-
7/31/2019 Kimberly D. Williams Master's Thesis
1/62
No Health Without Mental Health:
Innovative Solutions to Creating Change in Behavioral Health
Care
A Thesis
Submitted to the Faculty
of
Drexel University
by
Kimberly D. Williams
in partial fulfillment of the
requirements for the degree
of
Master of Public Health
May 2012
-
7/31/2019 Kimberly D. Williams Master's Thesis
2/62
Copyright 2012Kimberly D. Williams. All Rights Reserved.
-
7/31/2019 Kimberly D. Williams Master's Thesis
3/62
iii
ACKNOWLEDGMENTS
I would like to thank my advisor, Dennis Gallagher, MA, MPA.
Theopportunity for me to participate in this project would not have
been possible withouthis recommendation. I am truly indebted and
thankful for his generous guidance,motivating questions, thoughtful
feedback, and unwavering support to both the overall
project as well as the completion of this thesis.
I would like to express my appreciation and thanks to Joe Pyle,
MA of theThomas Scattergood Behavioral Health Foundation for
spearheading this project andinitiating the collaboration with
Drexel University. His commitment to theadvancement of behavioral
health care through collaborative and innovative effortshas been
truly inspiring.
Additionally, I would like to thank Jason D. Alexander, MA of
Capacity forChange, Larry Geiger of Geiger Design, and John A.
Rich, MD, MPH of DrexelUniversity School of Public Health for their
invaluable contributions throughout theentire course of this
project.
I would like to extend my gratitude to the preeminent community
stakeholderswho generously offered their time to participate in our
key informant interviews.Their invaluable feedback regarding the
current status behavioral health care elevatedour project as well
as my personal knowledge to a level of appreciation and
awarenessfor which I am very grateful.
Special thanks to Arthur C. Evans, Jr., PhD of the Philadelphia
Department ofBehavioral Health and Intellectual disAbility Services
for his additional support andendorsement of the Scattergood
Foundation design challenge.
Last but certainly not least, I would like to thank Katherine
Carroll and AlysonFerguson for graciously allowing me to contribute
to their Community-Based MatersProject as a part of my Block VIII
Independent Study. Without their steadfastdedication to the
project, this opportunity would not have been possible for me. I
amsincerely thankful for their support, patience, and insight. I
have no doubt that they
will each make an immeasurable contribution to the field of
public health in the yearsto come.
-
7/31/2019 Kimberly D. Williams Master's Thesis
4/62
iv
TABLE OF CONTENTS
LIST OF
TABLES.......................................................................................................v
LIST OF
FIGURES....................................................................................................vi
1. INTRODUCTION
...................................................................................................1
2. BACKGROUND
......................................................................................................4
2.1 No Health Without Mental Health
.......................................................................
4
2.2 National and Regional Mental Health Care Policy
.............................................. 5
2.3 National and Regional Mental Health
Status.....................................................10
2.4 Social Innovation for Wicked Problems
............................................................12
2.5 Design
Thinking.................................................................................................13
2.6 Human-Centered Design
....................................................................................15
2.6.1 Desirability, Feasibility, Viability
...............................................................15
2.6.2 Hear, Create, Deliver
...................................................................................17
2.7 Web 2.0 and Social
Media..............................................................................18
2.8 Philanthropy as a Change Agent
........................................................................19
2.8.1 Dorothy Rider Pool Health Care Trust
........................................................20
2.8.2 Advancing Colorados Mental Health Care
................................................ 21
2.8.3 Philanthropy 2.0
.......................................................................................
23
3. THE SCATTERGOOD PROJECT
.....................................................................24
3.1The Scattergood Foundation
..............................................................................24
3.2The Scattergood Project
.....................................................................................26
3.2.1 Project Development
...................................................................................26
3.2.2 Website Development
.................................................................................28
3.2.3 IRB
Submission...........................................................................................
29
3.2.4 Interview Recruitment
.................................................................................29
3.2.5 Phase 1: Hear
..............................................................................................
30
3.2.6 Phase 2: Create
...........................................................................................
31
3.2.7 Phase 3:
Deliver..........................................................................................
33
3.2.8 Report
Writing.............................................................................................
363.3Future of the Scattergood
Project.......................................................................
37
4. LESSONS
LEARNED...........................................................................................38
4.1Personal Narrative
..............................................................................................
38
4.2Future Executive MPH Student
Opportunities...................................................41
LIST OF
REFERENCES..........................................................................................43
APPENDIX A: INTERVIEW
GUIDE....................................................................50
APPENDIX B: DESIGN BRIEF DRAFT
..............................................................52
APPENDIX C: LINKS FOR ADDITIONAL
INFORMATION..........................54
-
7/31/2019 Kimberly D. Williams Master's Thesis
5/62
v
LIST OF TABLES
1. Scattergood Project Timeline (2011
2012)........................................................26
2. Key Informant Interview
Themes........................................................................32
3. Design Challenge
Model........................................................................................
33
-
7/31/2019 Kimberly D. Williams Master's Thesis
6/62
vi
LIST OF FIGURES
1. Human-Centered Design: Desirability, Feasibility,
Viability...........................16
2. Human-Centered Design: Hear, Create,
Deliver...............................................18
-
7/31/2019 Kimberly D. Williams Master's Thesis
7/62
-
7/31/2019 Kimberly D. Williams Master's Thesis
8/62
1
1. INTRODUCTION
As the former U.S. Surgeon General, Dr. David Satcher, aptly
declared,
There is no health without mental health. In addition to calls
for the integration of
mental and physical health systems, the field of public health
should improve the
extent to which mental health factors are incorporated into its
objectives and
strategies.
Over the past 50 years, there have been numerous legislative
advancements to
improve that quality of and access to health care for undeserved
Americans including
Medicaid, Medicare, and most recently the Patient Protection and
Affordable Care
Act (PPACA) (Barr, 2011). In addition to these measures,
specific improvements
have been implemented to improve behavioral health care
including the Mental
Health Parity Act (MHPA) as well as the expanded Paul Wellstone
and Pete
Domenici Mental Health Parity and Addiction Equity Act (MHPAEA)
(Frank &
Giled, 2006). However, the national prevalence and incidence of
mental disorders
remains disturbingly high at 46.4% and 26.2% respectively
(Kessler & Wang, 2008).
As such, the quality and accessibility of behavioral health care
continue to be a
pressing concern. In addition to financial concerns that reduce
access to health
insurance coverage and health care services, another major
barrier is the persistence
of personal and societal stigma surrounding mental illness
(Corrigan, 2004; Corrigan,
Markowitz, & Watson, 2004).
The multi-faceted issues that contribute to the barriers and
deficiencies in the
behavioral health care systems may be classified as wicked
problems. Rittel and
Webber (1973) cited that due to their complex nature, wicked
problems cannot be
addressed by utilizing traditional scientific methods. Instead,
sources of wicked
problems could be mitigated by the creation and administration
of disruptive social
-
7/31/2019 Kimberly D. Williams Master's Thesis
9/62
2
innovations (Brown & Wyatt, 2010; Kolke, 2012). Employing
the use of design
techniques may be an effective way to inspire and generate
social innovations. Brown
(2009) asserted that the application of design thinking
methodologies, such as human-
centered design, may in fact be a systematic and integral way to
achieve socially
innovative solutions.
As design practice has evolved into the application of design
thinking methods
for social causes and concerns, the world of technology has also
progressed. Two
primary examples include the evolution of the World Wide Web
into what has been
coined Web 2.0 as well as the subsequent creation of social
media applications.
The advent of Web 2.0 and its social media tools have enabled
users to capitalize on
the inherently interactive nature and social networking
potential of this technology
(Treese, 2006). As a result, users provide as much information
as they receive and
thus, have shifted from a passive consumer role to a role of
active participation
(Brown, 2009).
While the introduction of design thinking and Web 2.0 have made
significant
contributions to society, philanthropic foundations have also
served as a unique agent
of change. Specifically, philanthropies have played an integral
part in improving the
health of the local communities they serve. Examples of two
local foundations which
exemplify innovative ways to improve the health of their
communities include the
Dorothy Rider Pool Health Care Trust and Advancing Colorados
Health Care Trust
(Meehan, Kaufman, Carlin, & Palmer, 2001; TriWest Group,
2011a).
The era of philanthropy 2.0 is seen as another evolution in the
development
of philanthropic foundation operations. This has been
precipitated by their utilization
of Web 2.0 and social media applications to increase the level
of communication
-
7/31/2019 Kimberly D. Williams Master's Thesis
10/62
3
between the foundations, their grantees, and other strategic
partners (Brest, 2012;
Morozov, 2009).
The Thomas Scattergood Behavioral Health Foundation in
Philadelphia,
Pennsylvania is a key example of a foundation that has embraced
philanthropy 2.0
strategies. Its mission is to carry forth the goals of the
foundations namesake,
Thomas Scattergood, into the 21st century and continue to
advance the field of
behavioral health (Thomas Scattergood Behavioral Health
Foundation [Scattergood
Foundation], 2012). In addition, the Scattergood Foundation has
taken inspiration
from design thinking methodologies in order to promote social
innovations for
behavioral health care.
In anticipation of the 200th anniversary of the affiliated
Friends Hospital, the
Scattergood Foundation set out to retool its website. In doing
so, it collaborated with
the Drexel University School of Public Health, Geiger Design, as
well as a public
interest consulting group, Capacity for Change, to implement
this project. The
primary goal of the project was to utilize design thinking
practices and Web 2.0
applications in order to develop a design challenge for the
local community. Steps
from the human-centered design process were conducted in an
effort to achieve this
goal. The revised website went live on May 6, 2012. However, the
implementation
of the initial Scattergood design challenge was postponed until
after additional
feedback and engagement from website users in the community
could be obtained.
The delayed implementation of the Scattergood design challenge
presents an
ideal opportunity for future Drexel Master of Public Health
students to actively
participate in this project. Ultimately, it is anticipated that
the design challenges
presented on the Scattergood website will foster innovative and
sustainable
advancements for the regional and national arenas of behavioral
health.
-
7/31/2019 Kimberly D. Williams Master's Thesis
11/62
4
2. BACKGROUND
2.1 No Health Without Mental Health
The fields of mental health and public health are not mutually
exclusive. The
World Health Organization (WHO) asserted as such in their
Constitution when they
defined health as a state of complete physical, mental and
social well-being and not
merely the absence of disease or infirmity (1946, p. 1). Just as
calls to integrate
mental and physical health care increase, public health should
continue this trend by
improving the extent in which mental health is incorporated into
its policies,
educational programs, communication strategies, prevention
research, surveillance
practices, and epidemiological reviews (Centers for Disease
Control and Prevention
[CDC], 2011b; WHO, 2002).
Coinciding with the release of the seminal Surgeon General
report on mental
health (U.S. Department of Health and Human Services [DHHS],
1999), Dr. David
Satcher echoed the sentiments of the WHO Constitution and
declared, there is no
health without mental health. However, what if we took this one
step further and
concluded that there is nopublic health without mental health?
In essence, true
wellness cannot be achieved without holistically addressing the
physical, mental, and
social factors that play a role in our health and well-being. In
doing so, it may be
possible to expand the framework of public health promotion and
prevention
strategies to better include mental health components in their
objectives (CDC, 2011b;
WHO, 2002). With this in place, we may be one step closer to a
truly integrated
health care system where mental health will be accepted as an
undeniable and
invaluable factor in health and wellness.
-
7/31/2019 Kimberly D. Williams Master's Thesis
12/62
5
2.2 National and Regional Mental Health Care Policy
In an effort to offset the rising burden of costs as well as
improve the quality
of and access to services, several reforms to our health care
system have been
implemented during the past 50 years. As a result, our mental
health care policies
have undergone some critical revisions, which have led to
dramatic improvements in
the accessibility and quality of mental health care as well as
how society addresses
and views mental illness. Unfortunately, issues with cost,
access to care, system
fragmentation, and stigma remain a real concern (Giled &
Frank, 2009; Frank &
Giled, 2006; Frank & Giled, 2007).
In 1965, Medicare and Medicaid were enacted by Congress as
amendments to
the existing Social Security Act and thus, referred to as Title
XVIII and XIX
respectively. The passage of both federal programs marked one of
the most
significant chapters in our countrys history by increasing
access to health care for
millions of Americans. In addition, both reform measures would
contribute to
changing the landscape in which health care services are
evaluated and administered
(Barr, 2011).
Medicare provides health insurance coverage primarily for
individuals who
are eligible for Social Security benefits and 65 years of age or
older. However, it was
revised a few years later to also include two additional
categories of individuals under
this age limit: those deemed permanently disabled and those in
end-stage renal
disease or what is referred to as kidney failure (Barr,
2011).
Medicaid currently provides coverage for specified groups of
low-income
individuals and their families or disabled individuals who meet
the mandated
qualifications. Unlike Medicare, which is universally available
for all elderly
individuals, Medicaid was not initially intended to provide
coverage for all people
-
7/31/2019 Kimberly D. Williams Master's Thesis
13/62
6
who fall below the federal poverty line (FPL) and was only made
available to certain
subgroups that met the eligibility requirements (Barr, 2011).
Another notable
difference between the two programs is that Medicaid is managed
by the state and
local governments with a percentage of program costs being
funded by federal
reimbursements, whereas the federal government solely
administers Medicare (Barr,
2011).
While Medicaid was not specifically created to increase coverage
for
individuals with mental health concerns, it did considerably
reduce the states cost of
mental health care. As a result, the number of individuals with
diagnosable mental
disorders who received coverage through Medicaid dramatically
increased over the
years (Frank & Giled, 2006; Henry J. Kaiser Family
Foundation [KFF], 2011). As of
2011, approximately 24% of adult Americans enrolled in Medicaid
reportedly had a
diagnosable mental disorder (Garfield, Zuvekas, Lave, &
Donohue, 2011).
One of the mandates included in the initial implementation of
Medicaid was
that services at state and county mental health hospitals or
private psychiatric facilities
would not be covered. This was known as the Institution of
Mental Disease (IMD)
exclusion. The IMD exclusion was included to prevent state costs
from shifting to the
federal budget. Another goal was to encourage state health
systems to transition from
primarily long-term, in-patient mental health care to programs
that focused on
community-based treatments (Frank & Giled, 2006; KFF, 2011).
It is now clear that
the Medicaid IMD exclusion only partially succeeded in this
effort. Indeed, Medicaid
is considered to have played a significant role in the
deinstitutionalization of mental
health services by the dramatic decrease of patients at state
and county mental
hospitals. After a peak of over 550,000 in-patient residents in
1955, there was a
steady decrease of 1.5% per year during the next ten years.
Starting in 1965, the rate
-
7/31/2019 Kimberly D. Williams Master's Thesis
14/62
7
jumped to a patient decrease of 8% per year. This was especially
evident in the rapid
reduction of elderly in-patients from these facilities, which
totaled about 70.6%
between 1955 and 1973 (Frank & Giled, 2006). However, many
patients were in fact
only transferred to other types of in-patient care, specifically
psychiatric wards in
general hospitals and nursing homes. In particular, there was a
74% increase of
elderly patient residents in nursing homes between 1960 and 1970
(Frank & Giled,
2006).
Despite some improvements, the marginalization of behavioral
health care
continued and the fragmentation between behavioral and physical
health care was
only perpetuated by these new legislations (Frank & Giled,
2006). In fact behavioral
health services were literally carved out of the general health
system and thus
managed under a separate funding structure (Frank & Giled,
2006; Zuvekas, 2005).
A prime example of the fragmentation of mental health care can
be seen in
Pennsylvanias public welfare system. Under the states Department
of Public
Welfare (DPW), the HealthChoices program consists of two
divisions that administer
managed care programs for residents who receive medical
assistance (DPW, 2010a).
The Office of Mental Health and Substance Abuse Services
(OMHSAS) division runs
the behavioral health managed care organizations (DPW, 2012).
The Office of
Medical Assistance Programs (OMAP) runs the physical health
managed care
organizations and administers the Medicaid program for the state
(DPW, 2010b). As
such, state residents in need of medical assistance are forced
to navigate between two
complex health systems in order to receive comprehensive care
for behavioral and
physical conditions.
While many new Americans obtained health care coverage through
the
creation of Medicaid and Medicare, the costs for health care
rapidly increased since
-
7/31/2019 Kimberly D. Williams Master's Thesis
15/62
8
their inception (Barr, 2011). One response to these rising costs
was the increased
utilization of managed health maintenance organizations (HMOs)
and managed
behavioral health care organizations (MBHOs) during the 1980s
and 1990s (Barr,
2011; KFF, 2011). However, the increase usage of managed care
organizations
contributed to furthering the marginalization and fragmentation
of behavioral health
care services from the rest of the health care system
(Brousseau, Langill, & Pechure,
2003; KFF, 2011; Zuvekas, 2005).
In response to these issues, the Mental Health Parity Act (MHPA)
was enacted
in 1996. The MHPA set a historic precedent by mandating that
insurance carriers
provide mental health care benefits and limits that are equal to
medical and surgical
health care benefits and limits (KFF, 2011; Smaldone &
Cullen-Drill, 2010). In 2008,
the benefits provided by the MHPA were further increased with
the Paul Wellstone
and Pete Domenici Mental Health Parity and Addiction Equity Act
(MHPAEA). The
parity requirements under the MHPAEA were expanded to include
substance use
disorders as a mental health condition and eliminated arbitrary
limits on the frequency
of outpatient treatment services or inpatient days of coverage
(Smaldone & Cullen-
Drill, 2010). The additional mandates in the 2008 MHPAEA went
into effect on
January 1, 2010 (Smaldone & Cullen-Drill, 2010).
That same year would mark a historic evolution for general as
well as
behavioral health care with the passage of the Patient
Protection and Affordable Care
Act (PPACA), which was signed into law on March 23, 2010
(Garfield, Lave, &
Donohue, 2010). While the MHPAEA sought to equalize the mental
and physical
health care coverage, the PPACA attempted to take health care to
the next level by
increasing accessibility, improving quality, as well as
integrating mental and physical
health services (Barry & Huskamp, 2011; Garfield et al.,
2010). The principle behind
-
7/31/2019 Kimberly D. Williams Master's Thesis
16/62
9
the PPACA was that all Americans should be provided access to
affordable health
care insurance in order to have access adequate health care
services and thus, improve
to overall health status of the nation (Barry & Huskamp,
2011; Garfield et al., 2010).
Of the 59 million people currently enrolled in Medicaid,
approximately only
5% are eligible directly due to a mental disorder. The majority
of people currently
qualify for Medicaid based on their family or low-income status
(KFF, 2011). As a
direct result of the PPACA, approximately 2 million additional
Americans who meet
the criteria for a mental disorder will be eligible for Medicaid
after the full PPACA
provisions are enforced by 2014 (KFF, 2011). This increased rate
of coverage will
primarily be possible due to updated eligibility requirements
(Garfield et al., 2011).
Specifically, Medicaid will be expanded to include all persons
with household
incomes up to 133% of the FPL (Barr, 2011; KFF, 2011). In
addition, persons with
household incomes up to 400% of the FPL will be eligible for
subsidies to supplement
the purchase of health care coverage through health insurance
exchanges (Barr, 2011;
KFF, 2011).
Another crucial and historic component of the PPACA for the
mental health
community is the inclusion of behavioral health care services as
an essential health
benefit (Garfield et al., 2010). This will prohibit affected
health insurance plans from
excluding individuals with pre-existing behavioral health
conditions. As a result,
many more individuals with diagnosed mental illnesses or
substance use disorders
who were previously unable to obtain private insurance or
Medicaid benefits, will
now be eligible for some form of health insurance that will
cover their physical and
behavioral health care needs (Garfield et al., 2010). It is
expected that approximately
3.7 million Americans with mental disorders will be able to
obtain some form of
health care coverage by 2019 (Garfield et al., 2011; KFF, 2011).
The PPACA has the
-
7/31/2019 Kimberly D. Williams Master's Thesis
17/62
10
potential to reshape the way behavioral health services are
delivered in this country
and could measurably reduce the system fragmentation between
behavioral and
physical health care (Barry & Huskamp, 2011; Garfield et
al., 2011).
As of May 2012, the U.S. Supreme Court was currently debating
the
constitutionality of the PPACA. It remains to be seen whether
the court will uphold
the full PPACA, only certain provisions such as the individual
mandate to purchase
health insurance, or strike down the Act in its entirety (New
York Times, 2012).
Regardless of future outcomes, it is clear that more policy and
system changes are
needed to ensure that Americans receive truly adequate
behavioral health care
treatment and services. In addition, more needs to be done to
change societys
outlook on mental illness as well as the importance of overall
mental wellness.
2.3 National and Regional Mental Health Status
Kessler and Wang (2008) confirmed that the national prevalence
of mental
disorders remains exceedingly prohibitive. In their
epidemiological review of mental
disorders as categorized in theDiagnostic and Statistical Manual
of Mental
Disorders 4th Edition (DSM-IV) they reported that approximately
half (46.4%) of
the U.S. population would meet the diagnosable criteria for one
or more disorder
during their lifetime. In addition, more than a quarter (26.2%)
of the U.S. population
would meet the criteria for such a disorder during any given
12-month period (Kessler
& Wang, 2008). The state of Pennsylvania was slightly below
this national average
with approximately 17.74% of adults over the age of 18 meeting
the criteria for a
diagnosable mental illness between 2008 and 2009 (Substance
Abuse and Mental
Health Services Administration [SAMHSA], 2011). However, 26.24%
of young
adults between the ages of 18 and 25 did meet the criteria for a
diagnosable mental
-
7/31/2019 Kimberly D. Williams Master's Thesis
18/62
11
illness, which is an alarming rate for this age category and
more in line with national
prevalence rates of adults (SAMHSA, 2011).
The percentage of individuals who exhibit co-occurring mental
health
disorders as well as comorbid physical health conditions has
been identified as
another public health concern. Kessler and Wang (2008) cited
that well over a quarter
(27.7%) of Americans will experience two or more mental
disorders during their
lifetime and that approximately 17% are at risk for experiencing
three or more mental
disorders. In addition, several studies have confirmed that
adults with mental
disorders are more likely to be afflicted with comorbid physical
health conditions
such as high blood pressure, heart disease, stroke, diabetes,
and asthma (Chapman,
Perry, & Strine, 2005; Goodell, Druss, & Walker, 2011;
Institute of Medicine, 2006;
Parks, Svendsen, Singer, & Foti, 2006; SAMHSA, 2012a).
Adult Americans with mental disorders are also more likely to
utilize
emergency department (ER) services (38.8%) or be hospitalized
(15.1.%) than those
who do not have a diagnosed mental disorder (27.1% and 10.1%
respectively)
(SAMHSA, 2012a). The origin of such differences between the
health status of
individuals with and without mental disorders has yet to be
empirically identified.
However, it is clear that individuals with mental disorders
disproportionately suffer
from chronic health conditions and thus demonstrate a greater
need for physical health
care treatment in addition to mental health services (SAMHSA,
2012a; Goodell et al.,
2011).
Despite the known prevalence of mental health disorders as well
as their
association with an increased risk of comorbid physical health
conditions, many
individuals fail to seek out treatment for behavioral health
related concerns nor follow
through with recommended services (Corrigan, 2004; Corrigan et
al., 2004; KFF,
-
7/31/2019 Kimberly D. Williams Master's Thesis
19/62
12
2011). In fact, as many as 60% of adults with a diagnosable
mental disorder were
reported to not have received necessary mental health care
services (KFF, 2011). One
confirmed reason is due to the continuing high rates of
individuals who do not have
health insurance coverage and could not afford the cost of such
services (Garfield et
al., 2011; KFF, 2011, SAMHSA, 2012b). In 2010, about 43.7% of
adults reported
that the primary reason they did not receive necessary mental
health services was
directly due to issues with the cost of such care (SAMHSA,
2012b). In addition to the
known financial barriers to care, many individuals do not obtain
necessary behavioral
health treatment due the social stigma associated with mental
illness (Corrigan, 2004;
Corrigan et al., 2004).
2.4 Social Innovation for Wicked Problems
Rittel and Webber (1973) identified wicked problems as issues
that plague
our society and, due to the complex social systems in which they
are entrenched,
cannot be tackled with traditional scientific applications.
Instead, the exploration and
creation of disruptive innovations have been identified as a
possible means to mitigate
the factors that contribute to the wicked problems of our
society (Brown & Wyatt,
2010; Kolke, 2012). Thus a movement has been initiated to
develop social
innovations through alternative means in order to effectively
address such wicked
problems (Brown & Wyatt, 2010; Phills, Jr., Deiglmeier,
& Miller, 2008). In
response to this movement, the utilization of modified design
techniques have been
touted as an effective way to produce potentially innovative
solutions (Brown &
Wyatt, 2010; Kolke, 2012).
In order to reduce the many barriers to care and improve the
quality of
behavioral health services, disruptive social innovations may be
the best solution to
-
7/31/2019 Kimberly D. Williams Master's Thesis
20/62
13
their wicked problems. The application of design thinking
practices, including
human-centered design, may thus be an opportune way to foster
socially innovative
thinking and create tangible solutions to some of the critical
systemic and cultural
behavioral health concerns that affect our society.
2.5 Design Thinking
In his book, Change By Design, Tim Brown asserted that design
thinking is
a systematic and integral approach for achieving innovated
solutions (2009). Some
identified best practices for the design thinking process
include the use of dedicated
spaces, finite or well-defined timeframes, and
multi-disciplinary teams (IDEO, 2009).
In addition, Brown asserted that the design process includes
three fundamental levels
or spaces of thinking when trying to develop an innovative
solution: inspiration,
ideation, and implementation (Brown, 2009; Brown & Wyatt,
2010). These spaces of
thoughts are not classified as distinct steps in a process
because design thinking is
iterative (Brown, 2009; Liedtka & Ogilvie, 2011). In fact,
such levels of thinking are
not necessarily completed sequentially and may be repeated
throughout the process of
developing a product or solution (Brown, 2009; Brown &
Wyatt, 2010; Liedtka &
Ogilvie, 2011).
The initial level ofinspiration may involve creating a brief,
which documents
the facts and background concerning the issue at hand and
defines the problem. It
also includes the process of exploring the issues, needs and
barriers of the target
population affected by the problem. This can best be achieved by
immersing oneself
into the daily lives and routines of individuals and observing
them in natural
environment (Brown & Wyatt, 2010).
-
7/31/2019 Kimberly D. Williams Master's Thesis
21/62
14
The second concept, ideation, involves analyzing and
synthesizing the
information that was collected in order to eventually formulate
potential solutions.
Ideation largely involves active divergent thinking in which
many thoughts and ideas
are generated in order to facilitate the creation of potential
options or solutions.
Ideally, this involves brainstorming sessions with
multi-disciplinary teams that
provide varied backgrounds and alternative perspectives, which
advance the divergent
thinking process (Brown, 2009; Brown & Wyatt, 2010). In
addition, design
challenges have also proven to further develop divergent
thinking by successfully
fostering multiple ideas and potential solutions for the problem
in question. The
design challenge process is initiated when a challenge question
is posted in some
central location for individuals or teams to review, offer
comments, and design
potential solutions (Brown & Wyatt, 2010). Aside from
generating multiple thoughts
and idea, participating can elevate people from a passive
position to an active one
where they are engaged and committed to the issue as well as its
eventual solution
(Brown, 2009). During the ideation process, the team will
eventually transition from
a level of divergent thinking to a level of convergent thinking
where the abstract
information collected is focused down into a few concrete ideas
and solutions
(Brown, 2009; Brown & Wyatt, 2010).
Finally, implementation is self-explanatory to the extent that
it involves setting
up a plan for implementation to final solution. This also may
involve the creation of a
communication strategy and prototypes to ensure that the
solution is effectively and
efficiently implemented (Brown, 2009; Brown & Wyatt,
2010).
-
7/31/2019 Kimberly D. Williams Master's Thesis
22/62
15
2.6 Human-Centered Design
One of the core principles in design thinking is to maintain
processes and
goals that are fundamentally human-centered(Brown, 2009; Brown
& Wyatt, 2010).
As a result, the human-centered design methodology was created
in an effort to
systematically incorporate the needs of the people for whom the
design product is
intended. Originally created to enable for-profit corporations a
way to design
products and create innovative solutions or concepts for their
businesses, the tools in
human-centered design have been discovered to be an innovative
way to create
solutions and promote change for social causes and community
related concerns
(Brown, 2009; Brown & Wyatt, 2010).
By its very name, a human-centered process or project begins
with the people
it is tasked with supporting through its innovations. Constantly
keeping the
framework focused on the human component of the project and
involving the
consumers throughout the design process ensures that the final
product is truly
desirable, feasible, viable, and ultimately sustainable (Brown,
2009; Brown & Wyatt,
2010).
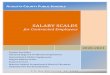
2.6.1. Desirability, Feasibility, Viability
The human-centered design process begins with three lenses by
which the
team views and evaluates the problem at hand: Desirability,
Feasibility, and Viability
(see Figure 1) (Brown, 2009; IDEO, 2009). The first
lens,Desirability, is the basis of
all human-centered thinking and processes. The consideration of
what the target
population desires and not what the evaluator believes that they
need is the framework
from which future solutions or concepts are derived (Brown,
2009; IDEO, 2009). The
second lens,Feasibility, reminds the team to ensure that all
solutions are anchored in
-
7/31/2019 Kimberly D. Williams Master's Thesis
23/62
16
proposals that are considered organizationally and technically
feasible (Brown, 2009;
IDEO, 2009). Finally, even the most organizationally and
technically feasible
solution cannot be sustainably implemented without being
financially viable.
Therefore, the third lens ofViability maintains that the
solutions achieved retain a
realistic and practical approach in their implementation (Brown,
2009; IDEO, 2009).
If the final solutions created from a human-centered design
process encompass all
three of these lenses in their product or concept then it
increases the likelihood that
they will be successfully implemented and received by the
community for which they
were conceived (Brown, 2009).
Figure 1. Human-Centered Design Lenses: Desirability,
Feasibility, Viability.Adapted fromHuman-Centered Design Toolkit,
2ndEditionby IDEO, 2009, p. 6.
Copyright 2012 by IDEO.
-
7/31/2019 Kimberly D. Williams Master's Thesis
24/62
17
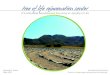
2.6.2. Hear, Create, Deliver
The actual steps of a human-centered design process are
implemented by
utilizing techniques and specific activities in three distinct
phases: Hear, Create, and
Deliver (see Figure 2) (IDEO, 2009). These phases mirror the
concepts of inspiration,
ideation, and implementation that Brown asserted are
instrumental in the design
thinking process (Brown, 2009; Brown & Wyatt, 2010).
TheHearphase begins with
compiling concrete information and facts about the problem at
hand as well as the
people affected by this problem. This information is obtained by
conducting field
research where people are observed in their environment and
encouraged to provide
stories about their daily lives and routines (IDEO, 2009).
During the Create phase,
the concrete information collected is analyzed and expanded into
abstract themes or
concepts. These multiple ideas are then synthesized into
opportunities or options and
eventually into concrete solutions for the problem (IDEO, 2009).
TheDeliverphase
prepares for the release of the agreed upon solution. This may
involve the
development of prototypes or models to serve as a guide for the
solution concept. In
addition, an implementation plan is created and eventually
initiated in order to
effectively release the final solution into the community (IDEO,
2009).
-
7/31/2019 Kimberly D. Williams Master's Thesis
25/62
18
Figure 2. Human-Centered Design Phases: Hear, Create, Deliver.
Adapted from
Human-Centered Design Toolkit, 2nd
Edition by IDEO, 2009, p. 7. Copyright 2012by IDEO.
2.7 Web 2.0 and Social Media
Technology is a continuously evolving factor within the
development of our
society. The evolution of the World Wide Web into what has been
coined Web 2.0
is yet another milestone in that development. During the past
two decades, the way in
which we utilize the Web to access and disseminate information
has shifted from a
unilateral experience to a multilateral phenomenon. Two
hallmarks of Web 2.0 are its
interactive nature and social networking capabilities (Treese,
2006).
Prime examples of both these functions are encapsulated in
current social
media tools such as Facebook, Twitter, and YouTube (CDC, 2011a).
Kaplan and
Haenlein (2010) defined social media as a group of
Internet-based applications that
build on the ideological and technological foundations of Web
2.0, and that allow the
creation and exchange of User Generated Content (p. 61). In
other words, social
media technologies allow for users to interact and actively
participate in the content
they are accessing rather than simply passively consuming
information. As asserted
by Brown (2009), Web 2.0 users have shifted from a consumer role
to a participatory
-
7/31/2019 Kimberly D. Williams Master's Thesis
26/62
19
role with the assistance of social media applications. As a
result, Web 2.0
applications are particularly well suited to serve as a forum
for the human-centered
design process where the users input is a fundamental part of
its method.
2.8 Philanthropy as a Change Agent
Philanthropic foundations are in an ideal positionto promote
change and
foster innovation in our society. Furthermore, local
philanthropies have the ability to
produce a great deal of change within the communities they
serve. Meehan,
Kaufmann, Carlin, & Palmer (2001) identified some of the
most distinct advantages
local philanthropies have when attempting to produce change.
First, they noted that a
well-designed philanthropic agenda could have a strong influence
on the local
communities served. Second, they have the ability to maintain a
neutral and honest
mediating position between the design and implementation of
change into a
community. Third, as a private foundation, they do not have the
same level of
political considerations as elected officials or departments. As
a result, they may be
in a position to fund or even implement more innovative and
groundbreaking
solutions. Fourth, philanthropies have the ability to dispense
smaller amounts of
funds in a more strategic and targeted fashion than larger
government organizations
and thus, are able to respond to a need more effectively and
efficiently. Fifth, they
can uphold a reputation of reliability and integrity by
championing causes that may
have been previously discarded for financial or political
reasons. Lastly, through
effective fundraising efforts, philanthropies can maintain a
greater level of financial
resources than other types of organizations in order to create
an improved and
sustainable system of care (Meehan et al., 2001).
-
7/31/2019 Kimberly D. Williams Master's Thesis
27/62
20
With health related issues being one of the foremost concerns
addressed today,
philanthropies have played a crucial role in advancing health
care systems as well as
the well-being of underserved populations (Grantmakers In Health
[GIH], 2005, 2010,
2012). One of the most underserved populations includes
individuals dealing with
behavioral health concerns. Philanthropies are particularly
suited to navigate a
complex behavioral health care system and improve some of its
deficiencies and
difficulties in order to increase its quality and access to care
(Brousseau, Langill, &
Pechura, 2003; LeRoy, Heldring, & Desjardins, 2006; Meehan
et al., 2001).
2.8.1 Dorothy Rider Pool Health Care Trust
A prime example of such a foundation is the Dorothy Rider Pool
Health Care
Trust (Pool Trust) located in Allentown, Pennsylvania. The Pool
Trust was created in
1975 with a mission to ensure quality health care for local
residents and provide
funding assets to Lehigh Valley Hospital that serves the region
(Dorothy Rider Pool
Health Care Trust, n.d.; Meehan et al., 2001). In an effort to
combat the increasing
challenges of the areas psychiatric system, the Pool Trust
attempted to reduce the
number of patients who sought out psychiatric services through
local emergency
departments and redirect their treatment to community-based
care. A second goal
was to implement a sustainable system that ensured the long-term
support of these
patients as well as their ability to thrive as functional
members of the community
(Meehan et al., 2001).
Several notable achievements have been documented despite the
fact that a
formal evaluation of this initiative has not been conducted.
First, over $5.2 million of
funds were provided by the Pennsylvania Department of Public
Welfare (DPW) to
support the expansion of community-based behavioral health
services. Thus, the
-
7/31/2019 Kimberly D. Williams Master's Thesis
28/62
21
amount of community services increased for patients classified
at a high risk for in-
patient care (Meehan et al., 2001). In addition, the utilization
of services at Allentown
State Hospital (ASH), which is a long-term and in-patient
psychiatric facility, were
reduced. This was demonstrated by the fact that more than 100
patients at ASH were
discharged and successfully integrated into the community.
Additional services for
psychiatric crises and alternatives to in-patient
hospitalization were also implemented
as a result of this program (Meehan et al., 2001). In order to
independently gauge the
communitys response to the program initiatives, local mental
health consumers and
their families created a Customer Satisfaction Team. They
monitored the services
provided and evaluated the systems efforts through the use of
surveys, which have
demonstrated positive results and sustained customer approval
(Meehan et al., 2001).
2.8.2 Advancing Colorados Mental Health Care
Local philanthropies can also collaborate among each other in
order to foster
change in a community. In 2002, eight local foundations
collaborated to assess the
status of mental health care in the state of Colorado. These
foundations included:
Caring for Colorado Foundation, The Colorado Trust, Daniels
Fund, The Denver
Foundation, First Data Western Union Foundation, HealthONE
Alliance, Rose
Community Foundation, and Rose Womens Organization. They
commissioned a
private consulting group, TriWest Group and Heartland Network
for Social Research
(TriWest Group), to complete an evaluation of the private and
public mental health
systems in Colorado. The result of this assessment was released
in the 2003 report,
The Status of Mental Health Care in Colorado (TriWest Group,
2003). This
evaluation revealed the extreme fragmentation of mental health
services and how this
inhibited access to care for the states residents. Specifically,
they noted that one in
-
7/31/2019 Kimberly D. Williams Master's Thesis
29/62
22
five residents are in need of mental health care, but only
approximately a third of
these individuals receive treatment. In addition, they
identified that children and
adolescents contribute to more than a third of the states severe
mental health needs,
but only comprise a quarter of the overall states population.
Only half of children
from households that were classified as low-income received
necessary mental health
care in 2000 (TriWest Group, 2003).
In response to the alarming findings in this report, Advancing
Colorados
Mental Health Care (ACMHC) was created through the joint funds
of the Caring for
Colorado Foundation, the Colorado Trust, the Denver Foundation,
and the Colorado
Health Foundation (previously known as the Health ONE Alliance).
Together they
committed $4.25 million for a five-year project between 2005 and
2010 to improve
Colorados mental health care system by increasing the
integration and coordination
of its services (TriWest Group, 2011a). The ACMHC project funded
six grantees for
three integration-related project goals. The first funded two
grantees for projects to
integrate mental health and substance use disorder services. The
second funded two
grantees for projects to integrate mental health and primary
health care services. The
third funded two grantees for projects to integrate mental
health services with school
settings (TriWest Group, 2011a).
In 2011, an updated report The Status of Behavioral Health Care
in
Colorado was released that reviewed the successes of the ACMHC
project as well
as what needs remained a concern for the state (TriWest Group,
2011b). This report
demonstrated the number of mental health and substance use
disorder practitioners
increased from 10,564 in 2003 to 14,217 in 2011. However, a high
need remained for
specialists who are able to treat complex behavioral health
issues and practitioners for
services in rural and frontier areas of the state (TriWest
Group, 2011b). Spending on
-
7/31/2019 Kimberly D. Williams Master's Thesis
30/62
23
public mental health care across the state did increase between
2002 and 2009, with a
per capita increase from $62 to $84 (TriWest Group, 2011b). In
addition, several
efforts have been made to reduce system fragmentation in the
states mental health
care system. For example, oversight of the mental health and
substance use disorder
care systems are now both managed by their Division of
Behavioral Health.
Increased availability of medical home services for children and
adolescents was also
reported (TriWest Group, 2011b).
2.8.3 Philanthropy 2.0
In the pursuit to find new ways to raise funds and create change
for their
prioritized causes, philanthropies have begun to utilize Web 2.0
and social media in
their operational and communication strategies (Brest, 2012).
The utilization of such
innovations has ushered in the advent of philanthropy 2.0 where
the lines of
communication between the foundations, their grantees, and other
partners are closer
than ever (Brest, 2012; Morozov, 2009).
Another transformation in the field of philanthropy was the
increased usage of
design thinking methods, which were initially developed within
the for-profit
industry. Prior to its incorporation by philanthropic
foundations, many non-profit
organizations began to adopt the for-profit design thinking
approaches in order to
create change and foster socially innovative ideas. This
resulted in the differences
between non-profit and for-profit organizations becoming blurred
and less distinct. In
fact, the increased demand for and creation of social
innovations has helped to bridge
the gap between non-profit and for-profit organizations (Phills,
Jr. et al., 2008). Many
philanthropic foundations have now begun to take inspiration
from for-profit and non-
profit organizations by incorporating design thinking techniques
into their initiatives
-
7/31/2019 Kimberly D. Williams Master's Thesis
31/62
24
as well. Being that the organizational goals of philanthropies
are already focused on
advancing social causes and thus human-centered, the application
of design thinking
strategies is a natural progression for their operational
strategies.
A current example of the recent changes to philanthropic
strategies can be
found in the Thomas Scattergood Behavioral Health Foundation of
Philadelphia,
Pennsylvania. With the assistance of Web 2.0 technology and
design thinking
methods, it continues to promote the creation of socially
innovative solutions in order
to address behavioral health issues and concerns of the
region.
3. THE SCATTERGOOD PROJECT
3.1 The Scattergood Foundation
The roots of the Thomas Scattergood Behavioral Health Foundation
can be
traced back to 1811 when Thomas Scattergood, a Quaker minister
moved by his
personal and missionary experiences with mental illness,
proposed creating an asylum
for individuals deprived of the use of their reason at the
Philadelphia Yearly
Meeting (Roby, 2011). In the following year, several Quaker
community members
including Thomas Scattergood gathered in Philadelphia,
Pennsylvania and established
the Friends Asylum for Persons Deprived of the Use of Their
Reason (Roby, 2011).
This asylum would later be founded as Friends Hospital in 1813
and was the first
private psychiatric hospital in the United States (Scattergood
Foundation, 2012).
Unfortunately, Thomas Scattergood died the following year of
Typhus fever.
However, his son, Joseph Scattergood, was given the opportunity
to continue his
fathers cause and was appointed one of the first managers of
Friends Hospital. In
memory of the man who pioneered the American mission to improve
the treatment
and quality of life for individuals suffering from mental
illness, the main building and
-
7/31/2019 Kimberly D. Williams Master's Thesis
32/62
25
heart of the Friends Hospital campus was named after Thomas
Scattergood (Roby,
2011; Scattergood Foundation, 2012).
The Thomas Scattergood Behavioral Health Foundation is a
philanthropic
organization that was established in 2005 as result of a joint
venture between Friends
Hospital and Horizon Health Systems (Scattergood Foundation,
2012). The mission
of the Scattergood Foundation is to continue the advancement and
awareness of
behavioral health issues that Thomas Scattergood had advocated
almost two centuries
before. With its headquarters located on the Friends Hospital
campus, the
Scattergood Foundation has strived to carry forth the mission of
Thomas Scattergood
into the twenty-first century by fostering a dialogue and
increasing learning
opportunities in the behavioral health field and promoting
innovative leadership and
community collaborations through philanthropic and grant-making
opportunities
(Scattergood Foundation, 2012).
Since its creation, the Scattergood Foundation has made several
contributions
to the advancement of behavioral health in the Southeastern
Pennsylvania community.
One example of its efforts included providing a grant to help
found the Scattergood
Program for the Applied Ethics of Behavioral Health at the
University of
Pennsylvania. Founded in June 2007, the Scattergood Ethics
program is dedicated to
the promotion, evaluation, and training of the clinical issues
and strategies
surrounding behavioral health care ethics (Scattergood
Foundation, 2012). In
addition, the Scattergood Foundation helped to advance the field
of the mental health
journalism by establishing a position at Philadelphias public
broadcasting station,
WHYY, with the objective of reporting on behavioral health
current events and issues
(Scattergood Foundation, 2012).
-
7/31/2019 Kimberly D. Williams Master's Thesis
33/62
26
3.2 The Scattergood Project
In anticipation of the 200th anniversary of Friends Hospital,
the Scattergood
Foundation set out to redesign its website and incorporate some
interactive Web 2.0
elements, including a design challenge initiative. By
revitalizing the website design,
the Scattergood Foundation sought to advance the level of
community dialogue
around current behavioral health issues in the region and foster
innovative ways to
address such concerns. Over the course of the past nine months,
the following
activities were conducted in an effort to meet this goal (see
Table 1).
Table 1. Scattergood Project Timeline (2011 2012)
Project Activity Sep Oct Nov Dec Jan Feb Mar Apr May
Project Development X X
Website Development X X X X X X X X X
IRB Submission/Approval X X* X
Interview Recruitment X X
Phase 1: Hear X X X* X*
Phase 2: Create X* X* X*
Phase 3: Deliver X* X*
Report Writing X X X* X* X* X* X*
Note. * Executive MPH student activity/participation
3.2.1 Project Development
The inception of the Scattergood Project began when the
president of the
Scattergood Foundation, Joseph Pyle, MA, approached faculty at
the Drexel
University School of Public Health, Department of Health
Management and Policy
Dennis Gallagher, MA, MPA and John A. Rich, MD, MPH and
requested Drexel to
collaborate with the Scattergood Foundation on an initiative to
retool the Scattergood
-
7/31/2019 Kimberly D. Williams Master's Thesis
34/62
27
website. In addition, Jason Alexander, MA, of the public
interest consulting firm,
Capacity for Change, was brought on as a design thinking advisor
for the project and
Larry Geiger of Geiger Designs was enlisted as the projects
graphic designer to build
the new website.
A final component of the project team included the recruitment
of Drexel
students in the Masters of Public Health (MPH) program.
Initially, two full-time
students, Katherine Carroll and Alyson Ferguson, were recruited
to participate in this
initiative for their Community-Based Masters Project (CBMP),
Fostering Social
Innovation Through the Use of Web 2.0. At a later point during
the development of
the project, I joined the team to collaborate with the full-time
students for the
completion of my Executive MPH Block VIII Independent Study.
Throughout
September and October 2011, the full-time MPH students initially
conceptualized the
project goals. As presented in a project proposal submitted to
the Drexel University
IRB, these goals were identified as:
Identify and prioritize system and policy gaps in the behavioral
healthsystem in Southeastern Pennsylvania using the human-centered
design
process. Evaluate the process of using human-centered design and
Web 2.0 in
respect to creating behavioral health content for public use on
theinternet.
Create a question(s) to post on the Scattergood website for
thebehavioral health community to discuss and potentially create
asolution using the human-centered design thinking process.
The students were tasked with collecting the necessary
information and ultimately
creating a design challenge question for the revised Scattergood
Foundation website.
The inspiration that would serve as the framework for the design
challenge question
was obtained by utilizing elements of the human-centered design
methodology in
order to identify some of pressing barriers, issues, and
concerns within the behavioral
health community. The purpose of the design challenge was based
on the dual goals
-
7/31/2019 Kimberly D. Williams Master's Thesis
35/62
28
of encouraging an open dialogue among community members and
ultimately fostering
innovative solutions to the proposed behavioral health
challenge.
It was noted that, as in any design project, the formulation of
the goals and
objectives are the result of an iterative process, and subject
to revision if necessary.
For example, it was initially expected that this design
challenge question would be
posted in tandem with the release of the new website. As
discussed during the
Deliver phase of this project, it would later be determined that
the design challenge
release would be postponed until after the website went
live.
3.2.2 Website Development
Starting in September 2011, Larry Geiger of Geiger Design began
working on
the graphic design development of the new website and continued
this process in
tandem with the rest of the projects development. It was
determined that the website
would be divided into four main quadrants or portals entitled:
The Foundation,
Community Impact, Innovation Awards, and Design Thinking.
TheFoundation
quadrant will provide background and contact information for the
Scattergood
Foundation. The Community Impactquadrant will describe the
impact grantmaking
opportunities can have on communities, provide a database of
current grants awarded
by the Scattergood Foundation, as well as the criteria and
guidelines for new grant
applications. Each year, the Scattergood Foundation presents an
award for an
innovative behavioral health solution, policy or project.
TheInnovation Award
quadrant will provide a background about the annual Scattergood
Innovation Award,
a database of past winners and nominees, as well as the
eligibility and judging criteria
for future contestants. TheDesign Thinkingquadrant will provide
some basic
information about design thinking in general and provide an
example of a design
-
7/31/2019 Kimberly D. Williams Master's Thesis
36/62
29
thinking application. This quadrant will also host the Design
Challenge, where a
behavioral health challenge question will be posed. Community
members will be
encouraged to participate and engage in this challenge issue as
well as create and
implement an innovative solution.
3.2.3 IRB Submission
To prepare the Institutional Review Board (IRB) application, the
team
established the project mission, goals, methods, and overall
timeline. In addition,
appropriate research level training compliance was confirmed for
all applications
listed on the IRB submission by obtaining the following
Collaborative Institutional
Training Initiative (CITI) program certificates: Human Subjects
Research and Health
Information Privacy Security. Once completed, an application for
human subjects
research was submitted October 2011 to the Drexel University
College of Medicine,
Office of Regulatory Research Compliance. By November 2011, the
project was
approved and deemed to be exempt from IRB review since the
source of the research
data would be obtained from interviews with behavioral and
public health
professionals. A secondary factor in this decision was based on
the fact that the
research data would not include the collection of identifying
medical data nor direct
interactions with behavioral health patients.
3.2.4 Interview Recruitment
Once IRB approval was received, the project was presented to
several key
stakeholders in the community in order to recruit them for key
informant interviews.
Access to many of the prospective stakeholders was facilitated
by referrals from the
project committee members at the Scattergood Foundation as well
as Drexel
-
7/31/2019 Kimberly D. Williams Master's Thesis
37/62
30
University School of Public Health faculty. During November and
December 2011,
the Drexel full-time MPH students coordinated the interview
recruitment process by
contacting these referrals, introducing a brief synopsis of the
project, and setting up
times to complete the interviews.
3.2.5 Phase 1: Hear
TheHearphase consisted of a literature review and the completion
of the key
informant interviews. A review of the literature was conducted
in order to further our
academic knowledge base of the current behavioral health topics
being explored.
This took place for the full-time students during the summer of
2011 and throughout
the spring of 2012 for myself.
The key informant interviews began once IRB approval was
received in
November 2011. The interviews were conducted in order to collect
qualitative data
from key stakeholders regarding behavioral health issues,
concerns, and barriers in the
Southeastern Pennsylvania region and national landscape. The
information these key
stakeholders offered during the interviews would serve as the
framework for the
design challenge question. In an effort to gain a rich
perspective regarding these
needs and concerns, a multi-disciplinary group of professionals
were approached for
the interviews. As a result, we were able to collect stories and
information from
individuals that represented a wide breadth of knowledge in the
behavioral health
community and included backgrounds in: law, academic, city
government, NGO and
advocate organizations, mental health practitioners, private
insurance, and public
insurance.
The interview format remained informal to allow for a natural
conversation to
emerge between the interviewer and interviewee. However, an
interview guide that
-
7/31/2019 Kimberly D. Williams Master's Thesis
38/62
31
included a prepared introduction about the project and a list of
question prompts was
approved by the IRB and utilized for the interviews (see
Appendix A). In addition, a
team approach was incorporated into the process by having a
primary interviewer lead
the discussion while a secondary interviewer listened and took
notes. The discussions
were recorded with the interviewees permission so that the
secondary interviewer
could later transcribe the interview. The final interview was
conducted in January
2012, with the final transcription completed in March 2012.
Beginning in January 2012, an initial design brief was created
that included
the content for the Design Thinking quadrant of the website.
While this brief was
continuously revised as the project progressed, the initial
draft served as a framework
for the information that would be provided in this section of
the website. By February
2012, this initial design brief draft was released for the
project team to review and
utilize as a reference for the Design Thinking quadrant (see
Appendix B).
3.2.6 Phase 2: Create
The Create phase of the project was conducted between February
and April
2012. It consisted of analyzing and synthesizing the information
collected during the
Hearphase. The initial goal was to code the data in order to
make sense of and
identify patterns in the information amassed from the key
informant interviews. This
was completed by individual preliminary analyses of interview
transcripts where key
phrases, words, and topics concerning behavioral health were
documented. We then
combined our individual analyses of the transcripts into a
classification of key words
and phrases. In order to verify our combined analyses of the
data, the interview
transcripts were then uploaded into a software program called
NVivo, which was
developed by QSR International specifically to analyze
qualitative data. Using the
-
7/31/2019 Kimberly D. Williams Master's Thesis
39/62
32
descriptive words identified during the preliminary analyses, a
query was run for the
NVivo program to identify the primary themes, which are referred
to as nodes in
the NVivo software. The output from this query resulted in
several themes or node
categories. The NVivo output was then reviewed to assess the
quality of content in
each node and ensure that the context and classification of each
categorization was
correct. To do so, the output data was compared to preliminary
individual data
analyses to identify any missing references or descriptive
words. This information
was loaded back into NVivo in order to run an additional query.
By March 2012 the
primary behavioral health themes that were identified from the
data analyses
included: public perception, funding, reimbursement, health care
reform, workforce,
integration, recovery, wellness, evidence-based practices, and
trauma (see Table 2).
Table 2. Key Informant Interview Themes
Note. Represents the number of interviews to mention each
theme.
The secondary goal of the Create phase was to define the
opportunities and
create potential ideas for a design challenge question. This was
achieved by
0 2 4 6 8 10 12
Trauma
Evidence-based Practices
Parity
Incentives
Siloes
Wellness
Treatment
Integration
Workforce
Health Care Reform
Reimbursement
Funding
Public Perception
-
7/31/2019 Kimberly D. Williams Master's Thesis
40/62
33
conducting several brainstorming sessions with the project team
during April 2012 in
order to progress the design thinking from a level of divergent
to convergent thinking.
These sessions evaluated the information collected and began to
form distinct and
concrete criteria for the design challenge.
3.2.7 Phase 3: Deliver
Once all of the abstract inspiration and ideas that were
collected during the
Hear phase were synthesized into concrete design challenge
opportunities during the
Create phase, the aim of theDeliverphase was to formulate the
design challenge
model, finalize the design challenge question, and identify the
steps needed for its
marketing and implementation. This process began with the
conceptualization of the
model by the full-time students in which the design challenge
would be framed (see
Table 3). This model encompasses the individual components that
are identified for
the design challenge question and will serve as the framework
for its marketing and
implementation.
Table 3. Design Challenge Model
Product Ideas
ParticipantsAmateur Individuals
Professional Individuals
Sponsors Open and Free
IncentivesRecognitionSocial Value
Intellectual PropertyParticipant Retain Ownership
Non-Exclusive License for Challenge Organization
-
7/31/2019 Kimberly D. Williams Master's Thesis
41/62
34
To ensure that an active level of interest and engagement was
established for
the design challenge, several marketing plan strategies were
devised. A part of the
marketing plan included a presentation of the project during the
165 th American
Psychiatric Association National Conference on May 6, 2012. In
addition, a Share
Your Story campaign was expected to be released on the new
Scattergood website.
This campaign would provide a forum where individuals will be
able to share
personal experiences relating to a mental health topic that
would be posted on the
website. Another resource that was identified would be the email
listserv of the
Scattergood Foundation grantees that could receive notifications
and periodic updates
about that the design challenge that could help build awareness
and increase the
number of participants for the challenge. In addition, the power
of developing
partnerships with regional organizations was recognized as a
useful tool to build
support and increase the level of community engagement in the
design challenge.
Several potential design challenge questions were conceived
during
brainstorming sessions in April 2012. Initially, it was
determined that the design
challenge would be posted with the release of the new
Scattergood Foundation
website on May 5, 2012. However, in keeping with the tradition
of the design
thinking as a nonlinear and iterative process, it was questioned
whether the
presentation of the design challenge should be postponed and
released on the website
at a later date. In doing so, the Hear phase of the project
would have been continued
an additional few weeks or months. The implementation of the
final Deliver phase
including the release of the first design challenge would have
been postponed until
late summer or early fall of 2012. This revised implementation
plan was the result of
several meetings and brainstorming sessions where the potential
design challenge
questions were reviewed. During those meetings it was discussed
whether there
-
7/31/2019 Kimberly D. Williams Master's Thesis
42/62
35
would be a sufficient level of community engagement in the
design challenge by May
2012. In an effort to heighten the level of interest, awareness,
and engagement in the
community about this project, it was proposed that the process
of divergent thinking
should be continued in order to obtain additional feedback from
the website users
about potential design challenge questions as supplemental
information to the key
informant interviews.
Apprehension regarding the level of community engagement was
assuaged
when the project received an official endorsement from Arthur C.
Evans, Jr., PhD,
Commissioner of the Philadelphia Department of Behavioral Health
and Intellectual
disAbility Services (DBHIDS). In May 2012, he provided the
following statement:
It is important for our field to reframe the issues as
behavioral health andwellness, over illness and diagnosis. My
experience is that people find itdifficult to talk about mental
illness. People are much more receptive whenyou talk about what you
can do to be healthy mentally. We need to developinnovative ways to
have that conversation. This design challenge is anexcellent
strategy for involving the community in our ultimate goal
ofimproving everyone's mental wellness.
In addition, the DBHIDS agreed to serve as a co-sponsor of the
design challenge by
partnering with the Scattergood Foundation to provide
consultation and feedback
throughout the design challenge initiative. During the
completion of the Scattergood
project, DBHIDS was in the process of implementing Mental Health
First Aid
(MHFA) training sessions within the Philadelphia area (DBHIDS,
2012). MHFA is
an international, evidence-based certification course designed
to improve mental
health literacy (MHFA, 2009). The program provides early
intervention training to all
individuals in order to assist fellow community members who are
experiencing
mental health issues. A key to this program is that it is
designed for all community
members to participate regardless of whether they have a
clinical or behavioral health
background. Trained individuals will be better equipped to
recognize, comprehend,
-
7/31/2019 Kimberly D. Williams Master's Thesis
43/62
36
and respond to mental health issues or crises. In addition, they
will be able to offer
their services until the crisis is resolved or professional
treatment can be administered
(DBHIDS, 2012; MHFA, 2009).
To capitalize on this important public health initiative being
undertaken by the
city of Philadelphia, the design challenge goals were modified
to include a targeted
effort to support the MHFA program in some capacity. As of the
completion of this
report, the first design challenge question was not yet
finalized. The release of the
design challenge was due to be implemented by the end of May or
June 2012.
3.2.8 Report Writing
The report writing process consisted of the full-time students
and myself
synthesizing all of the information we amassed during this
project as well as
recounting our experiences. Throughout my participation in this
project I educated
myself about the subjects addressed in the project including
mental health care
policies and treatment, social innovation, design thinking
including human-centered
design, Web 2.0 and social media, as well as the role of
philanthropy as a change
agent. This was achieved by a literature review that included
accessing government
and NGO reports, journal publications, and media articles about
these key topics. In
addition to my review of the current literature, I recorded my
thoughts and accounts
regarding my participant in the active Scattergood project
activities. These activities
were concurrently completed during my participation as a team
member of the project
between January and May of 2012.
-
7/31/2019 Kimberly D. Williams Master's Thesis
44/62
37
3.3 Future of the Scattergood Project
As with any design thinking process, the search for further
advancements and
improvements is ever present. Thus, the Scattergood Project set
a precedent to
constantly be open to new opportunities in order to consistently
grow and evolve from
their efforts. This is apparent in the decision to revise the
implementation plan for the
design challenge. With the release of the design challenge being
postponed, it
provides an excellent opportunity for future Drexel MPH students
to actively
participate in the implementation and management of the initial
design challenge with
the Scattergood Foundation. The goal is for the collaboration
with the Drexel
University School of Public Health to continue to grow and for
future Drexel students
to assist in the implementation of future design challenges on
the Scattergood
Foundation website. In addition, it is hoped that the support
provided by the
Philadelphia DBHIDS will encourage other partnership
opportunities to develop.
Eventually, it is expected that the winning design challenge
solution will be
implemented within the community. This may serve not only to
improve behavioral
health care in the region, but also set an example for other
communities to replicate
the innovative processes or programs presented in the winning
proposal. In addition,
it is hoped that such initiatives will serve as a foundation for
future design challenges
to be implemented by the Scattergood Foundation. Ultimately, I
anticipate that the
dialogue and opportunities generated from the design challenge
initiatives will
continue to foster innovative and sustainable advancements by
the consumers,
practitioners, and policymakers of our regional and national
behavioral health
systems.
-
7/31/2019 Kimberly D. Williams Master's Thesis
45/62
38
4. LESSONS LEARNED
4.1 Personal Narrative
Being involved in the Scattergood Project presented an
unexpected
opportunity for me to expand the resources from which I could
learn more about the
current public health systems and issues faced by the
Southeastern Pennsylvania
region and the nation overall. It was also a unique way to
absorb a large amount of
information regarding current behavioral health issues and
needed improvements
directly from some of the foremost service providers and policy
makers in the region.
My unconventional role in the project did result in some
personal challenges
that I needed to address. Perhaps the greatest challenge was
adjusting to my part-time
status in a full-time project. The students with whom I was
working were enrolled in
the program on a full-time basis and thus able to devote much
more time to this
project. Early in my involvement, I realized that my presence
and participation would
be limited by my part-time status in the program and full-time
job work commitments.
For example, I was not able to attend certain meetings or other
project activities that
took place during business hours. I tried to compensate for this
by participating in
any activities that took place during the evenings and, when
possible, called into
meetings and some key informant interviews by phone. In doing
so, my goal was to
demonstrate my dedication to the project while also not
committing to more than I
was capable of providing due to the time and scheduling
restraints.
It quickly became clear to me that I primarily had to adjust to
expectations for
myself rather then my project team members. In fact, my team
members were always
appreciative of any contribution I was able to make to the
project and easily
maintained reasonable expectations regarding my level of
participation. Due to my
personal dedication to the advancement of mental health issues
and the reduction of
-
7/31/2019 Kimberly D. Williams Master's Thesis
46/62
39
mental illness stigmatization, I found it difficult to not
devote the majority of my time
to this project. However, I knew that it would irresponsible of
me to commit more
time than I was capable of delivering. Therefore, for the
benefit of the project and my
own time management responsibilities, I had to realistically
establish what I would be
capable of contributing. Once these expectations were
established and my function
within the project became better defined, I eventually adjusted
to this role.
Some of the more overarching project challenges identified by my
team
members included adjusting to the application of design thinking
methodology. In
doing so, we had to consistently remind ourselves that design
thinking is a nonlinear
process that may include several iterations of the process as
well as its expected
outcomes. This experimental and non-standardized approach first
became apparent
during the key informant interviews as they were conducted in a
conversational rather
than survey format in order to retain the consumers voice and
opinion in our data.
Ultimately, this led to a richer experience as well as the
collection of more compelling
and valuable information. A few technical challenges were also
experienced with the
utilization of the NVivo program to code the project data.
First, the NVivo software
license only permitted a maximum of two coders. Second, the
program was only
available on one computer, which was located on the Drexel
University campus. As a
result, the program was only accessible during business hours
when the building itself
was open. This was particularly challenging for me since I
maintained a full-time job
during this program and my participation in the project
activities were primarily
conducted after standard business hours.
My overall experience in this project was primarily an extremely
positive one.
Perhaps the most compelling and unanticipated result of this
project experience was
the beginning inspiration towards a new career path for myself.
I entered this
-
7/31/2019 Kimberly D. Williams Master's Thesis
47/62
40
program with the general and vague expectation that I would be
attempting a career
change upon graduation. However, during the majority of this
program, I had no
clear idea of what new direction my career path would take. My
personal interests of
mental health and health care as well as my background in
clinical research motivated
me to choose a public health program over business school or
public policy-centered
programs. However I did not yet know how or where I wanted to
transition from a
career in pharmaceutical clinical research. During the course of
this program, I found
myself instinctively drawn to areas of focus that were tied to
my personal interests
while also demonstrating an unmet need as possible opportunities
for a meaningful
contribution to society. I believe that I discovered three areas
of interest that fit these
desired criteria.
First, the field of public health needs to improve and increase
the integration
of mental health prevention and promotion initiatives into its
academic research and
curriculum, its field-based interventions, as well as its
overall frame of thought as the
field itself continues to gain awareness and a more prominent
position in societys
infrastructure.
Secondly, the field of mental health needs to take advantage of
the increased
focus on health care reform and utilize this momentum to advance
the quality of and
access to mental health care. In addition, this is an
opportunity to further promote the
integration of mental and physical health care into a unified
health care system. By
participating in such a dialogue, mental health may finally
establish itself as a vital
and integral part of overall health care and wellness.
Lastly, the increased use of design thinking methods has the
potential to
revolutionize our increasingly fragmented health care system. In
addition, this school
of thought and practice presents an exceptional opportunity to
increase the
-
7/31/2019 Kimberly D. Williams Master's Thesis
48/62
41
understanding and awareness of mental health issues in our
society as well as the
importance of mental wellness while also reducing stigma. This
may just be the
disruptive innovation that is needed in order to fundamentally
shift the way we view,
address, and discuss mental health concerns.
Had I followed the path of a more traditional Block VIII project
in the form of
a research paper, I doubt I would have come to these same
meaningful conclusions.
Instead I drew a tremendous amount of inspiration from
behavioral health community
leaders we interviewed as well as the project group discussions
with the advisors and
full-time students concerning topics such as Web 2.0, social
media, design thinking,
and human-centered design to achieve socially innovative
solutions. These
experiences led me to incorporate additional readings about
these unfamiliar subjects
with my previously anticipated research on mental health and
health care reform. As
a result, I feel that my project took a direction that I would
not have considered had I
been left to my own devices while conducting traditional and
solitary research for a
literature review based project. Luckily, I was able to
participate as an active member
of a project team rather than simply as a passive consumer of
information. This
expanded my horizons and opened me up to a new way of evaluating
the current
systemic, policy, and social issues affecting behavioral health
care.
4.2 Future Executive MPH Student Opportunities
At the inception of this collaboration between Drexel University
and the
Scattergood Foundation, the goal has always been maintained that
future MPH
students could participate in this project as it continues to
evolve. Initially, it was
assumed that only full-time MPH students would participate as a
part of their
yearlong CBMP. However, the opportunity fortuitously presented
itself for me to
-
7/31/2019 Kimberly D. Williams Master's Thesis
49/62
42
contribute as an Executive MPH student in fulfillment of my
Block VIII Independent
Study requirement. After having completed this project, I can
conclude that this is
may serve as an exceptional opportunity for future Executive MPH
students to
complete










![LT Kimberly Williams examines a patient aboard USNSOn the Front Cover] LT Kimberly Williams examines a patient aboard USNS Mercy (T-AH 19) during humanitarian efforts off the coast](https://img.pdfslide.us/doc/110x75/5b0a26737f8b9abe5d8dc503/lt-kimberly-williams-examines-a-patient-aboard-on-the-front-cover-lt-kimberly-williams.jpg)