Embed Size (px)
Citation preview



Knowledge of the patient’s ability to take in oxygen and get rid of carbon dioxide is an important factor in patient care. • Some of the tests involved are done at the
bedside, others require that blood or urine samples be taken to a laboratory, while in other cases, the patient will have to go to a pulmonary laboratory for tests.

In every case. we are concerned with the following questions:
• Can the patient inhale and exhale a sufficient quantity of air at the proper rate?
• Are the gases—i.e.. oxygen (O2) and carbon dioxide (CO2)—moving across the lung membranes at the proper rate?
• Is the proper balance of O2 and CO2 being maintained in the blood?

The data required to answer these questions are obtained by pulmonary function testing and blood gas analyses.

PULMONARY FUNCTION TESTING

Lung Capacities and Volumes
If the lungs are expanded to their maximum volume, we refer to the volume involved as the total lung capacity, or TLC.
If the patient is asked to empty the lungs as much as possible, the remaining volume is called the residual volume (RV). • The difference between the TLC and the RV is called
the vital capacity (V C).

These volumes and some typical numerical values are shown in the figure.

The measurement of these volumes is of interest as a determinant of patient condition. • Note that normal breathing does not involve
maximum lung effort. • The so-called resting tidal volume (RTV) is
therefore used to measure the flow of air in and out of the lung under “resting conditions.”

The tidal volume is usually taken as a more “normaI” indication of the patient’s ability to breathe.

Measurement of Rate of Respiration
The preceding type of information is of interest in determining the patient’s lung volume and the ability of the chest muscles to expand and compress the lungs. • However, it provides no data on the rate at
which the patient can breathe, or on the amount of oxygen that actually passes from the lungs into the blood.

The rate at which the patient can breathe can be measured by a number of tests, one of which is called the forced vital capacity or FVC test. • The patient takes a deep breath and blows it
out as rapidly as possible. • The quantity of air expired in some given length of
time (say, 10 seconds) can be used to evaluate the degree of restriction or obstruction of lung function.

Restriction refers to the result of any interference with the bellows action of the lung itself, e.g., by fluid accumulation or fibrosis; • Obstruction in the passages leading to the
lungs. • If. there is a question about whether either or both
effects are present, the test is repeated after the administration of a bronchodilating agent.

The measurement of the impedance of the chest by means of attached electrodes is sometimes used in the determination of the rate of respiration.• This method is also used to determine the
amount of chest expansion.• Some of the older systems used devices that went
around the chest at the pressure of expansion or contraction would be registered via a pressure gauge or mercury manometer.

More commonly, the heater-thermistor system is used in determination of respiration rate.• A number of other related tests are used to
determine the rate at which patient can inspire air.

The major matter of interest is the determination of the problem is, i.e., • Whether it is a
• restriction,
• obstruction, or
• both.

Some specific tests and the acronyms used to designate them are:
Description of Test Name of Test Acronym
Largest volume measured on complete expiration after the deepest inspiration without forced or rapid effort.
Vital capacity VC
Vital capacity performed with expiration as forceful and rapid as possible
Forced vital capacity FVC
Volume of gas exhaled over a given time interval during the performance of forced vital capacity test
Forced expiratory volume (qualified by subscript indicating the time interval in seconds; e.g. 10 indicates an interval of 10 seconds)
FEVt
FEV10
FEV expressed as a percentage of the forced vital capacity.
Percentage expired (in t seconds) FEV
Average rate of flow for a specified portion of the forced expiratory volume test (usually between 200 and 1200 ml)
Forced expiratory flow FEF
Average rate of flow during the middle half of the forced expiratory volume test
Forced midexpiratory flow FEF
Volume of air that a subject can breathe with voluntary maximal effort for a given time.
Maximal voluntary ventilation MVV

Other Pulmonary Functions The term “volume” is used for a paramrter that
is measured as a function of time, whereas the term “capacity” refers to a measurement that does not involve time. • For example, the vital capacity is the largest volume
measured on complete expiration after complete inhalation, regardless of how long these take; thus, no time parameter is involved.
• The forced expiratory volume, on the other hand, is the total volume of air the patient expires in some fixed period of time, e.g., 10 seconds; the time factor is very important for FEV evaluations.

Another determination of importance is that of airway resistance, which is the ratio of pressure to the rate of air flow. • You can think of this flow (current) induced by
a pressure (voltage) through a resistance R (Ohm‘s law again).

Lung compliance is a measure of the change in lung as a function of a change in lung pressure. • Poor lung compliance is a sign of the
condition known as “stiff lung.”

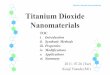
The Spirometer The apparatus most often used for pulmonary
tests is the water spirometer consists of a cone or bell that is designed to ride up and down in a cylinder of about 10cm diameter. • The bell is counterweighted to keep the pressure
inside the cylinder at atmospheric level, the water provides a seal, and the bell moves up and down in response to the patient’s inhalation and expiration. • The vertical motion of the bell is recorded on a moving
drum that is covered with calibrated chart paper. The rotation of the drum provides a time scale, and the resultant chart is called a spirogram

VL
TL
PA
Other signalprocessing
Strip-chartrecorder
Thermometer forspirometer gastemperature
One-wayvalves
Water seal
Bell
Uabs
Soda-limecanister
Pulmonarysystem
Spirometersystem
Mouthpiece
QAWO
Bloodflow
Kymograph
Counterweight
Rotationaldisplacementsensor
PS VS
TS
FS x
FA x
Ubs
A typical spirometer is shown in the figure.

The water spirometer can serve as a good example of the impedance concept. • The tube leading from the patient’s mouth to the
spirometer is a source of resistance, and the spirometer itself consists of a volume that must expand to contain the expired air.
• If the resistance of the tube is toohigh or if there are leaks, the output impedance of the source—i.e., that of the patient plus the tube—will be too high.

The total amount of air in the spirometer will be less than it should be, and the time required for the patient to exhale will be much too long (it may be considered equivalent to pumping up a tire with a pump that has a small and leaky hose). • If the patient’s respiratory system has high airway
resistance, this will raise the output impedance of the source;
• this will appear as a deviation from the normal FEV1 values and as such is valuable for diagnosis.

The point here is that any leaks in the hose or in the patient’s mouth fitting may show up as a clinical problem on the spirogram and lead to a false diagnosis.

The water spirometer is a bulky instrument that is not well suited for in-the-bed measurements. • For such applications or for mass screening tests, it is
common to employ the waterless spirometer.
• This unit is held in the patient’s mouth, and, as inhalation and exhalation occur, the time and rate of air flow are measured by one of a variety of flowmeters (the heated thermistor is one such device).

The rate of flow (liters per minute), multiplied by the time during which air flow occurs, yields the volume (liters).

Airway resistance has been noted as a cause of reduced flow during FEV measurements. • To separate this effect from any problem that
might exist in the lungs themselves, it is common practice to measure both the rate of flow with a spirometer and the intraalveolar pressure in a body plethysmograph at the same time.

A high alveolar pressure in conjuction with a reduced flow would be a sign of excessive airway resistance. • The body plethysmograph is used for a
number of other tests, including those for lung compliance and airway resistance, but the details of its operation are best left to specialized books on respiratory testing.

Oxygen-Carbon Dioxide Exchange
Another test of respiratory function is the measurement of the ability of the lungs to pass oxygen (O2) and carbon dioxide (CO2).
• In one such test, the patient breathes a mixture of air and carbon monoxide (CO).
• Carbon monoxide is used because it passes easily through the lung membrane and because no normal reserve of CO exists in the body to interfere with the measurements.
• The CO level is not high enough to cause any patient injury.

The CO normally passes very rapidly through the lungs and is absorbed by the blood. • In the test, the level of CO in the exhaled air is
measured by the respiratory technician and compared with a standard value. • If the exhaled air is high in CO, the patient’s ability
to exchange gases—including O2 and CO2—is impaired.

Helium Washout Test
A test of the physical condition of the lungs involves having the patient breathe a mixture of air and helium until an equilibrium mixture of helium has been distributed to all areas of the patient’s lungs. • Helium does not pass through lung tissue,
and the only loss of this gas will occur by expiration.

After the equilibration period, the flow of helium is cut off, and the patient breathes pure air. • During this period, the expired air is analyzed
for helium, and the rate at which the helium is “washed out” is determined.

If the patient requires an excessively long time to wash out the helium, this is taken as a sign that certain areas of the lung are open but inactive, in the sense that no expansion or contraction of these portions occurs during breathing. • This is often seen in emphysema, where the
enlarged areas are totally ineffective for gas exchange.

If the physician suspects that a problem is specific to only one lung, he may ask for a bronchospirometric test. • This involves passing a doublelumen catheter into the
trachea.
• One catheter tip is passed into each of the bronchi. and a balloon at the end of the catheter is inflated to insure that all the air entering or leaving the lung passes through the catheter.
• Under these conditions, the gas flow, composition. and pressure can be measured for each of the lungs.

DISTRIBUTION OF PULMONARY BLOOD FLOW
The test involves the injection of a radioactive substance into the blood vessels leading to the pulmonary area.• Postinjection scanning with radiation
detectors provides a measure the blood flow to the lungs.

BLOOD GAS AND pH ANALYSIS
The gas content and the pH of the blood are often the earliest indicators of a change in patient condition. • At one time, it was necessary actually to take blood
samples to the laboratory for blood gas and pH testing.
• The laboratory measurement of blood gases and pH involves the use of special electrodes that provide an electrical output proportional to the fraction of a particular chemical species (hydrogen, carbon dioxide, oxygen, or whatever) in the blood.

Blood Oxygen Measurements
Arterial blood is almost always taken for oxygen analysis, and it is vital that the sample get to the laboratory before the oxygen level changes. • If the patient is receiving oxygen therapy, this
should be noted, because it will affect the physician’s evaluation of the data on blood oxygen level.

ARTERIAL O2 TENSION (PO2) AND
ARTERIAL SATURATION (SO2)
• The PO2 is a measure of the actual partial
pressure of oxygen in the blood; its normal range is around 95 to 100 mm Hg. • When chronic pulmonary disease is present, the
PO2 level can fall as low as 70 to 75 mm Hg without
evidence of hypoxia.

Arterial saturation SO2, is the ratio of the
actual oxygen content to the content that would exist if the blood were saturated with oxygen. • Blood saturation will only occur if the patient
breathes 100% O2 for some length of time.

The change in arterial O2 content when the patient breathes a gas mixture that is high in O2 is often used as a measure of the patient’s ability to pass O2 across the pulmonary membrane.
• The correlation of PO2 and SO2
test data with
other respiratory function data provides information for diagnostic purposes.

OXYGEN MEASUREMENT TECHNIQUES
In some cases, special electrodes designed to respond to a specific dissolved gas like O2 have been inserted in the arteries for continuous PO2
measurements. • Their use is not yet as common as either the
method of taking laboratory samples or the ear Oximeter.

A major use of the Oximeter is in monitoring infants who were born prematurely or have respiratory problems.• For the continuous bedside measurement of
the blood oxygen or PO2 level, it is possible to
use the ear-probe Oximeter, which determines the amount of O2 combined as oxyhemoglobin.

In this device, a quartz-iodine lamp is used to generate white light. • The light is split into eight wavelengths in the
red and infrared regions. • This energy is passed through the pinna, or top
part of the ear, and the absorption of light at each wavelength is measured.

The absorption of light by hemoglobin increases with wavelength (going from the red to the infrared), while the absorption of oxyhemoglobin decreases in the same optical region.

The Oximeter can determine the PO2 in
the blood to within about ± 1% if the patient is in the normal range (95-100mm Hg). • In the range of 70-75 mm Hg, its accuracy
falls to about 3%, but this is usually quite adequate.

Instrument response is almost instantaneous, and the device can be left in place for long periods of time. • It is important that patient’s blood circulation
be adequate; • If the blood flow to the ear is impaired, the device
cannot be used.
• In this case, laboratory analysis techniques will be required.

BLOOD CARBON DIOXIDE MEASUREMENTS
The employment of special indwelling CO2 sensors has been investigated, but they are not yet in general use. • Laboratory tests on blood samples include the
measurement of arterial CO2 tension (PCO2) and the
CO2 combining power of plasma or serum.
• This latter test is usually performed on venous blood (which is why in blood sampling, both arterial and venous blood may have to be taken), and it serves as a measure of the patient’s “alkali reserve.”

pH Measurement
Once again, the blood pH can be measured by indwelling catheters, but it is usually done in the laboratory. • Respiratory acidosis, or excess acid in the
blood (low pH), may be caused by a high level of CO2 in the blood due to inadequate alveolar ventilation.

Metabolic acidosis occurs when there is excess production of organic acids or a sugar imbalance, as in diabetes. • In metabolic acidosis, the body will attempt to
compensate by means of hyperventilation to remove CO2 from the blood.
• Compensation may lower the blood acid level, but it does not solve the primary problem: the excess of nonvolatile, organic acids.

In many cases, this test is a reliable indicator of metabolic disturbances.

The measurement of pH is a good example of a simple idea that requires a good deal of electronics before it can be used in practice. • It depends upon the fact that blood and in fact
all body solutions contain ions (charged atoms of hydrogen, calcium, carbonate, etc.).

If two electrodes made of two different materials are inserted into the solution one electrode will become positive with respect to the other. • The ions respond to the resultant electrostatic
field, the positive ions move to the negative electrode and the negative ions to the positive electrode.

The resultant voltages are characteristic of the ions involved and their number; • If we measure the hydrogen ions we call the
result pH.
• If we measure the oxygen ions we call the result PO2
and so on.

All of this sounds easy but in practice we note first that these electrode systems have a very high output impedance. • This means we have to measure their
voltages with a meter having an even higher input impedance.

Another factor here is that different electrodes are used to measure different ions:• The pH electrode sees only hydrogen ions,
• the oxygen electrode is sensitive to oxygen ions. • All of these gadgets are subject to damage and
“blinding by fibrin or other deposited material.

The instructions for cleaning, storage, and operation should be carefully observed. • Good data require good instruments.

Respiratory alkalosis, or a high level of alkali in the blood (high pH), may be due to hyperventilation that produces a deficit of CO2.
• This is usually compensated by the kidney, which releases bicarbonate to the blood to yield more CO2.

Metabolic alkalosis may be due to excessive intake of alkaline salts, a deficit of potassium, or a loss of organic acids. • In this case, the patient will be encouraged to
hypoventilate and retain CO2 to restore the acid-base balance.

CORRELATION OF PULMONARY FUNCTION TESTS WITH RESPIRATORY ABNORMALITIES
A plot of maximum exhaled volume versus time will indicate a reduced vital capacity in patients with “stiff lung.” • Airway obstruction does not reduce the vital
capacity, but it will extend the time required for complete exhalation.

Some diseases, e.g., atrophic emphysema, may increase lung compliance and produce an excessively large volumetric flow during exhalation.• “Hypertrophic emphysema,” or chronic
obstructive pulmonary edema, reduces the contractability of the lungs so that they become permanentIy enlarged; • In this case, a reduced volumetric flow is observed.

Atelectasis, which is lung collapse in adults or incomplete lung expansion at birth, is manifested by a decrease in total lung capacity. • In some cases, the lung capacity will increase
if the lungs are momentarily inflated by the application of a positive pressure. i.e., a pressure above atmospheric pressure.

A decrease in lung diffusion, as manifested by impaired gas exchange, may indicate a collagen disease or the blocking of pulmonary capillaries by emboli.

In many cases, a patient will have more than one respiratory problem, which will make the diagnosis more complicated.