Embed Size (px)
Citation preview

[CANCER RESEARCH 45, 841-846, February 1985]
Keratin Expression in Normal Esophageal Epithelium and Squamous CellCarcinoma of the Esophagus1
Michael P. Grace,2 Kwan Hee Kim,3 Lawrence D. True, and Elaine Fuchs4
Department oÃBiochemistry, The University of Chicago, Chicago, Illinois 60637 [M. P. G., K. H. K., E. F.], and the Department of Pathology, Yale University,New Haven, Connecticut 06510 [L. D. T.]
ABSTRACT
The 8-nm keratin filament is a major component of the cyto-skeleton of epithelial cells and epithelial-derived cancers (carci
nomas). Recently, it has been shown that the pattern of keratinsproduced by an esophageal epithelial cell undergoes changeupon malignant transformation. In order to evaluate the potentialimportance of these differences in providing improved diagnostictechniques for pathology, we have investigated the consistencyof the patterns of keratins expressed in normal esophagealepithelium, squamous cell carcinoma (SQCC) of the esophagus,and cultured esophageal epithelial cells. In six patients, thekeratin pattern expressed by SQCC of the esophagus andcorresponding normal esophageal epithelium was consistentlydifferent as judged by immunoblot analysis of electrophoreticallyseparated protein extracts. Whereas the SQCCs typically expressed major keratins with molecular weights of 58,000,56,000, 50,000, and 46,000, the normal esophageal epitheliumproduced two major keratins with molecular weights of 58,000and 52,000 and a minor keratin with a molecular weight of56,000. When normal esophageal epithelial cells were grown intissue culture, their keratin pattern changed, and keratins withmolecular weights of 58,000, 56,000, 52,000, 50,000, 46,000,and 40,000 were expressed. Although some minor variations inkeratin patterns were seen, the major differences in keratinpattern expressed by normal esophageal epithelial tissue, SQCCof the esophagus, and cultured esophageal cells were consistentand reproducible.
INTRODUCTION
There will be an estimated 9000 new cases of esophagealcancer in the United States in 1984. Although this cancer accounts for only 1.5% of all cancers, it will be responsible for8600 deaths (33). The most common symptom, dysphagia,develops when the primary tumor is already an advanced lesionand has compromised one-half to two-thirds of the esophageallumen. There are no "early warning" symptoms or signs. In
addition, 90% of patients are found to have metastatic diseaseat autopsy (31). Patients with esophageal achalasia are at ahigher risk than the general population for developing esophagealcarcinoma (39). Despite advances in surgery and radiation therapy, the 5-year survival for esophageal cancer continues to be
1Supported in part by Grant RO1 AM31737 from the NIH.2 Recipient of a Damon Runyon-Walter Winchell Cancer Fund Fellowship, DRG-
018. Present address: Department of Hematology-Oncology, The University of
Connecticut Health Center, Farmington, CT 06032.3 Recipient of a postdoctoral fellowship from the National Cancer Institute.' Recipient of a Searle Scholar Fellowship, an NSF Presidential Young Investi
gator Award, and a NIH Career Development Award. To whom requests for reprintsshould be addressed.
Received June 4, 1984; accepted October 26, 1984.
less than 10% in most series (5, 37). Similarly, the objectiveresponse to chemotherapeutic agents such as c/'s-platinum and
bleomycin is only in the order of 20% or less, with responseslasting only 2 to 3 months (31). Patients die of pulmonaryaspiration or inanition following recurrent locoregional disease ormetastasis.
Squamous cell carcinoma accounts for 90% of esophagealcancers. SQCC5 of the esophagus is graded according to the
degree of histological differentiation. The well-differentiated and
moderately differentiated tumors display morphological featuresgenerally characteristic of normal epithelial differentiation (25). InSQCCs, these features include intercellular bridge formation andkeratinization manifested by dyskeratosis and squamous pearlformation. Biochemical alterations that accompany changes inmorphology are just beginning to be explored in this disease.Such molecular differences could be useful in the early detectionof SQCC of the esophagus.
Since keratins are a major constituent of the esophagealepithelium, they were chosen as a focal point for investigatingthe possible biochemical changes that may arise during thetransition from the stratified squamous epithelial lining of theesophageal lumen to SQCC of the esophagus. The humankeratins are a family of about 20 related proteins (M, 40,000 to70,000) that polymerize to form 8- to 10-nm-diameter cyto-
plasmic filaments in most if not all epithelial cells (for a review,see Ref. 20). Usually, only 2 to 6 keratins are expressed by anindividual cell. Variability in expression of different keratins isrelated to species, cell type, state of cellular differentiation, andextracellular factors. Keratins continue to be expressed in epithelial-derived cancers (carcinomas) (21, 29, 41).
Several laboratories have recently described alterations in thepattern of keratin expression in human esophageal epitheliumwhen compared to SQCC of the esophagus (1, 2, 21). In thisreport, we further biochemically define the consistency of thesealterations. We relate our findings to the potential of a biochemical approach to cancer detection of a cancer that expresses adifferent keratin pattern than its tissue of origin.
MATERIALS ANO METHODS
Tissue Collection. Six samples of esophageal carcinoma (histologi-cally confirmed as SQCC) and 6 samples of adjacent normal esophagealepithelium from 6 different patients were obtained from resected surgicalspecimens immediately after operation. Four samples of normal esophageal epithelium were obtained from surgical specimens of patientsoperated for reasons other than esophageal carcinoma. Three sampleswere obtained at autopsy.
Cell Culture. One sample of esophageal epithelium was minced finelyand prepared for culture according to the method of Rheinwald (27).
5The abbreviations used are: SQCC, squamous cell carcinoma; TioE10 buffer,
10 mm Tris:10 rriM EDTA (pH 7.6).
CANCER RESEARCH VOL. 45 FEBRUARY 1985
841
on July 31, 2020. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

KERATIN IN HUMAN ESOPHAGEAL SQCC
Cells were cultured in the presence of lethally mitomycin C-treated mouse3T3-fibroblasts in a 3:1 mixture of Dulbecco's modified Eagle's mediumand Ham's Medium F-12 (40), supplemented with 10% fetal calf serum,
hydrocortisone (0.4 ^g/ml), 0.1 nM cholera toxin, 20 pM triiodothyronine,human transferrin (5 Mg/ml), insulin (5 M9/ml) (3, 19), and epidermalgrowth factor (4 ng/ml) (30). The medium was changed every 3 to 4
days.Extraction of Keratins. Esophageal epithelium was separated from
underlying connective tissue by sharp and blunt dissection. Esophagealepithelium and cancer samples were each cut into 3- x 3-mm pieces,
placed in liquid N2, and ground into a powder. The powder was suspended in 5 ml of T10E10buffer containing 0.1% phenylmethylsulfonylfluoride (Sigma) and homogenized (10). The homogenate was centrifugedat 12,000 x g for 10 min at 4°.The pellet was washed 5 times in Ti0Ei0
buffer. Water-insoluble proteins were resuspended in 8 M urea:10% 2-
mercaptoethanol with the aid of sonication, followed by incubation at37°.
For extraction of keratins from cultured esophageal epithelial cells, theprimary culture and first and second subcultures were harvested when75% confluent. The 3T3 fibroblasts were selectively removed usingEDTA, and the remaining cells were scraped into 5 ml of T10E10buffer.The procedure for isolation of the keratins was identical to that described
above.Antibody Specificity. Antibodies specific for (a) keratins of cultured
human epidermal cells (M, 46,000 to 58,000) and (b) the gel-purified M,40,000 keratin of SCC-15, a cell line of SQCC of the tongue (29), were
raised in New Zealand White rabbits. A mixture of antisera was used forall immunoblot analyses. This mixture showed cross-reactivity with all
keratins of M, 40,000 to 58,000, with slightly stronger reactivity to theM, 50,000 and 56,000 keratins.
Immunoblot Analysis (Western Blot). Proteins were resolved bysodium dodecyl sulfate: polyacrylamide gel electrophoresis and transferred electrophoretically to nitrocellulose paper (4). The paper wasincubated at 37° for 2 hr in a solution of 5% bovine serum albumin
(Fraction V; Sigma), 0.9% NaCI solution (saline) containing a 1:100dilution of antisera against epidermal keratins, and gel-purified M, 40,000
keratin. The paper was then thoroughly washed in a saline: 10 mwTris:0.1% Triton X-100 solution. The keratins were identified by indirectlabeling of the bound antibody with 125l-labeled Staphylococcus aureus
Protein A (Amersham). Radiolabel was detected by autoradiography.Electrophoresis. Keratins were separated using 8.5% sodium dodecyl
sulfate:polyacrylamide slab gel electrophoresis according to the procedure of Laemmli (18). Gels that were not subjected to immunoblotanalysis were stained with a solution of 0.1% Coomassie blue, 50%methanol, and 10% acetic acid and then destained with a solution of 5%methanol and 10% acetic acid.
Immunofluorescence. Esophageal epithelial cells were grown ondouble-chamber Lab-Tek slides (Miles). The cultured cells and 5-^m
sections of esophageal tissue and SQCC of the esophagus were fixedin methanol (-20°) for 5 min. This was followed by incubation at 37°for
30 min with specific rabbit antiserum against human epidermal keratin(1:50 dilution) and then by incubation at 37°for 20 min with fluorescence-
conjugated goat anti-rabbit IgG (Miles; 1:20 dilution).
RESULTS
Previously, we demonstrated that an antiserum preparedagainst total keratins from cultured cells showed general cross-
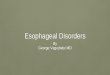
reactivity with all the keratins of cultured basal epidermal cellsand of differentiating epidermis (12, 17). When this antiserumwas incubated with normal human esophageal tissue, it reactedstrongly with all of the cells of the epithelial layer, but not withcells of the subepithelial connective tissue (Fig. 1a). With the useof this antikeratin antiserum, the invasive cells of an SQCC ofthe esophagus could also be easily distinguished from the sur
rounding smooth muscle and connective tissue (Fig. 1o). Whencells were cultured in vitro from normal esophageal epithelium,they continued to express keratins, as seen by the strongimmunofluorescence of a cultured esophageal colony (Fig. 1c).The surrounding fibroblast feeder layer showed no immunoreac-tivity with the anti-keratin antisera. In the cultured cells, thefilamentous network of the 8-nm keratin fibers was readily ap
parent, further clarifying the specificity of this antiserum in esophageal epithelial cells.
To explore the nature of the keratins synthesized by thesecells, water-insoluble proteins were first extracted from a sample
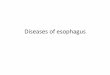
of esophageal tissue and then separated electrophoretically. Thepattern of proteins produced by this sample is shown in Fig. 2a,Lane 1. Major bands with molecular weights of 58,000 and52,000 and a minor band with a molecular weight of 56,000 canbe seen. The pattern of proteins changed significantly whenepithelial cells were cultured in vitro (Fig. 2a, Lane 2). The M,52,000 band diminished, and the M, 56,000 band increased inintensity. In addition, prominent new bands (M, 50,000 and46,000) appeared. With successive subculturing, the M, 40,000band became more pronounced (Fig. 2a, Lanes 3 and 4). Interestingly, this pattern was very similar to that produced by anSQCC of the esophagus (Fig. 2a, Lane 5), which in turn wassimilar to the pattern produced by a cultured SQCC of the tongue(Fig. 2a, Lane 6) (41).
The protein bands observed in Fig. 2a cross-reacted stronglywith the antisera against keratins of cultured human epidermalcells (Fig. 2b). The pattern of keratins seen by immunoblotanalysis was very similar to that visualized by Coomassie bluestaining, with the exception that the M, 50,000 and 56,000keratins cross-reacted somewhat more strongly with the antisera
than did the other keratins. Since this method was more specificand more sensitive for the keratins, it was chosen for subsequentanalyses.
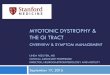
To determine the consistency of the patterns of keratinsproduced by esophageal SQCCs and normal esophageal epithelium, we examined the keratins synthesized by 6 samples ofcarcinoma and the corresponding normal epithelium obtainedfrom 6 different patients (Fig. 3). Five of 6 samples of SQCC ofthe esophagus produced keratins of M, 58,000, 56,000, 50,000,and 46,000. In one sample (Fig. 3, Lane 5C), the M, 58,000keratin band was weak or absent. In many of the tumor samples,additional keratins could be seen. Three carcinomas produced akeratin with a molecular weight of 52,000 (Fig. 3, Lanes 2C, 3C,and 4C). One expressed a minor keratin with a molecular weightof 40,000 (Fig. 3, Lane 4C). Two other minor bands with molecular weights of 42,000 (Fig. 3, Lanes 2C) and 44,000 (Fig. 3,Lanes 1C and 6C) showed cross-reactivity with the anti-keratin
antisera.Of the 6 esophageal SQCCs, 4 were histologically graded as
moderately differentiated, and 2 were poorly differentiated. Wedid not observe a trend in the variation of keratin pattern betweenthe moderately and poorly differentiated SQCCs of the esophagus.
All 6 samples of corresponding normal esophageal tissueexpressed 3 keratins with molecular weights of 58,000, 56,000,and 52,000. Four of the 6 samples produce low levels of the M,50,000 keratin characteristic of the tumors, but none of thesebiopsies expressed detectable levels of the smaller M, 40,000 to46,000 keratins. Thus, in all of the samples where the SQCC of
CANCER RESEARCH VOL. 45 FEBRUARY 1985
842
on July 31, 2020. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

KERATIN IN HUMAN ESOPHAGEAL SQCC
the esophagus could be compared with the normal esophagealepithelial tissue from the same patient, the keratin pattern wasmarkedly different. Although all of the major differences in keratinpatterns between tumor and normal tissue were constant, minorvariations in these patterns were clearly present.
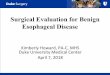
To further explore the frequency of occurrence of these minordifferences, we investigated the keratin patterns of 7 additionalsamples of normal esophageal tissue (Fig. 4). These samples allexpressed the triplet of keratins with molecular weights of58,000, 56,000, and 52,000 that seemed to be characteristic ofnormal esophageal tissue. However, 3 of these new samplesshowed an additional keratin with a molecular weight of 50,000(Fig. 4, Lanes 4 to 6). Its strong immunoreactivity gave no doubtas to its presence in these tissue samples, although the actuallevel of M, 50,000 keratin here was less than that of the M,52,000 keratin. Only one sample showed a keratin with a molecular weight of 46,000 (Fig. 4, Lane 5; patient with hepaticcirrhosis), and this band was extremely weak in relation to otherkeratins expressed. (Compare same lane, lighter exposure atright.) Another atypical keratin pattern included an M, 40,000band (Fig. 4, Lane 6), although the tissue was also unusual inthat it came from a 24-hr-old neonate who had died of congenital
anomalies. In summary, variations in the normal esophagealkeratin pattern could be identified, but these differences werelargely of a minor nature.
DISCUSSION
The reproducible triplet of 3 keratins with molecular weightsof 58,000,56,000, and 52,000 defines normal human esophagealepithelium and seems to be a pattern characteristic of thisepithelium. These results are in good agreement with the previous findings of Banks-Schlegel and Harris (1) and Moll ef a/.
(20). Although the molecular weight values for the 3 keratinsvary among laboratories, the reports are most likely identical,and the 3 keratins have been assigned numbers of 4 (Mr 58,000),6 (M, 56,000), and 13 (Mr 52,000) according to the cataloguesystem of Moll ef al. (20).
Whereas Keratins 4 and 6 remain predominant in tissue samples of SQCC of the esophagus, Keratin 13 is frequently presentin reduced, if detectable, levels (this paper; Refs. 2 and 21). Incontrast, the levels of M, 46,000 (No. 17) and M, 50,000 (Nos.14 and 15) keratins increase substantially in the carcinoma. Of11 samples of normal esophageal tissue, only one (Fig. 4, Lane4) showed relatively high levels of Keratins 14 and 15, and noneproduced large amounts of Keratin 17. Thus, these changes inkeratin synthesis seem to be consistent biochemical differencesbetween the normal epithelium and SQCC of the esophagus.
Our finding that the levels of M, 50,000 and M, 46,000 keratinsare usually elevated in esophageal carcinomas is in good agreement with that of Moll ef al. (21), who reported an increase inthe level of Keratin 14 (M, 50,000) for one type of SQCC of theesophagus and an increase in Keratin 15 (M, 50,000) for another.Consistent with our results, both types of SQCC of the esophagus produced large amounts of Keratin 17 (M, 46,000). Theseobservations differ from those of Banks-Schlegel and Harris (2),
who reported no change in keratins with molecular weights of46,000 to 50,500 as judged by anti-keratin immunoprecipitation
of proteins extracted from normal and tumor tissues. It is possible, however, that the distortion of the electrophoretic migration
of the keratins caused by the large amounts of immunoglobulin(M, 50,000) in the precipitates described in that study maskedthese differences in keratin levels.
Whereas the pattern of keratins produced by normal esophageal epithelium differs considerably from that of other humanepithelia, e.g., epidermis, tongue, and bronchus, the patternproduced by SQCC of the esophagus is largely indistinguishablefrom that produced by SQCCs arising in other organs (Refs. 21and 23; Footnote 6). The disappearance of differences in keratinpatterns also takes place in cells cultured from various rabbitand human epithelia (7,40). In the present study, we have shownthat 4 major keratins (M, 46,000, 50,000, 56,000, and 58,000)are produced by cultured human esophageal cells. This patternis very similar to that produced by cultured human epidermal,corneal, and conjunctival cells (35) and supports similar findingsrecently reported by Banks-Schlegel and Harris (1) and Wu ef al.
(40).We have shown that this in vitro pattern appears shortly after
placing the esophageal cells in culture and is maintained throughsuccessive subculturings. One interesting change in this keratinpattern is the appearance of the M, 40,000 keratin which increases steadily through several rounds of subculturing (Fig. 2A,Lanes 2 to 4). Wu ef al. (40) have also identified this keratin incultured human esophageal cells. It is present in large amountsis some normal epithelia (20, 36) and in some other cultured cells(11, 35, 40). It has also been found in a number of differentcarcinomas (21, 23, 41). Its role in the cytoskeleton remainsunknown.
The changes in keratin pattern observed for cultured esophageal cells are likely to be transient. Previously, it was shownthat, although epithelial cells from different sources develop anindistinguishable pattern of keratin expression in vitro, they reac-
quire their distinctive keratin patterns when the cultured cells areinjected s.c. into athymic mice (7). Recently, it has been shownthat the level of vitamin A in the culture medium can have aprofound influence on the pattern of keratins produced by anepithelial cell, thereby providing a possible basis for this observation (11).
The pattern of keratins produced by SQCCs may also beinfluenced by the level of vitamin A in the tissue. In some SQCCs,altered sensitivity to the vitamin has been observed and maycause changes in keratin expression (17). Although extracellularfactors most certainly play a role in altering the pattern of keratinsproduced by SQCCs, additional factors might contribute to permanent changes in keratin expression in the cancers (28). It isquite possible, for instance, that the altered program of differentiation which occurs during the development of the malignantstate leads to changes in keratin expression. Alternatively, thechanges in keratin synthesis may arise from the malignant transformation of a rare population of esophageal epithelial cells thatproduce a pattern of keratins different from most of the cells ofthe intact tissue.
It seems quite remarkable that, despite the many factorsknown to influence keratin gene expression, consistent differences exist between the pattern of keratins produced by SQCCof the esophagus and normal esophageal epithelium. Since theesophagus is accessible to endoscopie biopsy and cytologicalbrushing, it may be possible to take advantage of these biochem-
6M. P. GraceandE. Fuchs,unpublishedresults.
CANCER RESEARCH VOL. 45 FEBRUARY 1985
843
on July 31, 2020. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

KERATIN IN HUMAN ESOPHAGEAL SQCC
ical differences in conjunction with standard pathological techniques to develop improved methods for earlier detection of thiscancer. Techniques such as measurement of DNA content (22)and scanning electron microscopy (14) have already been usedto investigate and diagnose precancerous and early malignantlesions of the esophagus in humans. Mass screening programsin areas of high risk have resulted in earlier detection of esoph-
ageal carcinoma and possibly improved survival (42). The use ofpolyacrylamide gel electrophoresis and monoclonal antibodies inidentifying specific keratins characteristic of various malignantneoplasms has become increasingly valuable (13, 20,21, 23, 24,32). These diagnostic and investigational methods have thus farbeen utilized primarily for tumors that are clinically apparent orsymptomatic.
The development of monoclonal antibodies that recognizedistinct keratin patterns, cell types, and states of cellular differentiation has been described (6,9,26,36,38). As we learn moreabout the amino acid sequence differences between the manydifferent keratins (8,15,16,34), it should be possible to generateantibodies specific for each keratin, even if it shares a highdegree of homology with other keratins. It seems within thegrasp of existing technology to develop an antibody that woulddistinguish esophageal epithelium, dysplastic epithelium, andSQCC of the esophagus based on their differences in keratinexpression. Such an antibody may be useful in generating abiochemical method of cancer detection which, when used inconjunction with standard pathological techniques, may result inearlier detection of SQCC of the esophagus.
ACKNOWLEDGMENTS
The authors would like to thank Claire Doyle for typing the manuscript and PhilipCaliga for preparing the photographs for publication.
REFERENCES
1. Banks-Schlegel, S. P., and Harris, C. C. Tissue-specific expression of keratinproteins in human esophageal and epidermal epithelium and their culturedkeratinocytes. Exp. Cell Res., 746: 271-280,1983.
2. Banks-Schlegel, S. P., and Harris, C. C. Aberrant expression of keratin proteinsand cross-linked envelopes in human esophageal carcinomas. Cancer Res.,44: 1153-1157,1984.
3. Barnes, D., and Sato, G. Methods for growth of cultured cells in serum-freemedium. Anal. Biochem., 702.-225-270, 1980.
4. Burnett, W. N. "Western blotting": electrophoretic transfer of proteins fromsodium dodecyl sulfate-polyacrylamide gels to unmodified nitrocellulose, andradiographie detection with antibody and radioiodinated Protein A. Anal.Biochem., 772: 195-203, 1981.
5. Cukingnan, R. A., and Carey, J. S. Carcinoma of the esophagus. Ann. Thorac.Surg., 26: 274-286, 1978.
6. Debus. E., Moll, R., Franke, W. W., Weber, K., and Osborn, M. Immunohisto-chemical distinction of human carcinomas by cytokeratin typing with monoclonal antibodies. Am. J. Pathol., 774: 121-130,1984.
7. Doran, T. L., Vidrich, A., and Sun, T.-T. Intrinsic and extrinsic regulation of thedifferentiation of skin, corneal, and esophageal epithelial cells. Cell, 22:17-25,
1980.8. Dowling, L. M., Parry, D. A. D., and Sparrow, L. G. Structural homology
between «-keratinand the intermediate filament proteins desmin and vimentin.Biosci. Rep., 3: 73-78,1983.
9. Franke, W. W., Schmid, E., Wellsteed, J., Grund, C., Gigi, O., and Geiger, B.Change of cytokeratin filament organization during the cell cycle: selectivemasking of an immunologie determinant in interphase PtK2 cells. J. Cell Biol.97:1255-1260,1983.
10. Fuchs, E., and Green, H. Changes in keratin gene expression during terminaldifferentiation of the keratinocyte. Cell, 79:1033-1042, 1980.
11. Fuchs, E., and Green, H. Regulation of terminal differentiation of culturedhuman keratinocytes by vitamin A. Cell, 25: 617-625, 1981.
12. Fuchs, E., and Marchuk, D. Type I and type II keratins have evolved fromlower eukaryotes to form the epidermal intermediate filaments in mammalian
skin. Proc. Nati. Acad. Sci. USA, 80: 5857-5861,1983.13. Gatter, K. C., and Mason, D. Y. The use of monoclonal antibodies for histo-
pathologic diagnosis of human malignancy. Semin. Oncol., 9: 517-525,1982.14. Goran, D. A., Shields, H. M., Bates, M. L., Zuckerman, G. R., and De Schryver-
Kecskemeti, I. Esophageal dysplasia: assessment by light microscopy andscanning electron microscopy. Gastroenterology, 86: 39-50, 1984.
15. Hanukoglu, I., and Fuchs, E. The cDNA sequence of a human epidermalkeratin: divergence of sequence but conservation of structure among intermediate filament proteins. Cell, 37: 243-252,1982.
16. Hanukoglu, I., and Fuchs, E. The cDNA sequence of a type II cytoskeletalkeratin reveals constant but variable structural domains among keratins. Cell,33: 915-924,1983.
17. Kim, K. H., Schwartz, F., and Fuchs, E. Differences in keratin synthesisbetween normal epithelial cells and squamous cell carcinomas are mediatedby vitamin A. Proc. Nati. Acad. Sci. USA, 87: 4280-4284, 1984.
18. Laemmli, U. K. Cleavage of structural proteins during the assembly of the headof bacteriophage T4. Nature (Lond.), 227: 680-685,1970.
19. Maciag, T., Nemore, R. E., Weinstein, R., and Gilchrest, B. A. An endocrineapproach to the control of epidermal growth: serum free cultivation of humankeratinocytes. Science (Wash. DC), 277: 1452-1454,1981.
20. Moll, R., Franke, W. W., Schiller, D. L., Geiger, B., and Krepier, R. The catalogof human cytokeratins: patterns of expression in normal epithelia, tumors, andcultured cells. Cell, 37: 11-24,1982.
21. Moll, R., Krepier, R., and Franke, W. W. Complex cytokeratin polypeptidepatterns observed in certain human carcinomas. Differentiation, 23: 256-269,1983.
22. Mukada, T., Sasano, N., and Sato, E. Evaluation of esophageal dysphagia bycytofluorometric analysis. Cancer (Phila.), 47:1399-1404,1978.
23. Nelson, W. G., Battifora, H., Santana, H., and Sun, T.-T. Specific keratins asmolecular markers for neoplasms with a stratified epithelial origin. Cancer Res.,44: 1600-1603,1984.
24. Osborn, M., and Weber, K. Biology of disease: tumor diagnosis by intermediatefilament typing: a novel tool for surgical pathology. Lab. Invest., 48: 372-394,1983.
25. Ota, K., and Shin, L. H. Histological Typing of Gastric and OesophagealTumors. Geneva: WHO, 1977.
26. Ramaekers, F., Huysmans, A., Moesker, O., Kant, A., Jap, P., Herman, C.,and Vooijs, P. Monoclonal antibody to keratin filaments specific for glandularepithelia and their tumors. Lab. Invest., 49: 353-361,1983.
27. Rheinwald, J. G. Serial cultivation of normal human epidermal keratinocytes.Methods Cell Biol., 27: 229-254, 1980.
28. Rheinwald, J. G., and Beckett, M. A. Defective terminal differentiation in cultureas a consistent and selectable characteristic of malignant human keratinocytes.Cell, 22:629-632,1980.
29. Rheinwald, J. G., and Beckett, M. A. Tumorigenic keratinocyte lines requiringanchorage and fibroblast support cultured from human squamous cell carcinomas. Cancer Res., 47:1657-1663, 1981.
30. Rheinwald, J. G., and Green, H. Epidermal growth factor and the multiplicationof cultured human epidermal keratinocytes. Nature (Lond.), 265: 421-424,1977.
31. Rosenberg, J. C., Schwade, J. G., and Vaitkevicious, V. K. Cancer of theesophagus. In: V. T. DeVita, S. Hellman, and S. A. Rosenberg (eds.), Cancer:Principles and Practice of Oncology, pp. 499-533. Philadelphia: J. B. Lippin-cott, 1982.
32. Said, J. W., Nash, G., Banks-Schlegel, S., Sassoon, A. F., Murakami, S., andShintaku, I. P. Keratin in human lung tumors: patterns of localization of differentmolecular weight keratin proteins. Am. J. Pathol., 773: 27-32, 1983.
33. Silverberg, E. Cancer statistics. Cancer J. Clin., 34: 7-23, 1984.34. Steinert, P. M., Rice, R. H., Roop, D. R., Trus, B. L., and Steven, A. C.
Complete amino acid sequence of a mouse epidermal keratin subunit andimplications for the structure of intermediate filaments. Nature (Lond.), 302:794-800, 1983.
35. Sun, T.-T., and Green, H. Cultured epithelial cells of cornea, conjunctiva, andskin: absence of marked intrinsic divergence of their differentiated states.Nature (Lond.), 269: 489-493, 1977.
36. Tseng, S., Jarvinen, M. J., Nelson, W. G., Huang, J. W., Woodcock-Mitchell,J., and Sun, T.-T. Correlation of specific keratins with different types ofepithelial differentiation: monoclonal antibody studies. Cell, 30:361-372,1982.
37. Van Andel, J. G., Dees, J., Dijkhuis, C. M., Fokkens, W., van Houten, H., deJong, P. C., and van Woerkom-Eykenboom, W. M. H. Carcinoma of theesophagus: results of treatment. Ann. Surg., 790: 684-689,1979.
38. Van Muijen, G. N. P., Ruiter, D. J., Ponec, M., Huiskens-Van Der Mey, C., andWarnaar, S. O. Monoclonal antibodies with different specificities against cytokeratins: an immunohistochemical study of normal tissues and tumors. Am.J. Pathol., 774:9-17, 1984.
39. Whychulis, A. R., Woolam, G. L., Anderson, H. A., and Ellis, F. H. Achalasiaand carcinoma of the esophagus. J. Am. Med. Assoc., 275:1638-1641,1971.
40. Wu, Y.-J., Parker, L. M., Binder, N. E., Beckett, M. S., Sinard, J. H., Griffiths,C. T., and Rheinwald, J. G. The mesothelial keratins: a new family of cytoskeletal proteins identified in cultured mesothelial cells and nonkeratinizingepithelia. Cell, 37: 693-703,1982.
41. Wu, Y.-J., and Rheinwald, J. G. A new small (40 kd) keratin filament proteinmade by some cultured human squamous cell carcinomas. Cell, 25: 627-635,1981.
42. Yang, C. S. Research on esophageal cancer in China: a review. Cancer Res.,40: 2633-2644,1980.
CANCER RESEARCH VOL. 45 FEBRUARY 1985
844
on July 31, 2020. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

KERATIN IN HUMAN ESOPHAGEAL SQCC
y&S!f*¿;¿FE- LaT^—. «<£n-r-'u< e^^:iii* •r • •*«'<<••»V1* .•*"*JH
Üáü^ilI 23456 I 23456
F~ — "
«•» —«•»•» "* '••^
/58-V.56=^-52
5046A40
2a 2bFig. 1. Anti-keratin ¡mmunofluorescent staining of normal esophageal epithelium (a), SQCC of the esophagus (b), and cultured esophageal epithelial cells (e), se,
subepithelial tissue; ci. connective tissue; £.esophageal epithelium; C, SQCC of the esophagus. Note that only the epithelial tissue, the epithelial-derived cancer, andthe cultured esophageal colony show immunoreactivity with the anti-keratin antisera. Fibroblasts, connective tissue, and smooth muscle tissue show no reactivity. Notealso the fine cytoplasmic keratin intermediate filament network in the cultured esophageal epithelial cells (c). a, x 420; b. x 420; c, x 840
Fig. 2. a, electrophoretic separation of keratins. Water-insoluble proteins were separated by electrophoresis through an 8.5% polyacrylamide gel, and the protein
bands were visualized by staining with Coomassie blue. Lane 1, esophageal epithelial tissue; Lane 2, primary culture of esophageal epithelial cells; Lane 3, first subculture;Lane 4, second subculture; Lane 5, SQCC of the esophagus; Lane 6, SCC-15 [a cultured cell line of SQCC of the tongue (40)]. A, actin. b, immunoblot analysis of keratinpatterns using anti-keratin antibodies prepared against cultured human epidermal cells. Lanes are as in Fig. 2a.
CANCER RESEARCH VOL. 45 FEBRUARY 1985
845
on July 31, 2020. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

KERATIN IN HUMAN ESOPHAGEAL SQCC
_J 2_ 3456" 11 ii ~ii ~ ii ii "
ECECECECECEC
(MD) (PD) (PD) (MD) (MD) (MD)
I 234567
58,5652504640
Fig. 3. Immunoblot analysis of keratin patterns of normal esophageal epithelial tissue (£)and SQCC of the esophagus (C) from 6 patients, labeled 7 to 6. Tumorgrade: moderately differentiated (MD) and poorly differentiated (PD) SQCC of the esophagus.
Fig. 4. Immunoblot analysis of keratin patterns of esophageal epithelial tissue from an additional 7 patients, Lanes 1 to 7. Note the presence of an M, 46,000 band inLane 5. This esophageal tissue was obtained from a patient who died of hepatic cirrhosis. A shorter exposure time of the bands in Lane 5 is shown on the right. Notethat with a shorter exposure time, the M, 46,000 band is no longer visible. The keratin pattern in Lane 6 was from esophageal epithelial tissue of a neonate who died ofcongenital anomalies.
CANCER RESEARCH VOL. 45 FEBRUARY 1985
846
on July 31, 2020. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1985;45:841-846. Cancer Res Michael P. Grace, Kwan Hee Kim, Lawrence D. True, et al. Squamous Cell Carcinoma of the EsophagusKeratin Expression in Normal Esophageal Epithelium and
Updated version
http://cancerres.aacrjournals.org/content/45/2/841
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/45/2/841To request permission to re-use all or part of this article, use this link
on July 31, 2020. © 1985 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from