Embed Size (px)
Citation preview

KNOWLEDGE OF MICROTRENDS: THE GLOBAL EXAMPLE OF MDR-TB
SALMAAN KESHAVJEE, MD, PHD
HARVARD MEDICAL SCHOOL BRIGHAM AND WOMEN’S HOSPITAL
PARTNERS IN HEALTH
SW 25October 1, 2009

Anthropology of policy (1)
• An area of anthropology that analyzes how policies construct subjects of power, transforms norms, institutions, and ideologies.[1]
Why study policies?
• Policies are interesting in the context of international health because:– They are viewed as “pragmatic” approaches to certain problems– They are treated as if they were ideologically neutral
• They are instruments of international governance– “Policy” is actually, in many ways, a political technology: political
discourse is taken and recast in the seemingly neutral language of science– What appears “pragmatic” – rational, collective, universal – is actually
something highly subjective, ideological and sometimes irrational.
[1] Shore, Chris and Wright, Susan. “Policy: A new field of anthropology”, in Anthropology of Policy: Critical perspectives on governance and power, edited by Cris Shore and Susan Wright, Routledge: London and New York, 1997, pp. 3-39.

Anthropology of policy (2)
• They are created by bureaucracies.
• The object of policy is constructed in a particular way: they are never seen. They become the subject of bio-power (of control)
• Policies are what Mauss (1954) referred to as a “total social phenomenon” because they have economic, legal, cultural and moral implications.
• Policies are where bio-power and the iron-cage meet

Tuberculosis Facts• Caused by Mycobacterium
tuberculosis
• One third of the world’s population infected
• Kills approximately 1.8 million people each year
• Poor and/or immuno-compromised at considerable risk of disease
• TB is acquired when a person with active untreated TB spreads the bacteria through coughing or sneezing.
• Infection usually occurs in individuals who have close, prolonged exposure to someone with the disease.
• Most people who are infected with TB do not get TB disease.
• Increasing number of resistant strains
• ~500,000 cases of MDR-TB each year

CASE EXAMPLE: RUSSIAN PRISONER

Patient History
• Patient GV
• Born June 27, 1975
• First diagnosed with TB in February 1997 in a Russian prison during a routine x-ray
• His weight was 59 kg with a height of 178 cm


Patient GV: Admission X-ray

• Drug sensitivity testing (DST) showed patient was susceptible to all first-line drugs
• Per local practice, GV was treated with first-line drugs for 11 months from February until November 1997
Patient History Continued…
First-line
•INH (H)
•RIF (R)
•EMB (E)
•PZA (Z)
NINE MONTHS
NINE MONTHS
TWO MONTHS
TWO MONTHS
2HREZ / 9HR

• Patient GV was initially feeling fine after completing treatment and was released from prison
• 3 months later he started having fevers, chills and cough
• He noticed blood in his sputum
• Visited the TB physician in February 1998
• His weight had dropped to 53 kg (from 59 kg at start)
Patient History Continued…

Patient GV: X-ray February 1998

• Drug sensitivity testing from March 1998 (received in May 1998) showed that he was resistant to H and R
Patient History Continued…
• Following international guidelines, GV was treated with WHO category II treatment (2HREZS / 1HREZ / 5HRE) starting in February 1998
First-line
•INH (H)
•RIF (R)
•EMB (E)
•PZA (Z)
THREE MONTHS
EIGHT MONTHS
EIGHT MONTHS
EIGHT MONTHS
2HREZS / 1HREZ / 5HR•SM
Injectable
TWO MONTHS
+

• In May 1998, GV was found to still be sputum smear positive
• He continued to have fever and night sweats
• His weight dropped to 49 kg (from 59 kg at start of treatment)
• The TB services ran out of streptomycin and decided to treat him with kanamycin (another aminoglycoside) instead
• He was started on a locally-modified regimen of 3HREZK / 6HREZ in May 1998
Patient History Continued…

• GV continued to have fevers, night sweats, and weight loss over the next six months; his weight dropped to 43 kg (from 59 kg)
• A repeat DST in December of 1998 showed a TB strain resistant to H-R-E-Z-SM-KM
Patient History Continued…
•Oflox
•Levo
•Moxi
•SM
•KM
•AMK
•CM•ETH
•CS
•PAS
Injectable
FQ
2nd-line
First-line
•INH (H)
•RIF (R)
•EMB (E)
•PZA (Z)

• There were not enough second-line anti-TB drugs available to create a full treatment regimen for MDR-TB, so no appropriate therapy could be provided
• Patient GV was hospitalized in the “chronic ward” and continued on a treatment of HRE indefinitely
Patient History Continued…
First-line
•INH (H)
•RIF (R)
•EMB (E)

• In November of 2000 (after almost two years without therapy), second-line anti-TB medications became available.
• He was started on the following regimen:
Patient History Continued…
•Oflox
•Levo
•Moxi
•SM
•KM
•AMK
•CM•ETH
•CS
•PAS
Injectable
FQ
2nd-line
First-line
•INH (H)
•RIF (R)
•EMB (E)
•PZA (Z)

• In early December, GV developed severe nausea and vomiting followed by cramps and seizures.
• His Cr was 2.3 (upper limit of normal for men is ~1.5) and his potassium was approximately 6.2. He was diagnosed with renal failure and hyperkalemia.
• He was unable to breathe and was started on steroids.
• All of his second-line anti-TB medications were stopped.
• Patient GV died on December 21, 2000.• Cause of death: drug-resistant tuberculosis complicated by
renal failure and hyperkalemia
Patient History Continued…

The Generation of MDR-TB
• Resistance to TB medications is due to chromosomal mutations.
• There is no transmissible resistance factor as is seen in other bacteria (e.g. gram negative rods or some gram positives)
• The mutations occur as independent events and are not associated.
• Mutations occur at low but predictable frequencies 1 per 10-6 to 10-8 replications.– The probability of a bacteria acquiring resistance to two
drugs is the product of independent events.

The Creation of MDR-TB
• Because these spontaneous chromosomal mutations rarely occur in the same bacteria, the use of multiple medications protects against acquired resistance.
• Mutations conferring resistance to drug A (e.g. INH) are killed by drug B (Rif) and mutations resistant to drug B (Rif) are killed by drug A (INH)

Treating tuberculosis: a crash course
First-line
•INH (H)
•RIF (R)
•EMB (E)
•PZA (Z)
•SM (S)
Multi-drug Resistant TB (MDR-TB):
•Resistant to at least the most effective first-line drugs: isoniazid (INH) and rifampin (RIF)
• Requires 18 to 24 months of treatment with second- and third-line medications given under direct observation and with assistance and aggressive management of side effects
Other 2nd-line
Injectable
Fluoroquinolone
•OFLOX
•LEVO
•MOXI
•KM
•AMK
•CM•ETH
•CS
•PAS
Second-line
• AMX/CLV
• Clofazamine
• Clarithromycin
Third-line
Other agents

Is this new?

Source: Dr. Mario Raviglione, Stop TB Department, WHO

The WHO/ IUATLD Global Project on Anti-tuberculosis Drug Resistance Surveillance 1994-2007
1997 The 1st Global report covered 35 countries/geographic settings
2000 The 2nd Global report covered 58 countries/geographic settings
2003 The 3rd Global report covers 77 countries/ geographic settings
2008 The 4th Global report covers 93 countries/ geographic settings

Source: WHO 2008

Source: WHO 2008

Source: WHO 2008

Source: WHO 2008

Forces driving the MDR TB epidemic
1. Incomplete or inadequate therapy, often due to inadequate drug supply
2. Inappropriate usage and quality of second-line drugs
3. On-going transmission of drug-resistant strains (poor case detection, poor treatment)
4. Increased failures to short-course chemotherapy
5. Amplification of drug-resistance due to inability to properly deliver the medicines for the required time period
6. HIV/AIDS


TEN YEARS AGO…
RELUCTANCE TO TREAT MDR-TB IN POOR SETTINGS

MDR-TB Policy: 1996-1997
1. Treatment with second-line (“reserve”) drugs discouraged because countries were deemed too poor

“The WHO Tuberculosis Programme has recommended that treatment of chronic cases with [second-line] drugs remain a low priority for national tuberculosis programmes in developing countries due to their high costs and the limited prospects for cure of those cases.”
— Porter J, McAdam K, eds. Tuberculosis: Back to the Future. 1994

The World Development Report 1993
Source: Dr. Jim Kim, Harvard University

“In many high TB prevalence countries, second-line drugs are prohibitively expensive and unavailable… Multi-drug resistant TB is therefore often untreatable.”
— WHO TB/HIV: A Clinical Care Manual,
1996
“MDR-TB is too expensive to treat in poor countries; it detracts attention and resources from treating drug-susceptible disease.”
—WHO. Groups At Risk, 1996.

The dominant narrative in global health
• Since the 1950s global economic climate, including health care, has been defined by the Bretton Woods Agreement, which created the World Bank and the IMF
• These agencies, along with USAID a bit later on, have had an enormous impact on the global health agenda
• Very early on, these two agencies placed a lot of emphasis on the private sector providing health care (without any proof that it could or would be more efficient). Over the years they began advocating structural adjustment policies (SAPs) with the aim of getting rid of “bloated government”
• SAPs , and loan conditions, call for privatization, decentralization, building of markets—in connection with reduced social spending

• They exerted a lot of influence because they were part of a policy-making class: this class serves as the “foci for generating the policy consensus for the maintenance and defense of the system”.
• They control the terms of the debate, resources, support of research, etc., through the occupation of key nodes in the global policy network. [1]
[1] Cox, R.W. 1987 Production, power and world order: social forces in the making of history, New York: Columbia University Press.
The dominant narrative in global health (2)

MDR-TB Policy: 1996-1997
1. Treatment with second-line (“reserve”) drugs discouraged because countries were deemed too poor
2. Scientific data was shaped around policy: incorrect claims made regarding efficacy of SCC in treating MDRTB

“DOTS makes it virtually impossible to cause a patient to develop the incurable forms of TB that are becoming more common. Other treatment strategies are actually causing multidrug-resistant TB, and may be doing more harm than good.”
— WHO TB Treatment Observer, 1997

Table II: TB Incidence, Prevalence, and Mortality in Tomsk Oblast Penal Sector, 1998-2003
1998 1999 2000 2001 2002 2003
Holding Section TB case notification/100,000 3565 3081 3388 3416 2720.2 1983.1
Holding Section TB Prevalence/100,000 3743.5 2830.8 2753.5 2012.9 2550.1 2784.8
Prison TB case notification/100,000 4042 4523 3357 3008.9 2809.8 2192.9
Prison TB Prevalence/100,000 21581.7 18995.3 18320.2 16469.2 16101.0 15366.8
TB Mortality/100,000 353.1 383.9 129.9 107.7 0 11.85
Percentage of MDR-TB among new cases 28.0 18.6 13.1 15.9 12.2 14.9
Percentage of MDR-TB among re-treatment cases 54.4 25.0 34.9 77.4 63.6 85.7
Source: Tomsk Oblast Penitentiary Tuberculosis Services, Tomsk, Russian Federation, July 2005.

…best practice SCC may even reduce the incidence of MDR-TB where it has already become endemic…
-- Dye et al. Science 2002

BASELINE SITUATION, 1996-1997
1. Treatment with second-line (“reserve”) drugs discouraged because countries were deemed too poor
2. Scientific data was shaped around policy: incorrect claims made regarding efficacy of SCC in treating MDRTB
3. Fear the treating patients would MDR-TB would harm patients with regular TB
• Countries would not take up DOTS
• Countries would use scarce resources on MDR-TB

DOTS and the World Health Organization
Source: Dr. Jim Kim, Harvard University

BASELINE SITUATION, 1996-1997
1. Treatment with second-line (“reserve”) drugs discouraged because countries were deemed too poor
2. Scientific data was shaped around policy: incorrect claims made regarding efficacy of SCC in treating MDRTB
3. Fear the treating patients would MDR-TB would harm patients with regular TB
• Countries would not take up DOTS• Countries would use scarce resources on MDR-TB
4. “Lack of data” to support global policy change

SHIFTING THE PARADIGM
Article 25.(1) Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his control.

Shifting the MDR-TB treatment paradigm
Building international consensus (convincing policy-makers and creating a counter discourse):
• A meeting was convened by Howard Hiatt (BWH) and Arata Kochi (Director, WHO Stop TB Initiative) in Cambridge in 1998 to bring together key decision-makers in global TB
• This group developed the concept of “DOTS-Plus”, a programmatic approach for the treatment of MDR-TB built on WHO’s DOTS strategy for the treatment of drug-sensitive TB.
1

WHO Constitution (1946): “Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. The enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition.”

The creation of a new technical mechanism to promote treatment of MDR-TB:
• Dr. Jim Kim and others at Harvard, working with the WHO and other international partners, created the Green Light Committee (GLC)
Shifting the MDR-TB treatment paradigm
2

PURPOSE OF THE GLC
Created in 2000 by the WHO and the Stop TB Partnership to ensure:
Access to quality assured second line drugs at affordable prices
Monitoring and evaluation of second-line drug use in approved projects
Promotion of technical assistance for MDR-TB projects
Provide policy advice to the WHO

GLC approved projects as of December 2008GLC approved projects as of December 2008134 applications in 61 countries 134 applications in 61 countries
~ 50'000 patients approved for enrolment~ 50'000 patients approved for enrolment
1. Bangladesh2. India
3. Indonesia4. Myanmar
5. Nepal6. Timor-Leste
1. Burkina Faso
2. Cameroon3. DR Congo4. Ethiopia5. Guinea6. Kenya 7. Lesotho
8. Mozambique9. Rwanda10. Uganda
11. Tanzania
1. Belize2. Bolivia
3. Costa Rica4. Dominican
Republic5. Ecuador
6. El Salvador 7. Guatemala
8. Haiti9. Honduras
10. Mexico11. Nicaragua12. Paraguay
13. Peru14. Uruguay
1. Egypt2. Jordan
3. Lebanon4. Pakistan
5. Syria6. Tunisia
1. Armenia2. Azerbaijan
3. Belarus4. Bulgaria5. Estonia 6. Georgia
7. Kazakhstan8. Kyrgyzstan
9. Latvia 10. Lithuania11. Moldova 12. Romania13. Russia14. Serbia
15. Tajikistan16. Ukraine
17. Uzbekistan
1. Cambodia
2. China3. Microne
sia4. Mongoli
a5. Philippin
es6. Samoa 7. Vietnam

The creation of models of care and strategies for scale-up:
• “DOTS-Plus” pilot projects:
– Lima, Peru
– Tomsk, Russian Federation
– Latvia
– Manila, Philippines
– Estonia
Shifting the MDR-TB treatment paradigm
3

PERU

BASELINE SITUATION IN PERU 1996-1997
• In 1980s, history of therapeutic anarchy and incomplete treatment that led to drug-resistance
• A very good national TB program
• Good coverage in urban slum areas
• Decentralized; free
• MDR-TB was 3% of new cases and 15% of re-treatment cases



DOTS-Plus proposed
Goals:
• Improve clinical care
• Scale-up DOTS-Plus in
Peru and in other high-
burden settings
• Bring evidence to bear on
policy
• Enhance NTP capacity
Mechanisms:
• Diagnosis
• Treatment
• Training
• Clinical support
• Infection control
• Documentation
• Coalition building
• Scale-up and replication

August 1996DOTS-Plus project initiated in Lima’s Northern Cone by Partners In Health and Harvard
Medical School, with the Peruvian National TB Program

System of Health Promoters and Social Supports
• Accompaniment
• Food
• Housing
• Transportation
• Individual and group therapy




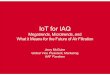
73%
7%
1%
19%
Cured
Abandoned
Failed
Died
Treatment outcomes at completion among DOTS-Plus patients (N=75)
Source: Mitnick et al. NEJM, 2001

Project Accomplishments
• Individualized regimens for MDR patients have cure rate of over 80% in resource-limited settings
• Increased capacity for drug sensitivity testing and reduced delays in treatment
• Contributed to a change in international policy: the first major project in the world

Expanding the community-based treatment model
• Possible to successfully treat TB and MDR TB in an ambulatory setting• Critical components of care:
– Accompaniment: proper patient supervision, aggressive adverse-effects management and monitoring, and psycho-social support
– “Wraparound services”: food, transportation stipends, economic assistance, etc.
• Expanded collaboration from one area in Lima to all of Lima, and subsequently, to 11 rural regions– Hired and trained 700 community health workers – 6227 patients ever enrolled as of April 2007
Outcomes in 66 pts (Mitnick et al 2003)Outcomes in 66 pts (Mitnick et al 2003)
Treatment outcomesas of April 2007

The revision of international guidelines for the treatment of MDR-TB using new models
Shifting the MDR-TB treatment paradigm
Source: http://whqlibdoc.who.int/publications/2008/9789241547581_eng.pdf
4

New treatment and funding initiatives
• Millennium Development Goals
• GFATM
• PEPFAR
• UNITAID
Shifting the MDR-TB treatment paradigm
5

Successful collaboration with donorsSuccessful collaboration with donors
"To help contain resistance to second-line anti-TB drugs and consistent with the policies of other international funding sources, all procurement of medications to treat MDR-TB must be conducted through the Green Light Committee (GLC)" Third Board Meeting, 10-11 October, 2002
Second-line drugs for low and lower-middle income countries; thousands of patients to be
enrolled in 2007-2011; creation of a Global Buffer Stock of SLDs and a Revolving Fund
Funds for Technical Assistance and
Monitoring/Evaluation

CHRONOLOGY OF MDR-TB POLICY DEVELOPMENT
0
5
10
15
20
25
30
35
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 20060
5000
10000
15000
20000GLC approved countries
GLC approved patients
Adapted from Raviglione, Presentation to PARTNERS Meeting, Atlanta, May 2006
WHO/IUATLD
DRS project
First DRS report
New MDR-TB
guidelines
Global Fund requires GLC
Second DRS report
Third DRS report
DOTS-Plus Working Group
GLCCambridge MDR-TB meeting
DRSguidelines

Thank You!









![The Prophetic Biography[Introduction of ash-Shaykh Mashhoor Hasan Salmaan] Verily, all praise is due to Allaah; we praise Him, and seek His aid and forgiveness. We seek refuge in Allaah](https://img.pdfslide.us/doc/110x75/6056ea8685e19c7da372e3dc/the-prophetic-biography-introduction-of-ash-shaykh-mashhoor-hasan-salmaan-verily.jpg)