Embed Size (px)
Citation preview

9/6/2017
1
Know Pain, Know GainCara Brock, PharmD, BCGP, CPEJulie H. McGinley, PharmD, MHS
Disclosure and Conflict of Interest
Drs. Brock and McGinley declare no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings and honoraria.
Pharmacist Objectives
At the conclusion of this program, the pharmacist will be able to:
1. Identify first line medications and treatments used in common pain pathologies.
2. Illustrate main counseling points and strategies for patients’ common pain pathologies.
3. Describe non-pharmacological approaches to common pain pathologies.

9/6/2017
2
At the conclusion of this program, the technician will be able to:
1. Identify common medications and treatments used in pain management.
2. Illustrate main counseling points and strategies for patients with pain.
3. Describe common barriers for providing optimal pain management.
Technician Objectives
Gabapentin vs Pregabalin
Gabapentin vs Pregabalin
Fudin, J. Pharmacy Times. September 21, 2015. http://www.pharmacytimes.com/contributor/jeffrey-fudin/2015/09/how-gabapentin-differs-from-pregabalin?p=3Pop-Busui R, Boulton AJM, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM, Ziegle Diabetes Care, 2017;40:136-154.
Pregabalin Gabapentin
Class Anticonvulsant
MOA Binds to the alph2-delta subunit of voltage-gated Ca++ channels
FDA
Approved Indications
Partial-onset seizures
Postherpetic neuralgiaFibromyalgia
Neuropathic pain, diabetes-
associated and spinal cord injury
associated
Partial-onset seizures
Postherpetic neuralgia
Absorption Quickly throughout the small
intestine and the into the ascending colon
Not saturable
Linear PK profile
Time to peak 1.5 hours (3 hours
with food)
Slowly and variably throughout the
small intestine
Saturable
Non-linear PK profile
Time to peak 3 hours
Gabapentin vs Pregabalin
Fudin, J. Pharmacy Times. September 21, 2015. http://www.pharmacytimes.com/contributor/jeffrey-fudin/2015/09/how-gabapentin-differs-from-pregabalin?p=3Pop-Busui R, Boulton AJM, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM, Ziegle Diabetes Care, 2017;40:136-154.
Pregabalin Gabapentin
Oral
Bioavailability
> 90% from 75 mg – 900 mg
dividedLess variability among
patients
80% at 100 mg q 8 hours
27% at 1600 mg q 8 hoursWith greater variability among
patients
Metabolism Metabolized to a negligible extent
No interactions with CYP enzymes or P-gp
Excretion Renally, 90% unchanged
drug, with minor metabolitesRenal dose adjustments
begin at CrCl of 59
Renally, proportional to renal function
as unchanged drugRenal dose adjustments begin at CrCl
of 59

9/6/2017
3
Gabapentin vs Pregabalin
Fudin, J. Pharmacy Times. September 21, 2015. http://www.pharmacytimes.com/contributor/jeffrey-fudin/2015/09/how-gabapentin-differs-from-pregabalin?p=3Pop-Busui R, Boulton AJM, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM, Ziegle Diabetes Care, 2017;40:136-154.
Pregabalin Gabapentin
Side Effects Dizziness
SomnolenceConfusion
Psychoactive effects
Peripheral edema
Dose dependent and reversible
Taper to d/c over a week at least
Potency Pregabalin is estimated to be about 2.4x more potent than gabapentin
Dose-
response curve
Steeper
Pain-relieving effect continued to max dose
Pain-relieving effect plateaus
Gabapentin vs Pregabalin
Fudin, J. Pharmacy Times. September 21, 2015. http://www.pharmacytimes.com/contributor/jeffrey-fudin/2015/09/how-gabapentin-differs-from-pregabalin?p=3Pop-Busui R, Boulton AJM, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM, Ziegle Diabetes Care, 2017;40:136-154.
Pregabalin Gabapentin
Conversion 6:1 gabapentin to pregabalin
Gabapentin 900 mg/day � pregabalin 150 mg/dayDirect switch or
gabapentin dose decrease by 50% and 50% of desired pregabalin
dose given concurrently for 4 days
Final
Thoughts
Predictable PK profile
More bioavailableIncreased potency
Steeper dose-response curve
without plateau
Some studies suggest more
efficacious for neuropathic pain
Fewer side effects?
Controlled substance
More costly
Less predictable PK profile
Less bioavailableLess potent
Dose-response curve plateaus
Not controlled
Less expensive due to generic
Fibromyalgia1st Line Treatments
Presentation & Diagnosis
• Prevalence 2%
• Time to diagnosis
– Average 3.7
consultations with specialists
• Symptoms
– Widespread pain
– Fatigue
– Sleep disturbance
• Diagnosis
– Clinical presentation
– Tender points
– Symptom survey
• Widespread pain index (WPI)
• Symptom severity
– Labs
• Rule out other conditions
Wolfe, F., Clauw, D.J., Fitzcharles, M.A., Goldenberg,et al.2011. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR
Preliminary Diagnostic Criteria for Fibromyalgia. The Journal of rheumatology, 38(6), pp.1113-1122.
Kodner, C. (2015). Common Questions About the Diagnosis and Management of Fibromyalgia. American Family Physician, 91(7), pp.472 - 478.
Macfarlane, Gary J., et al. "EULAR revised recommendations for the management of fibromyalgia." Annals of the rheumatic diseases (2016): annrheumdis-2016.

9/6/2017
4
Pharmacologic Treatment
• Nonpharmacologic
– Aerobic and strengthening exercise
– Multicomponent therapies
– Acupuncture
– Hydrotherapy
– Meditative movement therapy
• Yoga, quigong, tai chi
• Pharmacologic
– Amitriptyline
– Duloxetine
– Milnacipran
– Tramadol
– Pregabalin
– Cyclobenzaprine
Macfarlane, Gary J., et al. "EULAR revised recommendations for the management of fibromyalgia." Annals of the rheumatic diseases (2016): annrheumdis-2016.
PharmacologicDrug Dose Role Comments
Amitriptyline 25mg at bedtime Reduce pain Reduce fatigue
Sleep disturbance
ADR
Duloxetine*(Cymbalta®)
Starting dose: 30mg dailyTarget dose: 60mg daily
Reduce painSmall effect on sleep
Small effect on disabilityNo effect on fatigue
No difference in outcomes at 120mg
dailyAvoid use in GFR <
30mL/min
Milnacipran*(Savella®)
Day 1: 12.5 mg once Days 2-3: 12.5 mg twice daily
Days 4-7: 25 mg twice daily After Day 7: 50 mg twice daily
MAX 200mg/day
Reduces pain Reduce fatigue
Reduce disability
No effect on sleepAdjust in moderate –
to severe renal impairment
Tramadol 200 - 300mg/day Improves pain Try other treatments first
Pregabalin*(Lyrica®)
75mg q12h150mg q12h
225mg q12hMAX 450mg/day
Reduce pain Renal adjustmentDose dependent side
effects
Cyclobenzaprine 10mg HS Titrated to
10mg AM & 20mg HS
Improves sleep quality 85% of patients experienced side
effects
Macfarlane, Gary J., et al. "EULAR revised recommendations for the management of fibromyalgia." Annals of the rheumatic diseases (2016): annrheumdis-2016.Tofferi, J. K., Jackson, J. L. and O'Malley, P. G. (2004), Treatment of fibromyalgia with cyclobenzaprine: A meta-analysis. Arthritis & Rheumatism, 51: 9–13. doi:10.1002/art.20076Lyrica® [package insert]. NY, NY: Parke Davis; 2011.
Cymbalta® [package insert]. Indianapolis, IN: Eli Lily and Company; 2016.Savella® [package insert]. NY, NY:Forest Laboratories; 2011.
Diabetic Peripheral Neuropathy
Diabetic Peripheral Neuropathy
Pop-Busui R, Boulton AJM, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM, Ziegler D. Diabetes Care, 2017;40:136-154.
• Peripheral Neuropathy is associated with:
– Hyperglycemia
– Height
– Smoking
– Elevated blood pressure
– Elevated weight
– Elevated lipid measures

9/6/2017
5
Diabetic Peripheral Neuropathy
Pop-Busui R, Boulton AJM, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM, Ziegler D. Diabetes Care, 2017;40:136-154.
Diabetic Peripheral Neuropathy
Pop-Busui R, Boulton AJM, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM, Ziegler D. Diabetes Care, 2017;40:136-154.
• Examination
– Ankle reflexes
– Vibration perception
– Monofilament exam
– Proprioception
– Thermal discrimination
– Pinprick sensation
• Signs and Symptoms
– Numbness
– Tingling
– Burning
– Electric shocks
– Stabbing
– Poor balance
Diabetic Peripheral Neuropathy
Pop-Busui R, Boulton AJM, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM, Ziegler D. Diabetes Care, 2017;40:136-154.
• Treatment
– Tighter glycemic control and LSM
– Pharmacotherapy
• Anticonvulsants
• SNRIs
• TCAs
Diabetic Peripheral Neuropathy
* FDA approval for DPNPop-Busui R, Boulton AJM, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM, Ziegler D. Diabetes Care, 2017;40:136-154.
• Anticonvulsants
– Pregabalin*
• ADA recommended initial approach
– Gabapentin
• ADA states may also be used as an effective initial approach, taking into account patients’ socioeconomic
status, comorbidities, and potential drug interactions

9/6/2017
6
Diabetic Peripheral Neuropathy
* FDA approval for DPNPop-Busui R, Boulton AJM, Feldman EL, Bril V, Freeman R, Malik RA, Sosenko JM, Ziegler D. Diabetes Care, 2017;40:136-154.
• SNRIs
– Duloxetine*
• ADA recommended initial approach
– Venlafaxine
• TCAs
– Amitriptyline
Diabetic Peripheral Neuropathy
*FDA approval for DPN
Initial
Dose
Effective
Dose
Common ADEs Major ADEs
Pregabalin* 25-75 mg, 1-3x/day
300-600 mg/day
Somnolence, dizziness,peripheral edema, headache, ataxia, fatigue, xerostomia,
weight gain
Angioedema, hepatotoxicity, rhabdomyolysis, SI, seizures,
thrombocytopenia
Gabapentin 100-300 mg,
1-3x/day
900-3600 mg/day
Weight gain, somnolence, dizziness, ataxia, fatigue
Stevens-Johnson syndrome, SI, seizures
Duloxetine* 20-30mg/day
60-120 mg/day
Somnolence, dizziness, constipation, dyspepsia,
diarrhea, xerostomia, anorexia, headache, diaphoresis,
insomnia, fatigue, decreased libido
Stevens-Johnson syndrome, hepatotoxicity,HTN crisis, GI hemorrhage, delirium, MI,
cardiac arrhythmias, glaucoma, SI, shift to mania in bipolar disorder, seizures,
hyponatremia, fragility, serotonin syndrome, neuroleptic malignant syndrome
Venlafaxine 37.5 mg/day
75-225 mg/day
Nausea, somnolence, dizziness, constipation, dyspepsia,
diarrhea, xerostomia, anorexia
Amitriptyline 10-25 mg/day
25-100 mg/day
Xerostomia, somnolence, Fatigue, headache, dizziness,
insomnia, orthostatic HTN,hypotension, anorexia, nausea, urinary retention, constipation, blurred vision, accommodation
disturbance, mydriasis,weight gain
Delirium, cardiac arrhythmias, conductionabnormalities, MI, HF exacerbation, stroke,
seizures, hepatotoxicity, bone marrow suppression, SI, shift to mania in bipolar
disorder, neuroleptic malignant syndrome, serotonin syndrome, hyponatremia, fragility
bonefractures
Postherpetic Neuralgia (PHN)
Post Herpetic Neuralgia
• Annual incidence 3.4 cases/1000 persons
• Age > 90 yrs 11 cases/1000 persons
• Risk factors
– Age
– In acute phase severity of
• Prodrome
• Rash
• Pain
– Chronic disease states
– Immunocomprimised patients
Johnson R, Rice A. Postherpetic Neuralgia. New England Journal of Medicine. 2014;371(16):1526-1533. doi:10.1056/nejmcp1403062.

9/6/2017
7
Pathophysiology & Presentation
VZV infection
Reactivation of VZV
Vesicular rash
Rash resolves
Peripheral nerve damage
PHN � pain lasting > 90 days after rash onset
Johnson R, Rice A. Postherpetic Neuralgia. New England Journal of Medicine. 2014;371(16):1526-1533. doi:10.1056/nejmcp1403062.
PHN Management - Topical
Drug/ Starting Dose NNT
(for one person to have 50% pain relief)
Side Effects
Lidocaine Patch 5%
Up to 3 patches/day for12 hours
2.0 (1.4 – 3.3) Local erythema
Capsaicin Cream 0.075%
four times daily
3.3 (2.3 – 5.8) Pain on application
Local erythemaRash
Capsaicin Patch 8%
apply for 30 – 90 minutes
11.0 (6.1 – 62.0) Pain on application
Local erythemaRash
Systemic adverse effects
Johnson R, Rice A. Postherpetic Neuralgia. New England Journal of Medicine. 2014;371(16):1526-1533. doi:10.1056/nejmcp1403062.
PHN Management - OralDrug/ Starting Dose Average
Effective
Dose
Dose Adjustment NNT Side Effects
Gabapentin100mg q8h
2572 mg/d Increase dose by 100 – 300 mg every 3 – 7 days up to
1800mg/day
4.4 (3.3 – 6.1) SedationDizziness
Peripheral Edema
Pregabalin150 – 300mg daily
divided BID or TID
398 mg/d Increase to 300mg/d within 1 week
Max 600mg/d
4.2 (3.4 – 5.4) SedationDizziness
Peripheral Edema
TCAAmitriptyline
Nortriptyline10 – 25mg at bedtime
95 mg/d
122 mg/d
Increase by 10 – 25mg every 3 – 7 days up to 75 – 100mg/d
2.6 (2.1 – 3.5) SedationDry mouth
Weight gainUrinary retention
Blurred vision
MorphineOxycodone
5 – 15mg q4h PRN
90 mg/d45 mg/d
After 1 – 2 weeks convert to long acting, continue PRN
2.8 (2.0 – 4.6)2.5 (1.7 – 4.4)
DrowsinessDizziness
ConstipationN/V
Mood change
Tramadol50mg q4-6h
298 mg/d Increase by 50 – 100mg/d every 3 – 7 days
Max 400mg/d (300mg/d >75yrs)
4.8 (2.6– 27.0) DrowsinessDizziness
ConstipationN/V
Mood change
Johnson R, Rice A. Postherpetic Neuralgia. New England Journal of Medicine. 2014;371(16):1526-1533. doi:10.1056/nejmcp1403062.
PHN Prevention
• Antiviral drugs
• Glucocorticoids
• Amitriptyline
• VZV vaccine
– Reduces incidence of HZV by 51%
– Reduces incidence of PHN by 66%
– Patients > 70 years reduces HZV by 38%
Johnson R, Rice A. Postherpetic Neuralgia. New England Journal of Medicine. 2014;371(16):1526-1533. doi:10.1056/nejmcp1403062.

9/6/2017
8
Rheumatoid Arthritis1st Line Treatments
Rheumatoid ArthritisNon-biologic DMARDS
Singh JA, Saag KG, et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis & Rheumatology, 2016;68(1):1-26.
Agent Time to Onset
Dose
Methotrexate (MTX) 1 – 3 months
7.5 – 15 mg po q week; 10 – 25 mg IM/SQ q week
Hydroxychloroquine(HCQ)
2 – 4 months
Initial: 400 – 600 mg po daily for 4 -12 weeks; maintenance: 200
– 400 mg po daily
Leflunomide 1 – 2 months
100 mg po daily x 3 days; then 20 mg po daily
Minocycline 3 + months 100 mg po BID
Sulfasalazine 1 – 3 months
50 – 100 mg po daily; titrate to 1000 mg po BID
Singh JA, Saag KG, et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis & Rheumatology, 2016;68(1):1-26.
Agent Time to Onset Dose
TNF-α inhibitors
Adalimumab 1 – 4 weeks 40 mg SQ q 14 days (up to 40 mg SQ q 7 days if not taking MTX
Certolizumab 1 – 4 weeks 400 mg SQ weeks 0, 2, 4 then 200 mg SQ q 2 weeks
Etanercept 1 – 4 weeks 50 mg SQ weekly or 25 mg SQ twice weekly
Golimumab 1 -4 weeks 50 mg SQ monthly; must be used in conjunction with MTX
Infliximab Days to weeks 3 mg/kg IV infusion weeks 0, 2, 6 and then q 8 weeks; must be used
in conjunction with MTX
Rheumatoid ArthritisAnti-TNF Biologics
Singh JA, Saag KG, et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis & Rheumatology, 2016;68(1):1-26.
Agent Time to Onset Dose
Anti-CD 20
Rituximab Up to 3 months 1000 mg IV days 1 and 15 may repeat q 24 weeks (no sooner than 16 weeks); must be used with MTX
T-cell costimulation modulator
Abatacept 1 – 3 months IV: < 60 kg: 500 mg; 60 – 100 kg: 750 mg; > 100
kg: 1000 mg; Weeks 0, 2, 4, then monthly
SQ: 125 mg SQ weekly +/- weight based loading IV infusion within 24 hr prior to 1st SQ dose
IL-1 receptor antagonist
Anakinra Not given 100 mg SQ daily
IL-6 receptor antagonist
Tocilizumab Not given IV: 4 mg/kg IV every 4 weeks (up to 8 mg/kg IV
every 4 weeks)SQ: <100: kg 162 mg SQ once every other week,
increase to 162 mg SQ every week
> 100 kg: 163 mg SQ once every week
Rheumatoid ArthritisNon-TNF Biologics

9/6/2017
9
Singh JA, Saag KG, et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis & Rheumatology, 2016;68(1):1-26.
Agent Time to Onset Dose
Janus kinase enzyme inhibitor
Tofacitinib Not given IR: 5 mg po BID
ER: 1 mg po once daily
Rheumatoid ArthritisNon-TNF Biologics
Rheumatoid Arthritis
Singh JA, Saag KG, et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis & Rheumatology, 2016;68(1):1-26.
Early RA
(< 6 months)
Low Disease Activity
DMARD Monotherapy
Moderate or High Disease Activity
DMARD Monotherapy,
DMARD Combo Therapy,
anti-TNF agent +/- MTX or non-TNF Biologic +/- MTX
NSAID or Corticosteroid as
bridge and initial pain management
Rheumatoid Arthritis
Singh JA, Saag KG, et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis & Rheumatology, 2016;68(1):1-26.
Low, Moderate or High Disease
Activity
DMARD Monotherapy
Moderate or High Disease Activity
Remains
DMARD Combo Therapy, anti-TNF agent +/- MTX,
non-TNF Biologic +/- MTX or Tofacitinib +/- MTX
DMARD NaiveEstablished RA
(> 6 months)
Rheumatoid Arthritis
Singh JA, Saag KG, et al. 2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis & Rheumatology, 2016;68(1):1-26.
DMARD Combo Therapy, anti-TNF agent +/- MTX, non-TNF Biologic +/- MTX or Tofacitinib
+/- MTX
Single Anti-TNF Failure
Non-TNF Biologic +/- MTX or Anti-
TNF +/- MTX
Single Non-TNF Biologic Failure
Another Non-TNF biologic +/- MTX
Moderate or High Disease Activity
Remains
Established RA(> 6 months)

9/6/2017
10
Chronic Lower Back Pain1st Line Non-Invasive Treatments
Low Back Pain
• American College of Physicians (2017)
Chou, Roger, et al. "Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain SocietyDiagnosis and Treatment of Low Back Pain." Annals of internal medicine 147.7 (2007): 478-491.Qaseem, Amir, et al. "Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain." Annals of internal medicine 166.7 (2017): 514-530.
Acute Subacute Chronic
Recommendation 1
• For acute or subacute LBP
• Most acute/subacute LBP will improve over time regardless of treatment– Superficial heat (moderate)
– Massage/acupuncture/spinal manipulation (low)
– NSAID or skeletal muscle relaxers (moderate)
– NOT recommended: APAP & corticosteroids
• Inform patient of favorable prognosis– Substantial improvement in first month
• Remain active as tolerated
• Shared decision making
Qaseem, Amir, et al. "Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of
Physicians: Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain." Annals of internal medicine 166.7 (2017): 514-530.
Recommendation 2
• For patients with chronic low back pain (CLBP)
– First select non-pharmacologic treatments
– Harms were poorly reported
• No serious harms
• Muscle soreness
Qaseem, Amir, et al. "Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of
Physicians: Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain." Annals of internal medicine 166.7 (2017): 514-530.
ExerciseMultidisciplinary
rehabilitation Acupuncture
Mindfulness based stress
reduction
Cognitive behavioral
therapy (CBT)
Spinal manipulation

9/6/2017
11
Recommendation 3
• In patients with CLBP with inadequate response to non-pharmacologic treatments
– First line: NSAID
– Second line: tramadol or duloxetine
– Opioids
• Patient has failed NSAID, tramadol or duloxetine
• Benefits outweigh risks
Qaseem, Amir, et al. "Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of
Physicians: Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain." Annals of internal medicine 166.7 (2017): 514-530.
NSAID
• First pharmacologic choice
• No difference amongst NSAID
• Consider patient specific factors
• Use lowest effective dose
• Shortest periods necessary
Qaseem, Amir, et al. "Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of
Physicians: Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain." Annals of internal medicine 166.7 (2017): 514-530.
HematologicHematologic GI GI RenalRenal Cardiovascular Cardiovascular
Second and Third Line Recommendations
• Tramadol
– Moderate effect on pain (moderate)
– Small effect on function (moderate)
• Duloxetine
– Small effect on pain and function (moderate)
• Opioids
– Small effect on short-term pain and function (mod)
– No difference amongst long-acting opioids
Qaseem, Amir, et al. "Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of
Physicians: Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain." Annals of internal medicine 166.7 (2017): 514-530.
LBP General Recommendations
• Acute/subacute LBP will improve regardless of treatment
– Avoid costly and/or harmful treatments
– Avoid corticosteroids
• Chronic LBP
– Select therapies that have fewest harms and lowest cost
– TCA and SSRI not effective
Qaseem, Amir, et al. "Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of
Physicians: Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain." Annals of internal medicine 166.7 (2017): 514-530.

9/6/2017
12
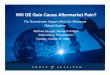
NSAID: First Pharmacologic Choice for Lower Back Pain
First line: NSAID MOA
Arachadonic acid
COX – 1
Prostaglandins & Thromboxane A2
Gastroprotection, platelet aggregation
Vasoconstriction
COX – 2
Prostaglandins
Pain, Fever
Love BL, Thoma MN. Chapter 20. Peptic Ulcer Disease. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic
Approach, 9e. New York, NY: McGraw-Hill; 2014.http://accesspharmacy.mhmedical.com/content.aspx?bookid=689&Sectionid=48811467. Accessed March 12, 2016.
Buys LM, Elliott M. Chapter 71. Osteoarthritis. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach,
9e. New York, NY: McGraw-Hill;
First line: NSAID Selectivity
• Relative selectivity
• Comparable efficacy in reducing pain
Non-selective Indomethacin
PiroxicamIbuprofen
Naproxen
Sulindac
Ketoprofen
Ketorolac
Flurbiprofen
Partially-selective Etodolac
NabumetoneMeloxicam
Diclofenac
COX-2 Selective Celecoxib
Love BL, Thoma MN. Chapter 20. Peptic Ulcer Disease. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A
Pathophysiologic Approach, 9e. New York, NY: McGraw-Hill; 2014.http://accesspharmacy.mhmedical.com/content.aspx?bookid=689&Sectionid=48811467. Accessed March 12, 2016.Buys LM, Elliott M. Chapter 71. Osteoarthritis. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic
Approach, 9e. New York, NY: McGraw-Hill;
NSAID Adverse Effects
Body System Non-Selective COX-2 Selective Considerations
Hematologic
Reversible inhibition of
COX-1Ibuprofen negates ASA cardioprotection
Do not negate
cardioprotection of ASA
Anticoagulation
CoagulopathyThrombocytopenia
GI
Dose dependent risk
of GI events
Ketorolac – potent COX-1 inhibitor
Lower risk of GI
events
Lower risk of liver damage
Concomitant use of
anticoagulantsPrevious GI bleeding episodesUse lowest dose for shortest timeAvoid alcoholLiver disease
Herndon, CM. (2017). Principles of Analgesic Use. 7th ed. Chicago: American Pain Society, pp.18 - 26.

9/6/2017
13
NSAID Adverse Effects
Body System Non-Selective COX-2 Selective Considerations
RenalBoth selective and non-selective NSAID can
induce renal insufficiency
Decreased synthesis of renal vasodilator prostaglandins Interstitial nephritisImpaired renin secretionEnhanced tubular water and sodium reabsorption
Risk factors: CHF,
chronic renal insufficiency, cirrhosis w/ ascites, SLE, diuretics, atherosclerosis in elderly patients, multiple myeloma, volume depletion
CardiovascularAll NSAID regardless of selectivity are
associated with increased risk of cardiovascular eventsHigher risk in patients with cardiac comorbidities
Recent CV event
CV surgeryCV risk factors or history of CV disease
Opioid Adverse Effects
Opioid Adverse Effects
• Central Nervous System
• Dermatologic
• Gastrointestinal
• Cardiovascular
• Endocrine and metabolic
• Genitourinary
• Hematologic and oncologic
• Hepatic
• Neuromuscular and skeletal
Opioid Adverse Effects
Villars P, et al. J Pain Symptom Manage. 2007; 33: 67-77.
Non-propulsive contractions
Pyloric, ileocolonic and anal sphincters
stimulated
Segmental contraction in
the small bowel and
colon
Decreased ion and fluid secretion
Increased tone, decreased motility, increased transit
time and less secretions
Effect of
Opioids on GI Tract
Mu Receptors

9/6/2017
14
Opioid Adverse Effects Opioid Adverse Effects
Dorn, S., Lembo, A. and Cremonini, F. The American Journal of Gastroenterology Supplements, 2014;2(1):31-37.
Villars P, et al. J Pain Symptom Manage. 2007;33: 67-77.
• Mush and Push
• Laxatives
– Bulk Forming
– Osmotic Laxatives
– Stimulant Laxatives
• Chloride Channel Activators
• Peripherally Acting Mu-Opioid Receptor Antagonists (PAMORA)
Opioid Adverse Effects
Agent Dose
PEG 17 grams dissolved in 120 – 240 mL po daily
Lactulose 10 -20 g po daily, may increase to to 40 g
Senna 8.6 mg tabs; 2 tabs po QHS or BID; up to 8 tabs/day
Bisacodyl 10-30 mg po daily;Suppositories scheduled q48-72 hours
Lubiprostone 24 mcg po BID
Methylnaltrexone SQ: 12 mg SQ dailyOral: 450 mg po daily
Advanced Illness: weight-based, 1 dose every other day a needed
Naloxegol 25 mg po daily in the morning on an empty stomach (dose adjustments necessary with moderate and strong CYP3A4 Inhibitors)
Movantik (naloxegol) [prescribing information]. Wilmington, DE: AstraZeneca Pharmaceuticals; August 2016.Amitiza (lubiprostone) [prescribing information]. Deerfield,IL: Takeda Pharmaceuticals; September 2016.Relistor (methylnaltrexone) [prescribing information]. Raleigh, NC: Salix Pharmaceuticals; January 2017.
What Questions Do You Have?

9/6/2017
15
Speaker Contact Information
Cara Brock:
Julie McGinley:
Know Pain, Know GainCara Brock, PharmD, BCGP, CPEJulie H. McGinley, PharmD, MHS