Embed Size (px)
Citation preview
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 1
The Royal Borough of Kensington and Chelsea
and
Kensington and Chelsea Primary Care Trust
Strategy for service provision to
adults with a physical and/or sensory disability
2002 – 2005
Draft for Consultation MARCH 2002
(Version 15)
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 2
CONTENTS Page Introduction Background and Context of Change Aims and Principles Needs Assessment Local needs and issues raised through consultation Setting Priorities
What needs to be done (Action Plan) Resources Available and Current Expenditure Summary APPENDICES Appendix 1: The users, carers and providers questionnaire Appendix 2: Extracts from surveys on disability Appendix 3 Description of current services Appendix 4: NHS Continuing Care Services Appendix 5: Glossary of terms and abbreviations
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 3
1. INTRODUCTION
1.1 This Strategy covers the health and social care needs of adults, aged between 18 and 64 years, with a physical disability or sensory impairment. It is recognised that many people over the age of 65 also have physical disabilities and sensory impairments. Many of the principles set out in this strategy apply equally to people of all ages, but service delivery recommendations are designed for people between the ages of 18 and 65. Specific reference for older people can be found elsewhere, including the Joint Investment Plan for Older People (2000) and the Older People’s Needs Analysis (2001). Carers form another key part of service delivery and reference should be made to the Royal Borough’s Carers Strategy (2001 – 2004).
1.2 In this Strategy, the term ‘disabled’ is used to include people with physical disabilities, sensory
impairments, early onset dementia, brain and other traumatic injuries. Whilst the Strategy is not intended to cover services for people with learning disabilities or HIV and AIDS, it will inevitably be of some benefit to those user groups. A strategy for people with learning disabilities was published in 2000 and a project plan for HIV/AIDS services is published annually.
1.3 Eligibility Criteria: to receive services from the specialist teams people must have a
permanent physical disability which has a long term effect on their ability to manage daily life. People with sensory impairments will always be seen by the specialist team. If people have needs which do not fit into the definition and yet are vulnerable (maybe for example a short term illness which has significantly impacted upon their ability to manage daily life) the Social Services Department may still be able to help.
1.4 The strategy has been produced jointly by the Royal Borough of Kensington and Chelsea and
Kensington and Chelsea Primary Care Trust, and covers services for the three year period from April 2002- 2005.
1.5 The draft strategy poses three questions namely:
Are the priorities in the strategy the right ones? Will the objectives in the strategy enable us to meet our priorities? Are we investing in the right areas for the future?
1.6 Service users, carers, service providers, voluntary organisations and advocacy groups are
invited to respond to these questions in writing or by telephone between 1st March 2002 and
1st May 2002 to:
The Partnership Group (Disability) C/o Hector Medora, Service Manager, Disability Services, (Tel: 020 7361 2408) or Trish Welton, Team Manager, Social Work Team, Disability, (Tel: 020 7361 2353) The Royal Borough of Kensington and Chelsea, Town Hall, Hornton Street, London W8 7NX
1.7 In drawing up the Strategy, we have taken into account the views of some users, carers and
providers. Their views are documented throughout this Strategy. 1.8 The Disability Partnership Group has also sought the views of service users, carers and
providers. Their comments have been used to develop this Strategy.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 4
2. BACKGROUND AND CONTEXT OF CHANGE 2.1 A number of recent policy changes at a national level have impacted on services. The
Government, through the publication of the NHS Plan 2000, signalled its intention to place people at the centre of care and to begin to break down some of the barriers that exist between health and local authorities.
2.2 The Local Government Act 1999 established Best Value reviews effective from April 2000.
These will act as a driver for the improvement in a range of services provided by councils and give local people more of a say in the services they receive. All council services are to be reviewed over a five-year period. The Best Value Review for Physical Disability and Sensory Impairment Services is scheduled for 2004/5.
2.3 The provisions of the Disability Discrimination Act 1995 have been implemented gradually
over the past few years and will take full effect in 2004. The main areas covered are employment and the provision of goods, facilities and services. This has important implications for all employers of over 15 people and for the NHS and Social Services Departments in particular as providers of goods and services. Since October 1999, it has been incumbent upon these service providers to make attempts to offer services by alternative means “where reasonable”. From 2004, it will also be necessary for service providers to make buildings accessible and consultation on the regulations for this will be carried out shortly. In addition, the Disability Rights Commission has, since April 2000, had powers to bring cases and launch investigations into breaches of the Act brought to it by individuals or organisations.
2.4 Better Services for Vulnerable People (1997), introduced the concept of Joint Investment
Plans (JIPs) to be agreed between local and health authorities, targeted at those vulnerable groups in most need of coordinated services. It set out the way that services needed to be reshaped and reinvested to better meet their needs. From March 2001, local and health authorities agreed a Welfare to Work JIP to better enable disabled people either to return to employment or to engage in the employment market for the first time.
2.5 The White Paper, Modernising Social Services (1998) reinforced previous guidance by
encouraging local authorities to promote independence and help service users to make the most of their own capacity and potential.
2.6 Another White Paper, The New NHS: Dependable, Modern (1997) led to the establishment of
the Primary Care Groups. In Kensington Chelsea and Westminster Health Authority (KCWHA) three Groups were established: Marylebone, Westway and South KCW. Following consultation in 2000 and 2001, two coterminous Primary Care Groups were created in June 2001. In April 2002 a new Kensington and Chelsea Primary Care Trust was created. Some services commissioned by the Health Authority, including disability services, are likely to be commissioned by the new Primary Care Trusts which will encompass some of the functions of the two Community Trusts, Riverside and Parkside. Health authorities in the London Region have also undergone further reconfiguration to accommodate further changes.
2.7 The 1997 White Paper further required health authorities to produce local Health Improvement
and Modernisation Programme (HImP), in association with their partner organisations, to improve both the health and care of the local population. In RBKC/KCWHA, progress was made through the HImP to tackle health inequalities. Key areas for the future include regeneration, housing, education, community safety, leisure, transport, environment, ethnicity and lifestyle factors.
2.8 The partnership arrangements under Section 31 of the Health Act 1999 have been developed
to give NHS bodies and local authorities additional flexibilities to be able to respond effectively to improve services for users. This introduced the concepts of pooled budgets; lead commissioning, and integrated provision. Pooled budgets provide an opportunity for partners to bring money together to pay for services under arrangements agreed in advance, thus reducing the likelihood of service users being inconvenienced by disputes between authorities about who might be responsible for providing services. Lead commissioning facilitates the strategic commissioning of services for a client group by a single agency (health authority,
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 5
local authority or primary care trust) so that services are better coordinated to the benefit of the user. Integrated provision enables different professionals to work together under a single management structure and could cover both the commissioning and provision of services e.g. local authorities and primary care trusts.
2.9 Local Authorities and partner agencies have worked together to ensure that new
arrangements under the “Supporting People” initiative are in place from April 2003. This will include developing specific priorities for new options and schemes, and making changes to current services for all vulnerable people over the age of 18 years.
2.10 The publication of the Audit Commission Report, Fully Equipped (March 2000) highlighted the
generally poor quality of some services across the country in a number of areas that have a very direct impact on the lives of disabled people, orthotic services, prosthetic services, wheelchair and seating services, community equipment and audiology services. Apart from a number of recommendations to be addressed by health authorities, NHS Trusts and social services departments to improve the quality of equipment services, the report also contains benchmarks of performance against which current services can be assessed. The National Service Framework for Older People (2001) has generated a requirement for a baseline audit of community equipment services to be undertaken with a view of working towards integrated equipment stores. There are also equipment standards set out in the local charter for long term care “Better Care, Higher Standards”.
2.11 The Government has, through the publication of its National Strategy for Carers (1999), and
the Carers and Disabled Children Act 2000, demonstrated its commitment to the very valuable contribution that carers can make in people’s care and the importance of looking after the needs and interests of carers as well as the person being supported. The Government has increased the opportunities for obtaining respite breaks for carers and is concerned that the views of carers on services are taken fully into account by health and social care agencies.
2.12 As well as these national programmes, there are also a number of local initiatives that affect
services for disabled people. In line with the central initiatives towards partnership working, outlined above, RBKC and KCWHA have, since April 2000, established a partnership structure to promote a corporate focus for the development of health and social care services. Partnership groups now exist for a number of client groups, including one for people with a disability. These groups have commissioners, providers and user involvement and have been responsible for commenting on the initial draft of this strategy.
2.13 In June 2001, RBKC and KCWHA published their second Charter for Long Term Care, Better
Care, Higher Standards. This sets out agreed standards of care, particularly for people who have long term care needs. The Charter is currently being revised and due to be published in June 2002.
2.14 There are a number of other joint initiatives which allow for improved joint working arrangements eg. Health and Social Care Act 2001 re scrutiny of local NHS by the local authority; an opportunity to develop Care Trusts (single body able to commission and provide both social and health care) and patient and public involvement in NHS through Community Health Councils, Patient Forums, etc.
2.15 The Local Government Act 2000 supports the development of community plans, a local
strategic partnership and structural changes to the political structures in local authorities ie. the creation of Cabinet.
2.16 The government has recently (2001) issued a consultation document “Fair Access to Care
Services” which aims to establish some national consistency for authorities when deciding upon who should be eligible for services. The final guidance is awaited and due for implementation in 2002.
2.17 In March 2001 the Department of Health issued guidance under Section 7 of the Local
Authorities Social Services Act 1970. This guidance referred to services to people with a dual
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 6
sensory loss. Local authorities must now identify people with a dual sensory loss living in their area and make appropriate service provision.
2.18 This strategy was further influenced by the recommendations made in a recent Joint Review of the Social Services Department (October 2000) carried out by the Audit Commission and the Social Services Inspectorate.
2.19 The purpose of the review was to provide an objective assessment of how well people in the
Royal Borough were being served by the Department and to make a constructive contribution towards the further improvements of services provided. The Joint Review team concluded that Borough residents and users are generally well served.
3. AIMS AND PRINCIPLES 3.1 The following aims and principles seek to assist the inclusion of disabled people within
mainstream society and encourage full access to services. The aims and principles have been developed jointly by the health and social services agencies and with users, carers and providers.
3.2 These should reflect the way that services are delivered now and in the future. 3.3 We aim to:
1. promote independence and the opportunities for care and support to be provided as close to home as possible, and where appropriate offer real alternatives to residential care;
2. increase the control that disabled people and their carers have over their own lives and
the care and assistance that they need;
3. improve opportunities to provide a seamless service, including exploring opportunities to work in partnership with other agencies;
4. increase the physical and emotional well being of disabled people and their carers;
5. ensure that disabled people and their carers have access to a full range of high quality
services that are responsive to their needs across primary, secondary and specialist services and provide them with choice;
6. ensure that users and carers are involved and consulted appropriately about their care
and service developments;
7. ensure that users and carers receive high quality information about the services that are available to them;
8. ensure that there is access to advocacy services if people require them and recourse to a
responsive complaints system from which lessons for improvement can be learnt;
9. integrate health and social care service provision where this will benefit disabled people and their carers;
10. ensure that quality services are delivered;
11. maximise access to other services (housing, education, leisure, etc) to the fullest extent;
12. ensure that services are culturally sensitive;
13. sustain employment potential and opportunities to develop work skills for disabled people,
through the Joint Investment Plan for Welfare To Work published in March 2001.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 7
4. NEEDS ASSESSMENT 4.1 Epidemiology: it is not possible to arrive at a single estimate for the numbers of people with
disabilities in the Royal Borough. Abilities vary across a wide spectrum and any cut off point used to define ‘disability’ may be arbitrary. However, we need to make some estimate of the numbers of people who could benefit from services. We have therefore used a number of surveys to come to a conclusion about the number of people with a disability living in Kensington & Chelsea (Appendix 2).
4.2 The estimated total number of people aged 18-64 in RBKC with one or more disabilities varies
from about 5,000 to about 21,000.
4.3 Health Survey for England, 1995: this is a national household survey carried out on behalf of the Department of Health each year. Disability issues were addressed for the only time in 1995. Information was collected through interviews. The estimates of disability for this survey are not directly comparable to the OPCS survey for a variety of reasons, and cannot be used to look at trends over time. They are however useful for estimating current levels of need across broad groups of disability. The HSE estimates of prevalence are higher than the previous OPCS estimates. They give a total of about 13,400 adults aged 18-64 in RBKC with one or more disabilities.
4.4 The HSE figures have been used to estimate the current numbers of people with disabilities
that affect mobility and personal care. These can be usefully compared with the numbers of people using mobility services of various sorts and numbers receiving help with personal care at home. Both the OPCS and the HSE surveys found somewhat lower rates of disability in the Greater London and North Thames regions than in the country as a whole. Detailed breakdown however by region, age and type of disability was not available, so national rates have been used to estimate local numbers of people.
4.5 RBKC/KCWHA Survey 1998: a detailed, multidisciplinary needs assessment for physical
disability services for adults was conducted. It attempted to establish:
• estimates of the numbers of people with disabilities in 1996 by severity and type of disability
• projections for 2001, 2006 and 2011
• service availability and usage by type of health and social service
• qualitative assessments from interviews with clients. 4.6 The survey estimated that between 20 and 40 percent of people with different types and
degrees of disability were registered.
4.7 The disabilities identified in the survey were grouped together into five main areas. Applied to the RBKC population it is estimated that there are 8869 people with disabilities, aged 16-64 years:
• 5555 have a physical and sensory disability
• 1187 have a visual impairment
• 2675 have a hearing impairment
(some people will appear in more than one of the above categories) 4.8 OPCS Disability Survey: the epidemiological estimates in the 1998 needs assessment were
largely based on the rates of disability found in the OPCS Disability Survey, which was carried out in 1988, and population projections from the London Research Centre. The estimated total is about 7,400, with about 6000 having only physical and or sensory disabilities.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 8
4.9 Labour Force Survey (1999): this survey estimated that almost one in five people of working age have a disability of some sort. The LFS gives the highest estimate of all the sources available, a total of about 23,500 in RBKC. However, about half of those with disabilities in the LFS were in work.
4.10 Local Authority Disability Register: statutory registers maintained by local authorities are
generally incomplete and therefore need to be used with caution in service planning. The information however does contribute to offering a fuller picture (Appendix 2).
5. LOCAL NEEDS AND ISSUES RAISED THROUGH CONSULTATION 5.1 The views of users and carers have been sought in a variety of ways throughout the year. An
event held early in December 2000 to celebrate World Disability Day provided us with an opportunity to find out the views of some users and carers on the emerging priorities in the draft Strategy. A questionnaire (Appendix 1) was used and there were meetings in groups. About 50 people contributed to the process.
5.2 The following gaps or developments in services have been identified:
General
• The need to address the issues identified in the Audit Commission Report, Fully Equipped, NSF Older People Standards, as they relate to the availability of and access to modern and appropriate equipment. This includes continuing improvement of the wheelchair service addressed through the contract with Brent PCT. Users and carers also wanted more regular visits by an Occupational Therapist.
• Improving access to and knowledge of existing services, including improving information about the range and location of services.
• Improving access to communication aids and assistive technology.
• Maximising opportunities for the timely provision of adapted and supported housing.
• Exploring the specific needs of disabled parents.
• Improving support for people wishing to return to work or wanting employment and contribute to the development of the Welfare to Work JIP.
• Improved access to public buildings (see Corporate Disability Strategy)
• Clearer pathways to appropriate rehabilitation.
• Developing advocacy services.
• More individually tailored activities and services that take account of the needs of the individual rather than of groups of people who are disabled or sensory impaired.
• Improving access to mainstream services.
• Ensuring good links with Adult Protection Services to prevent abuse.
• Wider access to the Direct Payments system
• Greater transparency and clearer principles on the Council’s charging policies
• Better access to transport (see the Service Improvement Plan from the Best Value Review of Transport, 2001)
Sensory Impairments
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 9
• Improve key areas of service to deaf people, as identified in the user consultation exercise in October 2000 and June 2001. Particular emphasis will be placed on:
- access to information - more minicoms available in Council departments - better access to interpreter services - specialist assessments around the provision of equipment - greater availability of loop systems, especially in primary care services
• Improve services for those with low vision in particular offering more services at home and liasing with health services to cut down waiting lists.
• Develop a clear strategy and information around the services offered to people with a dual sensory loss. Expand the current guide communicator scheme and provide front line staff with specialist training on how to best help people with a dual sensory loss.
Brain Injury
• Develop an acquired brain injury service.
• Explore the feasibility of developing long-term local community facilities for the care of people with brain injuries with cognitive difficulties that are unable to be looked after at home.
Young Onset Dementia
• Develop closer working links with health colleagues and other professionals, with a view to providing a more ‘streamlined’ holistic assessment and provision of care. Possibility of a dedicated consultant and clinical team.
• Work closer with housing and link with them with a view to providing more long/short term and specialised/supported housing, possibly in self contained houses/flats.
• Develop a specialised outreach team to enable people to live in their own homes as independently as possible to: - take people to important appointments; - assist with small domestic household jobs; - provide emotional and practical support..
• Set up and develop a social club to provide ‘client led’ social stimulation. To be started up initially by social service/health staff, with an aim for it to be run by paid workers or volunteers. Service users as much as possible making their choice as to what activities they would like to take part in.
• Develop group discussion/support groups for carers to enable them to discuss issues around care service developments etc.
• Make it easier for people who have young onset dementia to get a ‘freedom pass’.
• Develop a dedicated homecare team with appropriate training for working with the issues related to YOD (may be able to cover for the Older Persons team if needed).
• Move towards small group homes in the community with the potential for rehabilitation and some respite care. Aim to be supported living as much as possible, with a move to more practical ‘hands on’ care as the need arises.
• Introduce life history/personal planning books not only for people who are placed in residential care but also for those who live with support in the community.
• Investigate the use of the latest technology to assist people with keeping important appointments, medication etc.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 10
6. SETTING PRIORITIES 6.1 Service users, carers and providers asked that the following criteria be applied when setting
priorities: 6.2 Priorities should:
• be agreed by users, carers and providers;
• deliver something tangible which makes a difference;
• be realistic in terms of cost;
• address real needs and gaps in services;
• recognise the value of continuity of service.
6.3 The main priorities for the next five years should be:
6.3.1 develop health and social services which are joint at the point of delivery and adopt a social model. Ensure the involvement of users, carers and service providers at all levels of service development and provision;
6.3.2 provide clear and accessible information;
6.3.3 ensure the support meets the needs of individuals;
6.3.4 develop and implement a housing strategy to provide a range of
accommodation for people who wish to live independently and for people with complex needs;
6.3.5 increase the range and quality of daytime opportunities by maximising access
to mainstream leisure, education and employment opportunities;
6.3.6 implement new initiatives to improve the quality of services and the choices available.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 11
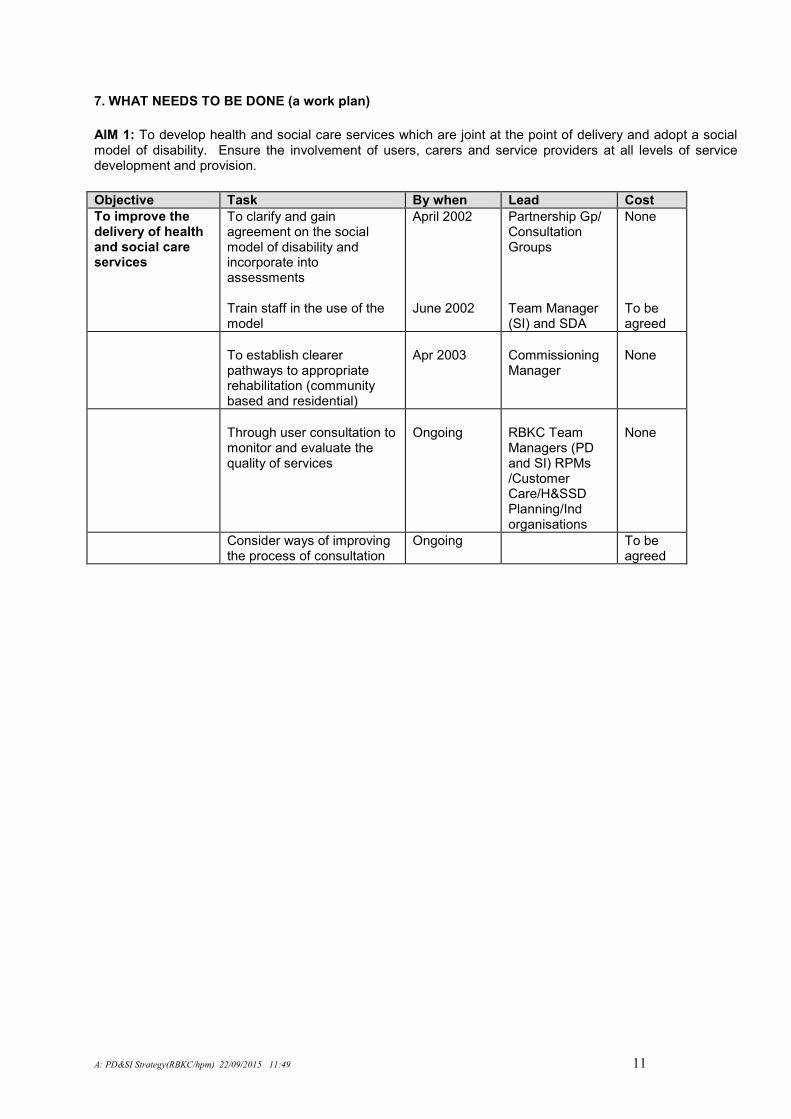
7. WHAT NEEDS TO BE DONE (a work plan)
AIM 1: To develop health and social care services which are joint at the point of delivery and adopt a social model of disability. Ensure the involvement of users, carers and service providers at all levels of service development and provision.
Objective Task By when Lead Cost
To improve the delivery of health and social care services
To clarify and gain agreement on the social model of disability and incorporate into assessments Train staff in the use of the model
April 2002 June 2002
Partnership Gp/ Consultation Groups Team Manager (SI) and SDA
None To be agreed
To establish clearer pathways to appropriate rehabilitation (community based and residential)
Apr 2003
Commissioning Manager
None
Through user consultation to monitor and evaluate the quality of services
Ongoing
RBKC Team Managers (PD and SI) RPMs /Customer Care/H&SSD Planning/Ind organisations
None
Consider ways of improving the process of consultation
Ongoing To be agreed
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 12
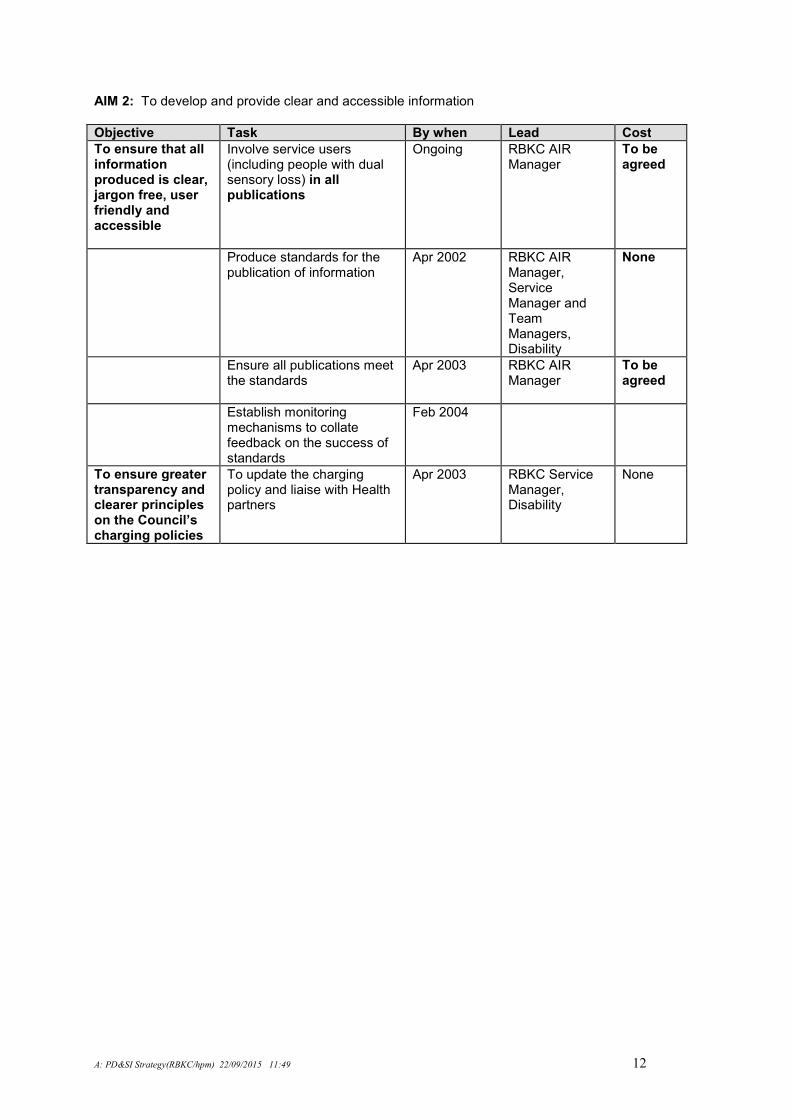
AIM 2: To develop and provide clear and accessible information
Objective Task By when Lead Cost
To ensure that all information produced is clear, jargon free, user friendly and accessible
Involve service users (including people with dual sensory loss) in all publications
Ongoing RBKC AIR Manager
To be agreed
Produce standards for the publication of information
Apr 2002 RBKC AIR Manager, Service Manager and Team Managers, Disability
None
Ensure all publications meet the standards
Apr 2003 RBKC AIR Manager
To be agreed
Establish monitoring mechanisms to collate feedback on the success of standards
Feb 2004
To ensure greater transparency and clearer principles on the Council’s charging policies
To update the charging policy and liaise with Health partners
Apr 2003 RBKC Service Manager, Disability
None
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 13
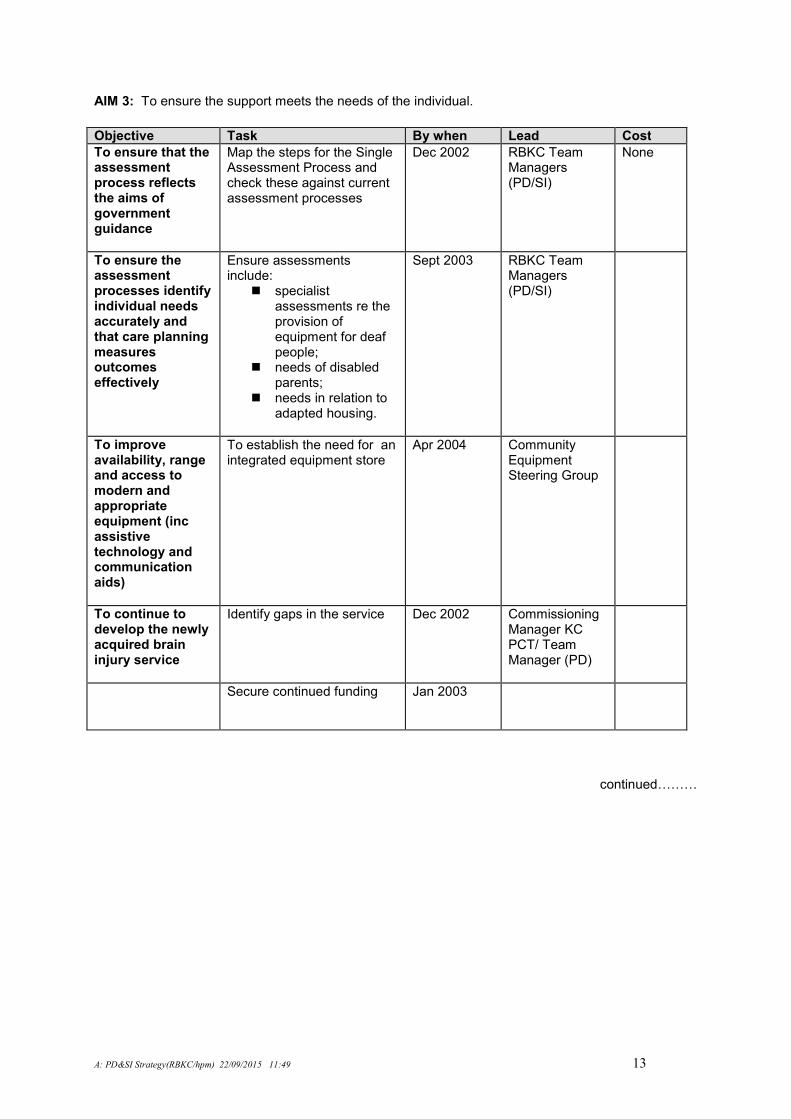
AIM 3: To ensure the support meets the needs of the individual.
Objective Task By when Lead Cost
To ensure that the assessment process reflects the aims of government guidance
Map the steps for the Single Assessment Process and check these against current assessment processes
Dec 2002 RBKC Team Managers (PD/SI)
None
To ensure the assessment processes identify individual needs accurately and that care planning measures outcomes effectively
Ensure assessments include:
� specialist assessments re the provision of equipment for deaf people;
� needs of disabled parents;
� needs in relation to adapted housing.
Sept 2003 RBKC Team Managers (PD/SI)
To improve availability, range and access to modern and appropriate equipment (inc assistive technology and communication aids)
To establish the need for an integrated equipment store
Apr 2004 Community Equipment Steering Group
To continue to develop the newly acquired brain injury service
Identify gaps in the service Dec 2002 Commissioning Manager KC PCT/ Team Manager (PD)
Secure continued funding Jan 2003
continuedLLL
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 14
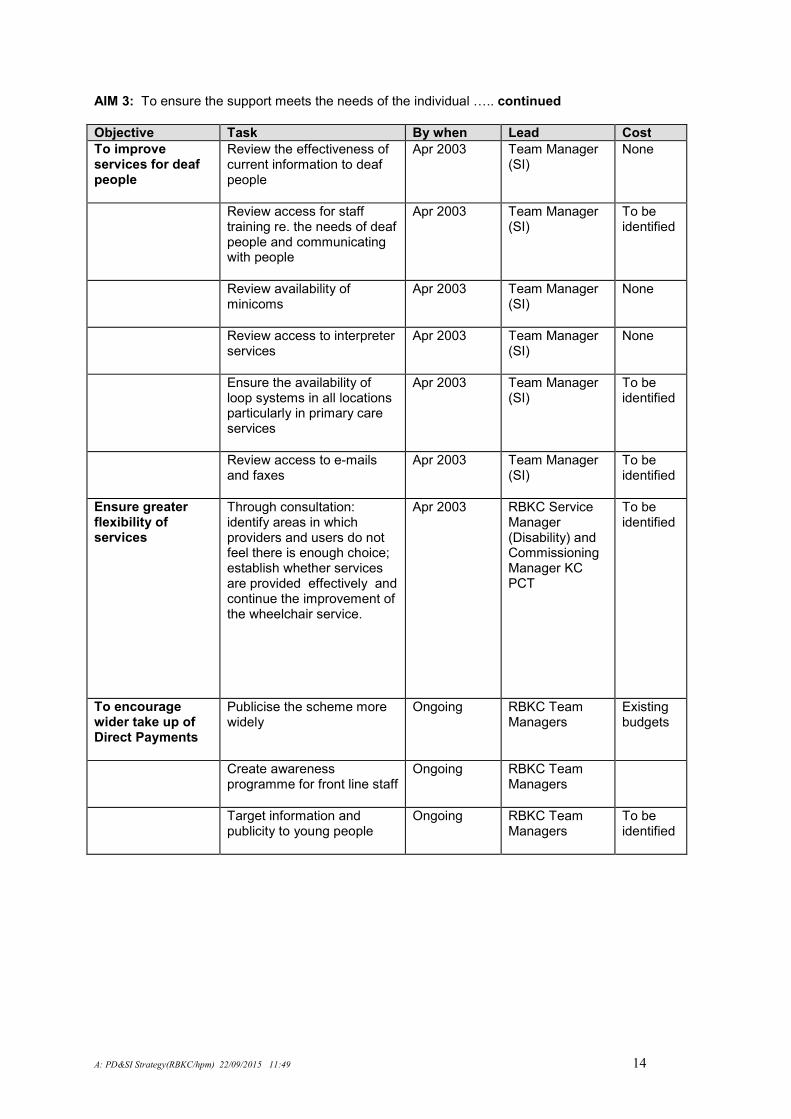
AIM 3: To ensure the support meets the needs of the individual L.. continued
Objective Task By when Lead Cost
To improve services for deaf people
Review the effectiveness of current information to deaf people
Apr 2003 Team Manager (SI)
None
Review access for staff training re. the needs of deaf people and communicating with people
Apr 2003 Team Manager (SI)
To be identified
Review availability of minicoms
Apr 2003 Team Manager (SI)
None
Review access to interpreter services
Apr 2003 Team Manager (SI)
None
Ensure the availability of loop systems in all locations particularly in primary care services
Apr 2003 Team Manager (SI)
To be identified
Review access to e-mails and faxes
Apr 2003 Team Manager (SI)
To be identified
Ensure greater flexibility of services
Through consultation: identify areas in which providers and users do not feel there is enough choice; establish whether services are provided effectively and continue the improvement of the wheelchair service.
Apr 2003 RBKC Service Manager (Disability) and Commissioning Manager KC PCT
To be identified
To encourage wider take up of Direct Payments
Publicise the scheme more widely
Ongoing RBKC Team Managers
Existing budgets
Create awareness programme for front line staff
Ongoing RBKC Team Managers
Target information and publicity to young people
Ongoing RBKC Team Managers
To be identified
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 15
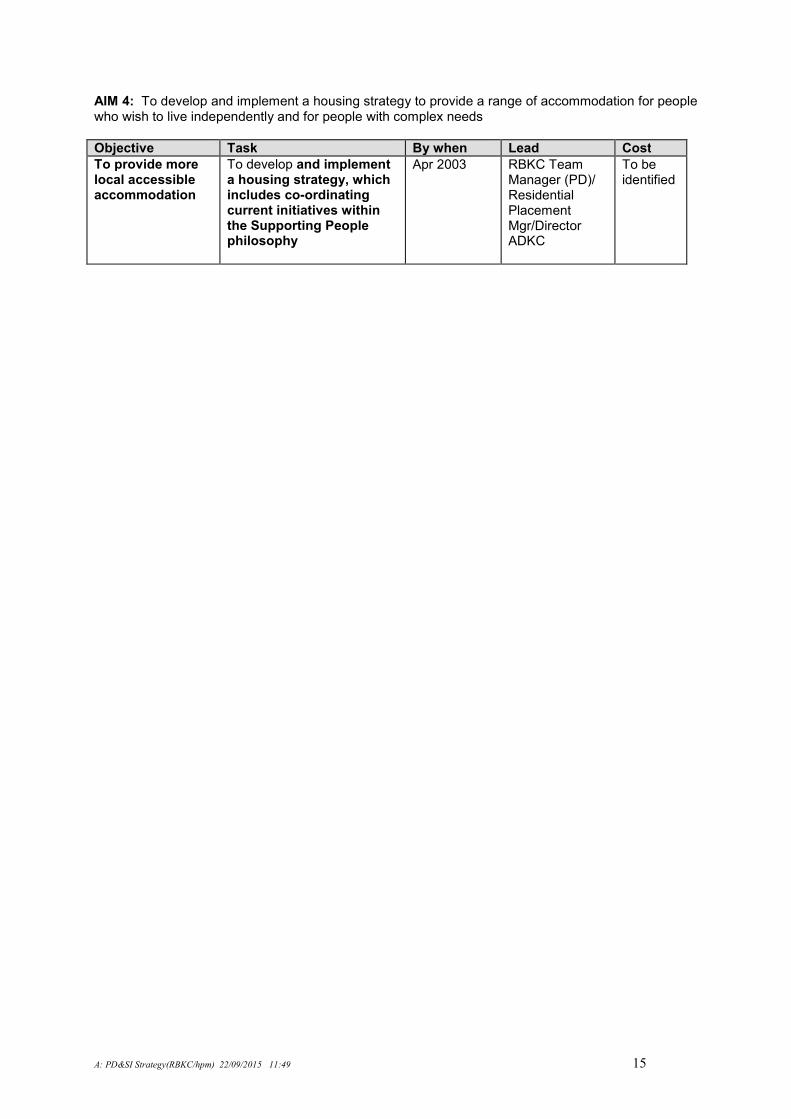
AIM 4: To develop and implement a housing strategy to provide a range of accommodation for people who wish to live independently and for people with complex needs
Objective Task By when Lead Cost
To provide more local accessible accommodation
To develop and implement a housing strategy, which includes co-ordinating current initiatives within the Supporting People philosophy
Apr 2003
RBKC Team Manager (PD)/ Residential Placement Mgr/Director ADKC
To be identified
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 16
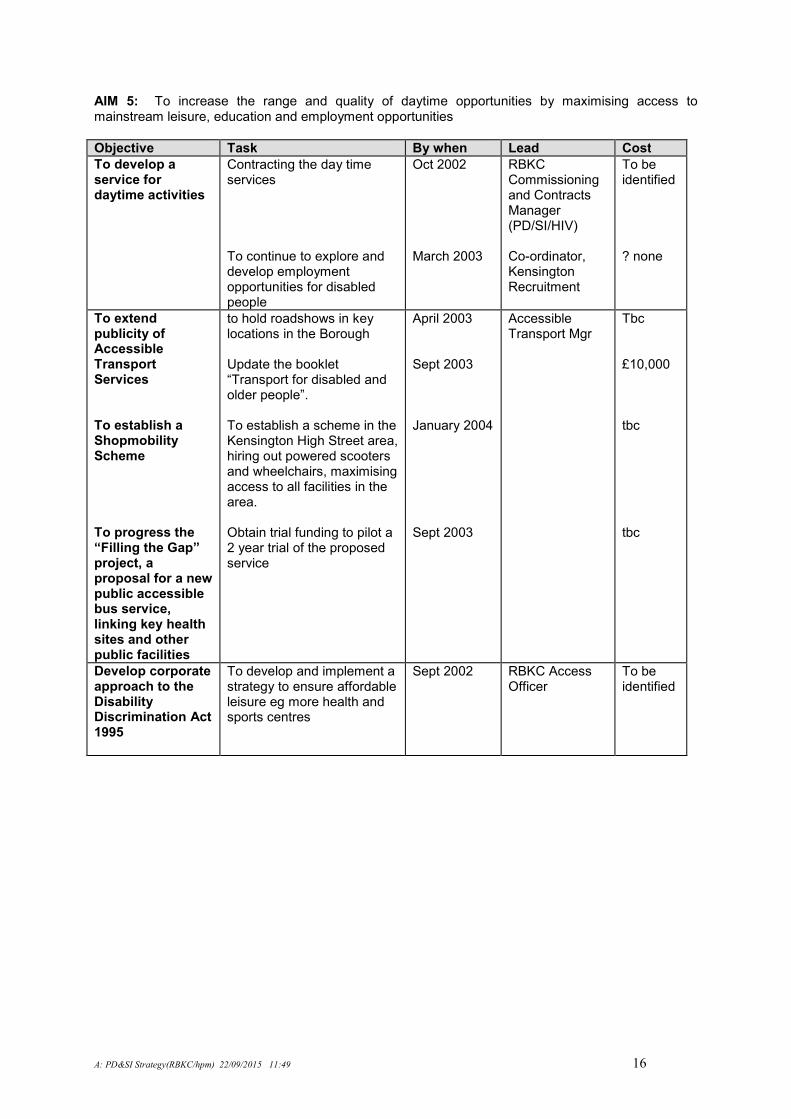
AIM 5: To increase the range and quality of daytime opportunities by maximising access to mainstream leisure, education and employment opportunities
Objective Task By when Lead Cost
To develop a service for daytime activities
Contracting the day time services To continue to explore and develop employment opportunities for disabled people
Oct 2002 March 2003
RBKC Commissioning and Contracts Manager (PD/SI/HIV) Co-ordinator, Kensington Recruitment
To be identified ? none
To extend publicity of Accessible Transport Services To establish a Shopmobility Scheme To progress the “Filling the Gap” project, a proposal for a new public accessible bus service, linking key health sites and other public facilities
to hold roadshows in key locations in the Borough Update the booklet “Transport for disabled and older people”. To establish a scheme in the Kensington High Street area, hiring out powered scooters and wheelchairs, maximising access to all facilities in the area. Obtain trial funding to pilot a 2 year trial of the proposed service
April 2003 Sept 2003 January 2004 Sept 2003
Accessible Transport Mgr
Tbc £10,000 tbc tbc
Develop corporate approach to the Disability Discrimination Act 1995
To develop and implement a strategy to ensure affordable leisure eg more health and sports centres
Sept 2002 RBKC Access Officer
To be identified
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 17
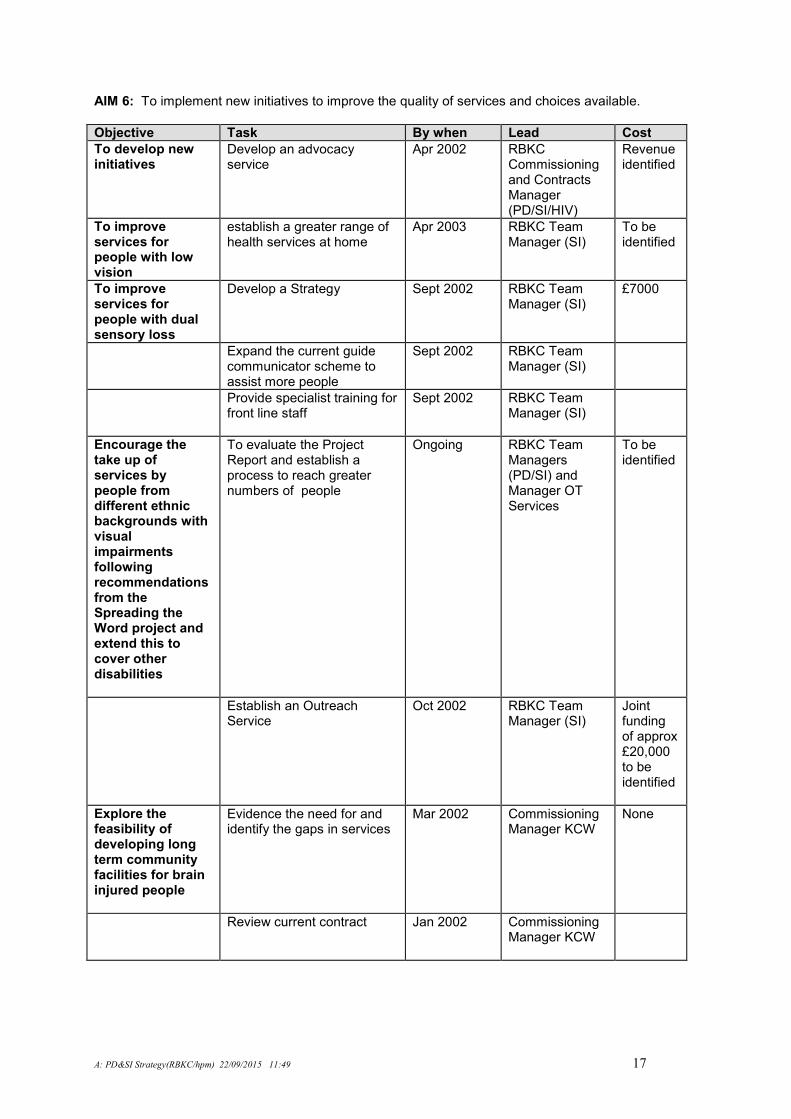
AIM 6: To implement new initiatives to improve the quality of services and choices available.
Objective Task By when Lead Cost
To develop new initiatives
Develop an advocacy service
Apr 2002
RBKC Commissioning and Contracts Manager (PD/SI/HIV)
Revenue identified
To improve services for people with low vision
establish a greater range of health services at home
Apr 2003 RBKC Team Manager (SI)
To be identified
To improve services for people with dual sensory loss
Develop a Strategy Sept 2002 RBKC Team Manager (SI)
£7000
Expand the current guide communicator scheme to assist more people
Sept 2002 RBKC Team Manager (SI)
Provide specialist training for front line staff
Sept 2002 RBKC Team Manager (SI)
Encourage the take up of services by people from different ethnic backgrounds with visual impairments following recommendations from the Spreading the Word project and extend this to cover other disabilities
To evaluate the Project Report and establish a process to reach greater numbers of people
Ongoing RBKC Team Managers (PD/SI) and Manager OT Services
To be identified
Establish an Outreach Service
Oct 2002 RBKC Team Manager (SI)
Joint funding of approx £20,000 to be identified
Explore the feasibility of developing long term community facilities for brain injured people
Evidence the need for and identify the gaps in services
Mar 2002 Commissioning Manager KCW
None
Review current contract Jan 2002 Commissioning Manager KCW
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 18
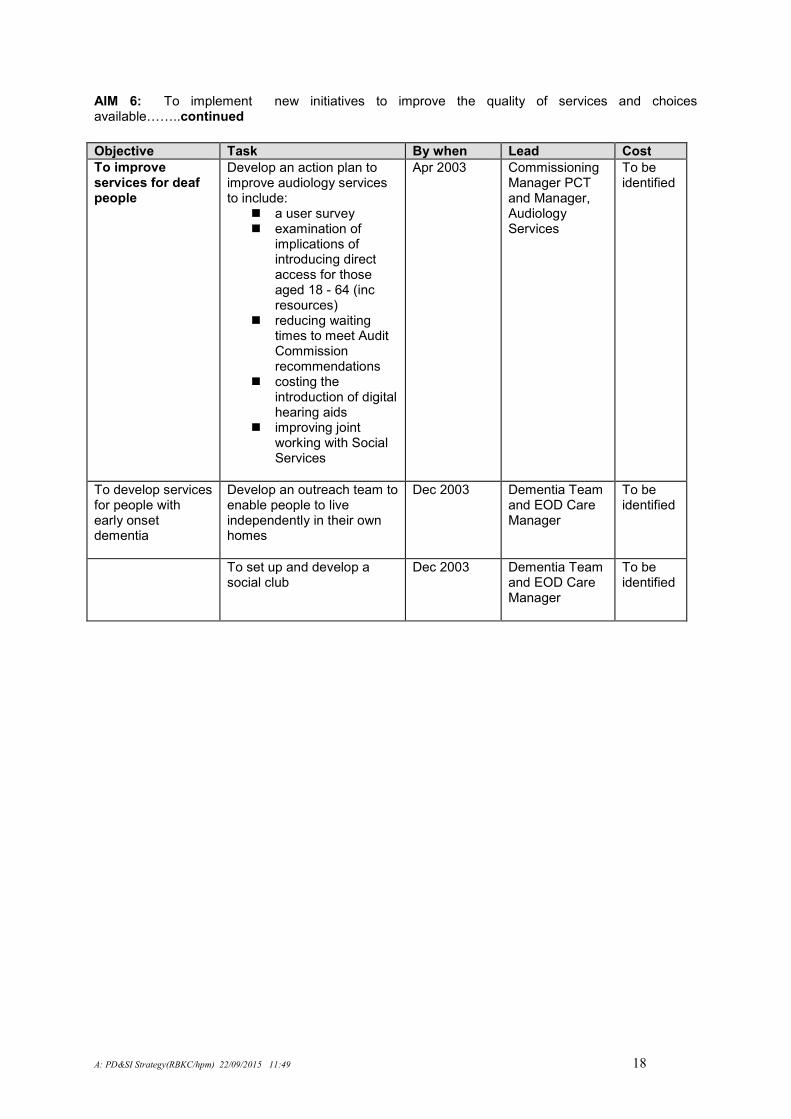
AIM 6: To implement new initiatives to improve the quality of services and choices availableLL..continued
Objective Task By when Lead Cost
To improve services for deaf people
Develop an action plan to improve audiology services to include:
� a user survey � examination of
implications of introducing direct access for those aged 18 - 64 (inc resources)
� reducing waiting times to meet Audit Commission recommendations
� costing the introduction of digital hearing aids
� improving joint working with Social Services
Apr 2003 Commissioning Manager PCT and Manager, Audiology Services
To be identified
To develop services for people with early onset dementia
Develop an outreach team to enable people to live independently in their own homes
Dec 2003 Dementia Team and EOD Care Manager
To be identified
To set up and develop a social club
Dec 2003 Dementia Team and EOD Care Manager
To be identified
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 19
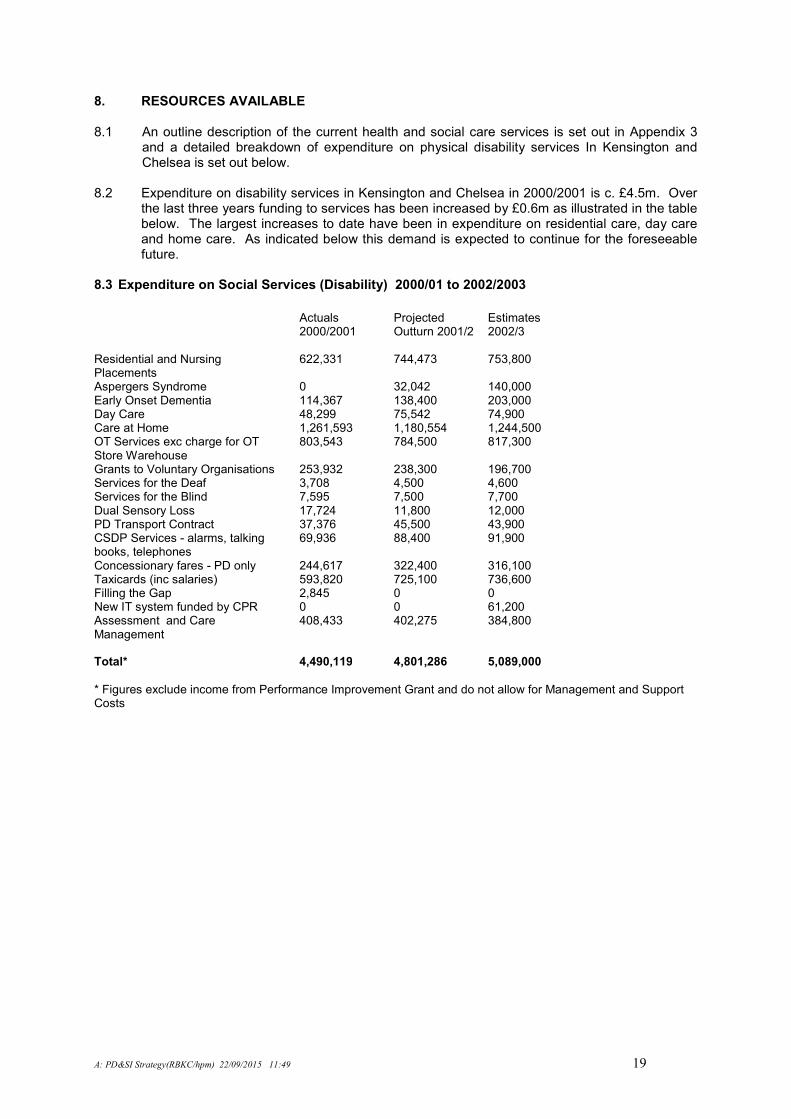
8. RESOURCES AVAILABLE 8.1 An outline description of the current health and social care services is set out in Appendix 3
and a detailed breakdown of expenditure on physical disability services In Kensington and Chelsea is set out below.
8.2 Expenditure on disability services in Kensington and Chelsea in 2000/2001 is c. £4.5m. Over
the last three years funding to services has been increased by £0.6m as illustrated in the table below. The largest increases to date have been in expenditure on residential care, day care and home care. As indicated below this demand is expected to continue for the foreseeable future.
8.3 Expenditure on Social Services (Disability) 2000/01 to 2002/2003
Actuals
2000/2001 Projected Outturn 2001/2
Estimates 2002/3
Residential and Nursing Placements
622,331 744,473 753,800
Aspergers Syndrome 0 32,042 140,000 Early Onset Dementia 114,367 138,400 203,000 Day Care 48,299 75,542 74,900 Care at Home 1,261,593 1,180,554 1,244,500 OT Services exc charge for OT Store Warehouse
803,543 784,500 817,300
Grants to Voluntary Organisations 253,932 238,300 196,700 Services for the Deaf 3,708 4,500 4,600 Services for the Blind 7,595 7,500 7,700 Dual Sensory Loss 17,724 11,800 12,000 PD Transport Contract 37,376 45,500 43,900 CSDP Services - alarms, talking books, telephones
69,936 88,400 91,900
Concessionary fares - PD only 244,617 322,400 316,100 Taxicards (inc salaries) 593,820 725,100 736,600 Filling the Gap 2,845 0 0 New IT system funded by CPR 0 0 61,200 Assessment and Care Management
408,433 402,275 384,800
Total* 4,490,119 4,801,286 5,089,000
* Figures exclude income from Performance Improvement Grant and do not allow for Management and Support Costs
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 20
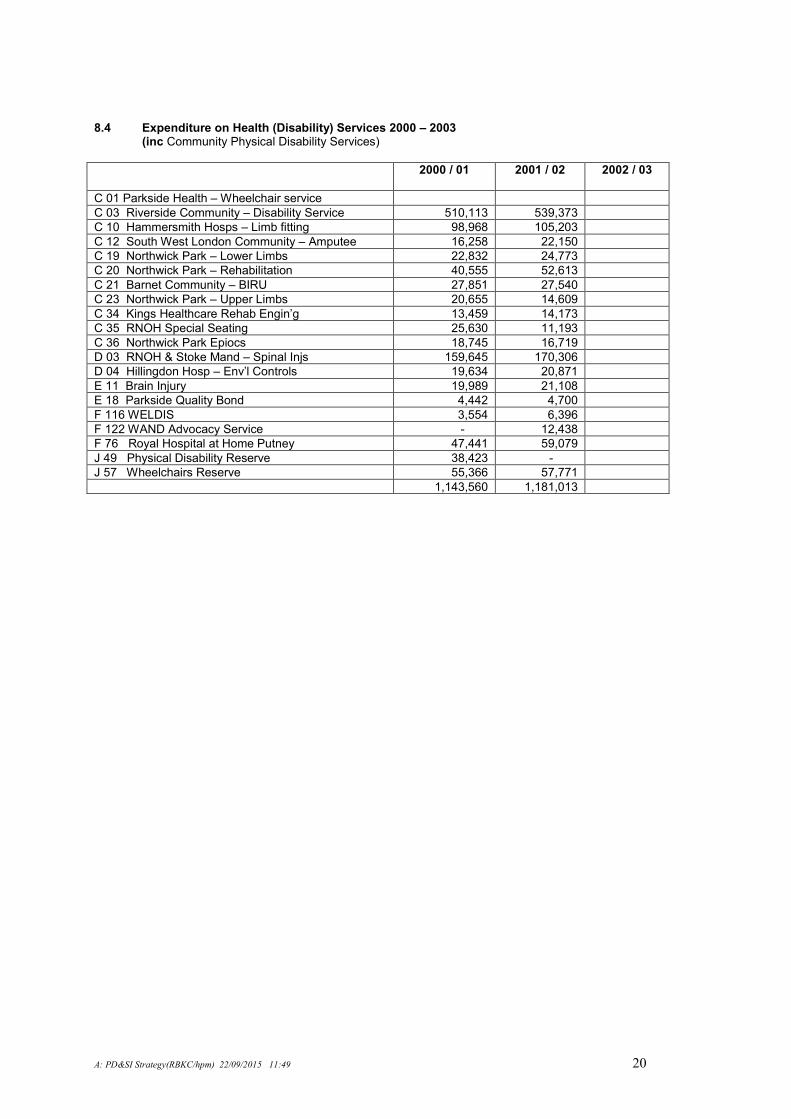
8.4 Expenditure on Health (Disability) Services 2000 – 2003
(inc Community Physical Disability Services)
2000 / 01 2001 / 02 2002 / 03
C 01 Parkside Health – Wheelchair service
C 03 Riverside Community – Disability Service 510,113 539,373
C 10 Hammersmith Hosps – Limb fitting 98,968 105,203
C 12 South West London Community – Amputee 16,258 22,150
C 19 Northwick Park – Lower Limbs 22,832 24,773
C 20 Northwick Park – Rehabilitation 40,555 52,613
C 21 Barnet Community – BIRU 27,851 27,540
C 23 Northwick Park – Upper Limbs 20,655 14,609
C 34 Kings Healthcare Rehab Engin’g 13,459 14,173
C 35 RNOH Special Seating 25,630 11,193
C 36 Northwick Park Epiocs 18,745 16,719
D 03 RNOH & Stoke Mand – Spinal Injs 159,645 170,306
D 04 Hillingdon Hosp – Env’l Controls 19,634 20,871
E 11 Brain Injury 19,989 21,108
E 18 Parkside Quality Bond 4,442 4,700
F 116 WELDIS 3,554 6,396
F 122 WAND Advocacy Service - 12,438
F 76 Royal Hospital at Home Putney 47,441 59,079
J 49 Physical Disability Reserve 38,423 -
J 57 Wheelchairs Reserve 55,366 57,771
1,143,560 1,181,013
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 21
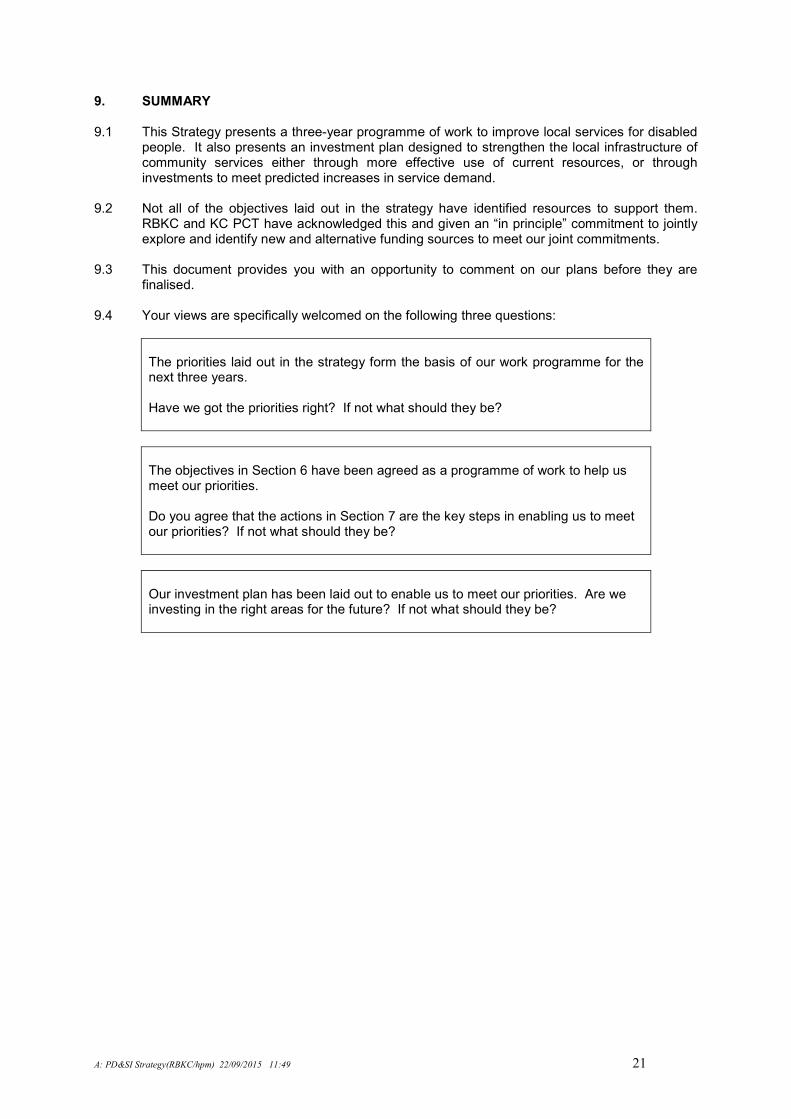
9. SUMMARY 9.1 This Strategy presents a three-year programme of work to improve local services for disabled
people. It also presents an investment plan designed to strengthen the local infrastructure of community services either through more effective use of current resources, or through investments to meet predicted increases in service demand.
9.2 Not all of the objectives laid out in the strategy have identified resources to support them.
RBKC and KC PCT have acknowledged this and given an “in principle” commitment to jointly explore and identify new and alternative funding sources to meet our joint commitments.
9.3 This document provides you with an opportunity to comment on our plans before they are
finalised. 9.4 Your views are specifically welcomed on the following three questions:
The priorities laid out in the strategy form the basis of our work programme for the next three years. Have we got the priorities right? If not what should they be?
The objectives in Section 6 have been agreed as a programme of work to help us meet our priorities. Do you agree that the actions in Section 7 are the key steps in enabling us to meet our priorities? If not what should they be?
Our investment plan has been laid out to enable us to meet our priorities. Are we investing in the right areas for the future? If not what should they be?
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 22
Service users, carers, service providers, voluntary organisations and advocacy groups are invited to respond to the following questions in writing. We would also be pleased to hear any other comments you wish to make. You can use this page to reply if you wish. Please send your replies: The Partnership Group (Disabilities) C/o Hector Medora Town Hall, Hornton Street, London W8 7NX Or telephone Hector Medora on 020 7361 2408 or Trish Welton on 020 7361 2353.
Have we got the priorities right? If not what should they be?
Do you agree that the actions laid out in Section 7 are the key steps in enabling us to meet our priorities? If not what should they be?
Are we investing in the right areas for the future? If not what should they be?
Other comments?
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 23
APPENDICES
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 24
Appendix 1 Questionnaire (December 2000)
Physical Disability
And Sensory Impairment services
- Planning for Improvement
Westminster City Council
Kensington, Chelsea & Westminster Health
Authority
Royal Borough of Kensington and
Chelsea
Your views count The agencies above and others are working closely together as part of the Government’s drive to make it easier for people with physical disabilities and sensory impairments to use services. To help plan the services needed to achieve this, please tell us what you think about services provided – what’s working well, what’s not working well, and what needs to be improved. How to help Tell us what you think now – either in person, or on the form below, or, alternatively, take the form away, write what you think and return it in the box provided. (If you have any queries about this form, please contact: John Crook, Kensington, Chelsea and Westminster Health Authority, 50 Eastbourne Terrace, London, W2 6LX (Tel 0207 725 3337)).
Our views about the priorities
These are what we think the priorities should be.
But what do you think?
Please tell us overleaf
Your views are important and make a difference
Better Information about services
Improved assessment process Better
deaf/hard of hearing
services (loops/ Minicom signing
Better blind/visually impaired services
Better access to services – communication aids and environmental controls, rehabilitation, specialised services
Greater availability of adapted housing
More information about how users and carers can help plan services
Better access to appropriate equipment
Looking at possibility facilities term care
More culturally sensitive services
Improved wheelchair services
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 25
What things do you like about the services?
What things do you dislike – what doesn’t work well?
What changes to services would make a positive difference to you?
What changes would make a positive difference to others?
What about the things in the surrounding boxes: are there
a) things that are missing? b) Things that are working well and
should be extended?
Anything else?
Please tell us what you think
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 26
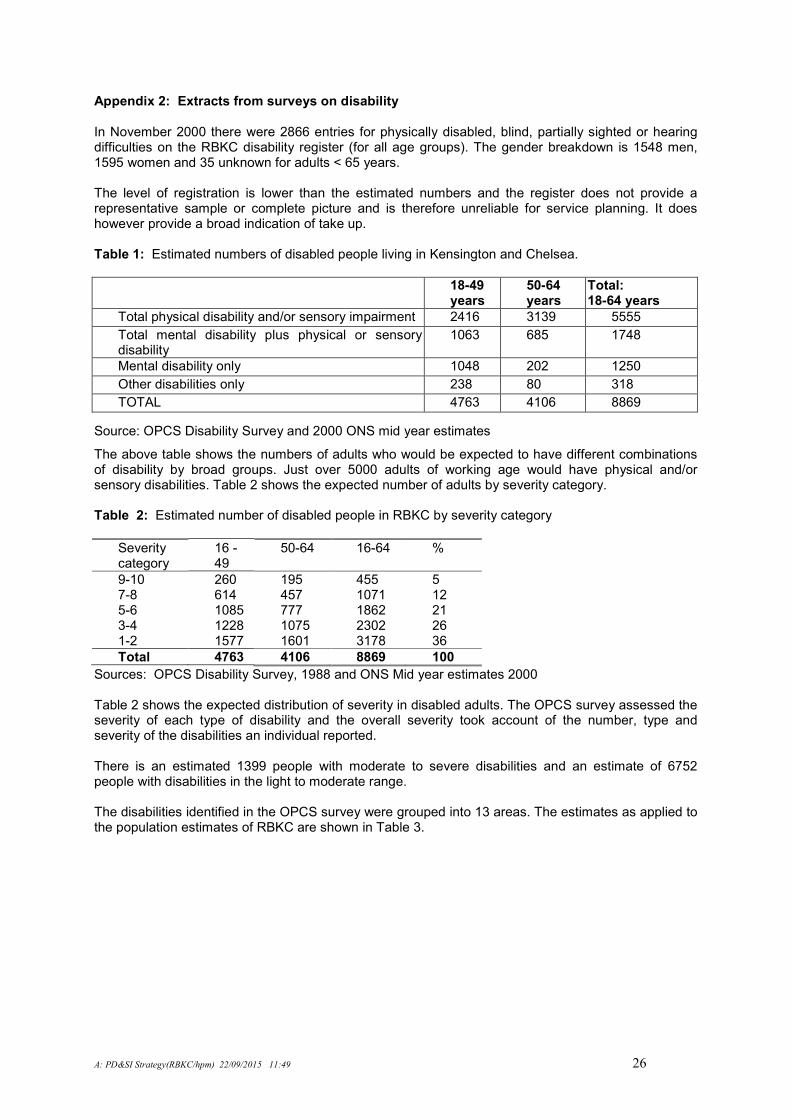
Appendix 2: Extracts from surveys on disability In November 2000 there were 2866 entries for physically disabled, blind, partially sighted or hearing difficulties on the RBKC disability register (for all age groups). The gender breakdown is 1548 men, 1595 women and 35 unknown for adults < 65 years. The level of registration is lower than the estimated numbers and the register does not provide a representative sample or complete picture and is therefore unreliable for service planning. It does however provide a broad indication of take up. Table 1: Estimated numbers of disabled people living in Kensington and Chelsea.
18-49 years
50-64 years
Total: 18-64 years
Total physical disability and/or sensory impairment 2416 3139 5555
Total mental disability plus physical or sensory disability
1063 685 1748
Mental disability only 1048 202 1250
Other disabilities only 238 80 318
TOTAL 4763 4106 8869
Source: OPCS Disability Survey and 2000 ONS mid year estimates
The above table shows the numbers of adults who would be expected to have different combinations of disability by broad groups. Just over 5000 adults of working age would have physical and/or sensory disabilities. Table 2 shows the expected number of adults by severity category. Table 2: Estimated number of disabled people in RBKC by severity category
Severity category
16 - 49
50-64 16-64 %
9-10 260 195 455 5 7-8 614 457 1071 12 5-6 1085 777 1862 21 3-4 1228 1075 2302 26 1-2 1577 1601 3178 36
Total 4763 4106 8869 100
Sources: OPCS Disability Survey, 1988 and ONS Mid year estimates 2000 Table 2 shows the expected distribution of severity in disabled adults. The OPCS survey assessed the severity of each type of disability and the overall severity took account of the number, type and severity of the disabilities an individual reported. There is an estimated 1399 people with moderate to severe disabilities and an estimate of 6752 people with disabilities in the light to moderate range. The disabilities identified in the OPCS survey were grouped into 13 areas. The estimates as applied to the population estimates of RBKC are shown in Table 3.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 27
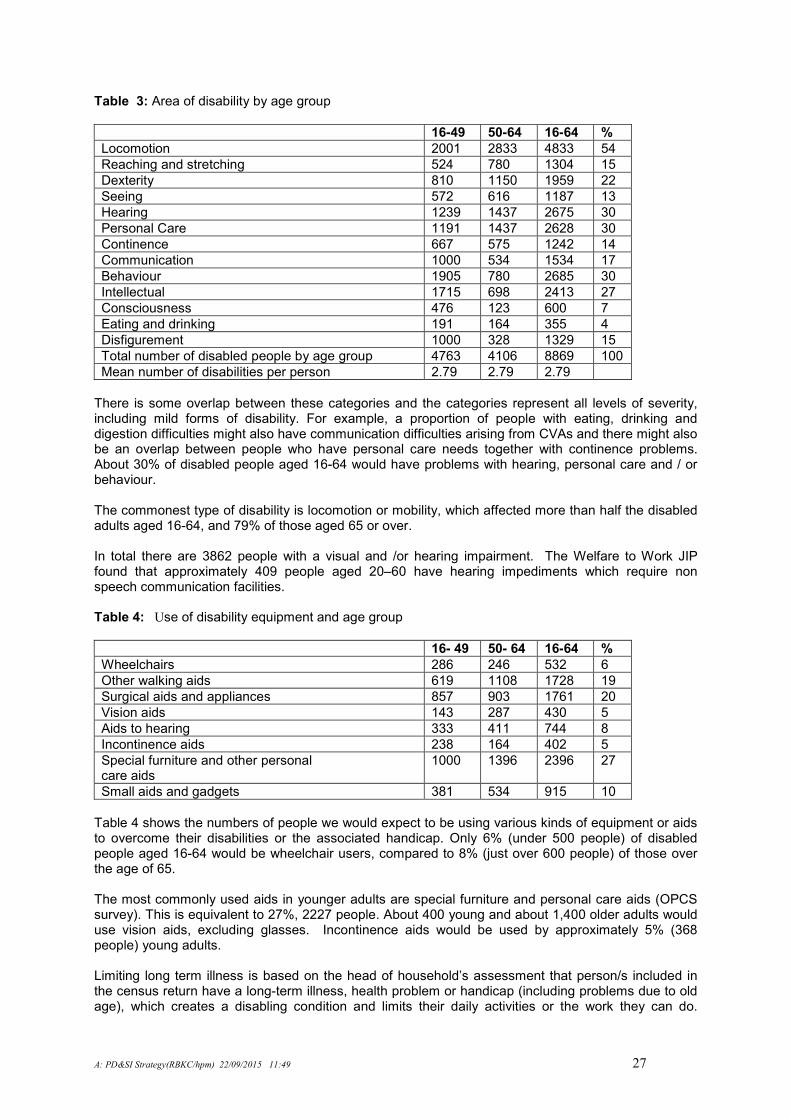
Table 3: Area of disability by age group
16-49 50-64 16-64 %
Locomotion 2001 2833 4833 54
Reaching and stretching 524 780 1304 15
Dexterity 810 1150 1959 22
Seeing 572 616 1187 13
Hearing 1239 1437 2675 30
Personal Care 1191 1437 2628 30
Continence 667 575 1242 14
Communication 1000 534 1534 17
Behaviour 1905 780 2685 30
Intellectual 1715 698 2413 27
Consciousness 476 123 600 7
Eating and drinking 191 164 355 4
Disfigurement 1000 328 1329 15
Total number of disabled people by age group 4763 4106 8869 100
Mean number of disabilities per person 2.79 2.79 2.79
There is some overlap between these categories and the categories represent all levels of severity, including mild forms of disability. For example, a proportion of people with eating, drinking and digestion difficulties might also have communication difficulties arising from CVAs and there might also be an overlap between people who have personal care needs together with continence problems. About 30% of disabled people aged 16-64 would have problems with hearing, personal care and / or behaviour. The commonest type of disability is locomotion or mobility, which affected more than half the disabled adults aged 16-64, and 79% of those aged 65 or over. In total there are 3862 people with a visual and /or hearing impairment. The Welfare to Work JIP found that approximately 409 people aged 20–60 have hearing impediments which require non speech communication facilities. Table 4: Use of disability equipment and age group
16- 49 50- 64 16-64 %
Wheelchairs 286 246 532 6
Other walking aids 619 1108 1728 19
Surgical aids and appliances 857 903 1761 20
Vision aids 143 287 430 5
Aids to hearing 333 411 744 8
Incontinence aids 238 164 402 5
Special furniture and other personal care aids
1000 1396 2396 27
Small aids and gadgets 381 534 915 10
Table 4 shows the numbers of people we would expect to be using various kinds of equipment or aids to overcome their disabilities or the associated handicap. Only 6% (under 500 people) of disabled people aged 16-64 would be wheelchair users, compared to 8% (just over 600 people) of those over the age of 65.
The most commonly used aids in younger adults are special furniture and personal care aids (OPCS survey). This is equivalent to 27%, 2227 people. About 400 young and about 1,400 older adults would use vision aids, excluding glasses. Incontinence aids would be used by approximately 5% (368 people) young adults. Limiting long term illness is based on the head of household’s assessment that person/s included in the census return have a long-term illness, health problem or handicap (including problems due to old age), which creates a disabling condition and limits their daily activities or the work they can do.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 28
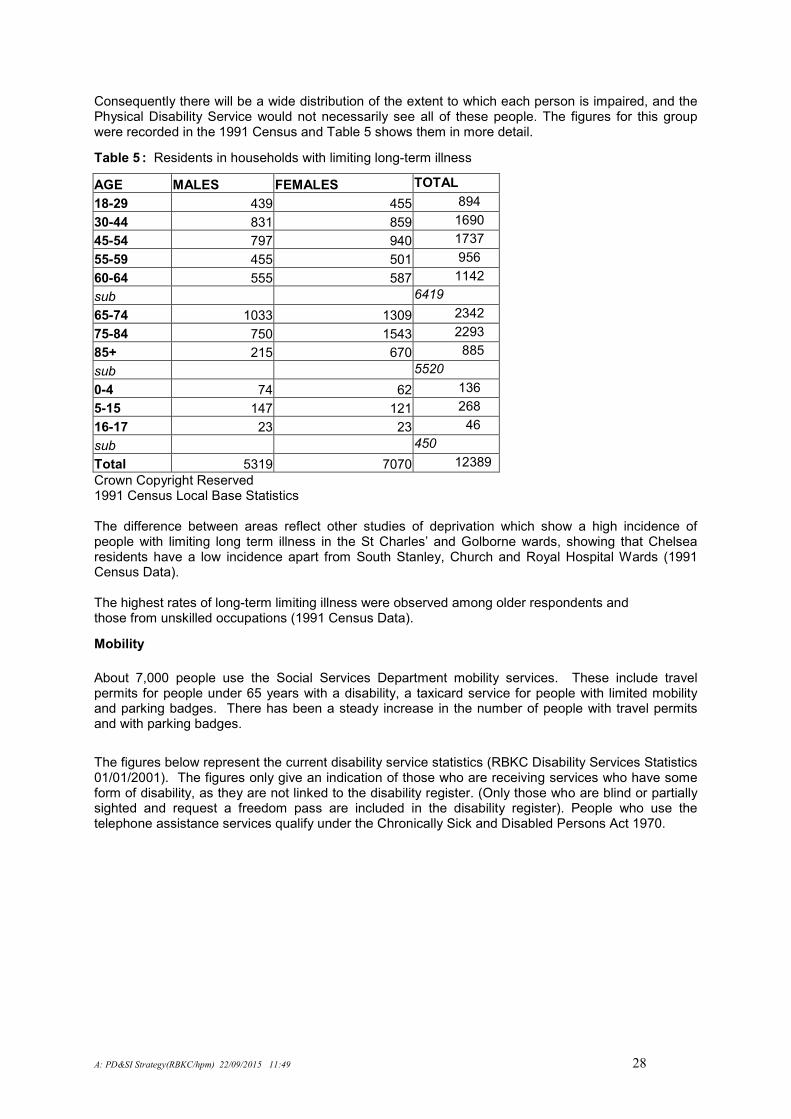
Consequently there will be a wide distribution of the extent to which each person is impaired, and the Physical Disability Service would not necessarily see all of these people. The figures for this group were recorded in the 1991 Census and Table 5 shows them in more detail.
Table 5 : Residents in households with limiting long-term illness
AGE MALES FEMALES TOTAL
18-29 439 455 894
30-44 831 859 1690
45-54 797 940 1737
55-59 455 501 956
60-64 555 587 1142
sub 6419
65-74 1033 1309 2342
75-84 750 1543 2293
85+ 215 670 885
sub 5520
0-4 74 62 136
5-15 147 121 268
16-17 23 23 46
sub 450
Total 5319 7070 12389
Crown Copyright Reserved 1991 Census Local Base Statistics
The difference between areas reflect other studies of deprivation which show a high incidence of people with limiting long term illness in the St Charles’ and Golborne wards, showing that Chelsea residents have a low incidence apart from South Stanley, Church and Royal Hospital Wards (1991 Census Data). The highest rates of long-term limiting illness were observed among older respondents and those from unskilled occupations (1991 Census Data).
Mobility
About 7,000 people use the Social Services Department mobility services. These include travel permits for people under 65 years with a disability, a taxicard service for people with limited mobility and parking badges. There has been a steady increase in the number of people with travel permits and with parking badges.
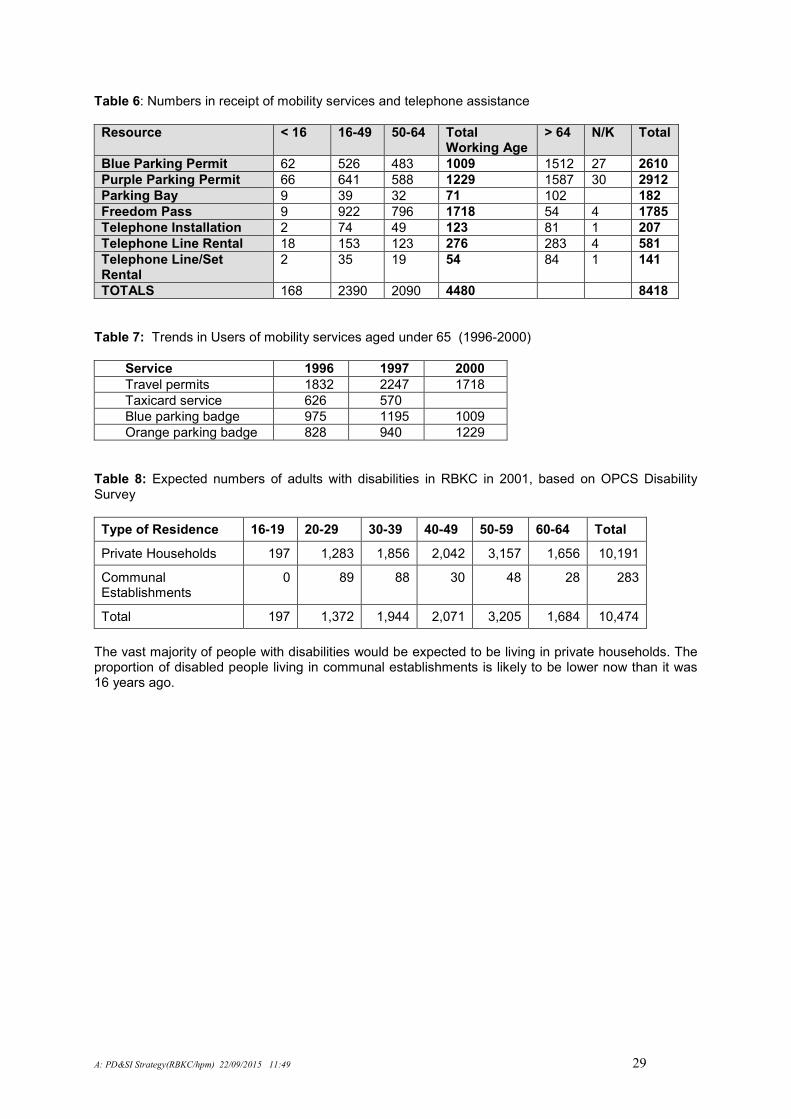
The figures below represent the current disability service statistics (RBKC Disability Services Statistics 01/01/2001). The figures only give an indication of those who are receiving services who have some form of disability, as they are not linked to the disability register. (Only those who are blind or partially sighted and request a freedom pass are included in the disability register). People who use the telephone assistance services qualify under the Chronically Sick and Disabled Persons Act 1970.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 29
Table 6: Numbers in receipt of mobility services and telephone assistance
Resource < 16 16-49 50-64 Total Working Age
> 64 N/K Total
Blue Parking Permit 62 526 483 1009 1512 27 2610
Purple Parking Permit 66 641 588 1229 1587 30 2912
Parking Bay 9 39 32 71 102 182
Freedom Pass 9 922 796 1718 54 4 1785
Telephone Installation 2 74 49 123 81 1 207
Telephone Line Rental 18 153 123 276 283 4 581
Telephone Line/Set Rental
2 35 19 54 84 1 141
TOTALS 168 2390 2090 4480 8418
Table 7: Trends in Users of mobility services aged under 65 (1996-2000)
Service 1996 1997 2000
Travel permits 1832 2247 1718
Taxicard service 626 570
Blue parking badge 975 1195 1009
Orange parking badge 828 940 1229
Table 8: Expected numbers of adults with disabilities in RBKC in 2001, based on OPCS Disability Survey
Type of Residence 16-19 20-29 30-39 40-49 50-59 60-64 Total
Private Households 197 1,283 1,856 2,042 3,157 1,656 10,191
Communal Establishments
0 89 88 30 48 28 283
Total 197 1,372 1,944 2,071 3,205 1,684 10,474
The vast majority of people with disabilities would be expected to be living in private households. The proportion of disabled people living in communal establishments is likely to be lower now than it was 16 years ago.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 30
Appendix 3: Description of Current Services
SOCIAL SERVICES Advocacy An advocacy service is currently being developed for all residents in Kensington and Chelsea in partnership with the local authority and voluntary organisations. If it is required at present, it is purchased from advocacy and interpretation services run by private and independent organisations. Assessment All new referrals for assessment of people with physical disability or sensory impairment go through the Care Management Team, which acts as the gateway to resources. In order to have an assessment by the Disability Care Management Team a person must: “be under 65 and have a permanent physical disability which has a long term adverse effect on their ability to manage daily life. People with a sensory impairment will always be seen by the Sensory Impairment Specialist team. If people have needs which do not fit into the above definition and yet are vulnerable (maybe for example a short term illness which has significantly impacted upon their ability to manage daily life) the social services department may still be able to help and the service user should approach their nearest social services office”.
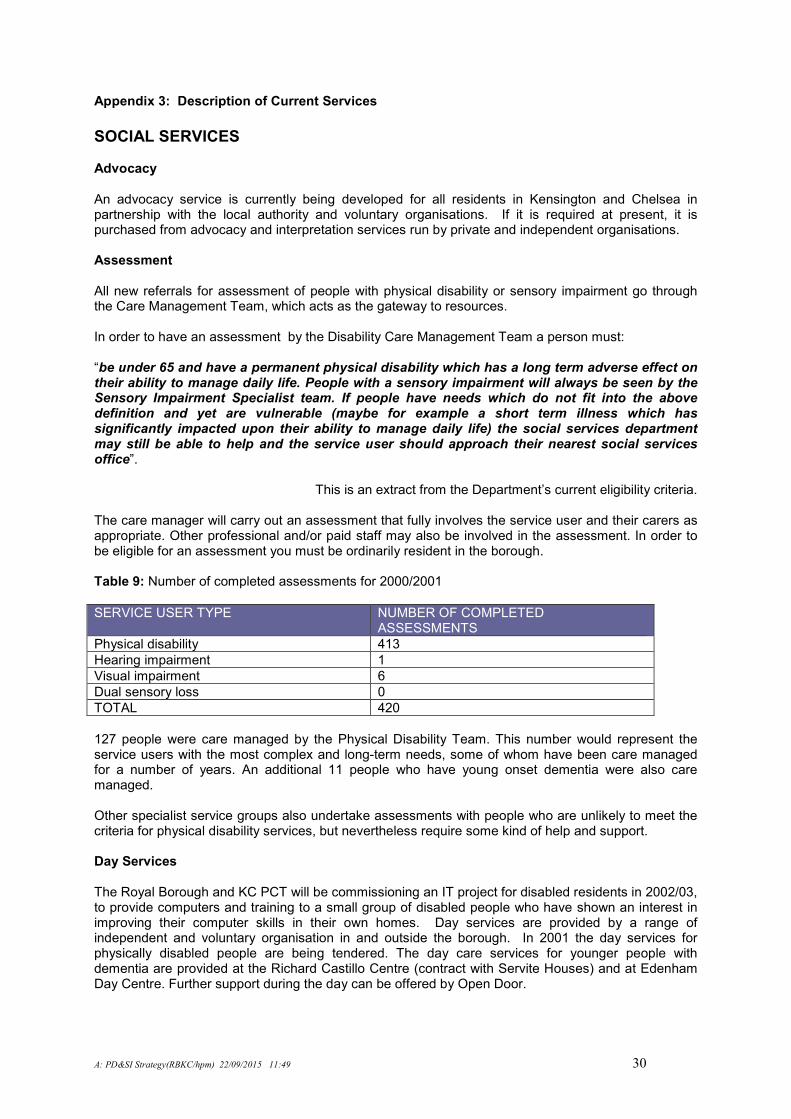
This is an extract from the Department’s current eligibility criteria. The care manager will carry out an assessment that fully involves the service user and their carers as appropriate. Other professional and/or paid staff may also be involved in the assessment. In order to be eligible for an assessment you must be ordinarily resident in the borough. Table 9: Number of completed assessments for 2000/2001
SERVICE USER TYPE NUMBER OF COMPLETED ASSESSMENTS
Physical disability 413
Hearing impairment 1
Visual impairment 6
Dual sensory loss 0
TOTAL 420
127 people were care managed by the Physical Disability Team. This number would represent the service users with the most complex and long-term needs, some of whom have been care managed for a number of years. An additional 11 people who have young onset dementia were also care managed. Other specialist service groups also undertake assessments with people who are unlikely to meet the criteria for physical disability services, but nevertheless require some kind of help and support. Day Services The Royal Borough and KC PCT will be commissioning an IT project for disabled residents in 2002/03, to provide computers and training to a small group of disabled people who have shown an interest in improving their computer skills in their own homes. Day services are provided by a range of independent and voluntary organisation in and outside the borough. In 2001 the day services for physically disabled people are being tendered. The day care services for younger people with dementia are provided at the Richard Castillo Centre (contract with Servite Houses) and at Edenham Day Centre. Further support during the day can be offered by Open Door.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 31
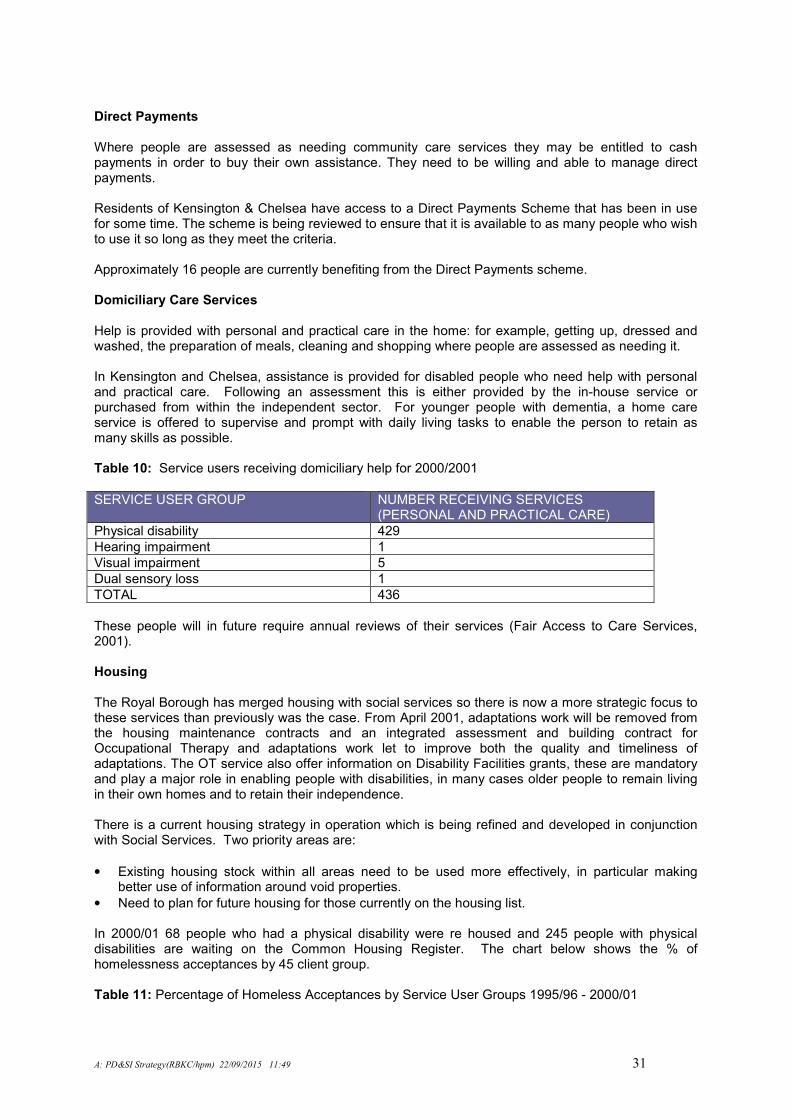
Direct Payments Where people are assessed as needing community care services they may be entitled to cash payments in order to buy their own assistance. They need to be willing and able to manage direct payments. Residents of Kensington & Chelsea have access to a Direct Payments Scheme that has been in use for some time. The scheme is being reviewed to ensure that it is available to as many people who wish to use it so long as they meet the criteria. Approximately 16 people are currently benefiting from the Direct Payments scheme. Domiciliary Care Services Help is provided with personal and practical care in the home: for example, getting up, dressed and washed, the preparation of meals, cleaning and shopping where people are assessed as needing it. In Kensington and Chelsea, assistance is provided for disabled people who need help with personal and practical care. Following an assessment this is either provided by the in-house service or purchased from within the independent sector. For younger people with dementia, a home care service is offered to supervise and prompt with daily living tasks to enable the person to retain as many skills as possible. Table 10: Service users receiving domiciliary help for 2000/2001
SERVICE USER GROUP NUMBER RECEIVING SERVICES (PERSONAL AND PRACTICAL CARE)
Physical disability 429
Hearing impairment 1
Visual impairment 5
Dual sensory loss 1
TOTAL 436
These people will in future require annual reviews of their services (Fair Access to Care Services, 2001). Housing The Royal Borough has merged housing with social services so there is now a more strategic focus to these services than previously was the case. From April 2001, adaptations work will be removed from the housing maintenance contracts and an integrated assessment and building contract for Occupational Therapy and adaptations work let to improve both the quality and timeliness of adaptations. The OT service also offer information on Disability Facilities grants, these are mandatory and play a major role in enabling people with disabilities, in many cases older people to remain living in their own homes and to retain their independence. There is a current housing strategy in operation which is being refined and developed in conjunction with Social Services. Two priority areas are:
• Existing housing stock within all areas need to be used more effectively, in particular making better use of information around void properties.
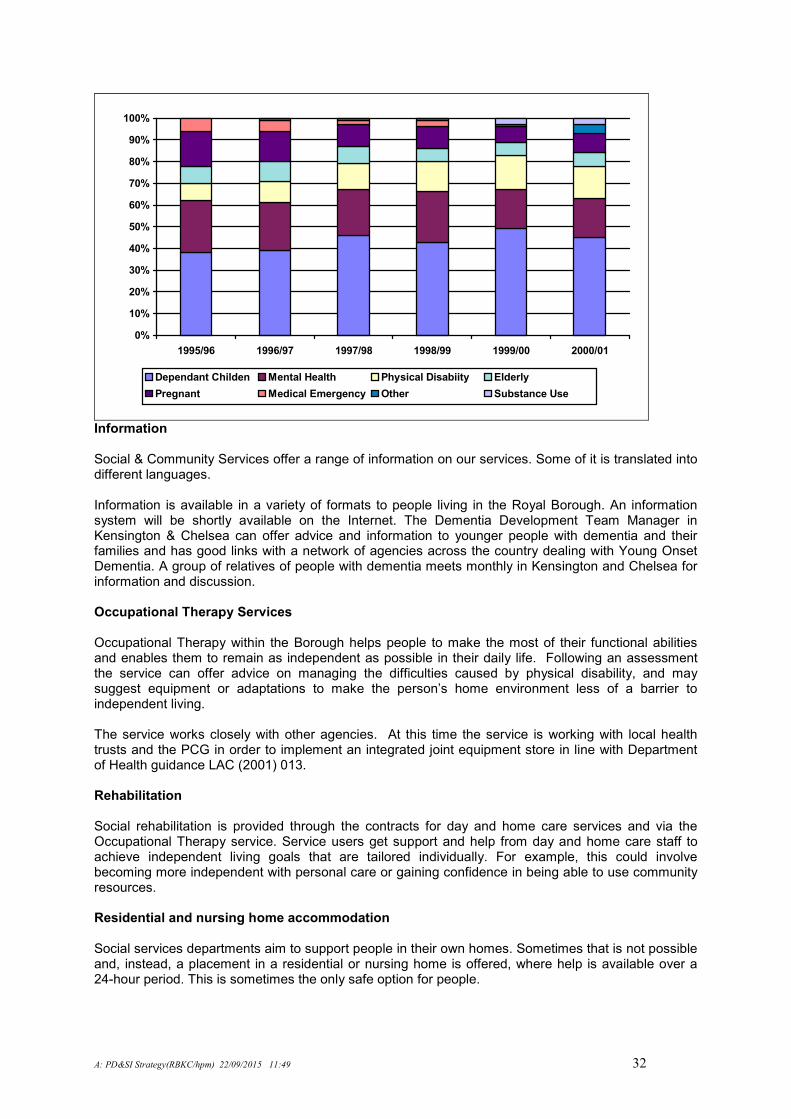
• Need to plan for future housing for those currently on the housing list. In 2000/01 68 people who had a physical disability were re housed and 245 people with physical disabilities are waiting on the Common Housing Register. The chart below shows the % of homelessness acceptances by 45 client group. Table 11: Percentage of Homeless Acceptances by Service User Groups 1995/96 - 2000/01
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 32
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1995/96 1996/97 1997/98 1998/99 1999/00 2000/01
Dependant Childen Mental Health Physical Disabiity Elderly
Pregnant Medical Emergency Other Substance Use
Information Social & Community Services offer a range of information on our services. Some of it is translated into different languages. Information is available in a variety of formats to people living in the Royal Borough. An information system will be shortly available on the Internet. The Dementia Development Team Manager in Kensington & Chelsea can offer advice and information to younger people with dementia and their families and has good links with a network of agencies across the country dealing with Young Onset Dementia. A group of relatives of people with dementia meets monthly in Kensington and Chelsea for information and discussion. Occupational Therapy Services
Occupational Therapy within the Borough helps people to make the most of their functional abilities and enables them to remain as independent as possible in their daily life. Following an assessment the service can offer advice on managing the difficulties caused by physical disability, and may suggest equipment or adaptations to make the person’s home environment less of a barrier to independent living. The service works closely with other agencies. At this time the service is working with local health trusts and the PCG in order to implement an integrated joint equipment store in line with Department of Health guidance LAC (2001) 013. Rehabilitation Social rehabilitation is provided through the contracts for day and home care services and via the Occupational Therapy service. Service users get support and help from day and home care staff to achieve independent living goals that are tailored individually. For example, this could involve becoming more independent with personal care or gaining confidence in being able to use community resources. Residential and nursing home accommodation Social services departments aim to support people in their own homes. Sometimes that is not possible and, instead, a placement in a residential or nursing home is offered, where help is available over a 24-hour period. This is sometimes the only safe option for people.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 33
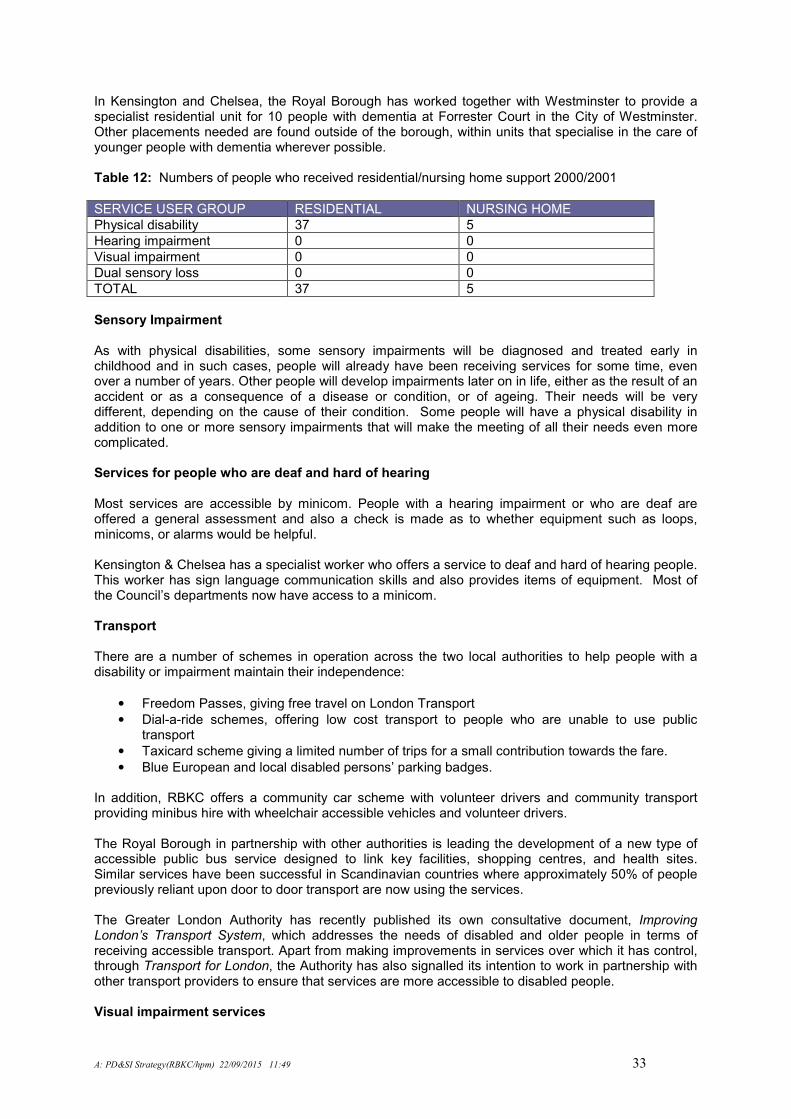
In Kensington and Chelsea, the Royal Borough has worked together with Westminster to provide a specialist residential unit for 10 people with dementia at Forrester Court in the City of Westminster. Other placements needed are found outside of the borough, within units that specialise in the care of younger people with dementia wherever possible. Table 12: Numbers of people who received residential/nursing home support 2000/2001
SERVICE USER GROUP RESIDENTIAL NURSING HOME
Physical disability 37 5
Hearing impairment 0 0
Visual impairment 0 0
Dual sensory loss 0 0
TOTAL 37 5
Sensory Impairment As with physical disabilities, some sensory impairments will be diagnosed and treated early in childhood and in such cases, people will already have been receiving services for some time, even over a number of years. Other people will develop impairments later on in life, either as the result of an accident or as a consequence of a disease or condition, or of ageing. Their needs will be very different, depending on the cause of their condition. Some people will have a physical disability in addition to one or more sensory impairments that will make the meeting of all their needs even more complicated. Services for people who are deaf and hard of hearing Most services are accessible by minicom. People with a hearing impairment or who are deaf are offered a general assessment and also a check is made as to whether equipment such as loops, minicoms, or alarms would be helpful. Kensington & Chelsea has a specialist worker who offers a service to deaf and hard of hearing people. This worker has sign language communication skills and also provides items of equipment. Most of the Council’s departments now have access to a minicom.
Transport There are a number of schemes in operation across the two local authorities to help people with a disability or impairment maintain their independence:
• Freedom Passes, giving free travel on London Transport
• Dial-a-ride schemes, offering low cost transport to people who are unable to use public transport
• Taxicard scheme giving a limited number of trips for a small contribution towards the fare.
• Blue European and local disabled persons’ parking badges. In addition, RBKC offers a community car scheme with volunteer drivers and community transport providing minibus hire with wheelchair accessible vehicles and volunteer drivers. The Royal Borough in partnership with other authorities is leading the development of a new type of accessible public bus service designed to link key facilities, shopping centres, and health sites. Similar services have been successful in Scandinavian countries where approximately 50% of people previously reliant upon door to door transport are now using the services. The Greater London Authority has recently published its own consultative document, Improving London’s Transport System, which addresses the needs of disabled and older people in terms of receiving accessible transport. Apart from making improvements in services over which it has control, through Transport for London, the Authority has also signalled its intention to work in partnership with other transport providers to ensure that services are more accessible to disabled people. Visual impairment services
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 34
All service users whose ophthalmic surgeons have assessed them as being partially sighted or blind, will be offered an assessment once social services receive notification from the doctor (on the form BD8). A general assessment to identify need is offered and this could lead to the issue of equipment or some form of rehabilitation, for example indoor or outdoors mobility training. Help for people to access education, leisure and employment services can also be provided if necessary. Kensington & Chelsea has a specialist team offering services to people with visual impairments. The Registration Officer visits all newly registered people whilst the care manager undertakes needs assessments. The rehabilitation worker offers practical assistance including mobility training. The Royal Borough also has a contract with Sense offering guide communication for people with a dual sensory loss.
SPECIALIST HEALTH SERVICES Some disabilities are genetic and therefore identified early on in childhood. Unless the person has a deteriorating condition, their needs ought to remain relatively stable until they enter the adult disability services at 18. The health and local authorities have developed a comprehensive children’s disability register that will allow for easier transfer to adult services. However, there may well be some issues around this transition from children’s to adult services such as need to ease the transition; also, because services are provided separately, there may well be issues around the separate criteria for equipment, where equipment provided by one service is not provided by another or where equipment provided by children’s services cannot continue to be used in adult services. When adults develop a physical disability, whether as the result of an accident or the development of a disease, their needs have to be assessed for the first time. The care pathways will be very different, depending on the cause. Some people with physical disabilities will also have sensory impairments that will call for a great deal of close co-ordination between the teams responsible for their care. In these cases, different streams for funding care may make it difficult for all their needs to be met. Acute/Secondary Care The two major acute Trusts serving the Borough are St Mary’s Hospital Trust and the Chelsea and Westminster Hospital Trust. Residents in the south of the Borough may also use St Thomas’ and Guy’ NHS Trust and Charing Cross Hospital Trust as these are more geographically convenient. Chronic/Progressive/Deteriorating Conditions There are a number of deteriorating conditions, such as Parkinson’s Disease, Huntington’s Disease, Multiple Sclerosis, Cystic Fibrosis, Young Onset Dementia, and Creuzfeld Jacob’s Disease, some of which can go into remission. The challenge for health and social services is to provide appropriate care that matches the individual’s changing needs. Community Brain Injury Service This is a KCW-wide service that has been established in 1999 for three years as a research and development project to establish the need for and make recommendations for a future community service (Appendix 6). It is an innovative project and is funded through Joint Finance and commissioned by the Partnership Group (Disability) in Westminster and Kensington & Chelsea. It offers direct rehabilitation. The setting up of this service has already facilitated the gathering of a great deal of information to inform future developments in the services for this “hidden” disability: this has led to the setting up of a joint project to examine the needs of this client group and to examine the feasibility of commissioning a long-term care facility closer to KCWHA, in collaboration with neighbouring Health Authorities. Community Care The two Community Trusts, Riverside and Parkside, both provide a range of local services to support people in their own homes: district nursing; occupational therapy; and speech and language therapy.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 35
In addition to this, Parkside Trust provides a comprehensive mainstream wheelchair service covering the whole of KCWHA as well as rehabilitation services at the Youth Disability Unit at Willesden and St Charles’ Hospitals and an Independent Living Team based at Willesden and serving the northern part of the district. Riverside Community Trust runs a Disability Service covering the whole of KCWHA, arranging packages of continuing health and social care for people who need it following their return to the community after they have received hospital care, in close collaboration with the two boroughs’ social services departments. Further information on NHS continuing care services and the financial pressures in this area is contained in Appendix 5. Diagnosis Most diagnoses will take place in acute hospitals and, occasionally, in specialist centres at the tertiary level, particularly so if the needs are complex or rare. Some diagnoses of diseases will take place in General Practice with people being referred on to a specialist in the acute sector for confirmation and a suitable treatment programme embarked upon. Holderness Centre, Charing Cross Hospital This Centre provides a prosthetic limb fitting service. Joint/Full NHS Care The Disability Service of the Riverside Community Health Trust is responsible for the commissioning of services for those disabled who need continuing care in the community, either because of a deteriorating condition or following discharge from an acute hospital or a specialist, tertiary centre, in close co-operation with the social services departments in the two boroughs. Financial pressures on this service and the effects of changes to the continuing care criteria in KCWHA are detailed in Appendix 4. Lower Limbs, Upper Limbs, Special Seating, Electrically Powered Indoor Outdoor Chairs (EPIOCs), Rehabilitation Engineering and Environmental Controls These consortia are for services based at Northwick Park Hospital, Hillingdon Hospital and the Disabled Services Centre at Stanmore. They provide specialist, technical aids to those with very severe and complex disabilities. Palliative Care Some disabling conditions will in time lead to death. The Riverside Disability Services arrange suitable care in these circumstances. For certain neurological conditions, such as Persistent Vegetative State, Creuzfeld-Jacob’s Disease and the latter stages of Huntington’s Disease, patients will be placed at the Royal Hospital for Neurodisability at Putney, mainly under continuing NHS care. For other, deteriorating conditions, people will be placed in nursing homes or hospices where their needs can be fully met and where they will be able to die with dignity. Primary Care The vast majority of KCW residents, including those with a pre-existing disability, will access health care through their GP practice. GPs and practice nurses are in an ideal position to monitor and identify the early onset of sensory impairments that affect those in middle age and older. Regional Rehabilitation Unit, Stanmore This is a specialist tertiary centre that provides a Specialist Rehabilitation Service for patients with severe, complex disability, which may include physical, cognitive and communication problems. Respite Care
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 36
For people with complex conditions or those whose behaviour is challenging, it is important that respite services are available either for service users, the carers or their relatives. The Riverside Disability Service is able to arrange for respite care for those care packages for which it is responsible. Royal Hospital for Neurodisability (RHND), Putney KCWHA has an agreement with RHND to provide a range of rehabilitation services for patients with a severe disability, including the Behaviour Development Unit and the Transitional Living Unit. South West London Community Trust A small prosthetic service is provided at St Mary’s Roehampton, mainly for people living in south of KCWHA. Specialised Services – individual agreements KCWHA has a number of individual agreements for services for people with a physical disability. Specialist Services – Consortia The Health Authority participates in a number of consortia with other Health Authorities to provide care for disabled people. These are provided in this way because the numbers needing the service are relatively small, but are of high cost. By pooling resources with other Health Authorities, the financial risks of providing the service are shared more evenly and those providing the service are guaranteed funding to continue with the development of those services. Specialist Services – Joint Finance KCWHA, together with RBKC fund a number of services: Day Services: This jointly financed project between KCWHA and RBKC aims to provide personal computers and bespoke training to a range of 10-12 interested disabled people in their own homes. Brain Injuries Project:
Spinal Injuries Consortium This consortium provides services based at the Royal National Orthopaedic Hospital (RNOH) at Stanmore and at Stoke Mandeville.
INDEPENDENT SECTOR Action Disability Kensington & Chelsea (ADKC) ADKC provide a number of services to disabled people with physical & sensory impairments. Information & Advice: The information service is available on the telephone in person at the ADKC centre or can be arranged with a home visit. The service is available to disabled people, their carers, and professionals. The information service also produces a six weekly newsletter and several fact sheets throughout the year. Independent Living Project: This new project is to support disabled people to live independently. The project also focuses on direct payments and managing your own personal assistance. Leisure & Community Project: ADKC provide a monthly programme of activities that are organised. The project also supports individuals to access local leisure opportunities.
Lifelong Learning Project: This project support individuals to access any form of learning, including college courses, vocational and/or recreational learning.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 37
Volunteer Project: ADKC recruit volunteers to support individuals in two ways, firstly by offering a help service, e.g. gardening, taking curtains down etc. Additionally it provides a matching scheme to enable disabled people to have a volunteer to accompany them on something of interest to both the volunteer and the disabled person. Young Persons Project: to support young disabled people aged 14 – 25 to access services and develop self-advocacy. Additional Services: ADKC also receives funding to provide a counselling service as required. They have a weighing scale for wheelchair users and are able to provide passport photo service. Cultural Groups The Migrant Refugee Forum based in the north of the Borough recently worked jointly with the sensory impairment team to undertake a study of the needs of visually impaired people from ethnic minority groups. It is very much hoped that the recommendations from this report can be taken forward to develop services to include all aspects of disability. RNIB The Royal Borough funds an outreach service based at Garrow House, Kensal Road. One full time and 2 part time workers offer support, advice and information to all Borough residents. There is a range of equipment for service users to test out and they can help arrange a befriending service and volunteers to assist at home. SENSE The Royal Borough funds Sense to provide a guide communicator scheme for people with a dual sensory loss who need assistance with guiding and communication. There are currently 15 people using the scheme and guide communicators can assist with shopping, correspondence etc. (To be expanded)
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 38
Appendix 4: NHS Continuing Care Services (? Amend)
NHS continuing care across KCWHA is administered by the Riverside Disability Services on behalf of KCWHA, which allocates a budget to meet the continuing health care needs of disabled people under the age of 65. Joint funding of services between the Health Authority and its local authority partners enables the purchase of good quality placements for those clients with brain injury and challenging behaviour and allows people who have very high health and social care needs to stay in their own homes or in the community. In July 2000, the criteria for full NHS continuing care in KCWHA were changed, in line with the Coughlan judgement. These are shown below. The criteria are currently being reviewed as a result of a government directive. Historically, the expenditure on disability services is unpredictable, being low volume, but high cost, as the table below illustrates. Survivors of traumatic injuries, including brain injury, require high levels of care and, with improved health care, are now surviving longer. There has been an increase in the number of clients receiving full NHS care since the changes to the continuing care criteria in July which has meant that a number of clients managed by the Disability Service now qualify for full NHS care. Increased longevity of clients has also resulted in a steady increase in the number of clients over the years. Expenditure Trends
£
1994/95 3 358,100
1995/96 3 388,700
1996/97 362,500
1997/98 410,000
1998/99 444,700
1999/2000 4 439,000
2000/2001 5 508,215
2001/2002 (projected)
670,000
It is clear that the upward trend in placements and costs will continue over the period, especially so given the need to provide clients with placements as close to home as possible and in the community. Criteria for Fully Funded NHS Continuing Health Care To be considered under these criteria patients must be between 18 and 64 years old and registered with a GP in a KCW Primary Care Group or unregistered
1 at the point of assessment.
The criteria will continue to apply to people of 65 or over assessed as meeting these particular criteria before their 65
th birthday until and unless their needs change, at which point they will be re-assessed
against the appropriate criteria. People 65 or over with needs resulting from traumatic injury, rather than old age, will be considered on a “case by case” basis.
Patients who have on-going neurological dependency, characterised by any one or more of the following, will automatically be eligible for fully funded NHS continuing care:
• Unconsciousness;
• Mechanical ventilation;
• Persistent vegetative state (following review by appropriate consultant physician). Other patients will be eligible for continuing care if they have deteriorating or unstable conditions that require constant monitoring and any two of the following conditions.
1 Patients not registered with any GP are allocated to the Primary Care Group in which they are ordinarily resident for the
purposes of NHS funding.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 39
• Chronic and unremitting double incontinence that is not responsive to medical treatment;
• Pressure sores, which have not responded to treatment and now require specialist equipment2
on an on-going basis;
• Chronic immobility, compounded by a medical condition rendering a patient at risk of physical injury during transfers;
• Long-term tube feeding, e.g. PEG3, or nasogastric tube;
• Complex medical regimens, including parental drugs necessitating regular consultant supervision.
• Severe and frequent challenging behaviour which presents a danger to themselves or others and which requires specialist nursing/medical/psychological management OR significant disabilities complicated by a history of severe and enduring mental health needs, substance misuse or early onset dementia requiring frequent intervention from a specialist consultant.
Additional NHS Health Care Support for Patients Not Meeting Full NHS Criteria The general criteria apply also in this section. They apply both to people whose continuing care needs will be met in residential and nursing home care and at home. All patients covered by the Kensington & Chelsea and Westminster HA Primary Care Groups are eligible for the full range of general community health care services that are provided. Patients, who receive local authority funded care will, if appropriate, receive additional health care services. These are set out below. All patients will be offered a multi-disciplinary assessment. The assessment will identify any health care needs beyond that which general community health care services and a patient’s General Practitioner can meet. For placements outside KCW, the host Health Authority is responsible for meeting the general health needs. KCWHA remains responsible for any additional health care agreed before placement. The range of specific NHS services that may be provided is as follows:
Additional specialist nursing care over and above that normally provided by a nursing home or district nursing service:
• Specialist pain relief;
• Additional mental health and/or psychological treatment or care;
• Additional therapy services over and above those normally provided, such as speech therapy, physiotherapy, occupational therapy and podiatry services.
• Nursing equipment or care not normally provided in a residential, nursing home or in a patient’s own home (e.g. PEG feeding equipment, specialist mattresses, management of a ventilator or dialysis).
• Advice, e.g. psychology, on the management of cognitive/behavioural problems associated with disability or traumatic head injury;
2 Specialist equipment would involve special beds, chairs and splints ordered on an individual basis.
3 Percutaneous endoscopy gastronomy = feeding tube placed in the stomach for people unable to eat (or eat sufficient
quantities).

A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 40
• Advice generally provided by the local NHS community trust, for matters such as tissue viability issues, continence and dietetics.
• Training and education on supporting health needs for carers and care workers.
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 41
Appendix 5: Glossary of Terms and Abbreviations AIDS: Acquired Immune Deficiency Syndrome Audiology: This is a branch of medicine dealing with the diagnosis, medical treatment, habituation and rehabilitation of children and adults with disorders of hearing and balance BD8: A form used in England and Wales to certify and register patients as blind or partially sighted. Brain Injury: There are two categories of brain injury, acquired and traumatic. Acquired and traumatic brain injuries have overlapping symptoms yet are very distinct from each other. Acquired brain injury is an internal disorder caused by neuro-organic malfunctions. Traumatic brain injuries are externally caused, as in car accidents, sports injuries and physical assaults. CVA: Cerebal Vascular Accident (Stroke) Creutzfeldt-Jakob Disease: Creutzfeldt-Jakob Disease ("CJD") is a rare, fatal brain disorder that causes a rapid, progressive dementia and associated neuromuscular disturbances. The disease is often referred to as a sub acute spongiform encephalopathy because it usually produces microscopic vacuoles in neurons that appear "sponge-like". Cystic Fibrosis: This causes the body to produce an abnormally thick, sticky mucus, due to the faulty transport of sodium and chloride (salt) within cells lining organs such as the lungs and pancreas, to their outer surfaces. The thick CF mucus also obstructs the pancreas, preventing enzymes from reaching the intestines to help break down and digest food. Disabled: This includes people with physical disabilities, sensory impairments, early onset dementia, brain injury and other traumatic injuries. EPIOC: Electrically Powered Indoor and Outdoor Chairs. Epidemiology: Epidemiology is the study of the distribution and determinants of diseases in the population; clinical epidemiology is the application of the same sorts of principles and methods to the diagnosis and treatment of disease HImp: Health Improvement and Modernisation Plan HIV: Human immunodeficiency virus, a retrovirus that causes Aids. HSE: Health Survey for England 1995 Huntington’s Disease: Huntington’s Disease is an inherited degenerative neuropsychiatric disorder that affects both body and mind. Symptoms most commonly begin between the ages of 35 and 50, although onset may occur any time from childhood to old age. JIP: Joint Investment Plan KCWHA: Kensington and Chelsea and Westminster Health Authority. LAC: Looked After Children LFS: Labour Force Survey 1999 Multiple Sclerosis: Multiple sclerosis is a chronic, often disabling disease of the central nervous system. Symptoms may be mild such as numbness in the limbs or severe paralysis or loss of vision. NHS: National Health Service NSF: National Service Framework
A: PD&SI Strategy(RBKC/hpm) 22/09/2015 11:49 42
OPCS: Orthotic: An artificial support or brace for the limbs or spine. PCG: Primary Care Group PCT: Primary Care Trust Parkinson’s Disease: Parkinson's disease belongs to a group of conditions called motor system disorders. Parkinson's and related disorders are the result of the loss of dopamine producing brain cells. Loss of dopamine causes the nerve cells to fire out of control, leaving patients unable to direct or control their movement in a normal manner. The four primary symptoms of Parkinson's are tremor or trembling in hands, arms, legs, jaw, and face; rigidity or stiffness of the limbs and trunk; bradykinesia, or slowness of movement; and postural instability or impaired balance and coordination Persistent Vegetative State: Patients in this vegetative state have no cerebral cortical function, meaning that they are unconscious and unaware, but exhibit sleep-wake cycles with either full or partial hypothalamic and brain stem autonomic functions. A persistent vegetative state is considered to be permanent when a diagnosis of irreversibility can be established based on the fact that the chances that the patient will regain consciousness are exceedingly small. Prosthetic: The branch of surgery concerned with the making and fitting of artificial body parts. Young Onset Dementia: Dementia is a syndrome due to disease of the brain, usually of a chronic or progressive nature, in which there is disturbance of multiple higher cortical functions, including memory, thinking, orientation, comprehension, calculation, learning capacity, language, and judgement. Consciousness is not clouded. Impairments of cognitive function are commonly accompanied, and occasionally preceded, by deterioration in emotional control, social behaviour, or motivation.
(To be expanded)