Embed Size (px)
Citation preview
Promoting partnership in knowledge translation: the NIHR CLAHRC approach
Kate Gerrish, PhD, RNProfessor of Nursing ResearchUniversity of Sheffield/Sheffield Teaching Hospitals NHS Foundation Trust
NIHR CLAHRC for South Yorkshire
5 year NIHR funded programme of applied research and implementation of research focusing on self management and self care for long-term conditions
BarnsleyDoncaster
Rotherham Sheffield
NIHR Collaboration for Leadership in Applied Research and Care for South Yorkshire (CLAHRC)
CLAHRC – key features
£20 million over 5 years – £10m from NIHR with matched funding from partners
Collaborative between universities, NHS commissioners and healthcare providers
Partnership working to support capacity building for research and implementation
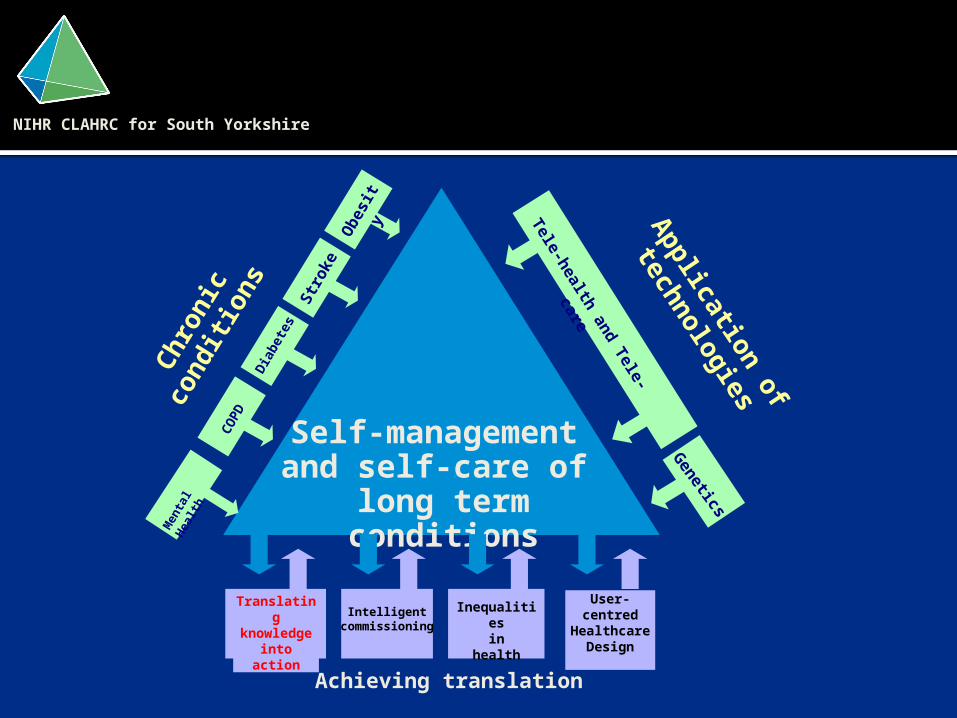
Self-management and self-care of
long term conditions
NIHR CLAHRC for South Yorkshire
Chro
nic
condit
ions
CO
PD
Dia
bet
esStr
oke
Obesi
ty A
pplication
of
technolog
ies
Genetics
Tele-health
and Tele-
care
User-centred
Healthcare Design
-
Achieving translation
Translating knowledge
intoaction
Intelligentcommissionin
g
Inequalitiesin
health
Men
tal H
ealth
Aim: To develop step change in the way research findings are implemented in practice • by …
• trialling and evaluating innovative implementation strategies to facilitate evidence-based care
• in order to …• enhance service quality,
contribute towards improving patient outcomes, and/or increase patient safety
Translating knowledge into action (TK2A)
Develop, pilot and evaluate implementation strategies to promote evidence-based practice in response to identified service priorities
Disseminate successful initiatives across CLAHRC partnership
Develop the capacity of health care professionals to engage in KT implementation & KT research
Establish collaborations between NHS and academic partners to facilitate knowledge translation
Contribute to the field of implementation science
TK2A objectives
Contribution to implementation science
Contribute new knowledge to the field of KT• Understanding the trajectory of complex innovation in
healthcare settingsTest and further refine existing theoretical frameworks for KT• Knowledge to Action - Graham et al 2005• Consolidated framework for implementation research -
Damschroeder 2009Contribute to the further development of key concepts in KT• Knowledge brokering• Boundary spanning
Undertake KT evaluation• Knowledge translation case book• Evaluation of After Action Review methodology
Knowledge translation
KT is a dynamic, iterative process that includes the synthesis, dissemination, exchange, and ethically sound application of knowledge within a complex system of interactions among researchers and users with the intention to improve the health of (Canadians), provide more effective health services and products, and strengthen the health care system
CIHR 2006
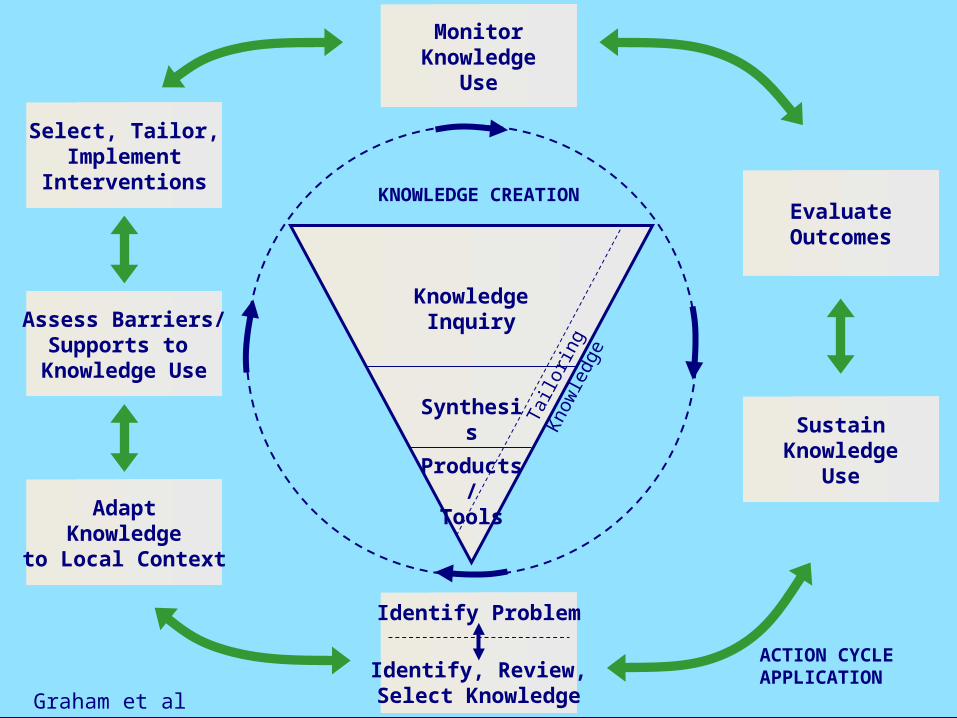
MonitorKnowledge
Use
SustainKnowledge
Use
EvaluateOutcomes
AdaptKnowledge
to Local Context
Assess Barriers/Supports to
Knowledge Use
Select, Tailor,Implement
Interventions
Identify Problem
Identify, Review,Select Knowledge
Products/
Tools
Synthesis
Knowledge Inquiry
Tailo
ring
Kno
wle
dge
KNOWLEDGE CREATION
ACTION CYCLEAPPLICATION
Graham et al 2006
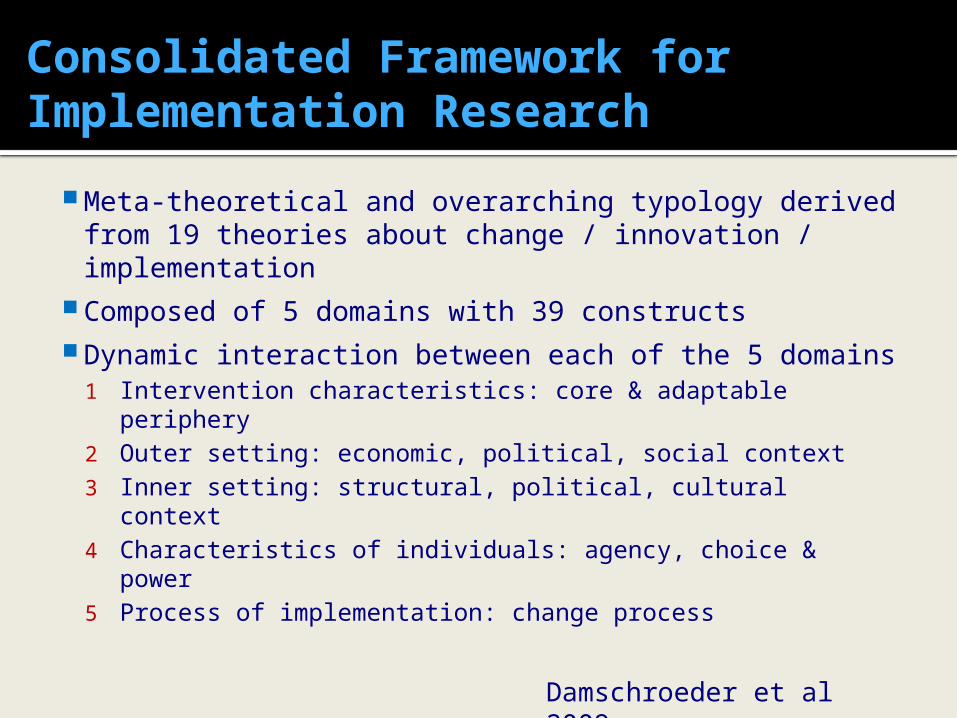
Consolidated Framework for Implementation Research
Meta-theoretical and overarching typology derived from 19 theories about change / innovation / implementation
Composed of 5 domains with 39 constructs Dynamic interaction between each of the 5
domains1 Intervention characteristics: core & adaptable
periphery2 Outer setting: economic, political, social context3 Inner setting: structural, political, cultural context4 Characteristics of individuals: agency, choice & power5 Process of implementation: change process
Damschroeder et al 2009
Clinically focused KT projects
Management of
patients with
dysphagia
Oral nutrition
support for patients at
risk of malnutritio
n
Reducing the risk of hospital acquired
VTE
TK2A - approach
Focus NHS
Priorities
Partnership
working
Evidence-based
approaches
Capacity building
Focus on healthcare (NHS) prioritiesPriorities identified by health care partners - links to national policy initiatives• Quality Innovation, Productivity, Prevention,
(QIPP)• Commissioning for Quality & Innovation
(CQIN).• NICE guidelines, national guidanceLocal health priorities
• Health needs• Identified shortfalls in care• Focus on complex issues rather than quick
fixes
Partnership working
Projects embedded within the NHS
Shared ownership & responsibility for success
Focus on multi-disciplinary teams to change practiceWorking at different levels across the organisationParticipatory ways of working to achieve changeBoundary spanning and knowledge brokering roles
Evidence-based approachUtilise knowledge from implementation science
CIHR ‘Knowledge to Action’ framework to guide implementation, informed by CFIR
Evidence-based approaches to implement change, adapted to local context
Embedded evaluation
Capacity building for KT
Individuals• Knowledge translation facilitator secondments from
NHS partners• Knowledge translation research secondments from
HEI partners• PhD, post doctoral fellowships• NIHR MSc Clinical Research, ACF medicine, CATP for
nurses, AHPsClinical teams• KT skills development – evidence appraisal, change
management, evaluation etc.
Managers• KT engagement / culture – evidence informed local
policy and practice, evaluative culture
Enhancing the quality of oral nutrition support: EQONS
Aim• To enhance the quality
of oral nutrition support provided by the multi-disciplinary team to adult patients with long-term conditions through the implementation of a malnutrition screening tool (MUST+) and associated care guidelines
Objectives• To trial and evaluate two
interventions designed to facilitate the uptake of MUST+ and care guidelines• Ward-based nutrition
champions• Facilitation of the
multi-disciplinary team by a dietitian
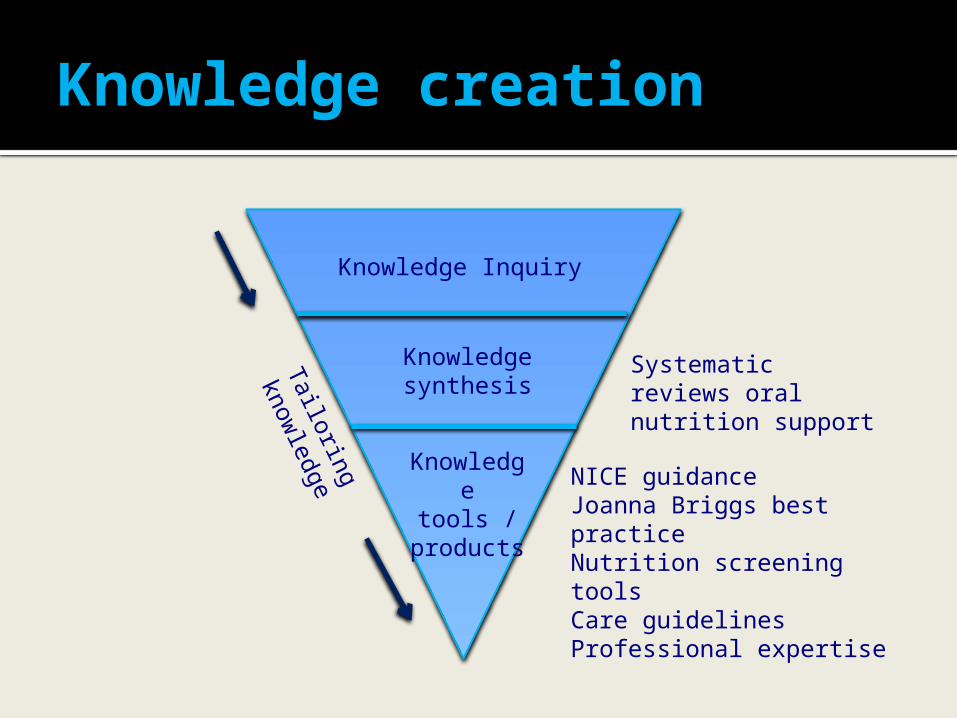
Knowledge Inquiry
Knowledge synthesis
Knowledge tools / products
Tailoring
knowledge
Systematic reviews oral nutrition support
NICE guidanceJoanna Briggs best practiceNutrition screening toolsCare guidelinesProfessional expertise
Knowledge creation
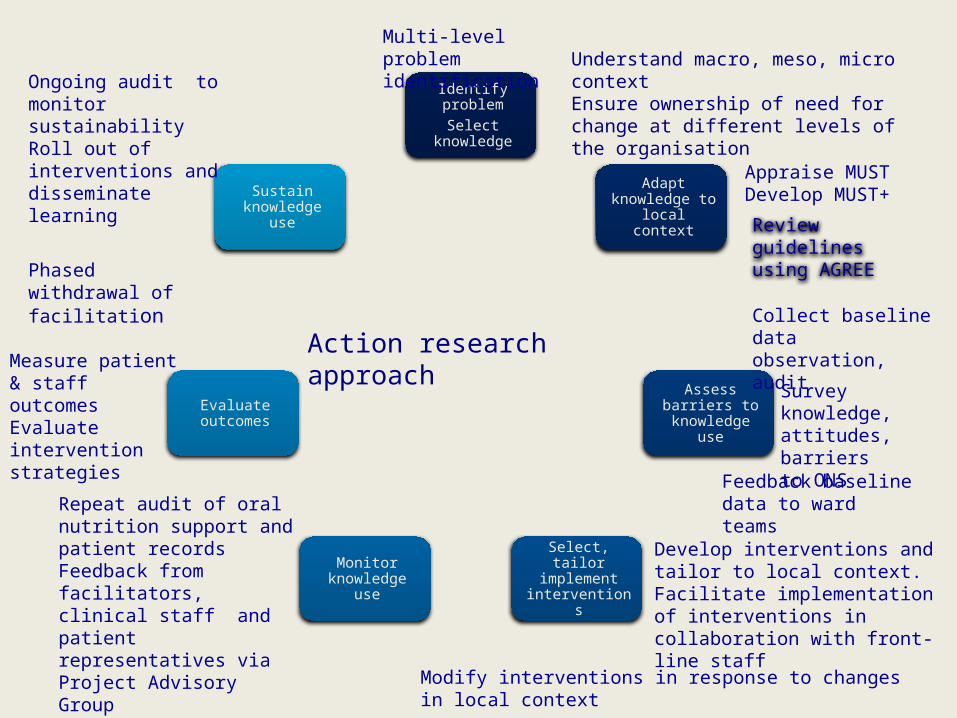
Identify problemSelect
knowledge
Adapt knowledge to local context
Assess barriers to knowledge
use
Select, tailor implement
interventions
Monitor knowledge use
Evaluate outcomes
Sustain knowledge use
Review guidelines using AGREE
Appraise MUST Develop MUST+
Action research approach
Multi-level problem identification Understand macro, meso, micro
contextEnsure ownership of need for change at different levels of the organisation
Collect baseline data observation, audit
Survey knowledge, attitudes, barriers to ONSFeedback baseline
data to ward teams
Develop interventions andtailor to local context.Facilitate implementation of interventions in collaboration with front-line staff
Modify interventions in response to changes in local context
Repeat audit of oral nutrition support and patient recordsFeedback from facilitators, clinical staff and patient representatives via Project Advisory Group
Measure patient & staff outcomesEvaluate intervention strategies
Phased withdrawal of facilitation
Ongoing audit to monitor sustainabilityRoll out of interventions and disseminate learning
Time and tide waiteth for no man • Geoffrey Chaucer
14th Century poet
Swampy lowlands of practice rather than hard ground of theory • Donald Schon
1983
Implementation in the real world
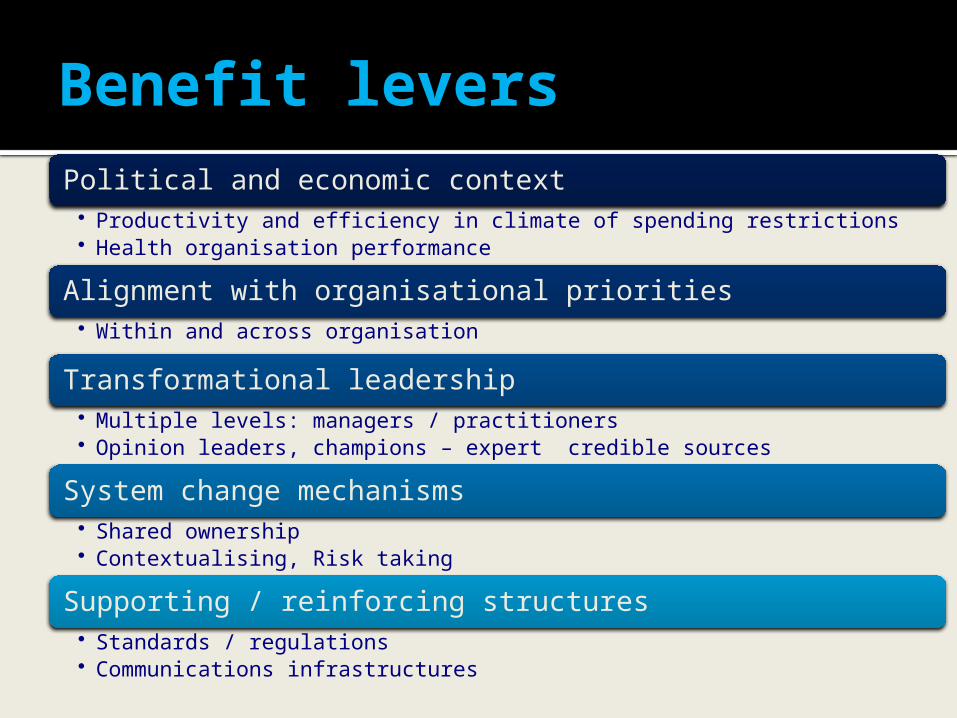
Benefit leversPolitical and economic context
• Productivity and efficiency in climate of spending restrictions• Health organisation performance
Alignment with organisational priorities• Within and across organisation
Transformational leadership• Multiple levels: managers / practitioners• Opinion leaders, champions – expert credible sources
System change mechanisms• Shared ownership• Contextualising, Risk taking
Supporting / reinforcing structures• Standards / regulations• Communications infrastructures
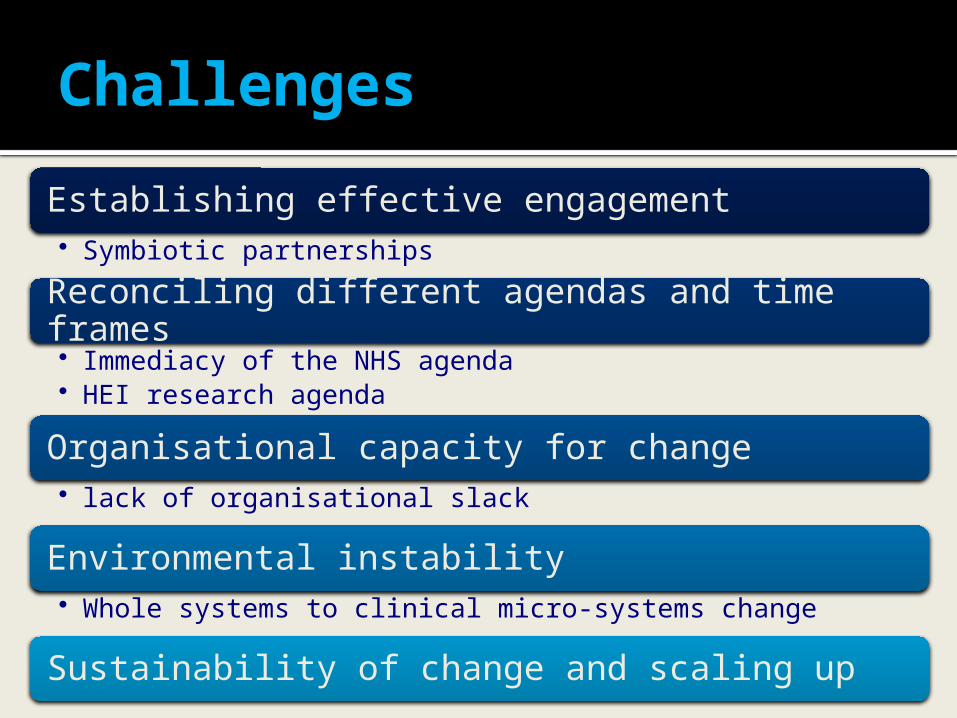
Challenges
Establishing effective engagement• Symbiotic partnerships
Reconciling different agendas and time frames• Immediacy of the NHS agenda• HEI research agenda
Organisational capacity for change• lack of organisational slack
Environmental instability• Whole systems to clinical micro-systems change
Sustainability of change and scaling up
Challenges
Implementation in the real world is complex and messyWe need to be prepared to deal with unpredictability, be able to adapt and cope with complexity
Lessons learnt Understanding the context at macro, meso and micro levelThe rapidly changing context requires different ways of workingEmbedding implementation projects within the organisation • Board to bedside ownership• Identifying champions at different levels• Partnership working at all levels of the organisation(s)• Drawing upon existing systems and processes
Boundary spanners• Understanding different cultures and contexts• Speaking different languages to different audiences / stakeholders• Managing different and at times competing agendas• Operating at different levels of the organisation
• Expertise in implementation science, change management, evaluation methodologies
• Extra resources to support healthcare providers to meet objectives linked to quality, safety, effectiveness agenda
• Use evidence-based approaches to implement change adapted to the local context
• Focus on complex issues rather than quick fixes
• Participatory ways of working with on-going feedback to enhance quality
• Focus on sustainability and spread of innovation
• Positive impact on meeting NHS priorities – e.g. CQUINS, CQC, QIPP
• Sharing learning and resources across CLAHRC SY
Added value to NHS
• Collaboration with healthcare providers to support research
• Enhanced grant capture• Mechanisms to facilitate greater
impact of research• Expertise in implementation science• Capacity building
Added value to HEI
Conclusions
The CLAHRC partnership model provides a means of harnessing the capacity of higher education and the NHS to facilitate knowledge translation