Embed Size (px)
Citation preview
Kris Buffington, MSW, [email protected]
Training ObjectivesTraining ObjectivesParticipants in this workshop will be able to:Id if hild i i i Identify ways child traumatic experiences can impact child development and a person’s entire life spanArticulate the rationale for use of evidence‐based Articulate the rationale for use of evidence based trauma‐focused treatmentUnderstand the core components of TF‐CBT and be bl d f l f h able to identify examples of therapeutic interventions that relate to each componentIncrease their skills in trauma‐focused assessment
Cohen, Mannarino, & Deblinger, 2008
Increase their skills in trauma focused assessment
Why are we here today?
Cohen, Mannarino, & Deblinger, 2008
Cohen, Mannarino, & Deblinger, 2008
Sometimes things occur in children’s lives that can interfere with children’slives that can interfere with children s abilities to reach their beautiful
l h h ld b lpotential… such as child abuse, neglect, violence, loss, wars, oppression, racism, , , , pp , ,sexism, poverty, and other adversities…
Cohen, Mannarino, & Deblinger, 2008
There are things we can do toThere are things we can do to help…
Cohen, Mannarino, & Deblinger, 2008
Why Address Trauma ?
Cohen, Mannarino, & Deblinger, 2008
Higher Utilizers of Mental Health Study (OregonHigher Utilizers of Mental Health Study (Oregon Dept. of Mental Health, 1999)
During a 3 year time period in the mid 1990’s a group of 69 adults used 3.1 million dollars in mental health services; Over 90% of these adults had experienced services; Over 90% of these adults had experienced childhood sexual and/or physical abuse.
Cohen, Mannarino, & Deblinger, 2008
Risk of Juvenile Delinquency“Girls who have been abused or neglected are twice as likely to be arrested as juveniles” (Widom, 2000)
“ % f h i l d i h j il j i “60% of youth involved in the juvenile justice system suffer from diagnosable mental disorders” (Wood 2002, National Mental Health Association, 1999)
Cohen, Mannarino, & Deblinger, 2008
Adverse Childhood Experiences S dStudy (Kaiser Permanente and CDC)
Adults who experienced at least 4 traumatic events in their childhood have increased risk of morbid obesity, are 2 times more likely to smoke cigarettes and are are 2 times more likely to smoke cigarettes, and are over 9 times more likely to have injected street drugs.” (Felitti and Anda, 2003)
Cohen, Mannarino, & Deblinger, 2008
Prevalence of Trauma in the Lives of ChildChildren
9 million adolescents have witnessed serious violence during their lifetimes (Kil t i k & S d N ti l I tit t f J ti during their lifetimes (Kilpatrick & Saunders, National Institute of Justice, 1997)
Over one million children are assaulted, robbed, or raped h each year (U.S. Depart. Of Justice, 1999)
Approximately 879,000 children where neglected or abused in 2000 (Children’s Bureau, 2002)abused in 2000 (Childrens Bureau, 2002)Every year 3 to 10 million children in the U.S. are exposed to domestic violence between their parents (Carter, et.al., 1999; St )Straus, 1992).
Cohen, Mannarino, & Deblinger, 2008
Trauma and Costs to Society
Cohen, Mannarino, & Deblinger, 2008
Higher Utilizers of Mental Health Study (OregonHigher Utilizers of Mental Health Study (Oregon Dept. of Mental Health, 1999)
During a 3 year time period in the mid 1990’s a group of 6 d l d illi d ll i l h l h 69 adults used 3.1 million dollars in mental health services; Over 90% of these adults had experienced childhood sexual and/or physical abuse.childhood sexual and/or physical abuse.
Cohen, Mannarino, & Deblinger, 2008
Mental Health and School Failure“Children ith se ere emotional disturbances ha e Children with severe emotional disturbances have the highest rates of school failure. 50% of these children drop out of school as compared to a 30% p p 3of children with all other kinds of disabilities.” (President’s New Freedom Commission, 2003)
Cohen, Mannarino, & Deblinger, 2008
ResiliencyyDr. Ann Masten
“The great danger I see in the idea of resilience is in expecting children to overcome deprivation and danger on their own There is no magic here ”danger on their own…There is no magic here…
Cohen, Mannarino, & Deblinger, 2008
Resiliency (cont’d)yDr. Ann Masten
“…Resilient children have been protected by the p yactions of adults, by good nurturing, by their assets, and by opportunities to succeed...”
Cohen, Mannarino, & Deblinger, 2008
What happens to children under h i d ?chronic trauma and stress?
The emergency centers of the brain can be overused, overdeveloped, at the expense of the h f h b i h l i other parts of the brain that control reasoning,
learning, emotional and behavioral regulation, and the ability to manage social relationshipsthe ability to manage social relationships.Helgeson (1997) analogy of a network of dense streets (National Clearing House on Abuse & Neglect Early Child streets…(National Clearing House on Abuse & Neglect, Early Child Development…)
Cohen, Mannarino, & Deblinger, 2008
Trauma and MemoryExplicit Memory: is the non‐emergency memory;
i d d i t th b i i d d memories are encoded into the brain in words, and filed logically; we use this type of memory when we are learning in school and work etc…gImplicit Memory stores our habits; memories are encoded in physical sensations, in fragments, and are stored with emotional meaning...
Cohen, Mannarino, & Deblinger, 2008
Attention Deficit Hyperactive Disorder includesAttention Deficit Hyperactive Disorder includes the disabilities in the following areas:
Ability to be Reflective: the ability to think Ability to be Reflective: the ability to think before actingSelectivity: the ability to focus and screen out Selectivity: the ability to focus and screen out the important from the unimportantAbility to Resist DistractionContinuity of Attention: impacts ability to sustain attention and complete assignmentsS lf A d S lf R l i Thi Self‐Awareness and Self‐Regulation: This can explain why these children are not able to be responsive to positive or negative
Cohen, Mannarino, & Deblinger, 2008
responsive to positive or negative reinforcement.
PTSD Biased perceptionsAccording to Bessel van der Kolk, people can g , p pexperience PTSD biased perceptions, seeing themselves to be in perpetual danger, always watching for the next bomb to drop for the next watching for the next bomb to drop, for the next person to harm them. Van der Kolk points to the loss of the ability to feel safe, re‐experience joys in life and to engage in meaningful positive life, and to engage in meaningful positive relationships with others.
Cohen, Mannarino, & Deblinger, 2008
Bessel van der Kolkh d fi d l t fhas defined a cluster of symptoms in an effort to bettersymptoms in an effort to better capture the impact of traumatic stress on children’s development
Cohen, Mannarino, & Deblinger, 2008
Developmental Trauma DisorderDevelopmental Trauma Disorder
A. Exposure to one or more forms of developmental d i l d bj i adverse interpersonal trauma and a subjective experience of rage, betrayal, fear, defeat, shame, etc.
B. Triggered pattern of repeated dysregulation to trauma gg p p y gcues: dysregulation high or low: emotion, physical symptoms, behavioral, cognitive, relational, self‐blame
C. Persistently altered views and expectations of self, life, C. Persistently altered views and expectations of self, life, and others, loss of trust
D. Functional impairment: educational, familial, peer, legal vocationallegal, vocational
Cohen, Mannarino, & Deblinger, 2008
Learn about evidence‐based trauma‐f dfocused treatment
What does evidence‐based trauma‐ focused treatment mean?
d d ll d d h hRandomized controlled studies have shown its effectivenessTh i li d d h i The treatment is manualized and there is a structure of supervision and fidelity monitoringSt d di d t d i th Standardized assessments are used in the assessment and outcome evaluation process
Cohen, Mannarino, & Deblinger, 2008
TF‐CBT Research
TF‐CBT is the most rigorously tested treatment for traumatized children (6 randomized trials)I d PTSD d i i t h d Improved PTSD, depression, anxiety, shame and behavior problems compared to supportive treatmentsPTSD improved more with direct child treatmentImproved parental distress, parental support, and p p p ppparental depression compared to supportive treatment
Cohen, Mannarino, & Deblinger, 2008
Empirical Support for TF‐CBT: Pre‐fi dipost findings
1. Deblinger, E., McLeer, S.V. & Henry, D. E. (1990) Journal of the American Academy of Child and Journal of the American Academy of Child and Adolescent Psychiatry, 29(5), 747‐752.
2. Stauffer, L. & Deblinger, E. (1996). Child Maltreatment 1(1), 65‐76.
Cohen, Mannarino, & Deblinger, 2008
Lessons LearnedTreatment model demonstrated promise in both individual and group therapy formats
Additional component needed to more effectively address depression in childrenaddress depression in children
Cohen, Mannarino, & Deblinger, 2008
TF CBT R d i d C ll d T i lTF‐CBT Randomized Controlled Trials
3. Deblinger, e., Lippmann, J., & Steer, R. (1996). Child Maltreatment, 9(4), 310‐321.
4. Cohen, JA & Mannarino, AP (1996). JAACAP, 35(10), 42‐50.
5. Cohen, JA & Mannarino, AP (1998). Child Maltreatment 3(1), 17‐26.D bli E S ff L & S R ( ) 6. Deblinger, E., Stauffer, L., & Steer, R. (2001). Child Maltreatment, 6(4), 332‐343.
Cohen, Mannarino, & Deblinger, 2008
Lessons Learned…TF‐CBT showed greater benefits to preschool and school‐age g p gchildren in overcoming PTSD, depression, sexual and general behavior problems as compared to passage of time and nondirective, community treatments.Parent involvement as well as behavior rehearsal and homework improved children’s acquisition of personal safety skills (Deblinger, et al., 2001).Parental levels of distress and support influence children’s overall outcomes (Cohen & Mannarino, 1996;1997).Parental participation is critical to helping children p p p govercome depression and behavior problems (Deblinger, et al., 1996).
Cohen, Mannarino, & Deblinger, 2008
Follow‐up and replication studies
7. Cohen J. & Mannarino A., (1997). JAACAP, 36(9), 1228‐1235.
8 C h J & M i A ( 8) JAACAP ( ) 8. Cohen, J. & Mannarino, A. (1998). JAACAP, 37(1), 44‐51.
9 Deblinger E Steer R & Lippmann J (1999) 9. Deblinger, E., Steer, R., & Lippmann, J. (1999). Child Abuse and Neglect, 23(12), 1371‐1378.
10. King, N., Tonge, BJ., Mullen, P., & Myerson, et al. g g J y(2000) JAACP, 59(1), 1347‐1355.
Cohen, Mannarino, & Deblinger, 2008
Lessons Learned…
Symptoms improvements maintained over one and two year follow‐up periods (Deblinger, et al., 1999; Cohen & Mannarino 1996:1997)Cohen & Mannarino, 1996:1997).Findings were replicated and generalized across racial, ethnic and geographic boundaries (King et al 2000)ethnic, and geographic boundaries (King et al., 2000).
Cohen, Mannarino, & Deblinger, 2008
A Multi‐site Randomized Controlled Trail for Sexually Abused Children with PTSD Symptoms (2004). JAACAP, 43(4), 393‐402
Judith Cohen, M.D.*Esther Deblinger, Ph.D.**Anthony Mannarino, Ph/D.*Robert Steer, Ed.D.**
*Center for Traumatic Stress in Children and Adolescents, Allegheny General Hospital
** New Jersey CARES Institute, UMDNJ‐School of Osteopathic MedicineJ y , J p
Cohen, Mannarino, & Deblinger, 2008
Design
Multi‐site randomized controlled treatment trialSexually abused children 8‐14 years‐old and their non‐offending parents/primary caretakersoffending parents/primary caretakersHad to have 5 or more PTSD symptoms, and one or more in each cluster (89% met full diagnostic criteria)( 9 g )12 individual treatment sessionsRigorous training, supervision and adherence monitoringPre‐treatment, post‐treatment, 6 and 12 month follow‐up assessments
Cohen, Mannarino, & Deblinger, 2008
TreatmentSupportive Child–Centered Therapy (CCT)
Rogerian, supportive empowerment modelRepresentative of a commonly provided treatment i itiin our communitiesContent and pace of treatment directed by parent/child not therapistparent/child, not therapistActive listening, accurate empathy, unconditional positive regard, interpretation of feelingsp g p gTherapists asks about sexual abuse at specified points but child/parent decide how, whether, and h t di l b
Cohen, Mannarino, & Deblinger, 2008
when to discuss sexual abuse.
Treatment:Trauma‐Focused Cognitive Behavioral Therapy g py(TF‐CBT)
Trauma sensitive cognitive behavioral modelModified version of evidence based model used ith d ltwith adults
Content and paced directed by therapist, in context of a collaborative therapeutic relationshipcontext of a collaborative therapeutic relationshipTherapist structures sessions so that there is a focus on skill building and direct discussion and gprocessing of the abuse experience
Cohen, Mannarino, & Deblinger, 2008
Subjects
229 sexually abused 8‐14 year old children and parents (203 completed 3 or more sessions).79% female 21% male mean age 10 76 years79% female, 21% male, mean age 10.76 years60% Caucasian, 28% African American, 4% Hispanic American, 7% Bi‐racial, 1% Other
Cohen, Mannarino, & Deblinger, 2008
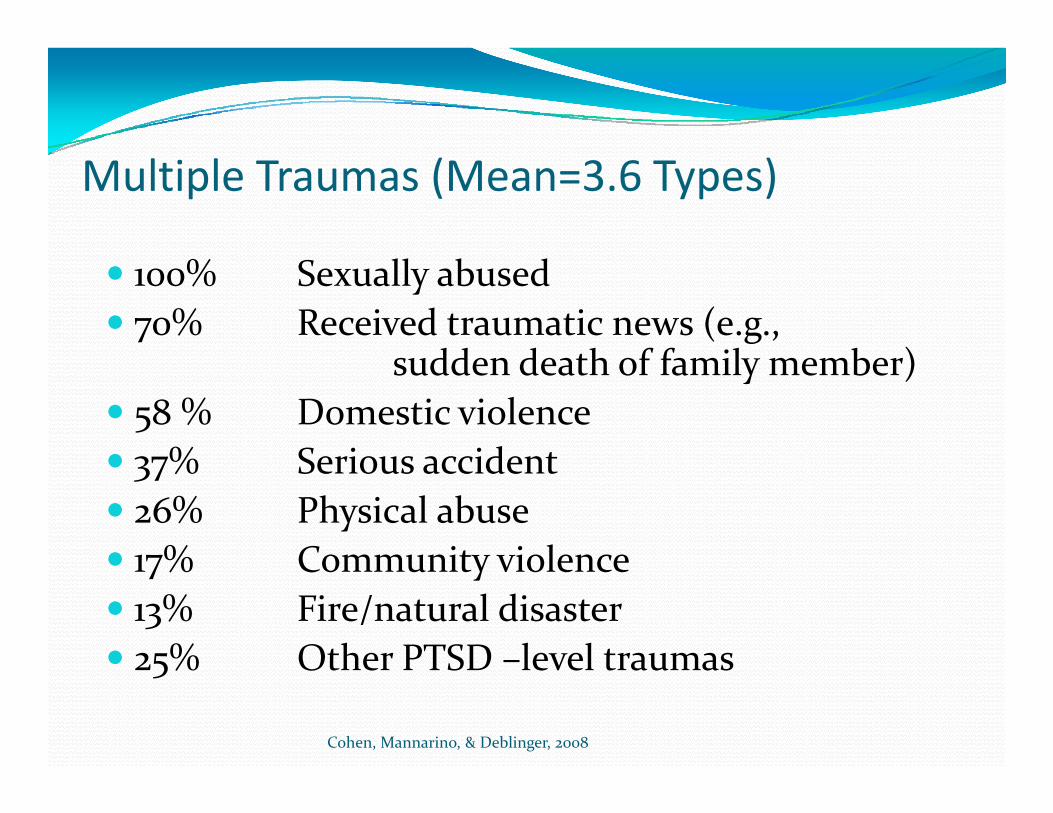
Multiple Traumas (Mean=3.6 Types)
100% Sexually abused70% Received traumatic news (e.g.,
dd d th f f il b )sudden death of family member)58 % Domestic violence37% Serious accident37% Serious accident26% Physical abuse17% Community violence17% Community violence13% Fire/natural disaster25% Other PTSD –level traumas
Cohen, Mannarino, & Deblinger, 2008
25% Other PTSD level traumas
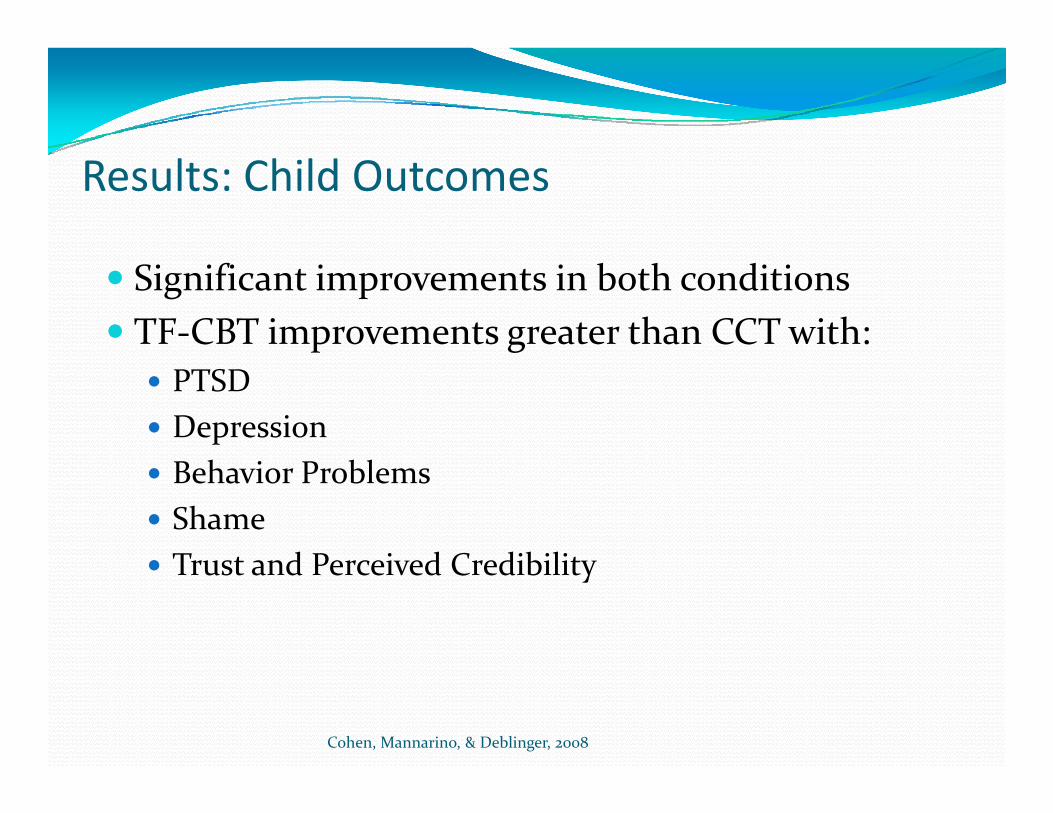
Results: Child Outcomes
Significant improvements in both conditionsTF‐CBT improvements greater than CCT with:
PTSDDepressionBehavior ProblemsShameTrust and Perceived CredibilityTrust and Perceived Credibility
Cohen, Mannarino, & Deblinger, 2008
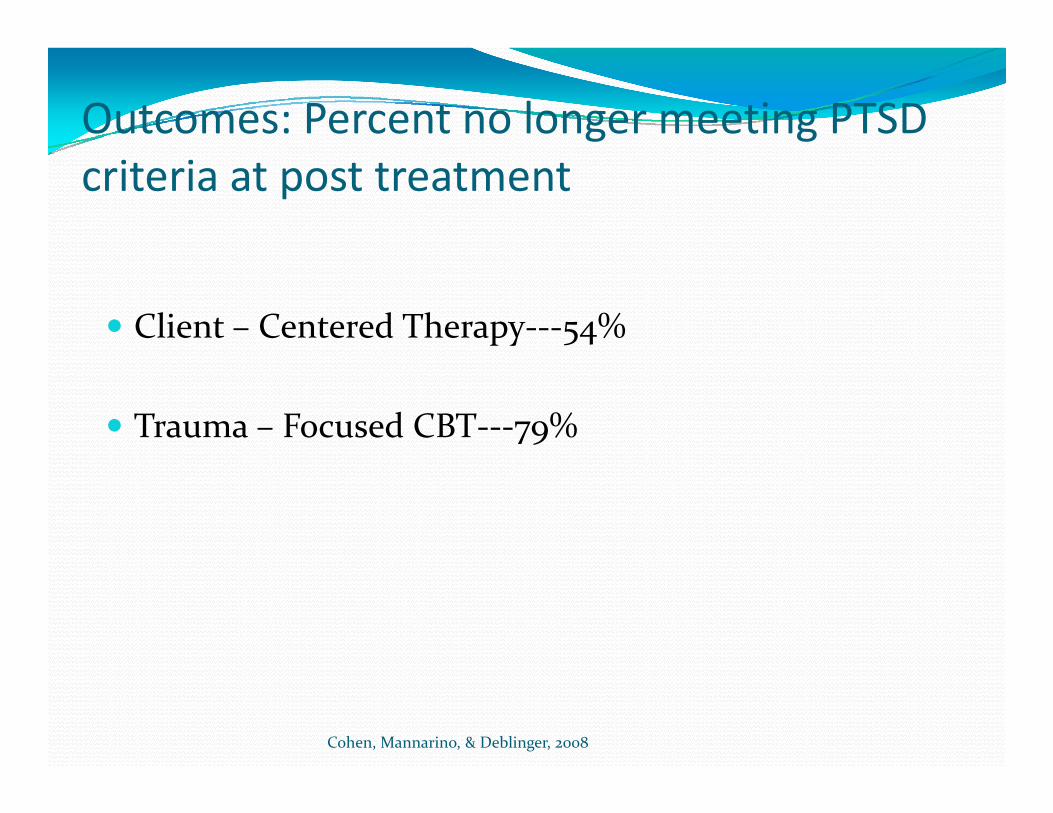
Outcomes: Percent no longer meeting PTSD criteria at post treatment
Client – Centered Therapy‐‐‐54%
Trauma – Focused CBT‐‐‐79%
Cohen, Mannarino, & Deblinger, 2008
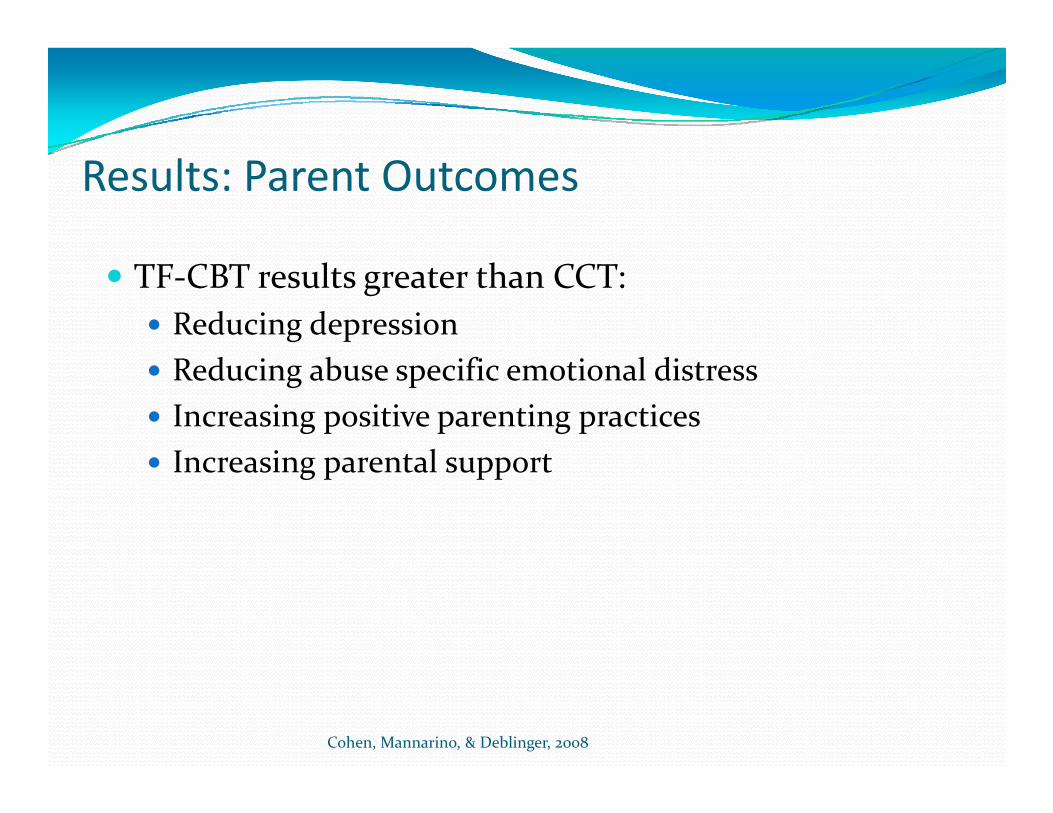
Results: Parent Outcomes
TF‐CBT results greater than CCT:Reducing depressionReducing abuse specific emotional distressIncreasing positive parenting practicesIncreasing parental supportIncreasing parental support
Cohen, Mannarino, & Deblinger, 2008
Lessons Learned…TF‐CBT is more effective than CCT in helping parents overcome depression and abuse specific di (C h l )distress (Cohen, et al., 2004).TF‐CBT is more effective than CCT in helping hild f li f h d children overcome feelings of shame and dysfunctional attributions (Cohen, et al., 2004).TF CBT appears to be preferable over CCT for TF‐CBT appears to be preferable over CCT for children with higher levels of depression and multiple traumas (Deblinger, et al, 2005).
Cohen, Mannarino, & Deblinger, 2008
multiple traumas (Deblinger, et al, 2005).
Integration of Evidence‐Based TTreatments
Families, professionals, and concerned citizens must demand quality, respectful, consumer‐ driven, and best practice evidence‐based care (Champions for the cause!)practice evidence based care…(Champions for the cause!)Establishment of learning communities to support the training and implementation of evidence‐based careAdministrators, political leaders, community leaders, funders, and consumers must work together
Cohen, Mannarino, & Deblinger, 2008
What is TF‐CBT?A hybrid treatment model that integrates:A hybrid treatment model that integrates:
Trauma sensitive interventionsCognitive‐behavioral principlesg p pAttachment theoryDevelopmental Neurobiologyp gyFamily TherapyEmpowerment TherapyHumanistic Therapy
Cohen, Mannarino, & Deblinger, 2008
Difficulties Addressed by TF‐CBT
CRAFTSCognitive problemsRelationship problemsAffective problemsFamily problemsFamily problemsTraumatic behavior problemsSomatic problemsSomatic problems
Cohen, Mannarino, & Deblinger, 2008
Core Values of TF‐CBT
CRAFTSComponents – basedRespectful of cultural valuesAdaptable and flexibleFamily focusedFamily‐focusedTherapeutic relationship is centralSelf‐efficacy is emphasizedSelf efficacy is emphasized
Cohen, Mannarino, & Deblinger, 2008
Cultural Sensitivity and Competence
Essential to understand family’s values related to religion, ethnicity, and cultureP i di h f l Previous outcome studies show successful treatment for diverse ethnic and racial populations.
Cohen, Mannarino, & Deblinger, 2008
Child and Parent Components
Individual sessions for both child and parentParent sessions‐generally parallel child sessionsSame therapist for both child and parent
Cohen, Mannarino, & Deblinger, 2008
TF‐CBT Components
PRACTICEPsycho‐education and parenting skillsRelaxationAffective modulationCognitive processingT iTrauma narrativeIn vivo desensitizationConjoint parent child sessionsConjoint parent‐child sessionsEnhancing safety and social skills
Cohen, Mannarino, & Deblinger, 2008
Psycho education
Goals:Normalize child’s and parent’s reactions to severe stressProvide information about psychological and physiological reactions to stressInstill hope for child and family recoveryInstill hope for child and family recoveryEducate family about the benefits and need for early treatment
Cohen, Mannarino, & Deblinger, 2008
Psycho education (Continued)Provide general information about the event
FrequencyWho experiences itWho experiences itWhat causes itProvide information about common emotional and behavioral
t th tresponses to the eventEmpirical information if availableClinician’s experiences with other childrenWritten literature by victimsProvide information about the child’s symptoms/diagnosisEmphasize positive coping
Cohen, Mannarino, & Deblinger, 2008
Emphasize positive coping
Parenting SkillsParenting Skills
TF‐CBT views parents as central therapeutic agents for changeagents for change.Establish the parent as the person the child turns to for help in times of trouble.Explain the rationale for parent inclusion in treatment; not because the parent is a part of the problem, but because the parent can be the p , pchild’s strongest source of healing.Emphasize positive parenting skills.E h j bl hild t i t tiEnhance enjoyable child‐parent interactions.Maximize perception/reality of effective parenting.
Cohen, Mannarino, & Deblinger, 2008
p g
Common Parental Issues in Child Traumatization
Inappropriate self‐blame and guiltInappropriate child blameOver protectivenessOver permissivenessPTSD symptoms
Cohen, Mannarino, & Deblinger, 2008
Praise
Focus on actively praising the childPraise a specific behaviorProvide praise ASAP after behavior occursBe consistentDo not qualify your praiseDo not qualify your praiseProvide praise with same level of intensity as criticismCatch your child doing good!Catch your child doing good!
Cohen, Mannarino, & Deblinger, 2008
Selective Attention
No reaction to certain negative behaviorsDefiant or angry verbalizations to parentNasty facesMocking or mimickingWalk away busy oneself with an activityWalk away, busy oneself with an activityRemain calm , dispassionate
Cohen, Mannarino, & Deblinger, 2008
Time Out
Purpose: To interrupt the child’s negative behaviors and allow him/her to regain controlE l i t hild hExplain to child whyLocation: quiet, least stimulatingDuration: 1 minute per year of ageDuration: 1 minute per year of ageTimer starts when child stops screamingOnce in time out parent should refrain from Once in time out, parent should refrain from comments and maintain calm demeanorBe consistent
Cohen, Mannarino, & Deblinger, 2008
Contingency Reinforcement Programs
Purpose: Decrease unwanted behaviors and increase desired behaviorsS l l b h i Select only one behavior to targetExplain process to childI l hild i d i i b dInvolve child in decisions about rewardsAdd stars and give rewards weekly and consistently
Cohen, Mannarino, & Deblinger, 2008
Behavior Management
Reasonable developmental expectationsLimit‐settingBehavioral interventions for:
AnxietiesSl blSleep problemsAggressive behaviorsSexually inappropriate behaviorsSexually inappropriate behaviors
Cohen, Mannarino, & Deblinger, 2008
Relaxation
Reduce physiologic manifestations of stress and PTSDExplain body responses to stress
Shallow breath, muscle tension, headachesFocused breathing, mindfulness, meditationP i l l tiProgressive muscle relaxationPhysical activity
Cohen, Mannarino, & Deblinger, 2008
Affective Modulation
Feeling IdentificationAccurately identify and express a range of different f lifeelings
Board gamesFeeling brainstormgColor my life or personDo not ask directly about feelings experienced during traumatic eventtraumatic eventEnd on a positive note
Cohen, Mannarino, & Deblinger, 2008
Affective Regulation (Continued)
Positive Self‐TalkFocus on child’s strengthsRemind child to verbalize these
Enhancing Sense of SafetyA k b t hild’ f f t i ht Ask about child’s sense of safety right nowDevelop a safety plan
Cohen, Mannarino, & Deblinger, 2008
Enhancing Problem Solving and Social Skills
Problem‐solvingDescribe the problemIdentify possible solutionsConsider the likely outcomesPi k th l tiPick the solutionEvaluate your choiceSocial SkillsSocial SkillsTaking turnsListening to others
Cohen, Mannarino, & Deblinger, 2008
g
Affect Modulation Example: the TARGET Model
Stress>brain alarm>over or under‐reactivityFREEDOM Steps
F=Focus SOSR=Recognizing triggersE=Emotions (reactive vs. main emotions)E=Evaluating thoughts (reactive vs. main)D Defining your goalsD=Defining your goalsO=Identifying OptionsM=Making a contribution
Cohen, Mannarino, & Deblinger, 2008
M=Making a contribution
Thought Interruption and Positive Imagery
Use when overwhelmed with trauma remindersTemporary measures early in treatmentT h hild t l th i th htTeaches child control over their thoughts
Changing the channelSaying “Go away” or “Snap out of it”Saying Go away or Snap out of itImagining a stop signReplace unwanted thought with a positive one
Cohen, Mannarino, & Deblinger, 2008
Cognitive Processing
Help children and parents understand the cognitive triad between thoughts, feelings, and behaviors.Help children distinguish between thoughts, feelings, and behaviors.H l hild d t i t i Help children and parents view events in more accurate and helpful ways.Encourage parents to assist children in cognitive g p gprocessing of upsetting situations, and to use this in their own everyday lives for affective modulation .
Cohen, Mannarino, & Deblinger, 2008
.
Types of Inaccurate Thoughts
Personal, Pervasive, PermanentAll or nothing AlanAgain and again AgnesCatastrophic CassieNegative NedNegative Ned
Cohen, Mannarino, & Deblinger, 2008