Embed Size (px)
Citation preview

1

2

Role of Kidney in Regulation of Arterial
Blood Pressure
3

Presentation Agenda
Kidney Functions .E.C.V. control .NaturesisRAS system
4

5

6

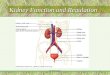
The kidneys - what are they for ?
Elimination of waste substancesSalvage of essential compoundsRegulation of ions: H+ (pH), Na+, K+, Ca2+
Regulation of plasma volume / blood pressureRegulation of plasma osmolalityProduction of hormones … 7

Regulation of body fluid osmolality & volume: Excretion of water and NaCl is regulated interacting with cardiovascular, endocrine, & central nervous systems
Regulation of electrolyte balance: Daily intake of inorganic ions (Na+, K+, Cl-, HCO3
-, H+, Ca2+, Mg+ & PO43-) should be
matched by daily excretion through kidneys.
Regulation of acid-base balance: Kidneys work in concert with lungs to regulate the pH in a narrow limits of buffers within body fluids. 8

Excretion of metabolic products & foreign substances :
urea from amino acid metabolism uric acid from nucleic acids creatinine from muscles end products of hemoglobin metabolites hormone metabolites
foreign substances ( e.g., drugs, pesticides, & other chemicals ingested in the food )
9

Production and secretion of hormones: Renin ( activates the Renin- Angiotensin - Aldosterone system, thus regulating blood pressure & Na , K balance ) Prostaglandins/ kinins ( bradykinin = vasoactive , leading to modulation of renal blood flow & along with AngiotensinII affect the systemic blood flow ) 1,25-dihydroxyvitamin D3
( stimulates Ca2+ resorption &bone deposit ) Erythropoietin ( stimulates red blood cell formation by bone marrow ).10

CONTROL OF EXTRACELLULAR FLUID VOLUME
Effective circulating volume
Volume sensors
Kidney
Adjustment to NaCl excretion
11

The 'effective circulating volume' (ECV) is that part of
the ECF that perfuses the tissues and is related to a
concept of the ‘fullness’ of the circulation.
Normally ECF and ECV are equivalent. However, under
pathological conditions, e.g. heart failure, the ECV may
be low in spite of the fact that ECF is normal.
Importantly the kidneys respond to changes of ECV:
when it is reduced Na excretion is reduced which also
retains water; when it is too high Na excretion is raised
(a natriuresis is induced) and water is correspondingly
lost.12

SENSORS OF EFFECTIVE CIRCULATING VOLUME
Most importantly ECV sensors exist in the high-pressure
(systemic arterial) and low pressure (systemic venous,
pulmonary) sides of the circulation.
High pressure ECV sensors:
Arterial baroreceptors (carotid sinus and aortic arch)
Juxtaglomerular apparatus of the kidney and the afferent arteriole
Low pressure ECV sensors:
Cardiac atria
Pulmonary vasculature 13

14

15

16

17

Arterial pressure is a signal for regulation of NaCl excretion. arterial pressure NaCl reabsorbed in the proximal tubule more NaCl to the MD TGF autoregulation RBF, GFR.
In addition, there is an accompanying increase in urine Na+ , volume output: pressure natriuresis/diuresis. Pressure natriuresis can normalize BP by decreasing the effective circulating volume – this response connects BP and ECFV.
18

2. Decrease PT NaCl reabsorption
3. I ncrease [NaCl] at macula
densa generates TGF signal
Natriuresis
Diuresis “Pressure Natriuresis”
1. I ncrease BP & renal
perfusion pressure
I ncrease NaCl
delivery to
distal nephron
4. I ncrease aff erent arteriole resistance
5. Autoregulate RBF, GFR
40% increase volume flow f rom PT
?
19

1. Summarize the chain of events known as “pressure natriuresis” - the effect of arterial blood pressure on renal excretion of NaCl.
2. Diagram the six feedback relationships connecting ECFV, BP and AngII/SNS.
3. Summarize how lesions in the regulation of renal sodium chloride transport and lesions in Na+ transporters themselves can lead to hypertension or hypotension.
4. Summarize the homeostatic mechanisms governing "escape" from mineralocorticoid excess (real or apparent excess): transport along the nephron, endocrine adjustments.
20

AII fluid retentionvia aldosterone Na reabsorption
BP
AIISNSECFV
+
+
+
-
-
-
BP ECFVvia
pressure natriuresis
AII/SNS vasoconstriction
BP
PV=nRT
BP AII/SNSvia
baroreceptorsmacula densa
ECFV ANP renin AII aldosterone
Feedback relationship among blood pressure (BP), Angiotensin II and sympathetic nervous system (AII/SNS), and extracellular fluid volume (ECFV, a function of Na+ reabsorption)
21

RENAL SYMPATHETIC NERVES
Decreased effective
circulating volume
Increased sympathetic
activity
baroreceptorreflex
Constriction of afferent and
efferent arterioles
Stimulation of renin secretion
Reduced GFR and filtered load of Na
Decreased Na excretion
Decreased Na excretion
NaCl reabsorption increased by
nephron
Sympathetic fibres innervate the afferent and efferent arterioles as well as cells of the nephron. The fibres respond as part of the efferent arm of the baroreceptor reflex.
An example
22

RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEMThe renin-angiotensin-aldosterone system is the key in regulating ECV by controlling NaCl, and water, reabsorption by the nephron.
podocyte
Bowman’s space
juxtaglomerular cells
capillaries
mesangial cells
afferent
arteriole
macula densa
efferent
arteriole
Cells in the afferent/efferent arterioles of the glomerulus are the site of synthesis, storage and release of renin
23

RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM1. Perfusion pressure
Decrease of perfusion pressure , as occurs if ECV is reduced, stimulates renin secretion
2. Sympathetic nerve activitySympathetic nerves activated, as occurs if ECV is reduced, increases renin secretion3. NaCl delivery to the macula densaWhen NaCl delivery to the distal tubule and macula densa is reduced , as would occur if ECV is reduced, increases renin secretion.In all three mechanisms renin secretion is reduced when the opposite conditions prevail.
24

Renin is a proteolytic enzyme, its substrate is circulating
angiotensiogen. The result is a decapeptide, angiotensin I This is converted to an octapeptide angiotensin II in
the lung by an angiotensin converting enzyme (ACE)
Angiotensin II has the following actions Stimulates aldosterone release from the adrenal cortex Is a systemic (include renal arteriolar) vasoconstrictor Stimulates ADH secretion Enhances proximal tubule NaCl reabsorption and
inhibits renin release
25

Liver
Lung
angiotensinogen
angiotensin I
Kidney
renin
Angiotensin II
aldosterone
Brain ADH
26

27

ACTIONS OF ALDOSTERONE
Na+
ATPNa+
H2O
aldo
RAR
Nucl
mito
Aldosterone binds to a baso-
lateral receptor. The receptor complex
stimulates transcription of
apical Na+ channels and ATP
synthesis
Aldosterone conserves Na+
An increase of circulating levels
increases NaCl reabsorption via
principal cells in the distal tubule/
collecting duct
Na+ uptake from the lumen is enhanced and Cl- and H2O follow.
The process is relatively slow. 28

BP BV
Na+ depletion
NE release from nerve
ending
RENIN RELEASE
BP BV
Na+ retention+ -
Vasoconstriction
Aldosteronesecretion
Angiotensin release
++ +
++
+
Stimulants for ADH 1) ECF volume 2) osmolality of plasma
+
29

30

Mean Arterial Pressure
MAP = CO X
CO = HR X SV
SNS Blood volume Heart contractility
Venous tone
PVR
myogenic tonevascular responsivenessnervous control
vasoactive metabolitesendothelial factorscirculating hormones
31

Renalfunction
Bloodvolume
Venoustone
Venousreturn
Heartrate
Nervouscontrol
Muscularresponsiveness
Myocardialcontractility
Strokevolume
Cardiacoutput
CNSfactors
Reninrelease
Angiontensin II formation
Intrinsic vascularresponsiveness
Peripheralresistance
Nervouscontrol
Renalfunction
Mean arterialpressure
Factors that Govern the Mean Arterial Pressure
32

HEMORRHAGE:
--- decreases arterial pressure
--- leading to activation of kidney sympathetic nerves via
baroreceptor reflex --- NOR elicits intense vasoconstriction of both afferent & efferent arterioles to cause lowering of RBF & GFR 33

--- A rise in sympathetic activity increases EPI & angiotensin II release , leading to further vasoconstriction (& thus RBF decrease) --- Resultant increase in vascular resistance in kidneys & elsewhere elevates total peripheral resistance => increase in blood pressure (BP = cardiac output . total peripheral resistance) => offsets the fall (due to hemorrhage) in mean arterial pressure
34