Embed Size (px)
Citation preview

KERATOPROSTHESIS WITH A PLASTIC FIBER MESHWORK SUPPORTING PLATE
REPORT OF AN EXPERIMENTAL AND COMPARATIVE HISTOLOGIC STUDY
HERNANDO CARDONA, M.D. New York
The densely vascularized, granular cornea responds poorly to almost any type of re-parative surgery, especially if it results from a chemical burn (lye). In prosthokera-toplasty, the situation is not much better since this operation has a high extrusion rate due to corneal erosion around the implant. When this occurs, additional operations are required in an effort to save the prosthesis but its ultimate extrusion is often inevitable. However, long-term retention of the acrylic keratoprosthesis has been observed in eyes with a good collagen fiber framework.1'2
Clinical observations have demonstrated that extrusion of the prosthesis is the result of thinning and erosion of the corneal stro-ma above and around the implant. Since this seemed to be caused by poor nutrition and dehydration of the cornea, an earlier attempt was made to correct this situation by reducing the size and amount of plastic material of the supporting plate.3 So far, this has failed to improve the retention rate of implants in devitalized corneas. Therefore, a search was made for a material that would allow free diffusion of fluids across these corneas and, at the same time, serve as an effective support for the implant. This paper reports the experimental observations and histologic results of tissue tolerance to several synthetic fibers.
MATERIAL AND METHODS
Seven synthetic fibers of the type used as suturing material in vascular surgery were
From the Corneal Center, Department of Ophthalmology, College of Physicians and Surgeons. This study was supported in part by grant No. NB-04968-03 from the National Institutes of Health, Bethesda, Maryland, and by a Fight for Sight grant-in-aid from the National Council to Combat Blindness, New York.
tested: Dacron (DuPont), Teflon (Du-Pont), siliconized Teflon (DuPont), Silastic (Dow Corning), fiber glass, nylon and cellulose. The basic design of the keratoprosthesis was the same for each fiber with an anterior projection of pure methyl methacrylate 2.0 mm in diameter and a posterior projection of the same pure plastic material, also 2.0 mm in diameter (fig. 1-A and B) . The interlamellar supporting plate, of a fiber meshwork, measured 5.5 mm in diameter and was 0.15-mm thick (fig. 1-C). The walls of the optical cylinder contained a thin layer of pigment to reduce light reflection. This was held in place by a thin layer of pure methyl methacrylate, as shown in Figure 1-D and P.
Seventy albino rabbits weighing about 3.5 kg each were used; 10 for each fiber tested. The test animals were killed at regular intervals beginning one month after insertion or upon extrusion of the keratoprosthesis. The eye was then enucleated and prepared for histologic study. Some rabbits from each group were maintained for microscopic study of the eye until extrusion of the implant or what was deemed sufficient time to determine that retention would probably be permanent in view of the good tolerance. A few animals are still under observation one year after implantation with no tendency to extrusion of the keratoprosthesis.
SURGICAL TECHNIQUE
General anesthesia was induced with sodium pentothal supplemented with ether. A 5.0-mm paracentral incision was made through the anterior two thirds of the corneal layers and an interlamellar pocket dissected. A 2.0-mm trephine, especially designed for this purpose, was used to perforate the corneas centrally. The keratopros-
228

VOL. 64, NO. 2 KERATOPROSTHESIS 229
thesis was introduced into this interlamellar pocket with the optical cylinder engaging the trephine perforations. The incision was closed with 8-0 silk sutures.
RESULTS
Dacron. Best results were obtained with the Dacron interlamellar supporting plate. Vascularization was minimal (fig. 2-A and B). The corneal tissue over the meshwork plate remained clear. None of the kerato-prostheses in this series of test animals extruded. Some of these eyes have now been under observation for one year and the corneal tissue over the implant is still transparent (fig. 2-B).
Teflon. Tolerance to the Teflon meshwork plate was good but, as a result of oxidation and macroscopically visible hydra-tion, the fiber showed signs of degradation, readily discernible through the transparent corneal tissue (fig. 2-C and D) . Some of these rabbits have been under postoperative observation for 11 months with no extrusions of the implant. The progressive degradation of the inferior surface of the interlamellar supporting plate is shown in Figure 2-D.
Siliconized Teflon. In view of the degradation and loss of tensile strength observed in the Teflon meshwork supporting plates, the test was repeated in 10 additional rabbits, using siliconized Teflon. Results with this fiber when it was siliconized were as good as those obtained with Dacron (fig. 2-A and B) and even better.
Silastic. This material was perforated to form a meshwork from which the interlamellar supporting plates were then fashioned. Tolerance and tissue reaction were similar to those observed with Dacron. Some of these eyes have been under observation for 11 months with no extrusions of the implant. However, the material is soft and requires excessive handling during insertion of the keratoprosthesis, which naturally complicates the surgical procedure.
Fiber glass. The eyes with a supporting plate of fiber glass developed pronounced corneal vascularization with subsequent ulcération and opacincation during the third postoperative week. Extrusion of the implants followed.
Nylon. Tolerance in this series of eyes was good for the first three postoperative months, after which the corneas vascular-
Fig. 1 (Cardona). Cross-section of Cardona through-and-through keratoprosthesis with meshwork supporting plate, showing dimensions in mm. (A) Anterior projection of the optical cylinder. (B) Posterior projection of the optical cylinder. (C) Synthetic fiber meshwork supporting plate. (D) Narrow ring of solid plastic fiber to prevent leakage. (P) Pigment.

230 AMERICAN JOURNAL OF OPHTHALMOLOGY AUGUST, 1967
Fig. 2 (Cardona). Photographs of rabbit eyes comparing the reaction to siliconized and nonsiliconized Teflon. (A and B) Keratoprosthesis with siliconized Teflon meshwork supporting plate. Results at 11 months. The fiber retains its structure and pattern with practically no reaction. The eye appears quiet (C) Supporting plate of nonsiliconized Teflon. Some blood vessels are visible, entering from the periphery toward the center of the cornea four months after the operation. (D) The same rabbit at 11 months. The blood vessels have disappeared. There is no visible reaction and the prosthesis appears to be well tolerated but the fiber has deteriorated.
ized, followed by opacification. Three of the 10 keratoprostheses had extruded by the end of the third postoperative month.
Cellulose. There was some reaction in these eyes, with corneal vascularization, ulcération and opacification over the keratoprosthesis at the end of the third postoperative month. Five of the 10 implants had extruded by the end of the seventh month.
HISTOLOGY
Siliconized Teflon. Gross appearance. Three months after the operation the collagen fibers maintained their normal structure with no discernible tissue reaction. No blood vessels were evident nor was there any opacification of the stroma (fig. 2-A). At 11 months only one blood vessel was visible, invading the cornea from the periphery (fig.
2-B) but there was still practically no tissue reaction.
Microscopic appearance. The meshwork pattern of this fiber could not be visualized in histologie sections of eyes from rabbits killed at 10 months. Tolerance to the fiber was even more pronounced. This fact was deemed of particular importance in the selection of the material to be used to fashion the meshwork supporting plate of the keratoprostheses for the clinical trial. The epithelium was intact. The synthetic fiber and a few epithelial cells were visible in the cornea and stroma. There were no giant cells. The plastic fibers could be clearly demonstrated by means of polarized light.
Teflon. Gross appearance. Some blood vessels invaded the cornea from the periphery but they disappeared at 10 months to
VOL. 64, NO. 2 KERATOPROSTHESIS 231
one year. The meshwork supporting plate, which at first appeared intact after observation periods ranging from eight to 12 months, began to lose its architectural structure and the pattern deteriorated as the result of oxidation and hydration (fig. 2-C).
Microscopic examination revealed degradation of the fiber, which appeared powderlike between the corneal layers where it was well tolerated. This degradation was easily overcome by siliconizing the Teflon fiber (fig. 2 -AandB) .
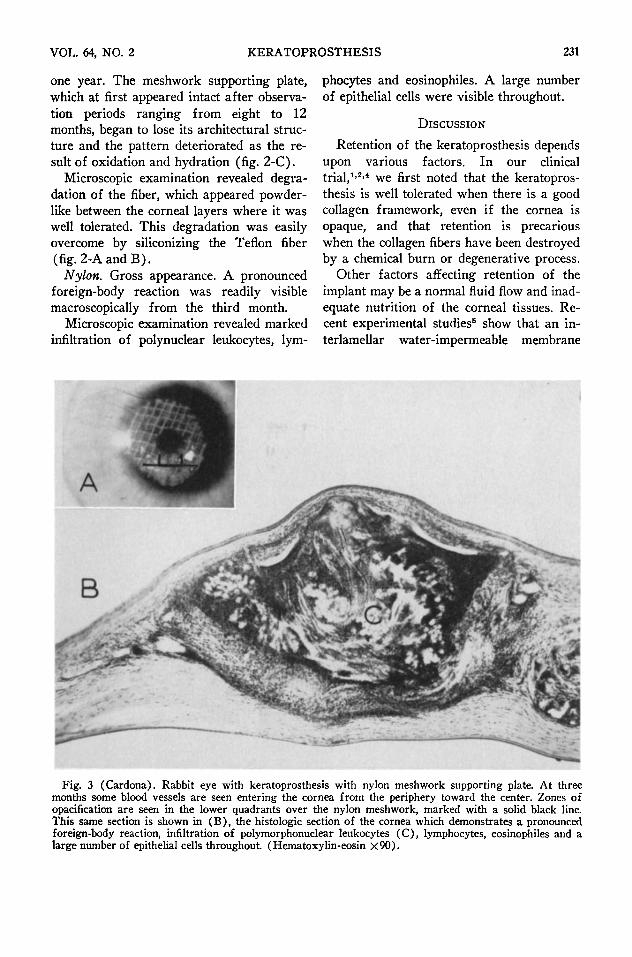
Nylon. Gross appearance. A pronounced foreign-body reaction was readily visible macroscopically from the third month.
Microscopic examination revealed marked infiltration of polynuclear leukocytes, lym
phocytes and eosinophiles. A large number of epithelial cells were visible throughout.
DISCUSSION
Retention of the keratoprosthesis depends upon various factors. In our clinical trial,1·2'4 we first noted that the keratoprosthesis is well tolerated when there is a good collagen framework, even if the cornea is opaque, and that retention is precarious when the collagen fibers have been destroyed by a chemical burn or degenerative process.
Other factors affecting retention of the implant may be a normal fluid flow and inadequate nutrition of the corneal tissues. Recent experimental studies5 show that an in-terlamellar water-impermeable membrane
Fig. 3 (Cardona). Rabbit eye with keratoprosthesis with nylon meshwork supporting plate. At three months some blood vessels are seen entering the cornea from the periphery toward the center. Zones of opacification are seen in the lower quadrants over the nylon meshwork, marked with a solid black line. This same section is shown in (B), the histologie section of the cornea which demonstrates a pronounced foreign-body reaction, infiltration of polymorphonuclear leukocytes (C), lymphocytes, eosinophiles and a large number of epithelial cells throughout. (Hematoxylin-eosin X90).

232 AMERICAN JOURNAL OF OPHTHALMOLOGY AUGUST, 1967
ΐ " ι · .~ .*Ό* -, β ; * " * * * Η ^ " -*-»H!i&***.*s*i.#itVä&aK*A-!>^%v ν*,*ν:Χ;
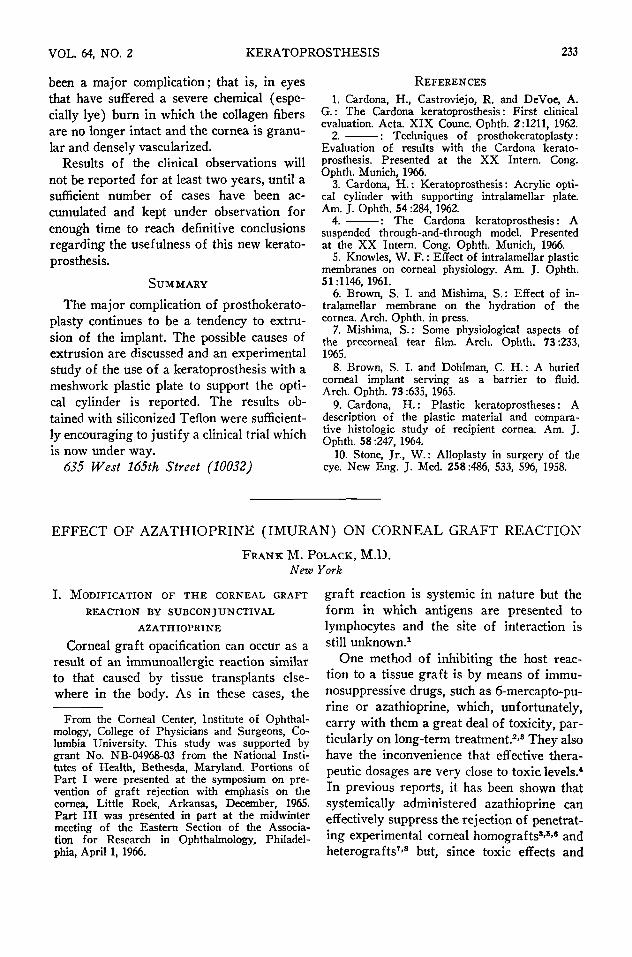
Fig. 4 (Cardona). (A) Rabbit eye with keratoprosthesis with siliconized Teflon meshwork supporting plates 10 months after insertion. There is practically no reaction in the upper half, marked with a solid black line over the meshwork, which corresponds to the histologie section (B), which shows perfect tolerance to the fiber. There is no infiltration of the surrounding stroma. The collagen fibers, epithelium and endothelium are practically intact. (Hematoxylin-eosin χ60).
inhibits the passage of fluids across the cornea, which could diminish the nutrition of the tissue anterior to the membrane, while a physiologic study of tears and the effect of interlamellar membranes on the movement of corneal fluid demonstrated that the evaporation of water from the corneal surface and subsequent changes in the composition of the tears enhance dehydration of the anterior layers.8-7 This excessive dehydration in turn leads to degeneration of the corneal tissue, as would inadequate nutrition.
When a solid plastic plate is used to support the optical cylinder of the keratoprosthesis, erosion of the host corneal tissue is frequently observed around the lower half of the optical cylinder and rarely around the upper half where the lid affords protection, maintaining the tissues moist or wet.8-8 This definite pattern of erosion may be explained by the fluid flow just described. Thus, it
seemed desirable to support the optical cylinder of the prosthesis with a structure that would permit the fluid and nutritional substances to diffuse to the anterior layer of the cornea. Stone10 advocates perforation of the interlamellar supporting plate.
In view of these considerations, a keratoprosthesis was designed with an improved system to support the optical cylinder and to serve the following purposes: (1) permit the free passage of fluids, (2) provide flexibility allowing adaptation to the corneal curvature and (3) assume the role of the damaged or destroyed collagen fibers.
The results of these experiments justified the continuation of clinical trials begun in 1962, using the keratoprosthesis with a meshwork supporting plate of siliconized Teflon. This material is now being used in unfavorable human eyes of the type in which extrusion of the original implant has
VOL. 64, NO. 2 KERATOPROSTHESIS 233
been a major complication; that is, in eyes that have suffered a severe chemical (especially lye) burn in which the collagen fibers are no longer intact and the cornea is granular and densely vascularized.
Results of the clinical observations will not be reported for at least two years, until a sufficient number of cases have been accumulated and kept under observation for enough time to reach definitive conclusions regarding the usefulness of this new kerato-prosthesis.
SUMMARY
The major complication of prosthokerato-plasty continues to be a tendency to extrusion of the implant. The possible causes of extrusion are discussed and an experimental study of the use of a keratoprosthesis with a meshwork plastic plate to support the optical cylinder is reported. The results obtained with siliconized Teflon were sufficiently encouraging to justify a clinical trial which is now under way.
635 West 165th Street (10032)
REFERENCES 1. Cardona, H., Castroviejo, R. and DeVoe, A.
G. : The Cardona keratoprosthesis : First clinical evaluation. Acta. XIX Counc. Ophth. 2:1211, 1962.
2. : Techniques of prosthokeratoplasty : Evaluation of results with the Cardona keratoprosthesis. Presented at the XX Intern. Cong. Ophth. Munich, 1966.
3. Cardona, H. : Keratoprosthesis : Acrylic optical cylinder with supporting intralamellar plate. Am. J. Ophth. 54:284, 1962.
4. : The Cardona keratoprosthesis: A suspended through-and-through model. Presented at the XX Intern. Cong. Ophth. Munich, 1966.
5. Knowles, W. F. : Effect of intralamellar plastic membranes on corneal physiology. Am. J. Ophth. 51:1146, 1961.
6. Brown, S. I. and Mishima, S. : Effect of intralamellar membrane on the hydration of the cornea. Arch. Ophth. in press.
7. Mishima, S. : Some physiological aspects of the precorneal tear film. Arch. Ophth. 73:233, 196S.
8. Brown, S. I. and Dohlman, C. H. : A buried corneal implant serving as a barrier to fluid. Arch. Ophth. 73:635, 1965.
9. Cardona, H. : Plastic keratoprostheses : A description of the plastic material and comparative histologie study of recipient cornea. Am. J. Ophth. 58:247, 1964.
10. Stone, Jr., W. : Alloplasty in surgery of the eye. New Eng. J. Med. 258:486, 533, 596, 1958.
EFFECT O F AZATHIOPRINE (IMURAN) ON CORNEAL GRAFT REACTION
FRANK M. POLACK, M.D. New York
I. MODIFICATION OF THE CORNEAL GRAFT REACTION BY SUBCONJUNCTIVAL
AZATHIOPRINE
Corneal graft opacification can occur as a result of an immunoallergic reaction similar to that caused by tissue transplants elsewhere in the body. As in these cases, the
From the Corneal Center, Institute of Ophthalmology, College of Physicians and Surgeons, Columbia University. This study was supported by grant No. NB-04968-03 from the National Institutes of Health, Bethesda, Maryland. Portions of Part I were presented at the symposium on prevention of graft rejection with emphasis on the cornea, Little Rock, Arkansas, December, 1965. Part III was presented in part at the midwinter meeting of the Eastern Section of the Association for Research in Ophthalmology, Philadelphia, April 1, 1966.
graft reaction is systemic in nature but the form in which antigens are presented to lymphocytes and the site of interaction is still unknown.1
One method of inhibiting the host reaction to a tissue graft is by means of immu-nosuppressive drugs, such as 6-mercapto-pu-rine or azathioprine, which, unfortunately, carry with them a great deal of toxicity, particularly on long-term treatment.2-3 They also have the inconvenience that effective therapeutic dosages are very close to toxic levels.* In previous reports, it has been shown that systemically administered azathioprine can effectively suppress the rejection of penetrating experimental corneal homografts8·5-6 and heterografts7'8 but, since toxic effects and