Embed Size (px)
Citation preview

Changes in attitudes, knowledge and behaviorassociated with implementing a comprehensive school
health program in a province of China
Carmen Aldinger1*, Xin-Wei Zhang2, Li-Qun Liu2, Xue-Dong Pan3, Sen-Hai Yu4,Jack Jones5 and Jared Kass6
Abstract
After successful pilot projects, Zhejiang Prov-ince, China, decided to systematically scale-uphealth promoting schools (HPS) over the entireprovince of 47 million. This study describes theinterventions and self-reported changes in atti-tudes, knowledge and behavior during the firstphase of scaling-up. Group interviews wereconducted with a sample of 191 participants(school administrators, teachers, students andparents) from nine schools with a total of;15 200 students. Grounded theory guideddata analysis. Schools implemented all HPScomponents (school health policy, physicalschool environment, psychosocial school envi-ronment, health education, health services, nu-trition services, counseling/mental health,physical exercise, health promotion for staffand outreach to families and communities),adapted to local circumstances. Participantsreported a range of changes in attitudes (payingmore attention to health, attaining better ‘psy-
chological quality’ and confidence, formingfriendships between teachers and students andfeeling more relaxed), knowledge and concepts(increasing knowledge about various healthissues, developing a broader concept of healthand gaining better understanding about theHPS concept) and behavior (actively participat-ing, increasing physical activity, improving san-itary habits, reducing or quitting smoking,eating more nutritiously, increasing safety be-havior, sustaining less injuries and improvingparent–child communication). This qualitativestudy shows the feasibility and efficacy of imple-menting HPS in Zhejiang Province, China.
Introduction
Health promoting schools in ZhejiangProvince, China
In response to the Global School Health Initiative of
the World Health Organization (WHO), regional
guidelines developed by the WHO Western Pacific
Regional Office (WPRO) and with endorsement of
the national Ministries of Health and Education,
some of China’s health and education agencies began
implementing the health promoting school (HPS)
concept in selected schools. In 1996, an HPS pilot
project was established that successfully reduced
parasitic helminth infections in rural schools [1].
This was followed in 1998 and 2000 by two HPS
projects in Zhejiang Province that successfully
addressed tobacco use prevention and nutrition, re-
spectively [2, 3]. A third project in Zhejiang Prov-
ince used materials from United Nations Children’s
Fund to address school-based injury prevention.
1Health and Human Development Programs, Education
Development Center, Newton, MA 02458, USA, 2Health
Education Institute of Zhejiang Province, Hangzhou 310000,
People’s Republic of China, 3Department of Education of
Zhejiang Province, Hangzhou 310000, People’s Republic of
China, 4Institute of Parasitic Diseases Chinese Center for
Disease Control and Prevention, Shanghai 200025, People’s
Republic of China, 5Formerly of Department of Chronic
Diseases and Health Promotion, World Health
Organization, 1211 Geneva 27, Switzerland and 6Graduate
School of Arts and Social Sciences, Lesley University,
Cambridge, MA 02138, USA
*Correspondence to: C. Aldinger.
E-mail: [email protected]
� The Author 2008. Published by Oxford University Press. All rights reserved.For permissions, please email: [email protected]
doi:10.1093/her/cyn022
HEALTH EDUCATION RESEARCH Vol.23 no.6 2008
Pages 1049–1067
Advance Access publication 13 May 2008
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

Based on the positive experiences of the pilot
projects, officials of Zhejiang Province decided to
systematically scale-up the HPS project over the
entire province, partially in an effort to achieve
the government-mandated ‘quality education’ that
focuses not only on academic achievement but also
on the child’s physical, social and emotional devel-
opment as well. With joint endorsement of the Pro-
vincial Departments of Education and Health and
support from the WHO, Zhejiang Province’s Health
Education Institute launched an effort in 2003 to
expand the development of HPS to all 11 prefec-
tures of the province. The program started with
a training workshop in Hangzhou in October
2003, for headmasters and teacher representatives
of 51 schools and health and education officers of
the prefectures, conducted by national and interna-
tional health promotion experts.
Insufficient evidence, especially fromdeveloping countries
Despite the successful pilot projects and a signifi-
cant body of theory and research that provides
a rationale for why health education, as part of
a comprehensive school health program, can be
useful and beneficial to health (e.g. [4–6]),
researchers still report insufficient evidence of the
feasibility and effectiveness of HPS. Some articles
reported that there is no universally accepted and
clear definition of what constitutes an HPS [7] and
no consensus on the criteria by which those schools
can be assessed [8, 9]. Also, studies by some of the
same authors concluded that there is currently in-
sufficient evidence in the literature to support the
efficacy and feasibility of implementing an HPS
approach [10, 11].
In addition, there is a lack of research from de-
veloping countries and particularly a scarcity of re-
search on scaling-up. An article from the WHO
Bulletin notes five factors that might underlie a lack
of evaluation research from developing countries:
poor research production, poor preparation of
manuscripts, poor access to scientific literature,
poor participation in publication-related decision-
making processes and bias of journals [12].
There are few evaluations of the full scope of
HPS interventions, as it is challenging to evaluate
the complexity of HPS. One study looked at the
incorporation of principles of the Ottawa Charter
for Health Promotion—healthy school policy, sup-
portive school environment, school community ac-
tion, developing personal skills and reorienting
services—in school-based programs published be-
tween 1983 and 1995 that targeted smoking and/or
alcohol and/or solar protection. The study found
that none of the programs incorporated all five com-
ponents of the HPS approach. Only four programs
(4.5%) utilized four of the five components and two
programs (2.3%) addressed three components [13].
A 2006 systematic review of school health promo-
tion and the HPS approach also found that none of
the schools in 12 controlled before and after studies
(mostly conducted in the United States) imple-
mented all the components of the HPS approach.
This study endorsed the HPS approach and con-
firmed the challenge of implementing and evaluat-
ing a comprehensive approach [14].
Research questions and purpose
In an effort to fill some of these gaps in research, to
investigate how the complex framework of HPS is
being implemented in a developing country and
how it affects participants, this study seeks to an-
swer the following questions: What interventions
have schools in Zhejiang Province implemented
to become HPS? What self-reported changes took
place in the lives of individuals during the imple-
mentation process?
Materials and methods
Theory
This study falls into what Smith called institutional
ethnography, a process in which interviewing is
part of an approach to investigate organizational
and institutional processes rather than informants’
inner experiences [15]. An institution, in this case,
does not refer to a particular type of organization,
but to coordinated and intersecting work processes,
such as health care or, in this case, HPS. The
C. Aldinger et al.
1050
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

purpose of this research is to discover and describe
processes of ‘how it happens’ based on putting to-
gether an integrated view from the otherwise trun-
cated accounts of each informant [15].
Context
This study provided a unique opportunity to add
a qualitative evaluation component to an ongoing
HPS project. The WHO asked Zhejiang Province,
as part of the HPS project, to conduct a series of
surveys to gather quantitative data: the Global
School-based Student Health Survey (GSHS) for
13- to 15-year olds, which assessed risk and pro-
tective behaviors related to health; evaluation index
for HPS Bronze Awards (from WHO/WPRO),
which assessed in detail the various aspects of
HPS components that the schools implemented;
WHO Psychosocial Environment Profile, which
assessed perceptions of the social and emotional
school environment and a content-related question-
naire from former pilot projects in China, which
assessed knowledge, attitudes and behaviors. The
first three instruments were generated through
WHO, the latter was developed by Chinese experts.
As a complement to these quantitative measures,
authors of this study developed qualitative meas-
ures to assess the process and procedures of imple-
menting HPS and participants’ experience with the
project.
Participants
This study was part of a WHO project in China with
specific goals and cultural considerations. Partici-
pation was controlled by the Chinese colleagues.
The Health Education Institute of Zhejiang Prov-
ince chose the participating schools based on guid-
ance from the research team: For the first round of
data collection, one former pilot school and two
schools that joined the project in the first scaling-
up phase—one from a resource-poor area and one
from a resource-rich area—were included. The fol-
lowing two rounds of data collection included only
schools from the scaling-up phase. At least one
school from a resource-poor area was investigated
in each round. The rationale for this choice was to
examine if and how HPS could be implemented in
both resource-rich and resource-poor environments.
Schools chose the interviewees based on the guid-
ance in the protocol: one to two school administra-
tors (e.g. principal and vice principal), four to six
teachers (from different subject areas) and/or other
implementers (such as school doctor), four to six
students (from different grade levels) and four to six
parents (from different socioeconomic back-
grounds), representing a mixture of males and
females for each group.
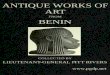
Nine schools with a total population of ;15 200
students participated in the study. The sample of
191 interview participants for this qualitative study
included 26 school administrators (19 males and
7 females), 56 teachers and school staff (21 males
and 35 females), 64 students (25 males, 34 females
and 5 gender not recorded by research team) and
45 parents (14 males and 31 females). Gender bal-
ance was not always possible for practical reasons
such as more males than females being in the
school’s administrative positions. This sample rep-
resented two elementary schools, two middle
schools, two junior high schools, one high school
and two vocational schools. Demographics of par-
ticipants are presented in Fig. 1.
Instruments
Protocols contained questions for interviews with
school administrators, teachers and other imple-
menters, students and parents. The Institutional Re-
view Board (IRB) of the employer of one of the
authors reviewed the initial protocol and deter-
mined on 19 April 2004 that the protocol met the
criteria for exemption from expedited or full IRB
review. Subsequently, the Human Subjects Com-
mittee at the authors’ academic institution waived
on 7 May 2004 the need for the IRB to review the
research.
For each round of data gathering, a questionnaire
with structured, open-ended questions, developed
by the research team, had a different focus. The first
round of data gathering focused on planning, the
second round focused on implementation and the
third round focused on monitoring and evaluation.
In the second and third round, participants were
Comprehensive school health program in a province of China
1051
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

School 1 School 2 School 3 School 4 School 5 School 6 School 7 School 8 School 9
Date
Interviewed
June 4,
2004
June 7,
2004
June 8–9,
2004
Nov 22,
2004
Nov 24,
2004
Nov 25,
2004
Nov 14–
15, 2005
Nov 16,
2005
Nov 18–19,
2005
Type of school Elementary Middle
School
High
School
Middle
School
Experime
ntal Junior
High
Vocational
school
Vocational
school
Elementary Junior High
School
Location Urban Suburban/
Rural
Suburban Urban Urban Suburban Rural/
Suburban
Rural Urban
Entry point Nutrition Nutrition Psycholog
ical health
Tobacco
control
Psycholog
ical health
Nutrition Injury
prevention
Injury
prevention
Psychologic
al health
Number of
students
n ~ 15,207
1,300 1,100 1,800 1,600 950 2,200 2,500 1,157 2,600
Number of
teachers and
staff
66 (not
recorded)
(not
recorded)
100 80 162 staff 100 51 full-
time
120–130
Interviewees:
Administrators
n = 26
7 females
19 males
n = 1
1 female:
Principal
n = 2
2 males:
Principal,
Vice
Principal
n = 2
2 males:
Principal,
Vice
Principal
n = 3
3 males:
Principal,
Vice
Principal,
Director
of Admin
n = 2
1 female:
Principal
1 male:
Vice
Principal
n = 3
3 males:
Principal,
Vice
Principal
(2)
n = 4
2 females:
Vice
Principal,
Office
n = 6
1 female:
Director
n = 3
2 females:
Vice
Principal,
Administrat
orDirector
2 males:
Vice
Principal,
Chairman
of Board
Teaching
5 males:
Principal,
Vice
Principal,
Consultg
Teacher,
Accountan
t, Director
of Teachg
1 male:
Principal
of
Fig. 1. Demographics of study participants.
C. Aldinger et al.
1052
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

School 1 School 2 School 3 School 4 School 5 School 6 School 7 School 8 School 9
Nurse;
Math
2 males:
Phys ed;
Researcher
3 males:
“Students’
work,”
Biology,
English
Nurse,
Chemistry
1 male:
Phys ed
3 males:
Phys Ed
(2), Math
Sociology
1 male:
Math
3 males:
Phys Ed,
Cooking,
Sociology
ce
3 males:
Public
Relations,
Secretarie
s, Infor-
mation &
Career
Dev
Chinese
(2), Phys
Ed, Math
Sociology,
School
Nurse
1 male:
Chinese
Students
n = 64
34 females
25 males
5 not recorded
n = 7
3 females,
4 males
n = 5
(not
recorded)
n = 6
3 females,
3 males
n = 7
5 females,
2 males
n = 7
4 females,
3 males
n = 7
5 females,
2 males
n = 6
4 females,
2 males
n = 14
7 females,
7 males
n = 5
3 females,
2 males:
Teachers
n = 56
35 females
21 males
n = 7
5 females:
Morality;
English;
Chinese;
School
n = 6
3 females:
Math,
Physics,
Phys ed
n = 5
4 females:
Psycholog
ist,
Chinese,
School
n = 6
3 females:
Sociology,
English,
School
Nurse
n = 7
6 females:
Math,
Sociology,
Chinese
(3),
n = 6
3 females:
Music,
Chinese,
School
Nurse
n = 6
3 females:
Math,
Computer,
Document
Maintenan
n = 6
2 females:
Chinese
(2)
4 males:
n = 7
6 females:
English,
Phys Ed.,
Math,
Science,
Parents
n = 45
31 females
14 males
n = 6
6 females
n = 1
1 female
n = 2
2 females
n = 5
(including
1 grand-
parent)
2 females,
3 males
n = 7
4 females,
3 males
n = 6
3 females,
3 males
n = 4
2 females,
2 males
n = 8
7 females,
1 male
n = 6
4 females,
2 males
* Key schools are schools distinguished from ordinary schools by their academic reputation and are generally allocated moreresources by the state. Their original purpose was to quicken the training of highly needed talent for China’s modernization,but another purpose was to set up exemplary schools to improve teaching in all schools (p. 244). [24]
Fig. 1. Continued
Comprehensive school health program in a province of China
1053
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

asked to provide written answers during the first
part of the interview which were then collected at
the end of the interview. A summary of interview
questions is included in Fig. 2. The questionnaire
was translated from English into Chinese prior to
the interviews by an interpreter who was part of the
initial HPS training in Zhejiang Province.
Procedure
Data collection took place during three separate vis-
its to Zhejiang Province in June 2004, November
2004 and November 2005. Each round of data
collection included four group interviews in each
of three schools. Each group interview with one
of the target groups (school administrators, teach-
ers, students, parents, respectively) lasted ;1 hour.
The interpreter asked the questions in Chinese
and translated the responses into English. One
member of the research team was Chinese. He
assisted with translations or clarifications, as
needed. A different interpreter assisted on each of
these three rounds of data collection, arranged by
the Health Education Institute. Two other inter-
preters, hired by the research team, translated writ-
ten responses. In addition, the research team
reviewed files with documents and pictures at the
schools and toured all but one school (one school
was not toured for lack of time) to make observa-
tions in an effort to triangulate the data from the
interviews.
Prior to the interviews, the interpreter received
some background on the project, HPS documents
and the protocol and instructions for the interviews.
At the beginning of each interview, and as part of
the protocol, the interpreter mentioned that the
interviews were to gather the participants’ experi-
ences and opinions in order to strengthen the imple-
mentation of the HPS project. The interpreter
stressed that each participant’s opinion was impor-
tant, that there were no right or wrong answers, that
participants should feel comfortable expressing
their ideas about the topics discussed and that their
answers would be reported anonymously to ensure
confidentiality. Interviewees agreed to have the
interviews tape-recorded.
Data analysis
Data analysis consisted of preparing the
data—including transcriptions and translations—
and analyzing the data with the qualitative data
management program Atlas.ti in two stages. The
first stage of data analysis was guided by grounded
theory which provided an opportunity to generate
theory that is grounded in data [17]. The second
stage of data analysis was guided by theoretical
frameworks such as the HPS framework [18]. This
article focuses on the first stage of data analysis
which utilized open coding.
Results
The study provided detailed results about interven-
tions for implementing all the components of an
HPS and about self-reported changes in attitudes,
knowledge or concept and behaviors of partici-
pants. This article provides a summary.
Implementing the components of an HPS
Schools in Zhejiang Province implemented com-
prehensive interventions that addressed all of the
components of HPS as follows.
For ‘school health policy’: Schools made HPS
regulations for each school department, established
non-smoking policies and posted policies on school
walls or boards. To create a healthy ‘physical
school environment’: Schools improved facilities
such as dining rooms, dormitories, teaching and
sports facilities, enhanced cleanliness and held
beautification projects. To improve the ‘psychoso-
cial school environment’: Schools assured a harmo-
nious and caring psychosocial atmosphere,
established good relationships between teachers
and students and provided equal treatment. To im-
plement ‘health education’: Teachers integrated
health topics into regular teaching and increased
use of participatory teaching and learning methods,
held special health education classes, extracurricu-
lar activities and drawing and writing competitions.
For ‘health services’: Schools offered annual med-
ical checkups for students and staff, prevention and
treatment of common diseases and—those with
C. Aldinger et al.
1054
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

dormitories—had doctors on 24-hour duty. To im-
plement ‘nutrition services’: Schools offered nutri-
tious and balanced meals, more food variety and
training by nutritionists for kitchen staff. For ‘coun-
seling/mental health’: Schools offered psychological
consultation by specially trained teachers, hotlines,
First round: focus on planning (June 2004)
For school administrators:
What is your position at this school?
What health topic has your school selected as an entry point? How was that topic
selected?
Does your school have an HPS planning committee? Who is part of the planning
committee? How were these people chosen? What are their roles?
Does your school have a work plan developed (or will it develop a work plan)? Who was
(or will be) involved in developing this work plan? How did (or will) you decide what to
include?
For teachers:
What grades and subject do you teach?
How do you choose what topics to address and which methods to use? Why?
For students:
In which grade are you?
Do you know if any students are part of the working committee that plans the new health
activities? If so, what is their role?
For parents:
In which grade is your child?
Do you know if parents are involved in an HPS planning committee that plans the new
activities? How did they get involved?
For all:
Can you describe to me what you think a Health-Promoting School is?
How did you learn about the HPS concept? From whom?
How do you feel about your school becoming a Health-Promoting School? Why?
Which new activities have you done at school since April/May when the health
interventions started?
What challenges do you expect? How could they be handled?
Fig. 2. Interview questions.
Comprehensive school health program in a province of China
1055
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

special mailboxes and set up special consultation
rooms. To improve ‘physical exercise’: Schools re-
quired morning exercises and engaged in sports
matches. To encourage ‘health promotion for staff’:
Schools encouraged staff to quit smoking—for in-
stance, through smoke-free school regulations—
and to exercise more and offered psychological
consulting for teachers. For ‘outreach to families
make this school a Health-Promoting School?
What teaching and learning materials and methods have you used in your classroom? Have
you tried any new teaching and learning methods since last November? If so, what new
methods did you try and how well did they work?
For students:
In which grade are you?
What has been done differently in your school since last November to help make your school
a Health-Promoting School?
What (if anything) have you personally done differently since your school became a Health-
Promoting School?
In what ways, if any, are students helping their school to become a Health-Promoting
School? To what extent do you think students can help make a difference?
Second round: focus on implementation (November 2004)
For school administrators:
What is your position at this school?
What health topic (or topics) has your school selected as an entry point? How was that topic
selected?
Does your school have an HPS planning committee? Who is part of the planning committee?
How were these people chosen? What are their roles?
Does your school have a work plan to become a Health-Promoting School?
Which interventions have been implemented since last November?
How were these interventions chosen? Why were they chosen?
For teachers:
What grades and subject do you teach?
Do teachers choose the health topics that they address with their students? (If relevant), what
are some of the topics that you have chosen? Why did you choose these particular topics?
What interventions have been implemented since last November in support of your effort to
Fig. 2. Continued.
C. Aldinger et al.
1056
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

What challenges were encountered? How can these challenges be addressed?
What else can you tell me about what you have learned that would be helpful to others who
want to implement effective school health programs?
Do you have any further comments or questions?
Third round: focus on monitoring and evaluation (November 2005)
For school administrators:
What is your position at this school?
Please tell me if you did anything to assess the implementation or effectiveness of the
interventions. If so, please tell me what you did and what you found. Tell me if you made
any changes based on your findings, and if so, what kind of changes you made.
For teachers:
What grades and subject do you teach?
Please tell me if you did anything to assess the implementation or effectiveness of the
interventions. If so, please tell me what you did and what you found. Tell me if you made
any changes based on your findings, and if so, what kind of changes you made.
For students:
In which grade are you?
For parents:
In which grade is your child?
For parents:
In which grade is your child?
What has been done since last November to help make your child’s school a Health-
Promoting School?
What (if anything) has been different for you personally since your school began working to
become a Health-Promoting School?
In what ways, if any, are parents helping their school to become a Health-Promoting School?
To what extent do you think parents can help make a difference?
For all:
Can you describe briefly what you think a Health-Promoting School is?
So far, what went well in your school’s effort to become a Health-Promoting School?
Fig. 2. Continued.
Comprehensive school health program in a province of China
1057
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

and communities’: Schools distributed materials to
communities, sent letters, made calls to parents and
conducted parents’ school (teaching parents in the
evening or on the weekend about health).
Besides addressing all HPS components, schools
in Zhejiang Province also engaged various people
such as parents and community members in devel-
oping HPS, as suggested by the HPS framework.
A summary of interventions for each component
is included in Fig. 3.
Changes in attitudes
‘Attitude changes’ for many participants included
‘paying more attention to health’. For example,
people realized the importance of nutrition and of
healthy surroundings, the danger of smoking, the
importance of hygiene and safety and developed
health consciousness, including attention to psy-
chological health. Students (and staff) ‘attained
better psychological quality and confidence’. This
included the ability to handle difficulties, more
confidence, becoming more communicative and
improving emotional and self-control. This contrib-
uted to richer lives, increased motivation to study
and more enjoyment. School administrators ‘put
themselves in others’ shoes’ first to better under-
stand others’ behavior. Some schools experienced
‘friendships between teachers and students’. Stu-
dents turned to teachers for help if they had prob-
lems and treated teachers ‘like friends’. Teachers
felt valued, like a ‘big brother’, and experienced
more satisfaction with their work. This was cited
as unusual in China, where teachers are tradition-
ally responsible for teaching and disciplining stu-
dents, and schools and the society expect students
to focus on their studies. These developments made
parents ‘more relaxed’ because they gained confi-
dence that the school was taking good care of their
Please tell me your overall impression/assessment of the HPS project at your school.
(Why do you think this way?)
Please tell me: What was the (one) most important positive outcome/change since your
school has become a Health-Promoting School? How was it before your school became a
Health-Promoting School? How was it afterwards?
Please tell me what has been different in your life since your school became a Health-
Promoting School
Do you have any further comments or questions?
If time allows:
Please tell me what challenges were encountered with implementing and evaluating HPS
interventions. How can these challenges be addressed?
What else can you tell me about what you have learned that would be helpful to others
who want to implement and evaluate effective school health programs?
For all:
Hold up the Chinese characters for “Health-Promoting School.” Can you please describe
what this (the HPS concept) means to you?
Fig. 2. Continued.
C. Aldinger et al.
1058
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

Components of Health-Promoting Schools
School health policy
e.g., smoking ban
regulations for each school department and many health-related items
including safety regulations
posted policy on school walls or boards
handbook for student behavior
Physical school environment
e.g., improved facilities, including dining room, dormitories, sports facilities
multimedia classroom
improved sanitation facilities and reduced littering
green, clean and beautiful school environment
meeting WHO and national standards
Psycho-social school environment
e.g., teachers and students became friends
harmonious relationships
equal treatment
student support groups
Health education
e.g., integrating health into regular teaching
special health education classes
drawing and writing competitions
professionals gave lectures, workshops
Health services
e.g., annual medical check-ups for students and staff
prevention and treatment for common diseases
doctors on duty
Nutrition services
e.g., nutritious meals, more food variety
balanced fixed plates
training and advice from nutritionists for kitchen staff
Fig. 3. Examples of implemented HPS components.
Comprehensive school health program in a province of China
1059
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

children, that the school provided safe and harmo-
nious surroundings (e.g. with good relationships
between teachers and students and among students)
and that their child was improving his or her self-
control and psychological quality.
Changes in knowledge and concepts
‘Health-related knowledge gains’ included in-
creased knowledge about nutrition, hygiene, safety
and security, the harm of tobacco, how to avoid
injuries and psychological knowledge such as
how to relieve anxiety and what is normal and ab-
normal. (This will be further detailed elsewhere in
reports about the quantitative evaluation of the
interventions.) A knowledge transfer occurred from
children to parents. Participants also developed
a ‘broader concept of health’ that included not only
physical health but also psychological and social
health. An ‘understanding of the HPS concept’ de-
veloped over time. It included gaining of knowl-
edge and understanding of different components
of the concept for different participants. Actively
involved school administrators developed the most
complex understanding of the HPS concept, fol-
lowed by teachers, students and parents who devel-
oped a less complex but sufficient understanding to
recognize it as providing a positive quality to the
school.
Changes in behavior
‘Behavior changes’ included more ‘active partici-
pation’ in the project. Students and parents actively
participated in activities such as publicizing health
knowledge to neighbors and friends and taking part
Counseling/ mental health
e.g., psychological consultation by specially trained teachers
hotline, special mailbox, special consultation room
consultation for teachers
Physical exercise
e.g., morning exercises
sport matches such as football, basketball, volleyball
improved sports facilities
Health promotion for staff
e.g., encouraged staff to quit smoking
more exercise and walking
psychological consulting for teachers
Outreach to families and communities
e.g., distribution of materials, letters to parents
visits and calls to parents’ homes
parents’ school
increased parent-child communication
students distribute health information (“publicity”) in the community
Fig. 3. Continued.
C. Aldinger et al.
1060
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

in school events. Some participants ‘increased their
physical activity’ and did more physical exercise
such as utilizing the school playground or walking
to school rather than taking the bus. Students also
‘improved sanitary habits’ such as not throwing
litter on the ground, paying attention to personal
hygiene such as brushing teeth twice a day, washing
hands before and after dinner and after using the
toilet, cutting their nails regularly and washing their
clothes. Many teachers and parents ‘reduced or quit
smoking’. Some children persuaded their fathers
and grandfathers successfully to reduce or quit
smoking. Administrators and staff quit smoking
or did not smoke on school grounds, especially if
the school established no-smoking rules. Partici-
pants also ‘changed bad habits’ and developed
good habits. This included a variety of habits, such
as paying attention to personal health issues, dis-
playing civilized behaviors, improving living hab-
its, self-adjustment and adaptability. Students
persuaded their classmates and friends to change
their habits. Participants also ‘ate more nutritiously’
such as not eating fried food, intentionally buying
healthy food and balancing their diets rather than
having special food preferences. Vendors who sold
unqualified foods outside one school moved away
because students and teachers stopped buying from
them. ‘Increased safety behaviors’ included stu-
dents wearing yellow safety hats and walking to-
gether, not taking vehicles without certificates,
wearing safety helmets and obeying traffic rules
when riding a bike. Consequently, accidental ‘inju-
ries decreased’ significantly. For instance, in one
school, accidental injuries dropped ;41% within
1 year and a half, and in another school, injuries
decreased almost 39% from one school year to the
next, according to statistics kept by the school. ‘Par-
ent–child communication’ improved. As the only
child, children in China were at the center of their
family, and children could teach their parents and
grandparents about healthy behaviors. In turn,
parents had more communication with their child
and shared their own growing up experiences. Chil-
dren with lower academic scores got more commu-
nicative with parents after they had opportunities to
express their talents at school in different ways.
HPS helped parents and students to communicate
with each other, and children became more sociable
and shared new experiences that happened in
school with their parents.
A summary of these self-reported changes in par-
ticipants is included in Fig. 4.
Discussion
Unique aspects of this study included that schools
implemented truly comprehensive interventions, par-
ticipants expressed their understanding of the broad
concept of health and HPS and program implement-
ers recognized children’s status within the families in
China as a particularly unique and promising oppor-
tunity to influence the health of parents and grand-
parents. In addition, this study pointed to the need for
training and demonstrated the value of a qualitative
approach to school health research.
Implementing truly comprehensiveinterventions
This study showed that schools implemented com-
prehensive interventions in three aspects: first,
schools addressed all the components of an HPS;
second, schools addressed various health topics and
third, schools focused on holistic development of
students.
Schools used their full organizational potential
by implementing all HPS components. Thus, unlike
the studies by Lynagh et al. [13] and Stewart-
Brown [14] that showed that none of the programs
incorporated all five components of the Ottawa
Charter in the HPS approach, this study showed
that the visited schools in Zhejiang Province
addressed virtually all of the components of the
Ottawa Charter at school level (policy, supportive
environment, community action, personal skills and
health services). The variety of activities that
schools reported was a good example of the under-
standing and application of a comprehensive ap-
proach to health, as called for by the HPS
concept. As noted by a deputy headmaster, their
understanding of health became more comprehen-
sive and, consequently, their ideas and interven-
tions also became more comprehensive.
Comprehensive school health program in a province of China
1061
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

Attitude changes
Paying more attention to health
Realizing the importance of health and paying more attention to health
Attaining better “psychological quality” and confidence
Students, and some staff, improving their psychological qualities, including their
ability to handle difficulties, and increasing their confidence
Forming friendships between teachers and students
Teachers becoming like friends of students
Feeling more relaxed
Parents, some students and administrators, feeling more relaxed
Knowledge and conceptual changes
Increasing knowledge about health issues
Participants increasing their knowledge about health, nutrition, hygiene, safety and
security, the harm of tobacco, how to avoid injuries, and psychological knowledge
Developing a broader concept of health
Participants realizing that health is a broader concept that includes physical, mental and
social health
Gaining a better understanding about the HPS concept
Participants expressing a very comprehensive understanding of the components and
concept of a Health-Promoting School
Behavior changes
Actively participating in the project
Students and parents actively participating in the project, spreading knowledge and
forming good habits
Increasing physical activity
Some participants increasing their physical activity
Improving sanitary habits
Students decreasing littering and improving their hygiene habits, such as hand washing and
brushing teeth
Fig. 4. Participants’ self-reported changes.
C. Aldinger et al.
1062
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

Furthermore, schools implemented a truly compre-
hensive approach that addressed various health top-
ics. In contrast, school health programs in developed
countries often focus on one health issue. For in-
stance, in the United States, there is an extensive data-
base of programs that focus only on substance abuse
prevention and treatment programs that have pro-
duced favorable results (http://modelprograms.samhsa.
gov/). Schools in Zhejiang Province addressed not
only the health issue that they had chosen as entry
point, but all the schools in this study addressedvarious
health issues. Inmost cases, this included tobacco con-
trol, nutrition, exercise, psychological health, hygiene,
as well as other prevalent health issues such as inju-
ries or severe acute respiratory syndrome (SARS).
In addition, schools started to focus on holistic
or ‘all-around development’ of students, not just
academics. This was supportive of the approach
to quality education called for by the Chinese gov-
ernment. For example, in one school, a teacher
thought that the greatest achievement of this project
was that after implementing the project for
1.5 years, he focused on academic learning but
cared for the students in all aspects.
Thus, implementing HPS was a comprehensive
approach in many aspects: implementing a wide
range of interventions, addressing various health
topics and addressing holistic development of
students.
Understanding the broad concept of HPS
The apparently increased level of understanding of
a broad concept of health and of the HPS con-
cept—that is based on an understanding of a broad
Reducing or quitting smoking
Many teachers, fathers and grandfathers reducing or quitting smoking
Changing various bad habits
Many participants changing their bad habits such as sanitary and other living habits,
and persuading others to change their bad habits, too
Eating more nutritiously
Students and their families changing to a more balanced diet, less fried food, more
vegetables, etc.
Increasing safety behavior
Students wearing yellow safety caps and walking together, not taking bicycles or
vehicles without certificates to school
Parents and teachers wearing safety helmets
Sustaining less injuries
Injuries in two schools dropping by about 40 percent
(according to statistics on injuries kept by the schools)
Improving parent-child communication
Children having better communication with their parents
Parents communicating more with their child
Fig. 4. Continued
Comprehensive school health program in a province of China
1063
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

concept of health—might be one of the project’s
most important achievements. As has been docu-
mented in nursing, ‘an understanding of the client’s
concept of health is necessary to conduct relevant
and effective health assessment, planning, interven-
tion and evaluation’ [19]. This is also crucial in
health promotion.
Since data in Zhejiang Province could not be
gathered in the same schools during subsequent
visits, these data cannot prove with certainty that
the level of understanding has improved in any par-
ticular school. However, the findings clearly indi-
cate that, during the first round of data collection,
participants’ level of understanding of the health
concept was less well developed. For example, dur-
ing the first round of data collection, some parents
and children were reluctant to answer when asked
to describe an HPS. There was also a challenge of
translating the concept into Chinese. One teacher
asked during a training session if the characters
meant ‘Health Promotion School’ or ‘health pro-
motes school’. During the second round of data
collection, participants’ responses demonstrated
a much deeper and more detailed understanding
of the nature and scope of HPS than the earlier
interviews. For example, a school administrator de-
fined six features of HPS and thus demonstrated
a good understanding of the components of HPSs
as well as an understanding of health in a broad
sense. Participants’ responses during the third
round of data collection revealed a similarly de-
tailed concept of health and HPS. Respondents
reported repeatedly that their concept of health
changed during the implementation of this project
from a narrow focus on physical health to a broader
focus that included social and psychological health.
This implies that the level of understanding of
a broad concept of health grew profoundly in pro-
ject schools during the implementation period.
Engaging children in educating parents andserving as change agents
Children passed on health information to their
parents and grandparents, many of whom had
a lower level of education. Thus, children were
often effective teachers of their parents and initia-
tors of attitude and behavior changes.
For example, one school asked their students—
when they went home during their summer or win-
ter vacation—to explain the contents of the
students’ handbook, with basic knowledge about
health, to their parents. In another school, one
mother expressed that the students could serve as
a bridge to spread knowledge, and when children
said something, the adults would pay more atten-
tion to it. This was considered better than adults
spreading the knowledge to each other. Children
had a special role since they were usually an only
child—due to China’s one-child policy—so parents
and grandparents paid special attention to this ‘little
emperor’. The recognition of this unique status of
children in China and its potential to affect change
are unique to this study.
However, the role of children to educate their
families is not only a Chinese phenomenon. In
India, children have also been health promoters. A
2005 article reports ‘The school children, who are
the first generation to be educated, became the
agents of change. Their role was to promote healthy
behaviors amongst younger children, children of
same age, their immediate families and larger com-
munity’ [20, p. 148].
Thus, HPS projects can seize on unique circum-
stances of cultures and communities to enable chil-
dren to be effective change agents, especially in
developing countries and among a parents’ genera-
tion with low levels of education.
The need for training
One of the most frequently mentioned challenges
was a perceived lack of professional development
and support to expand knowledge, skills and expe-
rience about health promotion.
For instance, in some schools, teachers asked the
research team to pass on ‘advanced knowledge’.
In one school, teachers first thought that their nu-
trition knowledge was sufficient, but when the pro-
ject gained in intensity, they felt a need for more
professional instruction and hoped for more ex-
pert talks, though they also acknowledged that
C. Aldinger et al.
1064
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

‘knowledge is not enough’ and that some students
knew better than teachers. The research team also
observed that, while the schools conducted all the
required surveys, they did not seem to know how to
interpret the data to use for program planning.
Training has been shown to be crucial for health
education. For instance, evaluation of a comprehen-
sive health education curriculum in the United
States showed that trained teachers were better pre-
pared, implemented the curriculum with more fidel-
ity and achieved more positive effects on student’s
knowledge [21].
Thus, this study confirmed the importance of
teacher training and pointed to the need for more
professional development in health promotion con-
cepts, knowledge, skills and experiences about HPS
and related issues.
Qualitative approach to research
In addition to demonstrating positive behavioral
and attitudinal outcomes from this HPS project, this
study also demonstrated the value of a qualitative
approach to HPS research.
Through in-depth interviews and focused inves-
tigative dialogues with participants, this study gen-
erated a complex picture and understanding of the
multidimensional process of change which occurs
during an HPS project. Precisely, because HPS
projects promote change in the ‘whole person’
and the ‘whole system’ through which a school
operates, they require a multidimensional analysis
which is sensitive to the interplay between the in-
tellectual, social, emotional and systemic aspects of
learning and change. In such ‘holistic’ interven-
tions, qualitative approaches to data collection and
analysis provide important benefits.
The benefits of a qualitative approach do not
negate the value of quantitative assessments of prog-
ress. Rather, they can contribute a rich, more nu-
anced understanding of complex change processes
that quantitative methods cannot capture [22].
Limitations
There were a number of limitations in the method-
ological design of the study that were inherent in
the complexity of this HPS project that could not
be avoided. They were part of the real-world re-
alities in which such projects must operate. The
limitations of this study were related to the role
of the researcher, social desirability bias, language
and interpretation/translation, culture, timing of
interventions and surveys, study design and self-
reporting.
Particularly in qualitative research, it is important
to consider the role that the researcher plays [23]. It
was obvious that the Health Education Institute
paid special attention to the research team whom
they accompanied during the interviews, which
could potentially influence the responses. During
many of the group interviews, additional people
were present besides those being interviewed and
at least some of the participants seemed to be pre-
pared for the interviews and had notes. This was
understandable because of the high importance at-
tached to the visit of ‘foreign experts’. This has also
been observed in other settings [24]. Despite this,
many participants seemed to share very openly,
even about their challenges.
Language and cultural differences and the need
for interpretation/translation across languages can
contribute to misunderstandings and false interpre-
tations [22]. Ideally, a native speaker should con-
duct such research, but short of that, international
researchers can help bring findings from developing
countries into English-speaking literature.
The study revealed that some of the interventions
already existed before schools became HPS. How-
ever, it also showed that the HPS approach fit well
with existing activities and enabled schools to im-
plement a truly comprehensive approach.
The initial plan was to interview the same three
schools that were interviewed during the first round
of data gathering at two more time intervals. This
was culturally not appropriate because the schools
would have received a disproportional amount of
attention and resulting local publicity. Conse-
quently, different schools of the same cohort and
with similar characteristics were selected for the
second and third round of data gathering. Thus,
the study design had to be flexible in order to ac-
commodate the actual situation.
Comprehensive school health program in a province of China
1065
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

All of these data are self-reported, just as major
school health surveys such as the Youth Risk Behav-
ior Surveillance of the US Centers for Disease Con-
trol and Prevention and the GSHS of WHO also
depend on self-reporting. As in these major surveys,
it is difficult to verify the data. Talking to various
groups of people at various schools and time inter-
vals, supplemented by observations, allowed for
some triangulation in this study. Triangulation refers
to ‘using multiple methods in order to obtain more
thorough coverage of a subject by viewing it from
different angles’ [25]. This study design was based
on what was feasible in the given situation.
Conclusion and recommendations
This study showed that it was feasible and effective
to implement the HPS project in Zhejiang Province,
China, focusing on different health issues and with
different levels of resources. Based on these posi-
tive findings, and as participants suggested, the
HPS project should be implemented more widely
in China and in other parts of the world.
Funding
World Health Organization to Health Education In-
stitute of Centers for Disease Control in Zhejiang
Province HQ/05/121651, S.-H. Y. HQ/04/893602
and Education Development Center HQ/05/120607
and HQ/05/12011.
Acknowledgements
We want to sincerely thank all the 191 people who
were interviewed for this study.
Conflict of interest statement
None declared.
References
1. Xu L-S, Pan B-J, Lin J-X et al. Creating health-promotingschools in rural China: a project started from deworming.Health Promot Int 2000; 15: 197–206.
2. Ma HL, Geng L, Xia S-C et al. Development of health-promoting schools with tobacco use prevention as entrypoint. Chin J Health Educ 2002; 18: 414–7.
3. Xia S-C, Zhang X-W, Xu S-Y et al. Creating health-promoting schools in China with a focus on nutrition.HealthPromot Int 2004; 19: 409–18.
4. Mangrulkar L, Vince-Whitman C, Posner M. Life Skills Ap-proach to Child and Adolescent Healthy Human Develop-ment. Washington, DC: Pan American Health Organization,2001.
5. World Health Organization: Skills for Health. Skills-BasedHealth Education, Including Life Skills: An Important Com-ponent of a Child-Friendly/Health-Promoting School. WHOInformation Series on School Health; Document 9. Geneva,Switzerland: World Health Organization, 2003.
6. Vince-Whitman C, Aldinger C, Levinger B et al. ThematicStudies. School Health and Nutrition. World EducationForum Education for All 2000 Assessment. Paris, France:UNESCO: 2001.
7. Stewart DE, Parker E, Gillespie A. An audit of health pro-moting schools policy documentation. J Sch Health 2000;70: 253–4.
8. Lynagh M, Perkins J, Schofield M. An evidence-based ap-proach to health promoting schools. J Sch Health 2002; 72:300–2.
9. St Leger L, Nutbeam D. Research into health promotingschools. J Sch Health 2000; 70: 257–8.
10. Lynagh M, Knight J, Schofield MJ et al. Lessons learnedfrom the Hunter Region Health Promoting Schools Projectin New SouthWales, Australia. J SchHealth 1999; 69: 227–32.
11. St Leger L. School, health literacy and public health: possi-bilities and challenges. Health Promot Int 2001; 16: 197–205.
12. Langer A, Diaz-Olavarrieta C, Berdichevsky K et al. Why isresearch from developing countries underrepresented in in-ternational health literature, and what can be done about it?Bull World Health Organ 2004; 82: 802–3.
13. Lynagh M, Schofield MJ, Sanson-Fisher RW. School healthpromotion programs over the past decade: a review of thesmoking, alcohol and solar protection literature.Health Pro-mot Int 1997; 12: 43–60.
14. Stewart-Brown S. What is the Evidence on School HealthPromotion in Improving Health or Preventing Diseaseand, Specifically, What is the Effectiveness of the Health Pro-moting Schools Approach? Copenhagen, Denmark: WorldHealth Organization Regional Office for Europe, 2006.
15. DeVault M, McCoy L. Institutional ethnography. Usinginterviews to investigate ruling relations. In: Holstein JA(ed). Handbook of Interview Research. Context andMethod.Thousand Oaks, CA: Sage; 2002. 751–76.
16. Ristock JL, Pennell J. Community Research as Empower-ment. Toronto, Canada: Oxford University Press, 1996, 51.
17. Strauss A, Corbin J. Basics of Qualitative Research: Tech-niques and Procedures for Developing Grounded Theory.2nd edn. Thousand Oaks, CA: Sage, 1998.
18. World Health Organization. What Is a Health-PromotingSchool? 2006. Available at: http://www.who.int/school_youth_health/gshi/hps/en/index.html. Accessed on 31October 2006.
19. Long K. The concept of health. Rural perspectives. NursClin North Am 1993; 28: 123–30.
C. Aldinger et al.
1066
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from

20. Mukhopadhyay BB, Bhatnagar PC. Children as health pro-moters. Promot Educ 2005; 12: 148–9.
21. Ross JG, Luepker RV, Nelson GD et al. Teenage healthteaching modules: impact of teacher training on implemen-tation and student outcomes. J Sch Health 1991; 61: 31–4.
22. Patton MQ. Qualitative Research and Evaluation Meth-ods. 3rd edn. Thousand Oaks, CA: Sage Publications,2002.
23. AngrosinoMV,Mays de Perez KA. Rethinking observation.From method to context. In: Denzin NK, Lincoln YS (eds).
Handbook of Qualitative Research. 2nd edn. ThousandOaks, CA: Sage, 2000, 673–702.
24. Gokah TK. Health education in rural settings in Ghana:a methodological approach. Health Educ Res 2007; 22:907–17.
25. Marlow-Ferguson R, Lopez C. World Education Encyclo-pedia. 2nd edn. Farmington Hills, MI: Gale Group, 2002.vol. 1.
Received on October 18, 2007; accepted on March 23, 2008
Comprehensive school health program in a province of China
1067
by guest on August 17, 2012
http://her.oxfordjournals.org/D
ownloaded from