Embed Size (px)
Citation preview

Kia Afshar October 2015
Mitral Regurgitation Causes HF
Exacerbates HF

A Largely Untreated Patient Population
Total MR Patients1,2
Eligible for Treatment3,4 (MR Grade ≥3+)
4,100,000
1,700,000
Annual MV Surgery5
Annual Incidence3 (MR Grade ≥3+)
250,000
30,000 Only 2% Treated Surgically
14% Newly Diagnosed Each Year
1,670,000 Untreated Large and Growing Clinical Unmet Need
1. US Census Bureau. Statistical Abstract of the US: 2006, Table 12. 2. Nkomo et al. Burden of Valvular Heart Diseases: A Population-based Study, Lancet, 2006; 368: 1005-11. 3. Patel et al. Mitral Regurgitation in Patients with Advanced Systolic Heart Failure, J of Cardiac Failure, 2004. 4. ACC/AHA 2008 Guidelines for the Management of Patients with Valvular Heart Disease, Circulation: 2008 5. Gammie, J et al, Trends in Mitral Valve Surgery in the United States: Results from the STS Adult Cardiac Database, Annals of Thoracic Surgery 2010.
Mitral Regurgitation 2009 U.S. Prevalence

Key Points Etiology of MR: Primary (i.e., valvular or degenerative - DMR) Secondary (i.e., ventricular or functional - FMR)
Primary (DMR) is associated with heart failure and excess mortality in the absence of surgical repair.
The MitraClip COAPT Trial is THE pivotal trial for FMR.
The standard of care for secondary (FMR) is not defined. GDMT is essential Surgery decreases symptoms but appears to have little
influence on mortality.
Nkomo et al. Burden of Valvular Heart Diseases: A Population-based Study, Lancet, 2006; 368: 1005-11. Suri R et al., JAMA 2013;310:609-16 Nishimura R, et al., J Am Coll Cardiol 2014;63:2438-88

Why Do Mitral Valves Fail?
Degenerative (Primary) Functional (Secondary) Starts with the ventricle

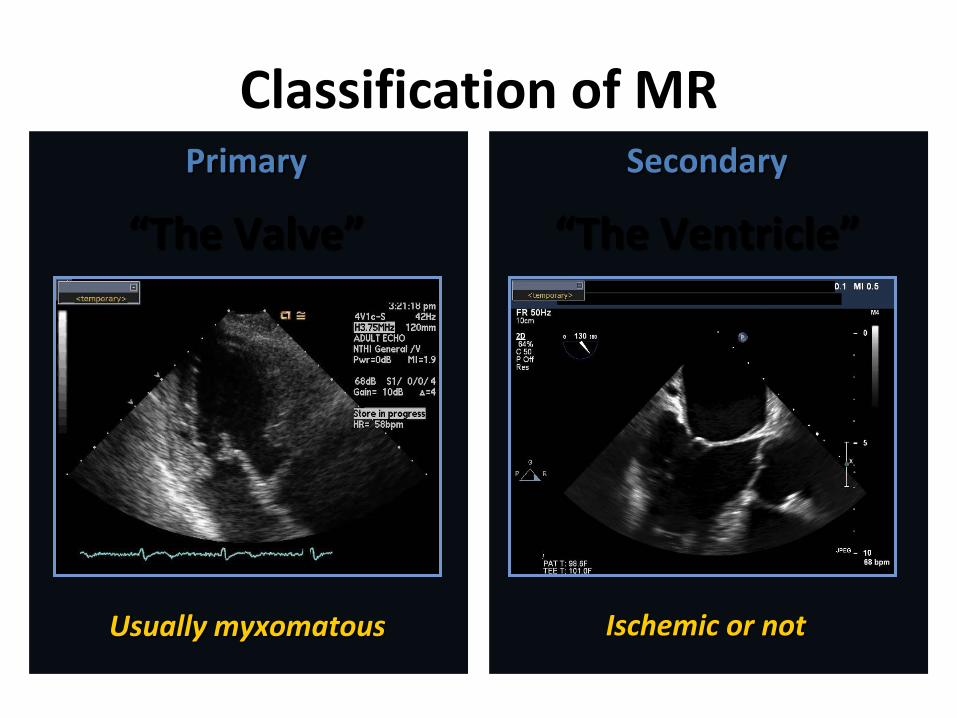
Classification of MR
Sorajja, Paul, MD; Abbott Northwestern Hospital
Primary
“The Valve”
Secondary
“The Ventricle”
Usually myxomatous Ischemic or not

Degenerative MR (Primary)
• Primary disease of valve and chordae with excess leaflet motion (prolapse flail)
• LV systolic function is initially normal but fails with time.

Degenerative MR
Ruptured chord leads to flail segment Barlow’s Valve

8
Asymptomatic MVP Natural History
Avierinos JF, et al. Circulation 2002;106:1355
100
90
80
70
60
50
Surv
ival
%
0 2 4 6 8 10
≥2 secondary RF
0-1 secondary RF
95 ±2
70 ±5
55 ±9
Risk Factors Primary • MR ≥3 • EF <50% Secondary • Age ≥50 yrs • Atrial fibrillation • LA enlargement • Flail leaflet
Years after diagnosis
Any primary RF

9
Asymptomatic Primary MR Severity and Survival
Enriquez-Sarano M et al. NEJM 2005;352:875-83
Worse Survival
100
90
80
70
60
50
0
Surv
ival
(%)
Years
0 1 2 3 4 5
P<0.01
ERO <20mm2 (91 ±3%)
ERO ≥40mm2 (58 ±9%)
ERO 20-39mm2 (66 ±6%)
More CV Events
70
60
50
40
30
20
10
0
Rate
of C
ardi
ac E
vent
s %
Years
0 1 2 3 4 5
ERO <20mm2 (15 ±4%)
ERO 20-39mm2 (40 ±7%)
ERO ≥40mm2 (62 ±8%)

10
Flail Mitral Leaflet Natural History
Ling L, et al. N Engl J Med 1996; 335:1417-1423
100
80
60
40
20
0
Surv
ival
%
Years After Diagnosis
0 1 2 3 4 5 6 7 8 9 10
P<0.001
Class I or II
Class III or IV
Mortality 4% per year
34% per year

Degenerative Mitral Regurgitation Indications for Repair
• Symptomatic patients with 3 or 4+ MR (Class I)
• Asymptomatic patients with 3 or 4+ MR
– Abnormal LV function (Class IIa) - LVEF < 0.60, LV ESD > 45 mm
– Normal LV function (Class IIb) • Consider if high likelihood
successful repair & atrial fibrillation or pulmonary hypertension
Mitral valve repair with posterior annular ring & resection of redundant tissue

MitraClip® System

Transcatheter Mitral Repair
May be considered for prohibitive risk patients with primary MR and severe symptoms
ACC/AHA Guidelines – Primary MR
Classification of MR
Sorajja, Paul, MD; Abbott Northwestern Hospital
Primary
“The Valve”
Secondary
“The Ventricle”
Usually myxomatous Ischemic or not

Functional MR valve is initially normal
MR results from tethered leaflets & annular dilatation


17
Secondary Mitral Regurgitation A Harbinger of Poor Outcome
Two-fold Increase Risk of Death Grigioni F, et al. Circulation 2001;103:1759-64; Basket JF, et al. Can J Cardiol 2007;23:797-800
1.0
0.8
0.6
0.4
0.2
0.0
Surv
ival
(%)
Years
0 1 2 3 4 5
P<0.001
50
40
30
20
10
0 De
ath
or h
eart
failu
re
hosp
italiz
atio
n %
Follow-up time (days)
0 365 730 1095
P=0.0006
MI w/o MR
MI with MR 61 ±6
38 ±5
Mitral Regurgitation
No Mitral Regurgitation
Post-MI SOLVD (EF >35%)

18
Hospitalization-free survival decreased with increased MR severity1
100
80
60
40
20
0
Hosp
italiz
atio
n-fr
ee S
urvi
val (
%)
Years
0 1 2 3 4 5 6 7
P<0.01
No MR(40%)
Severe MR 7%)
Mild/mod MR (25%)
Transplant-free survival decreased with increased MR severity2
100
90
80
70
60
50
40 Tr
ansp
lant
-free
Sur
viva
l (%
)
Days
0 500 1000 1500 2000
Grade IV (46.5 ±6.7%)
Grade III (68.5 ±4.6%)
Secondary Mitral Regurgitation Increased Severity = Increased Morbidity
1. Rossi A, Dini FL, Faggiano P, et al. Independent prognostic value of functional mitral regurgitation in patients with heart failure: a quantitative analysis of 1256 patients with ischemic and non-ischaemic dilated cardiomyopathy. Heart. 2011;97(20):1675-1680.
2. Bursi F, Barbieri A, Grigioni F, et al. Prognostic implications of functional mitral regurgitation according to the severity of the underlying chronic heart failure: a long-term outcome study. Eur J Heart Fail. 2010;12(4):382-388.
Grade II (64.4 ±4.9%)
No MR & Grade I (82.7 ±3.1%)

Pathophysiology of MR Increasing Mitral
Regurgitation
Increase Load/Stress
Muscle Damage/Loss
Dysfunction of Left Ventricle
Dilation of Left Ventricle
1 year mortality
up to 57%1
1 Cioffi G, et al. Functional mitral regurgitation predicts 1-year mortality in elderly patients with systolic chronic heart failure. European Journal of Heart Failure 2005 Dec;7(7):1112-7

Functional MR
• Treatment Goals: • - Reverse remodeling • - Improve survival • - Improve symptoms • - Decrease hospitalizations for CHF • - Increase time to transplant or VAD

Current Therapy Considerations
Medical Therapy
Less Invasive
Increased MR Reduction
MV Surgery
MitraClip®
*Reference Source: Instructions For Use See important safety information referenced within

Mitral Valve Surgery in DCM
A. Wu, et. Al. JACC 2005:45, 381-387
Even
t-fr
ee S
urvi
val
annuloplasty
control

MitraClip Proposition
Safe & Minimally Invasive Diminished Mitral Regurgitation
Increased forward stroke volume & cardiac output
Decreased Systemic Vascular Resistance
Decreased LVED Pressure & Volume
Decreased LA Pressure & Pulmonary Vascular Resistance

August 2009 Intermountain HF Clinic
HISTORY OF PRESENT ILLNESS: Mr. K. is a 64-year-old male referred to heart failure clinic with increasing short of breath, nausea and dry heaves. The patient had his first MI with a stent placed in Indiana at age 42. He had done well until June 2, 2009 when he had burning sensation in his stomach, along with severe chest pain starting at 7:00 p.m. He was transferred to the IMC at 5:00 AM the next day. He underwent coronary artery angiography and had 2 bare metal stents placed in the LAD and distal circumflex. The patient required an intra-aortic balloon pump. His initial troponin was 812. Since that time he has been hospitalized twice for decompensated heart failure. He has PND, dry heaves, right upper quadrant pain and constipation. He is short of breath at rest with orthopnea and class 4 CHF. Metoprolol and lisinopril were discontinued secondary to hypotension. Current medications are carvedilol 3.125 mg twice daily, lasix 20 mg once a day and Aldactone.

EP Consult
IMPRESSION AND RECOMMENDATIONS: Ischemic cardiomyopathy. The patient has an ischemic cardiomyopathy. Given his narrow QRS complex, he does not meet the criteria for a biventricular ICD. He had his myocardial infarction in June; now after 2.5 months of therapy his ejection fraction has worsened; I do not think that is going to get better. We should look towards an ICD implant. He is being considered for possible mitral valve treatment for his severe mitral regurgitation and possible heart transplant down the line if he does not get better. Thanks for the interesting consultation.

Baseline Echo

Qualifying Echo 10/09

MitraClip 1/2010

MitraClip 1/2010

MitraClip 1/2010

First MitraClip 1/2010
Jet isolated laterally

MitraClip 1/2010
Discharge Home POD #1

RHC 9/2010

2013 Echo
2009 2013
EF 27 32
LVIDd 5.84 5.31
LVIDs 4.87 4.34
LVOT VTI 9.4 15.2

2014 Intermountain HF Clinic
HISTORY OF PRESENT ILLNESS: Mr. K. is here for scheduled follow up. He is feeling very well with only one concern. He tried to restart pravastatin. . . NYHA classification: I.

36
Randomize 1:1
Clinical and TTE follow-up: Baseline, Treatment, 1-week (phone)
1, 6, 12, 18, 24, 36, 48, 60 months
Control group Standard of care
N=215
Symptomatic heart failure subjects who are treated per standard of care Determined by the site’s local heart team as not appropriate for mitral valve surgery
MitraClip N=215
Significant FMR (≥3+ by core lab)
Trial Design 430 patients
Clinical Investigational Plan 11-512: Version 5.1, November 11, 2013. COAPT protocol approved by FDA July 27, 2012

Conclusions • Mitral Regurgitation is undertreated • Primary MR warrants surgery or if high risk consider
mitraclip if: – Symptoms – Decreased EF, Pulmonary Hypertension, AF – Consider if severe and experienced repair surgeon
• Mitral Regurgitation exacerbates HF – Consider Mitraclip for symptomatic HF despite GDMT