Embed Size (px)
Citation preview

KEEPING ABREAST OF THE
CHAOS WITH LIPID
GUIDELINES
ROSHNI S. PATEL, PHARMD, BCPS
ASSISTANT PROFESSOR OF PHARMACY PRACTICE
JEFFERSON COLLEGE OF PHARMACY

DISCLOSURES
No conflicts of interest to disclose.

LEARNING OBJECTIVES
1. Compare and contrast the lipid lowering guidelines
published by the American College of
Cardiology/American Heart Association, American
Association of Clinical Endocrinologists, and the
National Lipid Association
2. Describe how emerging evidence has affected lipid
guidelines and clinical practice
3. Develop a patient-centered approach to the treatment of
dyslipidemia

QUESTION #1
Which set of clinical practice guidelines do you follow for the
management of dyslipidemia?
A. American College of Cardiology/American Heart
Association
B. American Association of Clinical Endocrinologists
C. National Lipid Association
D. Hybrid Approach – how?
E. I don’t use guidelines

TIMELINE OF EVENTS
National Cholesterol Education
Program’s Adult Treatment Panel III
(NCEP ATP III) ACC/AHA
ACC Expert
Consensus Decision
Pathway for Non-
statin Therapies
ACC Focused
update of 2016
consensus
pathway
May
2001
November
2013
June
2016 September
2017
Updated NLA Recommendations for
Use of PCSK9 Inhibitors
May 2017
NLA Recommendations
for Patient-Centered
Management of
Dyslipidemia: Part 1
September 2014
NLA Recommendations for
Patient-Centered Management
of Dyslipidemia: Part 2
November 2015
AACE Guidelines for
Management of Dyslipidemia &
Prevention of
Atherosclerosis
March 2012
AACE Guidelines for
Management of Dyslipidemia
& Prevention of
Atherosclerosis
April 2017
AHA
Statement
on TG
May 2011
NCEP ATP
III Update
July 2004

2001 NCEP ATP III GUIDELINES
Lipid Goals & Framingham Risk Stratification
Risk Category LDL-C Goal
LDL-C Level at Which to
Initiate Therapeutic
Lifestyle Changes (TLC)
LDL-C Level at Which
to Consider Drug
Therapy
CHD or CHD Risk
Equivalents
(10-year risk > 20%)
< 100 mg/dL ≥ 100 mg/dL
≥ 130 mg/dL
(100-129 mg/dL: drug
optional)
2+ Risk Factors
(10-year risk ≤ 20%) < 130 mg/dL ≥ 130 mg/dL
10-year risk 10-20%:
≥ 130 mg/dL
10-year risk <10%:
≥ 160 mg/dL
0-1 Risk Factor < 160 mg/dL ≥ 160 mg/dL
≥ 190 mg/dL
(160-189 mg/dL: LDL-
lowering drug optional)
NCEP. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection,
Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106:3143-421.

2004 NCEP ATP III UPDATE
Lipid Goals & Framingham Risk Stratification
Risk Category LDL-C Goal
LDL-C Level at Which to
Initiate Therapeutic
Lifestyle Changes (TLC)
LDL-C Level at Which
to Consider Drug
Therapy
CHD or CHD Risk
Equivalents
(10-year risk > 20%)
< 100 mg/dL
(optional: < 70
mg/dL)
≥ 100 mg/dL
≥ 100 mg/dL
(< 100 mg/dL: drug
optional)
2+ Risk Factors
(10-year risk ≤ 20%)
< 130 mg/dL
(optional < 100
mg/dL)
≥ 130 mg/dL
10-year risk 10-20%:
≥ 130 mg/dL
10-year risk <10%:
≥ 160 mg/dL
0-1 Risk Factor < 160 mg/dL ≥ 160 mg/dL
≥ 190 mg/dL
(160-189 mg/dL: LDL-
lowering drug optional)
NCEP Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines. Circulation 2004;110:227-39.

NCEP ATP III GUIDELINES
Treatment:
• HMG CoA Reductase Inhibitors (statins) – usually first
• Starting dose of statin is dependent upon baseline level of
LDL-C
• Increase the dose of statin if LDL-C target goals not
achieved
• Bile acid sequestrants
• Nicotinic acid
• Fibric acids
• Omega 3 fatty acids
NCEP. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection,
Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106:3143-421.

2013 ACC/AHA GUIDELINES
• No target goals
• New Pooled Cohort Equation to Identify Primary ASCVD
risk
• 4 Major Statin Benefit Groups
1. Clinical ASCVD
2. Primary elevations of LDL-C ≥ 190 mg/dL
3. Diabetes aged 40 to 75 years with LDL-C 70 to 189
mg/dL and without clinical ASCVD
4. Without clinical ASCVD or diabetes with LDL-C 70 to 189
mg/dL & estimated 10-year ASCVD risk ≥ 7.5%
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. Published online November 12, 2013. doi: 10.1161/ 01.cir.0000437738.63853.7a
Clinical ASCVD: ACS, history of MI, stable or unstable angina, coronary or
other arterial revascularization, stroke, TIA, or PAD

POOLED COHORT EQUATION

STATIN INTENSITY
Low Intensity Moderate Intensity High Intensity
Daily dose lowers LDL-C on average by <30%
Daily dose lowers LDL-C on average by 30% to <50%
Daily dose lowers LDL-C on average by ≥50%
Simvastatin 10 mg Pravastatin 10-20 mg Lovastatin 20 mg Fluvastatin 20-40 mg Pitavastatin 1 mg
Atorvastatin 10 (20) mg Rosuvastatin 5 (10) mg Simvastatin 20-40 mg Pravastatin 40 (80) mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg BID Pitavastatin 2-4 mg
Atorvastatin 40-80 mg Rosuvastatin 20 (40) mg
Bolded = specific statin + dose evaluated in RCT Italicized = specific statin + dose approved by FDA but not evaluated in RCT
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. Published online November 12, 2013. doi: 10.1161/ 01.cir.0000437738.63853.7a
Based on
LDL-C
lowering
potential
rosuvastatin atorvastatin simvastatin = pitavastatin pravastatin = lovastatin fluvastatin
P
O
T
E
N
C
Y

APPROACH TO THE PATIENT
Age ≤ 75: High Intensity Statin
Age > 75: Mod Intensity Statin
High Intensity Statin
Mod Intensity Statin ASCVD risk ≥ 7.5%:
High Intensity Statin
Mod Intensity Statin
No action or need to increase statin
< 70 mg/dL
Not in definite benefit group
ASCVD 10 year risk q 4-6 yr
yes
≥ 190 mg/dL
70 - 189 mg/dL
Age 40 – 75?
yes
yes
no
T1 or T2 DM?
≥ 7.5%
Clinical ASCVD?
LDL
< 7.5%
Consider other factors: a.LDL > 160 mg/dL b.Family hx c.High CRP d.CAC score e.ABI < 0.9 f.Lifetime ASCVD risk
High Intensity Statin
no
no
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. Published online November 12, 2013. doi: 10.1161/ 01.cir.0000437738.63853.7a

LIPID PANELS
**Use LDL–C reduction thresholds as an indicator of efficacy to assess response to therapy and adherence
Baseline fasting lipid panel
2nd fasting lipid panel after 4-12 weeks
q 3 to 12 months as clinically indicated
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. Published online November 12, 2013. doi: 10.1161/ 01.cir.0000437738.63853.7a

CAVEAT INCLUDED
“in those already on a statin, in whom baseline LDL-C is unknown, an LDL-C
level < 100 mg/dL was observed in most individuals receiving high-intensity
statin therapy”
Nonetheless, LCL-C < 100 mg/dL should not be used as a fixed-target.
Example:
• Patient 1 with ASCVD on low intensity statin achieves an LDL-C of < 100
mg/dL
• Patient 2 with ASCVD on high intensity statin achieves an LDL-C of < 100
mg/dL
• Outcome data suggests high intensity statin (if tolerated) provides
greater reduction in ASCVD events than low intensity statin
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. Published online November 12, 2013. doi: 10.1161/ 01.cir.0000437738.63853.7a

AFTER STATINS
“less evidence to support the use of non-statin drugs for
ASCVD prevention”
Safety recommendations provided for:
• Bile acid sequestrants
• Nicotinic acid
• Fibric acids
• Cholesterol absorption inhibitors
• Omega 3 Fatty Acids
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. Published online November 12, 2013. doi: 10.1161/ 01.cir.0000437738.63853.7a

2016 ACC CONSENSUS PATHWAY
FOR NON-STATIN THERAPIES
High risk patients who…
1. Have a less-than-anticipated response to statins
[% reduction in LDL-C from baseline (may consider LDL-C
targets of < 70 mg/dL or <100 mg/dL)]
2. Are unable to tolerate a less-than-recommended intensity
of a statin
3. Are completely statin intolerant
**Use drugs that have been shown in RCTs to provide ASCVD risk-reduction benefits that outweigh the potential for adverse effects and drug-drug interactions,
and consider patient preferences
2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk. J Am Coll Cardiol. 2016;68(1):92-125.

CHOICE FOR NON-STATIN
THERAPY
S T A T I N B E N E F I T G R O U P S
Group #1 (Clinical ASCVD)
Group #2 LDL-C ≥ 190 mg/dL
1st line
Add ezetimibe
2nd line
Add PCSK9i
or
Replace ezetimibe
with PCSK9i
or
Add bile acid
sequestrant
1st line
Add PCSK9i
or
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #3 40-75 y/o (w/o ASCVD)
+ DM + LDL-C 70-189
mg/dL
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #4 ASCVD risk > 7.5%
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk. J Am Coll Cardiol. 2016;68(1):92-125.

IMPROVE-IT TRIAL
Cannon et al. N Engl J Med 2015;372:2387-97.
Population:
Patients with recent acute MI with or without
ST elevation, or high-risk UA
Treatment arms:
Simvastatin 40 mg + ezetimibe 10 mg
Simvastatin 40 mg + placebo
Primary outcome:
Composite of death from CVD, a major
coronary event, or nonfatal stroke
Results:
32.7% vs. 34.7%, p=0.016

CHOICE FOR NON-STATIN
THERAPY
S T A T I N B E N E F I T G R O U P S
Group #1 (Clinical ASCVD)
Group #2 LDL-C ≥ 190 mg/dL
1st line
Add ezetimibe
2nd line
Add PCSK9i
or
Replace ezetimibe
with PCSK9i
or
Add bile acid
sequestrant
1st line
Add PCSK9i
or
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #3 40-75 y/o (w/o ASCVD)
+ DM + LDL-C 70-189
mg/dL
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #4 ASCVD risk > 7.5%
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk. J Am Coll Cardiol. 2016;68(1):92-125.

HPS2-THRIVE TRIAL
**ACC: No clear indications for routine use of niacin preparations as additional non-statin therapy (based on evidence of non-efficacy and potential harm)
HPS2-THRIVE Collaborative Group. N Engl J Med 2014;371:203-12.

CHOICE FOR NON-STATIN
THERAPY
S T A T I N B E N E F I T G R O U P S
Group #1 (Clinical ASCVD)
Group #2 LDL-C ≥ 190 mg/dL
1st line
Add ezetimibe
2nd line
Add PCSK9i
or
Replace ezetimibe
with PCSK9i
or
Add bile acid
sequestrant
1st line
Add PCSK9i
or
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #3 40-75 y/o (w/o ASCVD)
+ DM + LDL-C 70-189
mg/dL
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #4 ASCVD risk > 7.5%
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk. J Am Coll Cardiol. 2016;68(1):92-125.

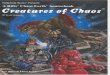
PCSK9 INHIBITORS
PCSK9
LDLR
Head to the
surface to
receive chlyo-
remnants, IDL,
and LDL
nucleus
ϒ ϒ
Mechanism of Action:
• Human monoclonal antibody inhibiting PCSK9 protein

COMPARATIVE EFFECTS OF LIPID-
LOWERING DRUG THERAPIES
Class Generic Brand Dose/day LDL-C HDL-C TG
HMG-CoA
Reductase
Inhibitors
(Statins)
Lovastatin Mevacor 20-80mg 20-40% 6-10% 7-12%
Simvastatin Zocor 5-40 mg 26-47% 7-12% 10-24%
Pravastatin Pravachol 10-80mg 22-34% 7-12% 15-24%
Fluvastatin Lescol 20-80 mg 22-24% small small
Atorvastatin Lipitor 10-80 mg 39-60% 5-9% 19-37%
Rosuvastatin Crestor 5-40 mg 45-63% 8-14% 10-35%
Pitavastatin Livalo 1-4 mg 32-43 5-7% 15-19%
PCSK9 Inhibitorsƚ Alirocumab Praluent Footnote 32-62% small 1-17%
Evolocumab Repatha Footnote 55-70% small 6-31%
Bile acid
sequestrants
Cholestyramine Questran 4-24 gm 10-20% 3-5% May
Cholestipol Colestid 5-30 gm 10-20% 3-5% May
Colesevelam Welchol 3.75 gm 9-18% 3-5% May
Nicotinic Acid IR/SR Niacin Niacor/Slo-Niacin
variable 10-25% 10-35% 10-50%
ER-Niacin Niaspan 9-17% 15-26% 11-35%
Fibric Acids derivatives Gemfibrozil Lopid 1200 mg 10-15% 10-15% 20-50%
Fenofibrate Tricor 48-145 mg 17-29% 0-15% 38%-57%
Cholesterol Absorption
Inhibitor Ezetimibe Zetia 10 mg 18% 1% 10%
Fish Oil Omega 3-FAs Lovaza
Vascepa 2-4 gm variable variable Up to 50%
MTP Inhibitor Lomitapide Juxtapid 5-60 mg 40% 7% 45%
ApoB Antisenseǂ Mipomersen Kynamro Footnote 25% 15% 18%
ƚAlirocumab dosed 75/150 mg every 2 weeks or 300 mg every 4 weeks; evolocumab dosed 140 mg every 2 weeks or 420 mg once monthly ǂMipomersen dosed 200 mg once weekly

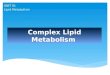
PCSK9
INHIBITORS
Navarese et al. Ann Intern Med 2015;163:40-51.
LDL-C Percentage of
Change from Baseline

PCSK9 INHIBITORS
Available Products:
• Alirocumab (Praluent®) 75 mg/150 mg SUBUTANEOUSLY every 2
weeks or 300 mg every 4 weeks
• Evolocumab (Repatha®) 140 mg SUBCUTANEOUSLY every 2
weeks OR 420 mg monthly
ADEs:
• Injection site reactions
• Nasopharyngitis and influenza
• Small incidence of elevations in liver enzymes and CK

CHOICE FOR NON-STATIN
THERAPY
S T A T I N B E N E F I T G R O U P S
Group #1 (Clinical ASCVD)
Group #2 LDL-C ≥ 190 mg/dL
1st line
Add ezetimibe
2nd line
Add PCSK9i
or
Replace ezetimibe
with PCSK9i
or
Add bile acid
sequestrant
1st line
Add PCSK9i
or
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #3 40-75 y/o (w/o ASCVD)
+ DM + LDL-C 70-189
mg/dL
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #4 ASCVD risk > 7.5%
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk. J Am Coll Cardiol. 2016;68(1):92-125.

2017 ACC UPDATE
S T A T I N B E N E F I T G R O U P S
Group #1 (Clinical ASCVD)
Group #2 LDL-C ≥ 190 mg/dL
1st line
Add PCSK9i
or
Add ezetimibe
2nd line
Add bile acid
sequestrant
1st line
Add PCSK9i
or
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #3 40-75 y/o (w/o ASCVD)
+ DM + LDL-C 70-189
mg/dL
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #4 ASCVD risk > 7.5%
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk: A Report of the American College
of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol 2017;70:1785-1822.

OSLER 1 & 2 TRIALS
Population:
Patients who previously completed 1 of 12 phase 2 or 3
trials (“parent trials”)
Treatment arms:
Evolocumab 140 mg every 2 weeks + standard therapy
Evolocumab 420 mg every month + standard therapy
Standard therapy alone
Exploratory analysis (outcome):
Composite of CV death, myocardial infarction, unstable
angina requiring hospitalization or coronary
revascularization, stroke, TIA, and heart failure requiring
hospitalization
Results:
0.95% vs. 2.18%, p=0.003
Sabatine et al. N Engl J Med 2015;372:1500-09.

FOURIER TRIAL
Sabatine et al. N Engl J Med 2017;376:1713-22.
Population:
Patients with ASCVD and LDL-C > 70 mg/dL
on statin therapy
Treatment arms:
Evolocumab 140 mg every 2 weeks
Evolocumab 420 mg every month
Matching placebo
Primary outcome:
Composite of CV death, myocardial infarction,
stoke, hospitalization for unstable angina, or
coronary revascularization
Results:
9.8% vs. 11.3%, p<0.001
MI, stroke, and coronary revascularization
were all lower in the evolocumab group

SPIRE 1 & 2 TRIALS
Population:
Patients with previous CV event or a history of
diabetes, CKD, or PVD with additional CV risk
conditions or a history of FH
Treatment arms:
Bococizumab 150 mg every 2 weeks
Matching placebo
Primary outcome:
Composite of nonfatal myocardial infarction,
nonfatal stroke, hospitalization for unstable
angina requiring urgent revascularization, or
CV death
Results:
Spire 1 (lower risk, shorter duration):
2% in each group
HR 0.99 (95% CI 0.80 to 1.22, p=0.99)
Spire 2 (higher risk, longer duration):
3.4% vs. 4.2%
HR 0.79 (95% CI 0.65 to 0.97, p=0.02)
Ridker et al. N Engl J Med 2017;376:1527-39.

2017 ACC UPDATE
S T A T I N B E N E F I T G R O U P S
Group #1 (Clinical ASCVD)
Group #2 LDL-C ≥ 190 mg/dL
1st line
Add PCSK9i
or
Add ezetimibe
2nd line
Add bile acid
sequestrant
1st line
Add PCSK9i
or
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #3 40-75 y/o (w/o ASCVD)
+ DM + LDL-C 70-189
mg/dL
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
Group #4 ASCVD risk > 7.5%
1st line
Add ezetimibe
2nd line
Add bile acid
sequestrant
2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-Statin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk: A Report of the American College
of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol 2017;70:1785-1822.

2017 AACE GUIDELINES
Risk Category Risk factors/10-year risk Treatment Goals
LDL-C Non-HDL-C Apo-B
Extreme risk
- Progressive ASCVD including unstable
angina in patients after achieving an
LDL-C < 70 mg/dL
- Established clinical cardiovascular
disease in patients with DM, CKD 3/4,
or HeFH
- History of premature ASCVD (<55
male, <65 female)
<55 mg/dL <80 mg/dL <70 mg/dL
Very high risk
- Established or recent hospitalization
for ACS, coronary, carotid, of
peripheral vascular disease, 10-year
risk > 20%
- Diabetes of CKD 3/4 with 1 or more
risk factor(s)
- HeFH
<70 mg/dL <100 mg/dL <80 mg/dL
High risk
- ≥2 risk factors and 10-year risk 10-
20%
- Diabetes or CKD 3/4 with no other risk
factors
<100 mg/dL <130 mg/dL <90 mg/dL
Moderate risk ≤2 risk factors and 10-year risk <10% <100 mg/dL <130 mg/dL <90 mg/dL
Low risk 0 risk factors <130 mg/dL <160 mg/dL NR
2017 AACE and ACE Guidelines For Management of Dyslipidemia and Prevention of Cardiovascular Disease. Endocr Pract 2017;23:1-87.

QUESTION #2
How low is too low for LDL-C?
A. <55 mg/dL is too low
B. <40 mg/dL is too low
C. <25 mg/dL is too low
D. There is no such thing as “too low”

2017 AACE GUIDELINES
Assessment of 10-year Risk for a Coronary Event:
• Framingham Risk Assessment Tool
• Multi-Ethnic Study of Atherosclerosis (MESA) 10-year ASCVD
Risk with Coronary Artery Calcification Calculator
• Reynolds Risk Score
• United Kingdom Prospective Diabetes Study Risk Engine to
Calculate ASCVD Risk in Individuals with T2DM
2017 AACE and ACE Guidelines For Management of Dyslipidemia and Prevention of Cardiovascular Disease. Endocr Pract 2017;23:1-87.

TREATMENT
• Statins primary pharmacologic agent to achieve target LDL-C
• BAS may be considered for reducing LDL-C and Apo B
• Nicotinic acid adjust for reducing TG
• Fibric acids for severe hypertriglyceridemia
• CAI may be considered as monotherapy for reducing LDL-C and
Apo B, specially in statin-intolerant patients
• O3FA for severe hypertriglyceridemia
• PCSK9i for use in combination with statin therapy for LDL-C lowering in
patients with FH, for patients with CVD unable to reach LDL-
C/non-HDL-C goals with maximally tolerated statin therapy
2017 AACE and ACE Guidelines For Management of Dyslipidemia and Prevention of Cardiovascular Disease. Endocr Pract 2017;23:1-87.

NLA’S TAKE ON “GOALS”
Treatment goals are useful as means to ensure that the
aggressiveness of therapy to lower atherogenic cholesterol is matched
to absolute risk for an event.
Treatment goals facilitate effective communication between patients
and clinicians, providing an easily interpretable means through which
the clinician can communicate progress toward meeting treatment
objectives, thus supporting efforts to maximize long-term adherence to
the treatment plan.
National Lipid Association Recommendations for Patient-Centered Management of Dyslipidemia: Part 1—Full Report. J Clin Lipidol 2015; 9:129-69.

NLA GUIDELINES
Risk
Category Criteria
Treatment Goals
LDL-C Non-HDL-C Apo-B
Low - 0-1 major ASCVD risk factors
- Consider other risk indicators, if known <100 mg/dL <130 mg/dL <90 mg/dL
Moderate - 2 major ASCVD risk factors
- Consider quantitative risk scoring
- Consider other risk indicators
<100 mg/dL <130 mg/dL <90 mg/dL
High - ≥3 major ASCVD risk factors
- Diabetes mellitus (type 1 or 2)
- 0-1 other major ASCVD risk factors
and
- No evidence of end organ damage
- CKD 3B or 4
- LDL-C ≥190 mg/dL
- Quantitative risk score reaching the high-
risk threshold
<100 mg/dL <130 mg/dL <90 mg/dL
Very High - ASCVD
- Diabetes mellitus (type 1 or 2)
- ≥2 other major ASCVD risk factors or
- No evidence of end organ damage <70 mg/dL <100 mg/dL <80 mg/dL
National Lipid Association Recommendations for Patient-Centered Management of Dyslipidemia: Part 1—Full Report. J Clin Lipidol 2015; 9:129-69.

NLA HIGH RISK THRESHOLDS
• ATP III Framingham risk calculator:
≥10% 10-year risk for a hard CHD event (myocardial infarction
or CHD death)
• Pooled Cohort Equations (American College of
Cardiology/American Heart Association):
≥15% 10-year risk for a hard ASCVD event (myocardial
infarction, stroke, or death from CHD or stroke)
• Framingham long-term (30-year to age 80) risk calculator:
≥45% risk for CVD (myocardial infarction, CHD death, or
stroke)
National Lipid Association Recommendations for Patient-Centered Management of Dyslipidemia: Part 1—Full Report. J Clin Lipidol 2015; 9:129-69.

NLA TREATMENT
1st line therapy: moderate or high intensity statin
• If cholesterol goals are not achieved, either increase statin
intensity or add on second agent
• References HPS2-THRIVE Trial
• References IMPROVE-IT Trial
National Lipid Association Recommendations for Patient-Centered Management of Dyslipidemia: Part 1—Full Report. J Clin Lipidol 2015; 9:129-69.

2017 NLA EXPERT PANEL PCSK9
INHIBITOR RECOMMENDATIONS
Disorder LDL-C/Non-HDL-C
Threshold for Rx
(md/dL)
Strength of Evidence Quality of Evidence
ASCVD + additional risk factors ≥ 70 / ≥ 100 A High
Progressive ASCVD ≥ 70 / ≥ 100
B Moderate
LDL-C ≥ 190, age 40-79
(no uncontrolled RF or key
additional risk markers)
≥ 100 / ≥ 130
B Moderate
LDL-C ≥ 190, age 40-79
(uncontrolled RF or key
additional risk markers)
≥ 70 / ≥ 100 B Moderate
LDL-C ≥ 190, age 18-39
(uncontrolled RF or key
additional risk markers or FH
causing mutation)
≥ 100 / ≥ 130
E Low
HoFH phenotype ≥ 70 / ≥ 100 B Moderate
ASCVD + statin intolerance Clinical Judgement C Low
Update on the use of PCSK9 inhibitors in adults: Recommendations from an Expert Panel of the National Lipid Association. J Clin Lipidol 2017;11:880-90.

QUESTION #3
Which set of clinical practice guidelines will you follow for
the management of dyslipidemia?
A. American College of Cardiology/American Heart
Association
B. American Association of Clinical Endocrinologists
C. National Lipid Association
D. Hybrid Approach – how?
E. I will not be using guidelines

DOES IT REALLY MATTER?
Patient Case: MC is a 60 year old African American woman with HTN, dyslipidemia, CKD (stage I), migraines,
and osteoarthritis. She has been taking all of her medications for 2 years and reports 100% compliance
(which is confirmed by refill records and pill counts). Denies CP, SOB, s/sx of CVA. Denies ADEs to any of her
medications. FH is significant for T2DM and CVD. No tobacco use.
Medications:
Lisinopril 40 mg PO daily
Amlodipine 10 mg PO daily
Atorvastatin 20 mg PO daily
Aspirin 81 mg PO daily
Sumatriptan 50 mg PO PRN
Acetaminophen 650 mg PO TID
VS: BP 128/90 mmHg, HR 70 bpm
Labs:
Baseline FLP: TC 240 mg/dL, LDL-C 170 mg/dL, HDL 38 mg/dL, TG 160 mg/dL
Today’s FLP: TC 250 mg/dL, LDL-C 164 mg/dL, HDL 42 mg/dL, TG 220 mg/dL
ACC/AHA
AACE
NLA

DOES IT REALLY MATTER?
Patient Case: MC is a 60 year old African American woman with HTN, dyslipidemia, CKD (stage I), migraines,
and osteoarthritis. She has been taking all of her medications for 2 years and reports 100% compliance
(which is confirmed by refill records and pill counts). Denies CP, SOB, s/sx of CVA. Denies ADEs to any of her
medications. FH is significant for T2DM and CVD. No tobacco use.
Medications:
Lisinopril 40 mg PO daily
Amlodipine 10 mg PO daily
Atorvastatin 20 mg PO daily
Aspirin 81 mg PO daily
Sumatriptan 50 mg PO PRN
Acetaminophen 650 mg PO TID
VS: BP 128/90 mmHg, HR 70 bpm
Labs:
Baseline FLP: TC 240 mg/dL, LDL-C 170 mg/dL, HDL 38 mg/dL, TG 160 mg/dL
Today’s FLP: TC 206 mg/dL, LDL-C 120 mg/dL, HDL 42 mg/dL, TG 220 mg/dL
ACC/AHA
AACE
NLA

DOES IT REALLY MATTER?
Patient Case: MC is a 60 year old African American woman with HTN, dyslipidemia, PAD, T2DM. She has
been taking all of her medications for 2 years and reports 100% compliance (which is confirmed by refill
records and pill counts). Denies CP, SOB, s/sx of CVA. Denies ADEs to any of her medications. FH is
significant for T2DM and CVD. No tobacco use.
Medications:
Lisinopril 40 mg PO daily
Amlodipine 10 mg PO daily
Rosuvastatin 40 mg PO daily
Aspirin 81 mg PO daily
VS: BP 128/90 mmHg, HR 70 bpm
Labs:
Baseline FLP: TC 250 mg/dL, LDL-C 180 mg/dL, HDL 38 mg/dL, TG 160 mg/dL
Today’s FLP: TC 176 mg/dL, LDL-C 90 mg/dL, HDL 42 mg/dL, TG 220 mg/dL
ACC/AHA
AACE
NLA