Embed Size (px)
Citation preview

Katrina Brogden
CCU pharmacist
FSH
Mr PW 64yr old admitted with NSTEMI
PMH – diabetes, hypertension, ex-smoker, PCI (2006), hypercholesterolemia
Previous medications:
Metoprolol 25mg morning
Atorvastatin 40mg morning
Empagliflozin/Linagliptin 25/5mg
morning
Metformin 1000mg morning

Mr PW Had angiogram and received a DES to the proximal
LAD
Medications on discharge 2/7 later:
Aspirin 100mg morning
Ticagrelor 90mg twice a day
Metoprolol 25mg twice a day
Ramipril 2.5mg morning
Atorvastatin 80mg morning
Diabetes medications unchanged
Mr PW So what are the recommended doses we should use?
What do the guidelines say?
Should we titrate the doses? And how/when can this occur?
What factors will affect our ability to titrate (either up or down)?
What observations are we aiming for?
Antiplatelet - Aspirin Inhibits cyclo-oxygenase pathway which inhibits
platelet activation
300mg load, then 100mg daily
Reduces coronary disease by 25%
Lifelong in most patients, particularly with stents
Consider enteric coated options in patients with GI concerns
Clopidogrel
PY12 inhibitor which provides platelet inhibition leading to a reduction in ischaemic events
300-600mg load, then 75mg daily
Prodrug – converted to active metabolite via the liver
Available in a combination tablet with Aspirin
Clopidogrel For at least 12 months in DES patients, but may be
longer in high risk patients
May cause a widespread red, itchy rash
Patient resistance is possible due to genetic variability in liver enzymes
Ticagrelor Same action as clopidogrel, PY12 inhibitor
180mg load then 90mg twice a day
For at least 12 months in DES patients
Common ADRs:
dyspnoea (10-15%)
bradycardia (5%)
switch to clopidogrel and re-load if these occur
Triple therapy Mr PW had an admission 2 weeks after d/c for new onset
AF. Started on Apixaban 5mg twice a day.
What do we do with his antiplatelets?
Most evidence says triple therapy should only be used for the shortest period of time possible.
Usually 1-3 months (although sometimes 6 months), then stop either the aspirin or clopidogrel (if the anti-coag can’t be stopped)
Usually change to clopidogrel
Use PPI cover (ie pantoprazole) for length of triple therapy
ACE inhibitors Ramipril/Perindopril etc
Block the Angiotensin Converting Enzyme (ACE) involved in the renin-angiotensin-aldosterone system
Used in ACS to reduce myocardial injury, to stabilize blood pressure and reduce risk of MI (30% risk reduction)
Starting doses are very varied, although usually start low and go slow. Ramipril starting doses 1.25-2.5mg daily in ACEi naïve
patients
Perindopril 2.5-5mg daily
ACE inhibitors Guideline doses are up to 10mg daily of Ramipril or
Perindopril with the ‘as tolerated’ caveat
When can we up-titrate?
High or unstable blood pressure (aiming for resting SBP<110)
LV impairment/reduced ejection fraction
Diabetic patients
Unstable heart failure symptoms
ACE Inhibitors
When do we need to down titrate
Dizzy/lightheaded on getting up
Recurrent falls
Low BP and patient is symptomatic
Increased creatinine or potassium
May need to stop if dry cough occurs (15%)
Try splitting dose to help increase tolerance
ARBs Irbesartan/Candesartan/Olmesartan/Valsartan etc
Angiotensin receptor blocker
Used in ACS only when a patient can’t tolerate ACEi
No trials in ACS patients
Same concerns for up/down titration, but shouldn’t cause a cough
ACEi/ARBs and COVID-19 No evidence of any correlation
No increased risk of death associated with the use of ARB/ACEi in trial of 8910 patients
Beta Blockers Metoprolol/Bisoprolol/Atenolol etc
Block Beta 1 receptors in heart and peripheral arteries
Used in ACS to reduce heart rate, decrease myocardial oxygen consumption and reduce risk of MI. They have also shown a 23% reduction in all cause mortality.
Starting doses are varied, although usually start fairly low unless patients are already on beta blockers or other heart rate medications
Beta blockers Metoprolol
Should be twice a day dosing
25-50mg BD up to max of 100mg BD
Bisoprolol
Once a day, but dose may be BD to increase tolerance
1.25mg daily, up to 10mg daily (guideline recommendations)
Atenolol
25-50mg daily (max 100mg daily)
Good if patients have disturbed dreams/hallucinations as it doesn’t cross the blood-brain-barrier
Beta blockers When can we up-titrate?
Increased HR (aiming for resting rate around 60)
Irregular heart rhythms
Reduced ejection fraction
Ongoing angina
Residual ischaemia
Beta blockers When do we need to down titrate?
Increased SOB
Bradycardia (if no PPM) and patient is symptomatic
Lethargy/weakness
Acute HF/cardiogenic shock – they need to be withheld
May need to split doses to increase tolerance
If no LV impairment or ongoing angina, the beta blocker may be stopped at 12 months.
Statins Rosuvastatin/Atorvastatin
HMG CoA reductase inhibitors which lower the plasma cholesterol concentration
Used to reduce plaque build-up in arteries and stabilise plaque against artery walls
Guidelines recommend to aim for:
Total cholesterol <4.0
LDL <1.8
Triglycerides <2.0

Statins Increase to maximum dose in acute setting
Can cause up to 50% reduction in LDL (diet alone can only provide 10% reduction)
Recommended doses:
Atorvastatin 40mg or 80mg daily
Rosuvastatin 20mg or 40mg daily
Statins Up titrate when
LDL remains >1.8
New event on statin
Plaque rupture causing MI
Significant CAD
Down titrate Increased LFTs
Patient tolerance (muscle aches)
Some is better than none – maybe use alternate day dosing
Other cholesterol agents Ezetimibe
Good to lower LDL after maximum statin trialled
Many combinations with statins available
Fenofibrate Good for high triglycerides
Evolocumab Fortnightly injection
Used if maximum doses of statins and ezetimibe trialled and LDL remains elevated
Recommended in familial hypercholesterolemia
What are the recommended guideline doses?
Aspirin 100mg daily
Ticagrelor 90mg twice daily
Clopidogrel 75mg daily
Perindopril/Ramipril 5-10mg daily
Metoprolol 25-50mg twice daily
Statin 40-80mg daily

Mr PW Admission meds Discharge meds
Metoprolol 25mg morning
Atorvastatin 40mg morning
Empagliflozin/Linagliptin 25/5mg morning
Metformin 1000mg morning
Aspirin 100mg morning
Ticagrelor 90mg twice a day
Metoprolol 25mg twice a day
Ramipril 2.5mg morning
Atorvastatin 80mg morning
Diabetes medications unchanged
Mr PW Can you identify the changes made?
Can you think about why we might have made these changes?
Do Mr PW’s meds follow guideline recommendations?
Mr PW – changes made and reasons for change Increased metoprolol to BD as not effective once daily
(short half life)
Increased statin as LDL 2.2 and patient has had a new ACS event
Added DAPT for DES (incl. restarting Aspirin – which should be lifelong for him)
Added ACEi at a low dose as BP 130/78
Diabetic meds remained the same, HbA1c was 7.2%
Do the changes follow guidelines? Mr PW Guidelines
Aspirin 100mg morning
Ticagrelor 90mg twice a day
Metoprolol 25mg twice a day
Ramipril 2.5mg morning
Atorvastatin 80mg morning
Diabetes medications unchanged
Aspirin 100mg daily
Ticagrelor 90mg twice daily
Clopidogrel 75mg daily
Perindopril/Ramipril 5-10mg daily
Metoprolol 25-50mg twice daily
Statin 40-80mg daily
Mr PW 8 weeks after d/c You see him in clinic 8 weeks after his hospital stay.
His BP is 145/91, HR at rest 67.
He states he has been taking his medications since discharge.
Aspirin 100mg morning
Ticagrelor 90mg twice a day
Metoprolol 25mg twice a day
Ramipril 2.5mg morning
Atorvastatin 80mg morning
Mr PW 8 weeks after d/c Would you titrate any of his medications?
Would you like to know a few things before changing his medications?
What other questions would you ask the patient?
Mr PW post d/c questions Has he had any BP readings done since d/c?
How is he actually taking his medications (does he have his medication list to show you?)
Did he get new scripts from the GP/pharmacy?
How has he been feeling since d/c?
Any symptoms of dizziness/lightheadedness/lethargy? (or other side effects relating to the medications)
Risks of non-adherence Inappropriate dose escalation (with potential for
harm)
Increased cardiac events +/- CV mortality
Repeat presentations to hospital (some registry data suggests 64% of readmissions is related to medication non-adherence)
Increased decompensations in heart failure
Increased symptoms of ACS
Risks of non-adherence
Poor adherence to medications in patients with stable coronary artery disease is associated with
10-40% increased risk of cardiovascular admissions
10-30% increased risk of coronary interventions
50-80% increased risk of cardiovascular mortality
Thakkar JB, Chow CK. Adherence to secondary prevention therapies in acute coronary syndrome. MJA 2014;201 (10):S106-S109
Non-adherence readmissions: Patient stopped DAPT 10 days ago for a surgical procedure,
wasn’t sure when/if to restart. Presented with USA and required new stent
Patient who had stent 10 months ago stopped second antiplatelet as couldn’t afford it until next pay. 3 days later presented with a STEMI and was restented.
Patient travelling for work from Sydney and forgot his meds, presented after 3 days with USA.
Patient living 30km out of Collie and his car broke down, so couldn’t get his script filled. Stopped all medications and presented to hospital one week later (mate drove him) with stenosis of his stent.
How prevalent is non-adherence? Most studies of ACS medications report around 60-
70% compliance
Some registries in Canada report that only 78% of patients filled an ACS script within 120 days of an MI and at 2 years only 36% were still
getting scripts dispensed
Reasons for non-adherence Lack of understanding of CAD
Not believing/understanding evidence for medication
Beliefs of friends/family or culture
Expectation of ADRs
Dr Google
Financial issues
Forgetting doses
Fasting for procedure
Don’t want to take medications
Reasons for non-adherence Travelling
Depression or other mental health diseases
Busy
Moved house/suburb
Lost the scripts
Too many tablets
Felt well
‘names change all the time’ – use of generics by pharmacies
Overcoming non-adherence Knowledge about CAD, what the medications are for
and the risks of not taking them
Ensuring counselling and information is provided in a format the patient can read/understand
Provision of the 1st month supply from the hospital on d/c
Cardiac rehabilitation groups/classes
Team approach to patient care
Higher doses split to last longer
Dosing once a day to increase compliance
Overcoming non-adherence Setting alarms/family reminders for dosing times
Updating patient lists when changes are made
Following days of the week on the pill packet
Mark off doses in a calendar
Poly pills/combinations
Use of Dose aids
Use of phone apps/text messages
Overcoming non-adherence A good medication reconciliation during hospital
admission
Communication with other prescribers/healthcare providers
Regular review of medications and removal of any that are no longer required
Enrolment of patients in the CTG program
Use 0f patient focussed medication information leaflets

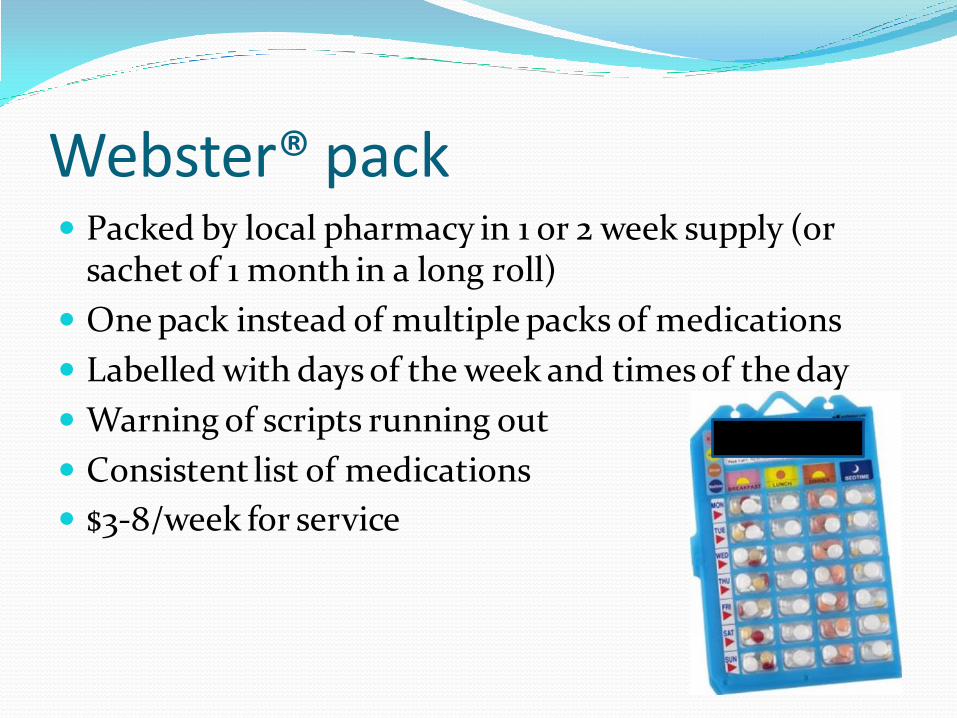
Webster® pack Packed by local pharmacy in 1 or 2 week supply (or
sachet of 1 month in a long roll)
One pack instead of multiple packs of medications
Labelled with days of the week and times of the day
Warning of scripts running out
Consistent list of medications
$3-8/week for service
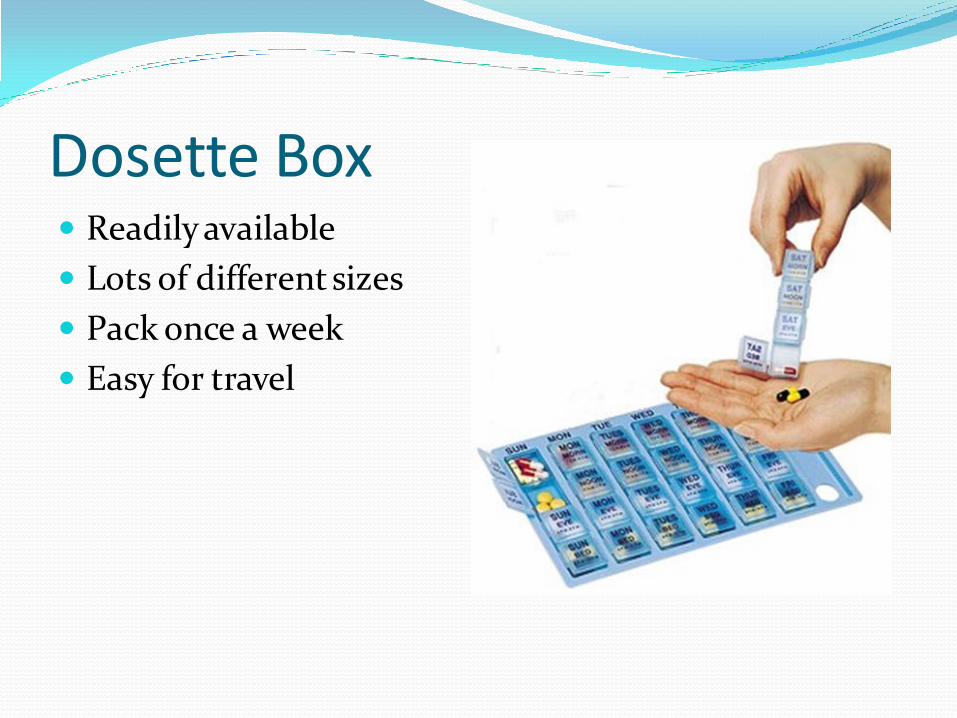
Dosette Box Readily available
Lots of different sizes
Pack once a week
Easy for travel

Phone apps MHML – heart foundation
Pharmacy app

My Heart My Life App
Manage and search for medicines
List the dose and frequency of medicines and set reminders to take them
Record and monitor health information such as weight, blood pressure and cholesterol
Learn about heart attack warning signs and what to do.
Search recipes to find healthier meals.
Missing doses Try not to miss doses
Better to miss than double up
If ever unsure/can’t remember – miss and take the next scheduled dose
Doubling up of doses can cause increased risk of ADRs or admissions to hospital
Mrs LC 46yr old female
Admitted with ACS May 2020
Brought her meds to hospital:
Aspirin/Clopidogrel 100/75mg morning
Ramipril 5mg morning
Atorvastatin 80mg night
Metformin/Sitagliptin 1000/50mg BD
Amlodipine 5mg morning
Gliclazide 120mg morning
Mrs LC Patient had all her usual medications charted and was
prepared for an angiogram.
A couple of hours after morning medications, Mrs LC suddenly dropped her BP, felt dizzy and nauseous.
What could be the cause??
Pharmacist did a medication reconciliation the day after her admission and discovered the patient’s boxes/bottles were all dispensed in January 2020!
Mrs LC On further questioning by the pharmacist:
Patient admitted to only taking the medications occasionally
She had issues with the costs of the medications
There were too many for her to remember
She felt well
She isn’t too sure of what they are for

Mrs LC Had an angiogram and received a new DES.
Agreed to take tablets as she didn’t ‘want to come back to this place or have that pain again’
Her medications were simplified to a once daily regimen and combined where possible.
She was given a new medication list and had the pharmacist write what each was for and explain the rationale for use after her stent.
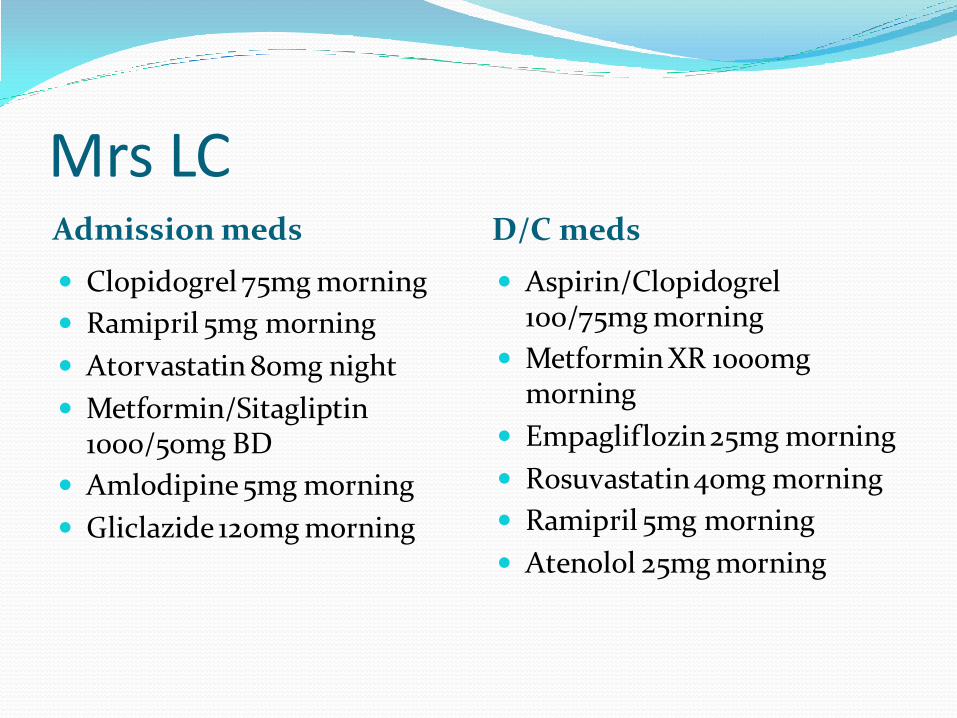
Mrs LC Admission meds D/C meds
Clopidogrel 75mg morning
Ramipril 5mg morning
Atorvastatin 80mg night
Metformin/Sitagliptin 1000/50mg BD
Amlodipine 5mg morning
Gliclazide 120mg morning
Aspirin/Clopidogrel 100/75mg morning
Metformin XR 1000mg morning
Empagliflozin 25mg morning
Rosuvastatin 40mg morning
Ramipril 5mg morning
Atenolol 25mg morning
Mr PW post d/c Has he had an BP readings
done since d/c? How is he actually taking his
medications (does he have his medication list to show you?)
Did he get new scripts from the GP/pharmacy?
How has he been feeling since d/c?
Any symptoms of dizziness/lightheadedness/lethargy? (or other side effects relating to the medications)
No
Yes he has the list in his phone
Yes, although he missed a few days of some of them as he couldn’t get to the pharmacy
Dizzy when he gets up sometimes
Some muscle aches at night
Questions What should we recommend to Mr PW?
Check BP regularly, pharmacy can provide this for free
Reminders about taking the medications regularly, setting an alarm on his phone etc
Move Ramipril to night to see if dizziness settles and consider up titration of the dose next visit depending on his BP readings
Magnesium for muscle aches as first line (before altering statin dose)
Mr LH 64yr old known heart failure patient who is admitted
in cardiogenic shock
Admission meds
Sacubitril/valsartan (Entresto®) 24/26mg morning
Bisoprolol 2.5mg morning
Apixaban 5mg twice daily
Spironolactone 25mg morning
Furosemide 40mg morning
Rosuvastatin 10mg morning
Entresto® Sacubitril/Valsartan (neprilysin inhibitor and ARB)
Used to decrease HF mortality, admissions and progression
Trial doses recommend 97/103mg twice daily
DO NOT use with ACEi (should have 36-48 hour wash out when swapping), but must have trialled ACEi or ARB first
Start with lowest dose and increase slowly
Common for causing dizziness and a fall in BP
Can cause hyperkalaemia and renal dysfunction
Entresto® Up titrate:
High BP
Regular HF admissions/decompensations
Down titrate:
Low BP
Dizziness or syncope
Hyperkalaemia
Worsening renal function
Spironolactone/Eplerenone Aldosterone Antagonists to help cardiac remodelling
Reduce HF mortality
Usually 12.5-50mg daily
Eplerenone is used only if patients have had recent MI
Spironolactone may cause galactorrhea or breast development in males
Watch for hyperkalaemia, increased creatinine
Spironolactone/Eplerenone up titrate when patients have more frequent HF
admissions or decompensations if:
BP can tolerate AND
Renal function remains stable
Down titrate if:
BP low and patient symptomatic
Renal function deterioration
Hyperkalaemia
Intolerance to side effects

Nitrates Used for symptomatic relief only (no mortality
benefit)
Short acting option is Nitrolingual® Spray
No dose titration, should be 1-2 doses over 10 mins then call an ambulance
Can drop BP and cause dizziness
Long acting option isosorbide mononitrate tablets (30-120mg daily) or glyceryl trinitrate patches (5-15mg daily)
Needs a nitrate free period (minimum 8 hours a day)
Nitrates Up titrate
Increasing angina symptoms
Increased BP
Increased nocturnal dyspnoea
Down titrate Low BP
Headache
Dizziness
No change to angina symptoms
Caution with other meds effecting BP – sildenafil etc
Diuretics Symptomatic relief, no mortality benefits To decrease fluid overload/SOB/ankle oedema Up-titrate
Increasing weight Increased SOB/inability to lay flat etc.
Down titrate: Dehydration Low BP Increased creatinine Rapid weight reduction
Patient’s often self titrate based on their fluid intake/daily weight
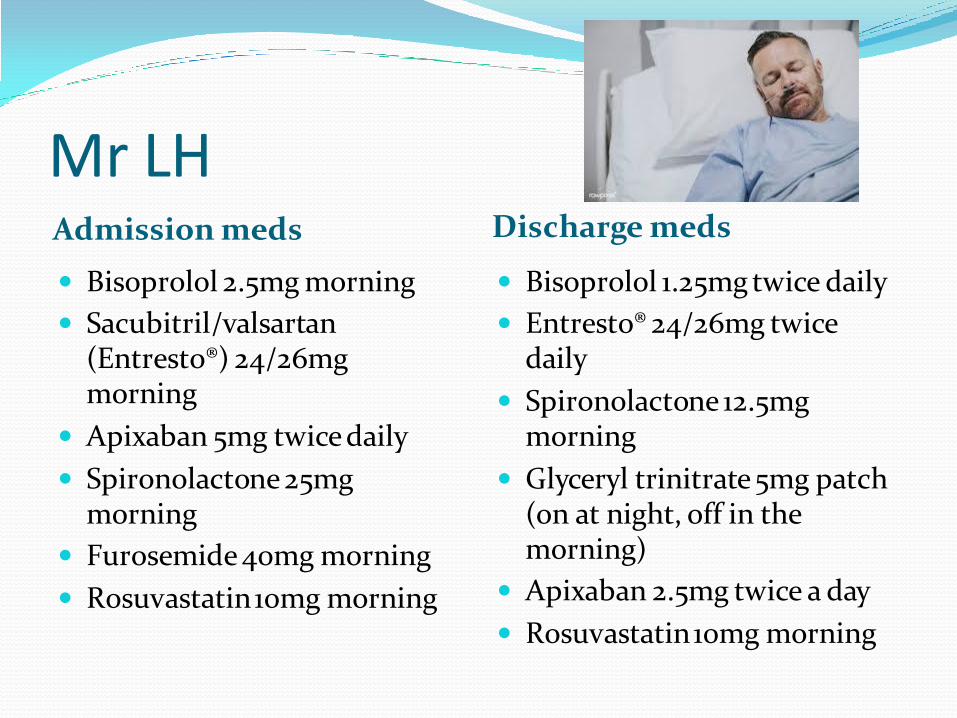
Mr LH Admission meds
Discharge meds
Bisoprolol 2.5mg morning
Sacubitril/valsartan (Entresto®) 24/26mg morning
Apixaban 5mg twice daily
Spironolactone 25mg morning
Furosemide 40mg morning
Rosuvastatin 10mg morning
Bisoprolol 1.25mg twice daily
Entresto® 24/26mg twice daily
Spironolactone 12.5mg morning
Glyceryl trinitrate 5mg patch (on at night, off in the morning)
Apixaban 2.5mg twice a day
Rosuvastatin 10mg morning
How do we involve the patient? Reporting symptoms – what do we want to know?
Does something cause them dizziness/light headedness?
Do they have to stop ADLs for any reason?
What are their weights? Is this changing?
When did they have a BP check?
Do they feel palpitations?
Do they have angina?
Are they having issues taking/remembering their medications?
What are “normal” obs? There are NO normal obs
What is normal for this patient?
What can a patient actually tolerate without symptoms?
In general we try to aim for:
SBP <110
Resting HR in 60s
Titration tips Try not to look at the numbers – look at the clinical
picture
Check adherence to medications before changing anything
Is the patient symptomatic?
Are they able to perform ADLs?
Treat the CV disease and not the number


References National Heart Foundation ACS guidelines
Non adherence to cardiovascular medications, EurHeartJ 2014
Cardiovasc Disease, Drug Therapy and Mortality in Covid -19, NEJM 1st May 2020
Heart Foundation website
FSH cardiac rehab talk and pharmacy department