-
8/3/2019 Kraushaar Paper2 Scribd
1/23
1
Title:1
Engaging self-correcting feedback control to increase physical
activity and reduce bodyweight2
and disease risk in overweight sedentary adults.3
4
Running Title: Self-correcting feedback control for weight
loss5
6
Authors:7
Kraushaar Lutz Erwin*, MSc., Department of Public Health
Medicine,8
School of Public Health, University of Bielefeld, POB 100131,
33501 Bielefeld,9
Germany, [email protected]
Krmer Alexander, M.D., Ph.D., Professor and Head, Department of
Public Health Medicine,11
School of Public Health, University of Bielefeld, POB 100131,
33501 Bielefeld,12
Germany13
* Corresponding author14
15
Date: 03/201016
17
This study was supported by Siemens Betriebskrankenkasse (SBK),
Siemensallee 84, 7618718
Karlsruhe, Germany19
-
8/3/2019 Kraushaar Paper2 Scribd
2/23
2
Abstract20
Objective: To investigate whether engaging web-enabled cognitive
feedback control over the21
introduction of leisure time physical activity (LTPA) will yield
adoption of health enhancing LTPA22
volumes among sedentary, overweight adults, and promote
clinically relevant improvements of23
anthropometric, metabolic and fitness-related vital signs.
Design: Longitudinal LTPA intervention24
study, commencing with a minimum weekly requirement of 3x20
minutes of high-intensity interval25
training (HIT), and requirement for web-based self-monitoring
andreporting of LTPA volume and26
body weight. Subjects: 83 overweight, sedentary, otherwise
healthy adults (age 26-68y, BMI 25.1-.27
41.7 kg/m2, 24% female). Measurements: Anthropometric
parameters, body fat (phase sensitive28
multi-frequency BIA), total-to-HDL cholesterol ratio, VO2peak
(cardiopulmonary exercise testing,29
CPET), self-reported time spent for LTPA, frequency and latency
of use of the web-enabled tool.30
Results: At 24-week follow-up, substantial voluntary increase of
time spent for LTPA (mean and31
median of 135 and 170 minutes per week respectively) in the
group of 72% of participants who32
successfully engaged cognitive feedback control (CFG), vs. no
increase in the remaining participants33
who served as the control group (CG). CFG witnessed
significantly improved peak oxygen34
consumption >1 metabolic equivalent (MET) vs. no improvement
in CG. CFG also reduced BMI, body35
weight, body fat and TCH/HDL by 1.6 kg/m2
, 4.8 kg, 3.6 kg and 0.25 respectively in CFG vs. 0.436
kg/m2, 1.4 kg, 1.1 kg and an increase in TCH/HDL ratio (0.16) in
CG. Conclusion: Engaging self-37
correcting feedback via internet-based self-monitoring and
feedback control may be a promising38
strategy for instituting sustainable health enhancing behavior
change in overweight adults, offering the39
possibility of open-ended intervention delivery at low
costs.40
41
Key words: Obesity, Physical Activity, Individual Behavior,
Homeostasis, Feedback42
43
-
8/3/2019 Kraushaar Paper2 Scribd
3/23
3
Background44
Excess body weight causally contributes to the development of
cardiometabolic disease [1]. That45
leaves the question how to institute lasting weight loss and
weight maintenance in individuals whose46
physical activity and dietary habits have promoted the onset of
overweight and obesity. Lifestyle47
interventions, which target participants deficits in LTPA and
their surfeits in caloric intake, may48
perform well in initiating weight loss and improvements of
disease risk. However, an almost complete49
reversal to baseline status within a 3-5 years post-intervention
period has been observed [2, 3], as well50
as a 95% failure rate of dieters attempts at losing weight and
maintaining weight loss in the long term 51
[4]. These data suggest that a sustainable public health
strategy for health behavior change has yet to52
be found. To this end we developed a biobehavioral model with
which to explain the observation of53
runaway weight gain in our society, and from which to formulate
a testable hypothesis for sustainable54
remedial intervention. Since intervention efficiency for public
health is our objective, we desired the55
intervention to allow for optimum reach into the at-risk
population under the given economic, regulatory56
and resource constraints which define the local German health
care system.57
The biobehavioral origin of the obesity epidemic58
The ecological observations guiding the development of our
hypothesis were (a) the absence of59
excess body weight in human societies of hunter/gatherers living
in their natural habitat [5, 6], (b) the60
obligatory physical activity cost for food acquisition in this
habitat [6, 7], and (c) mans progressive61
weight gain secondary to the abolition of obligatory energy
expenditure [7] and the introduction of62
processed foods of high energy density in modern society. We
posit that the latter derails the anabolic63
and catabolic constituents of a negative feedback loop, which
autonomously controls energy64
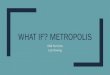
homeostasis. Figure 1 presents our proposed feedback loop model,
of which three essential aspects65
warrant further elaboration. Firstly, the model positions
catabolic foraging and anabolic feeding as the66
inextricable appetitive and consummatory components of ingestive
behavior (AIB & CIB) [8, 9]. Their67
underlying neurohormonal pathways autonomously establish energy
homeostasis through negative68
feedback control [10]. The hormones neuropeptide Y (NPY) and
leptin have emerged as the chief69
stimulator and moderator respectively of an organisms drive to
acquire food [11-14], which has been70
found to operate with remarkable similarity in all vertebrates
and even in some fish [15, 16].71
Secondly, there is dopamine as the neural substance that
actuates the wanting for hedonic72
experiences, which an organism has learned to associate with
certain stimulants [17]. Sweet and fatty73
tastes are such stimulants which fuel mans dopaminergic drive
[18] and consequently his cravings for74
-
8/3/2019 Kraushaar Paper2 Scribd
4/23
4
sweet and fatty foods [19]. The drive to preferentially select
such comestibles and their caloric content75
may have carried a distinct survival value for an organism
subsisting in a habitat which is76
characterized by volatile food supplies and constant demands for
physical activity. In modern human77
society however, the addictive power of typically sugar- and
fat-enriched processed foods conspires78
with the abolished need for physical activity to derail energy
homeostasis and its underlying79
neurohormonal system of negative feedback control.80
A functioning negative feedback control implies that once an
individuals drive to forage is activated,81
and food reward is presented free of the energy cost of
preceding PA, the eventual strengthening of82
the leptin signal, secondary to an accumulation of energy
reserves, would moderate any subsequent83
motivation to forage when the latter is initiated by energy flux
activated NPY signaling. However, at84
least two conditions have been observed which potentially derail
negative feedback control. First,85
there is leptin resistance, a condition frequently encountered
in overweight individuals [20]. Second,86
there is conditioned potentiation of feeding, a variant of
classical conditioning, in which a previously87
unrelated stimulus, when paired with food presentation, arouses
the dopamine driven wanting of food88
when the then conditioned cue and access to food are paired
subsequently [21]. Once stimuli, such as89
time of day, physical location or presence of others have been
conditioned into cues for food intake, a90
dopaminergic drive is engaged to eat in excess of physiological
need.91
In our model, the controlled parameter of negative feedback is
energy adequacy under the given92
environmental constraints, rather than bodyweight, as suggested
by set-point theory [22]. The latter is93
challengeable on observational and evolutionary grounds. Its
prediction of eventual weight stability94
fails to reconcile with the observation of longitudinally
increasing bodyweights of societies and of95
individuals. The ability to cap body weight would have increased
inclusive fitness only if environmental96
conditions had facilitated pathological weight increase to the
point of affecting an individuals chances97
to reproduce and survive. This is hardly reconcilable with our
current understanding of the scarcity and98
volatility of food supplies that has characterized the hominid
environment throughout evolution.99
In defense of the theory, the failure of set-point control has
been blamed on a purely100
cognitive/executive decision-override of homeostatic body weight
control [23], which amounts to101
blaming the overweight individual for his predicament.102
Contrary to this view, our model exonerates the overweight
individual, as it suggests his behavior to be103
driven by evolutionary conditioned neurohormonal mechanisms,
which are autonomous in nature [10]104
and maladapted to the challenges of the modern
environment.105
-
8/3/2019 Kraushaar Paper2 Scribd
5/23
5
In this context, voluntary LTPA offers itself as a cognitively
controllable means to correct the energy106
imbalance and metabolic consequences, which result from the
absence of the obligatory physical107
activity cost of food in the industrialized human society. In
support of this view, LTPA has been108
presented as the critical component of sustained weight loss in
the long-term follow-up of successful109
weight reducers [24, 25]. However, interventions aimed at
increasing LTPA suffer from high attrition110
rates of typically 50% within the first 6 months [26-28]. As an
explanation we offer (a) failure to111
consider participants time constraints, and (b) failure to
engage feedback control. With respect to time112
constraints, lack of time is sedentary individuals most
frequently cited obstacle to the cultivation of a113
regular exercise habit [29-31]. This real or perceived lack of
time emerges relative to current114
recommendations, such as those of the American College of Sports
Medicine [32] or the Institute of115
Medicine [33] who advocate 150-250 minutes per week and 60
minutes per day respectively of health116
enhancing physical activity (HEPA). Failure to overcome the
discrepancy between time required and117
time perceived available for HEPA may inadvertently either
freeze individuals into their sedentary118
habits, or promote recidivism from attempts at adopting
HEPA.119
With respect to cognitive feedback control, its sine qua nonis
self-monitoring, which, when practiced,120
has been found to significantly improve adherence to behavior
change [34].121
The hypothesis122
Taken together, the observations discussed above led to our
hypothesis that engaging self-monitoring-123
based feedback control over an initially minimal but acceptable
LTPA volume will promote the124
voluntary adoption of progressively increasing PA volumes in
previously sedentary overweight adults,125
who self-selected for participation in a weightloss
intervention. We further hypothesized that self-126
monitored and self-reported PA volume will correlate with
objectively measurable vital signs of body127
weight and physical fitness.128
Overcoming the economic obstacles to effective lifestyle
change129
The high costs of evidence-based lifestyle interventions, health
care providers time limitations and a130
lack of reimbursement for health care providers preventive
services constitute substantial barriers to131
the provision of preventive lifestyle change interventions [35].
In Germany, legislation mandates health132
insurers to subsidize, but not fully reimburse, members
voluntary participation in selected exercise133
and diet programs, up to an annual ceiling. However, utilization
of these funds typically is neither134
targeted to the beneficiarys health profile nor is it informed
by medical advice or guidance. This135
strategy renders the preventive efforts efficiency probably
sub-optimal. An internet-based intervention,136
-
8/3/2019 Kraushaar Paper2 Scribd
6/23
6
which is (a) targeted to an individuals health profile, which
(b) automates, standardizes and maintains137
the process of engaging feedback control over HEPA, and which
(c) integrates into the statutory and138
economic landscape of the health care system could constitute an
economically viable and evidence-139
based alternative. To this end we consulted with a medium-sized
statutory health insurance provider140
with the aim of operationalizing the intervention to meet with
the acceptance of the primary cost carrier141
of health care services in Germany.At a 12.- monthly deductible,
to be contributed out-of-pocket by142
the participants, the insurer considered the proposed
intervention to satisfy economic and statutory143
constraints, and subsequently agreed to its realization as a
pilot project within the community setting of144
an industrial estate in the South-Western German city of
Karlsruhe. The 12.- out-of-pocket145
benchmark had emerged from an evaluation of primary care
patients willingness-to-pay for preventive146
services, conducted in a primary-care setting of the close-by
community of Heidelberg [36]. Of the 967147
survey respondents (99.4% response rate) recruited from among 5
primary care practices, 27%, 40%148
and 12% had indicated willingness-to-pay less than 15, 15 -40,
and >40 respectively for149
preventive services.150
Methods151
The intervention was designed as a non-randomized controlled
trial in sedentary and overweight,152
apparently healthy adult men and women. The study protocol
conforms to the ethical guidelines of the153
1975 Declaration of Helsinki. Approval was obtained from the
ethics committee of the state medical154
board of Baden-Wrttemberg. All participants gave written
informed consent prior to enrollment.155
Subjects156
Subjects were recruited from among 200 German holders of a
compulsory health insurance policy who157
had taken up their insurers invitation to participate in a
subsidized fitness and physical activity158
examination. All subjects were employees at a large industrial
estate of a multinational German159
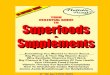
electronics manufacturer. Figure 2 presents an overview of the
recruitment process.160
Inclusion criteria were a self-reported current volume of LTPA
of 1 hour or less per week and a body161
mass index (BMI) in excess of 25 kg/m2.162
Exclusion criteria were known diseases and physical disabilities
preventive of participation in an163
exercise program. All participants were Caucasians of German
extraction.164
Intervention165
The minimum requirement for all participants was an unsupervised
exercise protocol of HIT of thrice166
weekly 20 minutes (either running or cycling) in line with U.S.
government recommendations,167
-
8/3/2019 Kraushaar Paper2 Scribd
7/23
7
published under the Healthy People 2010 initiative, and calling
for moderate-intensity exercise of at168
least 30 minutes on at least 5 days per week, or alternatively,
for 20 minutes high-intensity exercise at169
least thrice weekly [37]. Thrice weekly 15-minute HIT bouts have
shown to yield significant170
improvements of parameters of metabolism and exercise capacity
[38].171
Each 20-minute HIT session was to consist of 4 repeated 60-s
sprints at a heart rate commensurate172
with 85% to 95% of participants individual VO2peak with a 4-min
recovery phase between sprints.173
During recovery, subjects were to continue their mode of
exercise at an intensity level commensurate174
with their anaerobic threshold. Subjects were instructed not to
perform HIT on consecutive days, but175
were encouraged to additionally engage in moderate-intensity
endurance training at 95-115% of their176
individual anaerobic threshold.177
All participants who opted for the use of heart rate monitors
during exercise were given target heart178
rates for the HIT exercises and recommendations for the optimal
heart rates during continuous aerobic179
exercise. All heart rate recommendations were based on the
individuals cardiopulmonary exercise180
test results. Participants who decided against the use of heart
rate monitors were familiarized with the181
use of the 10-point OMNI rating scale of perceived exertion [39]
and instructed to perform the high-182
intensity intervals at an approximate rating of 8 and the
recovery phase at a rating of 5-6. The OMNI183
scale has been validated for use in equivalent populations [40,
41].184
Self-Monitoring185
To facilitate self-monitoring, and the supervision thereof by
the investigator, an electronic lifestyle file186
(ELF) was created into which participants were to report their
actual time spent on exercise and their187
bodyweight. The ELF facilitates a 6-weeks cumulative graphical
display of actual vs. target values.188
Target performance for the initial 6-weeks period was based on
the weekly 60-minutes HIT protocol.189
Upon completion of each 6-weeks period the target for the
following 6 weeks was set to increase by190
10% over the actual volume reported for the preceding 6-week
period. Participants were encouraged191
to log their actual PA performance and their bodyweight on a
daily basis, either by direct access to192
their secured web-page or through an applet installed on their
mobile phone facilitating SMS-based193
reporting of PA and bodyweight.194
Measurements195
Body weight and standing height were measured in light sports
clothing and without shoes to the196
nearest 0.1 kg and 1 cm, using a wall-mounted anthropometer and
a calibrated electronic scale,197
respectively. BMI was calculated as the ratio between weight and
height squared (kg/m2).198
-
8/3/2019 Kraushaar Paper2 Scribd
8/23
8
Body composition was measured using an impedance analyzer device
and software (BIA 2000-S,199
Data Input, Frankfurt, Germany) for tetrapolar bioelectrical
impedance analysis (BIA) measurement of200
resistance (R) and reactance (Xc) at frequencies of 5, 50 and
100 kHz. Measurements were made at201
the right side of the subject between the wrist and ankle while
in a supine position and after having202
rested for 5 minutes. The equipment, analytic algorithms and the
measurement protocol have been203
validated previously in comparable populations [42, 43].204
Exercise testing was performed as cardiopulmonary exercise test
on a cycle ergometer (Customed,205
Germany) using a ramp protocol to exhaustion with the ramp
increment chosen, based on age, weight,206
height and training history, as to reach exhaustion within 8 to
12 minutes [44]. For the first 3 minutes207
the workload was fixed at 5 W.208
The resistance on the cycle ergometer was controlled by the
ergospirometric software (Cortex,209
Leipzig, Germany) to be independent of pedal cadence.210
Spiroergometry was carried out using a breath-by-breath-system
(Cortex MetaLyzer 3B, Leipzig,211
Germany), which has been validated previously [45]. Expired air
was collected continuously using a212
facemask. The system was calibrated prior to each test in
accordance with manufacturers guidelines213
using a 3-L syringe for volume calibration and ambient air
measure for gas calibration.214
During all tests, heart rate was recorded with a wireless chest
strap telemetry system (Polar, Kempele,215
Finland). Simultaneous gas exchange measurements consisted of
minute ventilation (VE), oxygen216
uptake (VO2; electrochemical cell), and carbon dioxide output
(VCO2; infrared analyzer). For217
calculations, data were averaged over every 20 seconds.218
Peak oxygen uptake (VO2peak) was defined as the highest value
for oxygen uptake averaged over 20219
seconds.220
Venous blood was sampled in EDTA tubes in the morning between
07:30 and 08:45 after an overnight221
fast. Total and HDL cholesterol were determined by standard
laboratory methods using certified222
assays in a local clinical laboratory.223
All analyses performed at baseline were repeated at
follow-up.224
Adherence Definition225
Adherence was defined as meeting the minimum criteria of having
recorded a minimum weekly226
duration of endurance exercise (volume aspect of adherence) of
60 minutes (3 x 20 minutes of HIT) or227
more for at least 12 consecutive weeks (duration aspect of
adherence), with the last self-reported login228
not earlier than 1 week (latency aspect of adherence) prior to
the date of final assessment. With229
-
8/3/2019 Kraushaar Paper2 Scribd
9/23
9
physical fitness being the primary and measurable vital sign,
the 12-weeks duration is in keeping with230
published evidence, which suggests that measurable effects
accrue to VO2peak after such durations231
[46], with decay of the effect being observable within 14 days
of discontinuation of the exercise232
regimen [47]. Participants who did not meet the adherence
criteria were considered the control group.233
Statistical Analyses234
Prior to the study, we performed power and sample-size
calculations, with both calculations based on235
a hypothesized ratio between adherent and non-adherent
participants r=3. To achieve a power of236
90%, we needed 50 participants to detect a between-group
difference for VO2peak of 1 MET (3.5237
ml/kg/min) and for BMI of 1 kg/m2. Analyses for differences
between groups at baseline were238
performed using t-tests. Changes from baseline to follow-up were
tested using paired t-test for within-239
group changes, and unpaired t-tests for differences of changes
between groups. Statistical240
significance was accepted at p
-
8/3/2019 Kraushaar Paper2 Scribd
10/23
10
VO2peak of 2.4 ml/kgLBM/min, CFG had significantly increased
VO2peak by 6.2 ml/kgLBM/min, with261
p-value for within- and between-groups of 3, with a significance
for this between-group difference at p
-
8/3/2019 Kraushaar Paper2 Scribd
11/23
11
a web-based self-monitoring tool, to institute physical activity
in previously sedentary and overweight292
adults. The results of this study support the hypothesis that by
engaging self-correcting feedback, with293
weight-loss being its objective, users voluntarily and
significantly increase their physical activity294
volume over an initially prescribed minimum. To start with a
minimum prescription may be an295
important strategy to overcome sedentary individuals perceived
gap between time required and time296
available for HEPA. Engaging a cognitively controlled
self-correcting feedback loop may therefore help297
previously sedentary and overweight adults to voluntarily,
gradually and substantially increase their298
physical activity volume over an initially prescribed minimum,
resulting in significant reductions of body299
weight and associated disease risk. A call has been made very
recently for the EU to develop national300
physical activity recommendations along the new guidelines
formulated by the U.S. American Heart301
Association (AHA) and the American College of Sports Medicine
(ACSM) [54]. These guidelines302
specifically acknowledge the evidence-based need for all healthy
adults aged 18-65 to perform either303
moderate-intensity aerobic exercise for a minimum of 30 min five
times weekly, or 20 min of vigorous304
exercise 3 times weekly or any combination thereof [55]. This
interventions starting point was a305
CPET-based heart rate-controlled exercise recommendation for an
initial 3x20 minutes HIT routine.306
Individualizing an exercise prescription to a participants
personal cardiopulmonary dynamics307
maximizes the training effect. The hoped-for consequence is that
a perceivably improved performance308
powerfully promotes continued adherence.309
Letting participants self-determine their PA volume, given the
initial weekly requirement of 3x20310
minutes of HIT, yielded a substantially larger actually
performed volume of exercise. It is therefore311
tempting to suggest, that it may not so much be participants
fidelity to a pre-conceived one-size-fits-all312
exercise curriculum, which lifestyle change program providers
should be concerned with. Rather313
should we focus on getting people to commit to and commence with
a physical activity habit, which, if314
prescribed individually to yield some quick tangible effect,
will develop its own momentum. It is for315
future research to contrast these two strategies under the a
priorihypothesis of a significant difference316
in outcome.317
In this study, the term adherence does not relate to the volume
or duration of PA, but to the presence318
of a cognitively controlled feedback loop at the end of a
6-months observation period. This constitutes319
a small, but substantially different way of defining adherence,
which emerges from the theory and320
model underlying this intervention strategy. Its latency aspect
differentiates it from adherence321
definitions, which are exclusively based on any combination of
percentages of volume, of duration or322
-
8/3/2019 Kraushaar Paper2 Scribd
12/23
12
of attendance. It provides an answer to the question, what
proportion of study participants currently323
adheres to the PA protocol and has done so for durations and at
PA volumes, which are expected to324
yield tangible health benefits. Hence, the latency aspect is
essential for determining how successful an325
intervention has been at releasing its participants with a
modified health habit. With 72% of the326
participants meeting this criterion, the intervention compares
favorably with the 55% (CI 0.39-0.72)327
adherence rate achieved in a comparable worksite intervention of
a 24-weeks PA program consisting328
of 3 weekly 20-minutes high intensity aerobic workouts in
addition to strength training [56], and with329
the 60% adherence rates typically reported for PA interventions.
This difference in adherence is330
significant, two-tailed, at p(z=2.28)5 years, have found
self-337
monitoring, a high level of PA and a low-calorie-low-fat diet as
the three most important determinants338
of weight loss and maintenance of reduced body weight [25,
57].339
Strengths and Limitations340
One major strength of our study is its simulation of a real-life
implementation, designed to be341
economically acceptable to the provider of statutory health
insurance under which 90% of the resident342
population is covered. Another notable strength is the studys
objective measurement of changes in343
body weight, body composition, TCH/HDL ratio and physical
fitness resulting from an internet-344
delivered intervention which was designed to engage cognitive
feedback control over physical activity345
behavior.346
The primary limitation of our study is that (a) these results
represent initial improvements of weight and347
fitness status, and that (b) the study design, which
necessitated participants out-of-pocket348
contributions with the objective of simulating a future
real-life implementation, prevented us from349
randomizing participants into a control and intervention group.
The resulting selection of non-adherent350
participants as the control group may have led to selection
bias. However, there were no significant351
between-group differences of any of the parameters measured at
baseline. Expressed as Cohens d,352
the differences in parameters at baseline remained at d0.1, with
the exception of age, the difference353
-
8/3/2019 Kraushaar Paper2 Scribd
13/23
13
of which had a Cohens d=0.3. Conventionally, effect sizes are
considered small, medium and354
large fordvalues of 0.2, 0.5 and 0.8 respectively [58]. Also,
self-report of PA is inherently subject to355
bias. Since the self-reporting technique did not enable
participants to differentiate between levels of356
exercise intensity, the calorific equivalent of the reported
exercise volume cannot be determined.357
Hence, no dose-response relationship could be established
between PA volume and outcome. Also,358
subjects were free to record either daily or as and when PA was
performed. Enforcing daily login might359
have reduced the number of subjects who failed to engage a
cognitively controlled feedback loop. In a360
follow-up trial we are encouraging participants to perform daily
monitoring not only of body weight and361
PA but also of dietary intake. We hypothesize that daily
feedback will significantly improve adherence362
and outcome.363
Based on this hypothesis, the ELF is being further developed to
include dietary monitoring and to364
facilitate telemetric monitoring of PA volume and intensity as
well as telemetric monitoring of body365
weight, blood pressure, blood glucose and ECG. We encourage
fellow researchers to avail366
themselves to this tool, and welcome all enquiries related to
academic research.367
Conclusion368
This study demonstrates that a web-enabled engagement of
cognitive feedback control enables369
sedentary and overweight individuals to voluntarily increase
LTPA to yield clinically relevant370
improvements of anthropometric, metabolic and fitness related
vital signs. The internet-enabled371
implementation provides for a low-cost open-ended intervention
delivery to large at-risk groups,372
possibly facilitating sustainable improvements of health
behaviors. Follow-up research should373
elucidate the determinants of sustainability and efficiency
within the statutory and economic374
constraints of the given health care system.375
376
-
8/3/2019 Kraushaar Paper2 Scribd
14/23
14
377
Contributors378
L.E.K. contributed to the design of the study, collection and
assembly of the data, analysis and379
interpretation of data and drafting the article. A.K. took part
in the interpretation of data and drafting of380
the article. All authors approved the final manuscript. L.E.K.
accepts full responsibility for conducting381
the study.382
383
Funding384
The study was supported by Siemens Betriebskrankenkasse
(SBK).385
386
Acknowledgement387
We thank all participants who took part in this study.388
389
Conflict of Interest390
All authors declared to have no conflict of interest.391
-
8/3/2019 Kraushaar Paper2 Scribd
15/23
15
392
References393
1. Lavie, C.J., R.V. Milani, and H.O. Ventura, Obesity and
Cardiovascular Disease: Risk Factor,394
Paradox, and Impact of Weight Loss. J Am Coll Cardiol, 2009.
53(21): p. 1925-1932.395
2. Miller, W.C., How effective are traditional dietary and
exercise interventions for weight loss?396
Med Sci Sports Exerc, 1999. 31(8): p. 1129-34.397
3. Wing, R.R., et al., Behavioral science research in diabetes:
lifestyle changes related to398
obesity, eating behavior, and physical activity. Diabetes Care,
2001. 24(1): p. 117-23.399
4. Crawford, D., R.W. Jeffery, and S.A. French, Can anyone
successfully control their weight?400
Findings of a three year community-based study of men and women.
Int J Obes Relat Metab401
Disord, 2000. 24(9): p. 1107-10.402
5. O'Dea, K., CARDIOVASCULAR DISEASE RISK FACTORS IN AUSTRALIAN
ABORIGINES.403
Clinical and Experimental Pharmacology and Physiology, 1991.
18(2): p. 85-88.404
6. Eaton, S.B., S.B. Eaton, 3rd, and M.J. Konner, Paleolithic
nutrition revisited: a twelve-year405
retrospective on its nature and implications. Eur J Clin Nutr,
1997. 51(4): p. 207-16.406
7. Booth, F.W., et al., Waging war on modern chronic diseases:
primary prevention through407
exercise biology. J Appl Physiol, 2000. 88(2): p.
774-787.408
8. Day, D.E., E. Keen-Rhinehart, and T.J. Bartness, Role of NPY
and its receptor subtypes in409
foraging, food hoarding, and food intake by Siberian hamsters.
Am J Physiol Regul Integr410
Comp Physiol, 2005. 289(1): p. R29-36.411
9. Baird, J.P., N.E. Gray, and S.G. Fischer, Effects of
neuropeptide Y on feeding microstructure:412
dissociation of appetitive and consummatory actions. Behav
Neurosci, 2006. 120(4): p. 937-413
51.414
10. Qian, G. and L.H. Tamas, Neuronal control of energy
homeostasis. FEBS letters, 2008.415
582(1): p. 132-141.416
11. Grill, H.J. and J.M. Kaplan, The neuroanatomical axis for
control of energy balance. Front417
Neuroendocrinol, 2002. 23(1): p. 2-40.418
12. Grill, H.J. and J.M. Kaplan, Interoceptive and integrative
contributions of forebrain and419
brainstem to energy balance control. Int J Obes Relat Metab
Disord, 2001. 25 Suppl 5: p.420
S73-7.421
-
8/3/2019 Kraushaar Paper2 Scribd
16/23
16
13. Kalra, S.P., et al., Interacting Appetite-Regulating
Pathways in the Hypothalamic Regulation of422
Body Weight. Endocr Rev, 1999. 20(1): p. 68-100.423
14. Ammar, A.A., et al., NPY-leptin: opposing effects on
appetitive and consummatory ingestive424
behavior and sexual behavior. Am J Physiol Regul Integr Comp
Physiol, 2000. 278(6): p.425
R1627-33.426
15. Larhammar, D. and E. Salaneck, Molecular evolution of NPY
receptor subtypes.427
Neuropeptides, 2004. 38(4): p. 141-51.428
16. Cerda-Reverter, J.M., et al., Molecular evolution of the
neuropeptide Y (NPY) family of429
peptides: cloning of three NPY-related peptides from the sea
bass (Dicentrarchus labrax). 430
Regul Pept, 2000. 95(1-3): p. 25-34.431
17. Robinson, T.E. and K.C. Berridge, The neural basis of drug
craving: an incentive-sensitization432
theory of addiction. Brain Res Brain Res Rev, 1993. 18(3): p.
247-91.433
18. Berridge, K.C., Food reward: brain substrates of wanting and
liking. Neurosci Biobehav Rev,434
1996. 20(1): p. 1-25.435
19. Levine, A.S., C.M. Kotz, and B.A. Gosnell, Sugars and Fats:
The Neurobiology of Preference.436
J. Nutr., 2003. 133(3): p. 831S-834.437
20. Scarpace, P.J. and Y. Zhang, LEPTIN RESISTANCE: A
PREDIPOSING FACTOR FOR DIET-438
INDUCED OBESITY. Am J Physiol Regul Integr Comp Physiol, 2008:
p. 90669.2008.439
21. Seymour, B., Carry on Eating: Neural Pathways Mediating
Conditioned Potentiation of440
Feeding. J. Neurosci., 2006. 26(4): p. 1061-1062.441
22. Harris, R.B., Role of set-point theory in regulation of body
weight. FASEB J, 1990. 4(15): p.442
3310-8.443
23. Berthoud, H.R., Multiple neural systems controlling food
intake and body weight. Neurosci444
Biobehav Rev, 2002. 26(4): p. 393-428.445
24. Tate, D.F., et al., Long-term weight losses associated with
prescription of higher physical446
activity goals. Are higher levels of physical activity
protective against weight regain?Am J Clin447
Nutr, 2007. 85(4): p. 954-959.448
25. Wing, R.R. and S. Phelan, Long-term weight loss maintenance.
Am J Clin Nutr, 2005. 82(1):449
p. 222S-225.450
26. Robison, J.I. and M.A. Rogers, Adherence to exercise
programmes. Recommendations.451
Sports Med, 1994. 17(1): p. 39-52.452
-
8/3/2019 Kraushaar Paper2 Scribd
17/23
17
27. O'Neil, H.A. and S.N. Blair, Enhancing adherence in clinical
exercise trials. Quest, 2001. 53: p.453
310-317.454
28. Graffagnino, C.L., et al., Effect of a community-based
weight management program on weight455
loss and cardiovascular disease risk factors. Obesity (Silver
Spring), 2006. 14(2): p. 280-8.456
29. Courneya, K.S., et al., A longitudinal study of exercise
barriers in colorectal cancer survivors457
participating in a randomized controlled trial. Ann Behav Med,
2005. 29(2): p. 147-53.458
30. Ziebland, S., et al., Lack of willpower or lack of
wherewithal? "Internal" and "external" barriers459
to changing diet and exercise in a three year follow-up of
participants in a health check. Soc460
Sci Med, 1998. 46(4-5): p. 461-5.461
31. El Ansari, W. and G. Lovell, Barriers to exercise in younger
and older non-exercising adult462
women: a cross sectional study in London, United Kingdom. Int J
Environ Res Public Health,463
2009. 6(4): p. 1443-55.464
32. Donnelly, J.E., et al., American College of Sports Medicine
Position Stand. Appropriate465
physical activity intervention strategies for weight loss and
prevention of weight regain for466
adults. Med Sci Sports Exerc, 2009. 41(2): p. 459-71.467
33. Brooks, G.A., et al., Chronicle of the Institute of Medicine
physical activity recommendation:468
how a physical activity recommendation came to be among dietary
recommendations. Am J469
Clin Nutr, 2004. 79(5): p. 921S-930.470
34. Stevens, V., Learning habits and skills, in The ABC of
Behavior Change, J. Kerr, R. Weitkunat,471
and M. Moretti, Editors. 2005, Elsevier: Edinburgh.472
35. Whitlock, E.P., et al., Evaluating primary care behavioral
counseling interventions: an473
evidence-based approach. Am J Prev Med, 2002. 22(4): p.
267-84.474
36. Wiesemann, A., et al., Patient willingness to pay for
preventive measures in primary care: a475
study of five GPs in a German community. Soz Praventivmed, 2004.
49(4): p. 254-60.476
37. US Department of Health and Human Services, Objectives 22-2
and 22-3. In: Healthy people477
2010 (conference ed, in 2 vols), US Department of Health and
Human Services: Washington,478
DC.479
38. Babraj J, et al., Extremely short duration high intensity
training substantially improves insulin480
action in young sedentary malesBMC Endocrine Disorders, 2009.
9(3).481
39. Robertson, R.J., Perceived Exertion for Practitioners.
Rating Effort With the OMNI Picture482
System. 2004, Champaign, Ill.: Human Kinetics.483
-
8/3/2019 Kraushaar Paper2 Scribd
18/23
18
40. Utter, A.C., et al., Validation of the Adult OMNI Scale of
perceived exertion for walking/running484
exercise. Med Sci Sports Exerc, 2004. 36(10): p. 1776-80.485
41. Robertson, R.J., et al., Concurrent validation of the OMNI
perceived exertion scale for486
resistance exercise. Med Sci Sports Exerc, 2003. 35(2): p.
333-41.487
42. Bosy-Westphal, A., et al., Phase Angle From Bioelectrical
Impedance Analysis: Population488
Reference Values by Age, Sex, and Body Mass Index. JPEN J
Parenter Enteral Nutr, 2006.489
30(4): p. 309-316.490
43. Bosy-Westphal, A., et al., Patterns of bioelectrical
impedance vector distribution by body mass491
index and age: implications for body-composition analysis. Am J
Clin Nutr, 2005. 82(1): p. 60-492
68.493
44. Rolf F. Kroidl, S. Schwarz, and B. Lehnigk, Technische und
formale Grundlagen, in Kursbuch494
Spiroergometrie. 2007, Thieme: Stuttgart. p. 16.495
45. Meyer, T., et al., Reliability of gas exchange measurements
from two different spiroergometry496
systems. Int J Sports Med, 2001. 22(8): p. 593-7.497
46. Miyaki, A., et al., Effect of habitual aerobic exercise on
body weight and arterial function in498
overweight and obese men. Am J Cardiol, 2009. 104(6): p.
823-8.499
47. Solomon, T.P.J., et al., Effects of exercise training and
diet on lipid kinetics during free fatty500
acid-induced insulin resistance in older obese humans with
impaired glucose tolerance. Am J501
Physiol Endocrinol Metab, 2009. 297(2): p. E552-559.502
48. Laukkanen, J.A., et al., The predictive value of
cardiorespiratory fitness for cardiovascular503
events in men with various risk profiles: a prospective
population-based cohort study. Eur504
Heart J, 2004. 25(16): p. 1428-37.505
49. Franklin, B.A. and D.P. Swain, New insights on the threshold
intensity for improving506
cardiorespiratory fitness. Prev Cardiol, 2003. 6(3): p.
118-21.507
50. Varady, K., et al., Degree of weight loss required to
improve adipokine concentrations and508
decrease fat cell size in severely obese women. Metabolism,
2009.509
51. Anderson, J.W., et al., Long-term weight-loss maintenance: a
meta-analysis of US studies.510
Am J Clin Nutr, 2001. 74(5): p. 579-84.511
52. Festa, A., et al., The relation of body fat mass and
distribution to markers of chronic512
inflammation. Int J Obes Relat Metab Disord, 2001. 25(10): p.
1407-15.513
-
8/3/2019 Kraushaar Paper2 Scribd
19/23
19
53. Snijder, M.B., et al., What aspects of body fat are
particularly hazardous and how do we514
measure them?Int. J. Epidemiol., 2006. 35(1): p. 83-92.515
54. Oja, P., et al., Physical activity recommendations for
health: what should Europe do?BMC516
Public Health, 2010. 10(1): p. 10.517
55. Haskell, W.L., et al., Physical Activity and Public Health.
Updated Recommendation for Adults518
From the American College of Sports Medicine and the American
Heart Association. 519
Circulation, 2007: p. CIRCULATIONAHA.107.185649.520
56. Atlantis, E., et al., Worksite intervention effects on
physical health: a randomized controlled521
trial. Health Promot Int, 2006. 21(3): p. 191-200.522
57. Wing, R.R. and J.O. Hill, SUCCESSFUL WEIGHT LOSS
MAINTENANCE. Annual Review of523
Nutrition, 2001. 21(1): p. 323-341.524
58. Cohen, J., Statistical power analysis for the behavioral
sciences. 2nd ed. 1988, New York ::525
Academic Press.526
527528
529
-
8/3/2019 Kraushaar Paper2 Scribd
20/23
20
Table 1:Physiological and Anthropometric Characteristics of the
Participants530
Baseline ChangeMean SD Mean 95% CI
Age1 (years)non-adherent (N=22) 48 8 - -
adherent (N=60) 51 9 - -
Gender1 (% female)non-adherent (N=22) 23 - -
adherent (N=60) 25 - -
VO2peak1 per kg body weight(ml/kg/min)
non-adherent (N=22) 32.2 8.01 -0.59 (-0.36 to +1.54)adherent
(N=60) 32.3 8.10 +3.732; 4 (+2.71 to +4.74)
VO2peak1 per kg lean body mass(ml/kg/min)
non-adherent (N=22) 84.6 14.2 -2.4 (-5.0 to +0.3)adherent (N=60)
86.3 16.6 +6.22; 4 (+3.8 to +8.5)
TCH/HDL1non-adherent (N=22) 4.10 1.12 +0.16 (-0.13 to +0.46)
adherent (N=58) 4.42 1.06 -0.252;3 (-0.38 to -0.11)
BMI1 (kg/m2)non-adherent (N=22) 29.7 3.7 -0.4 (0 to -0.8)
adherent (N=60) 29.8 3.5 -1.62;4 (-1.1 to -2.0)
Body Weight1 (kg)non-adherent (N=22) 92.6 13.1 -1.42 (-0.1 to
-1.6)
adherent (N=60) 91.6 13.2 -4.82; 4 (-3.5 to -6.2)
Body Fat1 (kg)non-adherent (N=22) 27.5 9.0 -1.12 (-0.1 to
-2.0)
adherent (N=60) 27.5 8.4 -3.62; 4 (-2.6 to -4.7)
Abbreviations: VO2peak = Peak Oxygen Consumption; TCH = total
cholesterol; HDL = high-density lipoprotein cholesterol531
Data are mean SD unless otherwise specified.532
1: p>0.05 for between-group difference at baseline; 2:
significant difference from baseline to follow-up at p
-
8/3/2019 Kraushaar Paper2 Scribd
21/23
21
537
538
Fig.1. Negative Feedback Loop of Energy Homeostasis539
NPY = Neuropeptide Y540
541
542
-
8/3/2019 Kraushaar Paper2 Scribd
22/23
22
543
Fig. 2. Flowchart Recruitment544
545
-
8/3/2019 Kraushaar Paper2 Scribd
23/23
546
Fig. 3. Changes of vital parameters at 24-weeks follow-up.
P-values centered in each bar refer to547
within-group changes from baseline to follow-up. P-values
between the bars indicate significant548
between-group differences.549
550















![Scribd File [ D ]](https://img.pdfslide.us/doc/110x75/5695d43c1a28ab9b02a0c478/scribd-file-d-.jpg)