Embed Size (px)
Citation preview
Kasia Munson, MD
Emergency Medicine
PGY 2
*
*
*Define Hypothermia
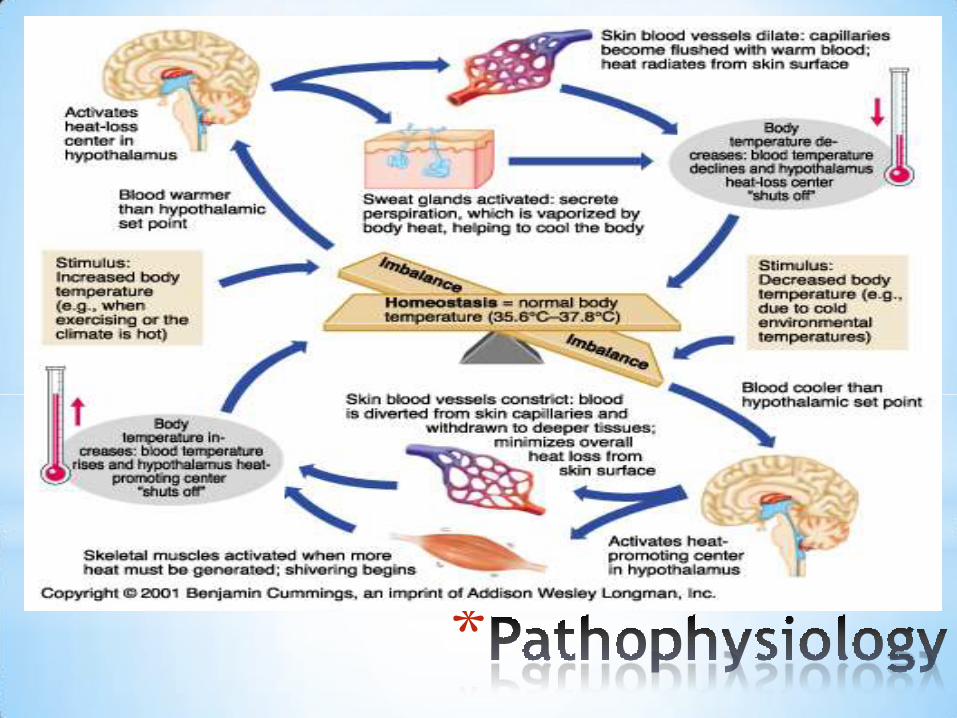
*Pathophysiology of temperature regulation
*Physiologic changes in hypothermia
*Labs and Drugs in hypothermia
*Various rewarming methods
*Disposition

*
Accidental Hypothermia is defined as an unintentional drop in core body temperature below 35 C.
Mild = 32C – 35C
Moderate = 28C – 32C
Severe = <28C
*
*Mortality (in-patient)
1999 to 2011, a total of 16,911 deaths in the United States, an average of 1,301 per yearOverall - 12%
Moderate - 21%
Moderate – severe – 40%
*Sex
67% Males
*Age
Increased risk at extremes of age
50% of the recorded deaths > 65 years old
*
*
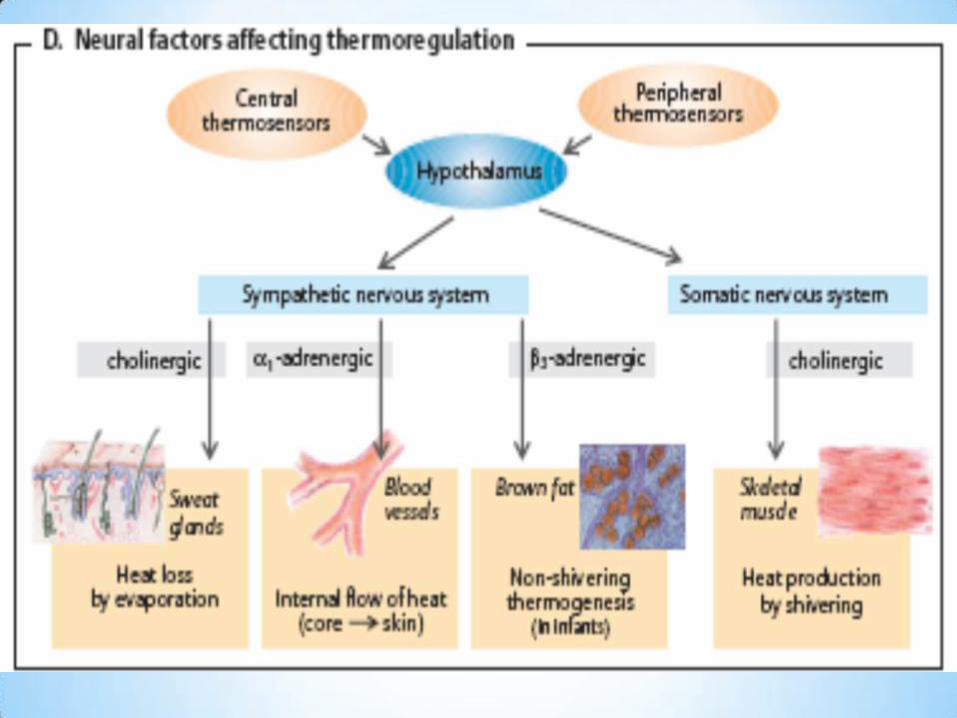
*Hypothalamus: Shivering thermogenesis and
non-shivering heat conservation and
dissipation.
*Cold hypothalamus TRH pituitary
gland TSH thyroid gland thyroxine
*Sympathetic vasoconstriction
*
*Evaporation –insensible losses and sweat
*Radiation – infrared electromagnetic energy
*Conduction –transfer to a cooler adjacent object
*Convection – transfer convective currents of air or water

*
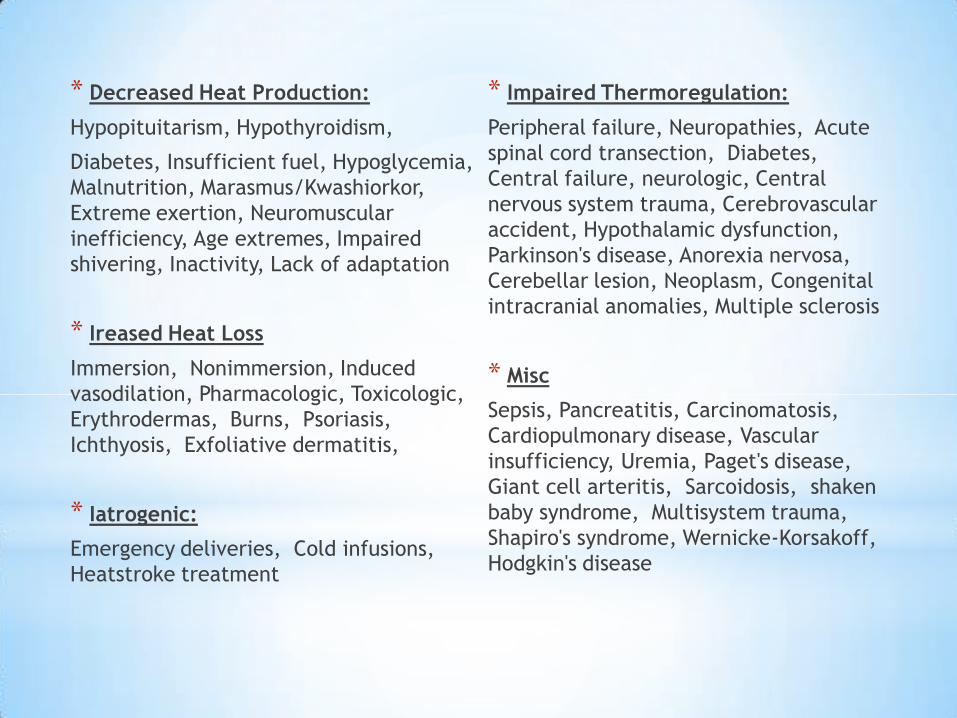
* Decreased Heat Production:
Hypopituitarism, Hypothyroidism,
Diabetes, Insufficient fuel, Hypoglycemia,
Malnutrition, Marasmus/Kwashiorkor,
Extreme exertion, Neuromuscular
inefficiency, Age extremes, Impaired
shivering, Inactivity, Lack of adaptation
* Ireased Heat Loss
Immersion, Nonimmersion, Induced
vasodilation, Pharmacologic, Toxicologic,
Erythrodermas, Burns, Psoriasis,
Ichthyosis, Exfoliative dermatitis,
* Iatrogenic:
Emergency deliveries, Cold infusions,
Heatstroke treatment
* Impaired Thermoregulation:
Peripheral failure, Neuropathies, Acute
spinal cord transection, Diabetes,
Central failure, neurologic, Central
nervous system trauma, Cerebrovascular
accident, Hypothalamic dysfunction,
Parkinson's disease, Anorexia nervosa,
Cerebellar lesion, Neoplasm, Congenital
intracranial anomalies, Multiple sclerosis
* Misc
Sepsis, Pancreatitis, Carcinomatosis,
Cardiopulmonary disease, Vascular
insufficiency, Uremia, Paget's disease,
Giant cell arteritis, Sarcoidosis, shaken
baby syndrome, Multisystem trauma,
Shapiro's syndrome, Wernicke-Korsakoff,
Hodgkin's disease

*
*Decreased Heat Production
*Increased Heat Loss
*Ethanol
*Impaired Thermoregulation
*Iatrogenic
*Infections
*Trauma
*Miscellaneous Causes

*
*
*Patients may recover completely after presenting in a rigid, apneic state with fixed and dilated pupils.
*Resuscitative efforts should be continued until core temperature is at least 30°C to 32°C
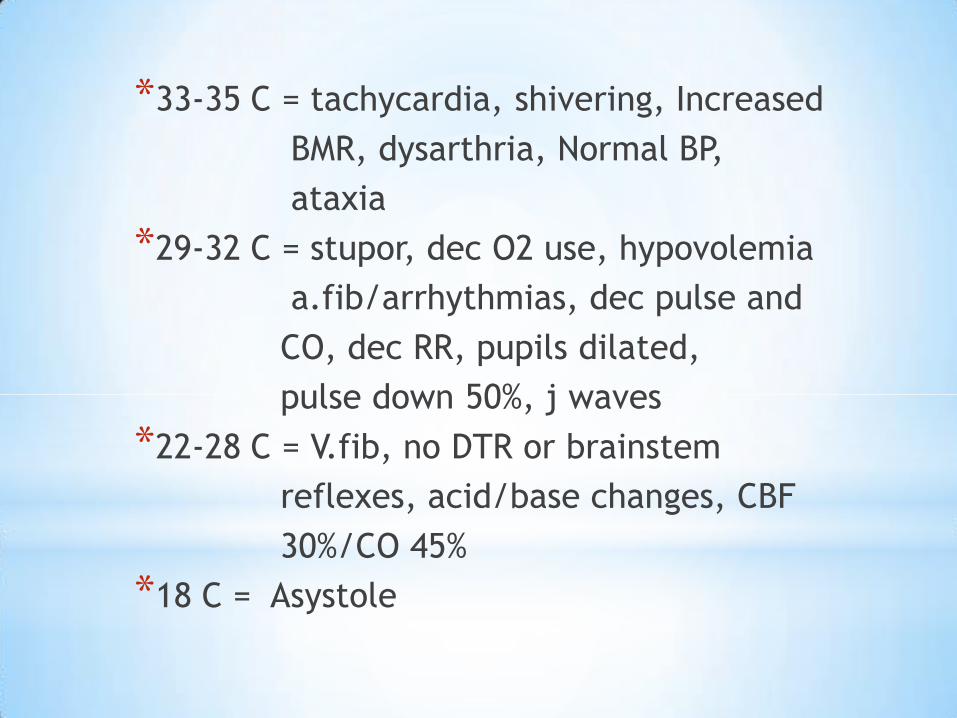
*33-35 C = tachycardia, shivering, Increased
BMR, dysarthria, Normal BP,
ataxia
*29-32 C = stupor, dec O2 use, hypovolemia
a.fib/arrhythmias, dec pulse and
CO, dec RR, pupils dilated,
pulse down 50%, j waves
*22-28 C = V.fib, no DTR or brainstem
reflexes, acid/base changes, CBF
30%/CO 45%
*18 C = Asystole
*Central Nervous System
*Cerebral autoregulation is maintained with an increase
in vascular resistance until 25° C.
*Progressive depression of CNS, some responsive with
intact reflexes at 27 to 25° C.
*EEG flat < 20C
*Reflexes hyperactive to 32C then hypoactive to 26C
then disappear.
*
*Tachycardia progressing to bradycardia
*Atrial fibrillation < 32° C.
*Pulse < 50% at 28° C.
*Asystole and VF spontaneously < 25° C.
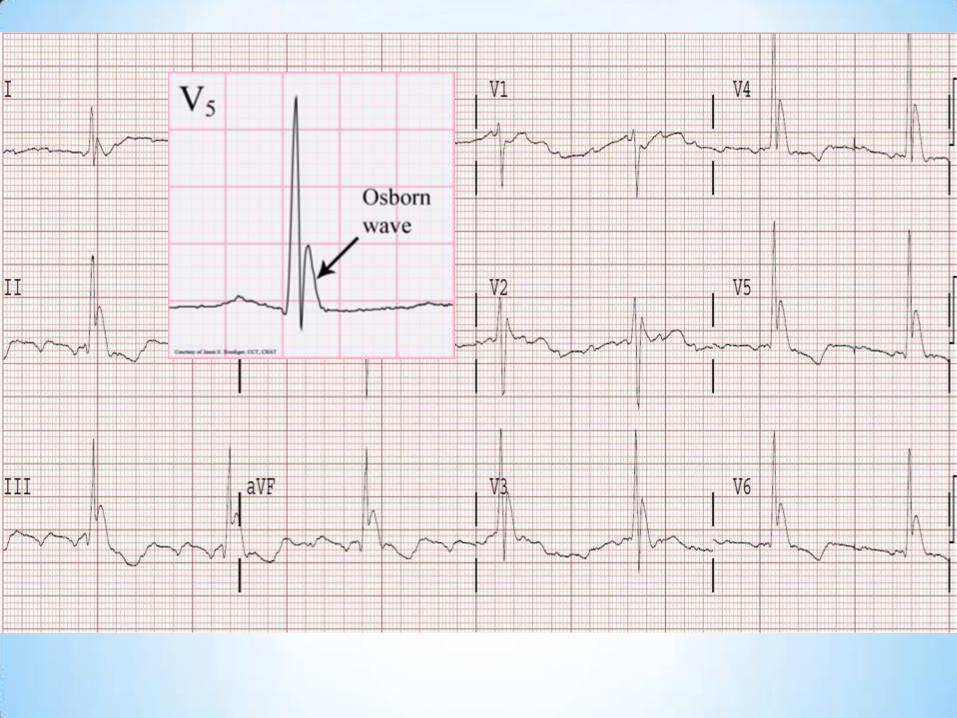
*EKG - the Osborn (J) wave
*
* Increased RR then progressive decrease
*Oxygen unloading capacity is <50%
*Carbon dioxide production decreases 50%
*Viscous bronchorrhea, and noncardiogenicpulmonary edema.
*depression of cough and gag reflexes
*
*Renal Blood Flow <50% at 27 to 30° C
*Cold induced diuresis
*Stiff to pseudo–rigor mortis to opisthotonos.
*Fixed, dilated pupils
*
*What exactly IS a core temperature?
*What is the best way to obtain one?

*

*
*Glucose (POC)
*ABG (uncorrected)
*CBC
*CMP (with Ca, Mg)
*Amylase and Lipase
*PT/PTT/INR
*ABG’s
*Acidosis - due to severe respiratory
depression and carbon dioxide retention
*Alkalosis - from diminished CO2
production with low metabolic rates
*Hypothermia causes a leftward shift of
the oxyhemoglobin dissociation curve
*
*CBC
*Leukocytes and platelets low
*Hct deceptively increased
*Electrolytes
*Potassium
*Glucose
*Sodium
*
*Increased thrombosis
*DIC picture
*Clinically coagulopathic

*
*Lipase
*Cortisol
*Thyroid
*
*The efficacy of most medications is
temperature dependent
*Pharmacologic manipulation of the pulse
and blood pressure should be avoided.
*Dysrhythmias: Most convert spontaneously
during rewarming
*Transvenous intracardiac pacing is
hazardous
*
*Thiamine
* Antibiotics, steroids, and thyroid hormone
*Hydrocortisone
*Thyroid hormone
*
*If a patient's mental status remains altered despite
rewarming, CNS injury or infection should be
suspected.
*In children younger than 3 months, empirical
antibiotics after culture are indicated.
*Adults - Antibiotics should be administered if the
clinical picture is consistent with septic shock, if
there is failure to rewarm, or if aspiration has
occurred.

*
*Patients who are cold, stiff, and cyanotic,
with fixed pupils and inaudible heart
tones, without visible thoracic excursions,
continue to be successfully resuscitated.
*
*Remove from the cold
*careful, gentle handling
*Warm Oxygen and IV fluids
*Most rhythm disturbances require no
therapy and revert spontaneously with
rewarming.
*
*Temperature
Esophageal probe is ideal.
Alternatively, rectal or bladder probe.
*Blood Pressure
May need doppler
*O2 Sat
Uncertain reliability with poor
perfusion.
*Urine Output
Foley should be placed for accurate
measurement.
*Volume Resuscitation
*Fluids administered intravenously should be heated to 40 to 42° C.
*Rapid central venous administration may produce myocardial thermal gradients
*Most patients will be free water depleted
*
*If VT or VF is present, defibrillation should be attempted. If the single defibrillation attempt is unsuccessful, active rewarming should be initiated and CPR continued until core temperature is above 30° C.
*Use ACLS?
*Use Vasopressors?
*Advanced Life Support
*CPR should not be withheld unless DNR, obviously lethal injuries, chest wall depression is impossible, signs of life are present.
*If possible, verify with Doppler ultrasound examination that there is no spontaneous mechanical cardiac activity before chest compressions are initiated.
*
*No controlled studies comparing
rewarming methods in hypothermia
exist, rigid treatment protocols
would not be evidence based
*
Passive rewarming
* Removal from cold environment
* Insulation
Active external rewarming
* Warm water immersion* Heating blankets set at
40°C (104°F)* Radiant heat* Forced air
Active Core rewarming
* Inhalation rewarming* Heated IV fluids* GI tract lavage* Bladder lavage* Peritoneal lavage* Pleural lavage* Extracorporeal
rewarming* Mediastinal lavage by
thoracotomy
*
*By far the most important consideration
in the selection of rewarming techniques
is the patient’s cardiovascular status; a
secondary consideration is the presenting
temperature.
*
*Mild Hypothermia = Passive or
minimally invasive
*Cardiovascular instability = rapid
rewarming. ECMO if available.
*Stable patients are more
controversial.
*
*Must have intact thermoregulatory
mechanisms and be capable of
metabolic heat production
*
*Non-Invasive
*Treatment of choice for mild
hypothermia
*Minimizes convection and
evaporation
*
*Direct transfer of exogenous heat to patient
*External or Internal
*Impaired thermoregulation
*DKA
*Cardiovascular instability
*Moderate or severe hypothermia (≤32.2° C)
* Inadequate rate of rewarming or failure to
rewarm
*Traumatic or toxicologic peripheral vasodilaton
*Inhalation rewarming = humidified oxygen
by facemask or ET tube
* IV fluids and blood should be warmed to
40°C (104°F) before administration
*
*The Bair Hugger is most practical in
the emergency department
*Arteriovenous anastomosis (AVA)
*Combining of truncal AER with core
rewarming can also be successful.
*
*Delivers dialysate at 40 to 45° C to
the peritoneal cavity
*Rates average 1 to 3° C/hr
*Hepatic rewarming
*
*Gastric or colonic irrigation can cause
fluid and electrolyte fluxes. These techniques are
rarely indicated.
*Closed thoracic lavage - reserved for the
severely hypothermic patient who does not respond
to standard techniques or the patient with another
indication for a chest tube. rewarming averages
3° C/hr
*Mediastinal irrigation and direct
myocardial lavage - only in patients without
spontaneous perfusion.
*
*Ultrasonic and low-frequency microwave irradiation.
* One study rewarmed 16 piglets with microwave irradiation, another 20 human babies.
*Diathermy is still experimental
*
*Venovenous (2-3° C/hr)
Central venous to central venous or peripheral
catheter. No oxygenator/circulatory support
*Hemodialysis (3-4° C/hr)
Single- or dual-vessel cannulation, Stabilizes
electrolyte or toxicologic abnormalities.
*
*Arteriovenous (3-4° C/hr)
Percutaneous 8.5F femoral catheters . Requires
blood pressure of 60 mm Hg systolic. No
perfusionist/pump/anticoagulation.
*Cardiopulmonary bypass (up to 9.5° C/hr)
Cardiopulmonary bypass circuit Full circulatory
support with the pump and oxygenator
*
*Uncomplicated - low mortality rate
*Significant associated diseases - worse prognosis
*Asphyxia or near-drowning – very poor
*Grave prognostic indicators include evidence of
intravascular thrombosis (fibrinogen < 50 mg/dL),
cell lysis (hyperkalemia > 10-12 mEq/L), and
ammonia levels greater than 250 mmol/L
*
*Mild = Home
*Almost all others = Admission

*
1. Aslam EF, Aslam AK, Vasavada BC. Hypothermiea: evaluation, electrocardiographic manifestations and management. AM J Med. 2006; 119:297-301
2. Brown D, Brugger H. Accidental Hypothermia. N Engl J Med 2012; 357:1930-8
3. Boue Y, Lavolaine J. Neurologic Recovery from Profound accidental hypothermia after 5 hours of cardioupulmonaryrescutation. Crit Care Med2014 42:e167-170
4. Center for Disease Control and Prevention. QuickStats: Number of Hypothermia-Related Deaths,* by Sex — National Vital Statistics System, United States,† 1999–2011§. Jan 2013 / 61(51);1050. MMWR
5. Danzl DF: Hypothermia and frostbite. In Fauci AS, et al (eds): Harrison's Principles of Internal Medicine, 17th ed. New York, McGraw-Hill, 2008.
6. Farstad M Andersen KS. Rewarming from accidental hypothermia by extracorporeal circulation, A retropective study. Euro J Cargio Surg 20:2001, 58-64
7. Freude T, Gillen S Therapeutic peritoneal lavage with warm saline solution as an option for critical hypothermia trauma patient. Cen Euro J Med Apr 2013
8. Gilbert M, Busund R Resuscitation from accidental hypothermia of 13.7C with circulatory arrest The Lancet Vol 355 Jan 2000
9. Guly H. History of Acceidental Hypothermia. Resusc 82; 2011 122-125
10. Hauty M, Esrig B Prognostic Factors in Severe Accidental Hypothermia: Experiencefrom the Mt. Hood tragedy. J Traumoct 1987 Vol 27 No 10 1107-12
11. Marx, J. A., Hockberger, R. S., Walls, R. M., Adams, J., & Rosen, P. (2010). Rosen's emergency medicine: Concepts and clinical practice. Philadelphia: Mosby/Elsevier.
12. Meyer M, Pelurson N Sequela-free long-term survival of a 65-year-old woman after 8 hours and 40 minutes of cardiac arrest from deep accidental hypothermia. J Thorac Vardiovasc Surg 2014 147 e1-2
13. Morley D, Tamane K Rewarming for accidental hypothermia in an urban medical center using extracorporeal membrane oxygenation. Am J Case Rep 2013: 14: 6-9
14. Tintinalli, J. E., Kelen, G. D., & Stapczynski, J. S. (2004). Emergency medicine: A comprehensive study guide. New York: McGraw-Hill, Medical Pub. Division.
15. UpToDate.com Accidental Hypothermia
16. Vanden Hoek T, Morrison L; 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science: Part 12: Cardiac Arrest in Special Situations
17. Wanscher M, Agersnap L Outcome of accidental hypothermia with or without circulatory arrest. Experience from the Danish Praeste Fjord boating accident. Resus 83 2012 1078-84





























