Embed Size (px)
Citation preview
Kevin Arnold RN, BSNCoordinator, PICC Program VA Long Beach, CA
Medicine & Inpatient Healthcare Group | Spinal Cord Injury | Community Living Center
Ultrasound Guided Peripheral IV Technique
Precision & Solution for the Hidden Veins
+ =
Ultrasound Guided PIVs
To learn when to utilize ultrasound technology for peripheral IV starts and blood draws
To understand peripheral venous anatomyTo become familiar with the basics of high frequency-low
depth - ultrasound machinesTo be familiar with potential complicationsTo understand vein/catheter selectionTo learn technique required to cannulate a deep veinTo be familiar with common pitfalls
Objectives
Common Difficult StickObeseEdematousDehydratedDiabeticDependent on
dialysis
Post chemotherapyPost mastectomyA drug abuserIn shock
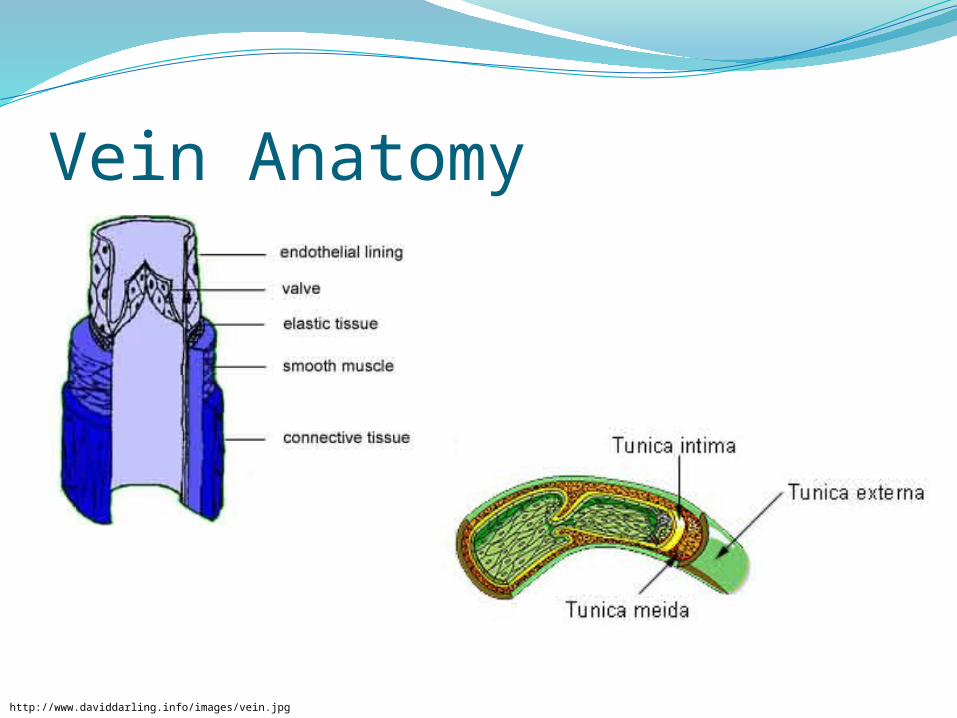
Vein Anatomy
http://www.daviddarling.info/images/vein.jpg
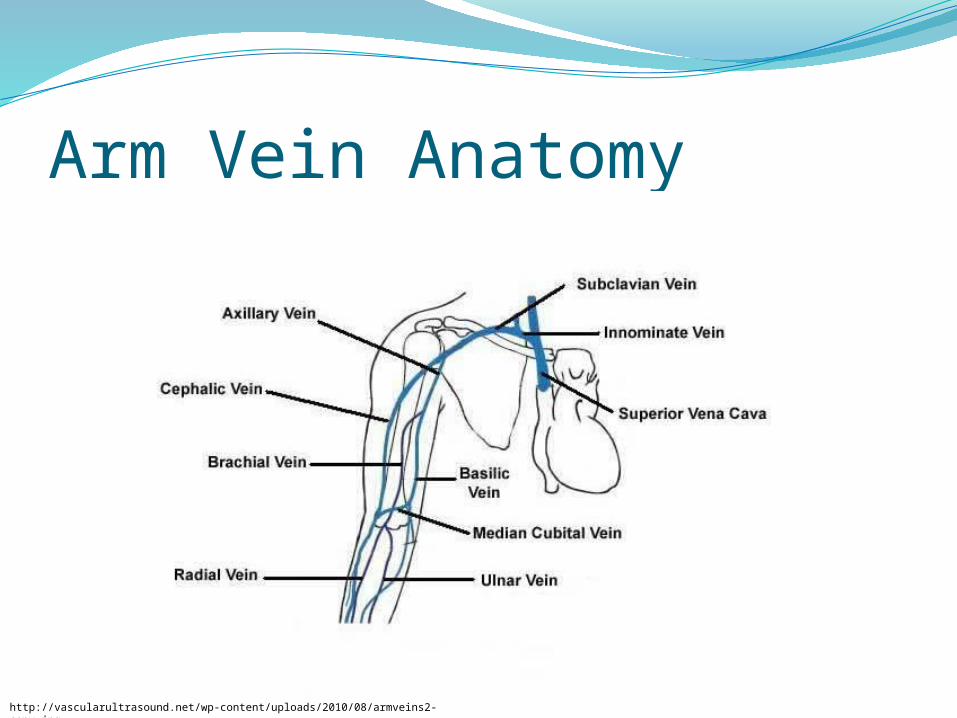
Arm Vein Anatomy
http://vascularultrasound.net/wp-content/uploads/2010/08/armveins2-copy.jpg
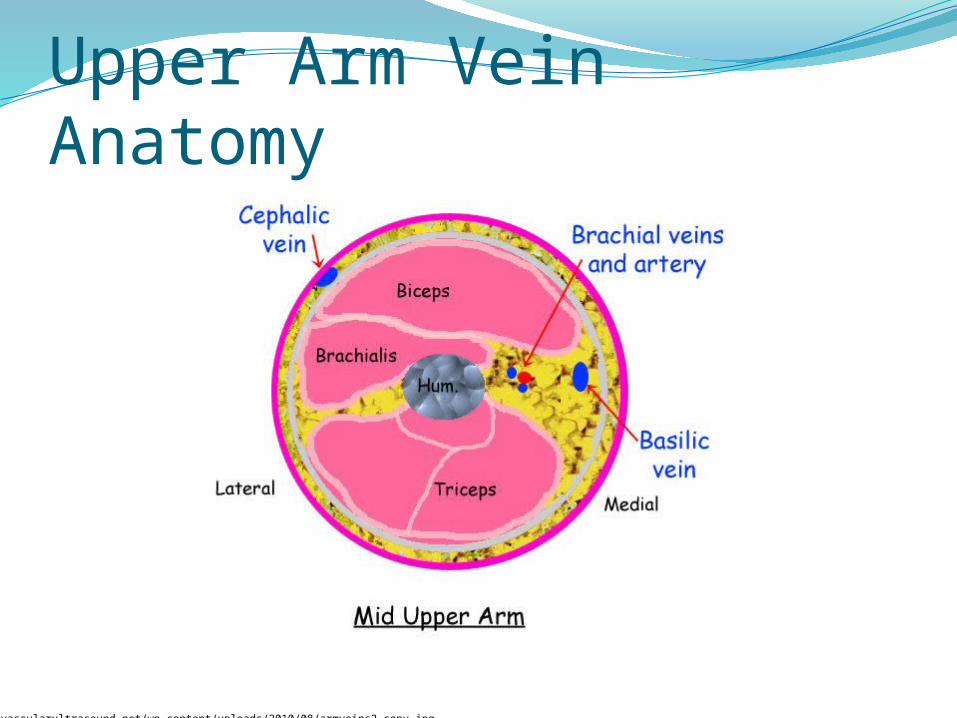
Upper Arm Vein Anatomy
http://vascularultrasound.net/wp-content/uploads/2010/08/armveins2-copy.jpg
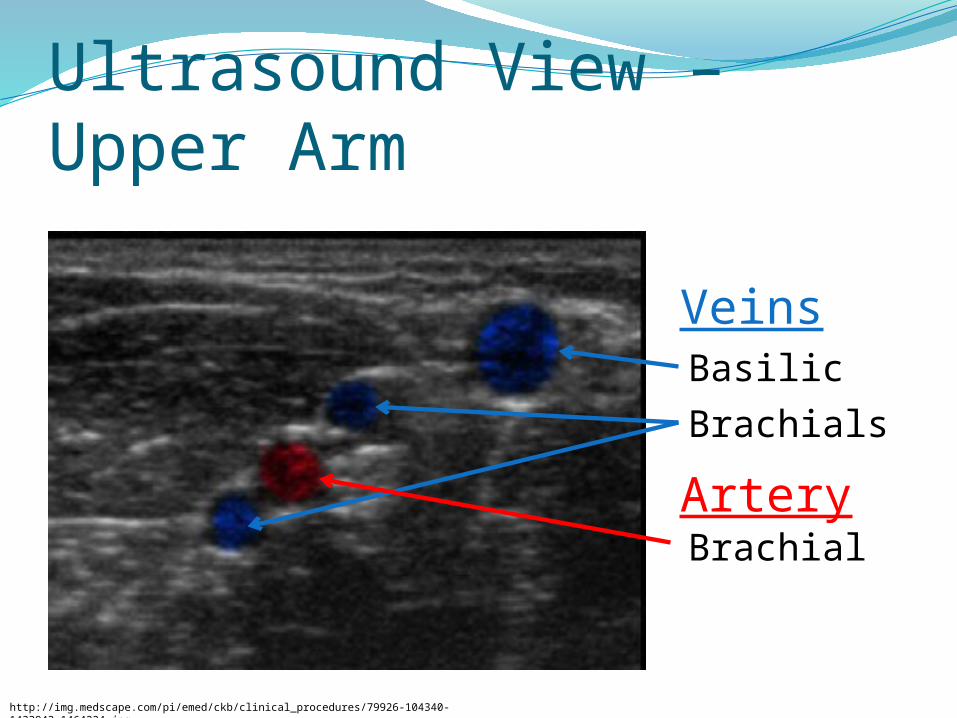
Ultrasound View – Upper Arm
Basilic
Brachials
Veins
ArteryBrachial
http://img.medscape.com/pi/emed/ckb/clinical_procedures/79926-104340-1433943-1464224.jpg
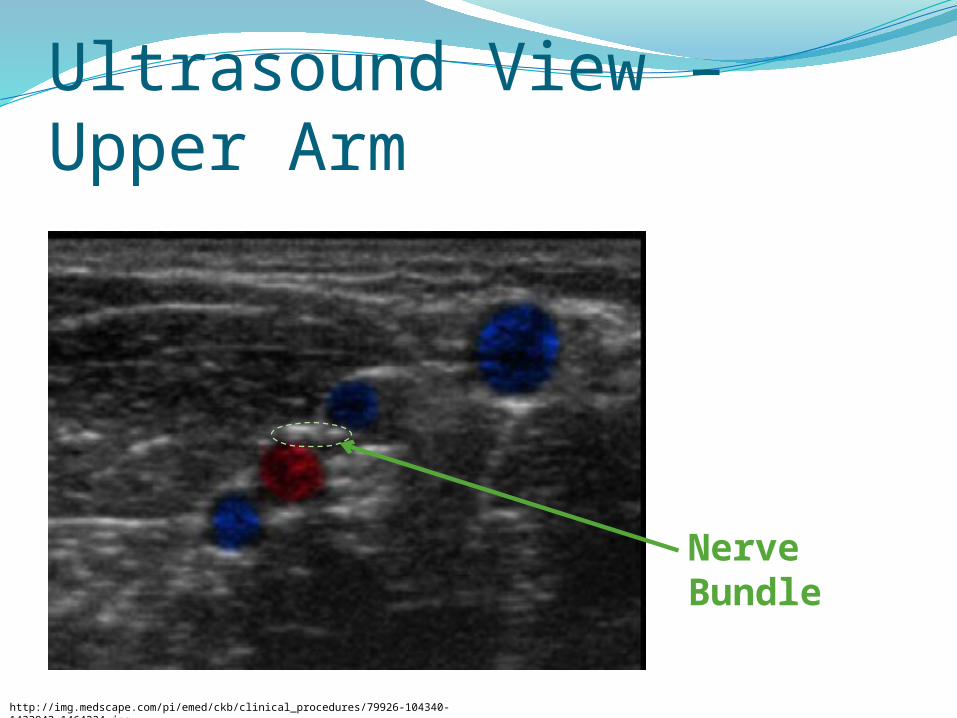
Ultrasound View – Upper Arm
Nerve Bundle
http://img.medscape.com/pi/emed/ckb/clinical_procedures/79926-104340-1433943-1464224.jpg
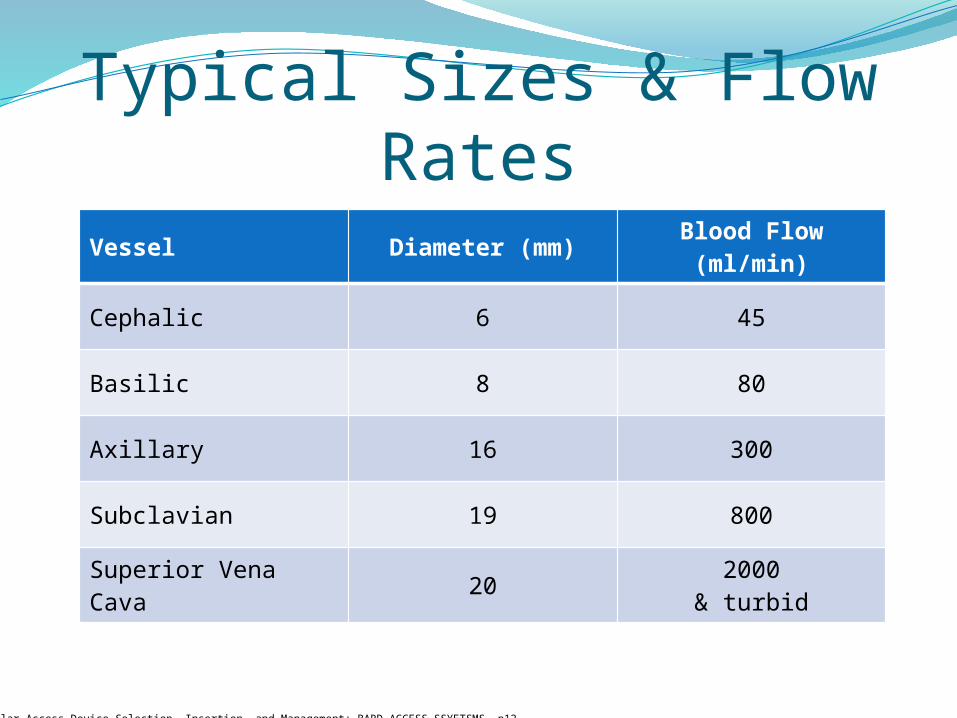
Typical Sizes & Flow RatesVessel Diameter (mm) Blood Flow (ml/min)
Cephalic 6 45
Basilic 8 80
Axillary 16 300
Subclavian 19 800
Superior Vena Cava 20 2000& turbid
Vascular Access Device Selection, Insertion, and Management: BARD ACCESS SSYETSMS, p12.
Anatomical PerformanceOpinion…Veins in forearms do not tolerate high rates well, but
are less likely to dislodgeVeins in dominant hands tolerate higher rates, but
are more likely to dislodge and develop phlebitis
“Rule of Thumb”Be patientLook for sites that will have the best possible successUse warm packs if extremities are cold to touchAvoid veins in ante-cubital fosa and wrists if possibleUse good judgmentAvoid sticking nerve bundlesWorst case scenario:
Helpful vein dilator – nitro paste between the fingers, with MD order, will dilate veins.
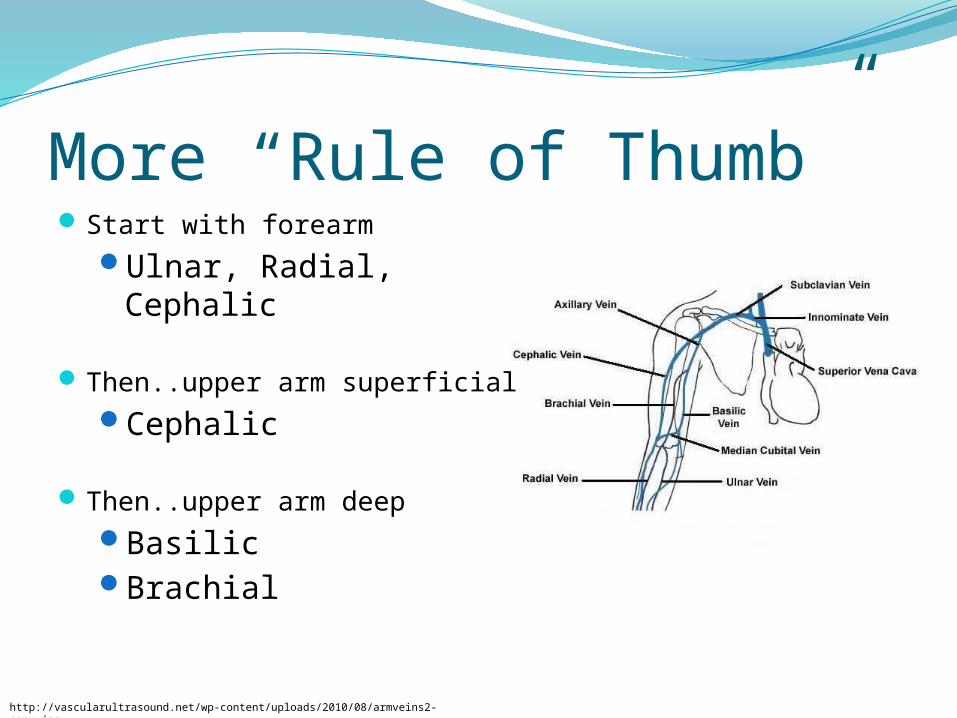
More “Rule of Thumb”Start with forearm
Ulnar, Radial, Cephalic
Then..upper arm superficialCephalic
Then..upper arm deepBasilicBrachial
http://vascularultrasound.net/wp-content/uploads/2010/08/armveins2-copy.jpg
Ultrasound Equipment
Insert your type of machine…Include location and instructions for checkout & use.
http://www.bardaccess.com/assets/images/products/ultrasound/siterite6_unit_hero.jpg
http://65.36.201.165/instrumentpics/sonositeiLook.jpg
Photo by Kevin Arnold, RN, BSN. [email protected]
Ultrasound TechnologyVery high frequency sound wavesRequires fluid medium for oscillating transmissionVisual images are the reflection of echoes of high
frequency sound beams from soft tissuesUltrasound waves do not transmit through airSound waves do not penetrate high density areas
well
Ultrasound MachinesAlways plug in power adapterBattery life is unpredictableMachine must be signed out in log book located at
respective nursing stationClean before and after usePlease take careful care in handling equipmentVery expensive… $15,000 - $25,000Replacement probe… $3,500 + (don’t drop it)
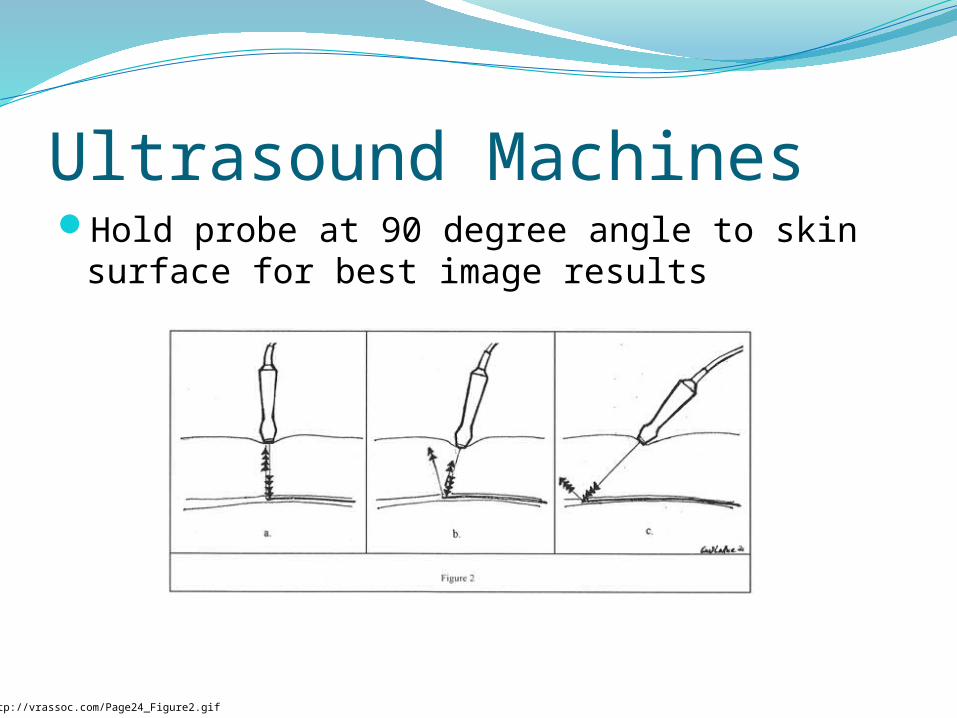
Ultrasound MachinesHold probe at 90 degree angle to skin surface for best
image results
http://vrassoc.com/Page24_Figure2.gif
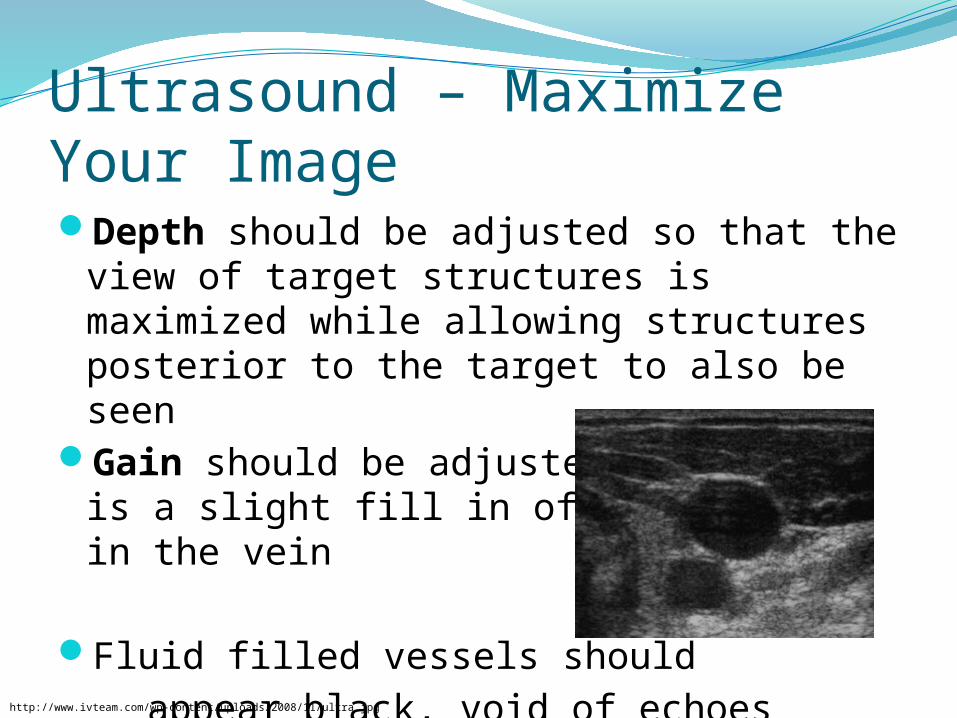
Ultrasound – Maximize Your ImageDepth should be adjusted so that the view of target
structures is maximized while allowing structures posterior to the target to also be seen
Gain should be adjusted until there is a slight fill in of white pixels in the vein
Fluid filled vessels should appear black, void of echoes
http://www.ivteam.com/wp-content/uploads/2008/11/ultra.jpg
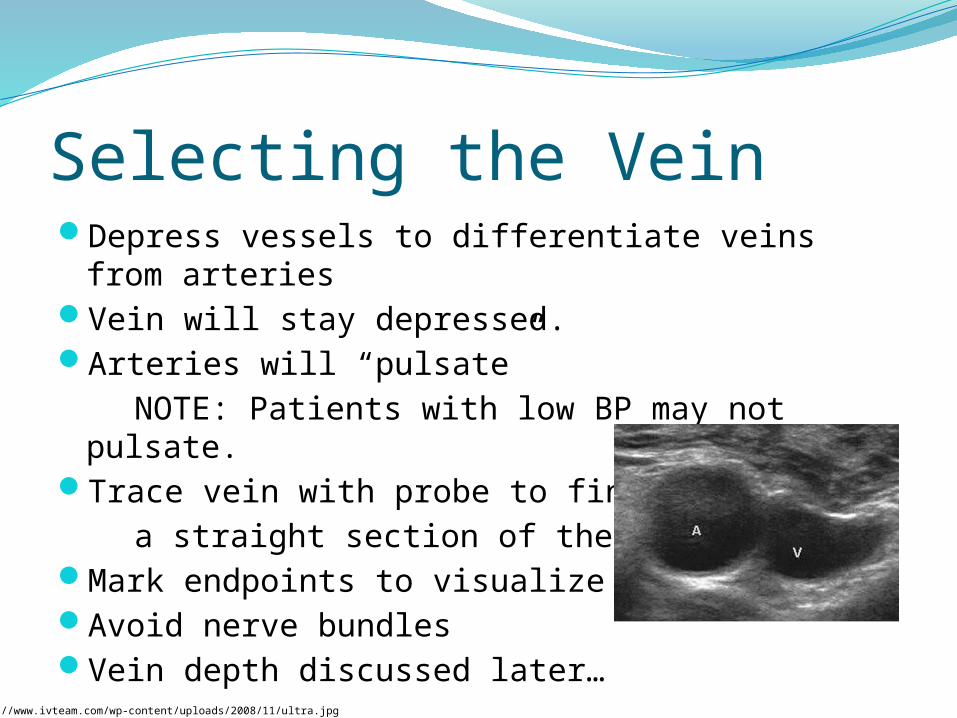
Selecting the VeinDepress vessels to differentiate veins from arteriesVein will stay depressed.Arteries will “pulsate” NOTE: Patients with low BP may not pulsate.Trace vein with probe to find a straight section of the veinMark endpoints to visualize vein pathAvoid nerve bundlesVein depth discussed later…
http://www.ivteam.com/wp-content/uploads/2008/11/ultra.jpg
Selecting the CatheterCatheter size selection should reflect size of available
vessel and type of therapy to minimize/prevent complications and maintain adequate access.
NOTE: Phlebogenic drugs are best given through a small catheter in the largest available vessel.
Catheter length should be adequate to ensure that ½ of the catheter will reside in the lumen of the vessel. Be sure to take the angle of approach into consideration when determining vessel depth (depth scale available on US screen).
Selecting the CatheterFloor Stock [ Insert your model ]
1.25 inch | 32 mm18, 20, 22, 24 gauge
U/S Cart Stock [ Insert your model ]1.75 in | 45 mm20 gaugeThis will require adding tubing
Choose one-handed use products
http://www.mtrhealth.com/ImageViewer.aspx?img=~/public/images/425-2543.jpg&w=150
http://catalog.bd.com/ecat/images/f10/bdnexiva.jpg
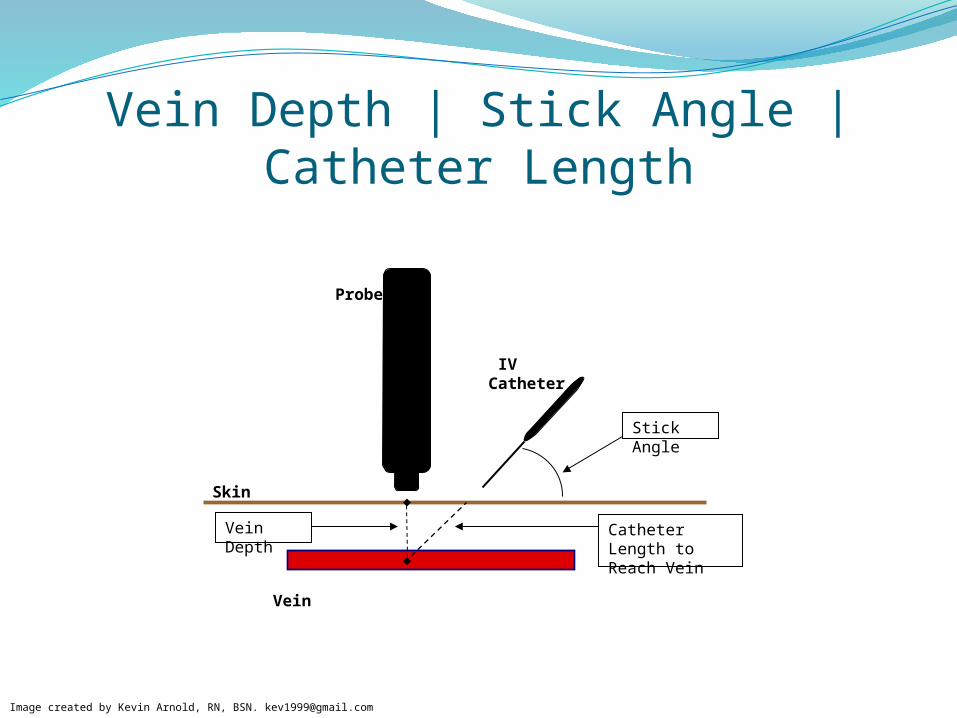
Vein Depth | Stick Angle | Catheter Length
Vein Depth Catheter Length to Reach Vein
Skin
Stick Angle
Probe
IV Catheter
Vein
Image created by Kevin Arnold, RN, BSN. [email protected]
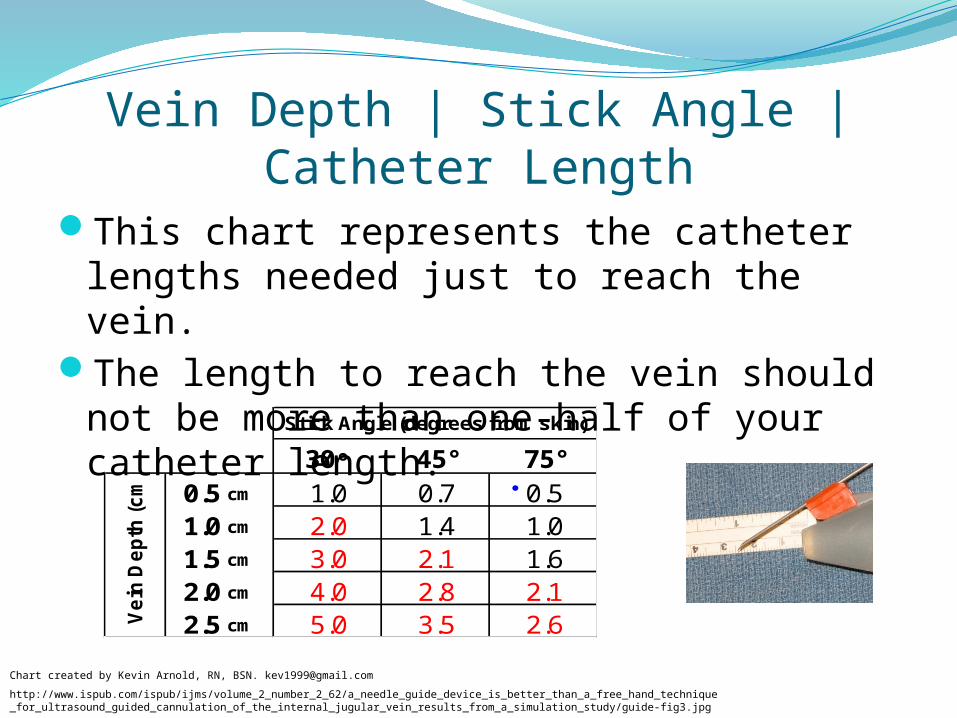
This chart represents the catheter lengths needed just to reach the vein.
The length to reach the vein should not be more than one-half of your catheter length.
30° 45° 75°
0.5 cm 1.0 0.7 0.51.0 cm 2.0 1.4 1.01.5 cm 3.0 2.1 1.62.0 cm 4.0 2.8 2.12.5 cm 5.0 3.5 2.6V
ein
De
pth
(c
m)
Stick Angle (degrees from skin)
Vein Depth | Stick Angle | Catheter Length
http://www.ispub.com/ispub/ijms/volume_2_number_2_62/a_needle_guide_device_is_better_than_a_free_hand_technique_for_ultrasound_guided_cannulation_of_the_internal_jugular_vein_results_from_a_simulation_study/guide-fig3.jpg
Chart created by Kevin Arnold, RN, BSN. [email protected]
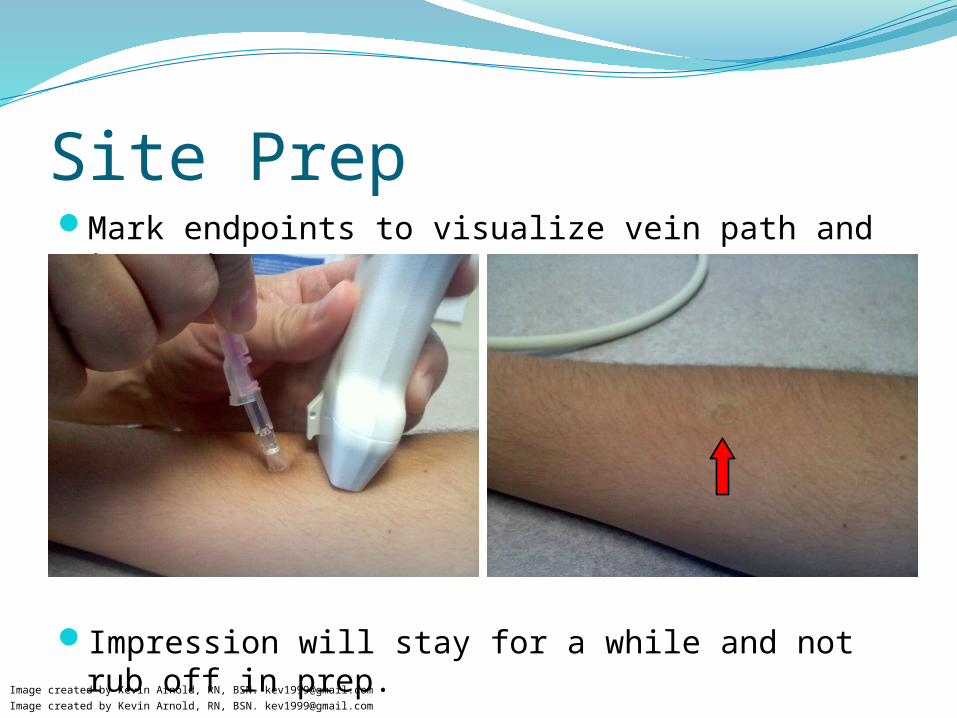
Site PrepMark endpoints to visualize vein path and insertion area
Impression will stay for a while and not rub off in prep.
Image created by Kevin Arnold, RN, BSN. [email protected]
Image created by Kevin Arnold, RN, BSN. [email protected]
Site PrepUsing friction, scrub the selected site about 3 inches in
diameter for 30 sec and allow to dry (2minutes for areas of dense hair)
NOTE: Do not blot or wipe on site to speed drying. Prep surface of transducer using ChloraPrep sponge
(once prepped, do not allow probe to contact non-prepped areas. )
Apply a small amount of sterile gel to probe or above selected insertion site
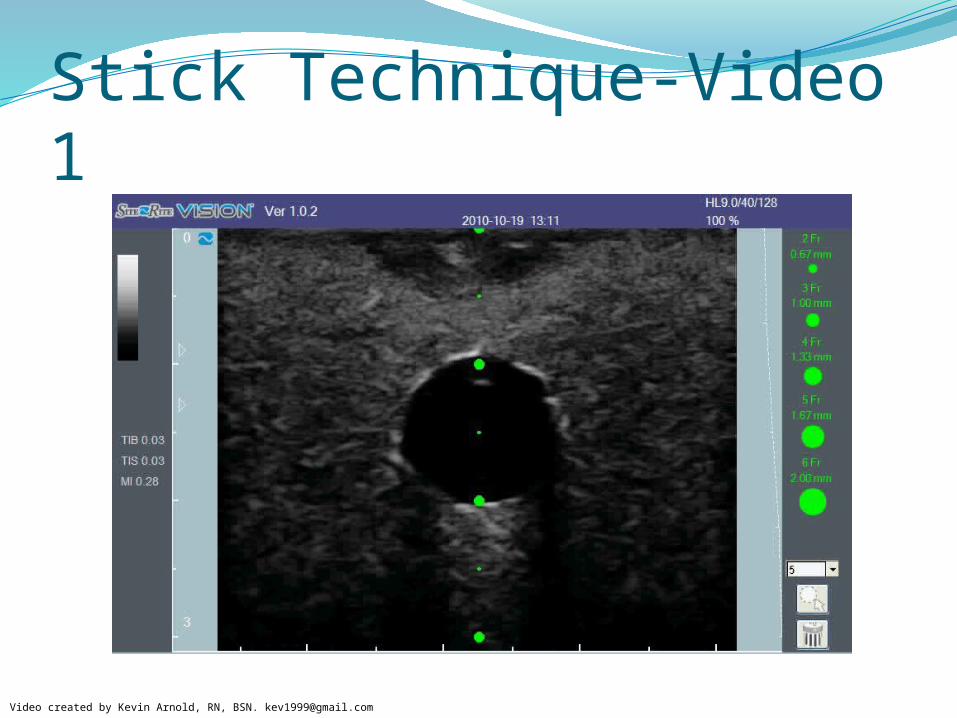
Stick TechniqueConsider the concept of catheter length vs. angle
of insertion. It is important to balance the two. Use on-screen guide to measure depth of vein
and direction. Each dot = ½ cm.Veins around 1.0 cm deep are usually the
easiest.Sticks will be easier with a higher angle of
insertion, but this must be balanced with the catheter’s ability to bend.
Avoid kinking the catheter.http://www.bardaccess.com/assets/images/products/ultrasound/supporting/product-siterite-needles.jpg
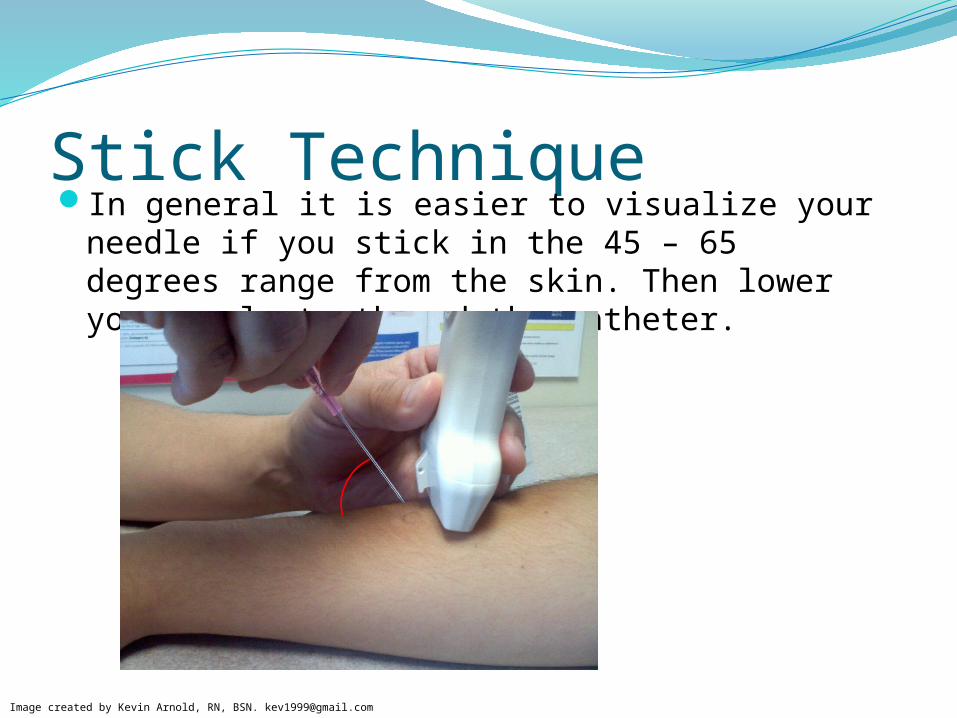
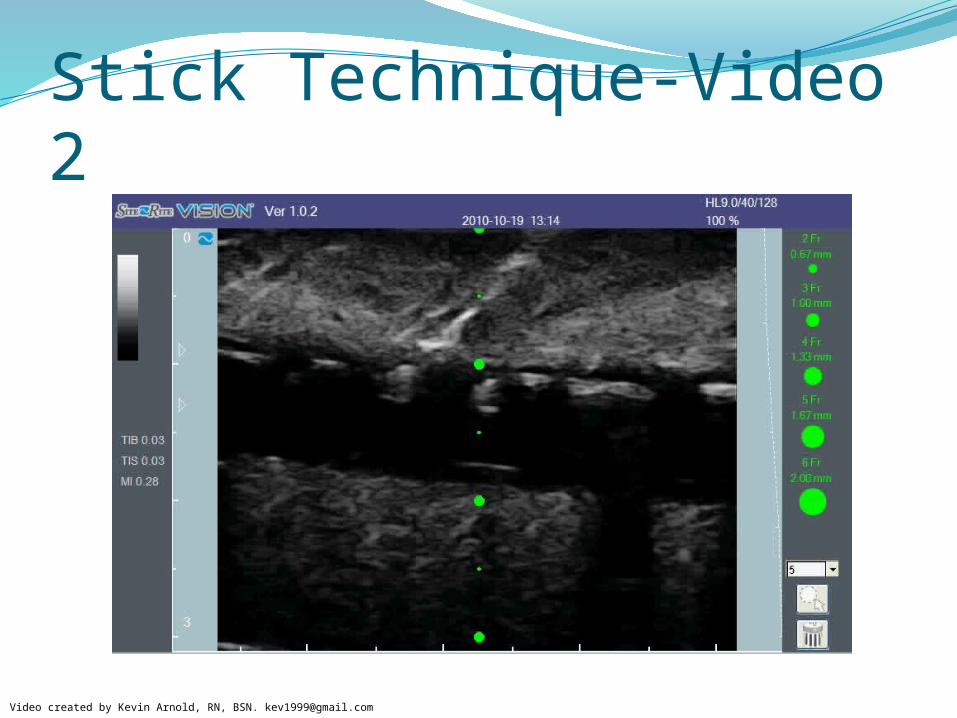
Stick TechniqueIn general it is easier to visualize your needle if you stick in
the 45 – 65 degrees range from the skin. Then lower your angle to thread the catheter.
Image created by Kevin Arnold, RN, BSN. [email protected]
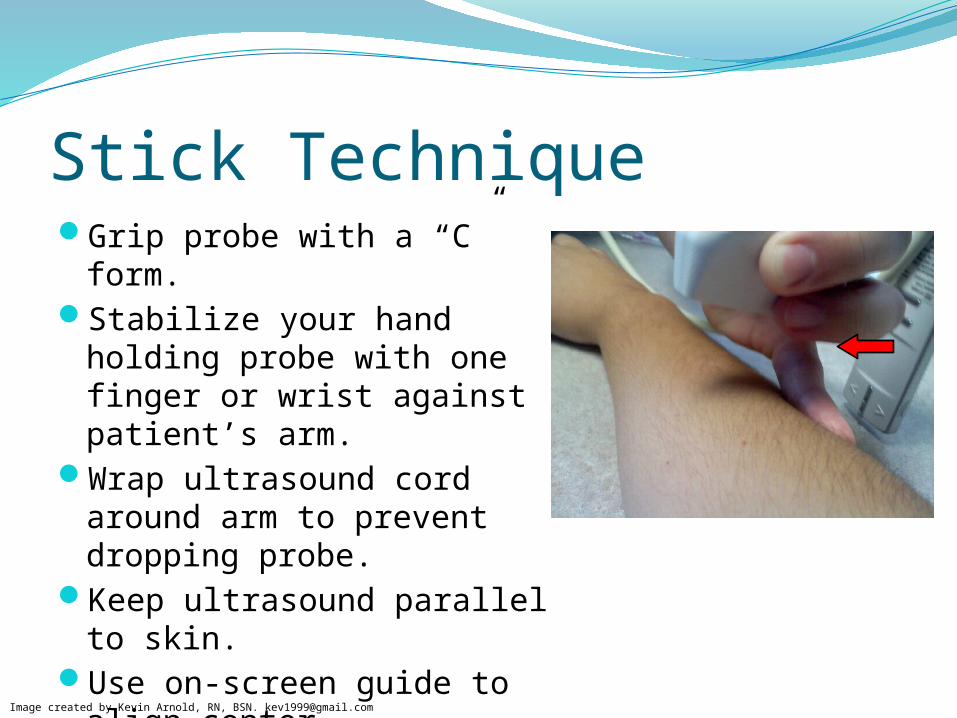
Stick TechniqueGrip probe with a “C” form.Stabilize your hand holding probe
with one finger or wrist against patient’s arm.
Wrap ultrasound cord around arm to prevent dropping probe.
Keep ultrasound parallel to skin.Use on-screen guide to align
center.
Image created by Kevin Arnold, RN, BSN. [email protected]
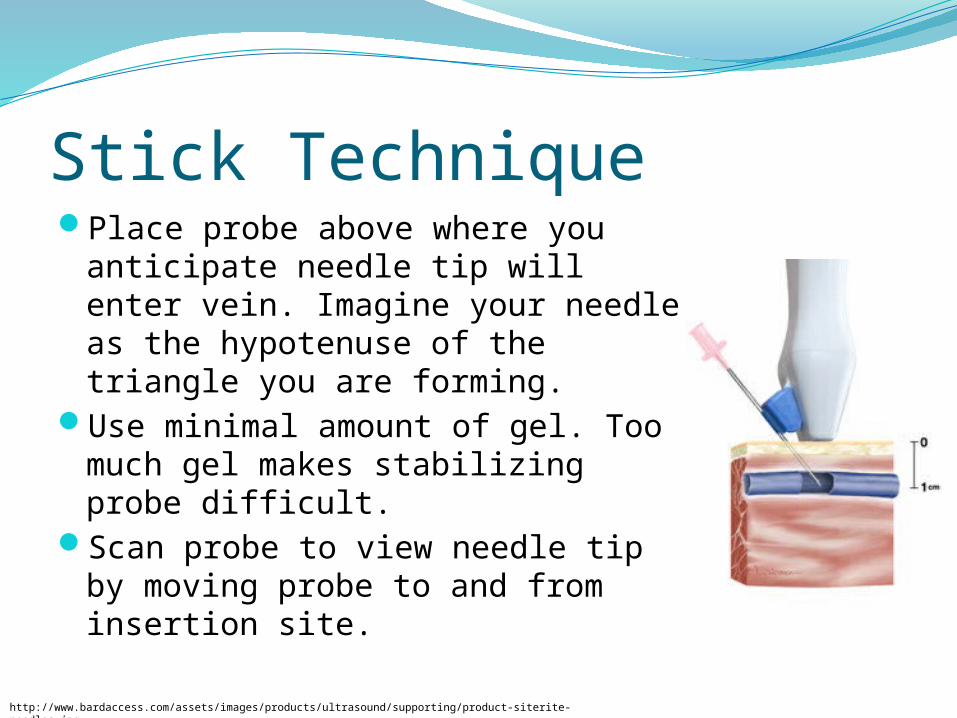
Stick TechniquePlace probe above where you anticipate
needle tip will enter vein. Imagine your needle as the hypotenuse of the triangle you are forming.
Use minimal amount of gel. Too much gel makes stabilizing probe difficult.
Scan probe to view needle tip by moving probe to and from insertion site.
http://www.bardaccess.com/assets/images/products/ultrasound/supporting/product-siterite-needles.jpg
Stick TechniqueYou may inadvertently stick through both sides of vein wall. If
so, you should see and feel the vein wall “pop” into place when retracting the needle out of the deeper side of the vein wall.
You should have excellent blood flow when tip is in the middle of the vein.
After visualizing tip of needle in center of vein, it is okay to lessen the angle of the needle as you begin to thread the catheter.
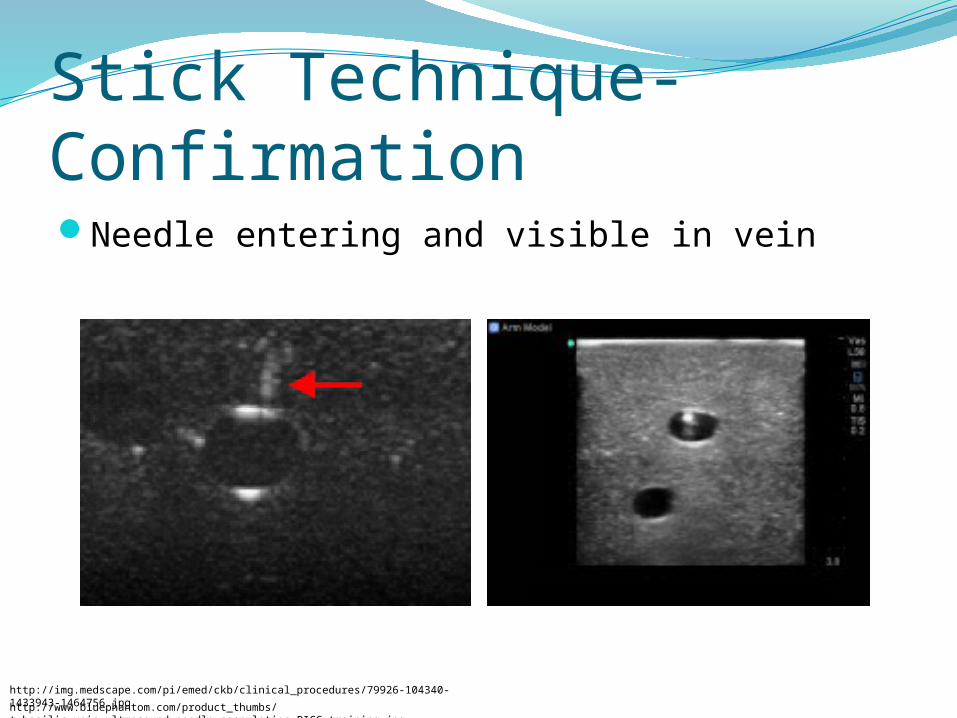
Stick Technique-ConfirmationNeedle entering and visible in vein
http://www.bluephantom.com/product_thumbs/t_basilic_vein_ultrasound_needle_cannulation_PICC_training.jpg
http://img.medscape.com/pi/emed/ckb/clinical_procedures/79926-104340-1433943-1464756.jpg
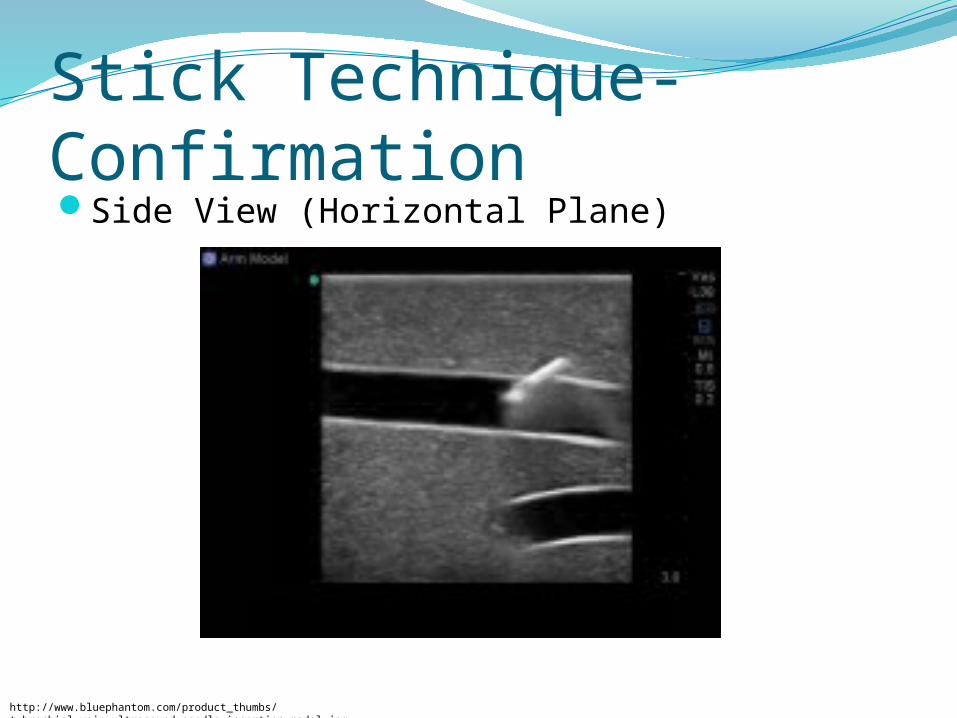
Stick Technique-ConfirmationSide View (Horizontal Plane)
http://www.bluephantom.com/product_thumbs/t_brachial_vein_ultrasound_needle_insertion_model.jpg
Potential ComplicationsArterial punctureAdjacent nerve damageInfiltrationInfection – local & systemicPotential DVT induced by repeated injury to vessel or the
presence of a catheterInjury to vessel preventing arterio-venous fistulas sites
for renal patients
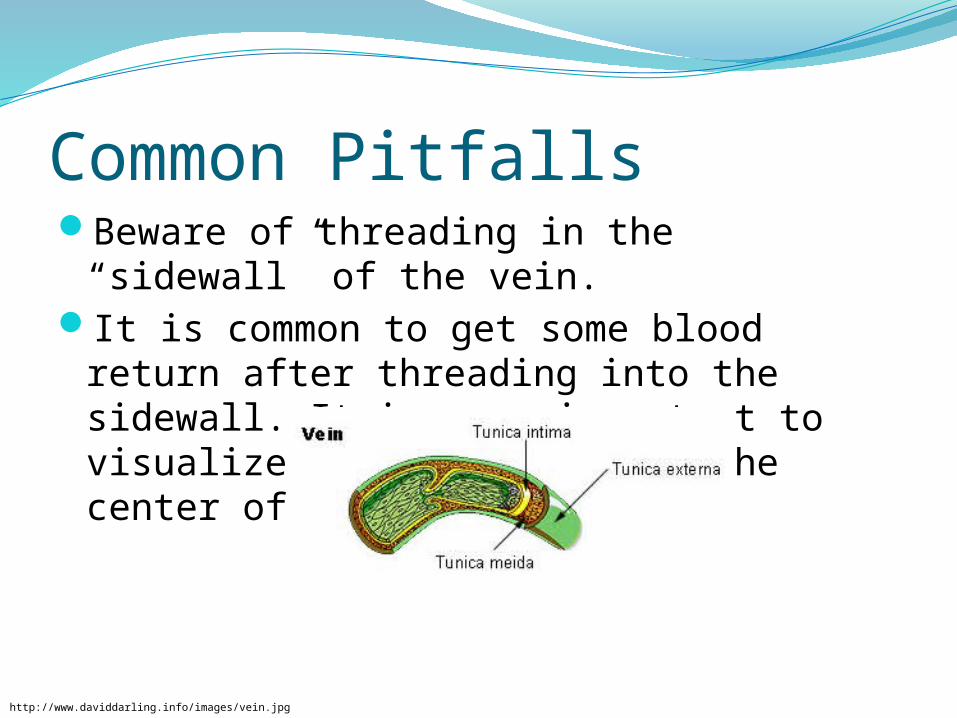
Common PitfallsBeware of threading in the “sidewall” of the vein.It is common to get some blood return after
threading into the sidewall. It is very important to visualize the needle tip in the center of the vein opening.
http://www.daviddarling.info/images/vein.jpg

Common PitfallsMy needle is under the skin but I cant see the tip?
After needle insertion, make sure the probe is directly above the insertion area.
Move the probe closer to the insertion site and scan outward
You may be too deep. Look for movement below vein
I buried my needle and I still can’t reach the vein?Retract and advance at a steeper angle, but make sure to
allow sufficient catheter length left for in the vein. Infiltration is likely if catheter is too short.
Common RemindersYou will constantly have to remind students:
Keep your eyes on the screen…not the insertion area.Stick steeper…steeper is much easier.Don’t hover over patient with needle…just stick quickly
through skin and then use the screen to guide the needle.Use your wrist/finger to stabilize your probe hand…free
handing the probe will allow too much movement.
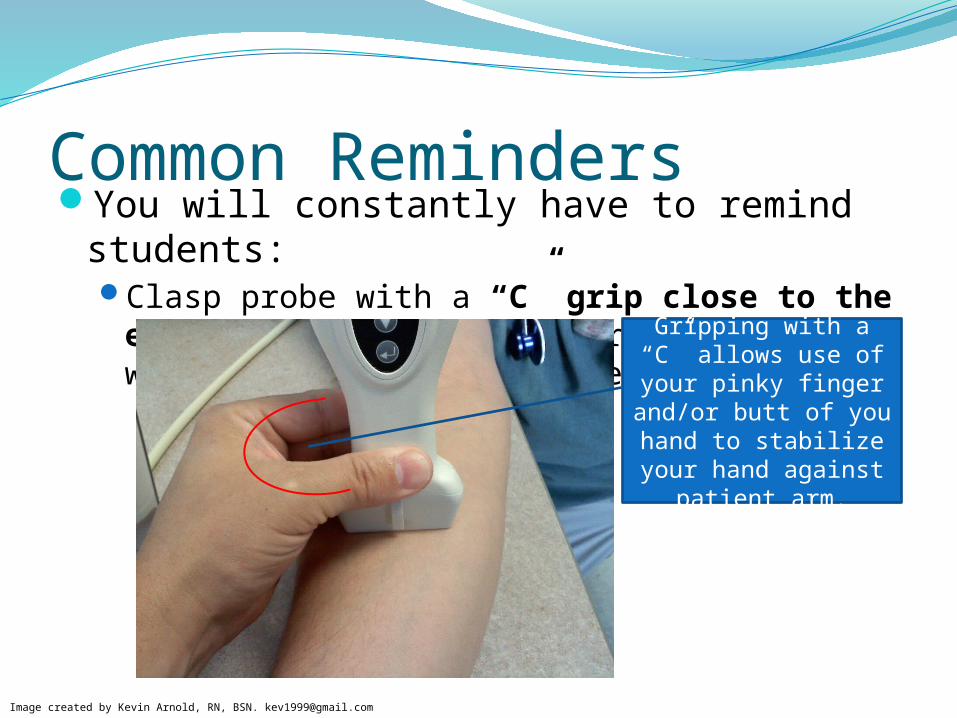
Common RemindersYou will constantly have to remind students:
Clasp probe with a “C” grip close to the end… holding the probe far from the end will allow too much movement.
Image created by Kevin Arnold, RN, BSN. [email protected]
Gripping with a “C” allows use of your pinky finger
and/or butt of you hand to stabilize your hand against
patient arm.
DocumentationDocument IV site location and preparation, gauge of
catheter, number of attempts, and type of dressing in the medical record.
Use of Ultrasound for guidance should be included in note.
Questions? Call…Kevin Arnold RN, BSN PICC RN, VA – Long Beach Medicine & Inpatient Healthcare Group | Spinal Cord Injury | Community Living Center
Bldg 126, 562.826.8000 Ext 5827Pager: 562.683.1200











![Finale 2008a - [Untitled1] › ... · B?? # # # ## ### ### # ## ## # # # # # # # # # # # # # # # Picc. Fl. Ob. E. Hn. Bb Cl. B.Cl. Bsn. Hn. I,II Hn. III,IV C Tpt. I,II C Tpt. III](https://img.pdfslide.us/doc/110x75/5f0f1df37e708231d44292f6/finale-2008a-untitled1-a-b-.jpg)
![Brain MusicTubular-Bells (soft beaters) div.-2 a nonensong Ma) Foxtrott-Tempo 126 (org. 92)] Picc. Bsn. C-Bsn. B-CI. Cb-C1. Alt-Sax. T-Sax. Bar-Sax. (org. 92)] Euph. Tuba arco Str](https://img.pdfslide.us/doc/110x75/6039dc7073a3200ee41fd1fd/brain-tubular-bells-soft-beaters-div-2-a-nonensong-ma-foxtrott-tempo-126-org.jpg)