Embed Size (px)
Citation preview

Epilepsy & Behavior 28 (2013) S40–S44
Contents lists available at SciVerse ScienceDirect
Epilepsy & Behavior
j ourna l homepage: www.e lsev ie r .com/ locate /yebeh
Review
Juvenile myoclonic epilepsy — Neuroimaging findings
Matthias J. Koepp a,⁎, Friedrich Woermann c, Ivanka Savic d, Britta Wandschneider b
a Department of Clinical Experimental Epilepsy, Institute of Neurology, University College London, London, UKb Epilepsy Society MRI-Unit, Epilepsy Society, Chalfont St Peter, UKc Bethel Epilepsy Center, Mara Hospital, Bielefeld, Germanyd Department of Clinical Neuroscience, Karolinska Institute, Stockholm, Sweden
⁎ Corresponding author at: UCL Institute of NeuroloWC1N 3BG, UK.
E-mail address: [email protected] (M.J. Koepp).
1525-5050/$ – see front matter © 2012 Elsevier Inc. Allhttp://dx.doi.org/10.1016/j.yebeh.2012.06.035
a b s t r a c t
a r t i c l e i n f oArticle history:Accepted 28 June 2012
Keywords:Functional magnetic resonance imagingIdiopathic generalized epilepsyJuvenile myoclonic epilepsyJMEPositron emission tomographyProton magnetic resonance spectroscopyQuantitative magnetic resonance imaging
Juvenile myoclonic epilepsy (JME) has been classified as a syndrome of idiopathic generalized epilepsy and ischaracterized by specific types of seizures, showing a lack of pathology using magnetic resonance imaging(MRI) and computed tomography scanning. However, JME is associated with a particular personality profile,and behavioral and neuropsychological studies have suggested the possible involvement of frontal lobedysfunction. The development of highly sensitive neuroimaging techniques has provided ameans of elucidatingthe underlying mechanisms of JME.Positron emission tomography demonstratedmetabolic and neurotransmitter changes in the dorsolateral prefron-tal cortex reflecting the particular cognitive andbehavioral profile of JMEpatients. 1H-magnetic resonance spectros-copy has shown evidence of thalamic dysfunction, which appears to be progressive. Such techniques provideevidence of multi-focal disease mechanisms, suggesting that JME is a frontal lobe variant of a multi-regional,thalamocortical ‘network’ epilepsy, rather than a generalized epilepsy syndrome. Quantitative MRI revealed signif-icant abnormalities of cortical graymatter inmedial frontal areas close to the supplementarymotor area and diffu-sion abnormalities with increased functional coupling between the motor and prefrontal cognitive systems. Thisaltered structural connectivity of the supplementary motor area provides an explanatory framework for theparticular imaging findings, seizure type, and seizure‐provoking mechanisms in JME.
This article is part of a supplemental special issue entitled Juvenile Myoclonic Epilepsy: What is it Really?© 2012 Elsevier Inc. All rights reserved.
1. Introduction
Juvenile myoclonic epilepsy (JME) is characterized by myoclonicjerks, generalized tonic-clonic seizures, and, less frequently, absenceseizures, with a typical sleep and wake pattern in relationship to sei-zures. The seizures may be precipitated by a variety of stimuli, includ-ing sleep deprivation, fatigue, alcohol intake, menses and stress, butmore specifically following complex cognitive tasks, described aspraxis-induction. Thalamocortical dysfunction is considered to be themajor mechanism of JME, and, as with other IGE syndromes, JME is de-fined by electrophysiological features that show involvement of bothcerebral hemispheres from the beginning of seizures. According to thecriteria of the International League Against Epilepsy, structural brain ab-normalities usingmagnetic resonance imaging (MRI) and computed to-mography (CT) are not found in JME.
Juvenile myoclonic epilepsy is associated with normal intelligence.However, it has been noted that JME is associated with a particularpersonality profile, and behavioral and neuropsychological studies
gy, 33 Queen Square, London
rights reserved.
have suggested subtle frontal lobe dysfunction. Moreover, neuropath-ological studies have provided evidence of microdysgenesis in IGE,in the form of cortical and subcortical dystopic neurons and othermicroscopic structural abnormalities.
The development of highly sensitive neuroimaging techniqueshas allowed the identification of subtle functional and structural ab-normalities, providing a means of elucidating the underlying mecha-nisms of JME and the relative contribution of focal versus generalizeddysfunction.
2. Neuroimaging in JME
2.1. Positron emission tomography
Positron emission tomography (PET) allows the tomographicdelineation of cerebral structures and the measurement of tissue con-centrations of injected radioactive tracers at the molecular level andmay be performed when the subject is at rest or during or followingthe occurrence of a seizure, the undertaking of a cognitive or motortask, or the administration of a drug. A study using PET and bolus in-jections of H2
15O was used to measure cerebral blood flow in patientswith IGE and a history of absence seizures [1]. It showed that in
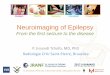
Fig. 1. Late uptake images. 11C‐WAY-100635 in a patient with juvenile myoclonicepilepsy (JME) and control. The images illustrate low uptake in the hippocampus andraphe in the patient. The patient's right side is to the left in the image.
S41M.J. Koepp et al. / Epilepsy & Behavior 28 (2013) S40–S44
addition to a global increase in cerebral blood flow during absenceseizures, there was a significant focal increase in thalamic bloodflow, providing evidence that the thalamus plays a key role in thepathogenesis of typical absence seizures.
Swartz and colleagues [2] performed a 18FGD-PET study using a vi-sual working memory paradigm in nine JME patients and 14 controls.Pairs of abstract images were presented and subjects had to indicateby pressing a button whether the images were matching or not.Defined by the delay between the two images, two conditions werecreated: the immediate match to sample task (IMS), with an imagedelay of 100 ms, controlled for attention, motivation, motor function,and habituation, whereas the delayed match to sample task (DMS;delay 8000 ms) evaluated the visual workingmemory. Two categoriesof mistakes (match-on-mismatch and mismatch-on-match) were re-corded as well as reaction times for correct and incorrect answers.The JME patients' performance was comparable to controls on the IMStask but impaired during the working memory condition. Consideringpossible confounders, groups showed no significant age difference.The authors concluded that dysfunctional thalamo-fronto-cortical net-works might account for both ictogenesis and poor working memoryperformance.
At resting state, 18FDG uptake in patients was decreased in theventral premotor cortex, caudate, the dorsolateral prefrontal cortex(DLPFC) bilaterally, and the left premotor area, representing wide-spread frontal impairment. Controls activated areaswhich are thoughtto support working memory function, whereas patients presentedwith a “hypofrontality state” in keeping with poorer performance inthe DMS task. Increased metabolism of the lateral orbital and medialtemporal regions was interpreted as compensatory mechanisms forprefrontal dysfunction.
In a resting FDG-PET study [3], regional cerebral rates of glucoseuptake values (rCMRGlc) were regressed on various executive func-tion test scores in patients with frontal lobe epilepsy (FLE; n=18),JME (n=10), and healthy controls (n=14). The executive functionbattery included measures of cognitive flexibility, fluency, responseinhibition, working memory, and sustained attention. In the JMEgroup, frontal hypometabolic values predicted impairment on mea-sures of figural fluency and cognitive flexibility.
Flumazenil (FMZ), a specific, reversibly bound, high-affinity neu-tral antagonist of cBZR, can be 11C-labeled and used with PET to pro-vide a marker for the integrity of γ-amino butyric acid (GABA)— theprincipal inhibitory neurotransmitter in the brain. A study using11C-FMZ-PET demonstrated that GABAA–cBZR binding is globally in-creased in the cerebral cortex of patients with JME and other formsof IGE [4]. Frontal lobe GABAA–cBZR binding was particularly elevat-ed in patients with JME but not in patients with other forms of IGE[5].
At a neurotransmission level, evidence exists that serotonergicprocesses may be involved in the pathophysiology of myoclonus. Inhuman subjects, serotonin 1A receptor binding can be examined invivo with positron emission tomography (PET) and the radioligand11C‐WAY-100635. Testing the hypothesis that JME may be associatedwith a disturbance (a hyperreactivity) of serotonergic neurons, leadingto altered serotonin 1A receptor binding, Meschaks et al. [6] observedreduced WAY-100635 binding potential in the dorsolateral prefrontalcortex, raphe nuclei, and hippocampus, but not motor cortex (Fig. 1).The observed reductions in serotonin 1A receptor binding suggest thatthe serotonin system is affected in JME, although provide no definitiveinformation about underlying mechanisms.
Based on previous data showing that the dopamine system isinvolved in motor as well as cognitive functions, Ciumas et al. [7]investigated the binding potential to the dopamine transporter(DAT) in the midbrain, substantia nigra, caudate, and putamen, andif such changes are linked to dysfunctions in 12 patients with JMEcompared to 12 healthy controls. Dopamine signaling seemed im-paired in the target regions for dopaminergic neurons with reduced
binding potential in the substantia nigra and midbrain (p=0.009and 0.007), but normal values in the caudate and putamen.
In a second study of Ciumas et al. [8], JME patients were comparedwith patients with epilepsy with generalized tonic-clonic seizures(GTCS) only. Both patient groups showed a reduced BP compared tocontrols, albeit in different locations. Juvenile myoclonic epilepsy pa-tients had a lower tracer binding than controls in the midbrain(0.8+/−0.1 vs. 1.0+/−0.2, p=0.019), whereas GTCS patients hadreduced tracer binding in the putamen (5.9+/−1.6 vs. 7.1+/−1.2,p=0.023). While GTCS patients showed impaired performance inmotor functions and on one test of executive function, JME patientsperformed poorly also in tests of working memory and several testsof executive function. Alterations in the DA system seem to exist inboth GTCS and JME. However, the regional distribution of thesechanges differs between the two syndromes, as does their associationwith psychomotor and working memory performance.
2.2. Proton magnetic resonance spectroscopy
Whereas conventional MRI provides structural information basedon signals from water protons, proton magnetic resonance spectros-copy (1H-MRS) provides information on the chemical compositionof the brain. Since N-acetyl aspartate (NAA) is found exclusively inneurons and neuronal processes, a reduction in the level of NAA canbe an indication of neuronal damage or dysfunction [9].
Using this technique, thalamic NAA concentrations were found tobe significantly lower in IGE patients than in controls [10]. VolumetricMRI did not identify a significant loss in thalamic volume in thesepatients, indicating thalamic neuronal dysfunction, rather than loss,in agreement with previous neuropathological studies [11]. More-over, a negative correlation was found between NAA levels and dura-tion of epilepsy, indicating that thalamic dysfunction in IGE may beprogressive.
Proton magnetic resonance spectroscopy has indicated that NAAlevels are reduced in the thalami of JME patients, supporting theidea that thalamic dysfunction is part of the underlying mechanismof epileptogenesis in JME [12].
However, 1H-MRS has also demonstrated that patients withJME have significantly reduced prefrontal concentrations of NAA,compared with controls, demonstrating that prefrontal cerebral

S42 M.J. Koepp et al. / Epilepsy & Behavior 28 (2013) S40–S44
changes – neuronal in origin – also exist in JME [13,14]. This findingseems to be specific to JME, compared with other forms of IGE, suchas pure primarily generalized tonic–clonic epilepsy [15].
In addition, 1H-MRS has revealed frontal lobe metabolite changesin IGE, by demonstrating increased levels of glutamate plus glutamine(GLX), an indication of increased neuronal excitability in this region[14]. Proton magnetic resonance spectroscopy has also demonstratedelevated levels of GLX and GABA in the occipital lobes of patients withIGE [15].
2.3. Functional MRI
Electroencephalography-correlated functional MRI (EEG–fMRI)provides a means of identifying and studying the neural correlates ofspontaneously occurring generalized spike–wave discharges (GSWD).This technique has been used to study a patient with IGE and frequentabsences, demonstrating the reciprocal participation of focal thalamicblood flow increases and symmetrical cortical deactivation, with afrontal maximum time-locked with prolonged runs of GSWD [16].
Subsequently, two EEG–fMRI series, conducted in Australia [17]and Canada [18], have replicated these findings of altered thalamicand cortical blood flow, in larger groups of patients with IGE. In theAustralian series, signal reductions in the posterior cingulate wereobserved in four out of five patients, whereas the Canadian seriesreported a variable, but – in the majority of patients – symmetrical,deactivation in the cortex of both hemispheres, involving the anterioras much as posterior head regions.
A more recent functional imaging study examined 19 JME patientsusing a verbal and non-verbal functional MRI (fMRI) working memo-ry paradigm [19]. During the visuo-spatial paradigm, subjects wereassessed with a modified version of the Sternberg Item RecognitionTest. A virtual grid was presented, holding either a triangle or asquare, and subjects were asked to memorize the positions of theitems within the grid. After an interval, the grid was presentedagain, containing either a triangle or a square. Participants had to de-cide whether one of the symbols had been in the same position in theprevious grid, irrespective of its shape. During the verbal memorytask, phonologically similar letters were shown, either capitalized ornot. During the response condition, a single letter was presented,and subjects had to decide whether it had been shown in the previouscondition, irrespective if capitalized or not. Both groups performedwell on these tasks and no significant group differences were detectedon fMRI activation patterns.
Roebling and colleagues compared patients on valproic acid (VPA)to untreated patients or patients on lamotrigine (LTG) monotherapyrespectively. The VPA group was significantly more impaired, andthe authors concluded that cognitive dysfunction in this cohort is atleast partially caused by medication side-effects, especially of VPA.The authors suggested that these inconsistent findings may indicatea heterogeneous epilepsy syndrome, in which frontal lobe dysfunc-tion is only present in a JME subgroup. However, they acknowledgethat absence of group differences might be caused by a workingmemory task that is not sufficiently challenging.
Vollmar et al. [20] investigated a larger JME population (n=30)with a different and, probably, more challenging working memoryfMRI paradigm. During the task, dots were randomly presented on ascreen. There were three different response conditions: during the“0-back” task, participants were instructed to move a joystick towardthe current position of the dot; in the “1-back” condition to the previ-ous position of the dot; and in the “2-back” condition to its secondprevious position. Patients and controls performed equally well onall three tasks and showed significant fMRI activation of workingmemory networks, after subtracting “0-back” from “1-back” and“2-back” in order to control for the motor component. However, theirfMRI cortical activation patterns differed significantly with increasingtask demand. During the “2-back” condition, the motor cortex and
supplementary motor area (SMA) increasingly co-activatedwith work-ing memory networks in patients.
The authors also described increased functional connectivitybetween the motor system and areas of higher cognitive functionswithin the frontal and parietal lobes. Precipitation of myoclonicjerks by cognitive tasks is a known clinical feature in some JME pa-tients [21]. Therefore, the increased functional connectivity wasinterpreted as possible mechanism for seizures triggered by cognitiveeffort. Regions of cortical hyper-excitability may overlap with areasphysiologically activated during cognitive or motor activities. Hence,a complex task involving several functional cortical systems maysummon a “critical mass of cortex activated” which leads to seizureprecipitation [22]. The abnormal motor cortex co-activation during aworking memory task may represent the functional correlate of thismechanism. In keeping with being the drug of choice, VPA had a ben-eficial effect in JME: abnormal left motor cortex co-activation corre-lated negatively with an increasing daily VPA dose, implying anormalization of function and possibly reflecting the positive effectVPA has on controlling myoclonic jerks.
2.4. Quantitative MRI
Although visual inspection of routine MRI in patients with IGEappears normal, neuropathological autopsy studies have providedevidence of gray and white matter microdysgenesis [11]. QuantitativeMRI can elucidate subtle changes in the ratio of cortical and subcorticalmatter in specified volumes of interest, providing a means of detectingstructural changes not normally visible using high-resolution MRI [23].This technique has been used to demonstrate subtle butwidespread ce-rebral structural changes in patients with IGE [24]. Of the patients withJME included in this study, 40% (8/20) had a significant abnormality ofcerebral structure.
When voxel-based statistical parametric mapping was used toanalyze structural MRI data, patients with JME were shown to havean increase in cortical gray matter in the mesial frontal lobes com-pared with healthy subjects [25]. This objective technique revealedsignificant abnormalities in the cortical gray matter of a quarter(5/20) of the JME patients studied; four of whom had previouslybeen shown to have widespread abnormalities using quantitative MRI.Two patients had bilateral areas of increased gray matter volume: onein the temporal posterior and the other in the mesioparietal region,while three had areas of decreased gray matter volume: two in thefrontopolar area and one in the frontomesial region. For the correct in-terpretation of these voxel-based techniques, it has to be emphasizedthat unilateral or bilateral findings very much depend on the level ofthresholding chosen for the analysis.
Further structural imaging studies in JME repeatedly reported sub-tle changes in the mesial frontal lobe of patients with JME. Morpho-metric studies based on T1‐weighted MRI reported both gray matterdecreases [26] and increases [25]. This may not only reflect changesin image analysis methodology, but also supports the existence ofmicro-structural changes in mesio-frontal regions. This could beshown in a meta-analysis of seven voxel-based morphometric studiesusing Signed Differential Mapping (Fig. 2) (SDM; http://sdmproject.com/).
Pulsipher et al. [27] aimed to investigate the integrity of thalamo‐fronto‐cortical networks in correlation to executive function inrecent-onset JME. 20 newly-diagnosed JME patients (diagnosis withinthe last 12 months) were compared to an epilepsy “control group” of12 patients with recent onset Benign Childhood Epilepsy withCentrotemporal Spikes (BECTS) and 51 healthy controls (first degreecousins). Groups were comparable for gender, duration of epilepsy,and IQ. Due to characteristic ages of onset, JME patients were signifi-cantly older than both BECTS patients and healthy controls, yetno significant correlations between standardized test scores and agewere observed. Participants were assessed with three subtests of the

Fig. 2. Meta-analysis of voxel‐based MRI studies showing increased gray matter inmesio-frontal regions (upper row) and reduced gray matter in perisylvian regionsbilaterally.
S43M.J. Koepp et al. / Epilepsy & Behavior 28 (2013) S40–S44
Delis–Kaplan Executive Function System (D-KEFS) and a parent ques-tionnaire, the Behavior Rating Inventory of Executive Function(BRIEF). Age-adjusted scores demonstrated poorer performance inJME patients than in controls on D-KEFS Inhibition. Behavioral regula-tion and metacognition scores of the BRIEF were also significantlylower in the JME group. Quantitative MRI measurements revealedsmaller thalamic volumes and greater frontal CSF in JME patientsthan in healthy controls and BCECTS patients. Only in the JME group,thalamic and frontal volumes predicted D-KEFS performance. Inter-estingly, JME patients showed volumetric abnormalities already with-in 12 months of seizure onset, suggesting a clinically significantdisruption of the thalamo‐fronto‐cortical circuitry, leading to both sei-zures and neuro-cognitive deficits. How early structural abnormali-ties present in disease evolution remains uncertain, though, in asmuch as the distinct volumetric abnormalities seem to be unlikelythe result of chronic seizures.
2.5. DTI-tractography
In a recent analysis of T1‐weighted MRI and diffusion tensor imag-ing (DTI), we could replicate the finding of decreased mesial frontalgray matter volume and also found a reduced fractional anisotropy(FA) in underlying white matter tracts, which are considered toform the basis for the observed neuropsychological and psychiatricchanges observed in patients with JME [26].
Vollmar et al. [28] investigated the structural segregation ofSMA and preSMA in JME using DTI‐based connectivity fingerprintingand clustering techniques. Patients with JME showed reduced con-nectivity of the anterior SMA cluster to prefrontal and frontopolarareas. Connectivity was increased to the central region, occipitallobe, and descending motor pathways and cerebellum. The posteriorSMA cluster showed relatively decreased connectivity to the primarymotor cortex and increased connectivity to the parietal lobe andtemporal neocortex explaining several imaging findings and clinicalobservations in JME.
3. Conclusions
Sensitive neuroimaging techniques provide qualitative and quanti-tative methods of elucidating the underlying pathological mechanismsinvolved in JME. Although JME has characteristics of a form of general-ized epilepsy, such techniques provide evidence of the involvementof additional, possibly multi-focal disease mechanisms – in particularinvolving the frontal lobes – in accordance with the findings of behav-ioral and neuropsychological studies. Increased functional connectivitybetween prefrontal cognitive areas and the motor system in JME sug-gests that connectivity alterations in the SMA might be the “missinglink” between seizure‐facilitating mechanisms and seizure type. Theincreased connectivity between the anterior cluster, which is part ofthe prefrontal cognitive network, and the central region reflects thestructural basis for increased functional connectivity in these patientsand helps to explain why, why cognitive activity elicits epileptiformdischarges and seizures in these patients. The increased connectivityto the occipital cortex may reflect a pathway, via which photic stimula-tion can elicit discharges and seizures. The reduced connectivity withinthe prefrontal cortex, on the other hand, may be the basis for impairedfrontal lobe functioning in these patients.
Conflict of interest
The authors declare that there are no conflicts of interest.
References
[1] Prevett MC, Duncan JS, Jones T, Fish DR, Brooks DJ. Demonstration of thalamicactivation during typical absence seizures using H2(15)O and PET. Neurology1995;45:1396-402.
[2] Swartz BE, Simpkins F, Halgren E, et al. Visual working memory in primary gener-alized epilepsy: an 18FDG-PET study. Neurology 1996;47:1203-12.
[3] McDonald CR, Swartz BE, Halgren E, Patell A, Daimes R, Mandelkern M. Therelationship of regional frontal hypometabolism to executive function: a restingfluorodeoxyglucose PET study of patients with epilepsy and healthy controls.Epilepsy Behav 2006;9:58-67.
[4] Koepp MJ, Richardson MP, Brooks DJ, Cunningham VJ, Duncan JS. Centralbenzodiazepine/gamma-aminobutyric acid A receptors in idiopathic generalizedepilepsy: an [11C]flumazenil positron emission tomography study. Epilepsia1997;38:1089-97.
[5] Koepp MJ, Duncan JS. Positron emission tomography in idiopathic generalizedepilepsy: imaging beyond structure. In: Schmitz B, Sander T, editors. Juvenilemyoclonic epilepsy: The Janz Syndrome. London: Wrightson; 2000. p. 91-9.
[6] Meschaks A, Lindstrom P, Halldin C, Farde L, Savic I. Regional reductions inserotonin 1A receptor binding in juvenile myoclonic epilepsy. Arch Neurol2005;62(6):946-50.
[7] Ciumas C, Wahlin TB, Jucaite A, Lindstrom P, Halldin C, Savic I. Reduced dopaminetransporter binding in patients with juvenile myoclonic epilepsy. Neurology2008;71(11):788-94.
[8] Ciumas C,Wahlin TB, Espino C, Savic I. Thedopamine system in idiopathic generalizedepilepsies: identification of syndrome-related changes. NeuroImage 2010;51(2):606-15.
[9] Savic I, Lekvall A, Greitz D, Helms G. MR spectroscopy shows reduced frontal lobeconcentrations of N-acetyl aspartate in patients with juvenile myoclonic epilepsy.Epilepsia 2000;41:290-6.
[10] Bernasconi A, Bernasconi N, Natsume J, Antel SB, Andermann F, Arnold DL.Magnetic resonance spectroscopy and imaging of the thalamus in idiopathicgeneralized epilepsy. Brain 2003;126:2447-54.
[11] Meencke HJ, Janz D. Neuropathological findings in primary generalized epilepsy:a study of eight cases. Epilepsia 1984;25:8–21.
[12] Mory SB, Li LM, Guerreiro CA, Cendes F. Thalamic dysfunction in juvenile myo-clonic epilepsy: a proton MRS study. Epilepsia 2003;44:1402-5.
[13] Savic I, Osterman Y, Helms G. MRS shows syndrome differentiated metabolitechanges in human-generalized epilepsies. NeuroImage 2004;21:163-72.
[14] Simister RJ, McLean MA, Barker GJ, Duncan JS. Proton MRS reveals frontal lobemetabolite abnormalities in idiopathic generalized epilepsy. Neurology 2003;61:897-902.
[15] Simister RJ, McLean MA, Barker GJ, Duncan JS. A proton magnetic resonancespectroscopy study of metabolites in the occipital lobes in epilepsy. Epilepsia2003;44:550-8.
[16] Salek-Haddadi A, Lemieux L, Merschhemke M, Friston KJ, Duncan JS, Fish DR.Functional magnetic resonance imaging of human absence seizures. Ann Neurol2003;53:663-7.
[17] Archer JS, Abbott DF, Waites AB, Jackson GD. fMRI “deactivation” of the posteriorcingulate during generalized spike and wave. NeuroImage 2003;20:1915-22.
[18] Aghakhani Y, Bagshaw AP, Benar CG, et al. fMRI activation during spike and wavedischarges in idiopathic generalized epilepsy. Brain 2004;127:1127-44.

S44 M.J. Koepp et al. / Epilepsy & Behavior 28 (2013) S40–S44
[19] Roebling R, Scheerer N, Uttner I, Gruber O, Kraft E, Lerche H. Evaluation of cognition,structural, and functional MRI in juvenile myoclonic epilepsy. Epilepsia 2009;50:2456-65.
[20] Vollmar C, O'Muircheartaigh J, Barker GJ, et al. Motor system hyperconnectivity injuvenile myoclonic epilepsy: a cognitive functional magnetic resonance imagingstudy. Brain 2011;134:1710-9.
[21] Inoue Y, Kubota H. Juvenile myoclonic epilepsy with praxis-induced seizures.Juvenile myoclonic epilepsy. The Janz Syndrome. Petersfield, UK: WrightsonBiomedical Publishing; 2000. p. 73-81.
[22] Ferlazzo E, Zifkin BG, Andermann E, Andermann F. Cortical triggers in generalizedreflex seizures and epilepsies. Brain 2005;128:700-10.
[23] Sisodiya SM, Free SL, Stevens JM, Fish DR, Shorvon SD. Widespread cerebral structuralchanges in patients with cortical dysgenesis and epilepsy. Brain 1995;118:1039-50.
[24] Woermann FG, Sisodiya SM, Free SL, Duncan JS. Quantitative MRI in patients withidiopathic generalized epilepsy. Evidence of widespread cerebral structural changes.Brain 1999;121:1661-7.
[25] Woermann FG, Free SL, Koepp MJ, Sisodiya SM, Duncan JS. Abnormal cerebralstructure in juvenile myoclonic epilepsy demonstrated with voxel-based analysisof MRI. Brain 1999;122:2101-8.
[26] O'Muircheartaigh J, Vollmar C, Barker GJ, et al. Focal structural changes and cogni-tive dysfunction in juvenile myoclonic epilepsy. Neurology 2011;76:34-40.
[27] Pulsipher DT, Seidenberg M, Guidotti L, et al. Thalamofrontal circuitry and execu-tive dysfunction in recent-onset juvenile myoclonic epilepsy. Epilepsia 2009;50:1210-9.
[28] Vollmar C, O'Muircheartaigh J, Barker GJ, et al. Altered microstructural connectiv-ity in juvenile myoclonic epilepsy: the missing link. Neurology 2012;78:1555-9.