Embed Size (px)
Citation preview
Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020
Dr Keith Holt
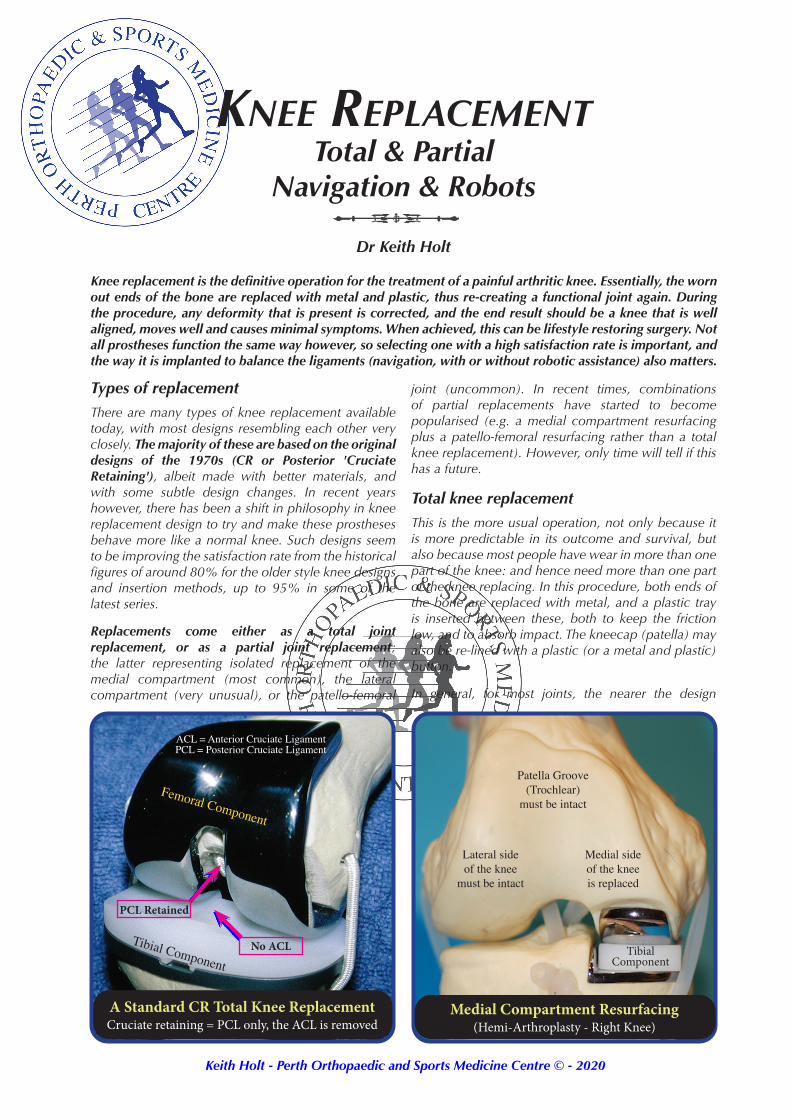
Knee replacement is the definitive operation for the treatment of a painful arthritic knee. Essentially, the worn out ends of the bone are replaced with metal and plastic, thus re-creating a functional joint again. During the procedure, any deformity that is present is corrected, and the end result should be a knee that is well aligned, moves well and causes minimal symptoms. When achieved, this can be lifestyle restoring surgery. Not all prostheses function the same way however, so selecting one with a high satisfaction rate is important, and the way it is implanted to balance the ligaments (navigation, with or without robotic assistance) also matters.
Types of replacementThere are many types of knee replacement available today, with most designs resembling each other very closely. The majority of these are based on the original designs of the 1970s (CR or Posterior 'Cruciate Retaining'), albeit made with better materials, and with some subtle design changes. In recent years however, there has been a shift in philosophy in knee replacement design to try and make these prostheses behave more like a normal knee. Such designs seem to be improving the satisfaction rate from the historical figures of around 80% for the older style knee designs and insertion methods, up to 95% in some of the latest series.
Replacements come either as a total joint replacement, or as a partial joint replacement; the latter representing isolated replacement of the medial compartment (most common), the lateral compartment (very unusual), or the patello-femoral
joint (uncommon). In recent times, combinations of partial replacements have started to become popularised (e.g. a medial compartment resurfacing plus a patello-femoral resurfacing rather than a total knee replacement). However, only time will tell if this has a future.
Total knee replacementThis is the more usual operation, not only because it is more predictable in its outcome and survival, but also because most people have wear in more than one part of the knee: and hence need more than one part of the knee replacing. In this procedure, both ends of the bone are replaced with metal, and a plastic tray is inserted between these, both to keep the friction low, and to absorb impact. The kneecap (patella) may also be re-lined with a plastic (or a metal and plastic) button.
In general, for most joints, the nearer the design
Knee ReplacementTotal & Partial
Navigation & Robots
A Standard CR Total Knee ReplacementCruciate retaining = PCL only, the ACL is removed
Medial Compartment Resurfacing(Hemi-Arthroplasty - Right Knee)
Femoral Component
Tibial ComponentTibial
Component
Patella Groove(Trochlear)
must be intact
Lateral side of the knee
must be intact
Medial side of the kneeis replaced
PCL Retained
No ACL
ACL = Anterior Cruciate LigamentPCL = Posterior Cruciate Ligament
Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 2
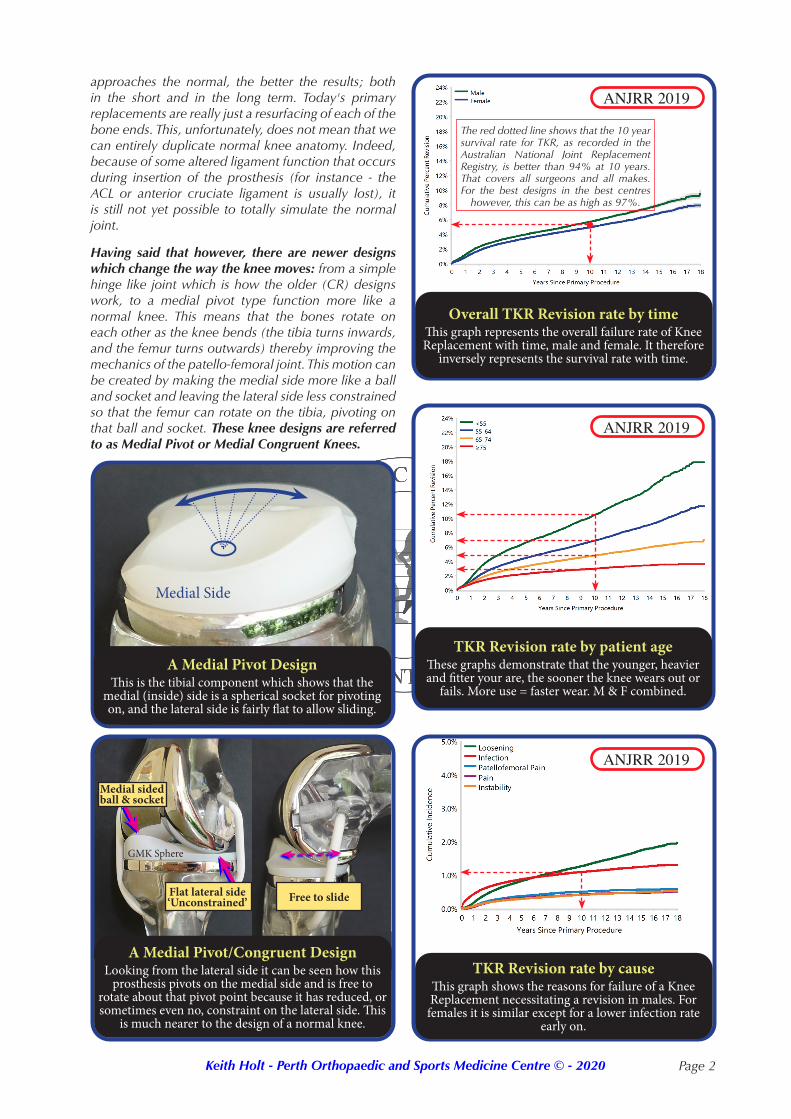
approaches the normal, the better the results; both in the short and in the long term. Today's primary replacements are really just a resurfacing of each of the bone ends. This, unfortunately, does not mean that we can entirely duplicate normal knee anatomy. Indeed, because of some altered ligament function that occurs during insertion of the prosthesis (for instance - the ACL or anterior cruciate ligament is usually lost), it is still not yet possible to totally simulate the normal joint.
Having said that however, there are newer designs which change the way the knee moves: from a simple hinge like joint which is how the older (CR) designs work, to a medial pivot type function more like a normal knee. This means that the bones rotate on each other as the knee bends (the tibia turns inwards, and the femur turns outwards) thereby improving the mechanics of the patello-femoral joint. This motion can be created by making the medial side more like a ball and socket and leaving the lateral side less constrained so that the femur can rotate on the tibia, pivoting on that ball and socket. These knee designs are referred to as Medial Pivot or Medial Congruent Knees.
Overall TKR Revision rate by timeThis graph represents the overall failure rate of Knee Replacement with time, male and female. It therefore
inversely represents the survival rate with time.
TKR Revision rate by patient ageThese graphs demonstrate that the younger, heavier and fitter your are, the sooner the knee wears out or
fails. More use = faster wear. M & F combined.
TKR Revision rate by causeThis graph shows the reasons for failure of a Knee Replacement necessitating a revision in males. For
females it is similar except for a lower infection rate early on.
ANJRR 2019
ANJRR 2019
ANJRR 2019
The red dotted line shows that the 10 year survival rate for TKR, as recorded in the Australian National Joint Replacement Registry, is better than 94% at 10 years. That covers all surgeons and all makes. For the best designs in the best centres
however, this can be as high as 97%.
A Medial Pivot/Congruent DesignLooking from the lateral side it can be seen how this
prosthesis pivots on the medial side and is free to rotate about that pivot point because it has reduced, or sometimes even no, constraint on the lateral side. This
is much nearer to the design of a normal knee.
A Medial Pivot DesignThis is the tibial component which shows that the
medial (inside) side is a spherical socket for pivoting on, and the lateral side is fairly flat to allow sliding.
Medial sided ball & socket
Flat lateral side ‘Unconstrained’
Medial Side
Free to slide
GMK Sphere
Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 3
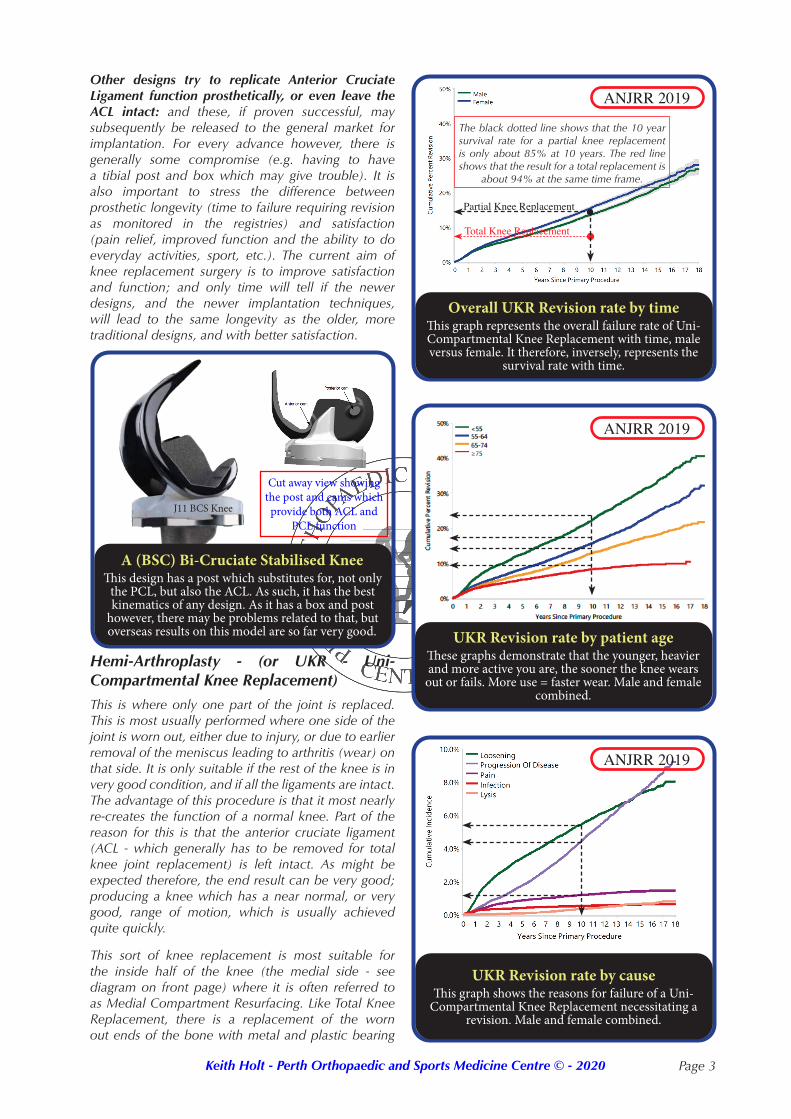
Overall UKR Revision rate by timeThis graph represents the overall failure rate of Uni-Compartmental Knee Replacement with time, male versus female. It therefore, inversely, represents the
survival rate with time.
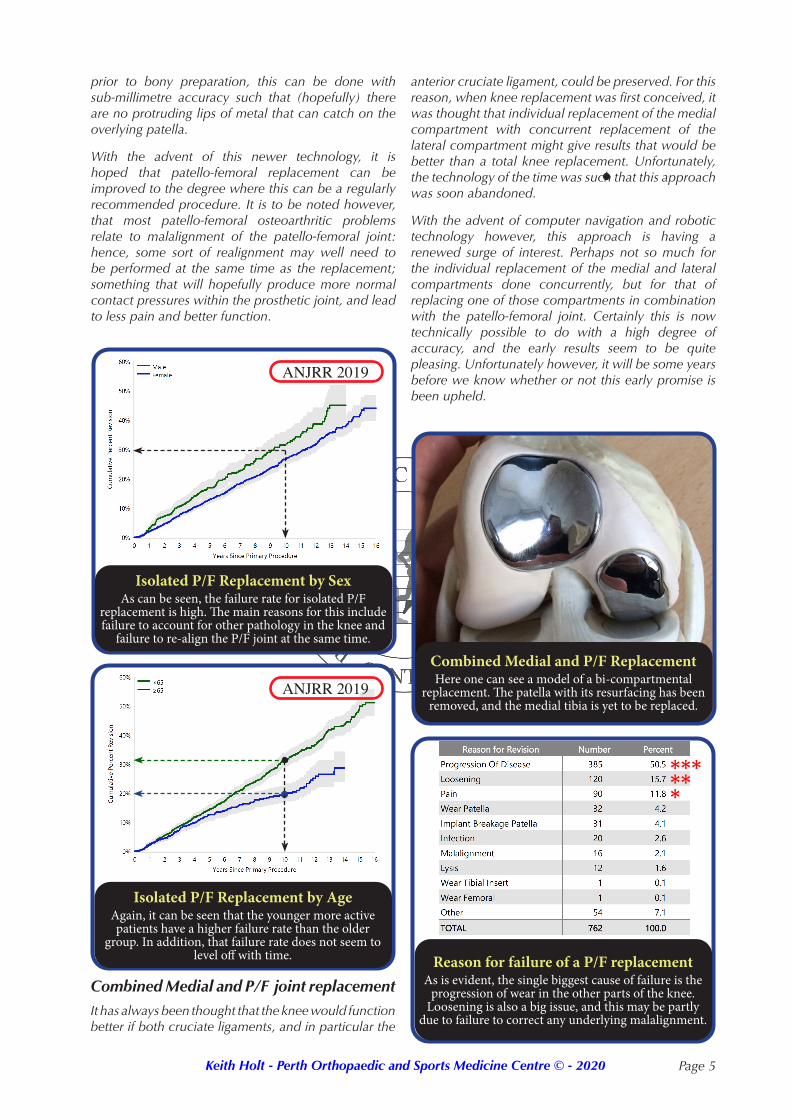
UKR Revision rate by patient ageThese graphs demonstrate that the younger, heavier and more active you are, the sooner the knee wears
out or fails. More use = faster wear. Male and female combined.
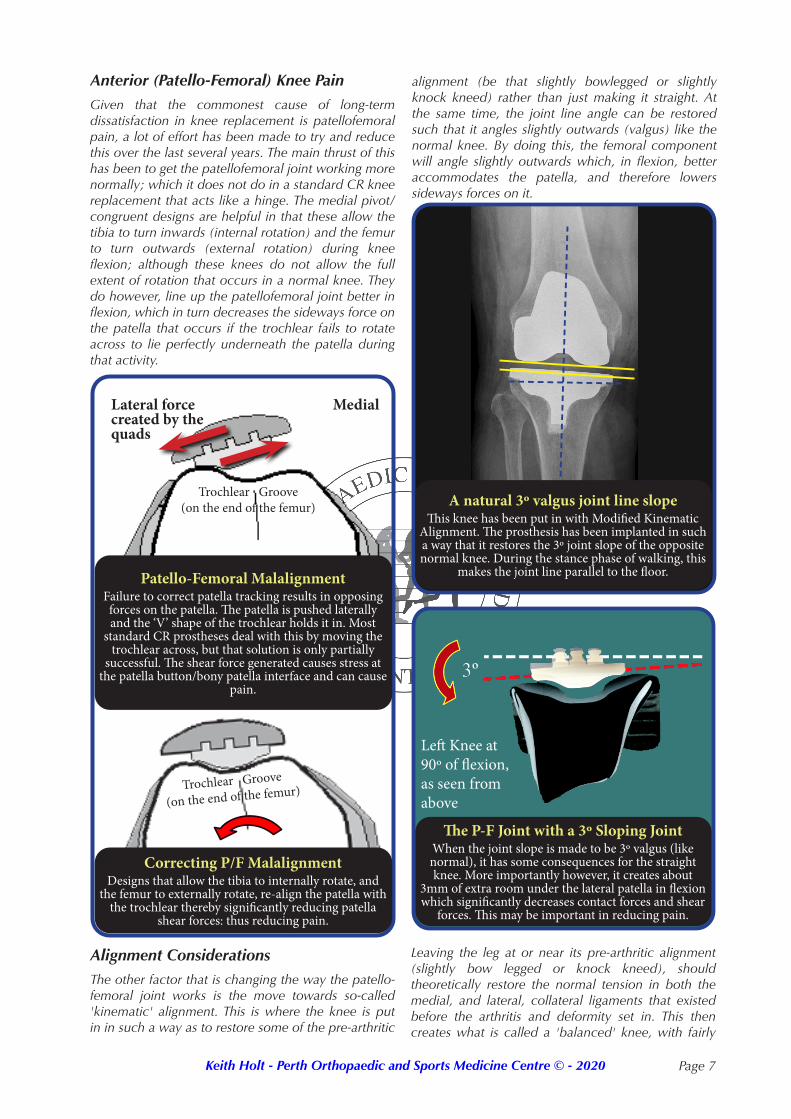
UKR Revision rate by causeThis graph shows the reasons for failure of a Uni-
Compartmental Knee Replacement necessitating a revision. Male and female combined.
Other designs try to replicate Anterior Cruciate Ligament function prosthetically, or even leave the ACL intact: and these, if proven successful, may subsequently be released to the general market for implantation. For every advance however, there is generally some compromise (e.g. having to have a tibial post and box which may give trouble). It is also important to stress the difference between prosthetic longevity (time to failure requiring revision as monitored in the registries) and satisfaction (pain relief, improved function and the ability to do everyday activities, sport, etc.). The current aim of knee replacement surgery is to improve satisfaction and function; and only time will tell if the newer designs, and the newer implantation techniques, will lead to the same longevity as the older, more traditional designs, and with better satisfaction.
The black dotted line shows that the 10 year survival rate for a partial knee replacement is only about 85% at 10 years. The red line shows that the result for a total replacement is
about 94% at the same time frame.
Partial Knee Replacement
Total Knee Replacement
ANJRR 2019
ANJRR 2019
ANJRR 2019
Hemi-Arthroplasty - (or UKR - Uni-Compartmental Knee Replacement) This is where only one part of the joint is replaced. This is most usually performed where one side of the joint is worn out, either due to injury, or due to earlier removal of the meniscus leading to arthritis (wear) on that side. It is only suitable if the rest of the knee is in very good condition, and if all the ligaments are intact. The advantage of this procedure is that it most nearly re-creates the function of a normal knee. Part of the reason for this is that the anterior cruciate ligament (ACL - which generally has to be removed for total knee joint replacement) is left intact. As might be expected therefore, the end result can be very good; producing a knee which has a near normal, or very good, range of motion, which is usually achieved quite quickly.
This sort of knee replacement is most suitable for the inside half of the knee (the medial side - see diagram on front page) where it is often referred to as Medial Compartment Resurfacing. Like Total Knee Replacement, there is a replacement of the worn out ends of the bone with metal and plastic bearing
A (BSC) Bi-Cruciate Stabilised KneeThis design has a post which substitutes for, not only
the PCL, but also the ACL. As such, it has the best kinematics of any design. As it has a box and post
however, there may be problems related to that, but overseas results on this model are so far very good.
Cut away view showing the post and cams which provide both ACL and
PCL functionJ11 BCS Knee

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 4
surfaces; only here it is only applied just to the medial compartment of the knee. The lateral compartment is not replaced, and nor is the patello-femoral compartment (underneath the kneecap). So these areas must be normal, or very near normal.
The big disadvantage of this sort of operation is that the current range of prosthetic devices have a less predictable outcome than do total knee replacements. The Australian National Joint Replacement Registry (ANJRR) shows that survival of these prostheses is considerably less than that of a total replacement, with a significant revision rate (8%-23% - age dependent - see page 2) in the first 10 years. Whilst a few revisions occur due to failure of the prosthesis, a good number are for pain and on-going problems with the rest of the knee. In particular, for progressive wear in the other the parts that have not been replaced.
The above emphasises the importance of restricting this operation to those who really do have wear in only one part of the knee. As such, it should not be considered where there is any wear in other parts of the knee which are either symptomatic, or are likely to become so, after uni-compartmental replacement. This means that, if there is no mechanical reason to explain why there is wear in only one part of the knee (injury, menisectomy, malalignment etc.), then it should be assumed that the wear is just maximum in that part of the knee, and that the rest will follow given time. In this situation, if only one part of the knee is replaced, the remainder may then eventually wear out with time. This is something that then inevitably leads to revision to a total knee replacement.
Where there is some doubt about the remainder of the knee, an MRI scan can prove invaluable. Whilst not necessary in every case, there is no doubt that it provides valuable information which helps to make an informed decision about the type of replacement that is going to provide the best pain relief and function, in association with acceptable prosthetic longevity.
Premature failure of a partial replacement, be that due to prosthetic failure, progression of disease, or pain, can only be treated by revision to a total knee replacement. Whilst this is possible to do, that conversion is not always simple, and the end result may not be as good as if a total knee replacement had been performed in the first place. Initial decisions therefore, are important.
The bottom line for hemi-arthroplasty then, is that whilst it can provide a very normally functioning knee, the failure rates are not insignificant - being double that of a total knee replacement in the first 10 years. Importantly, only about one person in ten with osteoarthritis of the knee is really suitable for it, which means that it is very important to confirm that all the right indications and criteria are fulfilled. For this reason, experienced, high-volume, knee replacement surgeons tend to use a total replacement for most
Isolated Patello-Femoral ReplacementHere, the trochlear groove is replaced with a metal
or ceramic coated prosthesis. The patella itself is resurfaced with a polyethylene button. The left side has been put in with saw cuts whereas the right side
(black ceramic prosthesis) is inlaid as with the robot.
Seen from above Seen from the front without the patella
Trochlear ResurfacingPatella
people (90% or more), using uni-compartmental replacements sparingly. Doing this, has been shown to lead to more predictable outcomes.
Isolated Patello-Femoral ReplacementReplacement of the patello-femoral joint in isolation is a relatively uncommon procedure. Whilst it has been possible to do this for the last 30 years, the absence of consistently good results has prevented this procedure from becoming popularised. A large review of a retrospective series of patello-femoral replacements was undertaken in a unit in France considered to be one of the best in the world. This showed that if patello-femoral replacement was done, using combined patellar realignment procedures where indicated, then whilst the results were satisfactory, it turned out that the average result was slightly worse than the average result for total knee replacement.
Isolated patello-femoral replacement is quite technically demanding. The patella itself is relatively easy to replace and getting the component in the correct position is generally possible. The problem however, has been to get the trochlear component (the component that sits in the groove that the patella articulates with) in the right position. It can be lined up with the original trochlear groove reasonably easily, but getting it to meld in with all the surrounding articular surfaces, which is a difficult three-dimensional problem, is hard.
In the last couple of years, robotic technology has allowed us to position that component much more accurately than ever before. The robot that is used is not strictly a robot in that it does not actually do the surgery, but it has a navigation system that allows the component to be positioned on a 3D model of the knee that has been previously generated by mapping out the landmarks within the knee. This then guides the use of a burr to accurately create a matching defect in the underlying bony trochlear into which the trochlear prosthesis can be cemented. By doing this on-screen, and making all the adjustments on screen
Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 5
Combined Medial and P/F ReplacementHere one can see a model of a bi-compartmental
replacement. The patella with its resurfacing has been removed, and the medial tibia is yet to be replaced.
prior to bony preparation, this can be done with sub-millimetre accuracy such that (hopefully) there are no protruding lips of metal that can catch on the overlying patella.
With the advent of this newer technology, it is hoped that patello-femoral replacement can be improved to the degree where this can be a regularly recommended procedure. It is to be noted however, that most patello-femoral osteoarthritic problems relate to malalignment of the patello-femoral joint: hence, some sort of realignment may well need to be performed at the same time as the replacement; something that will hopefully produce more normal contact pressures within the prosthetic joint, and lead to less pain and better function.
Isolated P/F Replacement by SexAs can be seen, the failure rate for isolated P/F
replacement is high. The main reasons for this include failure to account for other pathology in the knee and
failure to re-align the P/F joint at the same time.
Isolated P/F Replacement by AgeAgain, it can be seen that the younger more active patients have a higher failure rate than the older
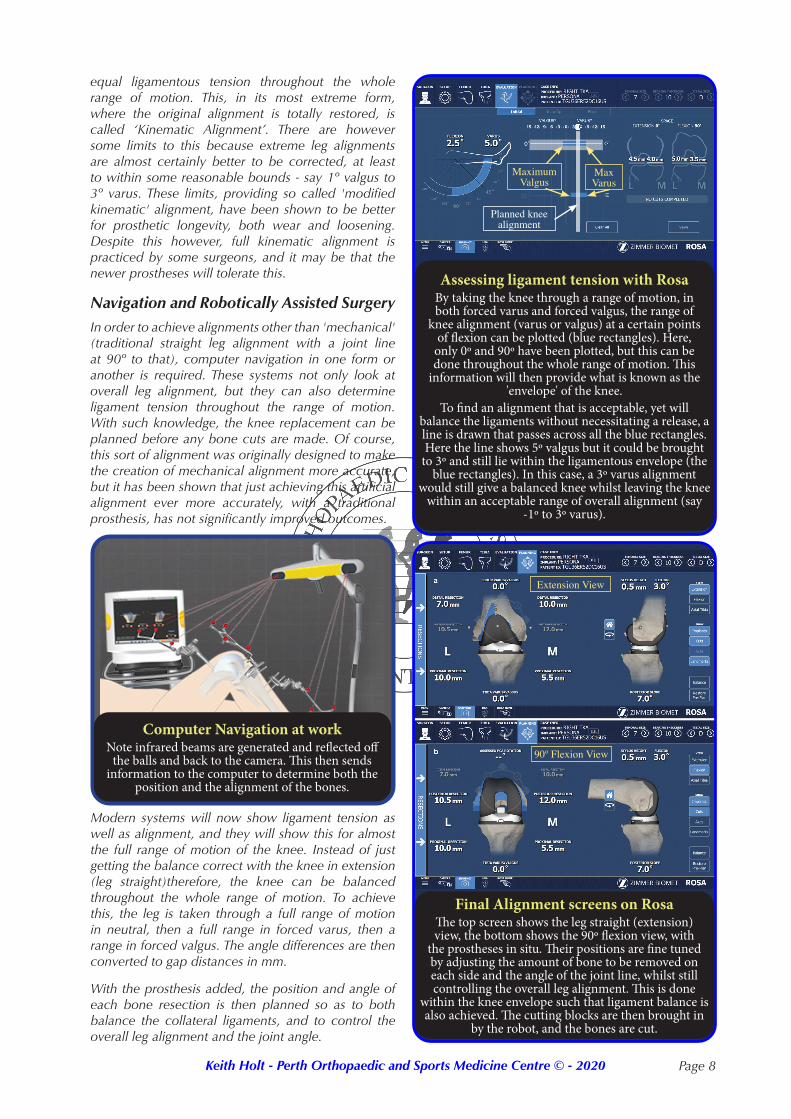
group. In addition, that failure rate does not seem to level off with time. Reason for failure of a P/F replacement
As is evident, the single biggest cause of failure is the progression of wear in the other parts of the knee.
Loosening is also a big issue, and this may be partly due to failure to correct any underlying malalignment.
ANJRR 2019
ANJRR 2019
******
Combined Medial and P/F joint replacementIt has always been thought that the knee would function better if both cruciate ligaments, and in particular the
anterior cruciate ligament, could be preserved. For this reason, when knee replacement was first conceived, it was thought that individual replacement of the medial compartment with concurrent replacement of the lateral compartment might give results that would be better than a total knee replacement. Unfortunately, the technology of the time was such that this approach was soon abandoned.
With the advent of computer navigation and robotic technology however, this approach is having a renewed surge of interest. Perhaps not so much for the individual replacement of the medial and lateral compartments done concurrently, but for that of replacing one of those compartments in combination with the patello-femoral joint. Certainly this is now technically possible to do with a high degree of accuracy, and the early results seem to be quite pleasing. Unfortunately however, it will be some years before we know whether or not this early promise is been upheld.

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 6
This absence of long term outcome data means that there are limited advocates for such procedures, and it remains to be seen whether these will become part of the standard armamentarium. Among the factors that may prevent this happening is the development of total knee replacements that either preserve both cruciate ligaments, or successfully duplicate the function of those ligaments. Given that the reason to consider combined Patello-Femoral and Medial Compartment Resurfacing is to preserve the cruciate ligaments, it may well turn out that using a Total Knee Prosthesis which substitutes for, or preserves, both of these will turn out to be a better option.
Cement or no cement? Traditionally joint replacements have been cemented into the bone. Theoretically this would seem to be a good idea. It means that the prosthesis is solidly glued into the bone at the outset, and that recovery should therefore be fairly quick. In addition, the cement seals the ends of the bone which cuts down the bleeding. Hence, there is less bruising and swelling after surgery, so motion should return more quickly.
The problem, whether cement is used or not, is that bone is living and, unlike wood, bone is constantly being removed and replaced. Whether, during this cycle of constant rejuvenation, it grows back as strong as, or even stronger than, it was depends on a number of factors, including local forces through the bone. As the prosthesis is being glued into something that is not just a biologically static material however, there is a small incidence of component loosening.
Independent of the problems however, both cemented and uncemented joints have proven to have excellent longevity, with the traditional cemented versions perhaps doing slightly better in the registry over 20 years. It is however, not quite that simple given that some ingrowth surfaces are better than others. Indeed, the porous tantalum surface (Trabecular Metal made exclusively by Zimmer for Nexgen and Persona knees)) has proven to be the best with virtually no loosening over the years. This then, at least on the tibial side (which is the difficult side to get good bonding on), seems to be somewhat better than say titanium ingrowth surfaces or Hydroxy-Appetite coated surfaces: but all types have their merits.
Dr Holt currently cements all his prostheses in except when using the Zimmer Persona - Medial Congruent Knee, which has a tantalum tibial baseplate. All femoral components and patella components remain cemented. Given that differences in results are small however, the decision to use either a cemented, or an uncemented, component remains a particular surgeons preference: and that often depends on his individual experience with the prosthesis he uses.
Patella Resurfacing or not? Resurfacing of the patella (kneecap) with a polyethylene button is one of the most controversial areas in knee replacement surgery. Most studies in the literature show that, at least in the first 5 years or so, there is little difference in the results whether the patella is replaced or not. In the last few years however, longer term results are starting to show that patella replacement may be advantageous. Kneecap pain is a not infrequent problem after replacement, whether or not it has been resurfaced. The incidence of this problem may be up to 25% in some designs when un-resurfaced, but in no designs is it completely avoided, even with a polyethylene button on the bearing surface.
Most big surveys of knee replacements are now showing that the ability to be able to climb and descend stairs is enhanced by having the patella resurfaced. Given the low complication rate of patella replacement therefore, it would seem reasonable to carry this out at the time of the initial procedure. Certainly, the advantages of this versus leaving the patella alone, are now becoming more compelling. For this reason, Dr Holt resurfaces every patella with a polyethylene bearing surface (button). This then avoids the problem of having to comeback and resurface it later if there is on-going patella pain: a procedure that in no way is guaranteed to remove the patella pain.
Femoral Component
Patella
Patella ButtonCement Line
View of the patella button from aboveThe polyethylene cannot be seen, but the cement line
around it can.
Oval versus round patella buttonThis shows alternatives to patella resurfacing. The
lower one shows the usual round patella. The upper one shows the same size patella top to bottom, but
being oval there is more coverage of the whole bone. This is only an option with a few models, but may help
pain and tracking in those.
Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 7
Anterior (Patello-Femoral) Knee PainGiven that the commonest cause of long-term dissatisfaction in knee replacement is patellofemoral pain, a lot of effort has been made to try and reduce this over the last several years. The main thrust of this has been to get the patellofemoral joint working more normally; which it does not do in a standard CR knee replacement that acts like a hinge. The medial pivot/congruent designs are helpful in that these allow the tibia to turn inwards (internal rotation) and the femur to turn outwards (external rotation) during knee flexion; although these knees do not allow the full extent of rotation that occurs in a normal knee. They do however, line up the patellofemoral joint better in flexion, which in turn decreases the sideways force on the patella that occurs if the trochlear fails to rotate across to lie perfectly underneath the patella during that activity.
alignment (be that slightly bowlegged or slightly knock kneed) rather than just making it straight. At the same time, the joint line angle can be restored such that it angles slightly outwards (valgus) like the normal knee. By doing this, the femoral component will angle slightly outwards which, in flexion, better accommodates the patella, and therefore lowers sideways forces on it.
Patello-Femoral MalalignmentFailure to correct patella tracking results in opposing forces on the patella. The patella is pushed laterally and the ‘V’ shape of the trochlear holds it in. Most
standard CR prostheses deal with this by moving the trochlear across, but that solution is only partially
successful. The shear force generated causes stress at the patella button/bony patella interface and can cause
pain.
Lateral force created by the quads
Medial
Trochlear Groove(on the end of the femur)
Correcting P/F MalalignmentDesigns that allow the tibia to internally rotate, and
the femur to externally rotate, re-align the patella with the trochlear thereby significantly reducing patella
shear forces: thus reducing pain.
Trochlear Groove
(on the end of the femur)
Alignment ConsiderationsThe other factor that is changing the way the patello-femoral joint works is the move towards so-called 'kinematic' alignment. This is where the knee is put in in such a way as to restore some of the pre-arthritic
A natural 3º valgus joint line slopeThis knee has been put in with Modified Kinematic
Alignment. The prosthesis has been implanted in such a way that it restores the 3º joint slope of the opposite normal knee. During the stance phase of walking, this
makes the joint line parallel to the floor.
The P-F Joint with a 3º Sloping JointWhen the joint slope is made to be 3º valgus (like normal), it has some consequences for the straight knee. More importantly however, it creates about
3mm of extra room under the lateral patella in flexion which significantly decreases contact forces and shear
forces. This may be important in reducing pain.
Left Knee at 90º of flexion, as seen from above
Leaving the leg at or near its pre-arthritic alignment (slightly bow legged or knock kneed), should theoretically restore the normal tension in both the medial, and lateral, collateral ligaments that existed before the arthritis and deformity set in. This then creates what is called a 'balanced' knee, with fairly
Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 8
equal ligamentous tension throughout the whole range of motion. This, in its most extreme form, where the original alignment is totally restored, is called ‘Kinematic Alignment’. There are however some limits to this because extreme leg alignments are almost certainly better to be corrected, at least to within some reasonable bounds - say 1º valgus to 3º varus. These limits, providing so called 'modified kinematic' alignment, have been shown to be better for prosthetic longevity, both wear and loosening. Despite this however, full kinematic alignment is practiced by some surgeons, and it may be that the newer prostheses will tolerate this.
Navigation and Robotically Assisted SurgeryIn order to achieve alignments other than 'mechanical' (traditional straight leg alignment with a joint line at 90º to that), computer navigation in one form or another is required. These systems not only look at overall leg alignment, but they can also determine ligament tension throughout the range of motion. With such knowledge, the knee replacement can be planned before any bone cuts are made. Of course, this sort of alignment was originally designed to make the creation of mechanical alignment more accurate, but it has been shown that just achieving this artificial alignment ever more accurately, with a traditional prosthesis, has not significantly improved outcomes.
Computer Navigation at work Note infrared beams are generated and reflected off
the balls and back to the camera. This then sends information to the computer to determine both the
position and the alignment of the bones.
Modern systems will now show ligament tension as well as alignment, and they will show this for almost the full range of motion of the knee. Instead of just getting the balance correct with the knee in extension (leg straight)therefore, the knee can be balanced throughout the whole range of motion. To achieve this, the leg is taken through a full range of motion in neutral, then a full range in forced varus, then a range in forced valgus. The angle differences are then converted to gap distances in mm.
With the prosthesis added, the position and angle of each bone resection is then planned so as to both balance the collateral ligaments, and to control the overall leg alignment and the joint angle.
Assessing ligament tension with RosaBy taking the knee through a range of motion, in both forced varus and forced valgus, the range of
knee alignment (varus or valgus) at a certain points of flexion can be plotted (blue rectangles). Here,
only 0º and 90º have been plotted, but this can be done throughout the whole range of motion. This
information will then provide what is known as the 'envelope' of the knee.
To find an alignment that is acceptable, yet will balance the ligaments without necessitating a release, a line is drawn that passes across all the blue rectangles. Here the line shows 5º valgus but it could be brought
to 3º and still lie within the ligamentous envelope (the blue rectangles). In this case, a 3º varus alignment
would still give a balanced knee whilst leaving the knee within an acceptable range of overall alignment (say
-1º to 3º varus).
Final Alignment screens on RosaThe top screen shows the leg straight (extension) view, the bottom shows the 90º flexion view, with
the prostheses in situ. Their positions are fine tuned by adjusting the amount of bone to be removed on each side and the angle of the joint line, whilst still controlling the overall leg alignment. This is done
within the knee envelope such that ligament balance is also achieved. The cutting blocks are then brought in
by the robot, and the bones are cut.
Maximum Valgus
MaxVarus
Planned knee alignment
Extension View
90º Flexion View

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 9
Robotically Assisted SurgeryNote that this is based on computer navigation. The near arm contains an infra red light source and the
camera. The silver balls which the light reflects off can be seen attached to the leg. On the other side of the table is the actual robotic arm that will bring in the
cutting blocks, and position them in line with the on screen plan. Cuts can then be made.
Once the above has been done, the cuts can be made as planned and the prosthesis inserted. The alignment and balance can then be re-checked and altered as necessary, making sure that the knee can go through a full range of motion including full extension (getting the knee fully straight, which is often something that is lost with progressive arthritis).
Using standard navigation tools alone, but current generation ones, the cutting blocks can be affixed to each bone in turn under the control of the navigation system. If a Robot is used, it will either manoeuvre the cutting blocs into place for fixation to the bones, or it will hold a saw in place directly. In neither case does the robot actually do the surgery. The surgery is robotically assisted, not done by the robot. Hence these are referred to as 'Passive' Robots rather than 'Active', noting that they do not really fit the established definition of a robot.
Is Robotic Surgery Better?Robots can more reliably achieve ligament balance throughout the full range of motion than other methods. This is to do with the fact that they have the latest versions of a computer navigation system rather than the robot actually being able to help. It is the package, not just the robot, that is important. Nevertheless, these systems are already showing benefits (but which are not yet proven) for partial knee replacements (uni-compartmental and patello-femoral), and it is expected that the newer systems will eventually lead to better and more reliable results in Total Knee Replacement. Currently however, this is not the case. The reason that robotically assisted systems have not yet been shown to improve outcomes for Total
Camera
Robot
arm
Planning Screen
Knee Replacement is that every different type of knee replacement seems to require a slightly different ligamentous balance and, surprising though it may seem given how long we have been doing this operation, the optimal balance of each various type of knee is still unknown. Use of robotic assistance, which is based on computer navigation, is now providing large amounts of data which, along with outcome follow up data, should ultimately provide the information that is required for scientific analysis. The hope is that, with such analysis, guidelines will become established to help determine how a particular type of knee should be balanced (how tight the ligaments should be), and in what alignment. At this stage however, this information remains some years away.
Choosing a robotic system is important because currently, each system is approved only to implant the brand of knee that the company selling the robot manufactures. It is important to know that while these systems could be programmed to put in any brand of knee, they are sold on the basis that they will not be so programmed (the profits come from the prostheses and not the robots - even though the latter are very expensive). It is therefore important to know which robotic system a given surgeon uses in order to look at the outcomes of the particular knee design related to that system. Such outcomes can be found in various registries, but the most comprehensive, and best kept one, is the AOA-NJRR (Australian Orthopaedic Association - National Joint Replacement Registry). It is very important to separate out claims of a better robotic system from claims of a better prosthesis because a ‘this years’ robot will not compensate for an older style prosthetic design with poorer satisfaction and/or premature failure.
Understand that a low revision rate is not the same as a high satisfaction rate. A given prosthesis may not have excellent satisfaction rates (traditionally about 80% good to excellent only) but, unless it is bad enough to come to revision, it will not show up in the registry as a poor outcome. This is because the registries were never set up to determine satisfaction: their measurement of failure is revision. They do not collect PROMS (Patient Reported Outcome Measures), meaning that they do not have any record of how well a given knee replacement performs, how suited it is to various activities such as stair climbing or kneeling, how much knee flexion or extension is possible, or even how sore it is at various time points after surgery. Only recently have registries started looking at PROMS, so any meaningful results are some years away.
Unless a replacement is bad enough to come to revision, the registry presumes that it is doing okay.Revision is defined as being where one or more components are changed. Hence, a subsequent

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 10
arthroscopy, patella re-alignment, synovectomy, or similar, will not be detected. Clearly therefore, there are many problems that decrease satisfaction rates but which are not captured by registries.
Joint StabilityJoint instability is a problem which can be improved by better prosthetic design and better ligamentous balance. We know that there is inherent instability in a traditional CR knee (posterior Cruciate ligament Retaining, but anterior cruciate ligament sacrificing). This design requires very good ligamentous balance to control laxity in mid-flexion and, even with advanced navigation and robotically assisted surgery, this cannot always be achieved. Whilst such knees may not feel ‘loose’ as such, they often have on-going pain (usually patello-femoral) and/or general dissatisfaction.
Increasing stability by using different prosthetic designs can significantly improve these symptoms. The literature shows that by moving to a PS knee (posterior cruciate ligament sacrificing but with inbuilt prosthetic Posterior cruciate ligament Stabilisation - and always with the ACL being sacrificed as well, as it is in almost all Total Knee Replacements), instability can be improved; but there are some problems that are then introduced because of the nature of the design of these knees. In essence, those problems relate to the central post required for posterior cruciate ligament function, and the central box in the femoral component that houses that post and makes it work.
Recent literature now shows that the most stable design is that of the medial pivot (medial ball-and-socket) joint. This provides the highest grade of stability throughout the range of motion, and it may be this, rather than anything else, that has led to the high rates of satisfaction that this design of knee provides.
In the graph: • LCS is a mobile bearing design
• Triathlon is a (traditional, standard) CR design
• MRK and SAIPH are medial pivot designs
Whilst traditional knee replacement has only shown an 80 to 85% satisfaction rate in all registries, the use of medial pivot/congruent designs, alignment restoration (albeit within limits), joint line restoration, and ligament balance all seem to improve satisfaction with new series suggesting over 95% good to excellent satisfaction in the medium term. These new advances therefore, seem beneficial.
TKR StabilitySagittal stability in four different knee designs. Walter,
Shimmin, et. al. Presented at ISTA, 2014
Overall Summary
Making Knee Replacement Better
Things to consider to improve satisfaction:
1. Design / type of prosthesis
2. What alignment is chosen for implantation
3. How tight the ligaments are made
4. What range of motion is achieved at the time of, and following, the surgery
5. What pain management and post operative protocol is used
6. What rehabilitation protocol is used
7. What patient related factors exist
The influence of contemporary knee design on high flexion 2: a kinematic comparison with the normal knee. Morra, Rosca, Greenwald and Greenwald, 2009
In this, the second of 4 articles on these matters co-authored by four authorities on knee replacement, and presenting computer analyses of various available knee designs, the following statement was made.(Seth Greenwald quoting G. Engh - 2009) “A knee arthroplasty, that closely resembles the feel and function of a healthy un-operated knee, is increasingly identified, by both patients and clinicians, as an objective of knee replacement surgery.”
With the passage of time, and with evolving prosthetic design and implantation techniques, this prophetic statement, increasingly, is being regarded as likely to be correct.
Dr Holt's Preferred Designs
• The Zimmer Persona Knee in it's Medial Congruent form. It has slightly less lateral sided freedom, but comes with Rosa. It has very good results.
• The Medacta GMK Sphere. This is a Medial Pivot design with a fully unconstrained lateral compartment to allow maximal tibial rotation. It has very high satisfaction rates.

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 11
A pre-operative clinic is run by the hospital, and it is important to try and get to that so that your hospital stay will be as smooth as possible. The hospital will contact you, and arrange this with you directly. During that clinic, pre-operative tests (blood tests, ECG etc.) will be carried out, and an orientation will be arranged so that you are familiar with the procedure and the post operative care. When surgery is booked you will be given, or given a script for, anti-bacterial ointment for your nose and a chlorhexidine solution for your skin to lower the bacterial count before surgery.
https://www.keithholt.com.au/resources/knee-replacement/Knee-Replacement---The-Journey-2020.pdf
Drug issues must sorted out in time for your surgery, and some of these will need a week or so to get right. For a general review of what to do, with what medications and when, please look at the information sheet on Dr Holt's website (Adjusting Your Medications in Preparation for Surgery).
https://www.keithholt.com.au/resources/general-info/Pre-op-Drug-information-2019.pdf
Sleep apnoea & lap bands can both be an issue with surgery. For those with sleep apnoea and for those who have a laparoscopic band in situ, there is information on the website (Lap banding & sleep apnoea info).
https://www.keithholt.com.au/resources/general-info/Lap-banding-&-sleep-apnoea-info-2019.pdf
Admission and time in hospital: For replacement surgery, health funds now insist on admission into hospital on the day of surgery whenever possible and, for cost reasons, they discourage earlier admission. Because of the DRG (Diagnostic Related Group) system that health funds now use, they will only pay for a certain number of days in hospital for a given procedure. For single knee replacement this is 3-4 days, and for bilateral replacement, it is 4-5 days: and this time is being reduced each year. This means that if you come into hospital a day early, you will have one less day to recover before your fund will stop paying for you.
Average length of stay for knee replacement has been coming down significantly over the last several years. This is particularly so because of the nerve blocks described below, and because of our ability to perform most replacements without the use of a tourniquet (which causes pain in its own right). Currently, those with a single knee replacement are frequently getting home on day three (range 2 to 4), and those with bilateral knee replacements are getting home on day four (range 3 to 5). (Day of surgery = day 1)
Anaesthesia: Our current preference is to use general
anaesthesia with adjunctive nerve blocks and local anaesthetic infiltration into the joint. The nerve block of choice is a so-called 'adductor canal' block which is performed in the mid to upper thigh. This blocks the saphenous nerve which supplies a good deal of the front of the knee where the wound is. In general, a catheter is left in situ so that local anaesthetic can be infused continuously for 2 to 3 days. It can also be topped up with stronger anaesthetic where necessary. This has proved extremely effective in reducing pain post surgery.
Blood transfusion is rarely necessary in knee replacement, even in bilateral simultaneous knee replacement. If there is chronic anaemia present, then iron stores can be measured and, if low, an iron infusion can be arranged. This can take a couple of weeks to work but it significantly helps recovery and decreases the chance of requiring a subsequent transfusion.
The routine use of tranexamic acid, both systemically and into the joint to prevent bleeding, has also proved to be a major factor in reducing the need for blood transfusion.
Knee replacement - the procedureThe procedure of knee replacement can be performed with a short anaesthetic (generally 1 hour per knee). The operation is done through a wound on the front of the knee and leaves a long, straight, vertical scar which fades over a period of about 1 year.
The alignment of the leg, and the positioning of a Total Knee Prosthesis, is always done using high end computer navigation, with or without a robotic interface: and that depends on the prosthesis chosen. Uni-Compartmental Replacement and Patello-Femoral Replacement is always done with the aid of a robot.
Knee replacement - post surgeryWard stay: During your hospital stay, physiotherapists will help you regain motion in the knee, and will get you walking again. The aim is to get over 90º of motion by the time of discharge, to be able to walk to the toilet or fridge and back, and to be able to get in and out of bed by yourself. Most people will use crutches for 2 weeks, but these are not compulsory.
Pain medication: Getting adequate pain relief that does not cause nausea, and does not interfere with bowel function, can be quite difficult and, in some people, this may take a fair bit of change and adjustment to their drugs. We would generally hope that this can be all sorted out by the time of discharge.
Standing may happen on the day of surgery but will certainly have happened by the next day.
Walking with a frame usually begins on day 2, but the aim is to progress to crutches early on.
Procedure and Progress
Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 12
Driving is allowed when you can manage without crutches. This usually happens at about the 6 week mark and, for legal reasons, 6 weeks post surgery seems to be about the right time.
Time off work, on average, is 2 - 3 months, but may be less if the job is relatively sedentary. It is best not to push to get back to work too early, and not to try and be better than average. Rest is a very important element in recovery, and is essential to allow early reduction of swelling. This, in turn, is important to maximise the amount of flexion that the knee can achieve post surgery.
Physiotherapy
Whilst in the hospital there will be on-going physiotherapy to help with recovery. Our current preference is for the 'Mini-Bike' regime which has been shown to make early recovery more rapid. This involves getting a 'Mini-Bike' (K-Mart ~$29)and bringing it in to the hospital. When leaving the hospital, a home program is provided. In some instances, further physiotherapy will be ordered but, for a lot of people, this is not necessary.
Home help etc.
If you think you are going to need home help, or the installation of home aids, the earlier these are organised the better so that it does not delay your discharge. The pre-op clinic is a good place to start this process off, and the staff there can advise if asked.
Rehabilitation
Most big hospitals now have a rehabilitation unit. This is run by the Geriatricians and space is always limited. In order to be considered for a period in the rehabilitation ward, you have to be assessed by those physicians: and the reason for admission into their care has to be medical. This cannot be organised ahead of time, and you cannot be pre-booked into this ward. If it seems necessary to prolong your stay because of medical reasons however, then Dr Holt will have one of the physicians come up to the Orthopaedic ward to assess you.
Please note that not all health funds will support a period in a rehabilitation ward and, even those that do, require a documented medical reason before they will cover such. Living alone, wanting the knee to be better than it is, wanting physiotherapy in hospital rather than at home, are all non-medical reasons - so these won't get you to the rehabilitation ward. Organising a family member or a friend to help you after discharge, even if they just check on you by phone, is important. Please look at the information sheet on Dr Holt's website (Total Knee Replacement - The Journey) for more information on this.
https://www.keithholt.com.au/resources/knee-replacement/Knee-Replacement---The-Journey-2020.pdf
Expectations and results
Pain Relief is, for most people, the single biggest reason to consider replacement: and the results of larger series do indeed show that the vast majority are pain free or have minimal aches and pains in the longer term. Overall however, it must be said that a knee replacement is not quite as pain free as say a hip replacement, and does not recover as quickly. This may be due to the fact that the knee is relatively superficial, and not surrounded by muscle like the hip. It may also be because of the complexity of this joint in comparison to a hip. Either way, the results, at least in the short term (the first year), are probably not quite as good as a hip replacement. However, with the newer prostheses, and the newer implantation techniques, the results are getting better, and the recovery rate is improving.
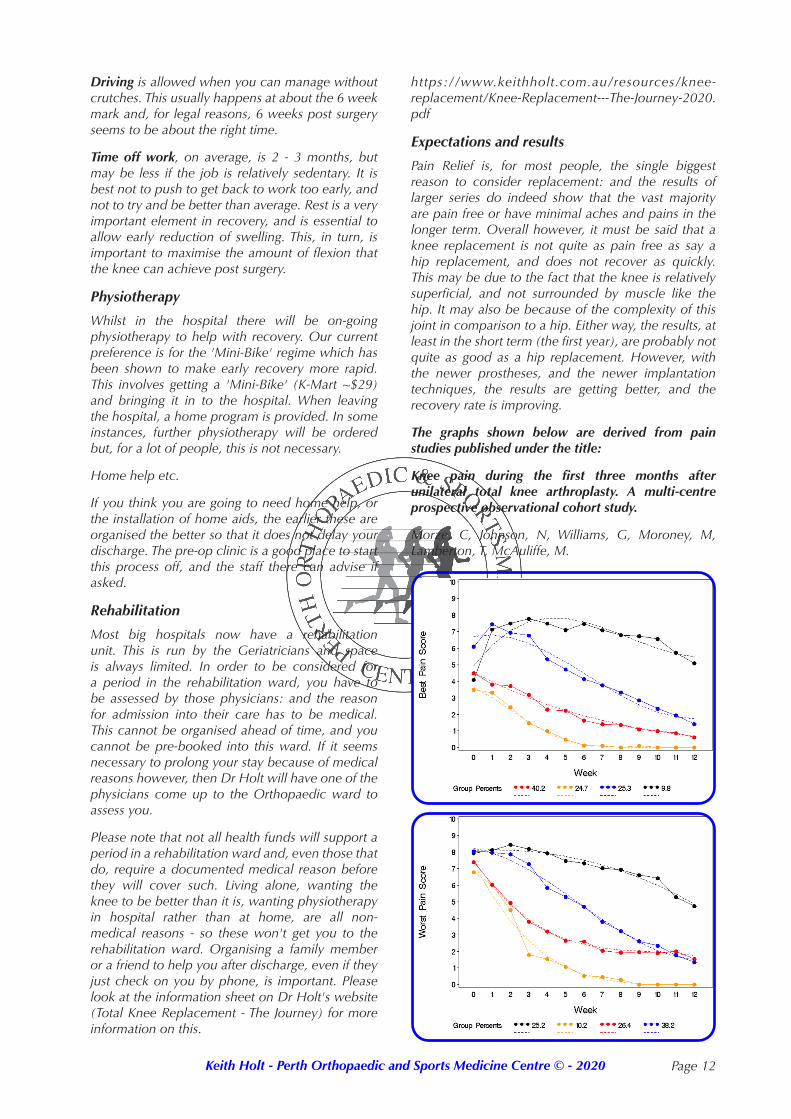
The graphs shown below are derived from pain studies published under the title:
Knee pain during the first three months after unilateral total knee arthroplasty. A multi-centre prospective observational cohort study.
Morze, C, Johnson, N, Williams, G, Moroney, M, Lamberton, T, McAuliffe, M.
Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 13
The concern with knee replacement is the group that have difficulty managing their pain (black line ~10%), and who still have 5 out of 10 'best pain' scores at 3 months. In the first 6 weeks this group are barely better than they are in the first week post surgery.
This 'worst' group is in complete contradistinction to the group at the other end of the scale who have almost no pain by 6 - 8 weeks (yellow line ~10%). The reasons for this are unknown, and it does not always seem to relate directly to swelling, stiffness or other operative factors, albeit that these may be the cause of some of the problem. One of the indicators for being in either the best or the worst group, is the degree and extent of arthritis that exists pre-operatively. We know for instance, that those people who have tolerated a really bad knee for a long time, will tolerate a knee replacement: and hence are expected to do well. On the other hand, those who come to replacement with significant on-going pain, and yet do not have a particularly arthritic knee, generally will not do so well. Obviously this has something to do with pain tolerance, but other factors are almost certainly at play as well: and fortunately, this guide is not always correct.
A lot of work has been done to try and improve the short term figures and to make the initial few weeks better. Various strategies have been implemented to try and help in those early weeks and, if the above study was to be re-done, it is likely that the outcomes would now be seen to be better. This is particularly so since the introduction of various interventions and techniques that are now part of Dr Holt's standard treatment plan.
The longevity of a knee replacement is probably the best of any joint that can be replaced. We know from the ANJRR (Australian National Joint Replacement Registry) that prostheses implanted in the early 1990s survived for 15 to 20 years before they all needed to be revised. The current prostheses, particularly those with a ceramic coating on the femur, in association with highly cross-linked polyethylene on the tibial tray, test out in the laboratory to over 30 years (Verilast - Smith & Nephew). The introduction of vitamin E infused polyethylene (Zimmer and others), which is used to decrease oxidative delamination of the material, also shows very low rates of wear - again however, in the laboratory. Of course, only time will tell if these newer prostheses are going to last that long when implanted, but there is every indication that this might prove to be the case.
Range of motion is variable and unpredictable, even from a left to a right knee in the same patient. Certainly all knees behave differently, and the results of replacement vary because of many different factors. Suffice it to say that, at one year post surgery, 120º of flexion (bend) is average. Being an average however, means that for every patient who achieves 140º, another will only get 90º. Maximum flexion is
rarely achieved under 12 months and improvement may continue for up to 24 months post surgery. To end up with less than 90º of flexion however, is very uncommon but, if this happens, there are things that can be done in the post operative period to help.
It is important to realise that knee motion is restricted by the arthritic process. It is also important to understand that it is difficult to achieve a better range of motion following surgery than existed pre-operatively. Hence, a knee can be left too long before opting for replacement. The corollary is that, if you only have 90º of flexion pre-operatively, then it is unlikely that you will reach the average range of 120º post-operatively.
The aim, for the most part, is to get as much motion as possible after surgery because this allows more activities to be possible. As a minimum, 90º of flexion is required to get in and out of a car with some facility, and to sit on a chair comfortably. To ride a bike usually requires 105º to 110º, and to climb stairs requires a similar range. To climb a ladder may require 120º and, only if more range than that is obtained, can squatting down be contemplated. For most people, the thought of being unable to squat down or kneel is of little concern compared to the benefits of pain relief and mobility. However, it may be very important in some trades, and particularly in those who are part of a religious group where kneeling for prayer is the custom.
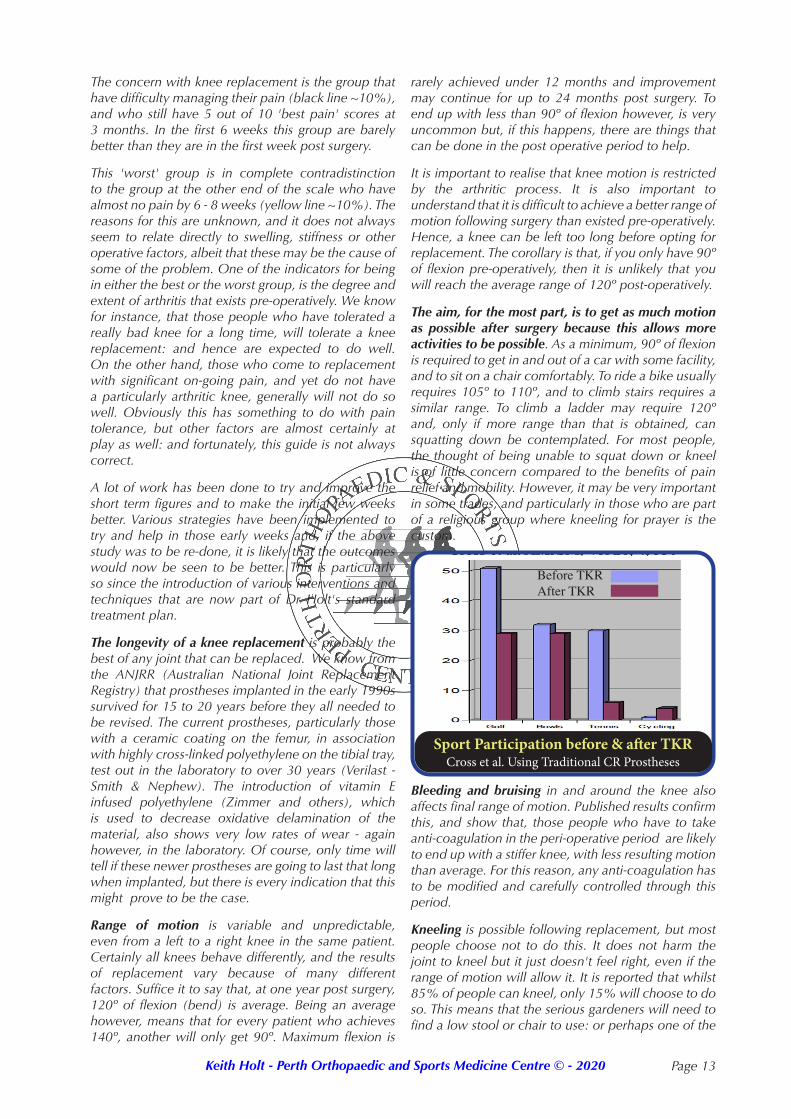
Sport Participation before & after TKRCross et al. Using Traditional CR Prostheses
Before TKRAfter TKR
Bleeding and bruising in and around the knee also affects final range of motion. Published results confirm this, and show that, those people who have to take anti-coagulation in the peri-operative period are likely to end up with a stiffer knee, with less resulting motion than average. For this reason, any anti-coagulation has to be modified and carefully controlled through this period.
Kneeling is possible following replacement, but most people choose not to do this. It does not harm the joint to kneel but it just doesn't feel right, even if the range of motion will allow it. It is reported that whilst 85% of people can kneel, only 15% will choose to do so. This means that the serious gardeners will need to find a low stool or chair to use: or perhaps one of the

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 14
Skin numbness on the outside of the scar is usual after surgery. This is because the small superficial skin nerves that supply that area come from the inside of the leg and are cut during the approach to the knee. Whilst this is initially quite noticeable, over a 1 - 2 year period some sensation appears to return. Ultimately this area becomes less numb and, as a consequence, becomes less noticeable.
Residual pain is rarely a major problem. Sometimes however, residual aches and pains occur which, despite the passage of 9 - 12 months, persist and are difficult to explain. Some are due to loosening, some to infection, some to mechanical problems and so on. Most however can be diagnosed, and most can be helped or treated. The problem is that this process may take time, and indeed, it is often a matter of excluding problems, rather than a definitively identifying one, that leads to a diagnosis or a treatment option. This explains why it often takes months to work out why some replaced joints are still symptomatic, and even longer to fix them.
Stiffness is perhaps the most common problem initially. Given time however, most problems relating to this resolve. Indeed, the range of motion will continue to improve for 12 or more months. If at the 2 month mark however, the knee does not have 90º of bend, then a manipulation under anaesthesia can be performed. This is generally a minor intervention and usually does not make the knee sorer. What it achieves is a breakdown of the restricting scar which, in turn, makes the knee feel freer and less sore. The best time for this is at about the 2 month stage, but it can be left as long as 3 months in some instances. After 3 months the scar gets quite thick and strong, making it harder to break down. This then makes manipulation more difficult and more risky. Accordingly, it is rarely performed after the 3 month mark.
If the knee still ends up with an inadequate bend despite a manipulation, then it may be possible to arthroscopically remove the restricting scar from within the knee joint. Importantly, this is usually not performed before the 9 month mark for fear of stirring the knee up and making it scar more. Indeed, it seems that the optimal time to remove this scar is between 9 and 15 months post surgery; once the knee has settled down and become quiescent. By doing this, increased motion can usually be obtained and, although some
of that motion may subsequently be lost again, it is usual to maintain over 90 degrees of flexion. Even if not much more motion ensues however, the removal of scar will often make the knee feel less stiff and tight, and this in itself can be a worthwhile improvement.
Clearly, the biggest problem with the arthroscopic approach, is that it has the potential to introduce infection into the knee: hence, it is only offered if the potential for improvement seems to justify that risk. Of course, antibiotics are used in the peri-operative period with this surgery, but this is not an absolute guarantee that an infection cannot be introduced.
Residual malalignment (an excessively crooked knee) is not very common with today's alignment systems. It is important to note that, whereas it was once thought important to make the knee perfectly straight (so called 'Mechanical Alignment'), it is now thought to be more important to balance the ligaments on each side of the knee such that they are not too loose nor too tight (so called 'Kinematic Alignment'). In essence, this means taking the knee back to an alignment similar to the one that existed prior to the deformity caused by the arthritis rather than making the leg dead straight.
Instability is uncommon. particularly with a medial pivot/congruent knee. Occasionally, ligament balance can end up being sub-optimal, and this is sometimes due to the requirement for releases to be used to help with alignment and balance. If the knee cannot be made intrinsically stable then a prosthesis with extra inbuilt stability can be used instead of a standard prosthesis. This can be either a Posterior Stabilised (PS) Knee, a so-called Constrained Knee, or a Hinge Knee.
Swelling is normal within the knee and may last 6 - 9 months. Swelling of the leg and foot also occurs, and sometimes this is more chronic. Generally, this latter problem relates to poor venous or poor lymphatic drainage after surgery. Anyone with bad veins, or who has had swelling in the legs before hand, is at significant risk of having longer lasting, or even permanent, swelling in the leg afterwards. Fortunately however, even when this occurs, it is usually relatively minor.
Infection is fortunately uncommon. In the NJRR it is reported in about 0.25% in the first 3 months but increases with time (see page 2) to about 1.2% by 10 years. It is however, higher in those at risk (diabetics, haemophiliacs, those on anticoagulation and so forth). Dr Holt's acute infection risk (in the first 3 months) is closer to 0.1% - i.e. 1 in 1000.
To decrease the risk, all patients are given antibiotics at the time of, and after surgery, and the cement that is used generally contains an antibiotic that leaches out into the joint over several weeks. Special lamina flow air-conditioning systems are required for this type of surgery, which means that not all hospitals, and
Problems and Complications
other fancy devices that are made specifically for this purpose.
Squatting is also difficult, mostly because of the limitation of knee bend that results from the procedure. Nevertheless, most people who come to replacement cannot squat pre-operatively, so for them this will not be a change.

Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 15
not all operating theatres, are suitable for this. Other precautions, such as the wearing of fully enclosed space suits, are also taken.
As discussed above, whilst the knee can become infected at the time of surgery, late infection is probably more common. It is thought that the organisms reach the prosthesis through the blood stream and then land on the metal. Because the metal is not living, the organisms can hide from the body's defences, and hence, can grow and multiply to the extent where a significant infection develops.
If infection occurs, and it is treated acutely, it can generally be managed with a washout of the knee and antibiotics. It is however, hard to totally eradicate the infection this way, which can sometimes mean life-long suppression with antibiotics. Usually, the polyethylene liner also needs changing to improve the chances of success. The reason for this is firstly, to get to the dead space between the polyethylene component and the underlying metal base plate where organisms can hide, and secondly, because the infective organisms can attach to the polyethylene and be difficult to remove from it. This latter method is thus preferred to a washout.
If this approach does not work, or the problem is chronic, then a 2 stage revision can be undertaken. This is a major undertaking, initially requiring removal of the prostheses and implantation of cement spacers (which contain antibiotics which leach out into the knee over time). This is combined with prolonged intravenous antibiotic therapy which typically lasts 2 months. The antibiotics are then stopped and, if the infection does not return or flare up, the spacers are removed and a new knee is inserted. This has a high chance of success but it is not 100%, and the new knee may never be as good as the first.
D.V.T.'s (Deep Venous Thromboses) can occur, and are relatively common if no preventative treatment is given. These represent clots in the deep veins of the leg, usually the calf. They may occur at the time of surgery and then get slowly bigger over several days, or they may come on sometime thereafter. If symptomatic, it is usually as an ache in the calf at the back of the leg. If this is thought to be occurring, then a doppler (ultrasound) scan can be used to investigate it, and, if confirmed, appropriate treatment then organised.
It is to be noted that not every clot in a calf vein is a deep venous thrombosis. A number of these events occur in more superficial veins, such as the soleal veins, where they are unlikely to spread the lungs: and therefore may not need the full anticoagulation required to treat a true deep venous thrombosis.
P.E. (Pulmonary Embolism) is a condition in which clots that form in the peripheral venous circulation spread to the lungs and block the small vessels of the lungs. By doing this they can create a significant block
to the circulation of the blood through the lungs, and hence can reduce the amount of oxygen that is taken up from the lungs into the bloodstream. This is a rare event but does represent a major and serious complication of this and other lower limb surgery. In the majority of cases, like DVT's themselves, it is treatable by thinning the blood. This prevents new clot from forming and allows the body time to slowly dissolve the clot that is present.
Because of the risk of these complications, almost all patients will be given some form of preventative treatment. This usually means a thinning of the blood with a low molecular weight heparin, such as clexane, for the first few days. After this, an oral anti-coagulant can be used, and mostly, this just means low dose aspirin (100mg taken once a day - e.g. Cartia - for 6 weeks).
If the risk is higher than normal, then other treatment may be advocated. This most usually means changing over to a factor 10a inhibitor such as Rivaroxaban (Xarelto), or Apixaban (Elequis), both of which are approved on the PBS for use after knee replacement. These drugs come in tablet form, and are used for 15 days after the clexane has been ceased.
We have previously tried to use factor 10a inhibitors immediately after surgery rather than clexane injections, but they can cause excessive bleeding and bruising if given too early. For that reason, clexane is still used for the first few days before moving to an oral agent.
The above prophylaxis significantly decreases the number of D.V.T.'s but, as a consequence, it does increase the amount of bleeding and bruising; albeit to a variable degree. Unfortunately, even though such partial anti-coagulation lowers the chance of getting a D.V.T. to less than 5%, the risk of getting a pulmonary embolus may be unchanged (currently around 1%).
Studies show that only full anticoagulation can change the incidence of P.E., and such treatment has serious complications of bleeding which are both detrimental to the knee in the longer term, and pose significant risks of bleeding elsewhere in the body. Hence, whilst Surgeons in the United States once used to advocate full anti-coagulation after Joint Replacement Surgery (to try and prevent pulmonary embolism at all cost), there now seems to be a more realistic approach similar to that advocated in this country. This emphasises that the risks should not exceed the benefits.
Travel after surgery: It is generally thought that the risk of getting a DVT or a PE is increased out to at least three months following surgery. Accordingly, if travel is contemplated in that period of time, then appropriate measures need to be taken. For short to medium distance car travel, the standard post-operative low-dose aspirin should be adequate. Longer car journeys, like aeroplane journeys, may require more aggressive
Keith Holt - Perth Orthopaedic and Sports Medicine Centre © - 2020 Page 16
anticoagulation such as the use of rivaroxaban or apixaban. In addition, flight socks or flight stockings, are advised.
Fat embolism risk is highest in the old alignment systems that require rods to be passed up the centre of the bones (intra-medullary) thereby increasing the pressure in the marrow cavity, and hence, squeezing the fat into the venous system. It does not happen to any extent with current computer navigation systems. It may however, be seen with the use of stems in revision surgery.
Foot drop occurs when one of the nerves that cross the side of the knee is stretched, usually in correcting a very valgus (knock kneed) knee. This occurs some 2 - 4% of the time and usually is transient, generally resolving over a period of days to weeks. Long term or permanent foot drop is rare, virtually all having recovered by 3 months.
Vascular injury is uncommon, but the artery at the back of the leg, the one that supplies all of the leg below the knee, is just millimeters behind the exposed back of the knee: theoretically therefore, it is at risk. The reality however, is that direct injury to this is rare, most problems relating not to surgical mis-adventure, but to poor blood supply in the first place. This particularly applies to smokers and diabetics and, if the blood supply to the foot in these people is poor, then the limb is at some risk. Despite this however, problems are rarely encountered, hence it would be unusual for poor circulation to actually preclude replacement surgery.
Failure of the prosthesis can occur for various reasons but, in the longer term, it usually relates to wear of the polyethylene (plastic) component. It is likely however, that modern polyethylene will last at least 20 years (and maybe even 30) if the knee is well looked after. The polyethylene undergoes straight forward mechanical wear and hence, younger more active people will wear it out more quickly than older more sedentary people. That having been said, in most prosthetic systems, worn plastic can be re-replaced without having to replace either of the metal components.
Debris from polyethylene wear may cause reactions in the tissues about the replacement. In its mildest form this means some irritation of the synovial lining of the knee causing minor aching and swelling. This is usually the first real sign of wear and should indicate the need for a review of the knee to see if polyethylene revision is indicated. This process can go on for months or even years before any significant damage is caused, but sometimes these signs can appear quite late in the process, suggesting that an earlier review rather than a later one, is a good idea.
Occasionally, if left too long, the plastic can wear right through, thus causing the metal components
to articulate directly on each other. This in turn leads to scratching and wearing of the metal components, which then have to be replaced as well. It also causes metallosis whereby the metal debris particles not only fill the joint cavity, but seep out into the soft tissues: thus making them all black. The problem with this is not only the difficulty in removing all the metal debris without sacrificing a good deal of the soft tissues, but also the tendency for some of those metal ions in the soft tissues to be taken up into the bloodstream. Of these, chromium and cobalt are the most significant, both being heavy metals which, in high doses, are toxic. This is now a rare complication, and tends only to be seen with the old-style polyethylene components (non-cross linked) sterilised in the presence of Oxygen. Not many of these components remain in use given that most of these problems were solved in the mid 90s.
Osteolysis (bone dissolution) and component loosening is, fortunately, very uncommon in knee replacement: and it is predominantly associated with the older style polyethylene components and not the newer 'highly cross-linked' ones (where radiation has been used to fuse the polyethylene molecules together to increase strength) and the 'vitamin E infused' ones.
Essentially, when wear occurs in the polyethylene component, small particles of plastic debris are distributed throughout the joint. These debris particles incite the body to make chemicals (prostaglandins) in order to try to remove or dissolve those particles. As one can imagine however, the plastic is relatively immune to this sort of attack, whereas the bone is not. Hence, with time, the bone around the edges of the prosthesis may gradually be eroded, eventually leading to large cysts in the bone and loosening of the components. Should this happen to a significant degree then, eventually, either the replacement will come loose, or the bone will fracture, or both.
This situation requires a full revision of all components, and possibly some bone grafting of any cysts. It means using revision prostheses that include stems, with or without augments, to make up bony deficiencies. In addition, because the soft tissues and ligaments are often damaged, the prosthesis that is chosen may well need to be constrained to provide extra stability; or even a hinge if ultimate stability is required.
Knowing the above, it is important to realise that, if there is any suggestion of wear (increased pain and swelling), then early consultation should be sought.
SummaryKnee replacement is a commonly performed and generally very successful procedure. It does have complications but most of these can be avoided, minimised or treated. For those with severe arthritic pain, the risks are generally well outweighed by the benefits.