Embed Size (px)
Citation preview
Karin Hahn MD, MSc2, MPH, FRCPC
Associate Professor, Schulich School of Medicine
and Dentistry, Western University, London, Ontario
Epidemiology
Approximately 3 in 10,000 deliveries are to women with breast cancer
Prevalence of pregnancy at diagnosis of breast cancer approximately 1.5%
In women < 30 years of age, the prevalence of pregnancy-associated breast cancer has been reported to be 9.7% and 25.6% (MSKCC and MDACC respectively)
Sanders CM, Baum M. J R Soc Med 1993;86:162; Anderson JM. BMJ
1979;1:1124; Anderson BO et al. Ann Surg Oncol 1996;3:204; Noyes RD et al.
Cancer 1982;49:1302
Pregnancy-associated Breast
Cancer (PABC) Breast cancer diagnosed during pregnancy or during
the 12 months following delivery.
Breast cancer diagnosed in the 12 months following
delivery is managed per standard guidelines.
Except: No breastfeeding if treatment includes
chemotherapy, trastuzumab and/or anti-estrogen
therapy.
BRCA1 and BRCA2 Mutations
and PABC
Multiple cohort studies: Women with germline BRCA1 mutations more
likely to have PABC than BRCA2 carriers.
Women with BRCA2 mutations may have increased risk of breast cancer after pregnancy.
Unclear whether association between mutations and PABC is causal or coincidental.
PABC does not appear to adversely affect survival among BRCA 1/2 survivors.
Johannsson O et al. Lancet 1998;352:1359; Tryggvadottir L et al. Breast Cancer Res
2003; 5: R121; Cullinane CA et al. Intl J Cancer 2005; 117: 988; Valentini A et al.
Breast Cancer Res Treat 2013;142:177
The Diagnosis of Breast Cancer During
Pregnancy: Diagnostic Imaging
Breast Ultrasound: studies report 100%
sensitivity and 100% negative predictive value
for PABC.
Mammography: Estimated radiation dose to
uterus 0.03 µGy (no risk of fetal harm when
exposure < the 50 mGy threshold dose).
MRI of the breast: very little published data
and controversy regarding the safety of
gadolinium in pregnancy (crosses placenta).
• Vashi R et al. Am J Roentgenol 2013;200:321
Additional Staging Investigations in
the Pregnant Breast Cancer Patient
Suspicious regional nodal disease: US and FNA
CXR: Fetal radiation exposure <0.005 cGy
Liver ultrasound
Bone scan: challenging because of radioactivity
Consider screening non-contrast MRI of the spine
if node positive disease or locally-advanced breast
cancer. Also, if complaining of persistent back pain
consider MRI.
• Hahn KME et al. Cancer 2006;107:1219; Baker J et al. Clin
Nuc Med 1987;12:519
Breast Cancer During Pregnancy:
Pathologic Diagnosis
FNA of the breast mass: cytology may be difficult to
interpret due to proliferative changes of pregnancy.
FNA of a suspicious lymph node: can diagnose
invasive breast cancer
Core biopsies: definitive histology, usually safe
although rare case reports of milk duct fistula in
pregnant or lactating women.
Obtain ER, PR and HER 2/neu status of tumor
NCCN Practice Guideline Invasive Breast Cancer V.3. 2013; Hahn
KME et al. Cancer 2006;107:1219; Schackmuth EM. Am J
Roentgenol 1993;161:961
Pathologic Features of Breast Cancer
Diagnosed During Pregnancy
Case series and case-control studies of pregnant
women with breast cancer:
Majority of tumors ER and PR negative
HER-2/neu expression: ranges from 29% to 58%
for HER-2/neu over-expression or amplification
Most commonly cancers are:
Invasive ductal carcinoma
Poorly differentiated
Diagnosed at more advanced stages (node positive)
Tobon H, Horowitz LF. Breast Dis 1993;6:127; Ishida T et al. Jpn J Cancer Res
1992;83:1143; Middleton L et al. Cancer 2003; 98:1055; Hahn KME et al.
Cancer 2006;107:1219; Ring AE et al. J Clin Oncol 2005;23:4192, Elledge R et
al. Cancer 1993;71:2499; Azim HA Jr et al. Acta Oncol 2012;51:653; Amant F et
al. J Clin Oncol 2013;31:2532
Treatment of Breast Cancer During
Pregnancy: Termination of Pregnancy
Termination of pregnancy does not improve survival in most case-control studies.
The decision to continue or terminate the pregnancy must be made by a woman who has been fully informed of the evidence with regard to pregnancy termination.
Reasons to consider termination of pregnancy: Known or suspected fetal teratogenesis
Health of the mother
Chervenak FA et al. Cancer 2004; 100:215; Oduncu FS et al. J Cancer Res Clin
Oncol 2003:129:133; Holleb AI, Farros JF. Surg Gynecol Obstet 1962;115:65;
Nugent P, O’Connel TX. Arch Surg 1985;120:1221; Clark RM, Chua T. Clin
Oncol 1989;1:11; Deemarsky LJ, Beishtadt EL. Breast 1981;7:17
Surgery in the Pregnant Patient Possibly an increased rate of spontaneous abortions with
general anesthesia:
primarily those having obstetric or gynecologic procedures
Possibly an increase in low and very low birth weight infants as well as IUGR
thought to be secondary to the underlying problem that resulted in surgery.
Mastectomy with ALND can be performed with minimal risk to the developing fetus or the continuation of pregnancy
Duncan PG et al. Anesthesiology 1986;64:790, Mazze RI, Kallen B. Am J Obstet Gynecol
1989;161:1178
Breast Conserving Surgery in the
Pregnant Woman with Breast Cancer
Radiation therapy required to complete breast
conservation:
Radiation exposure to the fetus increases as
pregnancy proceeds secondary to greater
proximity of the fetus to the radiation field (breast or
chest wall).
Usually delayed until after delivery.
Kuerer HM et al. Surgery 2002;131:108; Annane K et al. Fetal Diagn.Ther.
2005;20:442.
Sentinel Lymph Node Biopsy in the
Pregnant Woman with Breast Cancer
Technetium-99m: fetal radiation exposure estimated to be below the 5 cGy limit recommended by the National Commission on Radiation Protection
Isosulfan blue dye:
Pregnancy Category C: animal reproduction studies have not been conducted
should be given to a pregnant woman only if clearly needed. Although recent data from the Mayo Clinic suggests low level of fetal exposure.
risk of anaphylaxis
Morita ET et al. Surg Clin North Am 2000;80:1721; Keleher A et al. Breast J.
2004;10:492; Keleher A et al. J Am Coll Surg 2001;194:54; Pruthi S et al. Am J Surg
2011;201:70
Pregnant Breast Cancer Patients:
MDACC Surgery Experience
Of 67 pregnant breast cancer patients:
30 had preoperative chemotherapy: 10 had breast
conserving surgery (BCS) and 20 had mastectomy
37 had surgery first: 9 had BCS and 28 had
mastectomy
No difference in surgical complications between
mastectomy and lumpectomy patients
No significant complications from core biopsies
Dominici LS et al. Breast Diseases 2010; 31:1
Systemic Therapy in the Pregnant
Breast Cancer Patient Retrospective case series: often non-uniform
treatments
Anthracyline-based therapies have the most supporting evidence regarding safety:
AC, FAC, FEC when given in 2nd and 3rd trimesters
Limited dose-dense anthracycline safety and tolerance data
Dosing: should we use actual body weight versus ideal body weight?
www.fda.gov
Supportive Care Medications in Pregnant
Breast Cancer Patients (FDA category)
Antiemetics:
MDACC approach routinely uses dexamethasone (C)
and ondansetron (B).
promethazine and prochlorperazine (C)
Filgrastim has been given to pregnant patients with
chronic severe neutropenia (C).
Few published reports of using pegfilgrastim in pregnant
breast cancer patients (C).
Sangalli MR et al. Aust NZ J Obstet Gynaecol 2001;41:470; Cardonick E et al.
Ann Oncol 2012;23:3016
Treatment of the Pregnant Breast
Cancer Patient: Systemic Therapy
1st Trimester (139 cases): 17% fetal malformation
2nd and 3rd trimester (150 cases): 1.3 – 3.8% fetal
malformation
Similar to the rate than in the general population.
Doll DC et al. Semin Oncol 1989;16:337.
Chemotherapeutic Treatment of Pregnant
Breast Cancer Patients (MDACC) After the 1st trimester: adjuvant or neoadjuvant FAC every 21
days:
5-fluorouracil: 500 mg/m2 IV on days 1 and 4
Doxorubicin: 50 mg/m2 IV continuous infusion over 72h
Cyclophosphamide: 500 mg/m2 IV on day 1 only
No chemotherapy after 35 weeks gestation
Additional systemic therapies if appropriate:
- Paclitaxel or docetaxel postpartum.
- Trastuzumab postpartum.
- Tamoxifen postpartum. Hahn KM et al. Cancer 2006;107:1219.
Non-anthracycline Based Therapies in
Pregnant Breast Cancer Patients
Methotrexate contraindicated
Docetaxel and paclitaxel: multiple case reports in breast and gynecologic cancers
Trastuzumab: oligohydraminios- FDA pregnancy category D.
Lapatinib: FDA pregnancy category D
Tamoxifen: FDA pregnancy category D- case reports of fetal malformations
De Santis M et al. Eur J Cancer Care 2000;9:235; Zagouri F et al. Clin Breast
Cancer 2013;13:16; Gonzalez-Angulo AM et al. Clin Breast Cancer 2004;5:317;
Watson WJ. Obstet Gynecol 2005;105:642; Waterston AM, J Clin Oncol
2006;21:321; Fanale MA et al. Clin Br Cancer 2005;6:354
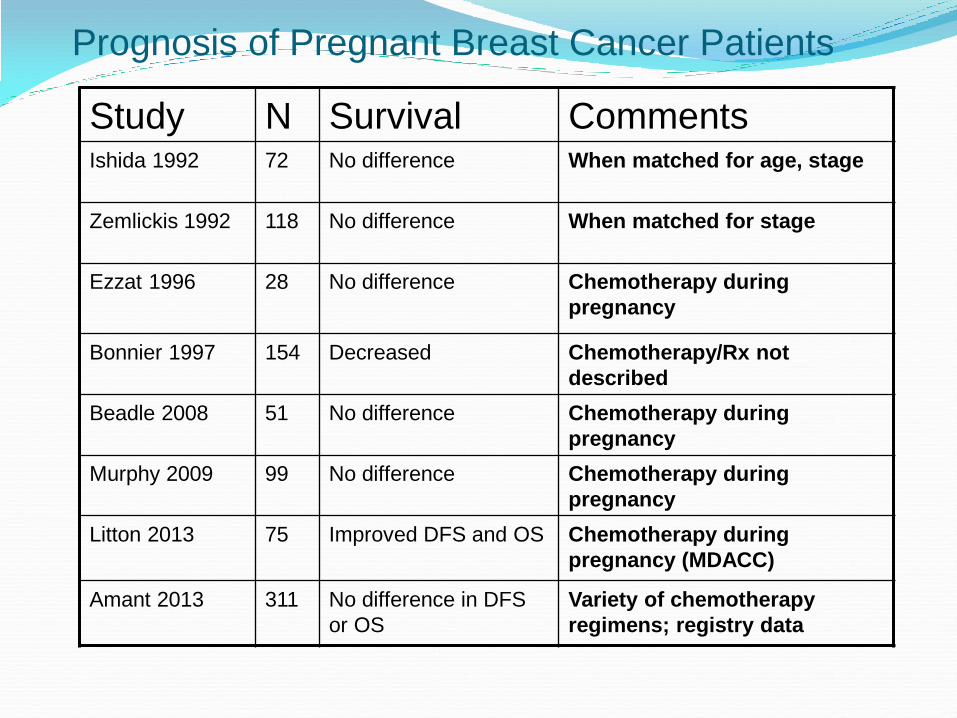
Prognosis of Pregnant Breast Cancer Patients
Study N Survival Comments Ishida 1992 72 No difference When matched for age, stage
Zemlickis 1992 118 No difference When matched for stage
Ezzat 1996 28 No difference Chemotherapy during
pregnancy
Bonnier 1997 154 Decreased Chemotherapy/Rx not
described
Beadle 2008 51 No difference Chemotherapy during
pregnancy
Murphy 2009 99 No difference Chemotherapy during
pregnancy
Litton 2013 75 Improved DFS and OS Chemotherapy during
pregnancy (MDACC)
Amant 2013 311 No difference in DFS
or OS
Variety of chemotherapy
regimens; registry data
Breast Cancer During Pregnancy:
Labor and Delivery Results
Some studies have shown low birth weight and
earlier deliveries
More recent series have allowed women to go
closer to term if possible
MDACC cohort had higher number of vaginal births
than C-sections with similar neonatal outcomes
Paucity of long term outcome data in children
Loibl S et al. Lancet Oncol 2012;13:887; Ebert U et al. Pharmacol
Ther 1997;74:207, Zemlickis D et al. Am J Obstet Gynecol
1992;166:781
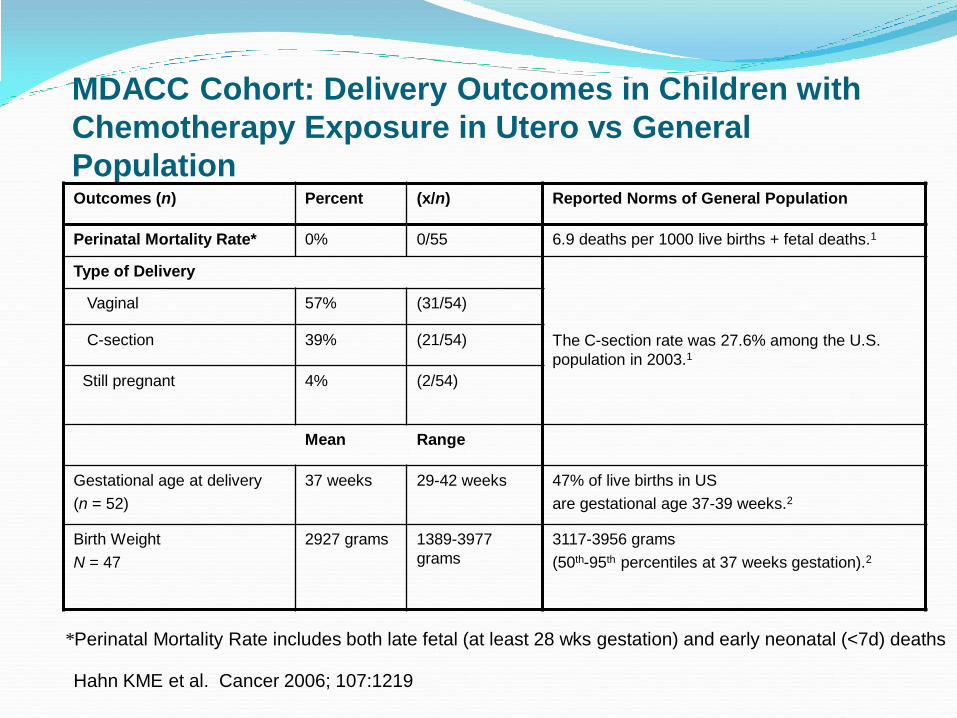
MDACC Cohort: Delivery Outcomes in Children with
Chemotherapy Exposure in Utero vs General
Population Outcomes (n) Percent (x/n) Reported Norms of General Population
Perinatal Mortality Rate* 0% 0/55 6.9 deaths per 1000 live births + fetal deaths.1
Type of Delivery
The C-section rate was 27.6% among the U.S.
population in 2003.1
Vaginal 57% (31/54)
C-section 39% (21/54)
Still pregnant
4% (2/54)
Mean Range
Gestational age at delivery
(n = 52)
37 weeks 29-42 weeks
47% of live births in US
are gestational age 37-39 weeks.2
Birth Weight
N = 47
2927 grams 1389-3977
grams
3117-3956 grams
(50th-95th percentiles at 37 weeks gestation).2
*Perinatal Mortality Rate includes both late fetal (at least 28 wks gestation) and early neonatal (<7d) deaths
Hahn KME et al. Cancer 2006; 107:1219
References for Preceding Tables 1. Martin, JA et al. Annual Summary of Vital Statistics– 2003.
Pediatrics 2005;115:619-34.
2. Cunningham FG et al. Williams Obstetrics 21st Ed, McGraw-Hill, 2001.
3. Agrawal V et al. Classification of acute respiratory disorders of all newborns in a tertiary care center. J. Natl Med Assoc 2003;95:585-95
4. Wen SW et al. Comparison of Maternal and Infant Outcomes between Vacuum Extraction and Forceps Deliveries. 2001;153:103-7
5. Moore KL, Persaud TVN. The Developing Human. Clinically Oriented Embryology. 7th Ed, Saunders 2003
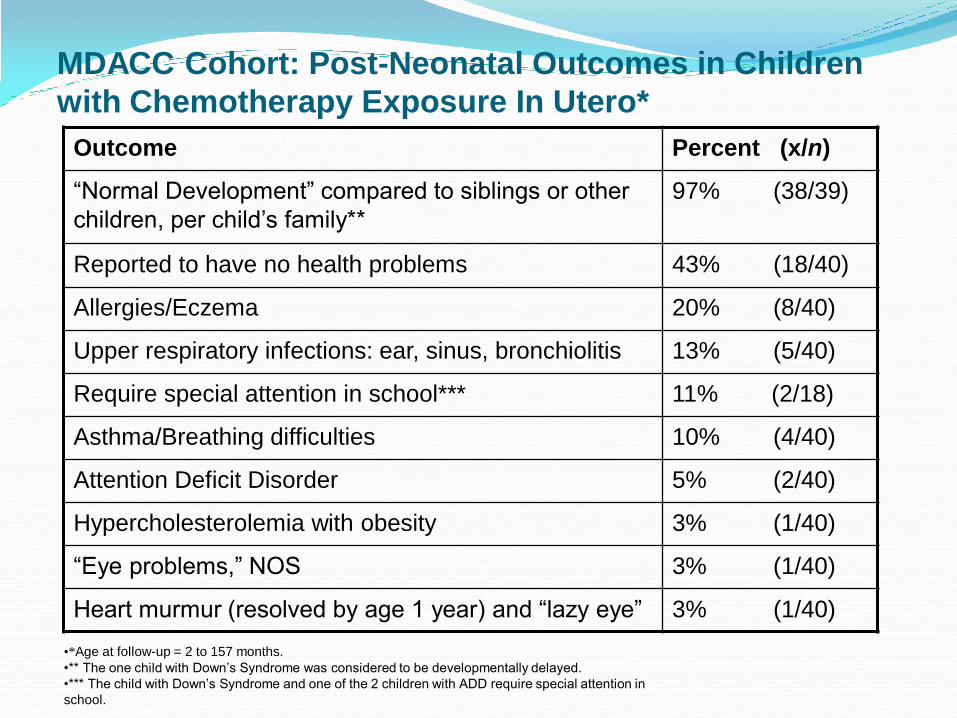
MDACC Cohort: Post-Neonatal Outcomes in Children
with Chemotherapy Exposure In Utero*
Outcome Percent (x/n)
“Normal Development” compared to siblings or other
children, per child’s family**
97% (38/39)
Reported to have no health problems 43% (18/40)
Allergies/Eczema 20% (8/40)
Upper respiratory infections: ear, sinus, bronchiolitis 13% (5/40)
Require special attention in school*** 11% (2/18)
Asthma/Breathing difficulties 10% (4/40)
Attention Deficit Disorder 5% (2/40)
Hypercholesterolemia with obesity 3% (1/40)
“Eye problems,” NOS 3% (1/40)
Heart murmur (resolved by age 1 year) and “lazy eye” 3% (1/40)
•*Age at follow-up = 2 to 157 months.
•** The one child with Down’s Syndrome was considered to be developmentally delayed.
•*** The child with Down’s Syndrome and one of the 2 children with ADD require special attention in
school.
Observational Study: Breast Cancer
Diagnosed and Treated During Pregnancy
Registry for breast cancer patients diagnosed during
pregnancy: 7 European countries
Of the 447 patients with early breast cancer
registered from April, 2003 to December 2011, 413
were treated with chemotherapy while pregnant.
Birthweight was lower for those exposed to
chemotherapy in utero despite gestational age.
No statistical difference in premature deliveries or
malformations or newborn complications
Loibl S et al. Lancet Oncol 2012;13:887
Conclusions: Breast Cancer
Diagnosed During Pregnancy Women diagnosed during pregnancy can be
considered for surgery at any time and chemotherapy after the first trimester
Anthracycline-based chemotherapy regimens have the most safety data to date, however, other agents such as docetaxel and paclitaxel have been described
Radiation, tamoxifen and trastuzumab should be administered after delivery
Further long term follow up of the children exposed to chemotherapy in utero is warranted
Pregnancy After a Diagnosis
of Breast Cancer
Pregnancy Following Breast
Cancer Treatment
Studies:
Often retrospective, cohort or case-control
Overall pregnancy after breast cancer treatment
does not appear to have worse prognosis
Some studies even show better prognosis:
“Healthy Mother” effect
Risk of recurrence does not appear to be
influenced by hormone receptor status of the
tumor.
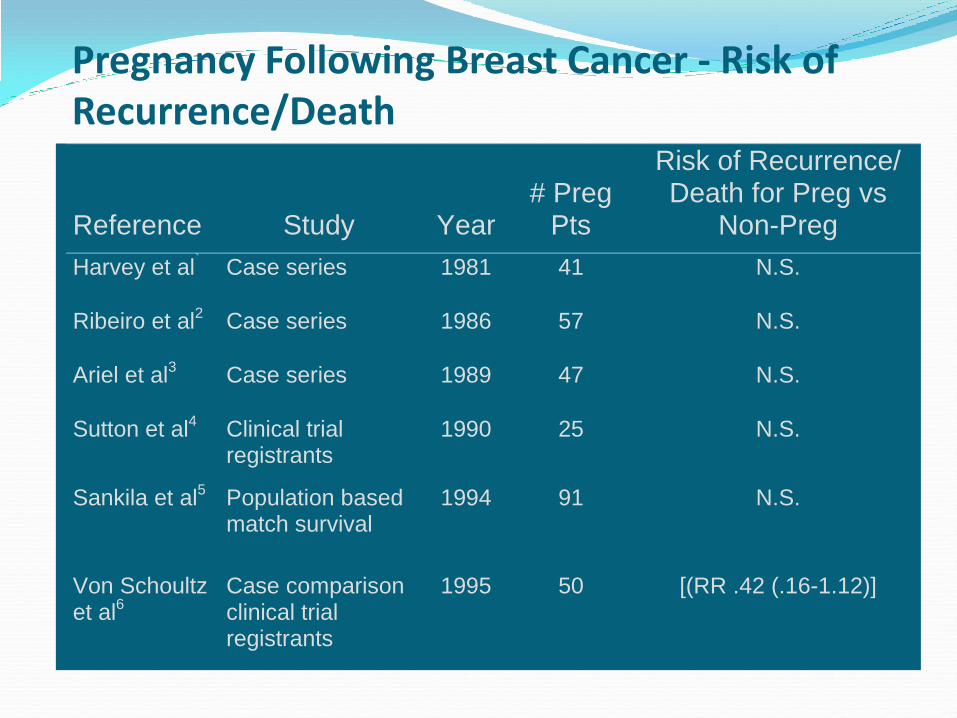
Pregnancy Following Breast Cancer - Risk of Recurrence/Death Reference
Study
Year
# Preg
Pts
Risk of Recurrence/ Death for Preg vs
Non-Preg
Harvey et al`
Case series 1981 41 N.S.
Ribeiro et al2
Case series 1986 57 N.S.
Ariel et al3
Case series 1989 47 N.S.
Sutton et al4
Clinical trial registrants
1990 25 N.S.
Sankila et al5
Population based match survival
1994 91 N.S.
Von Schoultz et al
6 Case comparison clinical trial registrants
1995 50 [(RR .42 (.16-1.12)]
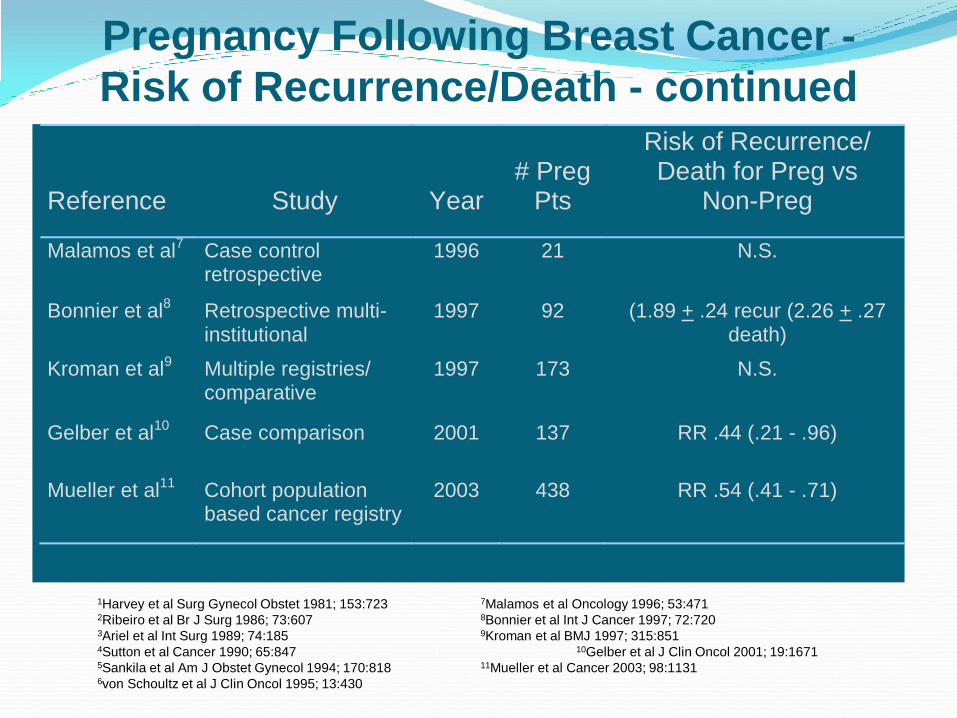
Pregnancy Following Breast Cancer -
Risk of Recurrence/Death - continued Reference
Study
Year
# Preg
Pts
Risk of Recurrence/ Death for Preg vs
Non-Preg
Malamos et al7
Case control retrospective
1996 21 N.S.
Bonnier et al8
Retrospective multi-institutional
1997 92 (1.89 + .24 recur (2.26 + .27 death)
Kroman et al9
Multiple registries/ comparative
1997 173 N.S.
Gelber et al10
Case comparison 2001 137 RR .44 (.21 - .96)
Mueller et al11
Cohort population based cancer registry
2003 438 RR .54 (.41 - .71)
1Harvey et al Surg Gynecol Obstet 1981; 153:723 7Malamos et al Oncology 1996; 53:471 2Ribeiro et al Br J Surg 1986; 73:607 8Bonnier et al Int J Cancer 1997; 72:720 3Ariel et al Int Surg 1989; 74:185 9Kroman et al BMJ 1997; 315:851 4Sutton et al Cancer 1990; 65:847 10Gelber et al J Clin Oncol 2001; 19:1671 5Sankila et al Am J Obstet Gynecol 1994; 170:818 11Mueller et al Cancer 2003; 98:1131 6von Schoultz et al J Clin Oncol 1995; 13:430
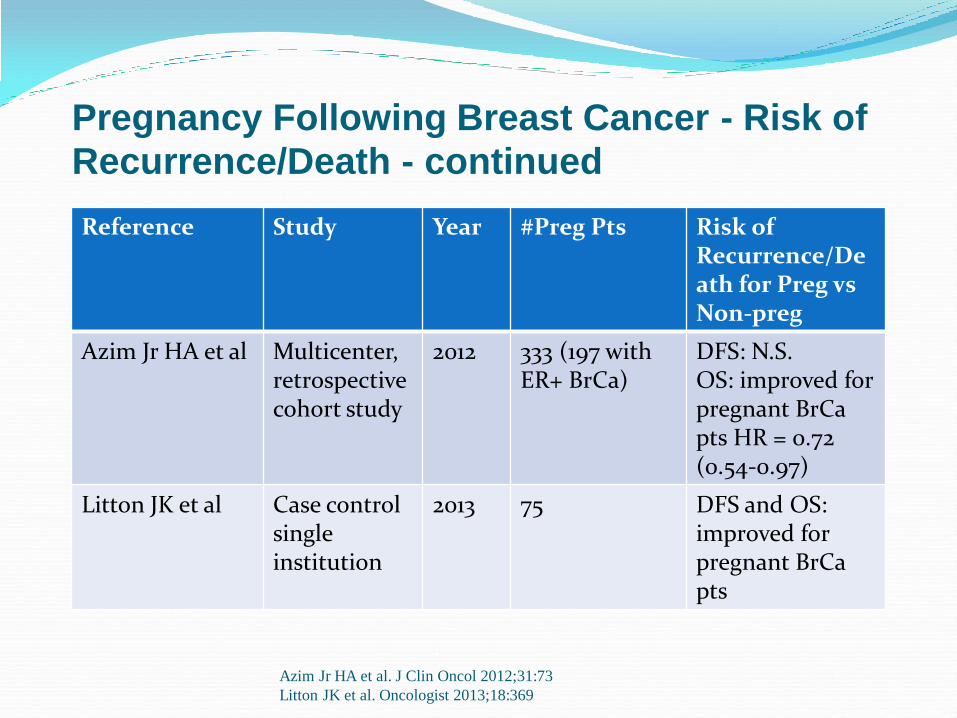
Pregnancy Following Breast Cancer - Risk of
Recurrence/Death - continued
Reference Study Year #Preg Pts Risk of Recurrence/Death for Preg vs Non-preg
Azim Jr HA et al Multicenter, retrospective cohort study
2012 333 (197 with ER+ BrCa)
DFS: N.S. OS: improved for pregnant BrCa pts HR = 0.72 (0.54-0.97)
Litton JK et al Case control single institution
2013 75 DFS and OS: improved for pregnant BrCa pts
Azim Jr HA et al. J Clin Oncol 2012;31:73
Litton JK et al. Oncologist 2013;18:369
Impact of Pregnancy on Breast Cancer Survival in
Women who Carry a BRCA1 or BRCA2 Mutation
From an international multicenter cohort study of 12,084
women with one of these mutations, 128 case subjects
were diagnosed with breast cancer during pregnancy or
became pregnant after a diagnosis of breast cancer.
Age-matched to 269 mutation carriers who did not
become pregnant (controls).
The 15-year survival rate was 91.5% among the cases
and 88.6% among the controls (adjusted HR 0.76; 95%
CI 0.31-1.91, p = 0.56)
Valentini A, et al. Breast Cancer Res Treat 2013, Oct
18;142:177
Meta-analyses on Safety of Pregnancy After Breast
Cancer Diagnosis Valachis A et al.(Obstet Gynecol Surv 2010;65:786)
Assessed the effect of pregnancy at least 10 months from diagnosis on overall survival (OS) among premenopausal breast cancer patients < 45 yoa
Of the 9 studies met the inclusion criteria and had data appropriate for analysis, OS was statistically better among BrCa survivors who became pregnant compared to controls: HR for death 0.51 (95% CI: 0.42-0.62)
Luo M et al. (Int J Gynecol Cancer 2014;24:1366) Of the 5 studies analyzed, women who had undergone
surgery for breast cancer and subsequently became pregnant had a better OS than those who did not (PRR 0.78; 95% CI 0.64-0.95)
Recommendations to Women Considering
Pregnancy After a Diagnosis of Breast Cancer
Women with larger tumors and/or positive lymph
nodes have a higher risk of breast cancer
recurrence
Some physicians have recommended waiting 2
years after diagnosis perhaps because the more
aggressive cancers have tended to recur more
quickly.
Women with a history of breast cancer must be
aware of their own estimated risk of recurrence.
Amenorrhea Among Breast Cancer
Patients Only 5% of women < 45 years of age have
undergone natural menopause
Average age of menopause in US: 50-52 yrs
SEER 2006-2010: Percentage of cases of breast
cancer:< 20 yrs: 0%; 20-34 yrs: 1.8%; 35-44 yrs:
9.6%
Chemotherapy-related amenorrhea (CRA): varies in definition- anywhere from 3 to 12 months without a menstrual period
http://seer.cancer.gov
CRA Among Breast Cancer Patients J. Bines et al (J Clin Oncol 1996;14:1718)
summarized the data available at that time:
< 40 years of age: 21-71%*
> 40 years of age: 49-100%*
* Depended upon regimen and duration of therapy
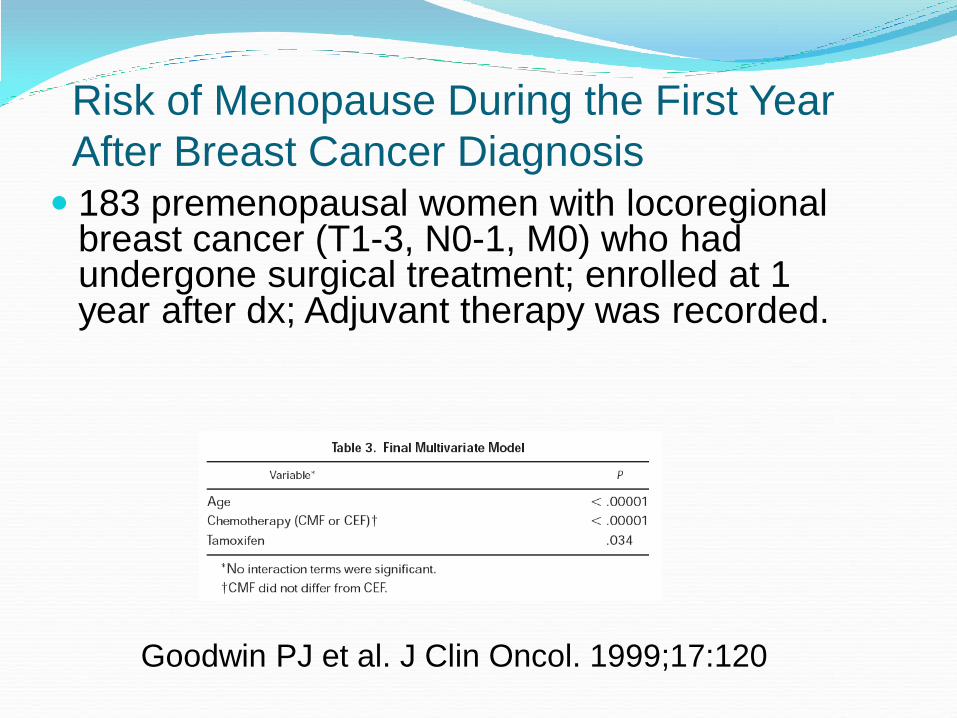
Risk of Menopause During the First Year
After Breast Cancer Diagnosis 183 premenopausal women with locoregional
breast cancer (T1-3, N0-1, M0) who had undergone surgical treatment; enrolled at 1 year after dx; Adjuvant therapy was recorded.
Goodwin PJ et al. J Clin Oncol. 1999;17:120
Effects of Paclitaxel, Dose Density, and Trastuzumab on Treatment-related Amenorrhea in Premenopausal Women with Breast Cancer
Retrospective review of 431 premenopausal
women with early breast cancer treated at DFCI
and MGH from 1997-2005.
Premenopausal: menses in the 6 months prior to
first visit
Postmenopausal: no menses in the 6 months
prior to first visit (natural, surgical, medical,
pharmacologic or radiation-induced)
Type of chemo and use of tamoxifen recorded
Abusief ME et al. Cancer 2010;116:791
Chemotherapy Regimens Included in this
Retrospective Review
1) AC x 4 cycles
2) AC x 4 cycles followed by paclitaxel 175 mg/m2 x 4
cycles (AC-T)
3) AC followed or preceded by:
a) weekly paclitaxel with weekly trastuzumab x 12 doses,
then trastuzumab up to 52 weeks total
b) weekly paclitaxel x 12 doses, then trastuzumab for up to
52 weeks.
(AC-T + trastuzumab)
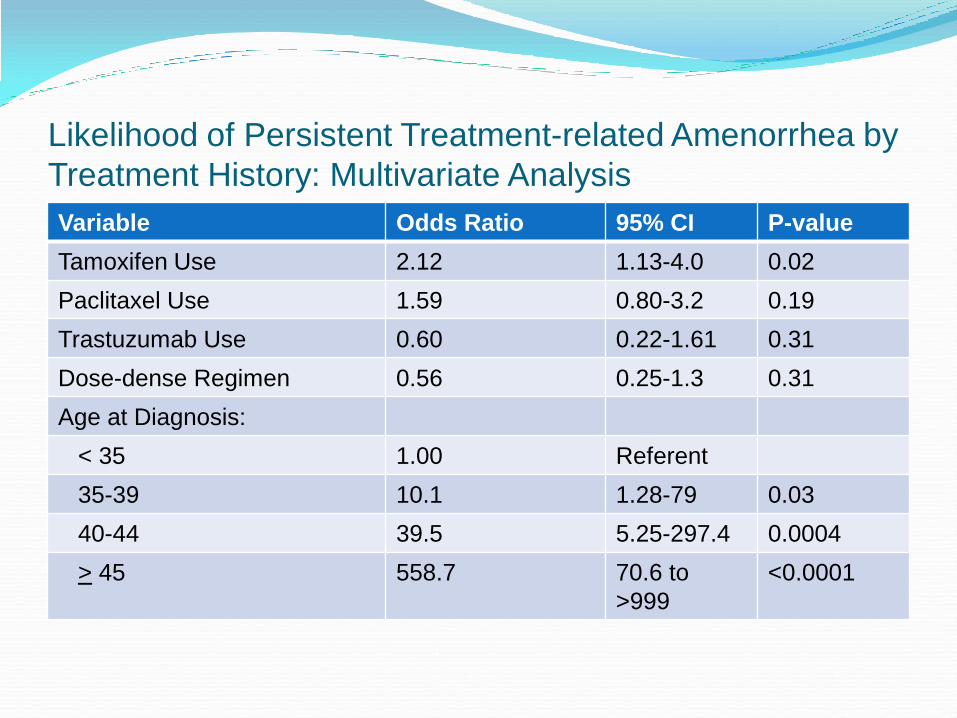
Likelihood of Persistent Treatment-related Amenorrhea by
Treatment History: Multivariate Analysis
Variable Odds Ratio 95% CI P-value
Tamoxifen Use 2.12 1.13-4.0 0.02
Paclitaxel Use 1.59 0.80-3.2 0.19
Trastuzumab Use 0.60 0.22-1.61 0.31
Dose-dense Regimen 0.56 0.25-1.3 0.31
Age at Diagnosis:
< 35 1.00 Referent
35-39 10.1 1.28-79 0.03
40-44 39.5 5.25-297.4 0.0004
> 45 558.7 70.6 to
>999
<0.0001
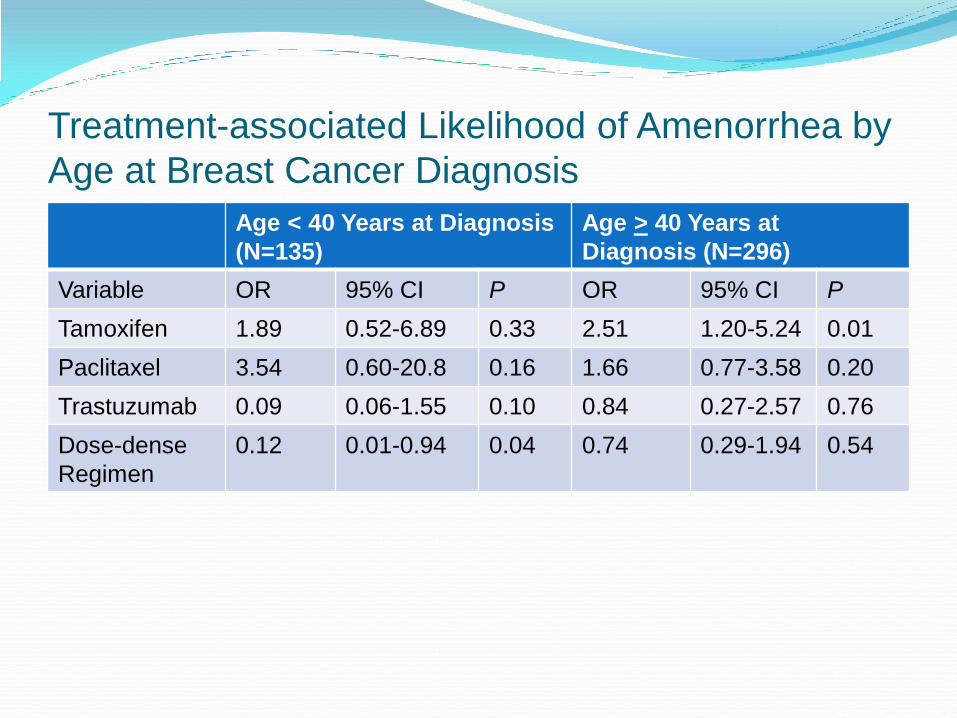
Treatment-associated Likelihood of Amenorrhea by
Age at Breast Cancer Diagnosis
Age < 40 Years at Diagnosis
(N=135)
Age > 40 Years at
Diagnosis (N=296)
Variable OR 95% CI P OR 95% CI P
Tamoxifen 1.89 0.52-6.89 0.33 2.51 1.20-5.24 0.01
Paclitaxel 3.54 0.60-20.8 0.16 1.66 0.77-3.58 0.20
Trastuzumab 0.09 0.06-1.55 0.10 0.84 0.27-2.57 0.76
Dose-dense
Regimen
0.12 0.01-0.94 0.04 0.74 0.29-1.94 0.54
ASCO Guideline Update 2013
Loren AW, et al.
www.asco.org
Key Recommendations Discuss fertility preservation with all patients of
reproductive age if infertility is a potential risk of therapy.
Refer patients who express an interest in fertility preservation (and patients who are ambivalent) to reproductive specialists.
Address fertility preservation as early as possible, before treatment starts.
Document fertility preservation discussions in the medical record.
Key Recommendations Answer basic questions about whether fertility
preservation may have an impact upon successful cancer treatment.
Refer patients to psychosocial providers if they experience distress about potential infertility.
Encourage patients to participate in registries and clinical trials.
Key Recommendations: Adult Females (non-gynecologic malignancies)
Present both embryo and oocyte cryopreservation as established fertility preservation methods.
Inform patients that there is insufficient evidence regarding the effectiveness of ovarian suppression (gonadotropin-releasing hormone analogs) as a fertility preservation method, and these agents should not be relied on to preserve fertility.
Inform patients that other methods (eg. Ovarian tissue cryopreservation, which does not require sexual maturity, for the purpose of future transplantation ) are still experimental.
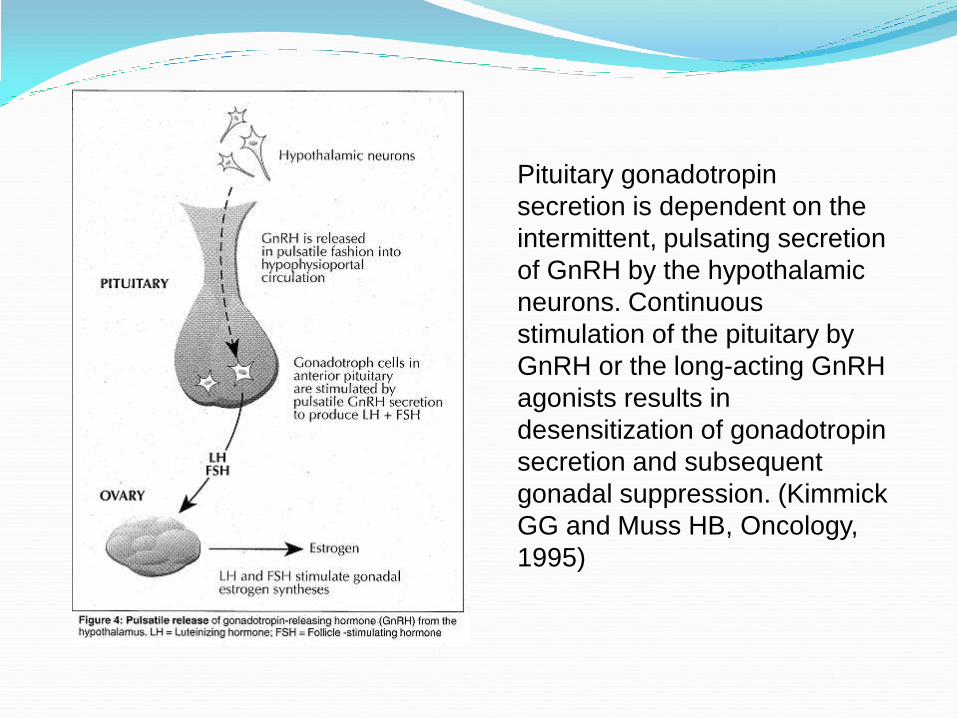
Pituitary gonadotropin
secretion is dependent on the
intermittent, pulsating secretion
of GnRH by the hypothalamic
neurons. Continuous
stimulation of the pituitary by
GnRH or the long-acting GnRH
agonists results in
desensitization of gonadotropin
secretion and subsequent
gonadal suppression. (Kimmick
GG and Muss HB, Oncology,
1995)
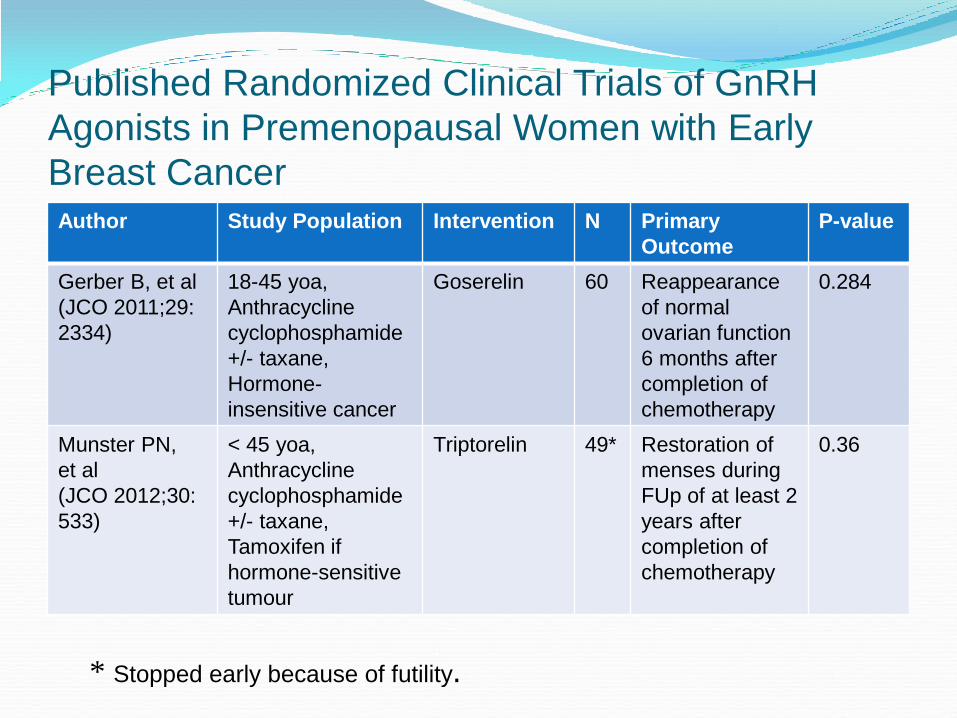
Published Randomized Clinical Trials of GnRH
Agonists in Premenopausal Women with Early
Breast Cancer Author Study Population Intervention N Primary
Outcome
P-value
Gerber B, et al
(JCO 2011;29:
2334)
18-45 yoa,
Anthracycline
cyclophosphamide
+/- taxane,
Hormone-
insensitive cancer
Goserelin 60 Reappearance
of normal
ovarian function
6 months after
completion of
chemotherapy
0.284
Munster PN,
et al
(JCO 2012;30:
533)
< 45 yoa,
Anthracycline
cyclophosphamide
+/- taxane,
Tamoxifen if
hormone-sensitive
tumour
Triptorelin 49* Restoration of
menses during
FUp of at least 2
years after
completion of
chemotherapy
0.36
* Stopped early because of futility.
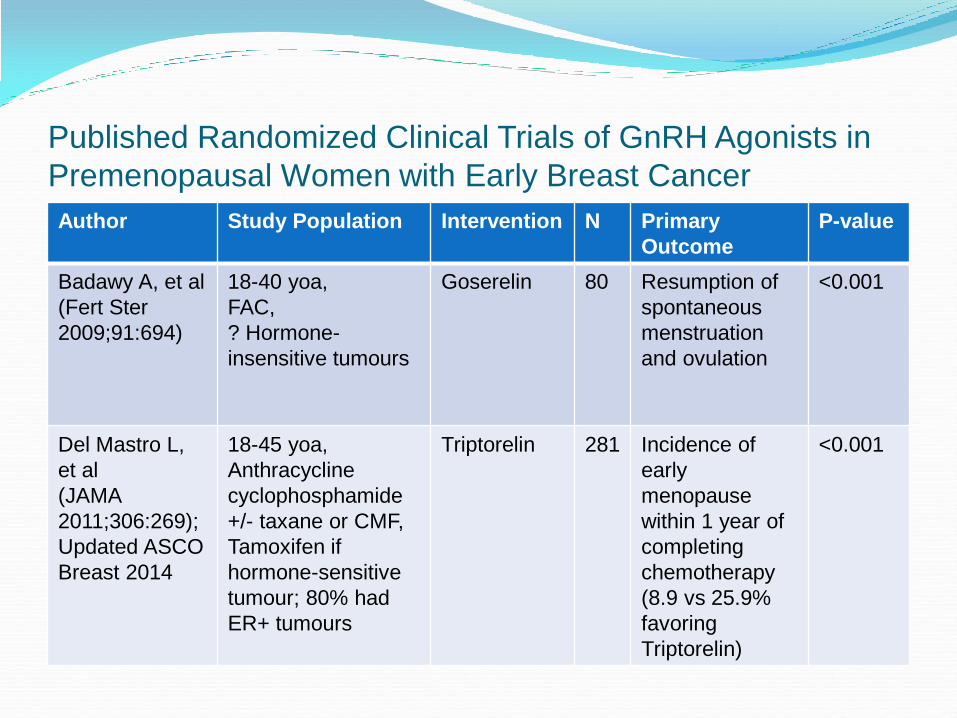
Published Randomized Clinical Trials of GnRH Agonists in
Premenopausal Women with Early Breast Cancer
Author Study Population Intervention N Primary
Outcome
P-value
Badawy A, et al
(Fert Ster
2009;91:694)
18-40 yoa,
FAC,
? Hormone-
insensitive tumours
Goserelin 80 Resumption of
spontaneous
menstruation
and ovulation
<0.001
Del Mastro L,
et al
(JAMA
2011;306:269);
Updated ASCO
Breast 2014
18-45 yoa,
Anthracycline
cyclophosphamide
+/- taxane or CMF,
Tamoxifen if
hormone-sensitive
tumour; 80% had
ER+ tumours
Triptorelin
281 Incidence of
early
menopause
within 1 year of
completing
chemotherapy
(8.9 vs 25.9%
favoring
Triptorelin)
<0.001
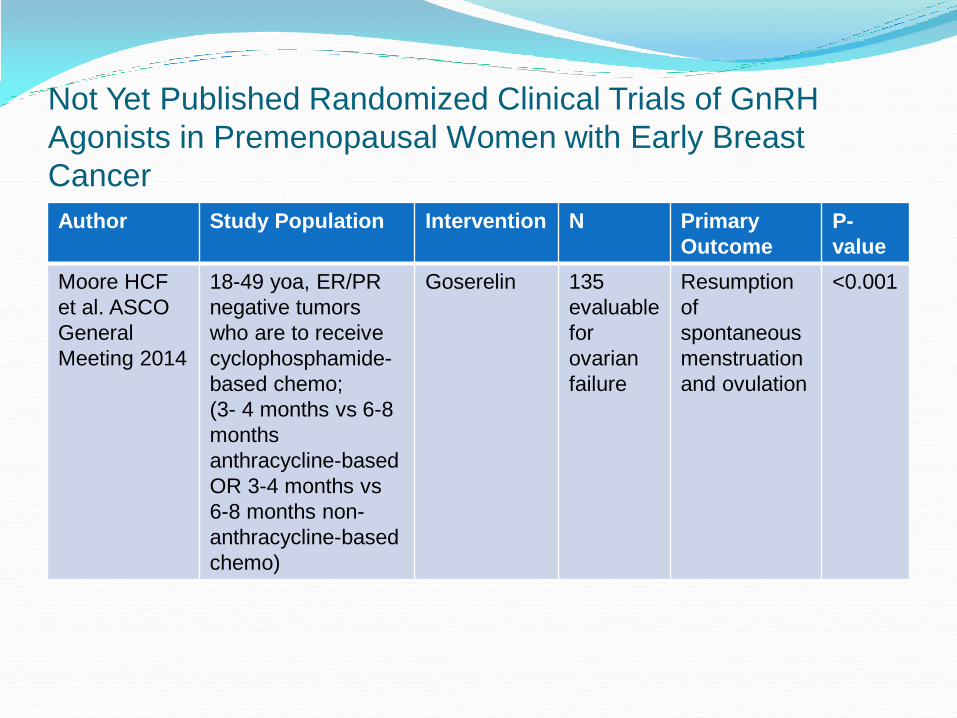
Not Yet Published Randomized Clinical Trials of GnRH
Agonists in Premenopausal Women with Early Breast
Cancer
Author Study Population Intervention N Primary
Outcome
P-
value
Moore HCF
et al. ASCO
General
Meeting 2014
18-49 yoa, ER/PR
negative tumors
who are to receive
cyclophosphamide-
based chemo;
(3- 4 months vs 6-8
months
anthracycline-based
OR 3-4 months vs
6-8 months non-
anthracycline-based
chemo)
Goserelin 135
evaluable
for
ovarian
failure
Resumption
of
spontaneous
menstruation
and ovulation
<0.001
Prevention of Early Menopause Study<br />(POEMS)-S0230<br /> Phase III trial of LHRH analog during chemotherapy to reduce ovarian failure in early stage, hormone receptor-
negative breast cancer: an international Intergroup trial of SWOG, IBCSG, ECOG, and CALGB (Alliance)
Presented By Halle Moore at 2014 ASCO Annual Meeting
Published Randomized Clinical Trials of GnRH Agonists in
Premenopausal Women with Early Breast Cancer
Author Study
Population
Intervention N Primary
Outcome
P-value
Badawy A, et al
(Fert Ster
2009;91:694)
18-40 yoa,
FAC,
? Hormone-
insensitive
tumours
Goserelin 80 Resumption of
spontaneous
menstruation
and ovulation
<0.001
Del Mastro L,
et al
(JAMA
2011;306:269)
18-45 yoa,
Anthracycline
cyclophosphamid
e +/- taxane or
CMF, Tamoxifen if
hormone-
sensitive tumour
Triptorelin 281 Incidence of
early
menopause
within 1 year of
completing
chemotherapy
<0.001
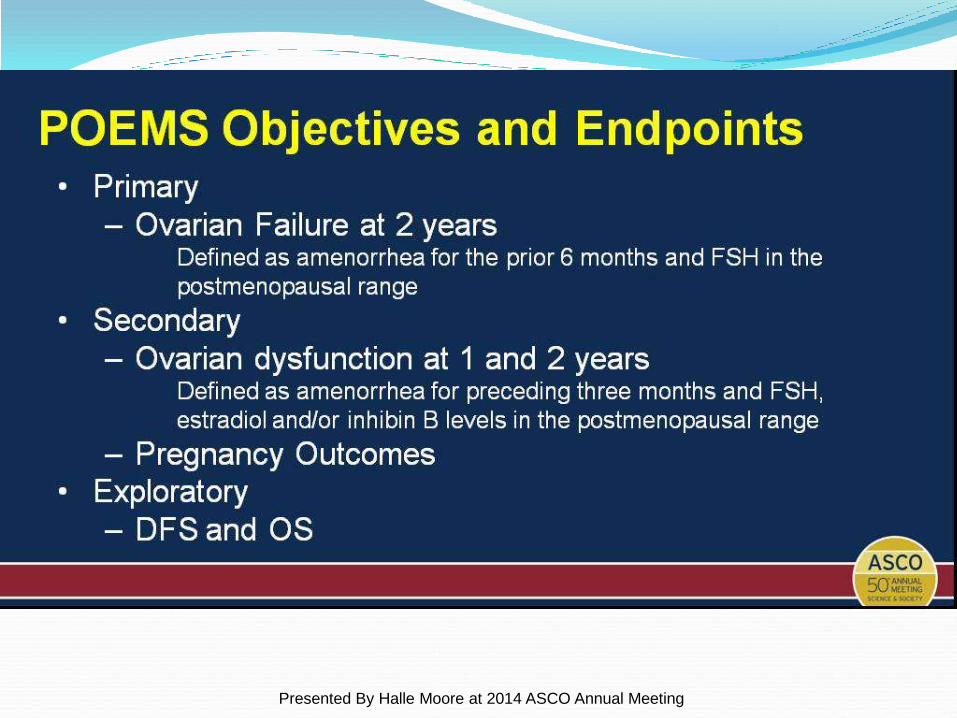
POEMS Objectives and Endpoints
Presented By Halle Moore at 2014 ASCO Annual Meeting
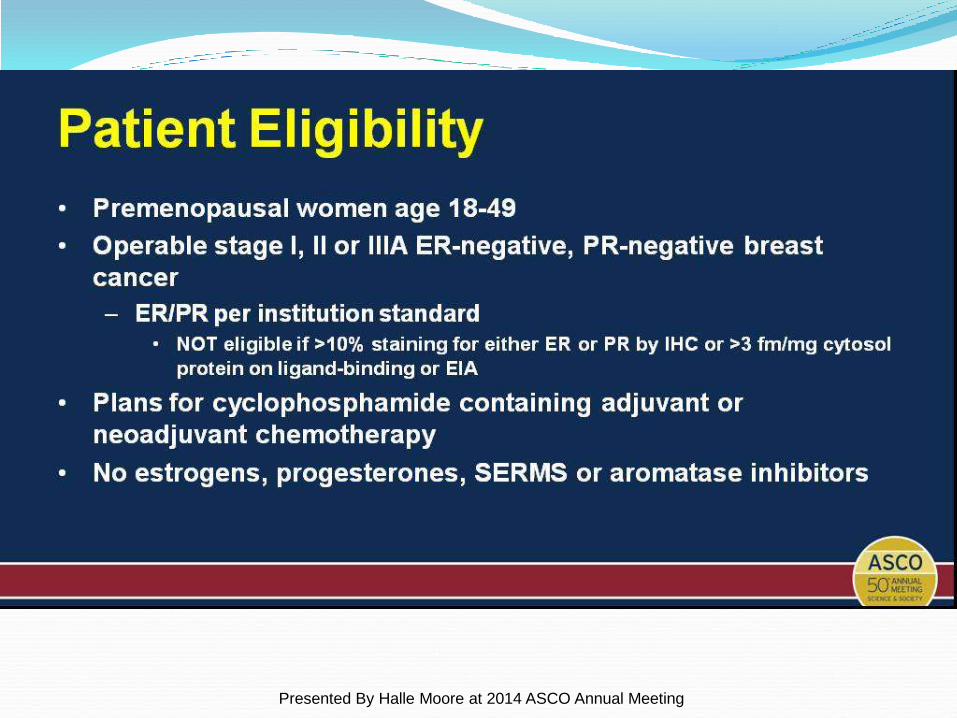
Patient Eligibility
Presented By Halle Moore at 2014 ASCO Annual Meeting
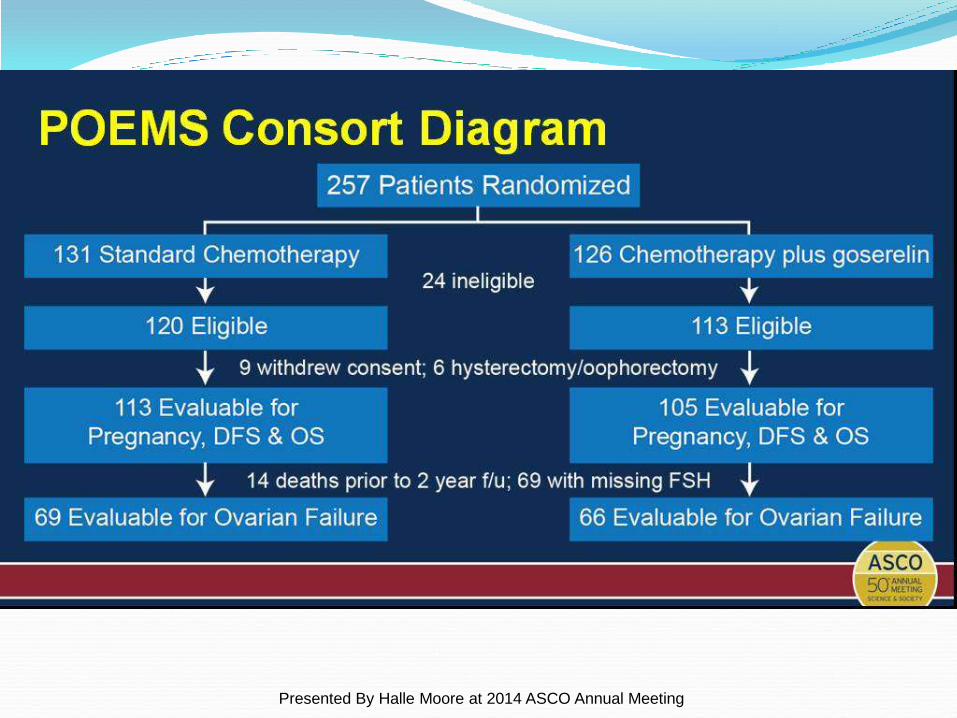
POEMS Consort Diagram
Presented By Halle Moore at 2014 ASCO Annual Meeting
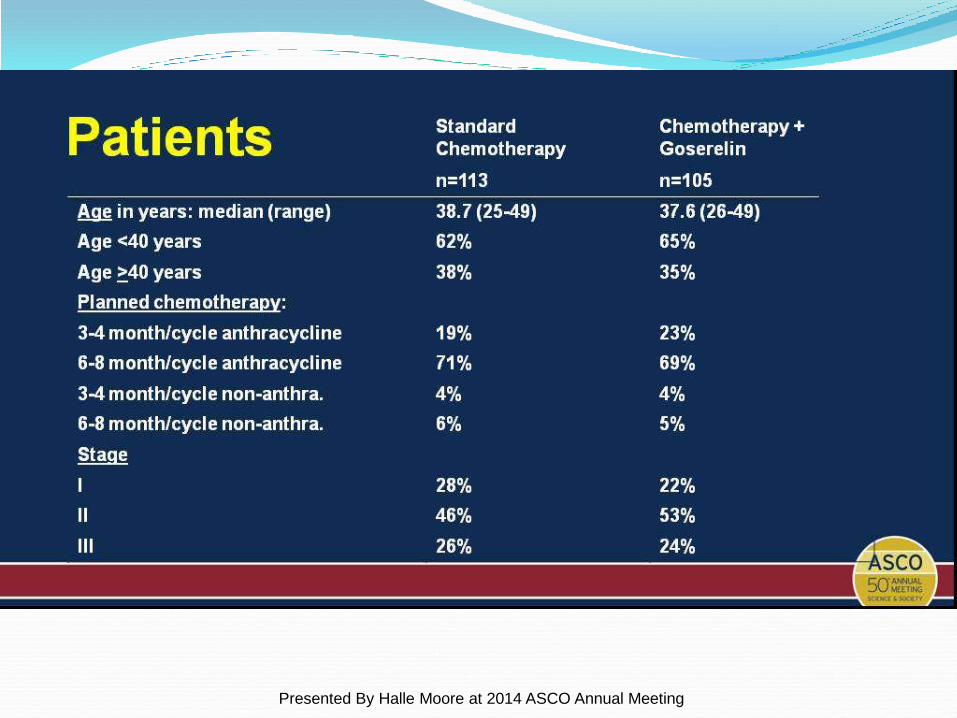
Patients
Presented By Halle Moore at 2014 ASCO Annual Meeting
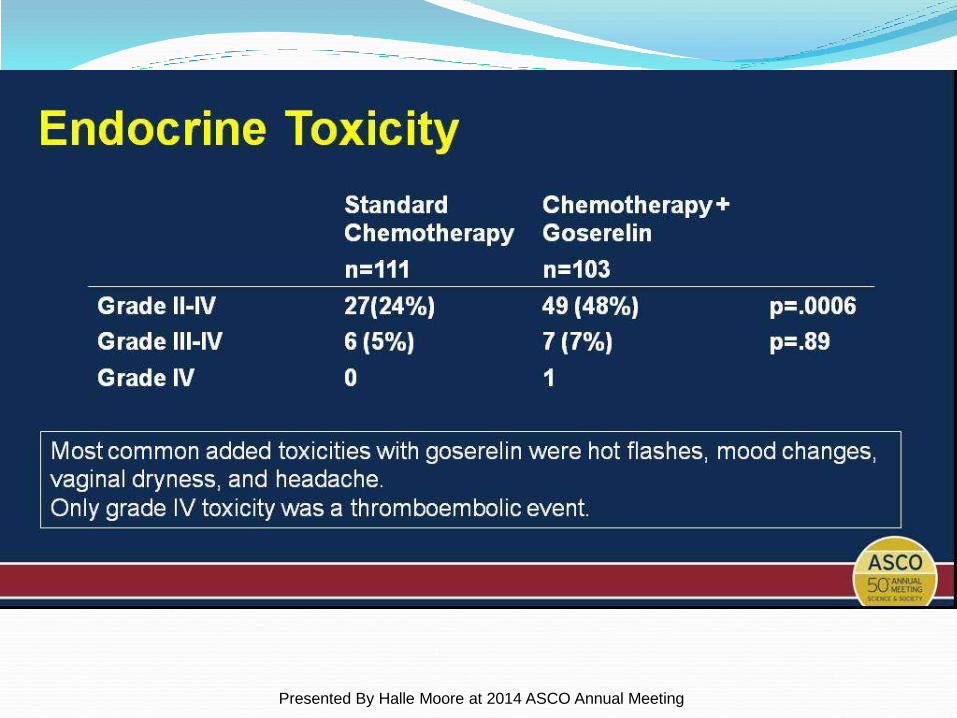
Endocrine Toxicity
Presented By Halle Moore at 2014 ASCO Annual Meeting
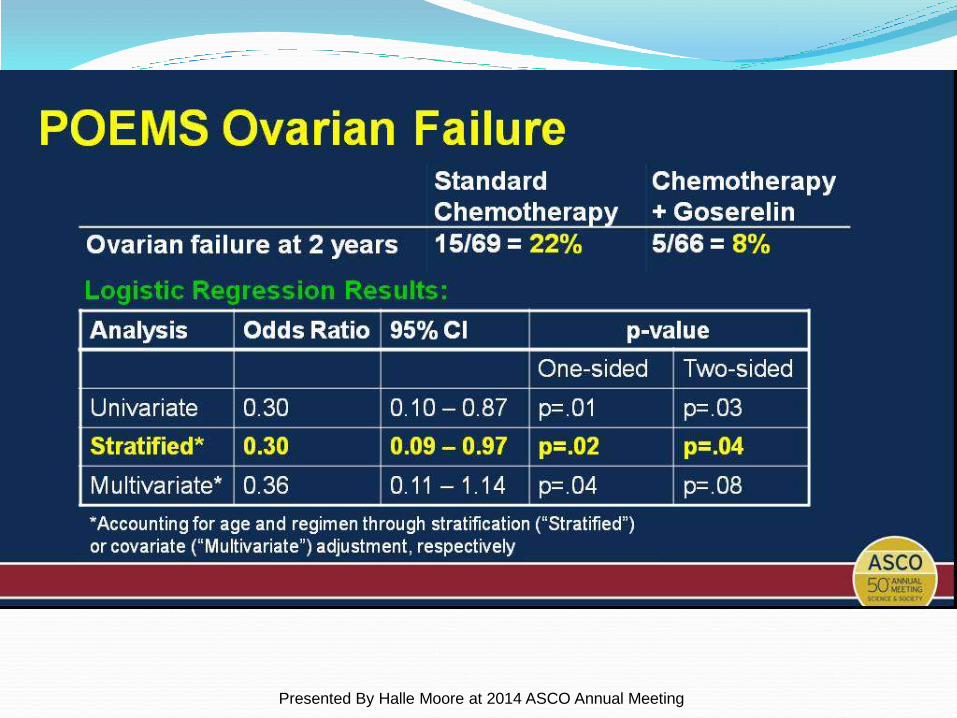
POEMS Ovarian Failure
Presented By Halle Moore at 2014 ASCO Annual Meeting
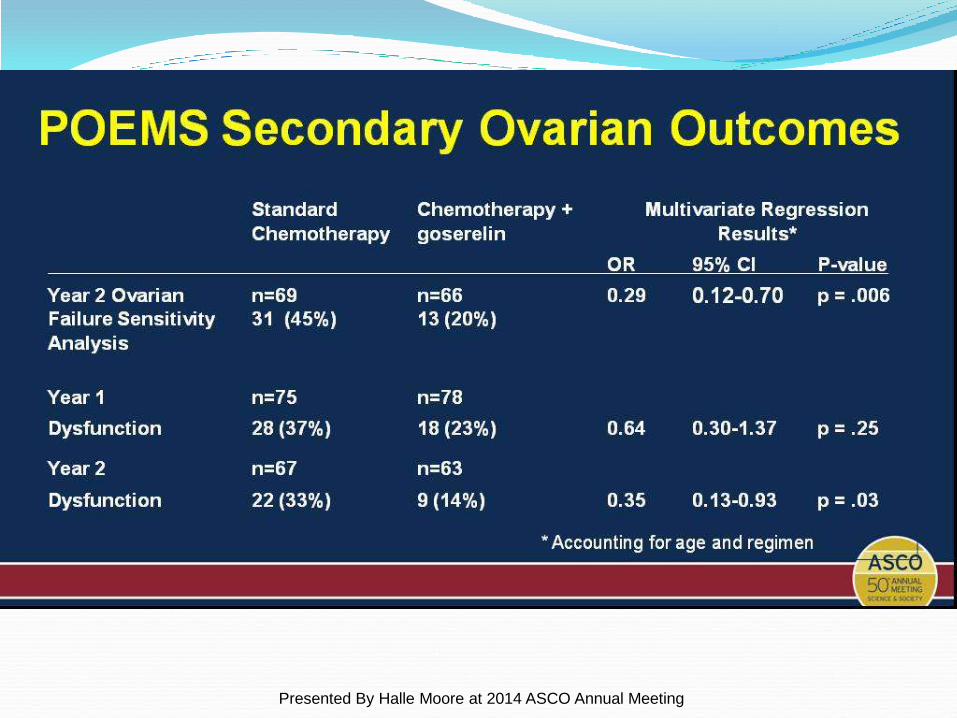
POEMS Secondary Ovarian Outcomes
Presented By Halle Moore at 2014 ASCO Annual Meeting
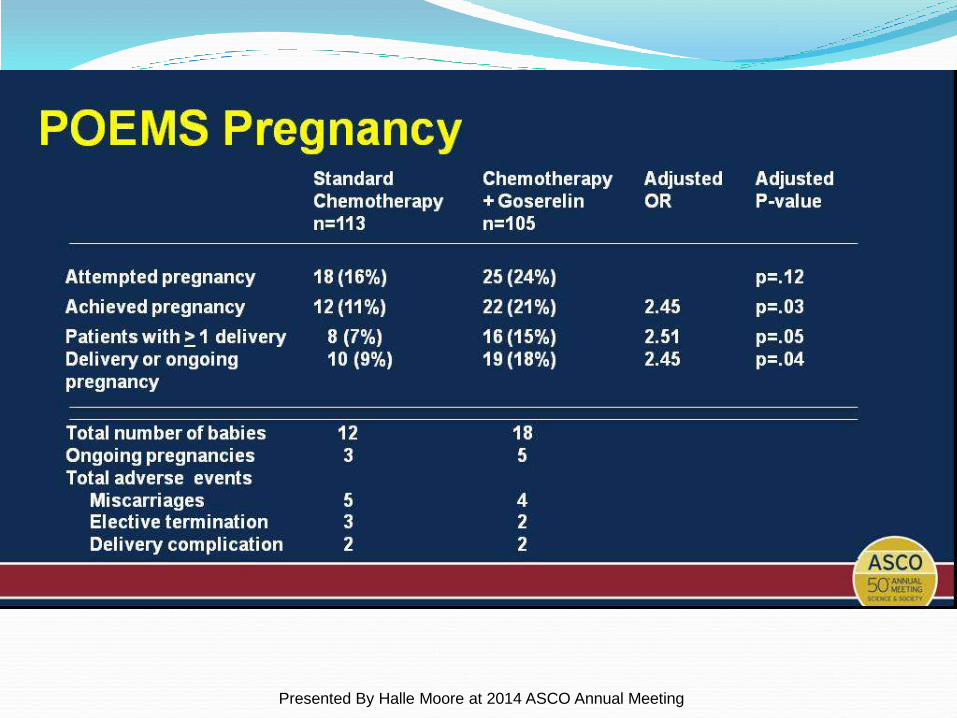
POEMS Pregnancy
Presented By Halle Moore at 2014 ASCO Annual Meeting
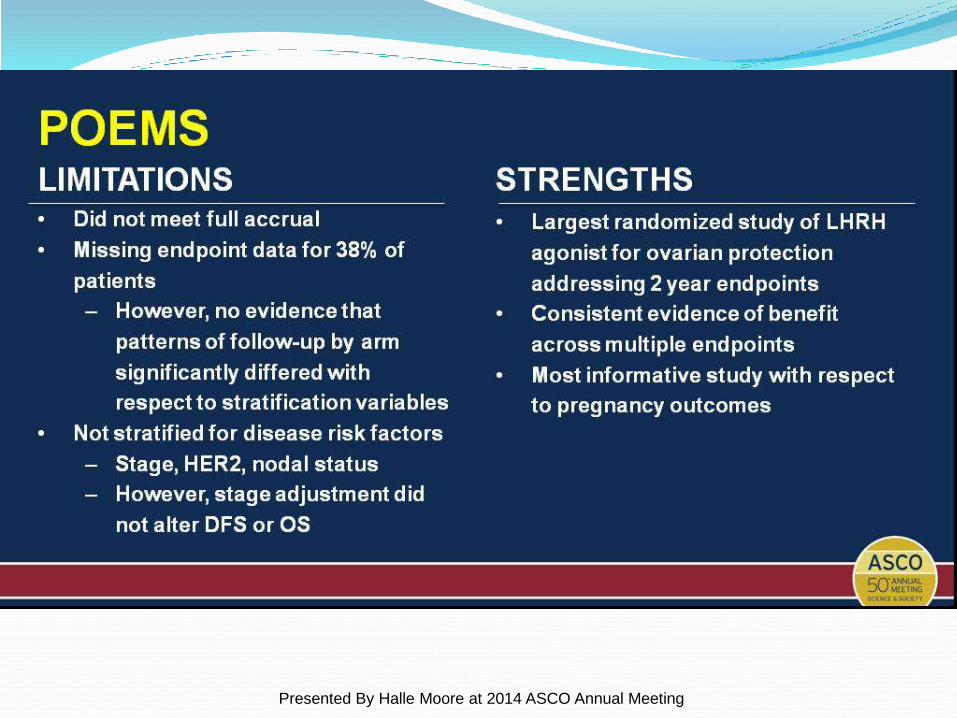
POEMS
Presented By Halle Moore at 2014 ASCO Annual Meeting
In Vitro Fertilization (IVF) IVF with embryo freezing
Can delay chemo 2-6 weeks
Best results for future pregnancies
High out of pocket cost (www.fertilehope.org)
Needs sperm donation
Safety of Fertility Preservation by Ovarian Stimulation
With Letrozole and Gonadotropins in Patients With Breast
Cancer: A Prospective Controlled Study
215 breast cancer pts prospectively evaluated for fertility preservation before adjuvant chemotherapy. 79 chose conservative ovarian stimulation (COS)
with letrozole and gonadotropins for embryo or oocyte cryopreservation
136 patients underwent no fertility-preserving procedure and served as controls.
Azim AA et al. J Clin Oncol 2008; 26:2630
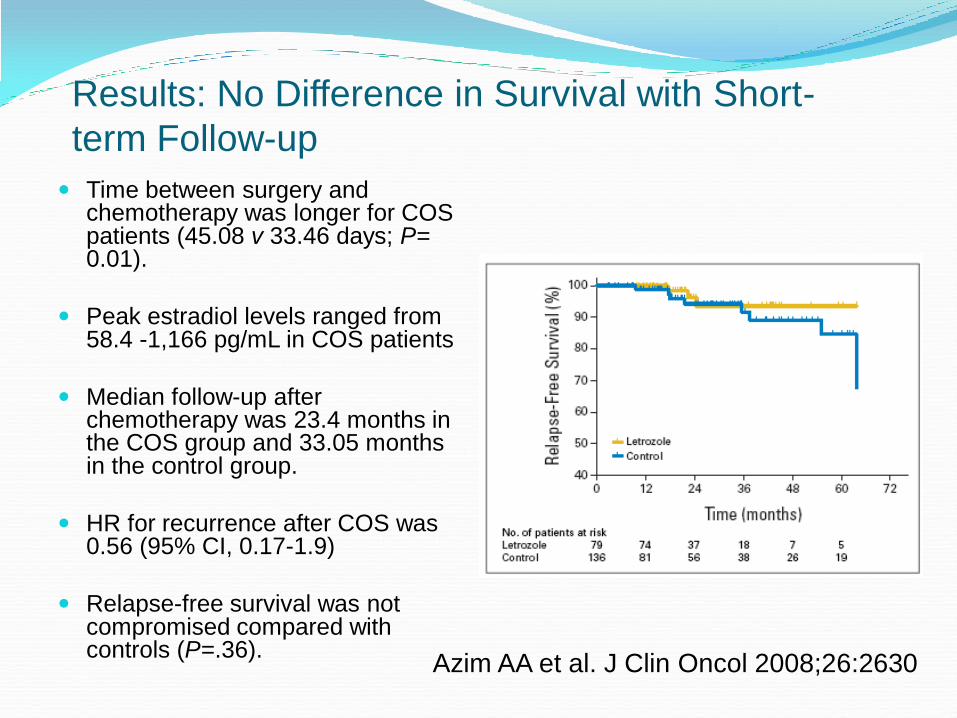
Results: No Difference in Survival with Short-
term Follow-up
Time between surgery and chemotherapy was longer for COS patients (45.08 v 33.46 days; P= 0.01).
Peak estradiol levels ranged from 58.4 -1,166 pg/mL in COS patients
Median follow-up after chemotherapy was 23.4 months in the COS group and 33.05 months in the control group.
HR for recurrence after COS was 0.56 (95% CI, 0.17-1.9)
Relapse-free survival was not compromised compared with controls (P=.36).
Azim AA et al. J Clin Oncol 2008;26:2630
Oocyte Freezing
Over 1500 pregnancies from frozen oocytes in the world
Oocyte preservation: compared to slow-freezing,
vitrification appears to result in higher oocyte survival rate,
higher fertilization rate, as well as improved embryo quality
and embryo cleavage rate
Could delay start of systemic cancer therapy by 2-6 wks
Eliminates immediate need for a sperm donor or male
partner
Out-of-pocket costs similar to IVF
Oktay K et al. Fertil Steril 2006;86:70; Cobo A, Diaz C. Fertil Steril 2011;96:277;
Borini A, Bianchi V. Clin Obstet Gynecol 2010;53:763; Huang JY et al. Am J Surg
2010:200;177; Rudick B et al. Fertil Steril 2010;94:2642
Ovarian Tissue Freezing
Experimental
Few pregnancies reported (19; www.asco.org)
Restoration of endocrine function and embryo
development in several studies
Uncertain transplantation site
Potential transmission of cancer cells
Oktay K et al. Fertil Steril 2010;93:762, Anderson RA et al. Reproduction 2008;136:681
Other Roads to Parenthood Adoption
Surrogacy
Donor egg
Online resources for patients and health care
professionals include:
www.fertilehope.org: Fertile Hope is a LIVESTRONG
initiative dedicated to providing reproductive
information, support and hope to cancer patients and
survivors whose medical treatment present the risk of
infertility.
Conclusions: Pregnancy After a
Breast Cancer Diagnosis
Women who become pregnant after breast
cancer treatment do not appear to have
increased risk of recurrence
Fertility preservation should be discussed with
all premenopausal breast cancer recognizing
the potential challenges of the available
options.
Ovarian function and fertility preservation
options continue to be investigated.