Embed Size (px)
Citation preview
Jerold Chun, M.D., Ph.D. (Sanford Burnham Prebys) and
Eric Gershwin, M.D. (UC Davis Health) to Present
January 29, 2018
NON-CONFIDENTIAL
Key Opinion Leader Event: S1P Modulation and Etrasimod - The Next High
Potential Class of Autoimmune Therapies
2
Forward-Looking Statements
This presentation includes forward-looking statements that involve a number of risks and uncertainties, including
statements about our investigative stage drug candidates, including with respect to their potential (including to become
first or best-in-class), preclinical data, safety, efficacy, applications, indications, significance of data, commercialization,
expected data readouts, initiation of new clinical trials, and comparisons to other compounds; our focus, goals, strategy,
plans, timelines and guidance; drug targets, including with respect to potential therapeutic utility; our partnered
programs; financial and other guidance; and other statements that are not historical facts, including statements that may
refer to development plans, differentiation, the market and unmet needs, and statements that may include words such as
“may,” “might,” “will,” “intend,” “plan,” “expect,” “potential,” “possible,” “promise,” “goal” or other similar words. For
such statements, we claim the protection of the Private Securities Litigation Reform Act of 1995. Actual events or results
may differ materially from expectations, and you are cautioned not to place undue reliance on these forward-looking
statements, which speak only as of the time they were made. Factors that could cause actual results to differ materially
from such statements include, without limitation: the timing and outcome of research, development and regulatory review
is uncertain; results of clinical trials and nonclinical studies are subject to different interpretations and may not be
predictive of future results; clinical and nonclinical data is voluminous and detailed, and regulatory agencies may interpret
or weigh the importance of data differently and reach different conclusions than Arena or others, request additional
information, have additional recommendations or change their guidance or requirements; unexpected or unfavorable new
data; our drug candidates may not advance in development or be approved for marketing; clinical trials and other studies
may not proceed at the time or in the manner expected or at all; data and information related to our programs may not
meet regulatory requirements or otherwise be sufficient for further development, regulatory review, partnering or
approval; top-line data may not accurately reflect the complete results of a particular study or trial; analyzing or
comparing data from different clinical trials or nonclinical studies is unreliable and may not result in accurate conclusions
or predictions; other risks related to developing, seeking regulatory approval of and commercializing drugs, including
regulatory, manufacturing, supply and marketing issues and drug availability; we expect to need additional funds to
advance all of our programs, and you and others may not agree with the manner in which we allocate our resources;
Arena's and third parties' intellectual property rights; competition; reimbursement and pricing decisions; risks related to
relying on partners and other third parties; and satisfactory resolution of litigation or other disagreements. Additional
factors that could cause actual results to differ materially from those stated or implied by our forward-looking statements
are disclosed in our SEC filings, including under the heading “Risk Factors” in our Quarterly Report on Form 10-Q for the
quarter ended September 30, 2017. We disclaim any intent or obligation to update these forward-looking statements,
other than as may be required under applicable law.
3
Agenda
Amit Munshi, Director, President and CEO, Arena
• Welcome and Company Overview
Dr. Jerold Chun• Sphingosine 1-Phosphate (S1P) Receptors: Validated Drug Targets
Dr. Eric Gershwin• The Broad Potential of S1P Receptor Modulators for the Treatment of Autoimmune
Diseases
Dr. Preston Klassen, EVP, Research & Development and CMO, Arena
• The Promise of Etrasimod: A Potentially Best-in-Class Oral, Next Generation, S1P Receptor Modulator Being Evaluated for Multiple Autoimmune Diseases
Q&A
4
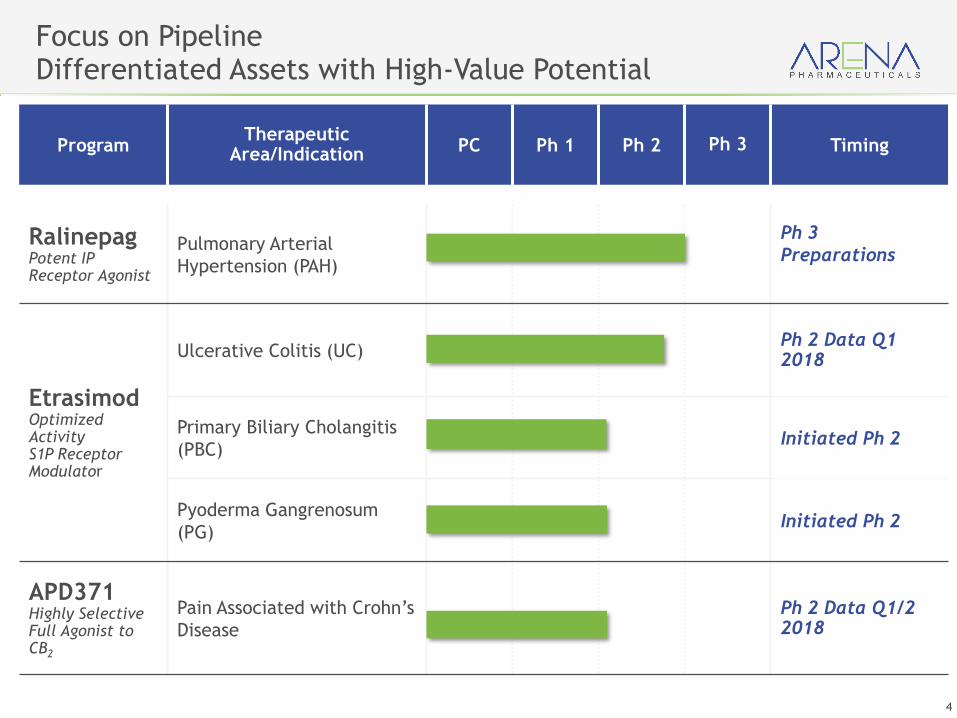
ProgramTherapeutic
Area/IndicationPC Ph 1 Ph 2 Ph 3 Timing
RalinepagPotent IP Receptor Agonist
Pulmonary Arterial
Hypertension (PAH)
Ph 3
Preparations
EtrasimodOptimizedActivityS1P Receptor Modulator
Ulcerative Colitis (UC)Ph 2 Data Q1 2018
Primary Biliary Cholangitis
(PBC)Initiated Ph 2
Pyoderma Gangrenosum
(PG)Initiated Ph 2
APD371Highly Selective Full Agonist to CB2
Pain Associated with Crohn’s
Disease
Ph 2 Data Q1/2 2018
Focus on Pipeline Differentiated Assets with High-Value Potential
5
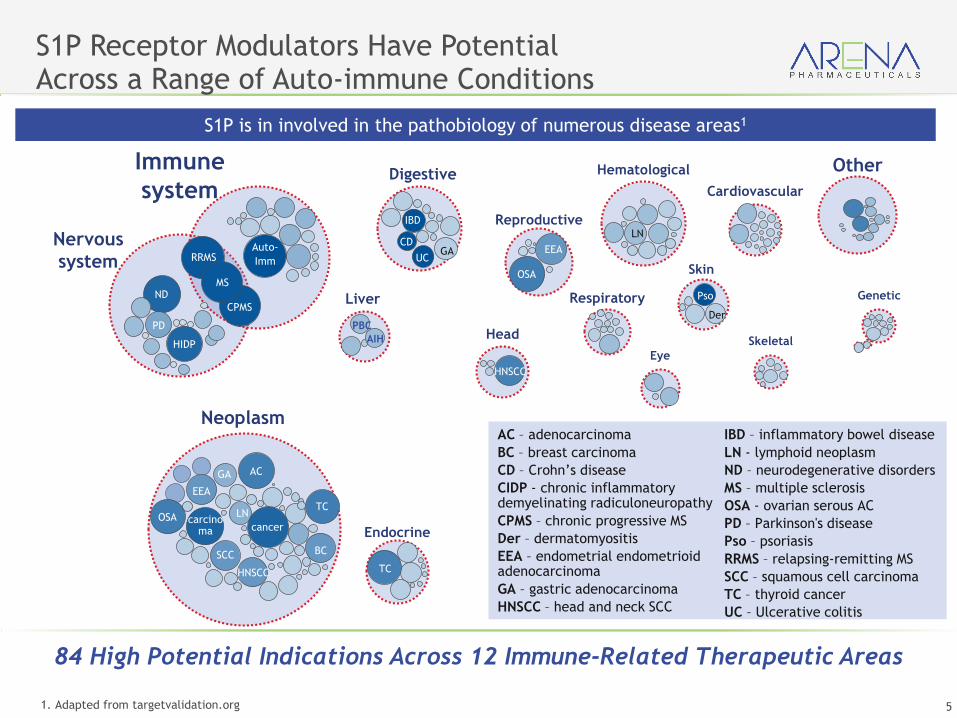
S1P Receptor Modulators Have Potential Across a Range of Auto-immune Conditions
1. Adapted from targetvalidation.org
S1P is in involved in the pathobiology of numerous disease areas1
84 High Potential Indications Across 12 Immune-Related Therapeutic Areas
Neoplasm
Nervous
system
Immune
systemOther
Endocrine
Reproductive
Digestive
Head
Hematological
Liver
Cardiovascular
Skin
GeneticRespiratory
Eye
Skeletal
ND
HIDP
PD
Auto-
Imm
TC
OSA
EEA
LN
Pso
Der
IBD
CDGA
HNSCC
OSA
EEA
AC
cancercarcino
ma
GA
LNTC
BC
HNSCC
SCC
AC – adenocarcinoma
BC – breast carcinoma
CD – Crohn’s disease
CIDP - chronic inflammatory demyelinating radiculoneuropathy
CPMS – chronic progressive MS
Der – dermatomyositis
EEA – endometrial endometrioidadenocarcinoma
GA – gastric adenocarcinoma
HNSCC – head and neck SCC
IBD – inflammatory bowel disease
LN - lymphoid neoplasm
ND – neurodegenerative disorders
MS – multiple sclerosis
OSA - ovarian serous AC
PD – Parkinson's disease
Pso – psoriasis
RRMS – relapsing-remitting MS
SCC – squamous cell carcinoma
TC – thyroid cancer
UC – Ulcerative colitis
UC
PBC
AIH
CPMS
RRMS
MS
6
Jerold Chun, M.D., Ph.D.Professor & Senior Vice President
Sanford Burnham Prebys (SBP) Medical Discovery Institute
La Jolla, California [email protected]
Sphingosine 1-Phosphate (S1P)
Receptors: Validated Drug Targets
Disclosures
Dr. Chun has received honoraria, consulting fees,and/or grant support from:
Abbott, Amira, Arena Pharmaceuticals, Biogen-IDEC,BiolineRX, Celgene, GlaxoSmithKline, InceptionSciences, Johnson and Johnson, Merck, MitsubishiTanabe, Novartis, Ono, Pfizer, Skai Ventures, and Taisho
7
Sphingosine 1-phosphate (S1P) is a phospholipid and sphingolipid
▪Sphingolipids (sphingomyelin) were first discovered in brain extracts by Johann Ludwig Wilhelm Thudichum in 1874
▪Named for their enigmatic “Sphinx-like” nature
▪Sphingosine 1-phosphate (S1P) is a naturally occurring bioactive phospho- & sphingolipid
8
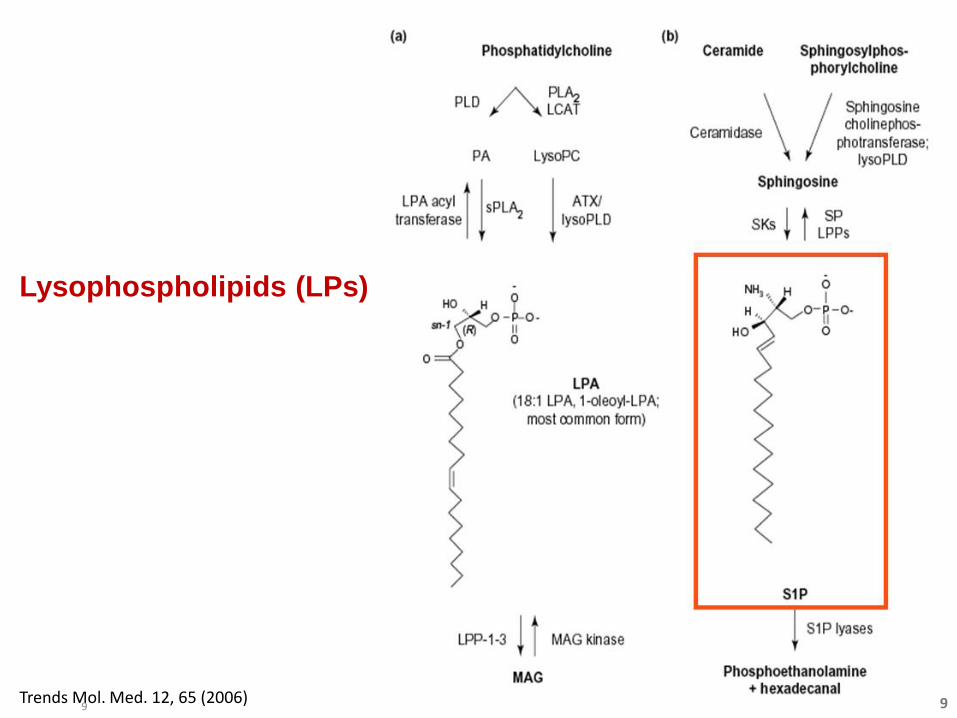
Trends Mol. Med. 12, 65 (2006)
Lysophospholipids (LPs)
9 9
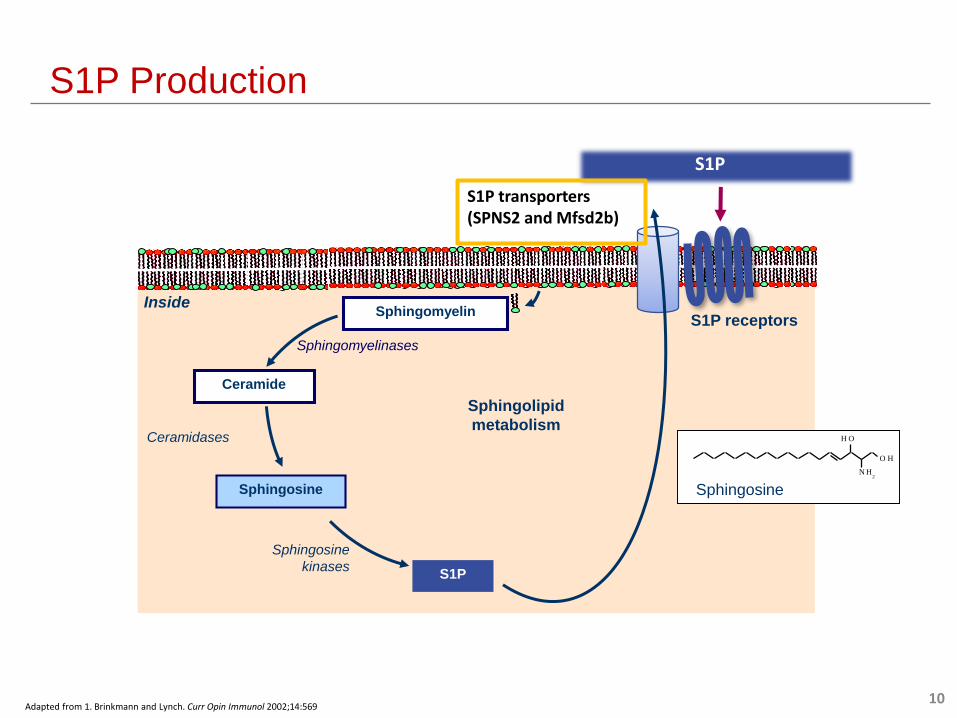
S1P Production
Sphingolipid
metabolism
Ceramide
Sphingosine
S1P
Ceramidases
Sphingosine
kinases
Sphingomyelinases
S1P receptors
OH
N H2
O H
Sphingosine
Inside
S1P
Sphingomyelin
Adapted from 1. Brinkmann and Lynch. Curr Opin Immunol 2002;14:569
S1P transporters (SPNS2 and Mfsd2b)
10
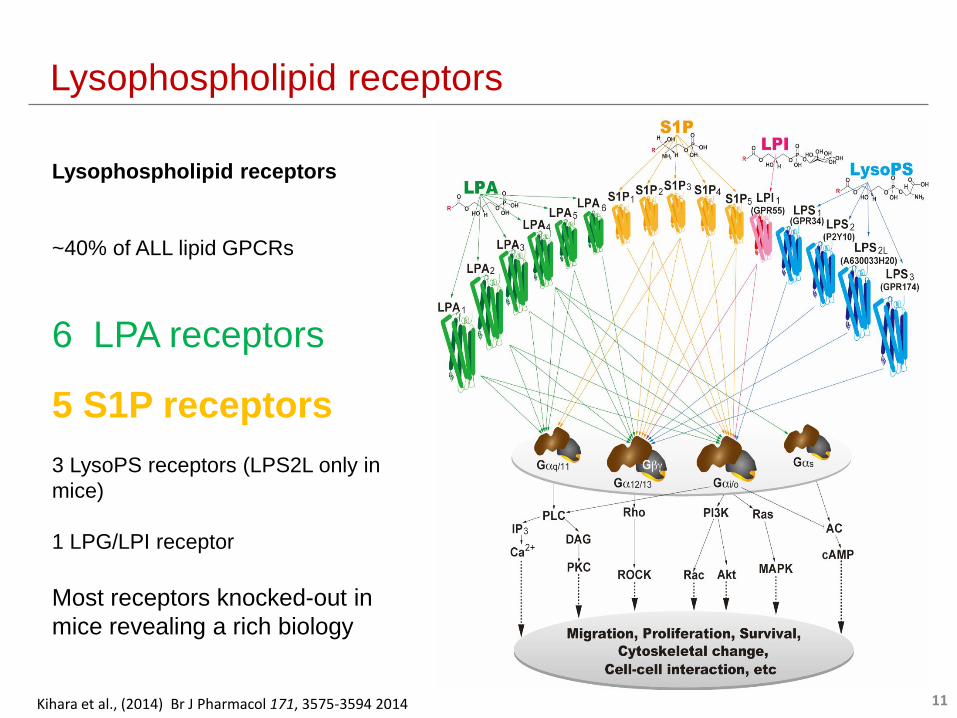
Lysophospholipid receptors
~40% of ALL lipid GPCRs
6 LPA receptors
5 S1P receptors
3 LysoPS receptors (LPS2L only in
mice)
1 LPG/LPI receptor
Most receptors knocked-out in
mice revealing a rich biology
Kihara et al., (2014) Br J Pharmacol 171, 3575-3594 2014
Lysophospholipid receptors
11
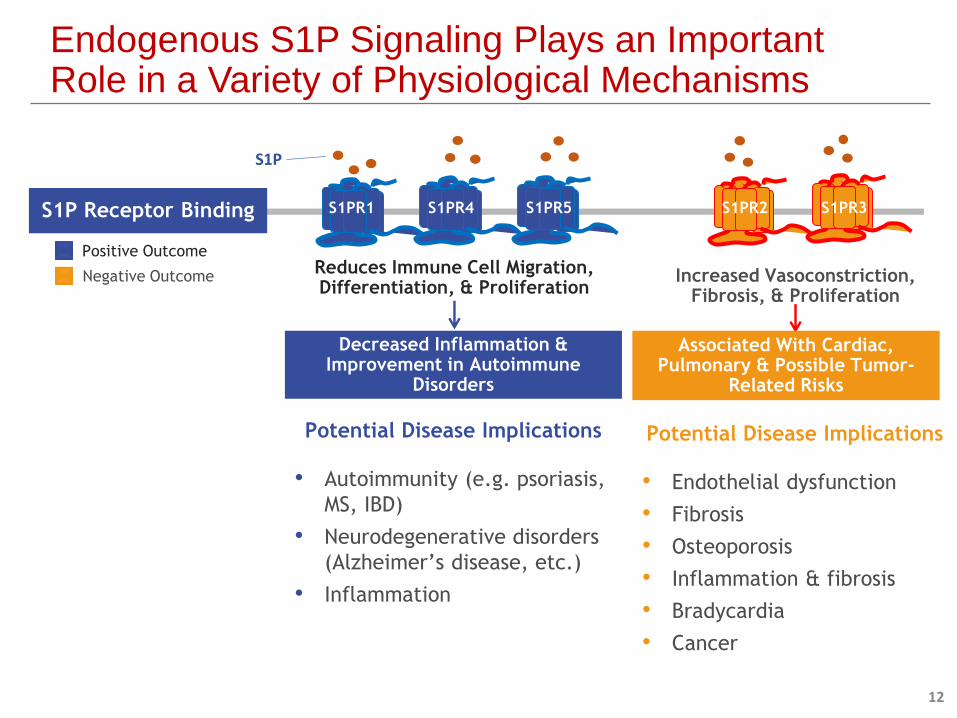
Endogenous S1P Signaling Plays an Important Role in a Variety of Physiological Mechanisms
Decreased Inflammation & Improvement in Autoimmune
Disorders
Positive Outcome
Negative OutcomeReduces Immune Cell Migration,Differentiation, & Proliferation
Increased Vasoconstriction, Fibrosis, & Proliferation
S1PR2 S1PR3S1P Receptor Binding S1PR1 S1PR4 S1PR5
Associated With Cardiac, Pulmonary & Possible Tumor-
Related Risks
Potential Disease Implications
• Autoimmunity (e.g. psoriasis,
MS, IBD)
• Neurodegenerative disorders
(Alzheimer’s disease, etc.)
• Inflammation
Potential Disease Implications
• Endothelial dysfunction
• Fibrosis
• Osteoporosis
• Inflammation & fibrosis
• Bradycardia
• Cancer
S1P
12
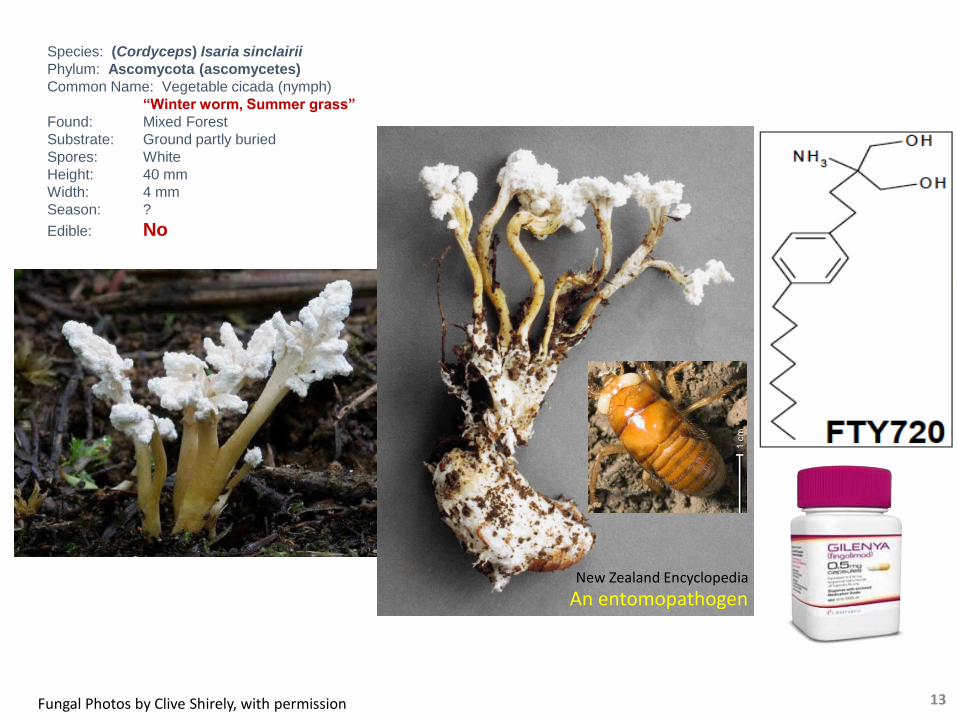
Species: (Cordyceps) Isaria sinclairii
Phylum: Ascomycota (ascomycetes)
Common Name: Vegetable cicada (nymph)
“Winter worm, Summer grass”
Found: Mixed Forest
Substrate: Ground partly buried
Spores: White
Height: 40 mm
Width: 4 mm
Season: ?
Edible: No
Fungal Photos by Clive Shirely, with permission
New Zealand Encyclopedia
An entomopathogen
13
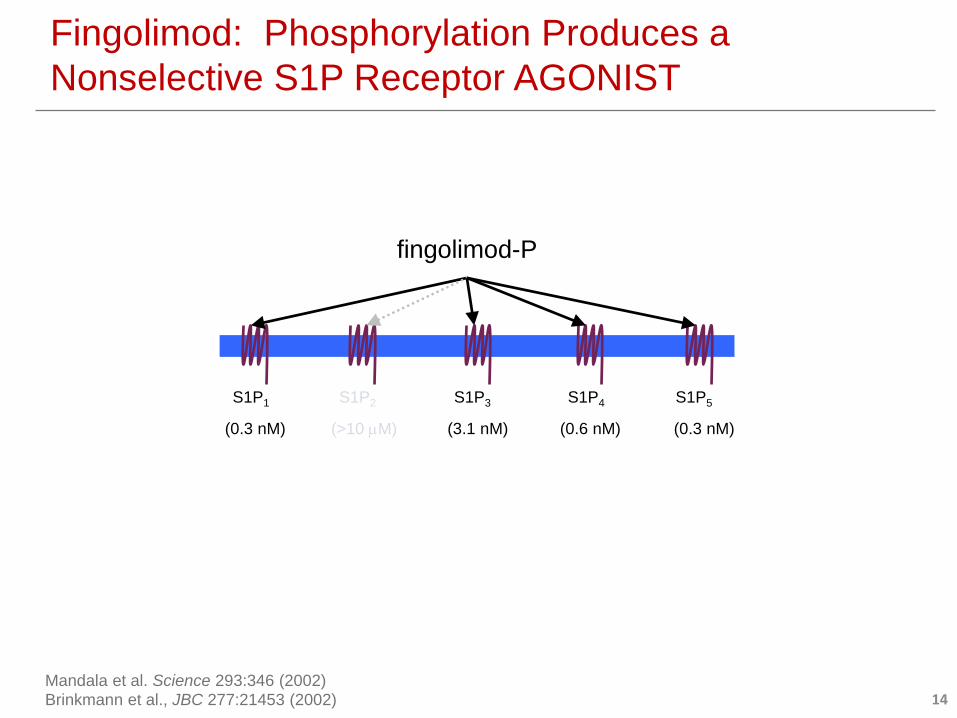
Fingolimod: Phosphorylation Produces a
Nonselective S1P Receptor AGONIST
fingolimod-P
S1P1 S1P2 S1P3 S1P4 S1P5
(0.3 nM) (3.1 nM) (0.6 nM) (0.3 nM)(>10 M)
Mandala et al. Science 293:346 (2002)
Brinkmann et al., JBC 277:21453 (2002) 14
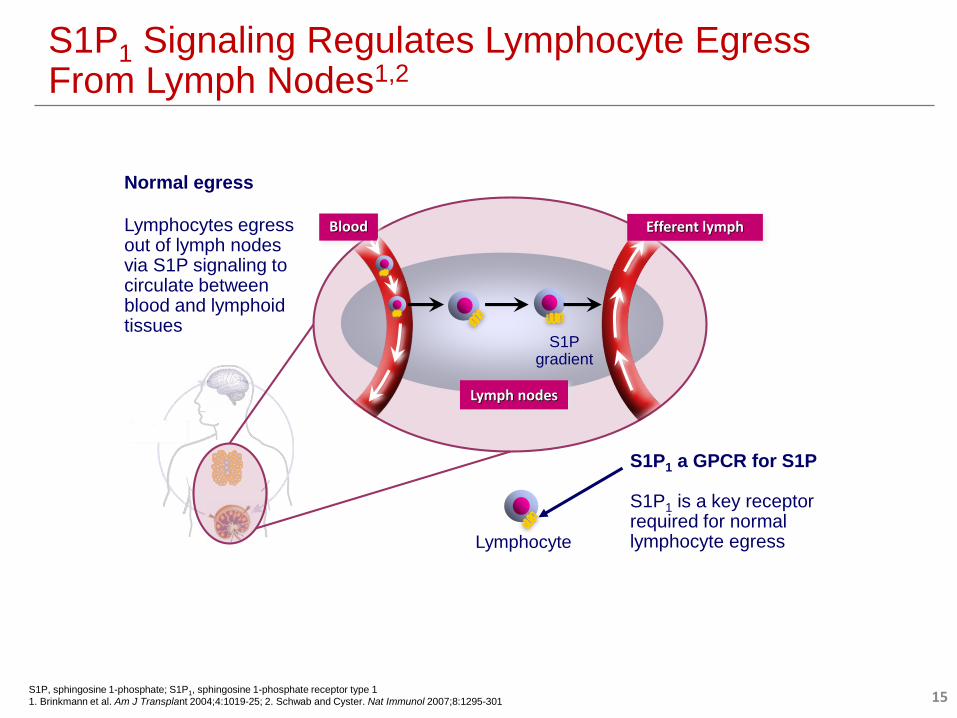
S1P1 Signaling Regulates Lymphocyte Egress From Lymph Nodes1,2
Blood Efferent lymph
Lymph nodes
S1P1 a GPCR for S1P
S1P1 is a key receptor required for normal lymphocyte egressLymphocyte
S1Pgradient
Normal egress
Lymphocytes egress out of lymph nodes via S1P signaling to circulate between blood and lymphoid tissues
S1P, sphingosine 1-phosphate; S1P1, sphingosine 1-phosphate receptor type 1
1. Brinkmann et al. Am J Transplant 2004;4:1019-25; 2. Schwab and Cyster. Nat Immunol 2007;8:1295-301 15

S1P1 Modulation Selectively Reduces Migration of Lymphocytes From Lymph Nodes
1. Peyrin-Biroulet L, et al. Automimmune Rev. 2017;16:495-503; 2.Olivera P, et al. Gut. 2017;66(2):199-209.
T cells exit lymph nodes
via systemic circulation
T cells move from lymph nodes to
organs/tissues, where they release
cytokines, causing inflammation &
damage
Autoimmune Disease 1
Circulating
T-Lymphocytes
Inflammatory
Cytokines
Target Cell
IFNg
IL23
TNF
IL2
T Cells
Lymph Node
S1P1
S1P Gradient
S1P
S1P Modulator
• Functionally antagonizes S1P1
induces receptor internalization and
degradation disrupting normal lymphocyte
subset egress
• Decrease release of inflammatory cytokines
and reduce organ/tissue damage
• Maintain immune surveillance
Treatment with S1P Receptor Modulator2
Potential Autoimmune Diseases that Might
be Treated with Sphingosine 1-Phosphate
Receptor Modulators
Eric Gershwin, M.D. Distinguished Professor of Medicine, the Jack and Donald
Chia Professor of Medicine, Chief of the Division of Allergy
and Clinical Immunology at the University of California School
of Medicine in Davis
Dr. Gershwin is a consultant to Arena Pharmaceuticals, Bayer, Genentech and Eli Lilly
Disclosures
18
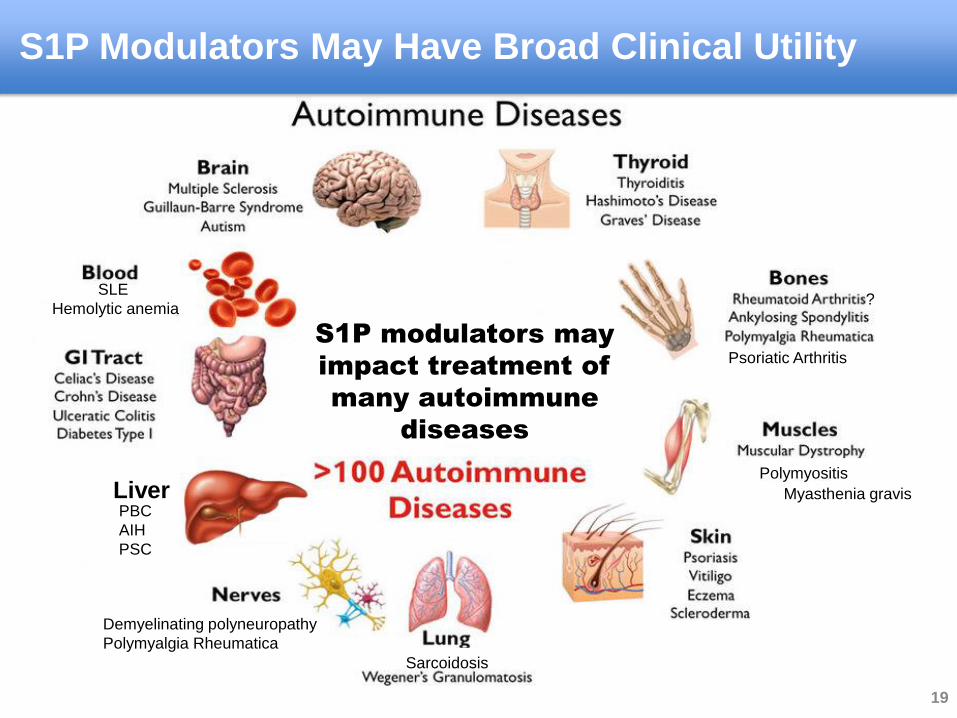
LiverPBC
AIH
PSC
Myasthenia gravis
SLE
Hemolytic anemia
Demyelinating polyneuropathy
Polymyalgia Rheumatica
S1P modulators may
impact treatment of
many autoimmune
diseases
Polymyositis
Sarcoidosis
Psoriatic Arthritis
S1P Modulators May Have Broad Clinical Utility
?
19
A T-cell mediated disease
Pathology is reversible (versus permanent damage)
T cell, Nk cell, T regs and DC contribute to pathology (nearly all AD)
AD with bad treatment options ( i.e. long term steroid use)
The Ideal Target Autoimmune Disease (AD) for S1P
Modulators
20
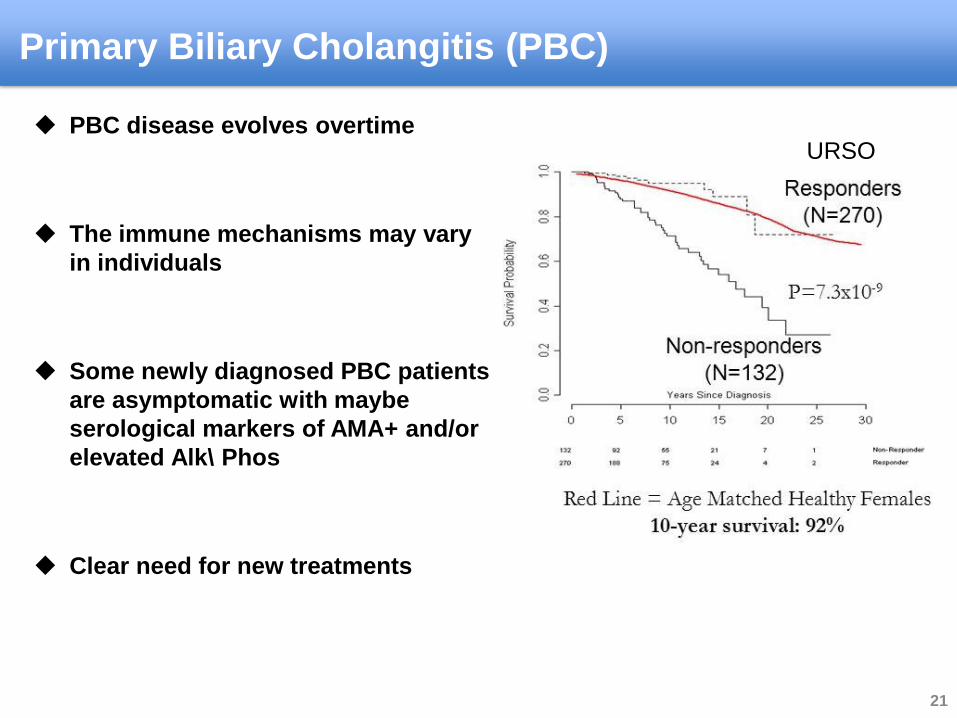
PBC disease evolves overtime
The immune mechanisms may vary
in individuals
Some newly diagnosed PBC patients
are asymptomatic with maybe
serological markers of AMA+ and/or
elevated Alk\ Phos
Clear need for new treatments
Primary Biliary Cholangitis (PBC)
URSO
21
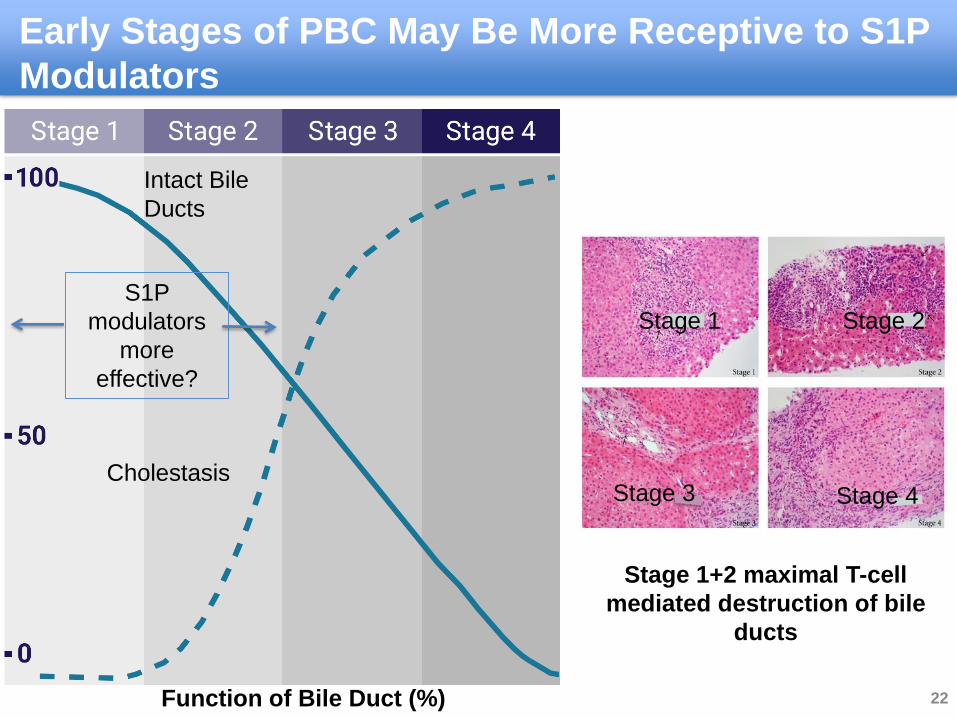
Intact Bile
Ducts
Cholestasis
Function of Bile Duct (%)
Early Stages of PBC May Be More Receptive to S1P
Modulators
Stage 1+2 maximal T-cell
mediated destruction of bile
ducts
Stage 1 Stage 2
Stage 4Stage 3
S1P
modulators
more
effective?
22
Arrest the progression the disease
Bring about normal Liver Function Test (LFT)
Reduce pruritus and fatigue
Doesn’t add new side effects or risks
Oral delivery
The Ideal Therapeutic?
23
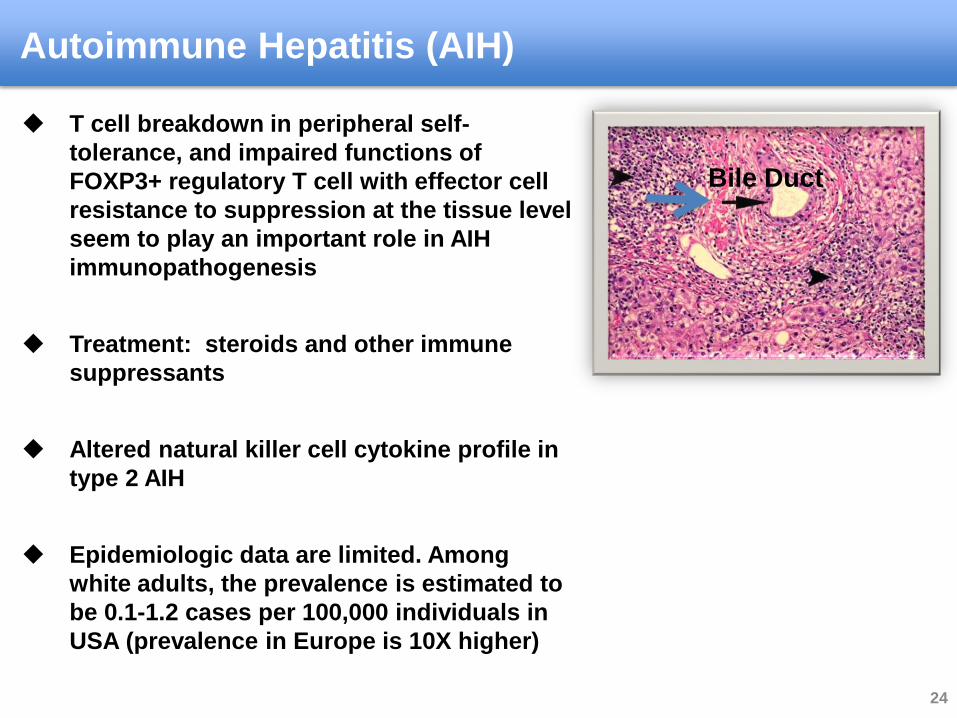
Autoimmune Hepatitis (AIH)
Bile Duct
T cell breakdown in peripheral self-
tolerance, and impaired functions of
FOXP3+ regulatory T cell with effector cell
resistance to suppression at the tissue level
seem to play an important role in AIH
immunopathogenesis
Treatment: steroids and other immune
suppressants
Altered natural killer cell cytokine profile in
type 2 AIH
Epidemiologic data are limited. Among
white adults, the prevalence is estimated to
be 0.1-1.2 cases per 100,000 individuals in
USA (prevalence in Europe is 10X higher)
24
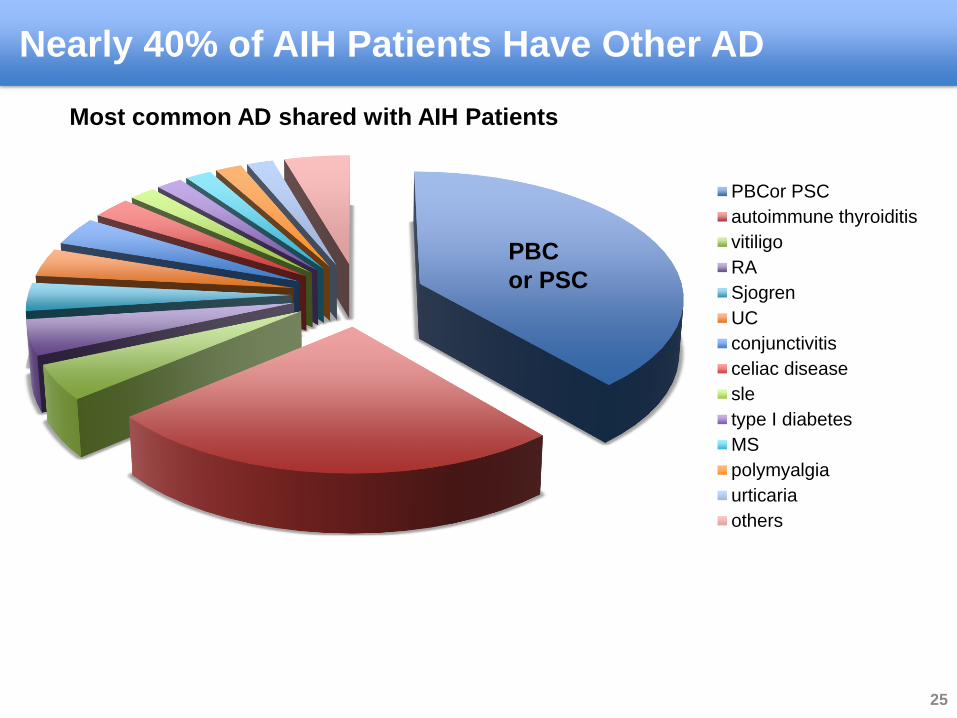
Nearly 40% of AIH Patients Have Other AD
PBCor PSC
autoimmune thyroiditis
vitiligo
RA
Sjogren
UC
conjunctivitis
celiac disease
sle
type I diabetes
MS
polymyalgia
urticaria
others
PBC
or PSC
Most common AD shared with AIH Patients
25
Autoimmune Hepatitis - Treatment Goals
Reduce steroid use - decreasing long term use steroid damage
Increase T regs numbers and improve suppression activity
Reduce T effector cells - less abundant in the liver
Return NK cells to more normal profile
Reduce the number of flares
26
Dermatomyositis
Dermatomyositis includes inflammation,
vasculitis, and perifascicular atrophy. The
predominant inflammatory infiltrate is in the
perimysial region and includes CD4+ T cells
Dermatomyositis affects children and adults
and is the most common inflammatory
myopathy in children
The estimated incidence of dermatomyositis is
9.63 cases per million population - prevalence
between 1/50,000 and 1/10,000
Treatment: dermatomyositis requires the use of
glucocorticoids, topical glucocorticoids, anti-
malarial agents, methotrexate, mycophenolate
mofetil, and/or intravenous immunoglobulin
(IVIg)
27
Polymyositis is a disease caused by
inflammation of the muscles
This occurs when immune cells (clonally
expanded CD8+ T lymphocytes and
macrophages) begin to invade the muscle
tissue
The muscles most severely affected are
typically those closest to the trunk or torso.
This results in weakness that can be severe
The first line treatment for polymyositis is
corticosteroids
The estimated annual incidence has been
reported to be between 1/250,000 and
1/130,000 new cases/year and prevalence
1/14,000
Polymyositis
Polymyositis, like
dermatomyositis, strikes
females with greater
frequency than males
28
Sarcoidosis
Granulomatous inflammation develops
under the regulatory influence of cytokines
produced by local mononuclear
phagocytes, T cells, dendritic cells, and
fibroblasts
Incidence 11 cases per 100,000, prevalence
48/100,000
Blood dendritic cells subsets may migrate
into the affected tissues, contributing to
the formation of the granulomas in
sarcoidosis. It is hypothesized that the
migrating DCs may regulate the T cell
response in sarcoidosis, at least in the
granulomatous lesions
29
Conclusion
S1P modulators biochemical profile makes it well suited to treat many
autoimmune diseases
Over 100 potential T cell mediated autoimmune conditions
Next generation compounds with more favorable risk/benefit profile may
have broader utility across conditions
Additional investigation is needed to explore these compounds in a broad
range of diseases
30
Oral, Next Generation, S1P Receptor Modulator
Optimized Activity Being Evaluated for Multiple
Autoimmune Diseases
Etrasimod
32
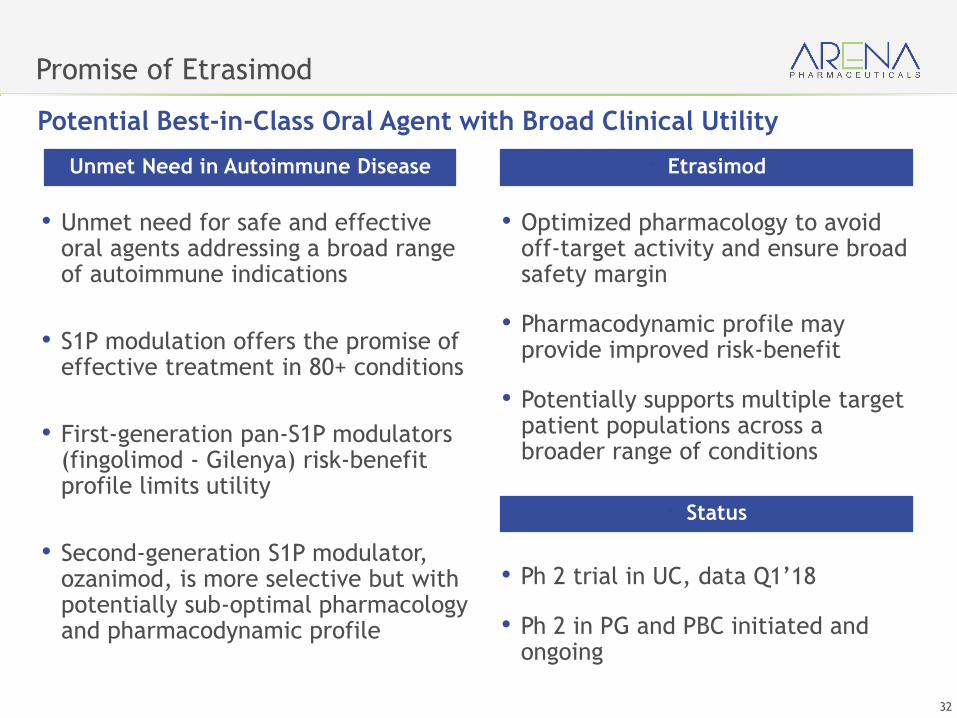
Promise of Etrasimod
• Unmet need for safe and effective oral agents addressing a broad range of autoimmune indications
• S1P modulation offers the promise of effective treatment in 80+ conditions
• First-generation pan-S1P modulators (fingolimod - Gilenya) risk-benefit profile limits utility
• Second-generation S1P modulator, ozanimod, is more selective but with potentially sub-optimal pharmacology and pharmacodynamic profile
Unmet Need in Autoimmune Disease
• Optimized pharmacology to avoid off-target activity and ensure broad safety margin
• Pharmacodynamic profile may provide improved risk-benefit
• Potentially supports multiple target patient populations across a broader range of conditions
• Etrasimod
• Ph 2 trial in UC, data Q1’18
• Ph 2 in PG and PBC initiated and ongoing
• Status
Potential Best-in-Class Oral Agent with Broad Clinical Utility
33
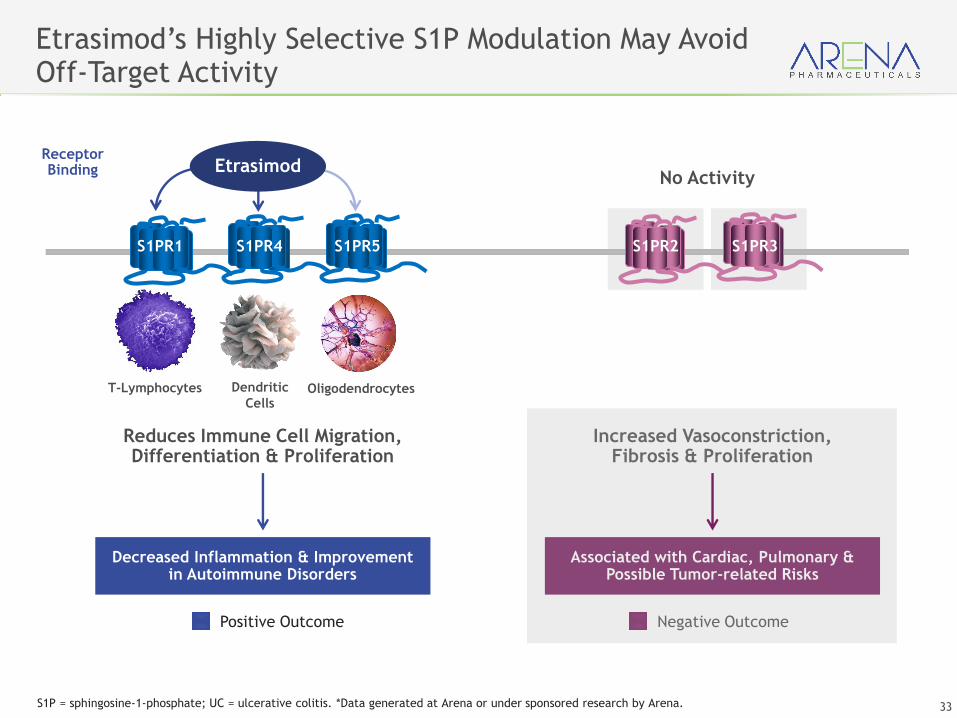
Associated with Cardiac, Pulmonary & Possible Tumor-related Risks
Decreased Inflammation & Improvement in Autoimmune Disorders
Positive Outcome Negative Outcome
Dendritic
Cells
Reduces Immune Cell Migration,Differentiation & Proliferation
Increased Vasoconstriction, Fibrosis & Proliferation
T-Lymphocytes Oligodendrocytes
S1PR2 S1PR3
Etrasimod’s Highly Selective S1P Modulation May Avoid Off-Target Activity
No Activity
Receptor Binding
S1PR1 S1PR4 S1PR5
Etrasimod
S1P = sphingosine-1-phosphate; UC = ulcerative colitis. *Data generated at Arena or under sponsored research by Arena.
34
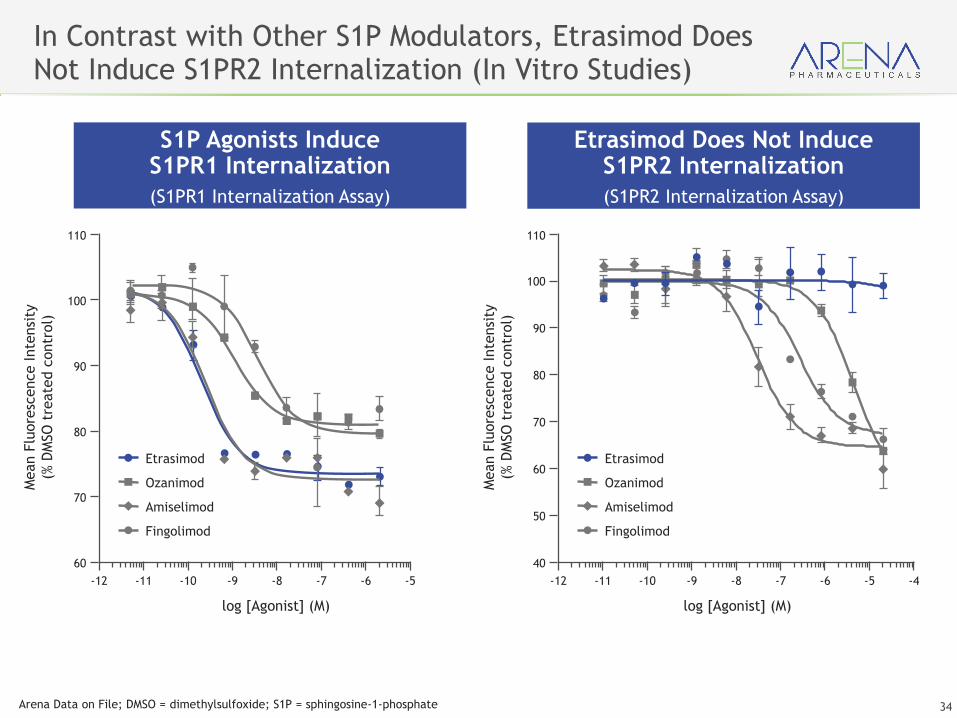
In Contrast with Other S1P Modulators, Etrasimod Does Not Induce S1PR2 Internalization (In Vitro Studies)
S1P Agonists Induce S1PR1 Internalization
(S1PR1 Internalization Assay)
Etrasimod Does Not Induce S1PR2 Internalization
(S1PR2 Internalization Assay)
-12 -11 -10 -9 -8 -7 -6 -5
log [Agonist] (M)
Mean F
luore
scence Inte
nsi
ty
(% D
MSO
tre
ate
d c
ontr
ol)
60
80
90
100
110
70
Etrasimod
Fingolimod
Ozanimod
Amiselimod
-12 -11 -10 -9 -8 -7 -6 -5 -4
log [Agonist] (M)
Mean F
luore
scence Inte
nsi
ty
(% D
MSO
tre
ate
d c
ontr
ol)
40
80
90
100
110
50
60
70
Etrasimod
Fingolimod
Ozanimod
Amiselimod
Arena Data on File; DMSO = dimethylsulfoxide; S1P = sphingosine-1-phosphate
35
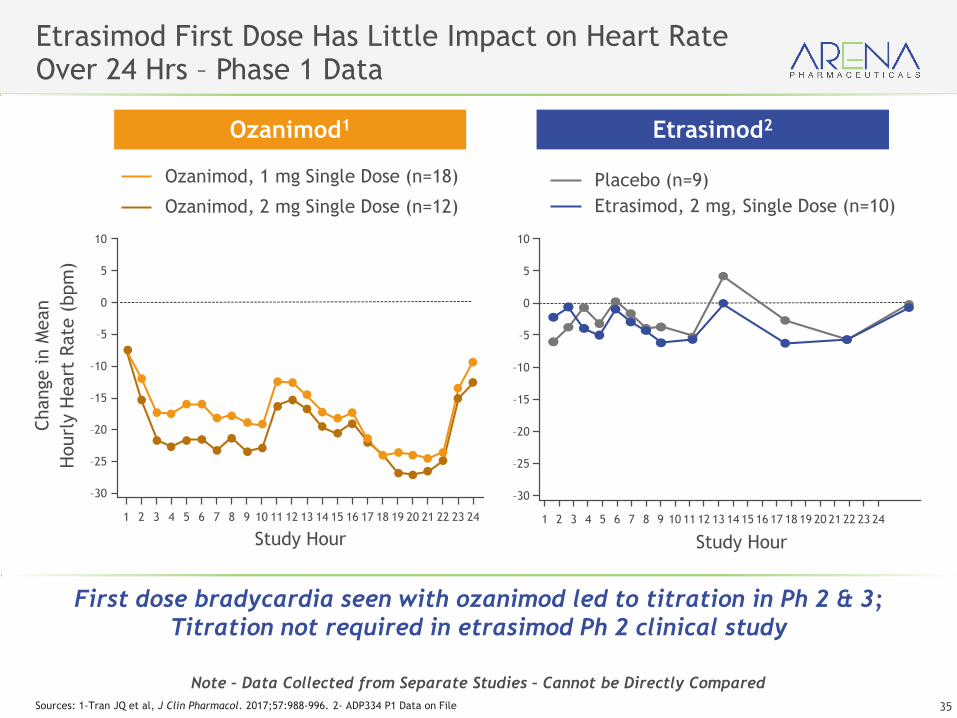
Etrasimod First Dose Has Little Impact on Heart Rate Over 24 Hrs – Phase 1 Data
Ozanimod, 1 mg Single Dose (n=18)
Ozanimod, 2 mg Single Dose (n=12)
Placebo (n=9)
Etrasimod, 2 mg, Single Dose (n=10)
Ozanimod1 Etrasimod2
Note – Data Collected from Separate Studies – Cannot be Directly Compared
Sources: 1-Tran JQ et al, J Clin Pharmacol. 2017;57:988-996. 2- ADP334 P1 Data on File
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
10
0
–10
–20
–30
5
–5
–15
–25
Study Hour
Change in M
ean
Hourl
y H
eart
Rate
(bpm
)
10
0
–10
–20
–30
5
–5
–15
–25
Study Hour
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
First dose bradycardia seen with ozanimod led to titration in Ph 2 & 3;
Titration not required in etrasimod Ph 2 clinical study
36
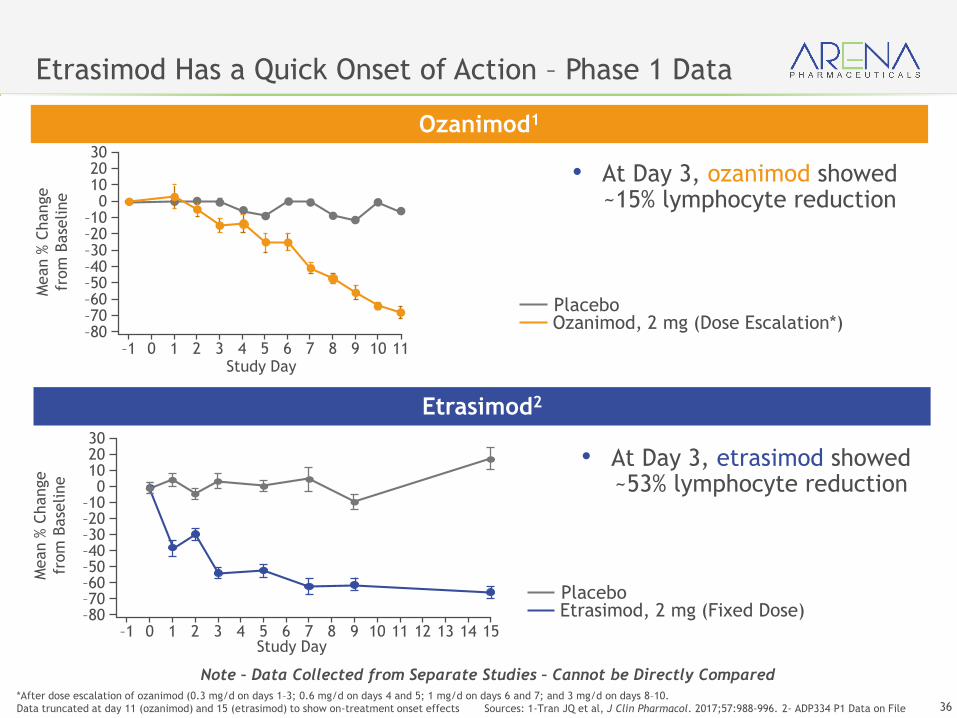
Etrasimod Has a Quick Onset of Action – Phase 1 Data
*After dose escalation of ozanimod (0.3 mg/d on days 1–3; 0.6 mg/d on days 4 and 5; 1 mg/d on days 6 and 7; and 3 mg/d on days 8–10.
Data truncated at day 11 (ozanimod) and 15 (etrasimod) to show on-treatment onset effects Sources: 1-Tran JQ et al, J Clin Pharmacol. 2017;57:988-996. 2- ADP334 P1 Data on File
Note – Data Collected from Separate Studies – Cannot be Directly Compared
Ozanimod1
Etrasimod2
Ozanimod, 2 mg (Dose Escalation*) Placebo
Mean %
Change
from
Base
line
3020100
–10–20–30–40–50–60–70–80
–1 0 1 2 3 4 5 6 7 8 9 10 11Study Day
Study Day
3020100
–10–20–30–40–50–60–70–80
–1 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Mean %
Change
from
Base
line
Etrasimod, 2 mg (Fixed Dose) Placebo
• At Day 3, etrasimod showed ~53% lymphocyte reduction
• At Day 3, ozanimod showed ~15% lymphocyte reduction
37
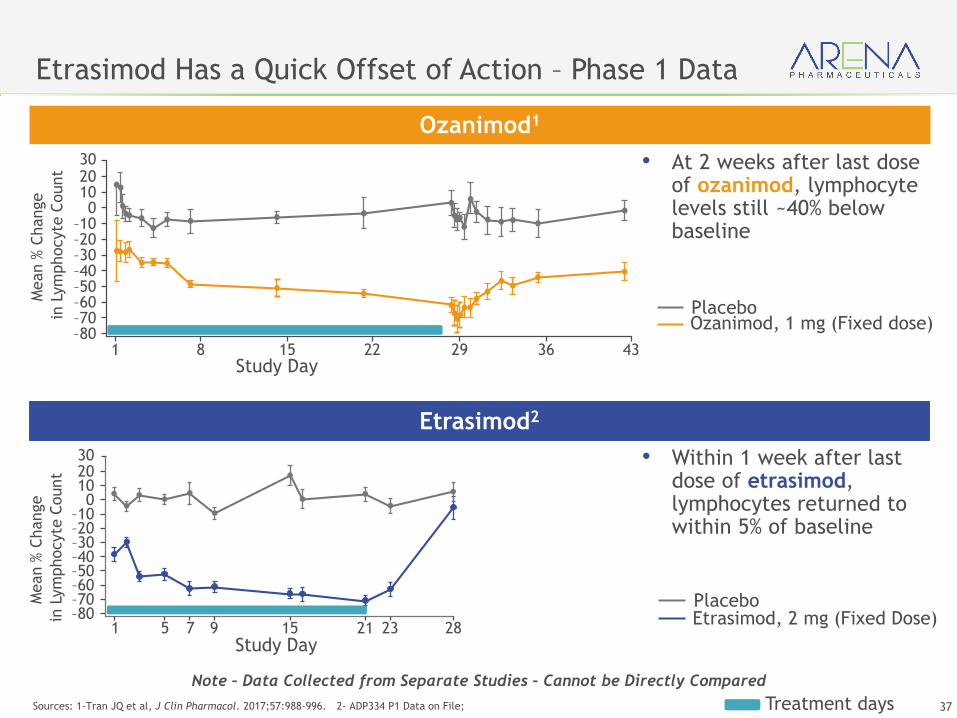
Etrasimod Has a Quick Offset of Action – Phase 1 Data
Sources: 1-Tran JQ et al, J Clin Pharmacol. 2017;57:988-996. 2- ADP334 P1 Data on File;
Ozanimod1
Etrasimod2
Ozanimod, 1 mg (Fixed dose) Placebo
Etrasimod, 2 mg (Fixed Dose) Placebo
Treatment days
• Within 1 week after last dose of etrasimod, lymphocytes returned to within 5% of baseline
• At 2 weeks after last dose of ozanimod, lymphocyte levels still ~40% below baseline
Study Day
30
Mean %
Change
in L
ym
phocyte
Count 20
100
–10–20–30–40–50–60–70–80
1 8 15 22 29 36 43
Study Day
30
Mean %
Change
in L
ym
phocyte
Count 20
100
–10–20–30–40–50–60–70–80
1 5 7 9 15 21 23 28
Note – Data Collected from Separate Studies – Cannot be Directly Compared

38
Optimal Selectivity
Opportunity to be
best-in-class therapy
More Selective
S1P2 internalization
Ozanimod2
(Celgene)
Nonselective
Promiscuous binding can lead to off-
target effects4 & more AEs5
a Elevated LFTs ≥ 3 × upper limit of normal. *Note – Data Collected from Separate Studies – Cannot be Directly Compared
MAD, multiple ascending dose; LFT, liver function test; PFTs, pulmonary function tests.
1. Gilenya® Prescribing Information. Novartis Pharmaceuticals, East Hanover, NJ; 2016. 2. Sandborn WJ, et al. N Engl J Med. 2016;374:1754-1762. 3. Data on File, Arena
Pharmaceuticals. 4. Blaho VA, et al. J Lipid Res. 2014;55:1596–1608. 5. Olivera P, et al. Gut. 2017;66(25):199-209. 6.Kappos L, et al. N Engl J Med 2010;362:387-401.
Newer S1P Receptor Modulators Promise Improved Efficacy and Safety
Etrasimod3
(Arena)Fingolimod1
(Novartis)
First-Generation S1P Receptor Modulator
Second-Generation S1P Receptor Modulator
Rapid lymphocyte lowering &
recovery (2 mg/day)
• Phase 1: ~69%
• Phase 2: TBD
Lymphocyte lowering
(Up to 2 mg/day)
• Phase 1: ~65%
• Phase 2: ~49%
Lymphocyte lowering
(0.5 mg/day)
• Phase 1: ~70%1
• Phase 2 & 3: ~73%6
Safety
No LFT elevationsa
No abnormal PFTs
No titration
No clinically significant first dose
bradycardia
Safety
Elevated LFTsa
Abnormal PFTs
Titration required to blunt
bradycardia
Safety
Elevated LFTsa
Abnormal PFTs
Bradycardia, AV Block
Macular Edema
Carcinoma
Potential Best-in-Class
S1P Receptor Modulator
39
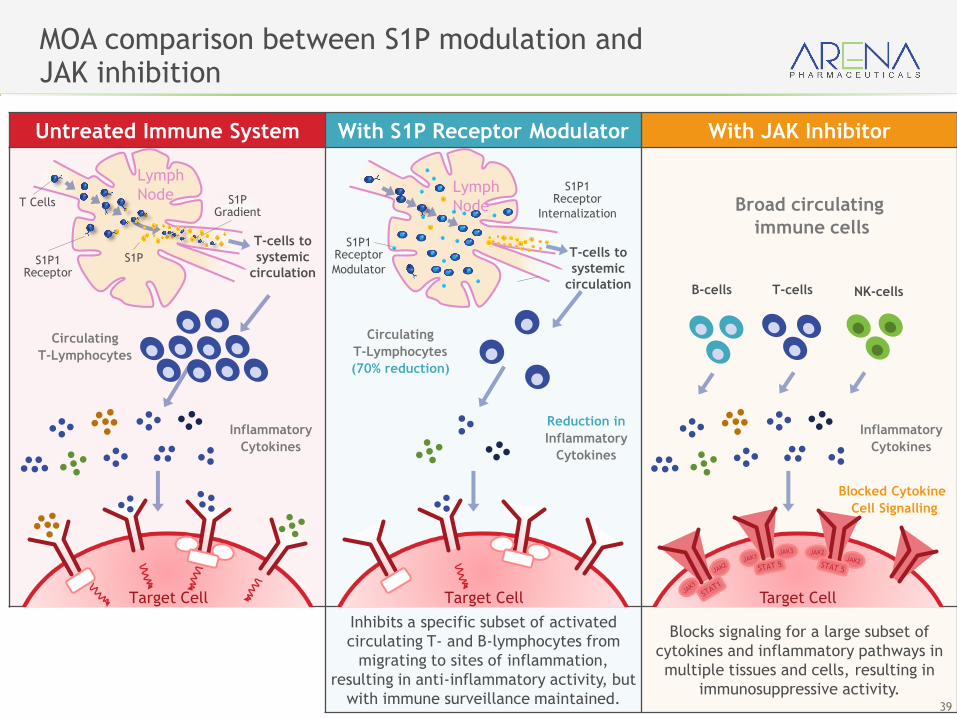
MOA comparison between S1P modulation andJAK inhibition
Untreated Immune System With S1P Receptor Modulator With JAK Inhibitor
Inhibits a specific subset of activated
circulating T- and B-lymphocytes from
migrating to sites of inflammation,
resulting in anti-inflammatory activity, but
with immune surveillance maintained.
Blocks signaling for a large subset of
cytokines and inflammatory pathways in
multiple tissues and cells, resulting in
immunosuppressive activity.
T-cells to
systemic
circulation
T Cells
S1PS1P1Receptor
S1PGradient
Lymph
Node
Circulating
T-Lymphocytes
Inflammatory
Cytokines
Target Cell
T-cells to
systemic
circulation
Lymph
Node
S1P1Receptor
Internalization
Circulating
T-Lymphocytes
(70% reduction)
Reduction in
Inflammatory
Cytokines
Target Cell
S1P1Receptor
Modulator
Broad circulating
immune cells
Inflammatory
Cytokines
Target Cell
Blocked Cytokine
Cell Signalling
B-cells T-cells NK-cells
40
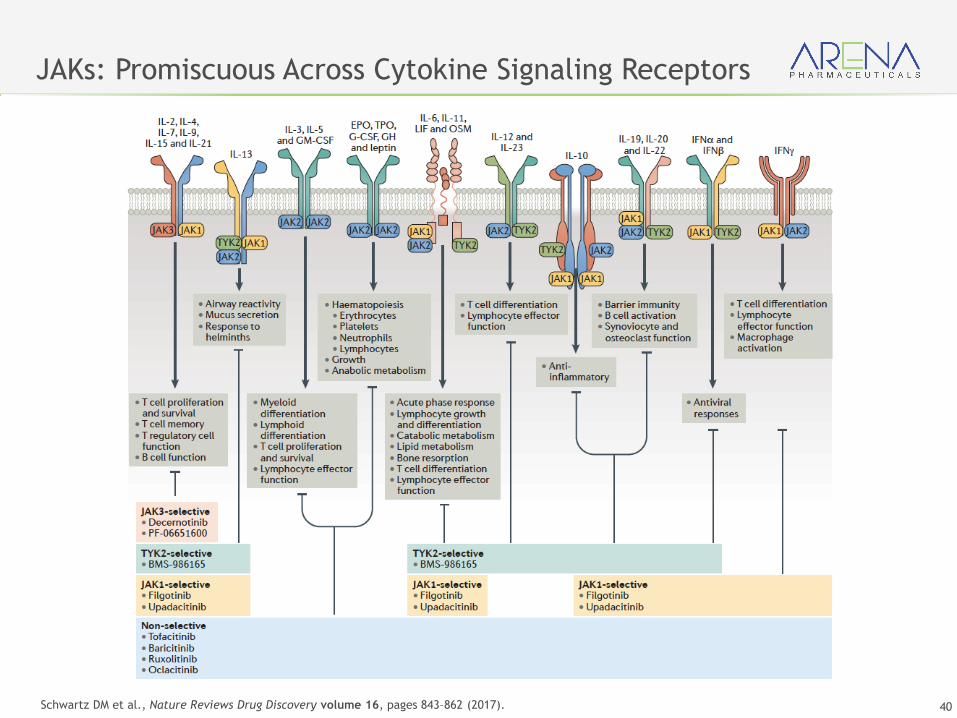
JAKs: Promiscuous Across Cytokine Signaling Receptors
Schwartz DM et al., Nature Reviews Drug Discovery volume 16, pages 843–862 (2017).
41
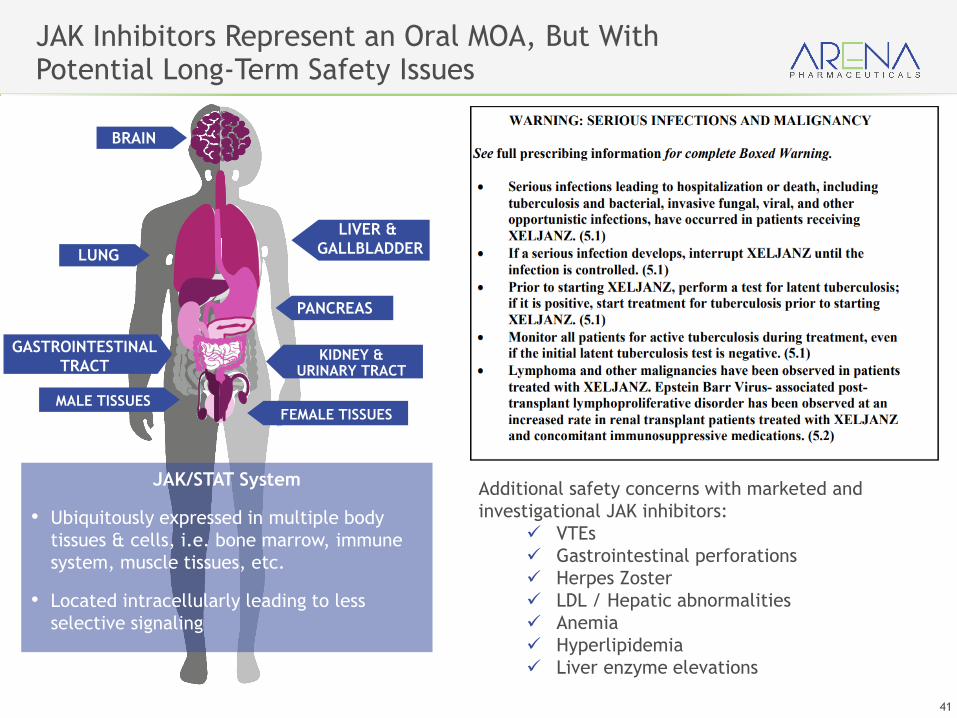
JAK Inhibitors Represent an Oral MOA, But With Potential Long-Term Safety Issues
Additional safety concerns with marketed and
investigational JAK inhibitors:
✓ VTEs
✓ Gastrointestinal perforations
✓ Herpes Zoster
✓ LDL / Hepatic abnormalities
✓ Anemia
✓ Hyperlipidemia
✓ Liver enzyme elevations
BRAIN
LIVER &
GALLBLADDER
PANCREAS
GASTROINTESTINAL
TRACTKIDNEY &
URINARY TRACT
FEMALE TISSUESMALE TISSUES
JAK/STAT System
• Ubiquitously expressed in multiple body
tissues & cells, i.e. bone marrow, immune
system, muscle tissues, etc.
• Located intracellularly leading to less
selective signaling
LUNG
42
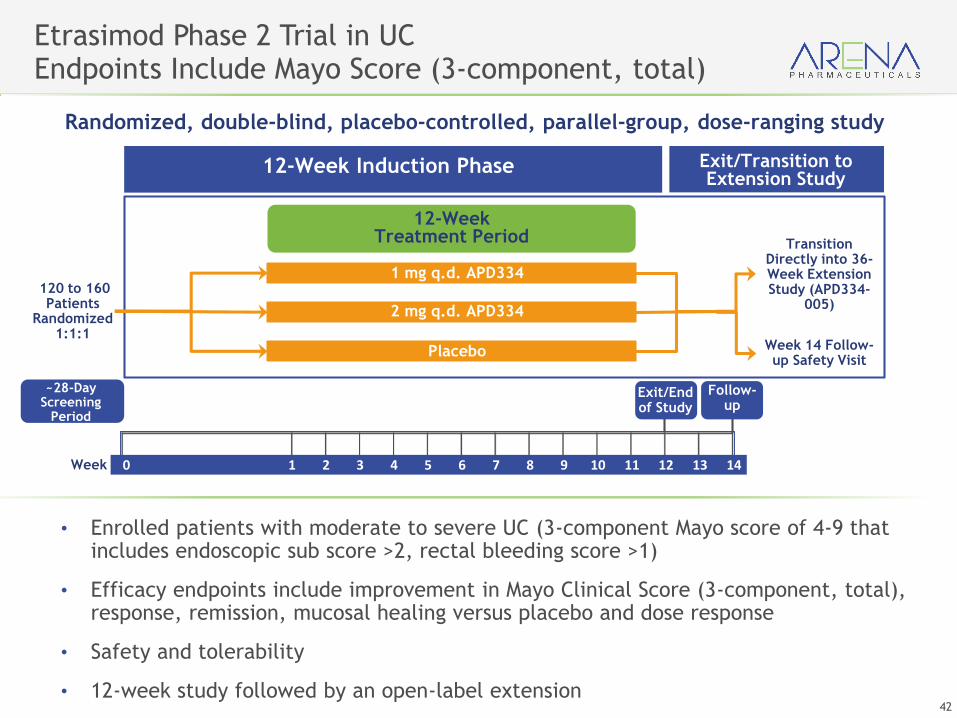
• Enrolled patients with moderate to severe UC (3-component Mayo score of 4-9 that includes endoscopic sub score >2, rectal bleeding score >1)
• Efficacy endpoints include improvement in Mayo Clinical Score (3-component, total), response, remission, mucosal healing versus placebo and dose response
• Safety and tolerability
• 12-week study followed by an open-label extension
Etrasimod Phase 2 Trial in UCEndpoints Include Mayo Score (3-component, total)
Week 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Randomized, double-blind, placebo-controlled, parallel-group, dose-ranging study
12-Week Induction Phase Exit/Transition to Extension Study
12-Week Treatment Period
1 mg q.d. APD334
2 mg q.d. APD334
Placebo
Transition Directly into 36-Week Extension Study (APD334-
005)120 to 160 Patients
Randomized1:1:1
Week 14 Follow-up Safety Visit
Exit/End of Study
~28-Day Screening
Period
Follow-up
43
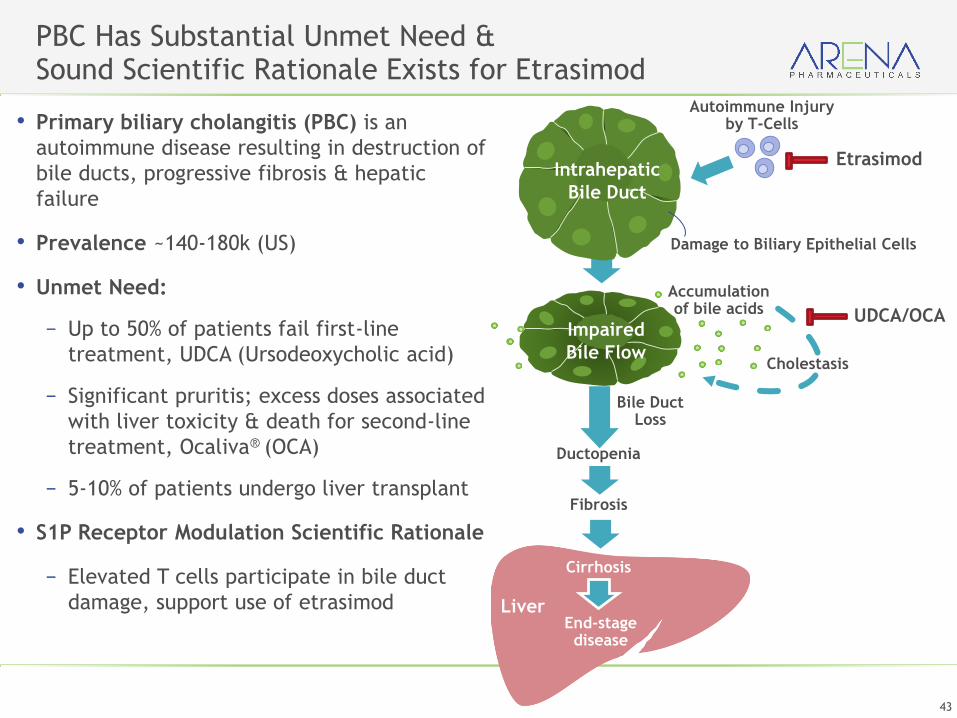
PBC Has Substantial Unmet Need & Sound Scientific Rationale Exists for Etrasimod
• Primary biliary cholangitis (PBC) is an
autoimmune disease resulting in destruction of
bile ducts, progressive fibrosis & hepatic
failure
• Prevalence ~140-180k (US)
• Unmet Need:
− Up to 50% of patients fail first-line
treatment, UDCA (Ursodeoxycholic acid)
− Significant pruritis; excess doses associated
with liver toxicity & death for second-line
treatment, Ocaliva® (OCA)
− 5-10% of patients undergo liver transplant
• S1P Receptor Modulation Scientific Rationale
− Elevated T cells participate in bile duct
damage, support use of etrasimod
Cholestasis
Liver
Autoimmune Injury by T-Cells
Intrahepatic
Bile Duct
Impaired
Bile Flow
Accumulation of bile acids
Bile Duct Loss
Ductopenia
Fibrosis
Cirrhosis
End-stage disease
Damage to Biliary Epithelial Cells
Etrasimod
UDCA/OCA
44
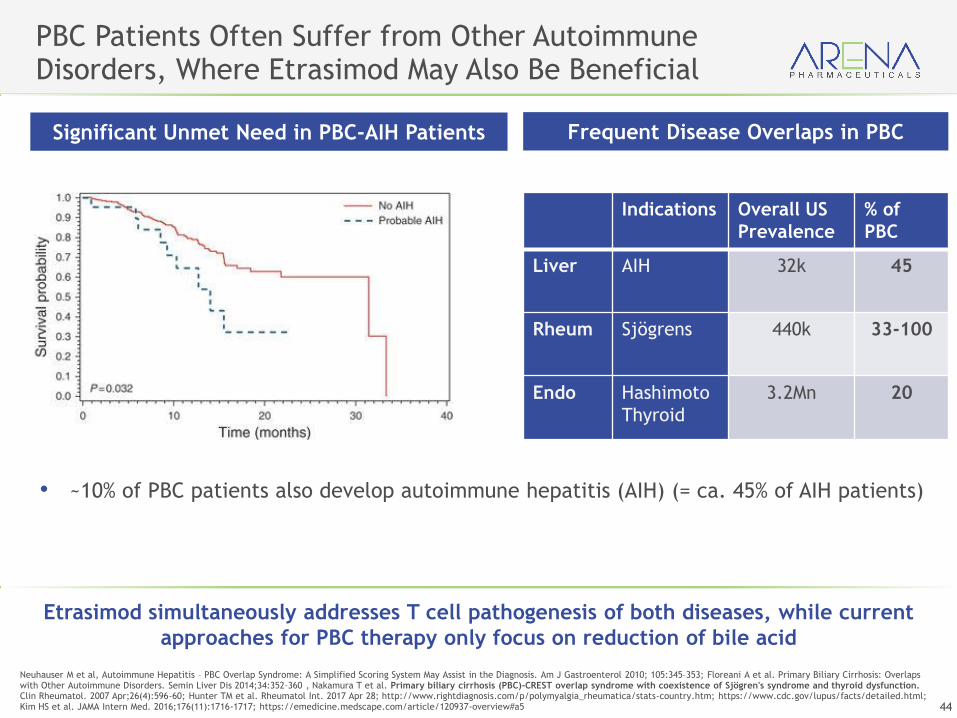
PBC Patients Often Suffer from Other Autoimmune Disorders, Where Etrasimod May Also Be Beneficial
Neuhauser M et al, Autoimmune Hepatitis – PBC Overlap Syndrome: A Simplified Scoring System May Assist in the Diagnosis. Am J Gastroenterol 2010; 105:345–353; Floreani A et al. Primary Biliary Cirrhosis: Overlaps with Other Autoimmune Disorders. Semin Liver Dis 2014;34:352–360 , Nakamura T et al. Primary biliary cirrhosis (PBC)-CREST overlap syndrome with coexistence of Sjögren's syndrome and thyroid dysfunction. Clin Rheumatol. 2007 Apr;26(4):596-60; Hunter TM et al. Rheumatol Int. 2017 Apr 28; http://www.rightdiagnosis.com/p/polymyalgia_rheumatica/stats-country.htm; https://www.cdc.gov/lupus/facts/detailed.html; Kim HS et al. JAMA Intern Med. 2016;176(11):1716-1717; https://emedicine.medscape.com/article/120937-overview#a5
• ~10% of PBC patients also develop autoimmune hepatitis (AIH) (= ca. 45% of AIH patients)
Significant Unmet Need in PBC-AIH Patients
Indications Overall US
Prevalence
% of
PBC
Liver AIH 32k 45
Rheum Sjögrens 440k 33-100
Endo Hashimoto
Thyroid
3.2Mn 20
Frequent Disease Overlaps in PBC
Etrasimod simultaneously addresses T cell pathogenesis of both diseases, while current
approaches for PBC therapy only focus on reduction of bile acid

45
Etrasimod Emerging as a PotentialBest-in-Class S1P Receptor Modulator
Optimal S1P Receptor Subtype Activity
Excellent Lymphocyte Modulation with Rapid Onset/Offset and No Titration Schedule
Broad
Clinical Potential
Superior
Clinical
Utility
Promise Across a Broad
Range of Autoimmune Conditions
Superior
PK / PD
Potential Best-in-Class
Safety Profile
Selectively Targets S1PR1,4,5
& Avoids S1PR2,3
NASDAQ: ARNA
Thank you