Embed Size (px)
Citation preview

Management of Melanoma in a PatientPopulation: Using Electronic Health Recordsto Enhance Postdiagnosis Surveillance
E arly detection of melanoma reduces morbidityand mortality, yet research to evaluate theeffectiveness of total-body skin examinations
(TBSEs) is lacking. Because a history of melanomaconfers a greater risk for developing subsequent pri-mary melanomas (SPMs),1 the Dermatology Divisionof Kaiser Permanente Hawaii recommends at leastannual TBSEs in these patients. Our study evaluatedthe benefit of using electronic health records (EHRs)to track patients with a history of melanoma to ensureannual TBSEs.
Methods. Individuals diagnosed as having an SPM be-tween February 1, 2010, and February 28, 2011, wereincluded using Kaiser Permanente’s KP HealthConnectEHR. Chart review was performed to determine if the SPMwas diagnosed during a Kaiser Permanente–initiated an-nual screening TBSE or a patient-initiated encounter. Pa-tient awareness of the lesion was also assessed. One samplet test was used to determine whether the SPM incidencein the Kaiser Permanente Hawaii population differed fromthe baseline melanoma incidence in Hawaii. Multiple re-gression analysis using stepwise backward eliminationevaluated age, sex, and patient awareness of lesion as pre-dictors of Breslow thickness. Statistical analyses were per-formed using SAS software, version 9.1 (SAS Institute Inc).
Kaiser Permanente Hawaii’s institutional review boardapproved this study.
Results. During our study period, 48 SPMs were diag-nosed in 42 patients. The incidence of SPMs was signifi-cantly higher than the baseline melanoma incidence inHawaii (P� .001).2
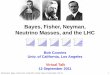
Of the 48 SPMs, 40 (83%) were diagnosed in patientswho were contacted for a timely annual TBSE and an ad-ditional 4 (8%) were diagnosed in patients who were con-tactedbecause theywereoverdue for this examination.Noneof these patients were aware of their melanomas (Figure,groups A and B). Four SPMs (8%) were diagnosed in pa-tients who were not due for TBSEs but who detected a wor-risome lesion on themselves (Figure, group C).
The time lapse between the SPM and the most recentprior melanoma ranged from 3 months to 31 years(mean, 4.4 years) (Table). The mean Breslow thicknessof the invasive SPMs was 0.39 mm. Twenty-seven per-cent of SPMs were thicker than the most recent priormelanoma (13 of 48); 13% were the same thickness (6 of48); 50% were thinner (24 of 48); and 10% had unknownprior melanoma thicknesses (5 of 48). Sixty-five percentof SPMs occurred on non–sun-exposed skin, presumablydecreasing the ease of patient self-detection for theselesions.
With multivariate regression using stepwise back-ward elimination, age and gender were found not to pre-dict Breslow thickness, but patient awareness of the le-sion was a predictive factor. The melanomas detected bypatients (group C, average Breslow thickness, 0.57 mm)were significantly thicker than those detected by the der-matologists during screening examinations (groups A andB, average Breslow thickness, 0.22 mm) (P � .01).
Comment. A history of melanoma confers an increasedrisk for SPMs, often occurring within a few months to 2years after the primary melanoma is identified. How-ever, some studies have shown significantly longer in-tervals between the initial and second primaries.3 The longinterval found in our study lends support to the conceptof lifelong annual follow-up.
Screening TBSEs performed by physicians during theSCREEN study4 resulted in an increase in melanoma in-cidence, proving TBSEs to be an effective screening tool.Brobeil et al5 found that 93% of SPMs were dermatologist
48 Lesions diagnosedin 42 PTs
4 Overdue for annualTBSE (tracked bymelanoma database)
0 PTs awareof lesion
Group B:4 PTs unaware
of lesion∗
Group C:4 PTs awareof 4 lesions
Group A:34 PTs unawareof 40 lesions∗
44 Not overdue forannual TBSEin 38 PTs
Figure. Second primary melanomas diagnosed during 13-month studyperiod. PT indicates patient. *Kaiser Permanente–initiated appointment forscreening total-body skin examination.
Table. Characteristics of Subsequent Primary Melanomas by Group
Lesion Group
Breslow Thicknessof Original
Primary Melanoma,Mean, mm
Time LapseBetween
Melanomas,Mean, y
Breslow Thickness,Mean, mm
SPMs Thicker ThanMost Recent Prior
Melanoma, No. (%)
SPMs onNon–Sun-Exposed
Skin, No. (%)
A (n = 40)a 0.48 (� 10 MIS) (� 4d) 3.7 0.35 (� 17 MIS) 9 (23) 25 (63)B (n = 4)b 1.85 (� 3 MIS) 4.6 0.43 3 (75) 4 (100)C (n = 4)c 1.01 (� 1d) 10.1 0.57 1 (25) 2 (50)Total 0.56 (� 13 MIS) (� 5d) 4.4 0.39 (� 17 MIS) 13 (27) 31 (65)
Abbreviations: MIS, melanoma in situ (for which no Breslow thickness is available); TBSE, total-body skin examination; SPM, subsequent primary melanoma.aPatient not overdue for TBSE; patient unaware of lesion.bPatient overdue for TBSE; patient unaware of lesion.cPatient not overdue for TBSE; patient aware of lesion.dNumber of melanomas other than MIS with unknown Breslow thickness.
JAMA DERMATOL/ VOL 149 (NO. 3), MAR 2013 WWW.JAMADERM.COM365
©2013 American Medical Association. All rights reserved.
Downloaded From: on 06/22/2018

detected, which correlates with the 90% rate in our study.Given the high number of SPMs diagnosed in our patientpopulation over 13 months, at least annual TBSEs for pa-tients with a history of melanoma seems advisable.
Breslow thicknesses of SPMs detected throughscreening examinations are usually thinner than theinitial melanomas, but a substantial minority (up to30%) are thicker.3 Similarly, in our study, 50% of SPMswere thinner, while 27% were thicker than the most re-cent prior melanomas. This suggests that routine TBSEslead to earlier detection of melanomas, thinner Breslowmeasurements, and therefore improved overall patientsurvival.
This study evaluated the effect of screening TBSEs onshort-term disease detection rates in a high-risk popu-lation but did not address long-term effects on patientoutcomes or cost-effectiveness. Incidence of SPM in thisstudy is likely increased due to enhanced screening ef-forts.4 The utility of screening TBSEs in a low-risk pa-tient population was not addressed. Furthermore, Kai-ser Permanente patients may be more amenable to regularpreventive health screenings. For dermatology prac-tices without an EHR, a manual spreadsheet of patientswith melanoma could be created to track annual fol-low-up visits.
In conclusion, this study lends further support to thehypothesis that annual TBSEs for patients with a historyof melanoma leads to the detection of asymptomatic dis-ease. Using an EHR to identify high-risk patients who aredue or overdue for annual TBSEs leads to earlier detec-tion of second primary melanomas and increases pa-tient survival.
Accepted for Publication: August 21, 2012.Author Affiliations: Departments of Dermatology (DrReisenauer), Nephrology (Dr Lee), and Pathology (MrTabacchini), Hawaii Permanente Medical Group, Ho-nolulu, Hawaii; and University of Hawaii John A. BurnsSchool of Medicine, Honolulu (Drs Akamine andGolden).Correspondence: Dr Reisenauer, Kaiser Permanente, 80Mahalani St, Wailuku, HI 96793 ([email protected]).Author Contributions: Dr Reisenauer had full access toall of the data in the study and takes responsibility forthe integrity of the data and the accuracy of the data analy-sis. Study concept and design: Reisenauer. Acquisition ofdata: Reisenauer, Lee, Akamine, Tabacchini, and Golden.Analysis and interpretation of data: Reisenauer, Lee, Aka-mine, and Golden. Drafting of the manuscript: Lee, Aka-mine, Tabacchini, and Golden. Critical revision of themanuscript for important intellectual content: Reisenauer,Lee, Akamine, and Golden. Statistical analysis: Lee.Administrative, technical, and material support: Lee andTabacchini. Study supervision: Reisenauer.Conflict of Interest Disclosures: None reported.
1. DiFronzo LA, Wanek LA, Elashoff R, Morton DL. Increased incidence of sec-ond primary melanoma in patients with a previous cutaneous melanoma. AnnSurg Oncol. 1999;6(7):705-711.
2. Howlader NA, Krapcho M, Neyman N, et al. SEER Cancer Statistics Review,1975-2008. http://seer.cancer.gov/csr/1975_2008/. Accessed July 16, 2011.
3. Titus-Ernstoff L, Perry AE, Spencer SK, et al. Multiple primary melanoma:two-year results from a population-based study. Arch Dermatol. 2006;142(4):433-438.
4. Waldmann A, Nolte S, Weinstock MA, et al. Skin cancer screening partici-pation and impact on melanoma incidence in Germany: an observational studyon incidence trends in regions with and without population-based screening.Br J Cancer. 2012;106(5):970-974.
5. Brobeil A, Rapaport D, Wells K, et al. Multiple primary melanomas: implica-tions for screening and follow-up programs for melanoma. Ann Surg Oncol.1997;4(1):19-23.
COMMENTS AND OPINIONS
Smoking, a Dangerous Habit for the Skin
W e are all acutely aware of the causal associa-tion of UV radiation exposure and skin can-cers, and we warn our patients about the haz-
ards of sun exposure. In the August issue of this journal,Leonardi-Bee et al1 published an important systematic re-view and meta-analysis on the effects of smoking on therisk of nonmelanoma skin cancer. Their study clearly dem-onstrated that smoking increases the risk of cutaneoussquamous cell carcinoma, although it does not appearto modify the risk of basal cell carcinoma. Verkouterenand Nijsten,2 in commentary published in the same is-sue, shed light on the practical implications of the find-ings and explain how they translate into clinical prac-tice. The authors of this comment justifiably urge us totake advantage of this association and “collaborate withsmoking cessation programs as an element of good pa-tient care,”2 suggesting that “physicians could make useof the current cancer experience in motivating patientsto discontinue smoking, which has many additional im-portant health benefits.”2
I would like to raise another point that I believe willbe even more alarming to the smoking public, who, inspite of our efforts to promote our antismoking cam-paign, appear not to be deterred by the threats of cancerand death. As dermatologists, we are “lucky” to possesswhat may be even more convincing reasons and moti-vations for supporting the antismoking campaign. We pro-pose that, for many smokers, particularly the young ones,the evidence that smoking is associated with irrevers-ible aesthetic damage (ie, premature aging and wrin-kling of the skin and discoloring of the teeth3) and del-eterious effects on male sexual potency4 will be much morecompelling than the proof that smoking can cause skincancer and kill. One glance at the figures of how muchis spent on fillers for wrinkles and teeth-whitening pro-cedures is enough to reveal what the public really caresabout. As such, we dermatologists are armed with ex-tremely potent ammunition in the war against smoking,and we should use it to the fullest. Articles such as theanalysis of Leonardi-Bee et al1 and the comments of Verk-outeren and Nijsten2 are a most welcome addition to ourarmamentarium.
Amy Reisenauer, MDBrian J. Lee, MDKristie Akamine, MDMichael Tabacchini, CT(ASCP)Spring Golden, MD
Ronni Wolf, MD
JAMA DERMATOL/ VOL 149 (NO. 3), MAR 2013 WWW.JAMADERM.COM366
©2013 American Medical Association. All rights reserved.
Downloaded From: on 06/22/2018