Embed Size (px)
Citation preview

KUA
T
T1mompw
pctsed
t
©3
T
idney Preserving Solutions Containing Lidocaine May Increaserological Complication Rate After Renal Transplantation:n In Vitro Study
.A. Drewa, Z. Wolski, P. Galazka, Z. Wlodarczyk, and A. Wozniak
ABSTRACT
Objective. The frequency of urological complications after renal transplantation is up to12%. Some authors consider that lidocaine addition to preservation solutions produces afavorable influence on allograft function. However, lidocaine may influence urinary tractepithelial cells. The aim of this work was to establish the influence of lidocaine on culturedprimary rabbit urothelial cells (PRUC) as a tool to understand mechanisms of urologicalcomplications after kidney transplantation.Design and Methods. A PRUC culture was established from an 8-month-old malerabbit bladder. The cells were cultured alone and then with in various concentrations oflidocaine for 24 hours or 1 hour. After an additional 24 hours, cell viability was assessedby the trypan blue exclusion test. Student’s t test was used for statistical analysis, withsignificance set at P � .05.Results. The cytotoxic effects of lidocaine on PRUC were concentration dependent.One-hour exposure of PRUC culture to 0.5 or 1.0% lidocaine decreased cell viability. Bothlidocaine concentrations decreased cell viability in PRUC culture after a 24-hourincubation; even 0.25% lidocaine caused changes in the PRUC culture morphology aftera 1-hour incubation. Cells became rounded and detached from the growth surface. No cellswere observed in the monolayer after 1-hour incubation with 1% of lidocaine.Conclusions. The toxic effects of lidocaine on PRUC may forecast problems withsupplementation of kidney preservation solutions, leading to impaired epithelial layer
healing with an increased risk of urological complications.alsiHpu
lc
N
M
HE FREQUENCY OF isolated urological complica-tions after renal transplantation ranges from 2% to
2%.1,2 Ureteral obstruction, leakage, and fistulas are theost common complications.3–7 Surgical skill kidney anat-
my, ureteral vasculature, and perioperative drug manage-ent may influence urological complications.1,8,9 Renal
elvis or ureteral necrosis after transplantation may occurith preservation of renal function.1,10,11
Although lidocaine is not a component of common kidneyreservation solutions, like EuroCollins or University of Wis-onsin, its addition has been proposed to favorably influencehe postischemic reperfusion injury.12–15 Schulak et al15
howed that donor pretreatment with intravenous lidocainenhanced renal excretory function after transpalantation andecreased the incidence of acute tubular necrosis.Following intravenous application, lidocaine is delivered
o all tissues, resulting in hepatic production of nonactive p
2005 by Elsevier Inc. All rights reserved.60 Park Avenue South, New York, NY 10010-1710
ransplantation Proceedings, 37, 2107–2110 (2005)
nd active toxic lidocaine derivatives.16 A toxic effect ofidocaine and its metabolites on neuronal cell lines has beenhown.17 Lidocaine concentrations within the graft may bencreased during preservation with enriched solutions.
owever, its effect on urinary tract epithelial cells areoorly understood particularly as they may predispose torological complications.The aim of this work was to establish the influence of
idocaine on primary rabbit urothelial cells (PRUC)ulture.
From the Medical Biology Department, Collegium Medicum,icolaus Copernicus University, Bydgoszcz, Poland.Address reprint requests to Tomasz A. Drewa, MD, Collegiumedicum, Nicolans Copernicus University, Medical Biology De-
artment, Karlowicza 24, Bydgoszcz 85-094, Poland.0041-1345/05/$–see front matterdoi:10.1016/j.transproceed.2005.03.018
2107

MC
Au(eBmw3roe((c(wwscwM
C
C2
cTtdhg
ifch
uwCap
ts
R
TdPsl
Fcc
Fpw
2108 DREWA, WOLSKI, GALAZKA ET AL
ATERIALS AND METHODSells
PRUC culture was established from 8-month-old male rabbitrinary bladder wall. After ketamine (25 mg/kg mc IM) and scoline50 mg/kg) euthanasia, a bladder wall sample (5 � 5 cm) wasxcised, immersed in sterile phosphate buffered saline (PBS,iomed), and underwent mechanical separation of the urinaryucosa from the muscle layer. The mucosa samples of two mm3
ere digested in 0.1% collagenase type I (Sigma) for 2 hours in7°C. Finally, the cell pellet after centrifugation (800 g/5 min) wasesuspended in the complete culture medium, which was composedf 1:1 DMEM and F-12 mixture supplemented with 10% FBS,pidermal growth factor (EGF, Sigma), bovine pituary extractSigma), cholera toxin (30 ng/mL) (Sigma), penicillin (100 IU/mL)Polfa), and streptomycin (100 ug/mL) (Polfa). Under sterileonditions, the cells were plated into 25-cm2 culture dishesGreiner). Cells were grown at 37°C in a humidified atmosphereith 5% CO2. When confluence was reached, cells were detachedith trypsin 1� solution (2.5 g trypsin per litre HBSS, Sigma) for
ubculture. After three passages, cells were identified as epithelialells by morphological criteria under an inverted microscope, asell as by quantification of cytokeratins (Anti-Cytokeratin Clone:NF 116, DAKO).
ytotoxicity Tests
ells, resuspended in complete culture medium, were seeded into4-well plates at a density of .5 � 104/cm2. For the experiments,
ig 1. Cells viability after 1-hour incubation with lidocaine soluounted cells. Mean values (�SD) from 10 wells for each lidocainonsidered statistically significant.
ig 2. Results of cells treated with lidocaine solutions viabilitroportion of viable cells to all counted cells. Mean values (�SD)
ells of controls. P � .05 was considered statistically significant.ells were grown to confluence (approximately 5 � 104 cells/well).he possibly toxic effect of lidocaine was assessed by two tests. In
he first test, media were replaced with solutions containing serialilutions of lidocaine (0.5%, 0.25%, 0.13%, and 0.06% v/v) for 24ours. Thereafter, the media were replaced with complete cellrowth medium. Cells viability was assessed over the next 24 hours.
In the second test, media were replaced by solutions contain-ng serial dilutions of lidocaine (2%, 1%, 0.5% and 0.25% v/v)or 1 hour. Thereafter, the media were replaced with completeell growth medium. Cells viability was assessed after the next 24ours.Cell viability was examined using the trypan blue exclusion test
sing Neubauer’s cytologic chamber for cell counting. Cell viabilityas expressed as the proportion of viable to total counted cells.ell morphology after incubation with lidocaine solutions was alsossessed using inverted microscope and documented by photogra-hy.Mean values (�/�SD) from 10 wells for each lidocaine concen-
ration were compared to controls. Student’s t test was used fortatistical analysis with P � .05 considered significant.
ESULTS
he cytotoxic effect of lidocaine on PRUC culture wasependent on its concentration. One-hour exposure ofRUC cultures to lidocaine at 0.5 and 1.0% concentrationshowed decreased cell viability (Fig 1). As little as 0.06%idocaine concentration decreased cell viability in PRUC
. Cell viability was expressed by proportion of viable cells to allncentration were compared to 10 wells of controls. P � .05 was
lysis after 24-hour incubation. Cell viability was expressed by10 wells for each lidocaine concentration were compared to 10
tionse co
y anafrom
cnw2
Pmacta
D
Nattr
ata
psu
eaailf
(t
iculpevttc
ckpsoct
uthi
R
cJ
F(
LIDOCAINE MAY INCREASE UROLOGICAL COMPLICATIONS 2109
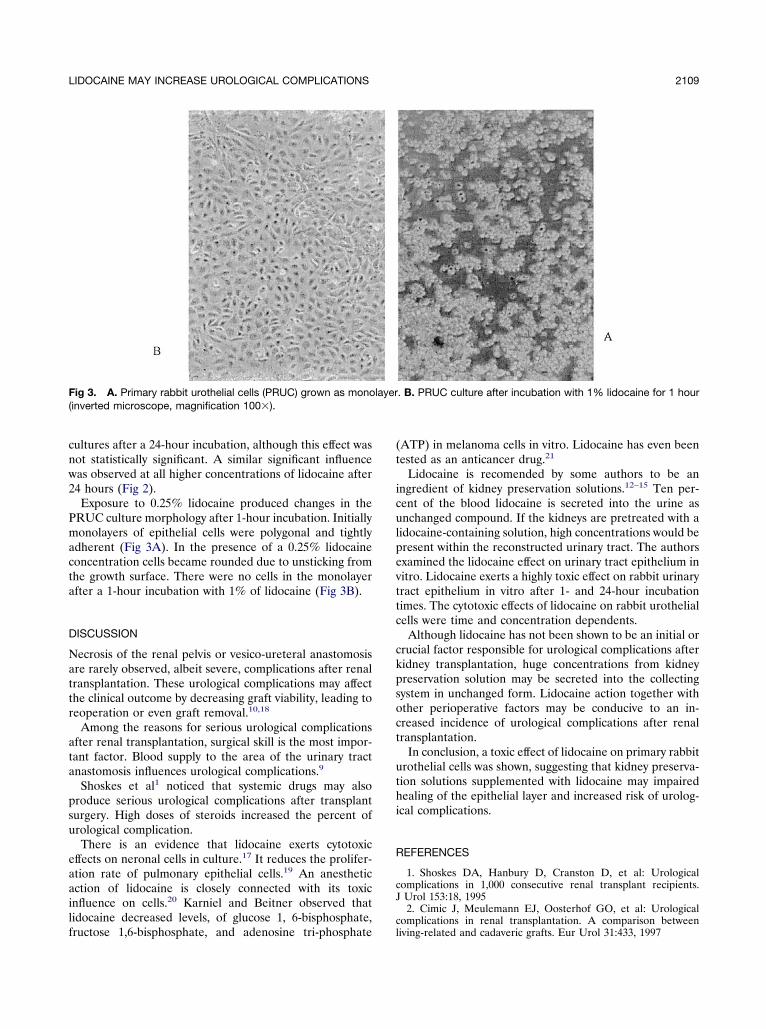
ultures after a 24-hour incubation, although this effect wasot statistically significant. A similar significant influenceas observed at all higher concentrations of lidocaine after4 hours (Fig 2).Exposure to 0.25% lidocaine produced changes in the
RUC culture morphology after 1-hour incubation. Initiallyonolayers of epithelial cells were polygonal and tightly
dherent (Fig 3A). In the presence of a 0.25% lidocaineoncentration cells became rounded due to unsticking fromhe growth surface. There were no cells in the monolayerfter a 1-hour incubation with 1% of lidocaine (Fig 3B).
ISCUSSION
ecrosis of the renal pelvis or vesico-ureteral anastomosisre rarely observed, albeit severe, complications after renalransplantation. These urological complications may affecthe clinical outcome by decreasing graft viability, leading toeoperation or even graft removal.10,18
Among the reasons for serious urological complicationsfter renal transplantation, surgical skill is the most impor-ant factor. Blood supply to the area of the urinary tractnastomosis influences urological complications.9
Shoskes et al1 noticed that systemic drugs may alsoroduce serious urological complications after transplanturgery. High doses of steroids increased the percent ofrological complication.There is an evidence that lidocaine exerts cytotoxic
ffects on neronal cells in culture.17 It reduces the prolifer-tion rate of pulmonary epithelial cells.19 An anestheticction of lidocaine is closely connected with its toxicnfluence on cells.20 Karniel and Beitner observed thatidocaine decreased levels, of glucose 1, 6-bisphosphate,
ig 3. A. Primary rabbit urothelial cells (PRUC) grown as monoinverted microscope, magnification 100�).
ructose 1,6-bisphosphate, and adenosine tri-phosphatecl
ATP) in melanoma cells in vitro. Lidocaine has even beenested as an anticancer drug.21
Lidocaine is recomended by some authors to be anngredient of kidney preservation solutions.12–15 Ten per-ent of the blood lidocaine is secreted into the urine asnchanged compound. If the kidneys are pretreated with a
idocaine-containing solution, high concentrations would beresent within the reconstructed urinary tract. The authorsxamined the lidocaine effect on urinary tract epithelium initro. Lidocaine exerts a highly toxic effect on rabbit urinaryract epithelium in vitro after 1- and 24-hour incubationimes. The cytotoxic effects of lidocaine on rabbit urothelialells were time and concentration dependents.
Although lidocaine has not been shown to be an initial orrucial factor responsible for urological complications afteridney transplantation, huge concentrations from kidneyreservation solution may be secreted into the collectingystem in unchanged form. Lidocaine action together withther perioperative factors may be conducive to an in-reased incidence of urological complications after renalransplantation.
In conclusion, a toxic effect of lidocaine on primary rabbitrothelial cells was shown, suggesting that kidney preserva-ion solutions supplemented with lidocaine may impairedealing of the epithelial layer and increased risk of urolog-
cal complications.
EFERENCES
1. Shoskes DA, Hanbury D, Cranston D, et al: Urologicalomplications in 1,000 consecutive renal transplant recipients.Urol 153:18, 19952. Cimic J, Meulemann EJ, Oosterhof GO, et al: Urological
. B. PRUC culture after incubation with 1% lidocaine for 1 hour
layeromplications in renal transplantation. A comparison betweeniving-related and cadaveric grafts. Eur Urol 31:433, 1997

st
eU
c
ct
ra
ct
bkn
n1
ce1
rtT
iti
Ec5
mi
a
lt
a3
it2
ca
ta
2110 DREWA, WOLSKI, GALAZKA ET AL
3. van Roijen JH, Kirkels WJ, Zietse R, et al: Long-term grafturvival after urological complications of 695 kidney transplanta-ions. J Urol 165:1884, 2001
4. Cullmann HJ, Prosinger M: Necrosis of the allograft ureter–valuation of different examination methods in early diagnosis.rol Int 45:164, 19905. Blaszak RT, Dunn JF, Finck CM: Use of appendix for
omplete transplant ureteral necrosis. Pediatr Transpl 7:234, 20036. Yang Y, Hong B, He Q, et al: Diagnosis and treatment of
omplete necrosis of the ureter after cadaveric renal transplanta-ion. Zhonghua Wai Ke Za Zhi 40:254, 2002
7. Hidalgo G, Vyas S, Hong J, et al: Complete necrosis of theenal pelvis and ureter after cadaveric renal transplantation. Pedi-tr Transplant 4:60, 2000
8. Butterworth PC, Horsburgh T, Veitch PS, et al: Urologicalomplications in renal transplantation: impact of a change ofechnique. Br J Urol 79:499, 1997
9. Wolters HH, Schult M, Heidenreich S, et al: The anastomosisetween renal polar arteries and arteria epigastrica inferior inidney transplantation: an option to decrease the risk of ureterecrosis? Transpl Int 14:422, 200110. Schlitt HJ, Hoffmann MW: Reconstruction of necrotic kid-
ey graft pelvis with a vascularized small bowel patch. Transpl Int4:95, 200111. Tanabe K, Takahashi K, Kawaguchi H, et al: Surgical
omplications of pediatric kidney transplantation: a single centerxperience with the extraperitoneal technique. J Urol 160:1212,99812. Walaszewski J, Rowinski W, Pacholczyk M, et al: Multiple
isk factor analysis of delayed graft function (ATN) after cadavericransplantation: positive effect of lidocaine donor pretreatment.
ranspl Proc 23:2475, 1991 613. Walaszewski J, Rowinski W, Chmura A, et al: Decreasedncidence of acute tubular necrosis after cadaveric donor transplan-ation due to lidocaine donor pretreatment and low-dose dopaminenfusion in the recipient. Transplant Proc 20:913, 1988
14. Erkasap N, Ates E, Erkasap S, et al: Lidocaine-containinguro-Collins solution prevents renal injury in the isolated perfused
anine kidney exposed to prolonged cold ischemia. Physiol Res1:493, 200215. Schulak JA, Novick AC, Sharp WV, et al: Donor pretreat-ent with lidocaine decreases incidence of early renal dysfunction
n cadaver kidney transplantation. Transpl Proc 2:353, 199016. Narang PK, Crouthamel WG, Carliner NH, et al: Lidocaine
nd its active metabolites. Clin Pharmacol Ther 24:654, 197817. Radwan IA, Saio S, Goto F: Growth cone collapsing effect of
idocaine on DRG neurons is partially reversed by several neuro-rophic factors. Anesthesiology 97:630, 2002
18. Schaul DB, Xie HW, Shimada H, et al: Venous ischemia ascause of ureteral necrosis in transplanted ureters. J Pediatr Surg
4:1725, 199919. Nishina K, Mikawa K, Morikawa O, et al: The effects of
ntravenous anesthetics and lidocaine on proliferation of culturedype II pneumocytes and lung fibroblasts. Anesth Analg 94:385,00220. Kasaba T, Onizuka S, Takasaki M: Procaine and mepiva-
aine have less toxicity in vitro than other clinically used localnesthetics. Anesth Analg 97:85, 2003
21. Karniel M, Beitner R: Local anesthetics induce a decrease inhe levels of glucose 1, 6- bisphosphate, fructose 1,6-bisphosphate,nd ATP, and in the viability of melanoma cells. Mol Genet Metab
9:40, 2000![5% Lidocaine Medicated Plaster for the Treatment of ... · Postherpetic neuralgia (PHN) is the most common complication of herpes zoster [1]. Transition from acute herpes zoster to](https://img.pdfslide.us/doc/110x75/60c008b7a73b1514f9212ab4/5-lidocaine-medicated-plaster-for-the-treatment-of-postherpetic-neuralgia-phn.jpg)