Embed Size (px)
Citation preview
KIDNEY FUNCTION TESTSRamzi Shawahna, PhD
An-Najah National University, Nablus

CHAPTER OUTLINES
Kidney function testing Urea, Creatinine, Cystain C, and the concepts
of GFR Urine analysis Creatinine, proteins and urine protein
electrophoresis. Renal diseases Interpretation of kidney function testing and
determination of renal diseases. Pre-renal, renal (tubular, glumular, or both), and post-renal disease

3
• A major part of homeostasis is maintaining the composition, pH, and volume of body fluids within normal limits
• The urinary system removes metabolic wastes and substances in excess, including foreign substances like drugs and their metabolites that may be toxic
• The urinary system consists of a pair of kidneys, a pair of ureters, a urinary bladder and a urethra
INTRODUCTION

4
Copyright © The McGraw-Hill Companies, Inc.
Kidney
Hilum
Ureters
Urethra
Renalvein
Renalartery
Inferiorvena cava
Abdominalaorta
Urinarybladder
Copyright © The McGraw-Hill Companies, Inc.
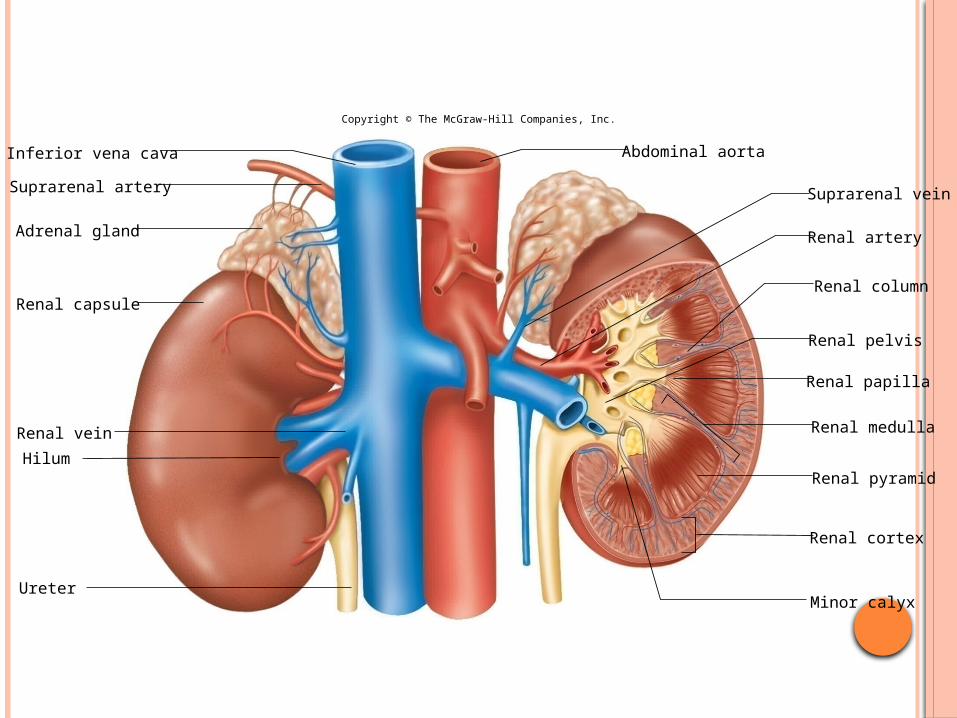
Copyright © The McGraw-Hill Companies, Inc.
Inferior vena cava
Renal cortex
Renal pyramid
Renal medulla
Minor calyx
Renal column
Renal papilla
Renal pelvis
Suprarenal artery
Abdominal aorta
Adrenal gland
Renal capsule
Hilum
Renal vein
Suprarenal vein
Ureter
Renal artery

6
Copyright © The McGraw-Hill Companies, Inc.
Glomerulus
Collecting duct
Nephronloop Ascending
limb
Descendinglimb
Peritubularcapillary
Efferentarteriole
Proximalconvolutedtubule
Renalmedulla
Renalcortex
Cortical radiateartery
Cortical radiatevein
Glomerularcapsule
Afferentarteriole
Distal convolutedtubule
From renalartery
To renalvein
NEPHRON

7
• The main function of the kidneys is to regulate the volume, composition, and pH of body fluids
• The kidneys remove metabolic wastes from the blood and excrete them to the outside of the body, including nitrogenous and sulfur-containing products of protein metabolism
• The kidneys also help control the rate of red blood cell production, regulate blood pressure, and regulate calcium ion absorption
•Endocrine function: 1- erythropoietin production 2- activation of vitamin D 3- renin-angiotensin production
• Urine contains wastes, excess water, and electrolytes
• Urine is the final product of the processes of:
• Glomerular filtration
• Tubular reabsorption
• Tubular secretion
FUNCTION OF THE KIDNEYS

ENDOCRINE FUNCTION OF THE KIDNEY

WHY TEST RENAL FUNCTION?
To asses the functional capacity of kidney Early detection of possible renal impairment Severity and progression of the impairment Monitor response to treatment Monitor the safe and effective use of drugs
which are excreted in the urine

WHEN?
Older age Family history of Chronic Kidney disease (CKD) Decreased renal mass Low birth weight Diabetes Mellitus (DM) Hypertension (HTN) Autoimmune disease Systemic infections Urinary tract infections (UTI) Nephrolithiasis Obstruction to the lower urinary tract Drug toxicity

WHAT?
Renal function tests are divided into the following:
Urine analysis Blood examination Glomerular Function Test Tubular Function Test

URINE

URINE
Color: pale yellow r due to pigments urochrome, urobilin and uroerythrin
Cloudiness: cellular material or protein, crystallization or precipitation of salts
Volume: 1-2.5 L/day (anuria, oliguria, polyuria)
Specific gravity: 1.001- 1.040 pH: 4.5 to 8 (normally it is slightly acidic lying
between 6 – 6.5).

GLOMERULAR FUNCTION Plasma is filtered by glomeruli @ 140 mL/min. The glomerular filtrate has the same composition as the
plasma without most of the proteins. Normal glomerular filtration rate (GFR) depends on:
Blood flow and pressure Body size Higher in men than women Decline in elderly
Impaired renal function is indicated by higher levels of some metabolites like creatinine and urea.
Creatinine is a breakdown product of creatine phosphate in muscle, and is usually produced at a fairly constant rate by the body depending on muscle mass
Creatinine is filtered but not reabsorbed in kidney Urea is major nitrogenous end product of protein and amino
acid catabolism, produced by liver and distributed throughout intracellular and extracellular fluid

CLEARANCE Amount of substance cleared from a volume of plasma over a period
of time
Volume of plasma cleared of “S” = (urine conc. of a substance S per L of plasma X volume of urine collected in a given time period)/(plasma conc of S)
Creatinine is a product of muscle metabolism is collected over a period of 24h and used to measure GFR
GFR is dependent on: Volume collection accuracy Ketones and heavy proteinuria

SERUM CREATININE AND UREA
Serum creatinine conc. is often used as convenient but insensitive
60-120 μmol/L


RENAL TUBULAR FUNCTION
Clearing the body from waste and toxic products
Water, sodium, glucose, and amino acids are reabsorbed
180 L of fluids pass and >90% is recovered Efficient clearance of waste products and
efficient reabsorption of essential consitiuents ensure prober renal functioning

INVESTIGATION OF TUBULAR FUNCTION
Osmolality: the number of moles of solute in 1 kg of solvent
Inability to concentrate urine: Intact tubular function and presence of
arginine vasopressin (AVP) ensure water reabsorption
The osmolality of urine is compared to that of plasma (ratio range 1-3), urine is more concentrate than plasma

WATER DEPRIVATION TEST
To understand the reasons behind polyuria WDT is conducted which involves depriving the patient from water for a period of 24h and measuring uring osmolality during the second 12h

Osmolality >700 mmol/kg should be attained and urine to plasma osmolality ratio of ≥2
In diabetes insipidus (AVP is lacking): ratio 0.2-0.7
In some hospitals patients are restricted from water from 8:00 pm till 10:00 am
Test is unpleasant and should be discontinued if more than 3L of urine lost

ACID LOAD TEST
Diagnosis of renal tubular acidosis: metabolic acidosis due to reduced tubular secretion of hydrogen ions.
Ammonium chloride is administered PO and urine is collected for 8h
In normal renal function: a sample pH should be 5.3 Type I: defective hydrogen ion excretion Type II: reduced capacity to reabsorb bicarbonate Type III: a pediatric variant of type I Type IV: impaired bicarbonate reabsorption due to
aldosterone deficiency, aldosterone receptor defect, or a drug that interfere with aldosterone actions

PROTEINURIA
The glomerular basement membrane does not usually allow passage of albumin and large proteins
A small amount of protein 25 mg/day

SPECIFIC PROTEINURIA: CAUSES

GLYCOSURIA Presence of glucose in urine when the glucose levels
in blood are normal Reflects inability of tubules to reabsorb glucose
Presence of amino acids in the urine Indicate excessive blood conc, reabsorption failure,
metabolic disorders or tubular damage
Describes occurrence of generalized tubular defects as renal tubular acidosis, aminoaciduria, tubular proteinuria.
Heavy metal poisoning, toxins, or cystinosis
AMINOACIDURIA
FANCONI SYNDROME

BILIRUBIN
In blood conjugated and unconjugated Conjugated is water soluble Bilirubinuria is the presence of conjugated
bilirubin in urine Bilirubin is secreted in the bile and
reabsorbed in the gut through enterohepatic circulation
Urobilinogen: conjugated bilirubin is broken in the gut to urobilinogen which is present in the circulation

KETONES
Ketones are products of fatty acid breakdown Indicates that the body is using fat instead of
glucose
Presence of blood and leucocytes in urine indicates acute urinary tract inflammation
Presence of blood may indicate malignancy
BLOOD AND LEUCOCYTES

RENAL STONES
Types: Calcium phosphate: hyperthyrodism or renal
tubular acidosis Magnesium, ammonium and phosphate:
urinary tract infection Oxalate: hyperoxaluria Uric acid: hyperuricaemia Cystine: inherited metabolic disorder
(cystinuria)

RENAL FAILURE
Renal failure is the cessation of kidney function.
It can be acute or chronic. In the acute type, kidneys fail over a period of hours or days while in chronic it develops over months or years and eventually leads to end stage failure.
Acute failure can be reversed whereas chronic is irreversible

CLASSIFICATION: ACUTE

PRE-RENAL
Decreased plasma volume: e.g. bleeding Diminished cardiac output Local factors like occlusion of renal artery
Findings:
Elevated serum urea and creatinine levels Metabolic acidosis Hyperkalaemia High urine osmolality

POST-RENAL
Renal stones Carcinoma of cervix, prostate or bladder
Acute blood loss Severe trauma Septic shock renal diseases like glomerulonephritis Nephrotoxins like aminoglycosides or
analgesics
ACUTE TUBULAR NECROSIS

MANAGEMENT OF RENAL FAILURE
Correction of pre-renal factors Treatment of underlying disease Biochemical monitoring Dialysis

CHRONIC: PROGRESSIVE AND IRREVERSIBLE
Sodium and water metabolism: may retain ability to reabsorb sodium but not water
Potassium metabolism: hyperkalaemia Metabolic acidosis Calcium and phosphate metabolism Erythropoietin synthesis


MANAGEMENT
Water and sodium intake balance Ion exchange resins (Resonium A) for
hyperkalaemia Aluminum or magnesium salts to sequester
phosphate ingestion in the gut Hydroxylated vitamin D to prevent secondary
hypothyroidism Protein restriction Dialysis Renal transplantation






























