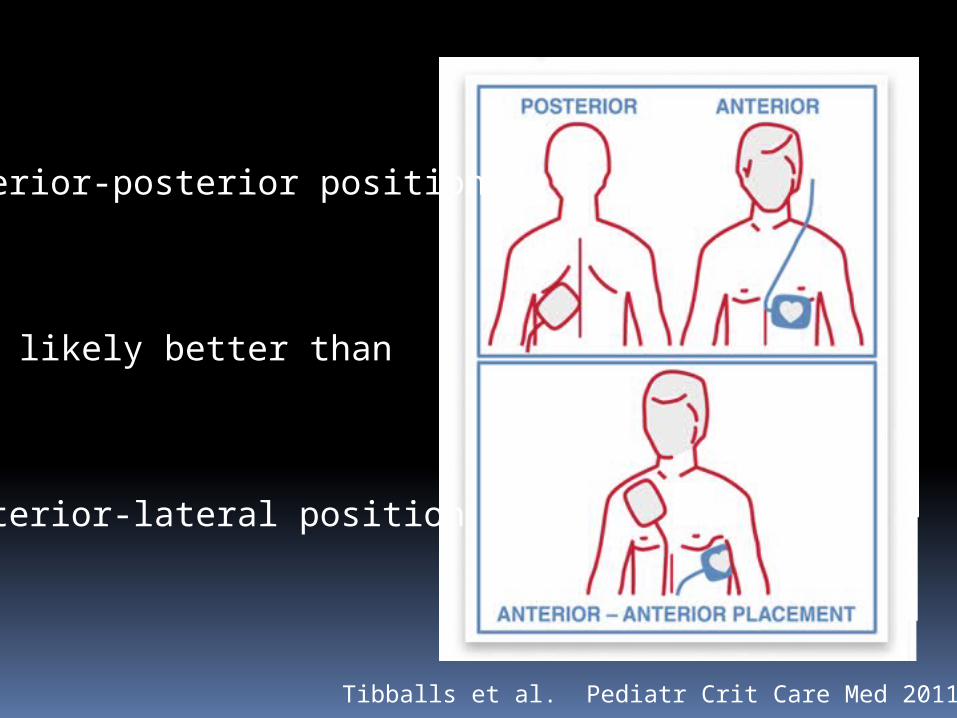
Anterior-posterior position
likely better than
Anterior-lateral position
Tibballs et al. Pediatr Crit Care Med 2011
Calcium associated with worse outcomes
Survival21% vs. 44%
Favorable neuro outcome15% vs. 35%
Exceptionselectrolyte abnormalitiestoxicological abnormality
Srinivasan et al. Pediatrics 2008
Bicarbonate not indicated in routine resuscitation Meert et al. 2009
Multi-center cohort study that found HCO3 administration associated with increased mortality
Lokesh et al. 2004 RCT showing no survival benefit in
neonates resuscitated with bicarbonate
17 year old brought in from drug house
Abdominal painThinks may be pregnant
10% of newborns will require some assistance after birth
<1% require extensive measures
<0.1% require chest compressions
< 23 weeks GA
Anencephaly
Known trisomy 13
Birth weight <400g
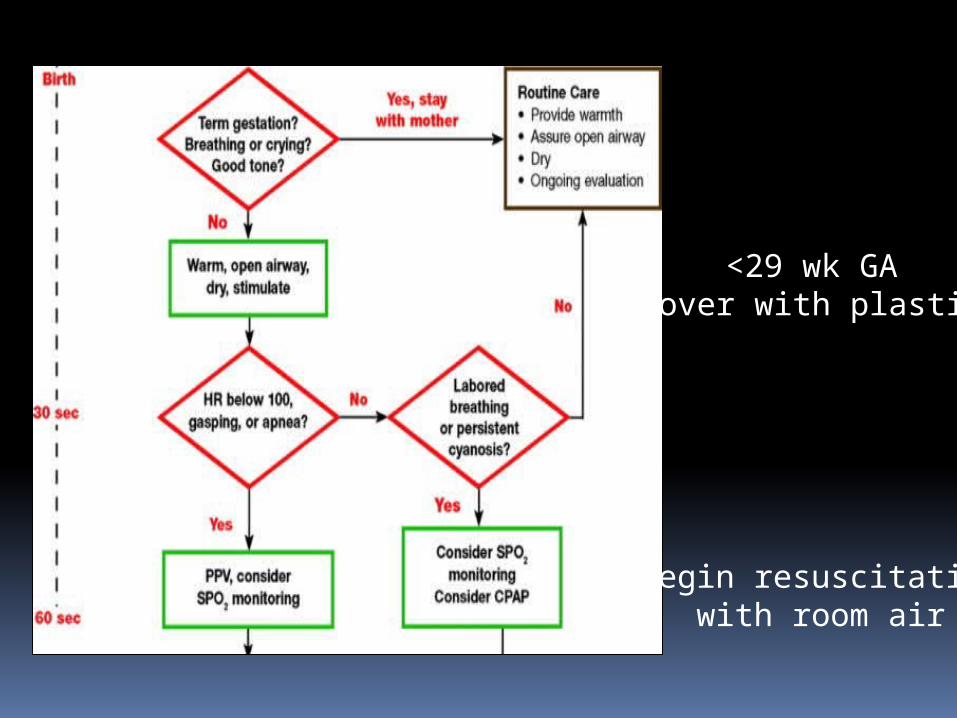
Begin resuscitationwith room air
<29 wk GACover with plastic
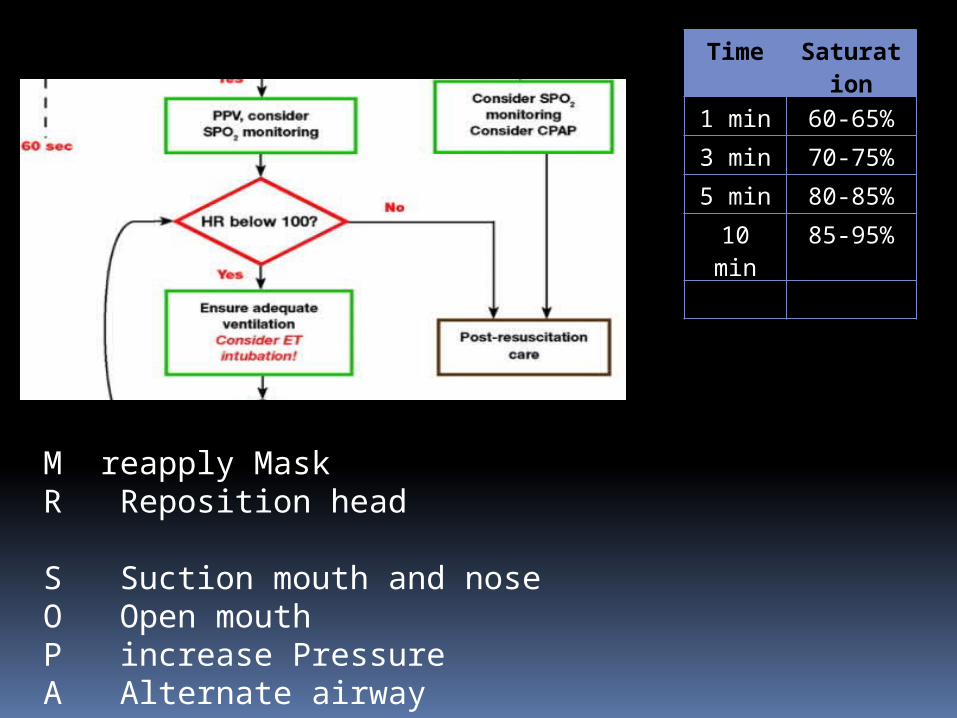
M reapply MaskR Reposition head
S Suction mouth and noseO Open mouthP increase PressureA Alternate airway
Time Saturation
1 min 60-65%
3 min 70-75%
5 min 80-85%
10 min
85-95%
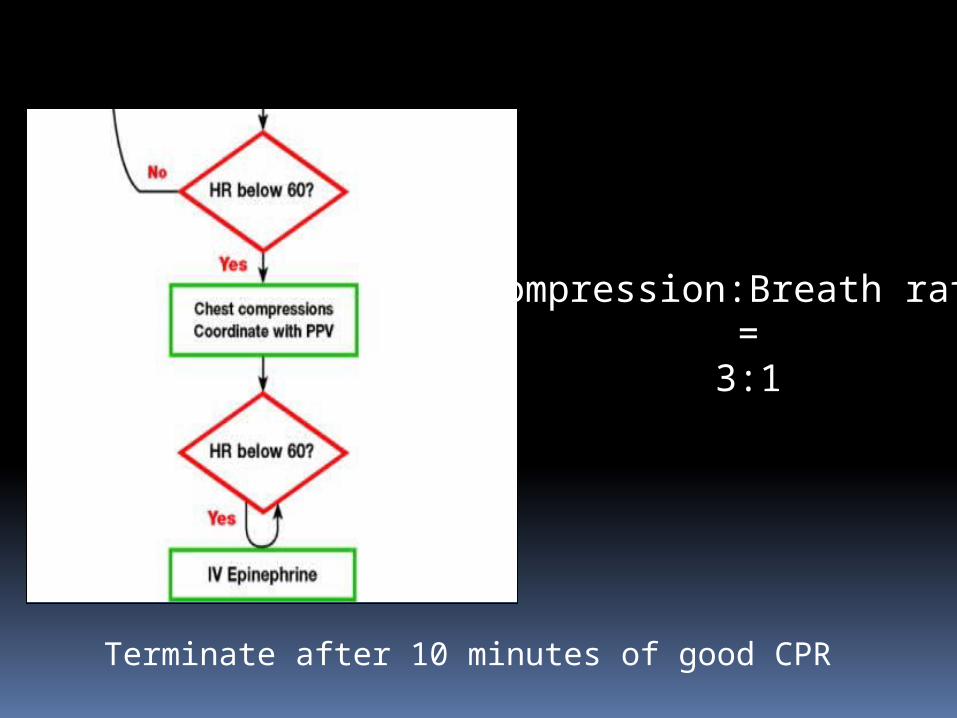
Compression:Breath ratio=
3:1
Terminate after 10 minutes of good CPR
THANKS