Embed Size (px)
Citation preview

1
Kevin D. Huffman D.O.
American Bariatric Consultant
866-270-5116
Bariatric Surgical Patient Carefor the Primary Care Physician
2013 Mid-Summer Medicine Digest

CME Content
• OverviewThis one-hour live lecture will help physicians to have a better understanding of their role
in preoperative and postoperative bariatric surgical patient care.
• Target AudienceThis activity is designed to meet the educational needs of Primary Care Physicians and
Advanced Nurse Practitioners who regularly are asked to treat and manage obese patients.
• Learning ObjectivesUpon completion of this activity, participants should be able to:
• List four medical conditions brought on by or aggravated by obesity
• Discuss the mechanisms by which bariatric surgery produces weight loss
• List three acute postop complications of a gastric bypass and sleeve gastrectomy
CME Content
• Activity Goal
This activity is designed to address the following ABMS / IOM competencies: Patient Care and Medical Knowledge
• Guest Speaker
Kevin Huffman, DOPresidentAmerican Bariatric Consultants
Disclosure: No relevant financial relationship(s) to disclose.
• Disclosures
Cine-Med adheres to ACCME Essential Areas, Standards, and Policies, regarding industry support of continuing medical education. Disclosure of the planning committee and faculty's commercial relationships will be made known at the activity. Speakers are required to openly disclose any limitations of data and/or any discussion of any off-label, experimental, or investigational uses of drugs or devices in their presentations.
All Cine-Med employees in control of content have indicated that they have no relevant financial relationships to disclose.

CME Content
• Accreditation
Ciné-Med is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
Ciné-Med designates this live activity for a maximum of 1.00 AMA PRA Category 1 Credit(s)™. Physicians should only claim credit commensurate with the extent of their participation in the activity.
• Supporters
This activity is being supported by an educational grant from Covidien.
• CME Credit Tracking / Evaluation
Use the following address to access Credit Certificates and complete an evaluation. http://cine-med.com/certificates/obesity20130702

5
Topics of this Presentation
• Classification of Obesity and Patient Selection• Preoperative Patient Care
– Preoperative Check List– Physician Supervised Weight Loss
• Bariatric Surgical Overview• Postoperative Patient Care

6
Moderate Obesity1 (BMI 35 to 39.9 )
Morbid Obesity1
(BMI 40 or more)Normal Weight1 (BMI 18.5 to 24.9)
Obese1
(BMI 30 to 34.9)
Overweight1
(BMI 25 to 29.9)
1. National Institutes of Health/National Heart, Lung and Blood Institute Clinical Guidelines Evidence Report. NIH Publication 98-4083, September 1998. 2. National Institutes of Health/National Heart, Lung and Blood Institute Clinical Guidelines Evidence Report. NIH Publication 98-4083, September 1998. 3. US Department of Health and Human Services. The Surgeon General’s Call to Action to Prevent and Decrease Overweight and Obesity;2001.
Class I Obesity
Class II Obesity Class III
Obesity
Classification of Overweight & Obesity by BMI, Waist Circumference & Associated Disease Risk*
Disease Risk ---- Increased High Very High Extremely High
*Disease risk for type 2 diabetes, hypertension, and CVD, relative to normal weight and waist circumference.
Additional Risks:• Large waist circumference (men >40 in; women >35 in)2
• Weight gain as little as 11 pounds increases risk of developing type 2 diabetes3
• Specific races and ethnic groups6

Obesity Treatment Guide
Treatment 25-26.9 27-29.9 30-34.9 35-39.9 >40
Diet, Exercise, Behavior Tx
With comorbidities
With comorbidities + + +
Pharmaco-therapy
With comorbidities + + +
Surgery With comorbidities
With comorbidities
7
1.The Practical Guide: Identification, Evaluation, and Treatment of Overweight and Obesity in Adults . National Institutes of Health. National Heart, Lung, and Blood Institute. October 2000, NIH Publication No. 00-4084.
BMI Category (kg/m2)

8
1998 NIH Obesity Clinical Guidelines
The Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults
http://www.nhlbi.nih.gov/guidelines/obesity/ob_gdlns.pdf

9
2005 American College of Physicians Issues Guidelines for Obesity Management
Calls on physicians to screen for obesity and treat it appropriately.
Recommends that all patients with a BMI of more than 30 receive information on diet and exercise.
When diet and exercise alone are insufficient for patients to reach their goals, available obesity drugs should be considered.
Patients who fail with medically supervised weight loss, should be referred to bariatric surgery centers with a strong record of experience in these procedures .

10
2011 CMS: IBT for Obesity
CMS announces payment for physician supervised: Intensive Behavioral Therapy for Obesity
http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/ICN907800.pdf
11
2013 AMA: Obesity IS a Disease
The AMA's decision makes diagnosis and treatment of obesity a physician's professional obligation.
Steps up pressure on health insurance companies to reimburse physicians for obesity screening, treatment and referral.

12
Obesity Treatment Pyramid
BMI > 40
35
30
25
Diet Physical Activity
Lifestyle Modification
Pharmacotherapy
Bariatric Surgery
BMI ≥ 40
35
30
25
Source: The Practical Guide: Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. National Institutes of Health. National Heart, Lung, and Blood Institute. October 2000, NIH Publication No. 00-4084.

13
Bariatric Surgery:Preop Patient Care

14
Bariatric Surgical Preop Checklist
• Contact bariatric surgical team to discuss preop process, preop orders, insurer requirements, preop seminar requirement.
• Discuss bariatric surgical options, risk/benefits, realistic expectations and postop compliance with patient, and patient’s support network

15
Bariatric Surgical Preop Checklist
• Collect documented weight history
• Collect weight loss program participation and attempts
• Document medical necessity for surgery, send letter of referral to surgical center

16
Bariatric Surgical Preop Checklist
• Review medical history, ROS, nutritional, exercise and behavioral assessment, complete comprehensive new physical exam
• Preop lab, vitamin level (Vit D, B12, Thiamine), CBC, CMP, serum ferritin, diagnostic studies (sleep, etc) coordinate with bariatric surgical team

17
Bariatric Surgical Preop Checklist
• Psych evaluation• Looking for undiagnosed/untreated psychiatric
conditions• R/O active chemical dependency• Determine readiness for surgery • Does the patient understand the preop and postop
requirements and orders, are they committed to living the require postop lifestyle, have they set realistic goals.

18
Bariatric Surgical Preop Checklist
• Stop smoking for minimum of 8 weeks preop
• History of DVT, prophylactic treatment per surgeon
• Fine tune all medications and CPAP settings
• ‘Medically supervised’ weight loss 3-6 months LCD with diet, exercise and behavior logs
• VLCD 2-4 weeks preop.

19
Physician Supervised Weight Loss

20
Documentation of Preop ‘Physician Supervised Weight Loss’
• Most insurers require from 3-12 months of ‘medically supervised’ preoperative weight loss in order to secure surgical authorization– Clearly document one office visit per month with a
diagnosis of morbid obesity (278.01)– Document that diet, exercise and behavior were
discussed in the plan of treatment.– In some cases a separate registered dietician visit
or two may be required (check with you local bariatric surgical billing staff)

21
Why Preoperative Weight Loss?
Many insurers require it. Some bariatric surgeons have upper BMI limits
for surgical candidates. Any preoperative weight loss decreases risk of
surgery, shrinks liver, reduces perioperative medication, reduces anesthesia risk, improves recovery
Prepare patients for a lifetime of change.

22
Preop Diet Progression
• Patient is placed on a nonrestrictive diet until 3 months prior to surgery when the diet begins to restrict total calorie and increase protein content.
• 2 months prior to surgery patient should be on 45-60 grams of supplemented protein and a preop vitamin
• 2-4 weeks prior to surgery patient should be on a VLCD

23
Bariatric Surgery Overview

24
Bariatric Surgical Procedures
• Duodenal Switch
• Adjustable Gastric Band
• Roux-en-Y Gastric Bypass (combo)
• Sleeve Gastrectomy
Malabsorptive Operation
Restrictive Operation

25
Adjustable Gastric Band

26
Adjustable Gastric Band
• Adjustment: Time and Cost Factors
• Activation of stretch receptors
• No Metabolic Benefit
• Weight Loss - Slow, Less Robust
• Cxs: Erosion, Slip, Tube/Port issues
• Approved for BMI 30 with co-morbid
• Implant numbers are slowing

27
Sleeve Gastrectomy
• Mechanism of action restrictive
• Metabolic benefit
• Cxs: Bleeding, Leak, Minimal Long-term
• Contraindicated: GERD?
• Weight loss: 65% EBWL
• Growing popularity

28
Roux-en-Y Gastric Bypass
• Mechanism of action: restrictive and mal-aborptive
• Metabolic benefit
• Cxs:– Early: Bleeding, Leak– Late: Hernia, Ulcer, Gallbladder,
Mineral malabs
• Weight Loss: 75% EBWL
• Most popular surgery

29
Bilio Pancreative Diversion
• Mechanism of action: mal-aborptive
• Metabolic benefit
• Cxs:– Early: Bleeding, Leak– Late: Hernia, Ulcer, Gallbladder,
Mineral malabs
• Weight Loss: 75-85% EBWL
• Not a common procedure today

30
30-Day Mortality
Author Data n RYGB Sleeve Band
Flum 2009
LABS-1 47760.2 (2.1
Open)0
Lancaster 2008
ACS-NSQIP 4756 0.14 0.09
Finks 2011
MBSC 25,469 0.1 0.1 0.04
Jackson 2012
ACS-BSCN 28,616 0.14 0.11 0.05

31
Risk of Not Having Surgery
• N= 1035 surg vs 5746 age, gender matched obese
controls without other diseases (Quebec Health Ins
Database)
• Surg ↓ cardiovasc, onc, endocrine, infxs, psych but ↑
digestive diseases
• 5 yr mort 0.68% surg vs 6.17% control
• RR dying 0.11 (95% 0.04 – 0.27)
• = 89% Reduction in risk of dying over 5 yrs
Christou Ann Surg. 2004; 240(3): 416-23
32
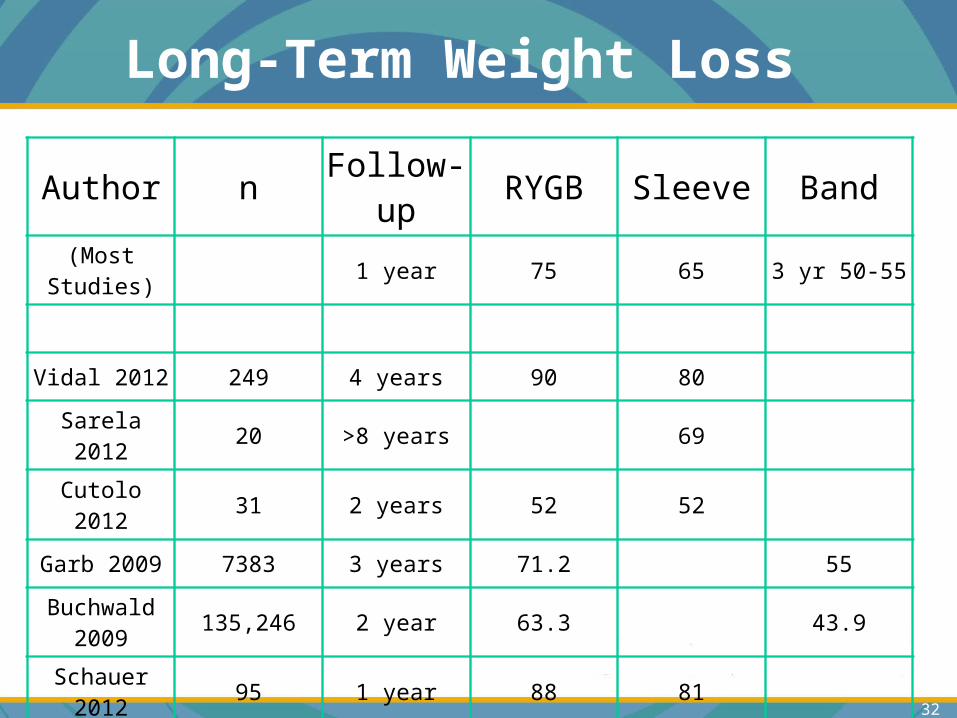
Long-Term Weight Loss
Author n Follow-up RYGB Sleeve Band
(Most Studies)
1 year 75 65 3 yr 50-55
Vidal 2012 249 4 years 90 80
Sarela 2012 20 >8 years 69
Cutolo 2012 31 2 years 52 52
Garb 2009 7383 3 years 71.2 55
Buchwald 2009
135,246 2 year 63.3 43.9
Schauer 2012
95 1 year 88 81
Higa 2011 242 10 year 57
33
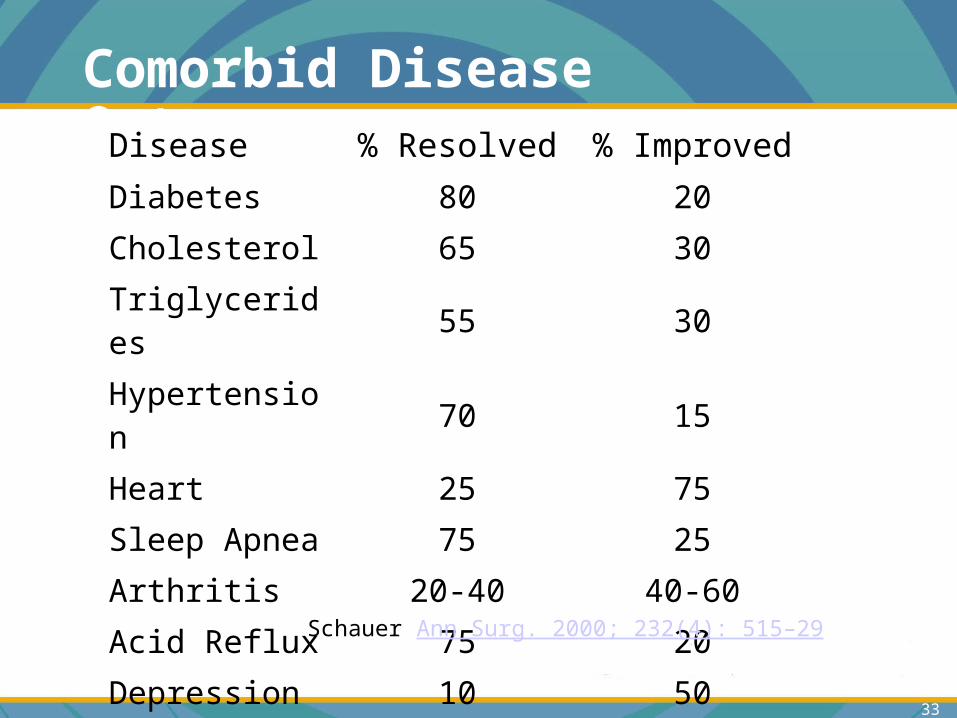
Comorbid Disease OutcomeDisease % Resolved % Improved
Diabetes 80 20
Cholesterol 65 30
Triglycerides 55 30
Hypertension 70 15
Heart 25 75
Sleep Apnea 75 25
Arthritis 20-40 40-60
Acid Reflux 75 20
Depression 10 50
Schauer Ann Surg. 2000; 232(4): 515–29

34
Bariatric Surgery:Postop Patient Care
35
Postop Complications
Lap-band: rare, slip, erosion, poorly adjusted
Gastric Bypass: strictures, leaks, stenosis, ulcers, vitamin/mineral deficiencies, anemia
Gastric Sleeve: staple line bleed, leak, stenosis, obstruction, vitamin/mineral deficiencies
Postop Complications
36
Pain or Vomiting
• Bypass: leak/abscess, sbo, stenosis
• Sleeve: leak, stricture
• All: VTE
• Bypass: gallbladder, ulcer, internal hernia
• Sleeve: leak, GERD
• Band: prolapse (slip), erosion, too tight
Early
Late

37
Postop Care
• Post-surgical care critical to optimal weight loss after bariatric surgery
• Postop compliant patients lost 35% more the 1st year postop and tend to keep more weight off up to 5 years. ASMBS survey 2008

38
Postop Care
•Discuss follow up schedule with bariatric surgical team
•Weekly OV first month, OV every other week for 2nd and 3rd month (to adjust medications and watch form postop complications) then once a month until 12 month postop.
• Second year OV every other month.
• Frequent need to adjust diabetic, hypertension, hyperlipidemic medications, adjust CPAP, encourage support group, follow up with bariatric surgical team,

39
Postop Care
•Progression of diet Phase 1-4
•Vitamin supplements
•Protein supplements
•Postop labs and vitamin levels
•Support group attendance
•STOP SMOKING

40
Vitamin and Mineral Needs
• Annually check Calcium, Folate, B12, Iron, Thiamine, Vit D, PTH
• Annually CMP, CBC, LFT, Lipid profile
• Dexa every 12-18 months
• Malabsorptive: Vit A, Vit D.
• Vomiting: Vitamin B1, Copper
• Daily Multivitamin, Calcium Citrate
41
Supplement Schedule: Gastric Bypass Gastric Sleeve
Breakfast•Multivitamin 200% of most nutrients •B12/folate 1,000mg B12 800mg folate•Iron glycinate 30 mgLunch•500 mg Calcium Citrate with Vitamin D3 Dinner•500 mg Calcium Citrate with Vitamin D3 Bedtime•500 mg Calcium Citrate with Vitamin D3
Additional vitamin supplements, per lab findings

42
Postop Care: meal progression
• Phase 1: clear liquids first 1-2 weeks postop– Maximum volume 60cc or 2oz
• Phase 2: full liquids 2-4 weeks postop• Phase 3: soft/pureed foods weeks 4-6 postop
– Maximum volume 60cc or 2oz– Maximum 3 meals a day no snack between meals
• Phase 4: solid foods – Avoid eating 3 hours prior to sleep– May add protein supplements between meals is
needed

43
Return to phase 2 diet for 24-72 hours:
– 1. after band adjustments
– 2. after overeating episode
– 3. after episode of nausea or vomiting
– 4. after period of weight gain

44
Postop Diet
• Chew food thoroughly and slowly taking 30 minutes to eat each small meal (three per day)
• No fluids 30 minutes prior to or after meals
• Avoid grazing or snacks between meals
• Avoid high calorie liquids at all times
45
Postop nutritional/medical malabsorption
•Small gastric pouch and bypass jejunum leads to insufficient protein intake and absorption
•Bypass: less absorptive surface in stomach, less acid in stomach, less contact with duodenum and jejunum.
•Stomach, duodenum and upper jejunum are major sites of absorption of iron, calcium and B vitamins
•Most oral meds absorb through the stomach and small intestine

46
Postop Complications: NSAIDs
• NSAIDs:– Prevent production of prostaglandins which protect the
anastomosis– Direct irritants
• Use cytotec and/or carafate if NSAIDs can’t be avoided– Cytotec is a prostaglandin producer– Carafate coats the stomach and intestine
• PPI decrease acid but no effect on prostaglandins; bypass patient already have reduced acid levels but further reducing acid on the anastomosis can be of benefit
47
Postop Exercise and Psych
• Exercise:– 30 minutes of exercise daily– Exercise can begin 6 weeks postop
• Psych:– It is very common to be emotionally labile for the
first 2-3 months post-op– Many patients face body image distortion postop– Postop group support a must– Postop psych follow may be necessary

48
Share Outcome Data
We all need to share 5-10 year outcome data to document long-term safety and efficacy of bariatric surgery

49
Topics we Discussed
• Classification of Obesity and Patient Selection• Preoperative Patient Care
– Preoperative Check List– Physician Supervised Weight Loss
• Bariatric Surgical Overview• Postoperative Patient Care

50
Thank You
Kevin D. Huffman D.O.
American Bariatric Consultants
866-270-5116





























