Embed Size (px)
Citation preview

Juvenile DermatomyositisJoseph Junewick, MD FACR
10/11/2015
HistoryChild with several month history of weakness, arthralgias and palpable abnormalities at the knee
DiagnosisJuvenile Dermatomyositis
DiscussionJuvenile dermatomyositis (JDM) is a rare multisystem, autoimmune, inflammatory disease of themuscles and the skin. In the United States an average of 3.2 per 1 million children under 17 years olddevelop JDM. More females are affected by JDM than males (>2:1) and have two peak ages fordeveloping JDM (6 and 11 years old) whereas males are more likely to develop JDM before 10 yearsof age. The exact etiology of JDM is unknown but it is thought to be secondary to an environmentaltrigger, such as infection, in genetically predisposed children leading to an autoimmune reaction. It isbelieved that both cell-mediated and humoral components of the adaptive immune system areresponsible for the vascular and muscle damage characteristic of JDM. The diagnostic criteria includesymmetric proximal muscle weakness, a heliotrope dermatitis and Gottron’s papules, elevated muscleenzymes, muscle denervation and myopathy by electromyography, and abnormal findings on musclebiopsy. Many patients with JDM experience arthralgias and arthritis early in the course of the diseasecommonly affecting, but not limited to, the knees.Unique to JDM compared to its adult counterpart is the development of calcinosis cutis in up to 30-70% of patients within the first few years after disease onset. While the cause of calcium deposition inthis disease is still under investigation, it is thought that autoantibodies directed against hostendothelial cells lead to activation of the membrane attack complex and perifasicular muscledestruction by CD4+ T-cells resulting in the release of alkaline phosphate, from lysosomal tissuedestruction, which causes organic phosphates to precipitate with calcium. Calcinosis often occurs atsites of the body prone to trauma, such as the elbows, knees, and buttocks, but does not ossify.There have been four recognized patterns of distribution in JDM with calcinosis occurring as 1)superficial firm, flesh colored nodules in the cutaneous or subcutaneous tissue 2) deep masses, 3)deep linear deposits within fascial planes, and 4) diffuse superficial deposits involving a majority ofthe body surface area. Patients at greater risk for soft tissue calcification include patients withuntreated or poorly controlled disease for any reason, a polycyclic or unremitting disease course. Thedevelopment of calcinosis often causes more morbidity for patients with JDM than the muscleinvolvement.Not only can radiography identify areas and patterns of calcinosis early, which can help predict thedisease course and prognosis, but it can also aid in establishing a diagnosis of JDM in the earlyphases by identifying muscle changes in the acute, inflammatory stage of the disease. MRI revealsedematous muscles, mostly of the arms, thighs, and chest wall, myositis, and elimination of thenormal tissue planes indicative of early JDM. The amount of edema within the muscle tissue can helpestimate the amount of inflammation and the findings on MRI can also help determine ideal musclebiopsy locations. The development of calcifications is associated with a chronic, continuous diseasecourse. As such, the presence or absence and severity of calcinosis on the initial radiographic

studies in a patient undergoing work-up for JDM hints at the disease duration prior to the diagnosticwork-up. Computed tomography (CT) scans and ultrasound are useful in evaluating the presence orabsence of calcification in patients and are very sensitive for identifying early calcifications andidentifying the exact location of the calcinosis. 99m Tc MDP scintigraphy is the most sensitive study toevaluate the total amount of dystrophic calcification for these patients.
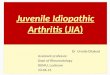
FindingsDR-Numerous globular calcifications, predominantly in the subcutaneous soft tissues.
ReferenceBatthish, M, Feldman, B. Juvenile Dermatomyositis. Current Rheumatology Reports.2011;13:216–224. doi:10.1007/s11926-011-0167-9.Sanyal, S. Radiographic Patterns of Soft Tissue Calcinosis in Juvenile Dermatomyositis and itsClinical Implications. Journal Of Clinical And Diagnostic Research. 2014;8(12):8–11.doi:10.7860/JCDR/2014/10787.5321.ContributorBrooke Boer, MS IV



Sponsored By
DisclaimerThis teaching site is partially funded by an educational grant from GE Healthcare and Advanced Radiology Services, PC. The material on this site isindependently controlled by Advanced Radiology Services, PC, and GE Healthcare and Spectrum Health have no influence over the content of this siteContent Download AgreementThe cases and images on this website are owned by Spectrum Health. Permission is granted (for nonprofit educational purposes) to download and printmaterials to distribute for the purpose of facilitating the education of health professionals. The authors retain all rights to the material and users arerequested to acknowledge the source of the material. Site DisclaimerThis site is developed to reach healthcare professionals and medical students. Nothing this site should be considered medical advice.Only your own doctor can help you make decisions about your medical care. If you have a specific medical question or are seeking medical care, pleasecontact your physician.The information in this website is provided for general medical education purposes only and is not meant to substitute for the independent medicaljudgment of a physician relative to diagnostic and treatment options of a specific medical condition.The viewpoints expressed in these cases are those of the authors. They do not represent an endorsement. In no event will Advanced RadiologyAssociates, PC, Spectrum Health Hospitals (Helen Devos Children's Hospital) or GE Healthcare be liable for any decision made or action taken inreliance upon the information provided through this website.