-
Khuram Ameen MDOregon Lung Specialists
-
Critically ill patients frequently require invasive monitoring
and other support that can lead to anxiety, agitation, and pain
Use of sedation is essential for the comfort and safety
More than 50 percent of patients received one or more sedatives
by intravenous infusion.
-
The most common agent was propofol (82 percent), followed by
benzodiazepines (31 percent), and dexmedetomidine (4 percent).
Opiates were commonly combined with benzodiazepines.
Heavy sedation may increase mortality and morbidity has led to a
new model in which the emphasis is on maximizing the comfort of
these patients while they remain interactive, oriented,and able to
follow instruction
-
To determine whether the use of continuous i.v. sedation is
associated with prolongation of the duration of mechanical
ventilation
Prospective observational cohort study The primary outcome
measure was the
duration of mechanical ventilation. Secondary outcome measures
included ICU
and hospital lengths of stay, hospital mortality, and acquired
organ system derangements
-
The duration of mechanical ventilation was significantly longer
for patients receiving continuous i.v. sedation compared with
patients not receiving continuous i.v. sedation (185+/-190 h vs
55.6+/-75.6 h; p
-
Approaches to removal of sedation and mechanical ventilation for
critically ill patients vary widely. Our aim was to assess a
protocol that paired spontaneous awakening trials (SATs)-ie, daily
interruption of sedatives-with spontaneous breathing trials
(SBTs)
336 mechanically ventilated patients were randomized
-
Patients in the intervention group spent more days breathing
without assistance during the 28-day study period than did those in
the control group (14.7 days vs 11.6 days; mean difference 3.1
days)
They were discharged from intensive care (median time in
intensive care 9.1 days vs12.9 days; p=0.01) and the hospital
earlier (median time in the hospital 14.9 days vs 19.2 days;
p=0.04
-
More patients in the intervention group self-extubated than in
the control group (16 patients vs six patients; 6.0% difference,
95% CI 0.6% to 11.8%; p=0.03), but the number of patients who
required reintubation after self-extubation was similar (five
patients vs three patients; 1.2% difference)
-
Our results suggest that a wake up and breathe protocol that
pairs daily spontaneous awakening trials (ie, interruption of
sedatives) with daily spontaneous breathing trials results in
better outcomes for mechanically ventilated patients in intensive
care than current standard approaches and should become routine
practice.
-
Open-label, randomized, prospective, phase IV clinical trial
Patients were randomized to receive midazolamor propofol
sedation was titrated to achieve synchronization with mechanical
ventilation
All patients received 0.5 mg/kg/24 hrs of morphine chloride
When the patient was ready for weaning according to defined
criteria, sedation was interrupted abruptly and the time from
interruption of sedation to the first T-bridge trial and to
extubation was measured
-
Duration of sedation was 141.7 ± 89.4 hrs and 139.7 ± 84.7 hrs,
and cost (US dollars) attributed to sedation was $378 ±342 and
$1,047 ±794 (p =.0001) for the midazolam and propofol groups,
respectively.
In the midazolam group, time from discontinuation of the drug
infusion to extubation was 97.9 ± 54.6, In the propofolgroup, time
from discontinuation of the drug infusion to extubation was 34.8
±29.4 hrs
-
Cost per patient in the midazolam group (including ICU therapy
and sedation with midazolam) was $10,828 ± 5,734. Cost per patient
in the propofol group was $9,466 ±5,820, $1,362 less than in the
midazolam group.
-
To compare the effectiveness, characteristics, duration of
action, hemodynamic and biochemical effects, and side effects of
propofol and midazolam used for continuous intravenous sedation of
ventilated critically ill patients
Multicenter, prospective, randomized, nonblinded study.
Supported, in part, by a grant from Zeneca Pharmaceuticals
-
Propofol or midazolam was used for induction and maintenance of
continuous intravenous sedation for a maximum of 5 days
The effectiveness of those two regimens was assessed according
to their effects on ventilatory management and the presence of
agitation
-
The mean duration of sedation was 81 ±25 hrs and 88 ± 27 hrs for
the propofol and midazolam groups, respectively
There was no difference regarding the opiate and muscle relaxant
requirements between the two groups.
-
Sedation with propofol was more effective in achieving
patient-ventilator synchrony than that with midazolam after the
first hour of treatment
Patients sedated with propofol awoke more rapidly and with less
variability than those patients sedated with midazolam (23 ± 16
mins vs. 137 ± 185 mins,
-
Prospective,randomized study evaluate the efficacy of continuous
infusions
of lorazepam vs. midazolam for sedation in the intensive care
unit
Patients were randomized to Receive either lorazepam or
midazolam. The infusion rate was adjusted by the nurse to maintain
sedation at Ramsay’s 2 or 3
-
Mean time to return to baseline mental status was 216 minutes
for lorazepam and 815 minutes for midazolam
Average fluid used to infuse the lorazepam was 1.2 liters and
1.3 liters for midazolam
Time to wake up was occasionally delayed for 24 hours
-
Nine open label, randomized trials comparing long term sedation:
Most compared propofol with midazolam
▪ “Propofol consistently provided faster awakening [and
extubation] than midazolam with statistical and probable clinical
significance.”
Midazolam vs. lorazepam▪ Double-blind study of long-term
sedation
▪ No statistical difference in awakening time however, awakening
time with lorazepam was more predictable and cost-effective.
Jacobi J, et al. Clinical practice guidelines for the sustained
use of sedatives and analgesics in the critically ill adult. Crit
Care Med2002; 30(1): 119-142.
-
GABA Receptor agonist medications are the most commonly used
sedatives for intensive care unit (ICU) patients, yet preliminary
evidence indicates that the 2 agonist dexmedetomidine may have
distinct advantages
Prospective, double-blind, randomized trial conducted in 68
centers in 5 countries between March 2005 and August 2007
-
Percentage of time within target RASS range. Prevalence and
duration of delirium, Use of fentanyl and open-label midazolam,
and nursing assessments. Duration of mechanical ventilation,
ICU
length of stay, and adverse events
-
There was no difference in percentage of time within the target
RASS range (77.3% for dexmedetomidine group vs 75.1% for midazolam
group
The prevalence of delirium during treatment was 54% (n =
132/244) in dexmedetomidine-treated patients vs 76.6% (n = 93/122)
in midazolam-treated patients (difference, 22.6%
-
Median time to extubation was 1.9 days shorter in
dexmedetomidine-treated patients
ICU length of stay was similar (5.9 days)
Dexmedetomidine-treated patients were
more likely to develop bradycardia (42.2% [103/244] vs
18.9%),but had a lower likelihoodof tachycardia (25.4% vs 44.3%) or
hypertension requiring treatment (18.9% vs 29.5%)
-
many questions remain unanswered. Because benzodiazepines have
shown the greatest association with delirium, and guidelines
recommend midazolam only for short-term use due to “unpredictable
awakening and time to extubation” with longer use, it is perhaps
not surprising that infusion of midazolam for multiple days
resulted in longer time to extubation
-
It remains unclear whether dexmedetomidinewould produce the same
decrease in delirium and improvement in time to extubation if it
were compared with another medication such as propofol
Whether benzodiazepines given as bolus rather than infusion may
have reduced delirium and length of mechanical ventilation in the
midazolam group also remains an important question
-
Delirium is defined as an acute change or fluctuation in mental
status plus inattention, and either disorganized thinking or an
altered level of consciousness at the time of the evaluation
Several studies have now confirmed that delirium occurs in 60%
to 80% of mechanically ventilated patients
-
Increased incidence in ventilated patients
Incidence in critically ill patients range from 35-60%.
Up to 81.7% of mechanically ventilated pts developed delirium at
some point during Vanderbilt study.
Underdiagnosed condition
Delirium goes undiagnosed in >66% of patients
- Ely EW et al. Delirium as a predictor of mortality in
mechanically ventilated patients in the ICU. JAMA 2004; 291:
1753-62- Ely EW et al. The impact of delirium in the intensive care
unit on hospital length of stay. Intensive Care Med 2001; 27:
1892-1900- Inouye SK et al. Nurses’ recognition of delirium and its
symptoms. Arch Intern Med. 2001; 161: 2467-2473.
-
Eli EW et al. Delirium as a predictor of mortality in
mechanically ventilated patients in the ICU. JAMA 2004; 291:
1753-62Milbrandt EB et al. Costs Associated with Delirium in
Mechanically Ventilated Patients. Crit Care Med 2004; 32: 955-962,
2004
Independent predictor of mortality (3-fold increase) and
increased length of stay in ventilated pts.
After adjusting for confounders, delirium was also associated
with a 39% increase in ICU costs.
-
Term ICU psychosis is “old-fashioned, inaccurate and not
appropriate”
-
Hyperactive - paranoid, agitated
Readily recognized, best prognosis
Purely hyperactive: 1.6% of delirium episodes
Hypoactive - withdrawn, quiet, paranoid
“Quiet delirium”
Often not well recognized, misdiagnosed
Purely hypoactive episodes 43.5%
Mixed - combination
Most common in ICU patients 54.9%
Worst prognosis
Peterson JF, et al. Delirium and Its Motoric Subtypes: A Study
of 614 Critically Ill Patients. J Am Geriatr Soc 54: 479-484,
2006.
-
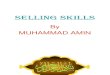
Richmond Agitation Sedation Scale (RASS)
Evidence of acute change from baseline?Fluctuating RASS, GCS or
other assessment?
Attention Screening Exam: Auditory or Visual
Questions: Will a stone float on water?Are there fish in the
sea?Does one pound weight more than two pounds?Can you use a hammer
to pound on a nail?
Confusion Assessment Method for ICU (CAM)
-
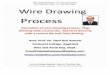
Richmond Agitation Sedation Scale (RASS)
-
Neurobiology of attention Cortical vs subcortical mechanisms
Neurotransmitter mechanisms
Acetylcholine plays a key role in pathogenesis
▪ Anticholinergic drugs caused delirium in healthy volunteers,
reserved by cholinesterase inhibitors
▪ Serum anticholinergic activity correlated with severity of
delirium
Mach, JR, Dysken, MW, Kuskowski, M, et al. Serum anticholinergic
activity in hospitalized older persons with delirium: A preliminary
study. J Am Geriatr Soc 1995; 43:491.
-
Haloperidol is agent of choice*
▪ Best antipsychotic, few anticholinergic side-effects▪ Unlikely
to cause sedation and hypotension
▪ Typical starting dose: 1-2 mg IV every 2-4 hours▪ Adjust for
elderly and degree of agitation
▪ Can double dose every 20-30 minutes if uncontrolled -->
continuous drip 5-10 mg/hr
▪ QT prolongation▪ Cardiac monitoring at higher doses, measure
K+ and Mg2+
▪ Discontinue if QTc>450ms or extrapyramidal symptoms
develop
American Psychiatric Association. Practice Guidelines for
Treatment of Patients with Delirium. 1999.UK Clinical Pharmacy
Association. Detection, Prevention and Treatment of Delirium in
Critically Ill Patients. June 2006.
-
Role for benzodiazepines
Specifically indicated for EtOH or BZD withdrawal delirium
If possible, avoid use
▪ Contribute to development of delirium
▪ Ineffective in treating delirium
In ventilated patients, sedation with benzodiazepines is often
necessary
-
No published data in critical care literature Antipsychotics may
still play a role
Treat like hyperactive delirium
Stimulants such as methylphenidate may be used
American Psychiatric Association. Practice Guidelines for
Treatment of Patients with Delirium. 1999.UK Clinical Pharmacy
Association. Detection, Prevention and Treatment of Delirium in
Critically Ill Patients. June 2006.