Embed Size (px)
Citation preview

Keeping afloat on golden pond : Stonechurch Seniors Collaborative Care Program
March 25, 2010
Stonechurch Family Health Centre, Hamilton ON

Overview
• Seniors at Stonechurch• Pilot study
– Objectives– Methods– Results
• Seniors Collaborative Care Program • Lessons learned

Seniors at Stonechurch
• 1,515 patients at SC > 65 years
• 20 % of visits at SC with seniors
(January 2009 – January 2010)
The Study Team
• Joy White - Nurse Practitioner• Shelly House – Pharmacist• Rachelle Gervais - Nurse• Ainsley Moore – Family md• Kalpana Nair - Research Assistant• AJ Kadhim –Research support• Chris Patterson - Geriatrician

Pilot Study
Funding:DFM Pilot study (May 2008)
Research Question: What is the feasibility of implementing
interdsiciplinary program program to address seniors at risk of CI and or falling at SCFHC

Pilot Study
Create the program:
• Standardize approach to cognitive impairment and risk of falls
• Establish a model - maximize provider input, continual feedback, communication

Pilot Study Recruit patients: • Telephone screening
Evaluate:• Feasibility and acceptability

Pilot StudyStandardize Approach Screens depression, medications, nutrition• GDS. Levy, SCREEN
Algorithm for assessment of cognitive assessment • ADEPT, CMAJ (Third Consensus on the Diagnosis and
Treatment of Dementia)
Algorithm for assessment of falls• ACOVE III, Health Canada, Cochrane

Collaborative Model
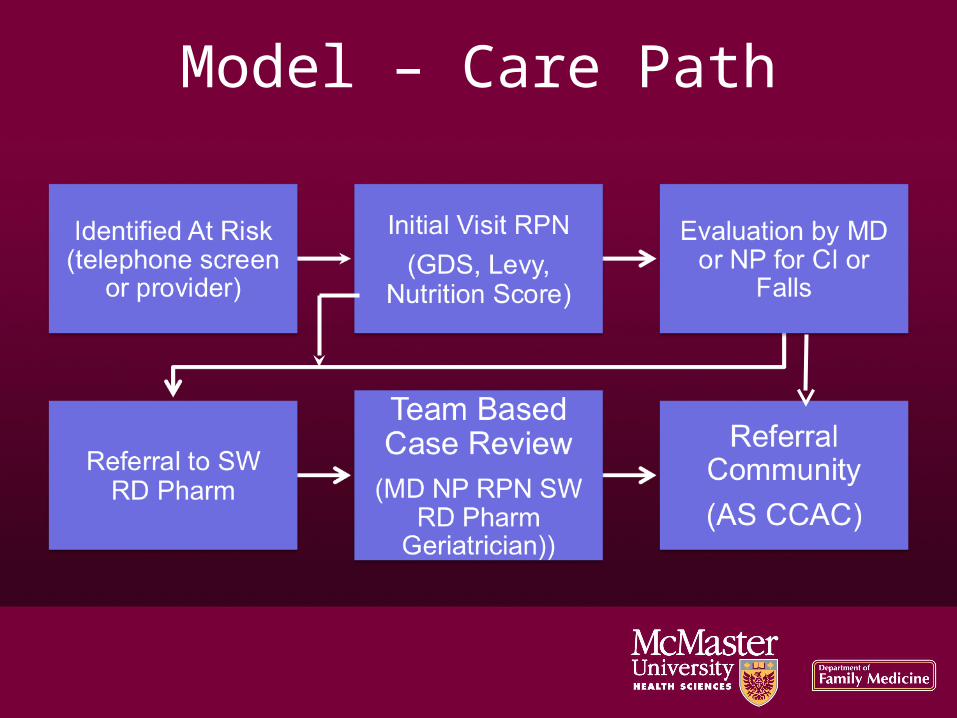
Model – Care Path

Pilot Study
Recruit Patients:
Random identification of seniors over 75 yrs at SCFHC
Screening for risk of CI and or falls

Pilot Study
Screening Questions:
Cognitive Impairment (verbal fluency -11 four legged animals in 60
seconds)
Risk of Falling (fear of falling, fall with injury, fall in the past yr)
Pilot Study
Evaluate feasibility (objectives) 1. Telephone screening to identify seniors at
risk of CI and or falling2. Logistics (patient and provider time involved
with the program) 3. Acceptability of program to patients and
providers
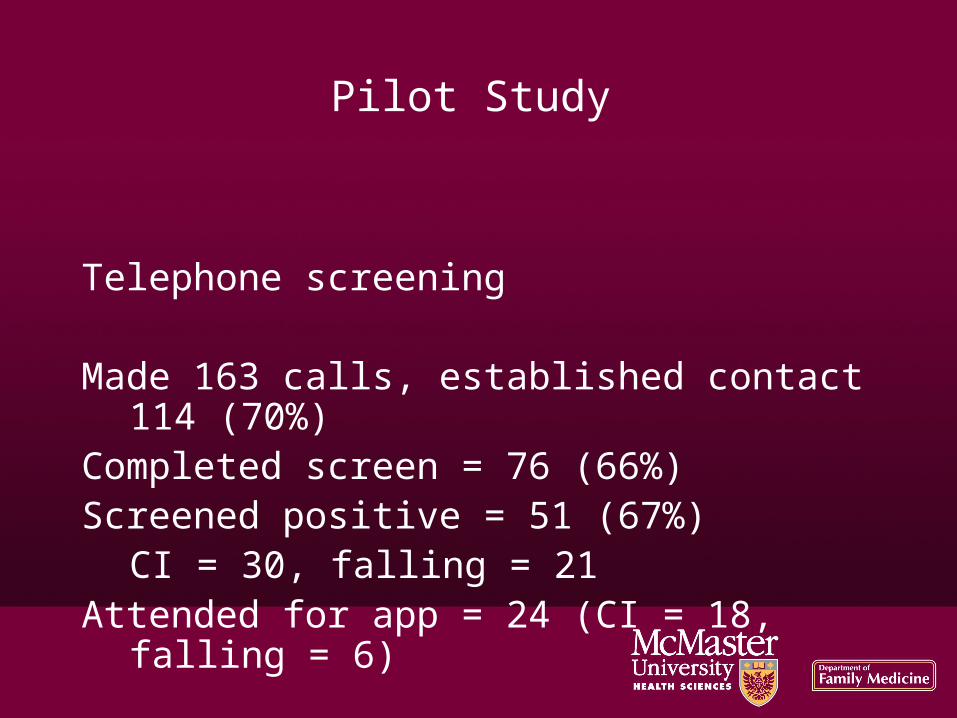
Pilot Study
Telephone screening
Made 163 calls, established contact 114 (70%)Completed screen = 76 (66%)Screened positive = 51 (67%)
CI = 30, falling = 21Attended for app = 24 (CI = 18, falling = 6)
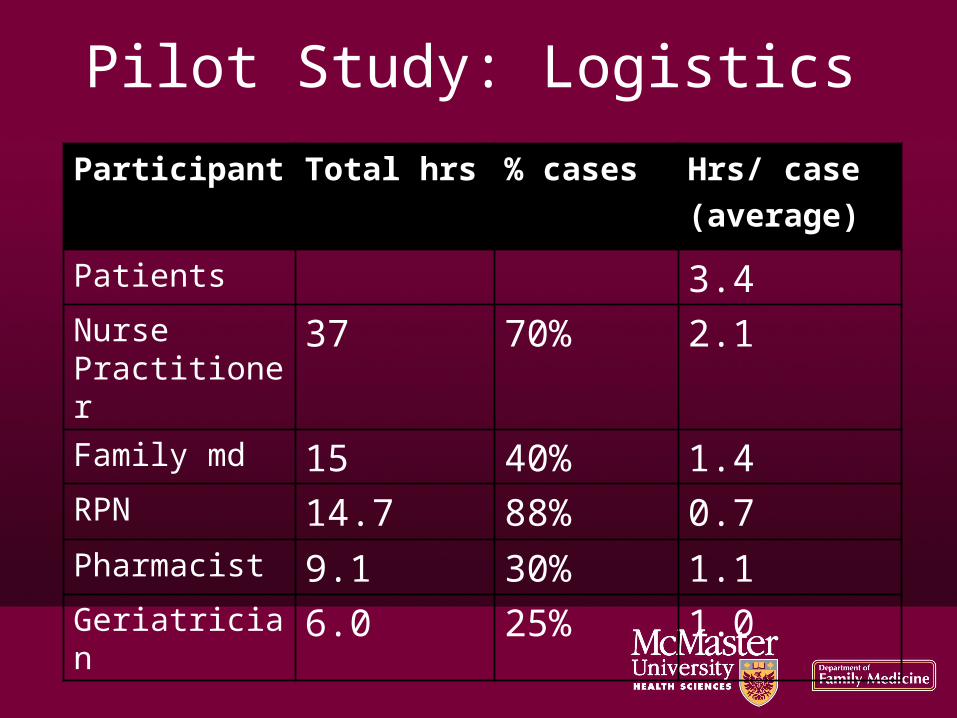
Pilot Study: Logistics
Participant Total hrs % cases Hrs/ case
(average)
Patients 3.4Nurse Practitioner
37 70% 2.1
Family md 15 40% 1.4RPN 14.7 88% 0.7Pharmacist 9.1 30% 1.1Geriatrician 6.0 25% 1.0
Summary
• Telephone Screening (Bad idea)
• Referral process much more efficient
• Logistics
• Provider time varies in concentration and total involvement

Acknowledgements
• Department of Family Medicine (pilot funding)• Hamilton FHT: Carrie McAiney• Seniors of SCFHC • CCAC: Nancy Easson• Alzheimer’s Society (Mary Burnett)• Lisa Dolovich• Chris Patterson

Acceptability of SCCP
• Objectives
• Methods
• Results

Objectives
• Experience of patients• Level of satisfaction• Program’s strengths• Areas of improvement• Program’s worth for seniors
• Experience of providers• Feasibility and worthwhile of expanding program• Clinician’s demographics
Methods
• Qualitative interviews• Patients, MDs and RPNs• In person or over telephone• 15-30 minutes • 5-point scale ratings & room for comments
Interview Guide1. a) Please rate your overall satisfaction with the SCCP
on a scale from 1 to 5, with 1 = very unsatisfied and 5 = very satisfied
b) Please describe your experience with this program
2. What worked well in this program?
3. What parts of the program did not work well? What would you change?
Interview Guide Cont’d4. a) How worthwhile do you feel this program is for seniors? Please
rate your assessment between 1 – 5, with 1 = not very worthwhile and 5 = very worthwhile
b) Please explain your response.
5. a) I believe that the Seniors’ Collaborative Care Program should be implemented in the McMaster FHT on a larger scale. Please rate on a scale of 1-5, where 1=strongly disagree, and 5= strongly agree
b) Please explain your response.
6. ) Do you have any other comments that you would like to make.
Interview Guide Cont’d
Demographics:
1. Role in McMaster FHT:______________
2. Hours worked per week:_____________
3. Length of time with McMaster FHT:______________
4. Average amount of time spent with program:_____________

Results- Patient’s Feedback• Overall satisfaction- Mean (SD): 4.4 (0.54)
• “felt more comfortable, help in optimizing care”
• Worthwhile program for seniors: 4.2 (0.44)• “Seniors need more attention. This program would be quite
beneficial”
• What worked well?• …”enough time to ask questions and get clarifications”• “discussing medications with a pharmacist”• “Meeting with a nurse at home to avoid falls”

Results- MDs’ Feedback
• Overall satisfaction: 4.8 (0.44)• “The program made me feel more comfortable”
• How worthwhile is program for seniors: 4.8 (0.44)• “Home visits were very helpful and informative”
• Should SCCP be expanded: 4.8 (0.44)• “…access to services in a timely manner…”
MDs’ Feedback Cont’d
• What worked well?• RN visit at home was essential and allowed for a
more complete picture • Communication is timely and useful• Multidisciplinary approach
• Areas of improvement/ Suggestions?• Taking a more proactive role in scheduling• Becoming comfortable with roles

Results- RPNs’ Feedback • Overall satisfaction: 4.9 (0.25)
• “…providers were able to prevent crises from happening.”
• How worthwhile is program for seniors: 5.0 (0.0)• “…helps in keeping patients in their homes longer.”
• Should SCCP be expanded: 5.0 (0.0)• “It would be beneficial to expand it to the rest of
Hamilton communities as there is a great need for it”
RPNs’ Feedback Cont’d• What worked well?
• Case presentation; receiving different perspectives• Learners (e.g. residents) were involved; good
experience• Collaboration between geriatric and primary care• Caregiver relief• Recognition of health concerns is faster
• Areas of improvement/ suggestions?• Organizing appointments with appropriate providers
requires familiarization with program

Clinical Program
• Referral based program
• Patients are referred from all the teams– Averaging 1-2 referrals per week
• Referrals are for complex elderly, and are not restricted to cognition or falls as the clinical issue
Clinical Team
• Family Doctor Dr. Ainsley Moore • NP Joy White • RPN Rachelle Gervais• Pharmacist Shelly House• Geriatrician Dr. Christopher Patterson• Dietitian Glenda Pauw
• Learners all are welcome!

Clinical Team

Clinical Program
• Assessment done over 2-3 visits• Case review informally with interdisciplinary
team• Case review with geriatrician as needed• Care plan reviewed with primary care provider

Structure of visits
• Initial Appointment– Booked by RPN on Friday mornings
• Initial 30 minutes with RPN • 60 min with MD or NP• Also double-booked with resident
– RPN: GDS, modified Levy, SCREEN II– MD or NP: Chart review and assessment of
presenting issues• Second Appointment
– Meeting with family• Third Appointment
– Physical exam– F/u as needed

Case Reviews
• Informal– Done in the team room following the patient
appointment
• Formal– Case reviews including Dr Patterson– Twice a month– Scheduled so physicians, allied health
care providers and learners can attend
Case Reviews
• Documentation is done during the case review
• Follow-up time is variable following case review ( 30 to 60 min)
• Follow-up is shared among the team members

Geriatrician role
• Dr. Christopher Patterson– Twice a month– Willing to do case reviews, see patients in the clinic or
at home, discuss topics
(management of depression in older adults)– Friday mornings 9 to 12 noon
• 3-4 case reviews and sees 1 patient
Wait to be seen by geriatrician is 2-6 weeks vs 6 months outside the clinic
Team Roles• MD
– Assess patients – provides consultation across the clinic for complex
elderly
• NP – assess patients– case management role – case review planning– support continuity of care– knowledgeable regarding community resources

Team Roles
• Pharmacist– Medication review– Recommend changes in drug therapy– Assist in implementing changes
• RPN– arranges initial appointments– initial screening– knowledge of community resources– provides continuity

Team Roles
• Social Work– Provides support for complex family dynamics– knowledge of community resources
• Dietitian– Nutrition knowledge for promotion of
seniors’ health– reducing health risk in the community

What are the benefits of our clinical program?
• Patient care
• Learners
• Health care team

What we have learned about patient care
• Patient care benefits– Improved continuity for patients– More timely specialist care– Chart reviews prior to seeing a complex senior is a good use of
time– Improved use of community resources (matched to patient need)– Time taken to include family caregivers is well worth the effort– How to structure our care for improved efficiency– MOCA is a good tool for primary care
What we have learned about geriatrican role in primary care
• Role of visiting Geriatrician– Generally sees patients with atypical presentations or when
multiple co-morbities are present, or when treatment plans conflict
What is the most helpful?– specialist expertise in diagnosis and management of complex
interacting medical issues . – Planning care at transition points.
• changing goals of care – Enhanced confidence
• skill building

What we have learned about health care teams
Interdisciplinary team care increases the range of solutions and improves providers satisfaction
– Interprofessional growth and development– Enhanced understanding and appreciation of each others roles
• There are disease specific guidelines but no multiple co-morbidity guidelines– this means health care teams need ongoing support when caring
for these populations– reduced provider burden (antecdotal)– Incorporation of learners – work
Benefits for learners
• Incorporating learners– structured times for case reviews
facilitate particiption– Residents are not always available on
Friday mornings– opportunity to go on home visits– opportunity to plan care with multiple
disciplines

What are the challenges?
– How is the approach different: slower, takes time, so should we be doing it? Improved our efficiency over time
– Latest literature: we can not continue usual care as it does not

Future directions
• Continued development of the team
• Further development of education goals and objectives for learners
• Care processes template for EMR
• Addressing continuity
• Group medical appointments for older adults

QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.





























