Embed Size (px)
Citation preview

The Meaning Of Hypokalemia In Heart Failure
AbstractMaintenance of normal potassium (K+) homeostasis has become an increasingly important limiting factor in the therapy of heart failure (HF). With the application of loop diuretics and digoxin, hypokalemia has become a frequent and feared side effect of treatment. Low serum K+ in HF may be also a marker of increased neurohormonal activity and disease progression.
To gain the maximum benefit from treatment, we need to individualize drug use and carefully monitor electrolytes. Symptomatic HF patients (New York Heart Association class III–IV) should be prescribed the lowest dose of diuretic necessary to maintain euvolemia. Mild hypokalemia may be corrected by the use of aldosterone receptor antagonists such as spironolactone or eplerenone. However, a more severe hypokalemia should preferably be corrected using K+
supplement. Serum K levels should be frequently checked and maintained between 4.0 and 5.5 mEq/l (mmol/l).
1. Epidemiology of Hypokalemia in Heart Failure (HF)Congestive heart failure carries a grim prognosis. The 5-year survival
rate is well below 40% [1], with half of the deaths classified as sudden [2,3]. These deaths were probably caused by ventricular arrhythmias or electromechanical dissociation [4–6]. Electrophysiological remodeling is associated with the progression of hypertrophy and heart failure (HF) [7].
Potassium (K+) is an important electrolyte essential for a healthy nervous system and a regular heart rhythm [7,8]. K+ concentration is important in cell metabolism and membrane excitability [8]. Hypokalemia has not been well defined in HF, but in the literature on hypertension, the definition has varied from < 3.5 to < 4.0 mEq/L (mmol/l) [9]. K+ depletion is commonly seen in patients with congestive heart failure, a condition that is characterized by several physiologic abnormalities predisposing to the development of electrolyte disturbances.
2. Etiology and Pathophysiology of Hypokalemia in HFThe sodium-rich diet of modern humans may produce sodium overload
and K+ depletion [10]. Hypokalemia contributes to the pathogenesis of cardiovascular disease, and many cardiovascular disorders and drugs cause hypokalemia [11,12].
Patients with HF may have difficulty with K+ transport into tissues. In patientswith HF, an increase in oxidative stress may result in a defect in Na+/K+-ATPase activity and thus in transport of K+ into tissues. Consequently,
0

tissue levels of K+ may be considerably lower than serum levels, which would place them at increased risk for myocardial fibrosis, hypertrophy, and sudden cardiac death. For example, patients with HF have been found to have a serum K+ level greater than 7.0 mEq/L (mmol/l) without any electrocardiographic changes or clinical manifestations of hyperkalemia because their tissue K+ level was normal or low, as reflected by the red-cell K+ concentration [13]. Thus, it has been suggested that the level of serum K+ should be maintained between 4.5 and 5.5 mEq/L (mmol/l) in patients with HF [14].
Among the pathogenic factors associated with HF are renal dysfunction and neurohormonal activation, which stimulate the renin–angiotensin–aldosterone axis, sympathetic nervous tone, and hypersecretion of catecholamines [15].
Serum K+ is negatively correlated with plasma renin activity and plasma noradrenaline, and patients who respond to treatment show increases in intracellular K+ concentrations [16,17]. Thus, neurohormonal activation contributes markedly to K+ depletion in HF. A drop in intravascular volume, such as that which occurs with left ventricular systolic dysfunction, and reduced cardiac output results in a pathologically elevated aldosterone level. In patients with congestive heart failure, aldosterone may reach plasma levels up to 60 times higher than those measured in normal subjects [18,19].
Cardiomyocytes, blood vessels, and adipocytes have also been shown to synthesize aldosterone [19]. Aldosterone induces sodium and water reabsorption with concomitant K+ excretion. The adverse effects attributed to hyperaldosteronism that may influence cardiovascular function include increased intravascular-fluid retention and volume overload, endothelial dysfunction, impaired vascular reactivity, sympathetic nervous system activation, decreased baroreceptor sensitivity, increased electrolyte excretion (K+ and magnesium ions), and cardiomyocyte apoptosis [18,20,21] (Fig. 1). Low levels of serum K+ in HF may be a marker of increased neurohormonal activity and disease progression [21,22].
Hypokalemia is a frequent and feared side effect of the treatment of HF with loop diuretics and digoxin [23] because the arrhythmogenic potential of digoxin is enhanced by hypokalemia. The main classes of diuretics are the loop diuretics, K+-sparing diuretics, and thiazides. Loop diuretics, the mainstay of acute and chronic therapy for HF, are “threshold drugs”; therefore, a dose adequate to achieve a pharmacodynamic effect must be prescribed [23].
Loop diuretics include the sulfonamide derivatives furosemide, bumetanide, and torsemide, as well as ethacrynic acid, which is used less often. These drugs inhibit the Na+-K+-2Cl−cotransporter (NKCC) in the thick ascending limb of the loop of Henle, which is responsible for reabsorption of
1

20% to 30% of the filtered sodium [24]. Thiazide diuretics, which are the most commonly used of the diuretic class, inhibit the sodium-chloride transporter in the distal tubule. Because this transporter normally reabsorbs only about 5% of filtered sodium, these diuretics are less efficacious than loop diuretics in producing diuresis and natriuresis [24]. Nevertheless, they are sufficiently powerful to satisfy most therapeutic needs requiring a diuretic. Their mechanism depends on renal prostaglandin production [24].
Fig. 1. The effect of impaired left ventricular (LV) function on aldosterone synthesis. A, A decrease in cardiac output as a result of LV systolic dysfunction is perceived as a decrease in efferent renal blood flow. B, This stimulates renin secretion from the juxtaglomerular apparatus. C, In the peripheral circulation, renin cleaves angiotensinogen to angiotensin I (AT I), which is converted to angiotensin II (AT II) by ACE in the pulmonary artery vasculature (D). E, Angiotensin II stimulates the zona glomerulosa in the adrenal cortex to secrete aldosterone. Elevated plasma levels of aldosterone have a number of adverse effects on the cardiovascular system. NO· indicates nitric oxide. (Heart images from U-Write patient education), © 1998 William Fridl, dba U-Write; kidney and glomerulus images from Bill Camelet; blood vessel images from John MacNeil; adrenal gland image reproduced from McGill Molson Medical Informatics Project, McGill University.
Because loop and thiazide diuretics increase sodium delivery to the distal segment of the distal tubule, K+ loss increases (potentially causing hypokalemia). This occurs because the increase in distal tubular sodium concentration stimulates the aldosterone-sensitive sodium pump to increase sodium reabsorption in exchange for K+ and hydrogen ions, which are lost to the urine [25–27].
2

Potentially harmful effects of administration of high doses of loop diuretics are neurohormonal activation of the renin–angiotensin–aldosterone system and increased levels of norepinephrine and arginine vasopressin, both of which are fundamentally involved in the progression of HF [25–27]. In patients with HF it is important to achieve euvolemia that improves patients clinical condition, on the other hand physicians should attempt to lower diuretic doses, when possible, due to the neurohormonal activation of renin–angiotensin–aldosterone system (RAAS).
Administration of loop diuretics may lead to electrolyte imbalances (such as hypokalemia, hyponatremia, and hypomagnesemia) that may exacerbate cardiac arrhythmias and increase the risk of sudden cardiac death [28,29]. In the Studies of Left Ventricular Dysfunction (SOLVD) trial, use of a diuretic was associated with a 37% increase in the risk of arrhythmic death after controlling for multiple other measures of disease severity [28,29].
Still, little is known about the effects of hypokalemia on outcomes in patients with chronic heart failure [30].
3. Effect of Hypokalemia in HFHypokalemia causes cellular hyperpolarity, increases resting potential,
hastens depolarization, and increases automaticity and excitability [31,32]. Because cardiac repolarization relies on K+ influx, hypokalemia lengthens the action potential and increases QT dispersion reflecting electrical inhomogeneity. Most patients with HF have increased ventricular ectopy, and 50% exhibit nonsustained ventricular tachycardia [33]. A total of 50% of deaths from HF are sudden, presumably due to arrhythmias. In victims of sudden cardiac death, the level of myocardial K+ is markedly lower than in controls, and survivors are often hypokalemic [34]. In HF, all-cause and cardiac mortality rates are higher in individuals taking non-K+-sparing diuretics [35]. The incidence of arrhythmic death is significantly and independently related to use of non-K+-sparing diuretics [34,35].
Hypokalemia predisposes a patient to digoxin toxicity by reducing renal clearance and promoting myocardial binding of the drug. This, in turn, produces increased automaticity and ventricular arrhythmias [36,37]. K+
depletion exacerbates diastolic dysfunction in animal and human models [38].The negative effect of hypokalemia in patients with HF has been
reported in clinical studies. The research by Bowling et al. [39] included 7788 patients with chronic heart failure in the Digitalis Investigation Group trial. Of these, 2793 had chronic kidney disease, defined as an estimated glomerular filtration rate (eGFR)<60 mL/min/1.73 m2. Propensity scores for hypokalemia [serum K+, <4 mEq/L (mmol/l)] were used to assemble a balanced cohort of
3

522 pairs of patients with hypokalemia and normokalemia. Death due to all causes occurred in 48% and 36% of patients with hypokalemia and normokalemia, respectively, during 57 months of follow-up (matched hazard ratio when hypokalemia was compared with normokalemia, 1.56; 95% confidence interval [CI], 1.25 to 1.95; P<0.0001). In patients with HF and chronic kidney disease, death from all causes occurred in 47% and 38% of patients with mild hypokalemia [3.5 to 3.9 mEq/L (mmol/l)] and normokalemia, respectively (matched hazard ratio, 1.31; 95% CI, 1.03 to 1.66; P=0.027) [39].
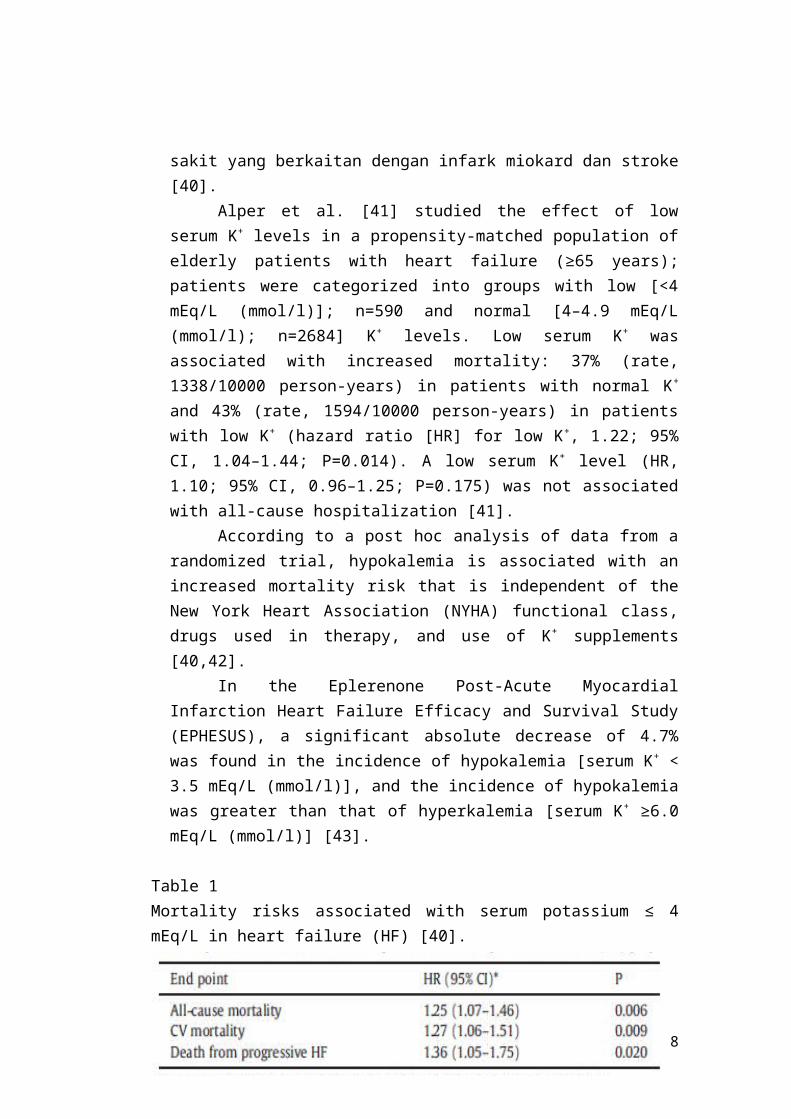
The analysis of Ahmed et al. [40] is based on patients followed for 32 months in the US-Canadian Digitalis Investigation Group (DIG) trial who had K+ levels <5.5 mEq/L (mmol/l). The DIG trial, which predated the recommended use of beta-blockers in HF, enrolled patients with chronic systolic or diastolic HF of any cause. The cohort's 1187 patients with levels of serum K+ < 4 mEq/L (mmol/l) were matched with the same number who had higher levels based on propensity scores encompassing a broad range of demographic, clinical, and treatment-related factors. Nearly all of those features became covariates in an analysis that showed low K+ to be independently associated with increased cardiovascular and all cause mortality, as well as death due to progressive HF (Table 1). Similar but insignificant trends were seen for all-cause, cardiovascular, and hospitalization related to myocardial infarction and stroke [40].
Analisis Ahmed et al. [40] didasarkan pada pasien yang diikuti selama 32 bulan di AS-Kanada Group Investigation Digitalis (DIG) percobaan yang memiliki tingkat K+ < 5.5 mEq /L (mmol/l). Percobaan DIG, yang mendahului rekomendasi penggunaan beta- blocker pada HF, mendaftarkan pasien dengan sistolik kronis atau HF diastolik sebab apapun. Kohort 1.187 pasien dengan kadar serum K+ < 4 mEq/L (mmol/l) yang cocok dengan angka yang sama yang memiliki tingkat yang lebih tinggi berdasarkan skor kecenderungan meliputi berbagai faktor demografi, klinis, dan pengobatan terkait. Hampir semua fitur tersebut menjadi kovariat dalam analisis yang menunjukkan K+
rendah untuk secara independen dikaitkan dengan peningkatan kardiovaskular dan semua penyebab kematian , serta kematian akibat progresif HF (Tabel 1). Tren serupa namun tidak signifikan terlihat untuk semua penyebab, kardiovaskular, dan perawatan rumah sakit yang berkaitan dengan infark miokard dan stroke [40].
Alper et al. [41] studied the effect of low serum K+ levels in a propensity-matched population of elderly patients with heart failure (≥65 years); patients were categorized into groups with low [<4 mEq/L (mmol/l)]; n=590 and normal [4–4.9 mEq/L (mmol/l); n=2684] K+ levels. Low serum K+
4
was associated with increased mortality: 37% (rate, 1338/10000 person-years) in patients with normal K+ and 43% (rate, 1594/10000 person-years) in patients with low K+ (hazard ratio [HR] for low K+, 1.22; 95% CI, 1.04–1.44; P=0.014). A low serum K+ level (HR, 1.10; 95% CI, 0.96–1.25; P=0.175) was not associated with all-cause hospitalization [41].
According to a post hoc analysis of data from a randomized trial, hypokalemia is associated with an increased mortality risk that is independent of the New York Heart Association (NYHA) functional class, drugs used in therapy, and use of K+ supplements [40,42].
In the Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS), a significant absolute decrease of 4.7% was found in the incidence of hypokalemia [serum K+ < 3.5 mEq/L (mmol/l)], and the incidence of hypokalemia was greater than that of hyperkalemia [serum K+ ≥6.0 mEq/L (mmol/l)] [43].
Table 1Mortality risks associated with serum potassium ≤ 4 mEq/L in heart failure (HF) [40].
Results are expressed as hazard ration (HR) and 95% confidence interval (CI).*Adjusted for demographics, HF etiology, cardiovascular diseases, diabetes, medications (including digoxin, ACE inhibitors, diuretics), use of potassium-sparing diuretics, potassium supplementation, HF signs and symptoms, NYHA functional class, chest Xray findings and serum creatinine.
Although many clinicians have become concerned about the risk of hypokalemia only when the level of serum K+ is <3.5 mEq/L (mmol/l), a recent analysis of the National Heart, Lung, and Blood Institute's Digitalis Investigation Group trial showed an increased risk of both sudden cardiac death and progressive HF in patients with a serum K+ level < 4.5 mEq/L (mmol/l), regardless of the use of K+ supplements [44].
This relationship of decreased serum K+ [< 4.4 mEq/L (mmol/l)] as an independent predictor of sudden cardiac death in patients with HF has been demonstrated in other studies. In the United Kingdom Heart Failure Evaluation and Assessment of Risk Trial, Nolan et al. found that low serum K+ levels were related to sudden cardiac death (n=433) [45].
5
Leier et al. [46] have recommended maintaining serum K+ levels in the range of 4.5 to 5.0 mEq/L (mmol/l). The importance of preventing hypokalemia is underscored by the finding that the risks of dysrhythmias, syncope, cardiac arrest, or death are greater in patients with HF. This result may be due in part to the cells of hypertrophied and failing hearts often having prolonged action potential duration, which in most cases is caused by a decrease in outward K+ currents [46].
4. Prevention and Treatment of Hypokalemia in HFThe combination drug therapy may simultaneously improve clinical
outcomes while it enhances the risk of K+-related adverse events [47]. The K+-sparing diuretics are important in preventing hypokalemia in HF [47].
The K+-sparing diuretics include spironolactone and eplerenone. Unlike loop and thiazide diuretics, these drugs do not act directly on sodium transport. Some drugs in this class antagonize the actions of aldosterone (aldosterone receptor antagonists) at the distal segment of the distal tubule, which cause more sodium (and water) to pass into the collecting duct and be excreted in the urine. By inhibiting aldosterone-sensitive sodium reabsorption, fewer K+ and hydrogen ions are exchanged for sodium by this transporter, and therefore, less K+ and hydrogen are lost via the urine. Other K+-sparing diuretics directly inhibit sodium channels associated with the aldosteronesensitive sodium pump, and therefore, they have similar effects on K+ and hydrogen ions as aldosterone antagonists [47]. Their mechanism depends on renal prostaglandin production [47]. Aldosterone blockade is effective in reducing death from all causes in patients after myocardial infarction complicated by left ventricular dysfunction and HF. The use of aldosterone blockade in these patients has been recognized as a class 1 indication in both U.S. and European guidelines [47].
The positive influence of these drugs is connected with their ability to inhibit the adverse effect of hyperaldosteronism in patients with HF (Fig. 1) [48,49].
Spironolactone is a nonselective aldosterone receptor antagonist that is metabolized extensively in the liver to its active metabolite and is structurally similar to progesterone, thereby allowing sex-steroid receptor cross-reactivity [50]. This phenomenon accounts for the antiprogesterone and antiandrogen effects observed in some patients treated with spironolactone [50].
In the pre-RALES (The Randomized Aldactone Evaluation Study) pilot study, [51] in 214 patients a dose response in the incidence of hyperkalemia defined as serum K+ > 5.5 mEq/l (mmol/l) was assessed in 4 groups treated with spironolactone in doses of 12.5, 25, 50 and 75 mg. The incidence of hyperkalemia was 5, 13, 20 and 24%, respectively, and predictors for the
6

development of hyperkalemia were the use of angiotensin-converting (ACE) inhibitors and a baseline elevation of K+ or creatinine. The treatment was considered safe, provided that serum K+ levels were monitored closely [51].
The RALES investigators performed a safety study regarding the use of spironolactone in patients in NYHA class III to IV with left ventricular systolic dysfunction. Of note, 10% of the patients in the control group in this study presented with hypokalemia [52].
In contrast, those patients assigned to receive 50 or 75 mg of spironolactone had no episodes of hypokalemia, and there was just one episode in those receiving 25 mg/day. This study showed a significant reduction in mortality of approximately 30%. Subgroup analysis showed similar improvement in mortality rates regardless of the creatinine or K+ concentration or the use of K+ supplements [52].
The positive experience in clinical trials contrasts with several reports of cases of serious hyperkalemia in patients given with spironolactone for chronic heart failure in clinical practice, some of which were associated with increased hospital admissions and death [53–55].
The occurrence of hyperkalemia in these trials may have been related to the higher doses used in this study [56] compared to those in the reference trials, EPHESUS and RALES. In clinical practice, patients are often older than in randomized trials andmay have a reduced eGFR that is not reflected by the level of serum creatinine, because serum creatinine is an inaccurate measure of true kidney function in the elderly [56].
During aldosterone antagonist treatment one should assess renal parameters and electrolyte concentration optimally after 1 week and then 4 weeks after treatment initiation; after an optimal dosage of the drug is established, measurements should be obtained at 1, 2, 3 and 6 months, and afterwards every 6 months [57]. It is recommended that whenever a change in electrolyte status is suspected, such as during an episode of vomiting or diarrhea or at initiation or dosage adjustment of concomitant diuretic therapy, serum K+ levels should be remeasured or the aldosterone blocker withheld until such measurement is possible [58].
Eplerenone is a selective aldosterone receptor antagonist derived from spironolactone, but because of its limited affinity for the progesterone and androgen receptors, it lacks sex-related adverse side effects [50].
In the EPHESUS trial [56], the selective aldosterone blocker eplerenone (25 to 50 mg/d) significantly reduced all-cause mortality (15%; P=0.008) and cardiovascular mortality or hospitalization (13%; P=0.002) when used in addition to standard therapy in patients with left ventricular systolic dysfunction, a left ventricular ejection fraction ≤40%, and HF after acute
7
myocardial infarction. Additionally, it reduced hospitalization for HF (15%; P=0.03) and sudden cardiac death (21%; P=0.03). Patients were excluded if the baseline K+ was < 5.0 mEq/L or serum creatinine was < 2.5 mg/dL (221.0 μmol/l).
A subanalysis of the EPHESUS study examined the relationship between eplerenone, serum K+, and clinical outcomes. These post hoc analyses demonstrated that eplerenone, when administered at a dose of 25 to 50 mg/d, is associated with a 4.4% absolute increase in the incidence of hyperkalemia [> 5.5 mEq/L (mmol/l)] and an absolute increase of only 1.6% in the incidence of more marked hyperkalemia [≥ 6.0 mEq/L (mmol/l)]. Overall, less than 1% of patients who were randomized to eplerenone had to discontinue therapy because of hyperkalemia [56]. Eplerenone can be used safely in patients with HF, provided they are monitored appropriately, as in the EPHESUS trial.
A positive effect of eplerenone was balanced by a significant reduction in hypokalemia [< 3.5 mEq/l (mmol/l)] episodes (8.4% vs 13.1%) in the eplerenone and placebo group, respectively [56]. This effect could theoretically lead to a significant reduction in the risk of arrhythmia in HF, which can be even greater since aldosterone antagonism reduces renal magnesium excretion [56]. It is likely that the reduction in hypokalemia was much more important than the potentially dangerous risk of hyperkalemia [56]. In this regard, it is interesting to consider mortality rates according to subgroups. When death rates were analyzed according to K+ concentration [cut-off value of 4 mEq/l (mmol/l)], there was no difference in all-cause mortality (P=0.29), but the difference was significant when considering cardiovascular death or hospitalization for cardiovascular events (P=0.02), favoring those patients with a K+ concentration<4 mEq/l (mmol/l) [59].
5. Potassium Supplements in HF PatientsK+ supplements are commonly used to treat hypokalemia and maintain
normokalemia. However, their long-term effects on outcomes in chronic heart failure are unknown. Ekundayo et al. used a public-use copy of the Digitalis Investigation Group (DIG) trial dataset to determine the association of K+
supplement use with outcomes with a propensity-matched design. Although the use of K+ supplements in chronic heart failure was not associated with mortality (HR when K+ supplement use was compared with non-use, 1.05; 95% CI, 0.94–1.18; P=0.390), it was associated with increased hospitalization due to cardiovascular causes (1.19; 1.08–1.32; P=0.001) and progressive HF (1.27; 1.12–1.43; P<0.0001) [60]. Ahmed et al. revealed that K+-supplement use was associated with no reduction in mortality, but with increased hospitalization (Fig. 2) [61].
8
Fig. 2. Association of potassium supplement use and all-cause hospitalization. Adopted from [61].
6. ConclusionsHypokalemia is common in HF patients, often due to a defect in
Na+/K+-ATPase activity and intracellular shift of K caused by oxidative stress and neurohormonal activation. Serum K+ levels have important therapeutic and prognostic implication for HF patients. While diuretics, commonly used in HF may cause hypokalemia, neurohormonal blockade using ACE inhibitors, angiotensin receptor blockers, beta-blockers, and aldosterone antagonists may cause hyperkalemia. Hypokalemia is associated with ventricular arrhythmias and sudden cardiac death. Mild hypokalemia may be corrected by the use of aldosterone receptor antagonists such as spironolactone or eplerenone. However, a more severe hypokalemia should preferably be corrected using K+
supplement. Patients with chronic hypokalemia requiring K+ supplements to maintain normokalemia may be treated with aldosterone antagonists instead. Some HF patients may remain hypokalemic despite therapy with aldosterone antagonists and should be treated with K+ supplements. HF in patients with chronic kidney disease and diabetes mellitus receiving aldosterone antagonists and/or K+ supplements should be monitored closely to avoid hyperkalemia (K+
>5.5 mEq/L). Symptomatic HF patients (NYHA class III–IV) should be prescribed the lowest dose of diuretic necessary to maintain euvolemia. Serum K levels should be frequently checked and maintained between 4.0 and 5.5 mEq/l (mmol/l).
9

Makna Dari Hipokalemia Pada Gagal Jantung
Abstrak
Pemeliharaan homeostasis kalium (K+) normal telah menjadi faktor
pembatas yang penting dalam terapi gagal jantung (HF). Dengan penggunaan
diuretik loop dan digoksin, hipokalemia telah menjadi efek samping yang sering
dan ditakuti dalam pengobatan. Serum K+ yang rendah pada HF mungkin juga
menjadi sebuah penanda meningkatnya aktivitas neurohormonal dan
perkembangan penyakit.
Untuk mendapatkan manfaat yang maksimal dari pengobatan, kita perlu
penggunaan obat-obatan secara individual dan memonitor elektrolit secara hati-
hati. Pasien dengan gejala HF (New York Heart Association kelas III-IV) harus
diberikan dosis terendah dari diuretik yang diperlukan untuk mempertahankan
euvolemia. Hipokalemia ringan dapat dikoreksi dengan menggunakan reseptor
aldosteron antagonis seperti spironolakton atau eplerenone. Bagaimanapun,
hipokalemia berat sebaiknya diperbaiki dengan menggunakan suplemen K+.
Serum K harus sering diperiksa dan dipertahankan antara 4,0 dan 5,5 mEq/l
(mmol/l).
1. Epidemiologi Hipokalemia pada Gagal Jantung (HF)
Gagal jantung kongestif membawa prognosis yang buruk. Angka
kelangsungan hidup hingga 5 tahun jauh di bawah 40% [1], dengan sebagian
merupakan kematian mendadak [2,3]. Kematian tersebut mungkin disebabkan
oleh aritmia ventrikel atau disosiasi elektromekanis [4-6]. Remodeling
elektrofisiologi dihubungkan dengan perkembangan hipertrofi dan gagal
jantung (HF) [7].
Kalium (K+) adalah elektrolit penting untuk sistem saraf yang sehat dan
teraturnya irama jantung [7,8]. Konsentrasi K+ penting dalam metabolisme sel
dan rangsangan membran [8]. Hipokalemia belum diartikan dengan baik dalam
HF, namun dalam literatur tentang hipertensi, definisi telah bervariasi dari <
3.5 hingga < 4.0 mEq/L (mmol/l) [9]. Deplesi K+ sering terlihat pada pasien
10

dengan gagal jantung kongestif, suatu kondisi yang ditandai oleh beberapa
predisposisi kelainan fisiologis untuk pengembangan gangguan elektrolit.
2. Etiologi dan Patofisiologi Hipokalemia pada HF
Diet tinggi natrium pada manusia modern dapat menghasilkan natrium
yang berlebihan dan deplesi K+ [10]. Hipokalemia memberikan kontribusi
dalam patogenesis penyakit kardiovaskular, dan gangguan kardiovaskular dan
obat-obatan yang dapat menyebabkan hipokalemia [11,12].
Pasien dengan HF mungkin mengalami masalah dalam transportasi K+
ke jaringan. Pada pasien dengan HF, peningkatan stres oksidatif dapat
menyebabkan kelainan dalam aktivitas Na+/K+- ATPase dan transportasi K+ ke
dalam jaringan. Akibatnya, tingkat K+ dalam jaringan mungkin jauh lebih
rendah daripada tingkat serum, dimana akan menempatkan mereka pada
peningkatan risiko fibrosis miokard, hipertrofi, dan kematian jantung
mendadak. Sebagai contoh, pasien dengan HF telah ditemukan memiliki serum
K+ yang lebih besar dari 7,0 mEq/L (mmol/l) tanpa perubahan
elektrokardiografi atau manifestasi klinis hiperkalemia karena K+ pada jaringan
mereka normal atau rendah, seperti konsentrasi K+ yang terdapat pada sel darah
merah [13]. Dengan demikian, disarankan tingkat serum K+ harus
dipertahankan antara 4,5 dan 5,5 mEq/L (mmol/l) pada pasien dengan HF [14].
Diantara faktor-faktor patogen yang terkait dengan HF adalah disfungsi
ginjal dan aktivasi neurohormonal, yang merangsang renin-angiotensin-
aldosteron, saraf simpatik, dan hipersekresi katekolamin [15].
Serum K+ berkorelasi negatif dengan aktivitas renin plasma dan plasma
noradrenalin, dan pasien yang respon dari pengobatan peningkatan konsentrasi
K+ intraseluler [16,17]. Dengan demikian, aktivasi neurohormonal memberikan
kontribusi nyata untuk deplesi K+ pada HF. Penurunan volume intravaskular,
seperti yang terjadi dengan disfungsi sistolik ventrikel kiri, dan mengurangi
hasil output jantung dalam patologis peningkatan aldosteron. Pada pasien
dengan gagal jantung kongestif, aldosteron dapat mencapai kadar plasma
hingga 60 kali lebih tinggi daripada yang diukur dalam subyek normal [18,19].
11

Kardiomiosit, pembuluh darah, dan adiposit juga menunjukkan sintesis
aldosteron [19]. Aldosteron menyebabkan reabsorpsi natrium dan air
bersamaan dengan ekskresi K+. Efek samping dikaitkan dengan
hiperaldosteronisme yang dapat mempengaruhi fungsi kardiovaskular yang
meliputi peningkatan retensi cairan intravascular dan volume overload,
disfungsi endotel, gangguan reaktivitas vaskular, aktivasi sistem saraf simpatik,
penurunan sensitivitas baroreseptor, peningkatan ekskresi elektrolit (K+ dan ion
magnesium), dan apoptosis kardiomyocyte [18,20,21] (Gambar 1). Rendahnya
tingkat serum K+ pada HF mungkin menjadi tanda meningkatnya aktivitas
neurohormonal dan perkembangan penyakit [21,22].
Gambar. 1. Pengaruh gangguan fungsi ventrikel kiri (LV) pada sintesis aldosteron. A, Penurunan curah jantung akibat disfungsi sistolik LV dianggap sebagai penurunan eferen aliran darah ginjal. B, ini merangsang sekresi renin dari apparatus juxtaglomeruler. C, Dalam sirkulasi perifer, renin memecah angiotensinogen menjadi angiotensin I (AT I), yang diubah menjadi angiotensin II (AT II) oleh ACE dalam pembuluh darah arteri pulmonalis (D). E, Angiotensin II merangsang zona glomerulosa di korteks adrenal untuk mengeluarkan aldosteron. Peningkatan kadar plasma aldosteron memiliki sejumlah efek buruk pada sistem kardiovaskular. NO • menunjukkan oksida nitrat. (Heart images from U-Write patient education), © 1998 William Fridl, dba U-Write; kidney and glomerulus images from Bill Camelet; blood vessel images from John MacNeil; adrenal gland image reproduced from McGill Molson Medical Informatics Project, McGill University.
Hipokalemia merupakan efek samping yang sering dan ditakuti dari
pengobatan HF dengan diuretik loop dan digoxin [23] karena potensi
12

arrhythmogenic dari digoxin adalah peningkatan terjadi hipokalemia. Kelas
utama diuretik adalah diuretik loop, diuretik K+ -sparing, dan tiazid. Diuretik
loop, merupakan terapi andalan untuk HF akut dan kronis, yaitu "obat
permulaan", sehingga dibutuhkan dosis yang adekuat untuk mencapai efek
farmakodinamik [23].
Diuretik loop termasuk derivat sulfonamide furosemide, bumetanide,
dan torsemide, serta asam ethacrynic, lebih jarang digunakan. Obat ini
menghambat Na+-K+-2Cl- cotransporter (NKCC) di cabang ascending tebal
pada loop of Henle, yang bertanggung jawab untuk reabsorpsi 20% sampai
30% dari penyaringan natrium [24]. Diuretik thiazide, yang paling umum
digunakan dari kelas diuretik, menghambat transporter natrium klorida - dalam
tubulus distal. Karena transporter ini biasanya menyerap kembali hanya sekitar
5% dari penyaringan natrium, diuretik ini kurang efisien dibandingkan diuretik
loop dalam memproduksi diuresis dan natriuresis [24]. Namun demikian,
mereka cukup kuat untuk memenuhi kebutuhan suatu terapi. Mekanisme
mereka tergantung pada produksi prostaglandin ginjal [24].
Karena diuretik loop dan thiazide meningkatkan pengiriman natrium ke
segmen tubulus distal, sehingga terjadi pengurangan K+ (berpotensi
menyebabkan hipokalemia). Hal ini terjadi karena peningkatan konsentrasi
natrium tubular distal merangsang pompa natrium aldosteron untuk
meningkatkan reabsorpsi natrium dalam pertukaran K+ dan ion hidrogen, yang
keluar melalui urin [25-27].
Efek yang berpotensi bahaya dari pemberian dosis tinggi diuretik loop
adalah aktivasi neurohormonal dari sistem renin-angiotensin-aldosteron dan
peningkatan kadar norepinefrin dan arginin vasopressin, yang keduanya secara
fundamental terlibat dalam perkembangan HF [25-27]. Pada pasien dengan HF
adalah penting untuk mencapai euvolemia yang meningkatkan kondisi klinis
pasien, di sisi lain dokter harus berusaha untuk menurunkan dosis diuretik, bila
mungkin, karena aktivasi neurohormonal sistem renin-angiotensin-aldosteron
(RAAS).
13

Pemberian diuretik loop dapat menyebabkan ketidakseimbangan
elektrolit (seperti hipokalemia, hiponatremia, dan hypomagnesemia) yang
dapat memperburuk aritmia jantung dan meningkatkan risiko kematian jantung
mendadak [28,29]. Dalam percobaan Studi Disfungsi Ventrikel Kiri (SOLVD),
penggunaan diuretik dihubungkan dengan peningkatan 37% dalam risiko
kematian dengan arrhythmic setelah mengendalikan beberapa keparahan
penyakit lainnya [28,29].
Namun, sedikit yang diketahui tentang efek hipokalemia pada hasil
pada pasien dengan gagal jantung kronis [30].
3. Pengaruh Hipokalemia pada HF
Hipokalemia menyebabkan hyperpolarity seluler, meningkatkan potensi
istirahat, mempercepat depolarisasi, dan meningkatkan otomatisitas dan
rangsangan [31,32]. Karena repolarisasi jantung bergantung pada masuknya
K+, hipokalemia memperpanjang potensial aksi dan meningkatkan dispersi QT
yang menggambarkan inhomogeneity listrik. Kebanyakan pasien dengan HF
memiliki peningkatan ektopi ventrikel, dan 50% nonsustained ventricular
takikardi [33]. Sebanyak 50% dari kematian akibat HF secara tiba-tiba,
mungkin karena aritmia. Pada korban kematian jantung mendadak, tingkat
miokard K+ tercatat lebih rendah daripada kelompok kontrol, dan korban sering
mengalami hipokalemia [34]. Pada HF, semua penyebab dan tingkat kematian
jantung lebih tinggi pada orang yang memakai diuretik non K+ -sparing [35].
Insiden kematian arrhythmic secara signifikan dan independen terkait dengan
penggunaan diuretik non K+ -sparing [34,35].
Predisposisi pasien hipokalemia untuk toksisitas digoxin dengan
mengurangi pengeluaran melalui ginjal dan meningkatkan penggunaan obat
miokard binding. Hal ini, pada gilirannya, menghasilkan peningkatan
otomatisitas dan aritmia ventrikel [36,37]. Deplesi K+ memperburuk disfungsi
diastolik pada hewan dan model manusia [38] .
Efek negatif hipokalemia pada pasien dengan HF telah dilaporkan
dalam studi klinis. Penelitian oleh Bowling et al. [39] termasuk 7788 pasien
14

dengan gagal jantung kronis dalam percobaan Group Investigation Digitalis.
Dari jumlah tersebut, 2793 memiliki penyakit ginjal kronis, yang didefinisikan
sebagai laju filtrasi glomerulus (eGFR)<60 mL/min/1.73 m2. Skor
kecenderungan untuk hipokalemia [serum K+, < 4 mEq/L (mmol/l)] digunakan
untuk menyeimbangkan kohort 522 pasang pasien dengan hipokalemia dan
normokalemia. Kematian karena semua penyebab terjadi pada 48% dan 36%
dari pasien dengan hipokalemia dan normokalemia, masing-masing, selama 57
bulan dan waktu tindak lanjut (cocok dengan rasio hazard ketika hipokalemia
dibandingkan dengan normokalemia, 1.56; 95% confidence interval [CI], 1.25
hingga 1.95; P < 0.0001). Pada pasien dengan HF dan penyakit ginjal kronis,
kematian dari semua penyebab terjadi pada 47% dan 38% dari pasien dengan
hipokalemia ringan [3,5-3,9 mEq/L (mmol/l)] dan normokalemia, masing-
masing (cocok dengan rasio hazard, 1.31; 95% CI, 1.03-1.66, P=0,027) [39].
Alper et al. [41] mempelajari efek dari tingkat serum K+ rendah pada
populasi pasien lansia dengan gagal jantung (≥ 65 tahun), pasien dikategorikan
ke dalam kelompok yang rendah [< 4 mEq/L (mmol/l)]; n = 590 dan normal K+
[4-4,9 mEq/L (mmol/l), n = 2684]. Serum K+ rendah dikaitkan dengan
peningkatan mortalitas: 37% (angka, 1338/10000 orang/tahun) pada pasien
dengan K+ yang normal dan 43% (angka, 1594/10000 orang/tahun) pada pasien
rendah K+ (rasio hazard [HR] untuk K+ rendah, 1.22; 95% CI, 1.04-1.44; P =
0.014). Suatu tingkat serum K+ rendah (HR, 1.10, 95% CI, 0.96-1.25, P =
0.175) tidak berhubungan dengan semua penyebab rawat inap [41].
Menurut sebuah posting hoc analisis data dari uji coba secara acak,
hipokalemia dikaitkan dengan peningkatan risiko kematian yang independen
dari New York Heart Association (NYHA) kelas fungsional, obat yang
digunakan dalam terapi, dan penggunaan suplemen K+ [40,42].
Dalam Efikasi Eplerenone Pasca Akut Myocardial Infarction Gagal
Jantung dan Studi Kelangsungan Hidup (EPHESUS), penurunan absolut
signifikan sebesar 4.7 % ditemukan pada kejadian hipokalemia [serum K+ < 3.5
mEq/L (mmol/l)], dan kejadian hipokalemia lebih besar dari hiperkalemia
[serum K+ ≥ 6,0 mEq/L (mmol/l)] [43].
15

Tabel 1
Risiko kematian yang terkait dengan serum kalium ≤ 4 mEq/L pada gagal jantung (HF) [40].
Hasil dinyatakan sebagai hazard ration (HR) dan 95% confidence interval (CI).
*Disesuaikan untuk demografi, etiologi HF, penyakit jantung, diabetes, obat-obatan (termasuk
digoxin, ACE inhibitor, diuretik), penggunaan diuretik hemat kalium, suplemen kalium, tanda dan
gejala HF, kelas fungsional NYHA, temuan Xray dada dan kreatinin serum.
Meskipun banyak dokter yang memperhatikan tentang risiko dari
hipokalemia hanya ketika tingkat serum K+ adalah < 3.5 mEq/L (mmol/l),
analisis terbaru dari National Heart, Lung, dan Blood Digitalis Group
Investigation Institute menunjukkan peningkatan risiko dari kematian jantung
mendadak dan HF progresif pada pasien dengan serum K+ < 4.5 mEq/L
(mmol/l), terlepas dari penggunaan suplemen K+ [44].
Hubungan penurunan serum K+ [< 4.4 mEq/L (mmol/l)] sebagai
prediktor independen kematian jantung mendadak pada pasien dengan HF telah
dibuktikan dalam penelitian lain. Evaluasi Gagal Jantung dan Penilaian Risiko
Percobaan Inggris, Nolan dkk. menemukan bahwa tingkat serum K+ rendah
terkait dengan kematian jantung mendadak (n=433) [45].
Leier et al. [46] telah merekomendasikan untuk mempertahankan
tingkat serum K+ di kisaran 4,5-5,0 mEq/L (mmol/l). Pentingnya mencegah
hipokalemia ditegaskan oleh temuan bahwa risiko disritmia, sinkop, serangan
jantung, atau kematian lebih besar pada pasien dengan HF. Hasil ini mungkin
disebabkan sebagian sel-sel hipertrofi dan gagal jantung seringkali memiliki
durasi potensial aksi berkepanjangan, yang dalam banyak kasus disebabkan
oleh penurunan K+ [46].
16

4. Pencegahan dan Pengobatan Hipokalemia pada HF
Terapi obat kombinasi dapat sekaligus meningkatkan hasil klinis
sementara kejadian hubungan risiko efek samping yang berhubungan dengan
K+ [47]. Diuretik K+ -sparing penting dalam mencegah hipokalemia pada HF
[47].
Pada diuretik K+ -sparing termasuk spironolactone dan eplerenone.
Tidak seperti diuretik loop dan thiazide, dimana obat ini tidak bertindak
langsung pada transportasi natrium. Beberapa obat dalam kelas ini merupakan
antagonis aldosteron (aldosteron antagonis reseptor) di segmen distal tubulus
distal, yang menyebabkan lebih banyak natrium (dan air) untuk masuk
berkumpul ke dalam saluran dan diekskresikan dalam urin. Dengan
menghambat reabsorpsi natrium aldosteron -sensitif, sedikit K+ dan ion
hidrogen dipertukarkan untuk natrium oleh transporter ini, dan karena itu, K+
berkurang dan hidrogen hilang melalui urin. Diuretik K+ - sparing lainnya
langsung menghambat saluran natrium dengan pompa natrium aldosterone, dan
karena itu, mereka memiliki efek yang sama pada K+ dan ion hidrogen seperti
antagonis aldosteron [47]. Mekanisme mereka tergantung pada produksi
prostaglandin di ginjal [47]. Blokade aldosteron efektif dalam mengurangi
kematian dari semua penyebab pada pasien setelah infark miokard komplikasi
oleh disfungsi ventrikel kiri dan HF. Penggunaan blokade aldosteron pada
pasien ini telah diakui sebagai pedoman kelas 1 indikasi baik di AS dan Eropa
[47].
Pengaruh positif dari obat ini terhubung dengan kemampuan mereka
untuk menghambat efek yang merugikan dari hiperaldosteronisme pada pasien
dengan HF (Gambar 1) [48,49].
Spironolactone adalah aldosteron nonselektif antagonis reseptor yang
dimetabolisme secara luas di hati untuk metabolit aktif dan secara struktural
mirip dengan progesteron, sehingga memungkinkan reseptor steroid reaktivitas
silang [50]. Fenomena efek antiprogesteron dan antiandrogen diamati pada
beberapa pasien yang diobati dengan spironolactone [50].
17

Dalam pra-RALES (Studi Evaluasi Aldactone Acak) studi percontohan,
[51] pada 214 pasien respon dosis dalam kejadian hiperkalemia didefinisikan
sebagai serum K+ > 5.5 mEq/l (mmol/l) dinilai dalam 4 kelompok diobati
dengan spironolactone dalam dosis 12.5, 25, 50 dan 75 mg. Insiden
hiperkalemiamasing-masing adalah 5, 13, 20 dan 24% dan prediktor untuk
pengembangan hiperkalemia adalah penggunaan angiotensin -converting
(ACE) inhibitor dan elevasi dasar K+ atau kreatinin. Pengobatan dianggap
aman, asalkan serum K+ diawasi secara ketat [51].
Peneliti RALES melakukan studi keamanan mengenai penggunaan
spironolactone pada pasien di NYHA kelas III sampai IV dengan disfungsi
sistolik ventrikel kiri. Dari catatan, 10% dari pasien dalam kelompok kontrol
dalam penelitian ini disajikan dengan hipokalemia [52].
Sebaliknya, pasien menerima 50 atau 75 mg spironolactone pada pasien
yang tidak mengalami hipokalemia, dan hanya satu pada mereka yang
menerima 25 mg/hari. Penelitian ini menunjukkan penurunan yang signifikan
dalam mortalitas sekitar 30%. Analisis subgroup menunjukkan peningkatan
serupa dalam angka kematian terlepas dari konsentrasi kreatinin atau K+ atau
penggunaan suplemen K+ [52].
Pengalaman positif dalam uji klinis dengan beberapa laporan kasus
hiperkalemia serius pada pasien yang diberikan spironolactone untuk gagal
jantung kronis dalam praktek klinis, beberapa di antaranya dikaitkan dengan
peningkatan masuk rumah sakit dan kematian [53-55].
Terjadinya hiperkalemia dalam uji coba tersebut mungkin berhubungan
dengan dosis yang digunakan lebih tinggi dalam penelitian ini [56]
dibandingkan dengan referensi percobaan, EPHESUS dan RALES. Dalam
praktek klinis, pasien yang lebih tua dalam uji acak dan memiliki eGFR
berkurang yang tidak didasarkan tingkat kreatinin serum, karena serum
kreatinin merupakan ukuran akurat dari fungsi ginjal yang benar pada orang
tua [56].
Selama pengobatan antagonis aldosteron harus menilai parameter ginjal
dan konsentrasi elektrolit optimal setelah 1 minggu dan 4 minggu kemudian
18

setelah memulai pengobatan, setelah dosis optimal obat ditetapkan, pengukuran
harus diperoleh pada 1, 2, 3 dan 6 bulan, dan setelah itu setiap 6 bulan [57].
Disarankan bahwa setiap kali terjadi perubahan status elektrolit, seperti saat
terjadi muntah atau diare atau inisiasi atau penyesuaian dosis terapi diuretik,
tingkat serum K+ harus diukur kembali atau blocker aldosteron tidak
dimasukkan sampai pengukuran tersebut memungkinkan [58].
Eplerenone adalah reseptor antagonis aldosteron selektif berasal dari
spironolactone, tetapi karena afinitas terbatas untuk progesteron dan androgen
reseptor, sehingga kurang berhubungan dengan efek samping [50].
Dalam percobaan EPHESUS [56], aldosteron eplerenone blocker yang
selektif (25 sampai 50 mg/d) secara signifikan mengurangi semua penyebab
kematian (15%; P = 0.008) dan mortalitas kardiovaskular atau rawat inap
(13%; P = 0.002) ketika digunakan selain untuk terapi standar pada pasien
dengan disfungsi sistolik ventrikel kiri, fraksi ejeksi ventrikel kiri ≤ 40 %, dan
HF setelah infark miokard akut. Selain itu, untuk mengurangi rawat inap pada
HF (15% ; P = 0.03 ) dan kematian jantung mendadak (21% ; P = 0.03). Pasien
dikeluarkan jika baseline K+ adalah > 5.0 mEq/L atau serum kreatinin adalah >
2.5 mg/dL (221.0 μmol/l).
Sebuah subanalysis studi EPHESUS menguji hubungan antara
eplerenone, serum K+, dan hasil klinis. Analisis post hoc menunjukkan bahwa
eplerenone, bila diberikan dengan dosis 25 sampai 50 mg/d, dikaitkan dengan
peningkatan absolut 4.4% dalam kejadian hiperkalemia [> 5.5 mEq/L
(mmol/l)] dan mutlak peningkatan hanya 1,6 % dalam kejadian yang ditandai
hiperkalemia [≥ 6,0 mEq/L (mmol/l)]. Secara keseluruhan, kurang dari 1%
pasien yang diacak untuk eplerenone harus menghentikan terapi karena
hiperkalemia [56]. Eplerenone dapat digunakan secara aman pada pasien
dengan HF, asalkan mereka dimonitor dengan tepat, seperti dalam percobaan
EPHESUS.
Sebuah efek positif eplerenone diimbangi dengan penurunan yang
signifikan dalam hipokalemia [< 3.5 mEq/l (mmol/l)] masing-masing (8.4% vs
13.1%) pada kelompok eplerenone dan plasebo [56]. Efek ini secara teoritis
19

dapat menyebabkan penurunan yang signifikan dalam risiko aritmia pada HF,
yang bahkan bisa lebih besar karena aldosteron antagonisme mengurangi
ekskresi magnesium ginjal [56]. Sangat mungkin bahwa penurunan
hipokalemia jauh lebih penting daripada risiko berbahaya hiperkalemia [56].
Dalam hal ini, menarik untuk mempertimbangkan tingkat kematian menurut
subkelompok. Ketika angka kematian dianalisis sesuai dengan konsentrasi K+
[nilai 4 mEq/l (mmol/l)], tidak ada perbedaan di semua penyebab kematian (P
= 0.29), tetapi berbeda signifikan ketika mempertimbangkan kematian
kardiovaskular atau kejadian kardiovaskuler di rumah sakit (P=0.02),
mendukung pasien dengan konsentrasi K+ > 4 mEq/l (mmol/l) [59].
5. Suplemen Kalium pada Pasien HF
Suplemen K+ biasanya digunakan untuk mengobati hipokalemia dan
menjaga normokalemia. Namun, efek jangka panjang terhadap hasil pada gagal
jantung kronis tidak diketahui. Ekundayo et al. menggunakan salinan publik
Group Investigation Digitalis (DIG) data set percobaan untuk menentukan
hubungan dari penggunaan suplemen K+ dengan hasil bentuk yang akan cocok.
Meskipun penggunaan suplemen K+ pada gagal jantung kronis tidak dikaitkan
dengan mortalitas (HR ketika penggunaan suplemen K+ dibandingkan dengan
non -penggunaan, 1.05, 95% CI, 0.94-1.18, P = 0.390), hal itu terkait dengan
peningkatan rawat inap karena penyebab kardiovaskular (1.19; 1.08-1.32, P =
0,001) dan HF progresif (1.27; 1.12-1.43; P<0.0001) [60]. Ahmed et al.
mengungkapkan bahwa penggunaan suplemen K+ tidak dikaitkan dengan
terjadinya penurunan angka kematian, tapi dengan peningkatan rawat inap
(Gambar 2) [61].
20

Gambar 2. Asosiasi penggunaan suplemen Kalium dan semua penyebab rawat inap.
6. Kesimpulan
Hipokalemia umum terjadi pada pasien HF, sering karena kelainan
dalam aktivitas Na+/K+ - ATPase dan pergeseran intraseluler K disebabkan oleh
stres oksidatif dan aktivasi neurohormonal. Tingkat serum K+ memiliki
implikasi terapeutik dan prognostik penting bagi pasien HF. Sementara
diuretik, yang biasa digunakan dalam HF dapat menyebabkan hipokalemia,
blokade neurohormonal yang menggunakan ACE inhibitor, angiotensin
receptor blocker, beta-blocker, dan antagonis aldosteron yang dapat
menyebabkan hiperkalemia. Hipokalemia dikaitkan dengan aritmia ventrikel
dan kematian jantung mendadak. Hipokalemia ringan dapat dikoreksi dengan
menggunakan aldosteron antagonis reseptor seperti spironolactone atau
eplerenone. Namun, hipokalemia yang lebih parah sebaiknya diperbaiki dengan
menggunakan suplemen K+. Pasien dengan hipokalemia kronis yang
membutuhkan suplemen K+ untuk menjaga normokalemia dapat diobati dengan
antagonis aldosteron sebagai gantinya. Beberapa pasien HF mungkin tetap
hipokalemia meskipun terapi dengan antagonis aldosteron dan harus dikoreksi
dengan suplemen K+. HF pada pasien dengan penyakit ginjal kronis dan
diabetes mellitus mendapatkan antagonis aldosteron dan/atau suplemen K+
harus dimonitor untuk menghindari hiperkalemia (K+ > 5.5 mEq/L). Gejala
21

pasien HF (NYHA kelas III - IV) harus diberikan dosis diuretik terendah yang
diperlukan untuk mempertahankan euvolemia. Serum K harus sering diperiksa
dan dipelihara antara 4,0 dan 5,5 mEq/l (mmol/l) .
22

References[1] Kannel WB, Ho K, Thom T. Changing epidemiological features of cardiac failure. Br Heart J
1994;72:S3–9 (suppl).[2] Cohn JN, Archibald DG, Ziesche S, et al. Effects of vasodilator therapy on mortality in
chronic congestive heart failure: a result of a veterans affairs comparative study (V-HEFT). New Engl J Med 1986;314:1547–52.
[3] Cohn JN, Johnson G, Ziesche S, et al. A comparison of enalapril with hydralazine–isosorbide dinitrate in the treatment of chronic congestive heart failure. New EnglJ Med 1991;325:303–10.
[4] Kempf FC, Josephson ME. Cardiac arrest recorded on ambulatory electrocardiograms. Am J Cardiol 1984;427:241–51.
[5] Luu M, Stevenson WG, Stevenson LW, Baron K, Walden J. Diverse mechanisms of unexpected cardiac arrest in advanced heart failure. Circulation 1989;80:1675–80.
[6] Stevenson WG, Stevenson LW, Middlekauff HR, Saxon LA. Sudden death prevention in patients with advanced ventricular dysfunction. Circulation 1993;88:2953–61.
[7] Tomaselli GF, Marban E. Electrophysiological remodeling in hypertrophy and heart failure. Cardiovasc Res 1999;42:270–83.
[8] Dursun I, Sahin M. Difficulties in maintaining potassium homeostasis in patients with heart failure. Clin Cardiol 2006;29(9):388–92.
[9] Macdonald JE, Struthers AD. What is the optimal serum potassium level in cardiovascular patients? J Am Coll Cardiol 2004;43:155–61.
[10] Meneely GR, Battarbee HD. High sodium-low potassium environment and hypertension. Am J Cardiol 1976;38:768–85.
[11] Schulman M, Narins RG. Hypokalemia and cardiovascular disease. Am J Cardiol 1990;65:4E–9E.
[12] Hoes AW, Grobbee DE, Peet TM, Lubsen J. Do non-potassium sparing diuretics increase the risk of sudden cardiac death in hypertensive patients? Recent evidence. Drugs 1994;47:711–33.
[13] Delgado-Almeida A, Delgado-Leon C. Changes in plasma ionized calcium and RBC K content in severe hyperkalemia: new electrocardiographic concept. Circulation 2006;114(suppl II):II-466.
[14] Macdonald JE, Struthers AD. What is the optimal serum potassium level in cardiovascular patients? J Am Coll Cardiol 2004;43:155–61.
[15] Cohn JN, Kowey PR, Whelton PK, Prisant LM. New guidelines for potassium replacement in clinical practice. A contemporary review by the National Council on Potassium in Clinical Practice. Arch Intern Med 2000;160:2429–36.
[16] Cleland JG, Dargie HJ, Robertson I, Robertson JI, East BW. Total body electrolyte composition in patients with heart failure: a comparison with normal subjects and patients with untreated hypertension. Br Heart J 1987;58:230–8.
[17] Cleland JG, Dargie HJ, East BW, et al. Total body and serum electrolyte composition in heart failure: the effects of captopril. Eur Heart J 1985;6:681–8.
[18] Maron AB, Leopold JA. Aldosterone receptor antagonists. Effective but often forgotten. Circulation 2010;121:934–9.
[19] Weber KT. Aldosterone in congestive heart failure. N Engl J Med 2001;345:1689–97.[20] Leopold JA, Dam A, Maron BA, et al. Aldosterone impairs vascular reactivity by decreasing
glucose-6-phosphate dehydrogenase activity. Nat Med 2007;13:189–97.[21] Gaddam KK, Verma A, Thompson M, Amin R, Ventura H. Hypertension and cardiac failure
in its various forms. Med Clin North Am 2009;93:665–80.
23

[22] Williams GH. Aldosterone and heart failure: the rest of the story. Heart Fail Rev 2005;10:5–6.
[23] Davidson C, McLachlan MS, Burkinshaw L, et al. Effect of long-term diuretic treatment on body-potassium in heart-disease. Lancet 1976;2:1044–7.
[24] Brater DC. Diuretic therapy. N Engl J Med 1998;339:387–95.[25] Francis GS, Benedict C, Johnstone DE, et al. Comparison of neuroendocrine activation in
patients with left-ventricular dysfunction with and without congestive-heart-failure — a substudy of the Studies of Left-Ventricular Dysfunction (SOLVD). Circulation 1990;82:1724–9.
[26] Francis GS, Siegel RM, Goldsmith SR, Olivari MT, Levine TB, Cohn JN. Acute vasoconstrictor response to intravenous furosemide in patients with chronic congestive heart-failure — activation of the neurohumoral axis. Ann Intern Med 1985;103:1–6.
[27] Bayliss J, Norell M, Canepaanson R, Sutton G, Poolewilson P. Untreated heartfailure — clinical and neuroendocrine effects of introducing diuretics. Br Heart J 1987;57:17–22.
[28] Klein L, O'Connor CM, Leimberger JD, et al. Lower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure: results from the outcomes of a prospective trial of intravenous milrinone for exacerbations of chronic heart failure (OPTIME-CHF) study. Circulation 2005;111:2454–60.
[29] Cooper HA, Dries DL, Davis CE, Shen YL, Domanski MJ. Diuretics and risk of arrhythmic death in patients with left ventricular dysfunction. Circulation 1999;100:1311–5.
[30] Cohn JN, Kowey PR, Whelton PK, Prisant LM. New guidelines for potassium replacement in clinical practice. A contemporary review by the national council on potassium in clinical practice. Arch Intern Med 2000;160:2429–36.
[31] Fisch C, Knoebel SB, Feigenbaum H, Greenspan K. Potassium and the monophasic action potential, electrocardiogram, conduction and arrhythmias. Prog Cardiovasc Dis 1966;8:387–418.
[32] Gettes L, Surawicz B. Effects of low and high concentrations of potassium on the simultaneously recorded Purkinje and ventricular action potentials of the perfused pig moderator band. Circ Res 1968;23:717–29.
[33] Packer M. Sudden unexpected death in patients with congestive heart failure: a second frontier. Circulation 1985;72:681–5.
[34] Salerno DM, Asinger RW, Elsperger J, Ruiz E, Hodges M. Frequency of hypokalemia after successfully resuscitated out-of hospital cardiac arrest compared with that in transmural acute myocardial infarction. Am J Cardiol 1987;59:84–8.
[35] Cooper HA, Dries DL, Davis CE, Shen YL, Domanski MJ. Diuretics and risk of arrhythmic death in patients with left ventricular dysfunction. Circulation 1999;100:1311–13315.
[36] Rosen MR, Gelband H, Merker C, Hoffman BF. Mechanisms of digitalis toxicity: effects of ouabain on phase four of canine Purkinje fiber transmembrane potentials. Circulation 1973;47:681–9.
[37] Macdonald JE, Struthers AD. What is the optimal serum potassium level in cardiovascular patients? J Am Coll Cardiol 2004;43:155–61.
[38] Srivastava TN, Young DB. Impairment of cardiac function by moderate potassium depletion. J Card Fail 1995;1:195–200.
[39] Bowling CB, Pitt B, Ahmed MI, et al. Hypokalemia and outcomes in patients with chronic heart failure and chronic kidney disease: findings from propensitymatched studies. Circ Heart Fail 2010;3(2):253–60.
[40] Ahmed A, Zannad F, Love TE, et al. A propensity-matched study of the association of low serum potassium levels and mortality in chronic heart failure. Eur Heart J 2007;28:1334–43.
24

[41] Alper AB, Campbell RC, Anker SD, et al. A propensity-matched study of low serum potassium and mortality in older adults with chronic heart failure. Int J Cardiol 2009;11(137(1)):1–8.
[42] Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med 1997;336:525–33.
[43] Pitt B, Bakris G, Ruilope LM, DiCarlo L, Mukherjee R. Serum potassium and clinical outcomes in the eplerenone post-acute myocardial infarction heart failure efficacy and survival study (EPHESUS). Circulation 2008;118:1643–50.
[44] Ahmed A, Pitt B, Rahimtoola SH, et al. Effects of digoxin at low serum concentrations on mortality and hospitalization in heart failure: a propensitymatched study of the DIG trial. Int J Cardiol 2008;123:138–46.
[45] Nolan J, Batin PD, Andrews R, et al. Prospective study of heart rate variability and mortality in chronic heart failure: results of the United Kingdom heart failure evaluation and assessment of risk trial (UK-heart). Circulation 1998;98:1510–6.
[46] Leier CV, Dei Cas L, Metra M. Clinical relevance and management of the major electrolyte abnormalities in congestive heart failure: hyponatremia, hypokalemia, and hypomagnesemia. Am Heart J 1994;128:564–74.
[47] Jessup M, Abraham WT, Casey DE, et al. 2009 Focused update: ACCF/AHA guidelines for the diagnosis and management of heart failure in adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation 2009;119:1977–2016.
[48] Desai A. Hyperkalemia associated with inhibitors of the renin–angiotensin– aldosterone system balancing risk and benefit. Circulation 2008;118:1609–11.
[49] Maron AB, Leopold JA. Aldosterone receptor antagonists. Effective but often forgotten. Circulation 2010;121:934–9.
[50] Perazella MA. Drug-induced hyperkalemia: old culprits and new offenders. Am J Med 2000;109:307–14.
[51] Effectiveness of spironolactone added to an angiotensin-converting enzyme inhibitor and a loop diuretic for severe chronic congestive heart failure. The randomized aldactone evaluation study (RALES). Am J Cardiol 1996;78:902–7.
[52] Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized aldactone evaluation study investigators. N Engl J Med 1999;341:709–17.
[53] Cruz CS, Cruz AA, Marcilio de Souza CA. Hyperkalaemia in congestive heart failure patients using ACE inhibitors and spironolactone. Nephrol Dial Transplant 2003;18:1814–9.
[54] Schepkens H, Vanholder R, Billiouw JM, et al. Life-threatening hyperkalemia during combined therapy with angiotensin-converting enzyme inhibitors and spironolactone: an analysis of 25 cases. Am J Med 2001;110:438–41.
[55] Svensson M, Gustafsson F, Galatius S, et al. How prevalent is hyperkalemia and renal dysfunction during treatment with spironolactone in patients with congestive heart failure? J Card Fail 2004;10:297–303.
[56] Pitt B, Bakris G, Ruilope LM, DiCarlo L, Mukherjee R. Serum potassium and clinical outcomes in the eplerenone post-acute myocardial infarction heart failure efficacy and survival study (EPHESUS). Circulation 2008;118:1643–50.
[57] European Society of Cardiology; Heart Failure Association of the ESC (HFA); European Society of Intensive Care Medicine (ESICM). ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the diagnosis and treatment of
25

acute and chronic heart failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur J Heart Fail 2008;10(10):933–89.
[58] Pitt B, Remme W, Zannad F, et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 2003;348:1309–21.
[59] Gao X, Peng L, Adhikari CM, et al. Spironolactone reduced arrhythmia and maintained magnesium homeostasis in patients with congestive heart failure. J Card Fail 2007;13:170–7.
[60] Ekundayo OJ, Adamopoulos C, Ahmed MI, et al. Oral potassium supplement use and outcomes in chronic heart failure: a propensity-matched study. Int J Cardiol 2010;141:167–74.
[61] Ahmed A, Adamopoulos Ch, Sui X, Love TE. Abstract 3395: potassium supplement use may increase hospitalization without affecting mortality in chronic heart failure: implications for use of aldosterone antagonists to maintain potassium balance in chronic heart failure. Circulation 2007;116:II-766.
[62] Shewan LG, Coats AJ. Ethics in the authorship and publishing of scientific articles. Int J Cardiol 2010;144:1–2.
26