Embed Size (px)
DESCRIPTION
jurnal anak
Citation preview

original article
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 363;26 nejm.org december 23, 20102522
Long-Term Mortality in Childhood-Onset Epilepsy
Matti Sillanpää, M.D., Ph.D., and Shlomo Shinnar, M.D., Ph.D.
From the Departments of Pediatric Neu-rology and Public Health, University of Turku and Turku University Hospital — both in Turku, Finland (M.S.); and the Departments of Neurology, Pediatrics, and Epidemiology and Population Health and the Comprehensive Epilepsy Manage-ment Center, Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY (S.S.). Address reprint requests to Dr. Shinnar at the Comprehensive Epilepsy Management Center, Montefiore Medical Center, 111 E. 210th St., Bronx, NY 10467, or at [email protected].
N Engl J Med 2010;363:2522-9.Copyright © 2010 Massachusetts Medical Society.
A BS TR AC T
Background
There are few studies on long-term mortality in prospectively followed, well-charac-terized cohorts of children with epilepsy. We report on long-term mortality in a Finnish cohort of subjects with a diagnosis of epilepsy in childhood.
Methods
We assessed seizure outcomes and mortality in a population-based cohort of 245 children with a diagnosis of epilepsy in 1964; this cohort was prospectively followed for 40 years. Rates of sudden, unexplained death were estimated. The very high autopsy rate in the cohort allowed for a specific diagnosis in almost all subjects.
Results
Sixty subjects died (24%); this rate is three times as high as the expected age- and sex-adjusted mortality in the general population. The subjects who died included 51 of 107 subjects (48%) who were not in 5-year terminal remission (i.e., ≥5 years seizure-free at the time of death or last follow-up). A remote symptomatic cause of epilepsy (i.e., a major neurologic impairment or insult) was also associated with an increased risk of death as compared with an idiopathic or cryptogenic cause (37% vs. 12%, P<0.001). Of the 60 deaths, 33 (55%) were related to epilepsy, including sudden, unexplained death in 18 subjects (30%), definite or probable seizure in 9 (15%), and accidental drowning in 6 (10%). The deaths that were not related to epilepsy occurred primarily in subjects with remote symptomatic epilepsy. The cumulative risk of sudden, unexplained death was 7% at 40 years overall and 12% in an analy-sis that was limited to subjects who were not in long-term remission and not receiving medication. Among subjects with idiopathic or cryptogenic epilepsy, there were no sudden, unexplained deaths in subjects younger than 14 years of age.
Conclusions
Childhood-onset epilepsy was associated with a substantial risk of epilepsy-related death, including sudden, unexplained death. The risk was especially high among chil-dren who were not in remission. (Funded by the Finnish Epilepsy Research Foundation.)
The New England Journal of Medicine Downloaded from nejm.org on October 20, 2015. For personal use only. No other uses without permission.
Copyright © 2010 Massachusetts Medical Society. All rights reserved.

Mortality in Childhood-Onset Epilepsy
n engl j med 363;26 nejm.org december 23, 2010 2523
Few studies have evaluated long-term mortality in well-characterized cohorts of children with epilepsy. With a few notable
exceptions,1-3 studies involving adults are usually retrospective.4-11 In pediatric series, the follow-up is generally 5 to 10 years.12-18 In all series, au-topsy confirmation of an absence of other causes of death, which is necessary to confirm sudden, unexplained death in persons with epilepsy,19 is rare. We present mortality data from a cohort of 245 subjects with childhood-onset epilepsy who were followed for 40 years. Rates of autopsy in this cohort were high.
Me thods
Subjects and Study Design
The study population included all children young-er than 16 years of age who were living in the catchment area of Turku University Hospital, Turku, Finland, at the end of 1964 and who had epilepsy, which was defined as at least two un-provoked seizures. The subjects were identified from the files of Turku University Hospital, other hospitals and institutions in southern Finland, and private surgeons and from Finland’s National Health Service registry, which covers the entire population of that country. Of the 245 patients identified, the majority (223 patients) were seen in Turku University Hospital. In the 1960s, all pediatric patients who had one or more epileptic seizures were referred for inpatient hospital eval-uation. The study population has been described previously.20-22
The 245 subjects included 150 subjects with incident cases of epilepsy (61%) whose initial visit for the evaluation of new-onset seizures occurred between 1961 and 1964. The remaining 95 sub-jects with prevalent cases of epilepsy (39%) were seen before 1961, but they were seen again dur-ing the 1961−1964 study period for active epilepsy (at least one epileptic seizure during the preced-ing 3 years and a prior diagnosis of epilepsy). Ex-cluded were children who had febrile seizures only or other acute symptomatic seizures and children with a single unprovoked seizure. Also excluded were children with an onset of epilepsy before 1961 who were either in remission or who died before 1961.
A follow-up examination was performed every fifth year up to 2002. Data on deaths were ob-tained from continuous follow-up of the patients
in the intervals between the 5-year examinations. Detailed information collected about this sub-group included the date and time of death, the immediate cause of death, the underlying cause of death, and autopsy data, when available. Writ-ten informed consent obtained from all subjects or their caregivers permitted access to the hospi-tal files in order to abstract data on the last stages of the disease before death. To ensure full cover-age of all deaths, we also sent a list of the names of all 245 subjects (and their unique identification numbers), except those known to be dead, to the Finnish National Death Register every 5 years and requested a list of deaths and copies of the death certificates. Five subjects migrated out of Finland and were last known to be alive 10, 19, 25, 32, and 36 years after the onset of epilepsy. Complete data until death or January 1, 2003, were avail-able for all the remaining subjects. The median duration of follow-up to the last follow-up contact or death was 40.0 years (range, 2 to 53) among all 245 subjects and 39.5 years (range, 2 to 42) among the 150 subjects with incident cases of epilepsy. The joint ethics review committee of the Univer-sity of Turku Medical School and University Hos-pital of Turku approved the study design.
Data on autopsies performed for clinical or forensic reasons, or both, were available for this study. The autopsy rate was 70% (42 of 60 deaths) for all deaths in the cohort and 80% (24 of 30 deaths) for incident cases. Full autopsies of all or-gans were performed, although in a few subjects, a less detailed forensic autopsy was performed. The results of toxicologic screening were obtained in all subjects. Of the six subjects with incident cases of epilepsy who were not examined at au-topsy, two had malignant, aggressive carcinoma and permission for an autopsy was not given by the subjects’ relatives; two had severe cognitive impairment, were completely bedridden, and died of pneumonia; one had progressive muscular dys-trophy with pneumonia; and one, who had mod-erate cognitive impairment, died after an epilep-tic seizure.
Definitions
Epileptic syndromes, epilepsies, epileptic seizures, and the causes of seizures were defined accord-ing to the guidelines for epidemiologic research of the International League Against Epilepsy.23-25 Subjects with remote symptomatic epilepsy had either a major neurologic impairment (e.g., cog-
The New England Journal of Medicine Downloaded from nejm.org on October 20, 2015. For personal use only. No other uses without permission.
Copyright © 2010 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 363;26 nejm.org december 23, 20102524
nitive impairment, clinically significant develop-mental delay [developmental quotient <70 in chil-dren younger than 7 years of age], cerebral palsy, or autism) or a history of a major neurologic in-sult (e.g., head trauma, stroke, or meningitis). The remaining subjects were determined to have cryp-togenic or idiopathic epilepsy. The classification of epilepsy was made in all subjects, and the de-tailed seizure types and epilepsy syndromes in this cohort have been reported previously.22 These clas-sifications were determined before the new clas-sifications of epilepsy syndromes26 and are used here for consistency with previous studies.
Sudden, unexpected death in a person with epilepsy was defined, in accordance with the defi-nition by Annegers,19 as sudden death with no evidence of a seizure and no other identified cause of death, with confirmation of these findings by autopsy. In almost all cases of sudden, unex-plained death in a person with epilepsy, pulmo-nary edema was detected on autopsy. We also ex-amined the rates of sudden, unexplained death among persons with epilepsy in accordance with the alternative definition by Nashef,27 which includes deaths for which there is evidence of probable or definite seizures, although it excludes deaths in persons with known status epilepticus.
Statistical Analysis
Our statistical methods took into account the time-dependent nature of the mortality data. The rate of death was calculated as the number of deaths divided by the person-years at risk during the study; direct adjustment for age and sex was per-formed on the basis of the 2002 Finnish popula-tion. The product-limit method was used to cal-culate the risk of death from the onset of epilepsy.28,29 Data on subjects were censored at the time of the last follow-up or on January 1, 2003. Standard errors and 95% confidence inter-vals were calculated with the use of a modifica-tion of the Greenwood formula.29 Univariate and multivariate analyses were performed with the use of the Cox proportional-hazards model, and re-mission status was treated as a time-dependent co-variate.29-31 Rates of death according to remission status were adjusted for the number of person-years at risk during the remission period. Rate ratios with 95% confidence intervals were calcu-lated with the use of the Cox regression models. When the cohort with incident epilepsy and the cohort with prevalent epilepsy were combined, ad-justment was made for the left truncation due to the delayed entry of the cohort with prevalent epi-lepsy.32 A direct age- and sex-adjusted standard
Table 1. Mortality among Subjects with Childhood-Onset Epilepsy.*
VariableAll Subjects
(N = 245)
Subjects with Idiopathic or Cryptogenic Epilepsy
(N = 122)
Subjects with Epilepsy Due to Remote Symptomatic Causes
(N = 123)†
Total deaths — no. 60 15 45
Age at death — yr
Median 23 26 21
Range 1–50 11–50 1–49
No. of person-yr 8692 4638 4054
No. of deaths/1000 person-yr (95% CI)
All 6.90 (5.3–8.9) 3.23 (1.9–5.4) 11.10 (8.3–14.9)
Men 7.33 (5.2–10.2) 2.69 (1.2–6.0) 11.63 (8.0–16.8)
Women 6.41 (4.4–9.4) 3.74 (1.9–7.2) 10.33 (6.4–16.6)
Remission status at time of death‡
Not in remission — no./total no. of deaths (%) 51/60 (85) 11/15 (73) 40/45 (89)
In remission — no./total no. of deaths (%) 9/60 (15) 4/15 (27) 5/45 (11)
Receiving medication — no. 5 2 3
Not receiving medication — no. 4 2 2
* CI denotes confidence interval.† A remote symptomatic cause of epilepsy indicates epilepsy associated with a major neurologic abnormality or insult.‡ A total of 107 subjects in the study cohort were not in 5-year terminal remission, and 138 were in 5-year terminal remission; of the 138 sub-
jects in 5-year terminal remission, 35 were receiving medication and 103 were not.
The New England Journal of Medicine Downloaded from nejm.org on October 20, 2015. For personal use only. No other uses without permission.
Copyright © 2010 Massachusetts Medical Society. All rights reserved.

Mortality in Childhood-Onset Epilepsy
n engl j med 363;26 nejm.org december 23, 2010 2525
mortality ratio was calculated; this was defined as the ratio of the number of deaths observed in the study group to the number that would be ex-pected if the age- and sex-specific rates of death in the study population were the same as those in the general population of the study area from 1945 through 2002.31,33 The standard mortality ratio adjusted for age, sex, and time period was calculated with the use of 5-year periods for 5-year age groups, and 95% confidence intervals were determined. The case fatality rate was defined as the proportion of persons who died during follow-up. Statistical computations were performed with the use of SAS software, version 9.1.3 (SAS In-stitute).
R esult s
Characteristics of the Study Population
A total of 245 subjects, 150 with incident cases of epilepsy and 95 with prevalent cases of epilepsy, were included in the study. The median age at the onset of epilepsy was 3 years (range, 0 to 14) among subjects with incident cases of epilepsy and 2 years (range, 0 to 12) among subjects with prevalent cases of epilepsy. A total of 122 sub-jects had idiopathic or cryptogenic epilepsy, and 123 subjects had remote symptomatic epilepsy (i.e., epilepsy associated with a major neurologic
abnormality or insult). The median duration of epi-lepsy before achieving 5-year long-term remission was 17 years (range, 1 to 52) for surviving sub-jects and 22 years (range, 1 to 50) for those who died during the follow-up period. At the time of the last follow-up contact or death, 110 patients (45%) were in 5-year terminal remission and were not receiving medication, 28 (11%) were in 5-year terminal remission and were receiving medica-tion, and 107 (44%) were not in 5-year remission.
Overall Mortality
During the median follow-up period of 40 years, 60 subjects died, for an overall case fatality rate of 24% and a rate of death of 6.9 per 1000 per-son-years among all subjects (Table 1). The rates of death among the subjects with incident cases of epilepsy (5.3 per 1000 person-years) and those with prevalent cases (9.6 per 1000 person-years) did not differ significantly, and the two groups were therefore combined. Details on incident cas-es are included in the Supplementary Appendix, available with the full text of this article at NEJM .org. The age- and sex-adjusted rates of death were 7.2 per 1000 person-years, with standard mortal-ity ratios of 5.5 (95% confidence interval [CI], 4.6 to 6.6) in incident cases and 6.4 (95% CI, 5.9 to 7.0) in the overall cohort; the latter ratio is an es-timate and was not adjusted for the delayed entry
Table 2. Causes of Death.
VariableAll Subjects
(N = 245)
Subjects with Idiopathic or Cryptogenic Epilepsy
(N = 122)
Subjects with Epilepsy Due to Remote Symptomatic Causes
(N = 123)*
Total deaths — no. 60 15 45
Death related to epilepsy — no./total no. of deaths (%)
33/60 (55) 9/15 (60) 24/45 (53)
Witnessed seizure — no. 6 0 6
Status epilepticus — no. 4 0 4
Probable seizure — no. 3 2 1
Drowning — no. 6 0 6
Sudden, unexplained death — no. 18 7 11
Death not related to epilepsy — no./ total no. of deaths (%)
26 (43) 6 (40) 20 (44)
Pneumonia — no. 12 0 12
Cardiovascular disease — no. 8 2 6
Suicide — no. 2 2 0
Other cause of death — no. 4 2 2
Cause of death unknown — no. 1 0 1
* A remote symptomatic cause of epilepsy indicates epilepsy associated with a major neurologic abnormality or insult.
The New England Journal of Medicine Downloaded from nejm.org on October 20, 2015. For personal use only. No other uses without permission.
Copyright © 2010 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 363;26 nejm.org december 23, 20102526
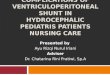
of subjects with prevalent cases of epilepsy. The causes of death and their relationship to remis-sion status and cause of epilepsy are summarized in Tables 1 and 2. The highest rate of death oc-curred among subjects who were not in 5-year ter-minal remission; only 4 deaths occurred in the 103 subjects in 5-year terminal remission who were not receiving medication at the time of death or the last follow-up contact (1.5 deaths per 1000 person-years), as compared with 5 deaths in 35 subjects in 5-year remission who were receiving medication (11.8 per 1000 person-years) and 51 deaths in the 107 subjects who were not in 5-year remission (15.9 per 1000 person-years) (P<0.001). As expected, the rates of death were significantly higher among subjects with epilepsy due to remote symptomatic causes (11.1 deaths per 1000 person-years) than among subjects with cryptogenic epi-lepsy (2.9 per 1000 person-years) and those with idiopathic epilepsy (3.5 per 1000 person-years) (P<0.001) (Fig. 1 and Table 1). More than three quarters of the deaths occurred in subjects who were not in 5-year terminal remission and in the groups with epilepsy due to remote symptomatic causes; these included 21 of the 26 deaths not directly related to epilepsy and 24 of the 33 deaths related to epilepsy. The difference in the rates of death between subjects with epilepsy due to re-mote symptomatic causes and subjects with idio-pathic or cryptogenic epilepsy was significant (11.1 deaths per 1000 person-years vs. 3.2 per 1000 per-son-years, P<0.001).
Deaths in childhood occurred primarily in the group of subjects with epilepsy due to remote symptomatic causes and were most often related not to epilepsy but to the underlying disease (Ta-ble 1). Deaths due to epilepsy-related causes in subjects with cryptogenic or idiopathic epilepsy occurred primarily in adolescence and adulthood. The risk factors for both overall death and epilep-sy-related death are summarized in Table 3. Uni-variate analysis showed that the hazard ratio for death was significantly increased among subjects who were not in 5-year terminal remission, those with a remote symptomatic cause of epilepsy, and those with a history of status epilepticus. Within the group of patients with remote symptomatic epilepsy, severe cognitive impairment was asso-ciated with an increased mortality (rate ratio, 4.1; 95% CI, 2.0 to 8.3; P<0.001). On multivariable analysis, only 5-year terminal remission was sig-nificantly associated with the hazard ratio for death. The other variables have previously been shown to be associated with a lack of remis-sion.20-22 Other factors, such as the type of epi-lepsy (localization-related epilepsy, temporal-lobe epilepsy, or another type of epilepsy) or cere-bral palsy, did not influence the risk of death in the group of subjects with remote symptomatic epilepsy.
Causes of Death
The causes of death are listed in Table 2. Among the 60 patients who died, the cause of death was not directly related to the seizure disorder but instead was related to the underlying neurologic problem or to another disease in 26 patients (43%) and was related to the epilepsy in 33 patients (55%); the latter group included sudden, unex-plained death in epilepsy in 18 patients (30%), probable or definite seizure in 9 (15%), and ac-cidental drowning in 6 (10%). With the use of the alternative classification of sudden, unexplained death in epilepsy,27 which includes possible or definite seizures as long as the seizures were not status epilepticus, 38% of the deaths were due to sudden, unexplained death in epilepsy, 7% were due to status epilepticus, and 10% were due to accidental drowning.
Sudden, Unexplained Death and Epilepsy-Related Deaths
There were 18 cases of sudden, unexplained death,19 including 15 cases that were confirmed by autopsy. Seven of the subjects with sudden,
Cum
ulat
ive
Rat
e of
Dea
th
50
30
40
20
0
10
0 5 10 15 20 35 4025 30
Years after the Onset of Epilepsy
Remote symptomatic cause
Idiopathic or cryptogenic cause
Figure 1. Cumulative Rate of Death According to Cause of Epilepsy.
A remote symptomatic cause indicates epilepsy that is associated with a major neurologic abnormality or insult.
The New England Journal of Medicine Downloaded from nejm.org on October 20, 2015. For personal use only. No other uses without permission.
Copyright © 2010 Massachusetts Medical Society. All rights reserved.

Mortality in Childhood-Onset Epilepsy
n engl j med 363;26 nejm.org december 23, 2010 2527
unexplained death had idiopathic or cryptogenic epilepsy, and 11 had epilepsy due to remote symp-tomatic causes. The median age at death among the subjects with sudden, unexplained death was 25 years (range, 4 to 49) overall, 27 years (range, 13 to 48) among subjects with idiopathic or cryp-togenic epilepsy, and 23 years (range, 4 to 49) among those with epilepsy due to remote symp-tomatic causes. Although there were two cases of probable sudden, unexplained death among chil-dren 6 and 8 years of age with remote symptom-atic epilepsy, all cases of sudden, unexplained death in the group with cryptogenic or idiopath-ic epilepsy occurred in adolescents and adults (Table 3). With the use of the alternative defini-tion of sudden, unexplained death in epilepsy,27 there were 23 cases, 17 of which were confirmed by autopsy.
Over the 40-year follow-up period, the risk of sudden, unexplained death among subjects with epilepsy was 7% (95% CI, 5 to 12) among all subjects and 12% (95% CI, 8 to 20) among those who were not in 5-year terminal remission and who were not receiving medication (Fig. 2). Among subjects with idiopathic or cryptogenic epilepsy,
the risk of sudden, unexplained death19 was 5% (95% CI, 2 to 11) overall, and the risk was 15% (95% CI, 7 to 31) among subjects who were not in 5-year terminal remission and no longer receiv-ing medication. On univariate analysis, the ab-sence of terminal remission and a history of sta-tus epilepticus, but not a remote symptomatic cause or a localization-related epilepsy syndrome, were associated with an increased risk of sudden, unexplained death among subjects with epilepsy (Table 3). On multivariate analysis, only the ab-sence of 5-year terminal remission was signifi-cantly associated with sudden, unexplained death.
The hazard ratios for all epilepsy-related deaths are shown in Table 3. Not surprisingly, these ratios are similar to those of sudden, unexplained death among subjects with epilepsy. According to the alternative Nashef criteria,27 most of the epilepsy-related deaths would qualify as sudden, unexplained death in subjects with epilepsy.
Discussion
The strength of this study is that it involves a co-hort that was prospectively followed for 40 years,
Table 3. Predictors of Death.*
Risk Factor Univariate Analysis Multivariate Analysis
Hazard Ratio (95% CI) P Value
Hazard Ratio (95% CI) P Value
All deaths
Absence of 5-yr terminal remission 5.3 (2.6−11.0) <0.001 4.7 (1.5−14.9) 0.007
Remote symptomatic cause of epilepsy 3.4 (1.9−6.1) <0.001 1.5 (0.7−3.6) 0.31
Prior status epilepticus 1.9 (1.2−3.2) 0.01 1.5 (0.7−3.0) 0.28
Age at onset <2 yr 1.4 (0.8−2.3) 0.20 1.7 (0.8−3.5) 0.13
Epilepsy-related deaths
Absence of 5-yr terminal remission 6.4 (2.2−18.8) <0.001 4.7 (1.5–14.9) 0.007
Remote symptomatic cause of epilepsy 3.1 (1.4−6.7) 0.004 1.5 (0.7−3.6) 0.31
Prior status epilepticus 2.1 (1.1−4.2) 0.03 1.5 (0.7−3.0) 0.28
Age at onset <2 yr 1.9 (0.96−3.8) 0.06 1.7 (0.8−3.5) 0.13
Sudden, unexplained deaths
Absence of 5-yr terminal remission 5.2 (1.4−18.5) 0.01 5.0 (1.2−20.1) 0.02
Prior status epilepticus 2.8 (1.1–7.0) 0.03 2.6 (0.9−7.5) 0.07
Age at onset <2 yr 2.1 (0.8−5.5) 0.11 1.9 (0.7−5.2) 0.20
Remote symptomatic cause of epilepsy 1.9 (0.7−4.8) 0.20 0.8 (0.3−2.4) 0.72
Localization-related epilepsy 0.8 (0.3−2.0) 0.60 0.5 (0.2−1.5) 0.21
* A Cox proportional-hazards model was used to assess the risk of death associated with an absence of 5-year terminal remission, with remission status treated as a time-dependent covariate. A remote symptomatic cause of epilepsy indi-cates epilepsy associated with a major neurologic abnormality or insult. CI denotes confidence interval.
The New England Journal of Medicine Downloaded from nejm.org on October 20, 2015. For personal use only. No other uses without permission.
Copyright © 2010 Massachusetts Medical Society. All rights reserved.

T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 363;26 nejm.org december 23, 20102528
with complete ascertainment of death and a high rate of autopsy-confirmed causes of death. With the longer follow-up, the epilepsy-related mortal-ity is substantially higher than that reported in the original 1998 study (33% vs. 20%).20 Also, classification of the causes of death with the use of the autopsy data and the more formal defini-tions of sudden, unexplained death in subjects with epilepsy also greatly increase the number of cases. The reclassification substantially changes the picture of epilepsy-related mortality in this cohort. Frequent causes of death in Finland in persons between birth and 54 years of age in 2002 were accidents (accounting for 24.0 deaths per 100,000 persons), vascular causes (18.0 per 100,000), suicide (13.3 per 100,000), gynecologic cancer (4.0 per 100,000), and congenital malfor-mations (1.6 per 100,000).
The increased risk of death associated with childhood-onset epilepsy that we observed was substantial and persisted into adulthood. The in-creased risk was limited to subjects who were not in terminal remission and those who had another neurologic disability, particularly severe cognitive impairment. The most important risk factor for death from any cause as well as for epilepsy- related death specifically was the absence of 5-year terminal remission. By definition, epilepsy-related deaths occurred exclusively in subjects who were not in 5-year terminal remission. Univariate analy-
sis showed that the absence of 5-year terminal remission, a remote symptomatic cause (epilepsy associated with a major neurologic abnormality or previous insult), severe cognitive impairment, and a history of status epilepticus also were sig-nificant predictors of death; multivariate analy-sis showed that only the absence of 5-year termi-nal remission remained an important predictor. It is somewhat surprising that other factors known to be associated with increased mortality among patients with epilepsy did not emerge as risk factors. Severe cognitive impairment has been associated with an increased risk of sudden, un-explained death among subjects with epilepsy, even after adjustment for seizure frequency in a group with active epilepsy.3,34 The most likely ex-planation for an absence of this association in our cohort is that the more severely affected chil-dren in the symptomatic group were also less likely to have seizure-free remission. Deaths un-related to seizures occurred primarily in the symp-tomatic group, and in the group with idiopathic or cryptogenic epilepsy, such deaths occurred at a much older age.
We had considerable data on and autopsy con-firmation of the majority of epilepsy-related deaths. Depending on which of the two definitions was used,10,18 sudden, unexplained death occurred in up to 9% of the entire cohort. This number, how-ever, included subjects who had been in remission for many years without receiving medication. The risk of sudden, unexplained death among sub-jects with epilepsy who were not in 5-year termi-nal remission was substantially higher. Given our 40-year follow-up period, it is likely that we have ascertained most of the cases of sudden, unex-plained death that will occur in this cohort, since the peak age period for sudden, unexplained death in patients with epilepsy is generally between 20 and 40 years of age,4,33 and after 50 years of age, it can become difficult to make this classifica-tion with certainty. Other studies of childhood-onset epilepsy with shorter periods of follow-up have shown that among children with idiopathic or cryptogenic epilepsy, the rate of death is no different from that in the general population, and in childhood, mortality is increased only among subjects with remote symptomatic epilepsy.5-9 However, in studies involving adults with sudden, unexplained death, the onset of epilepsy in child-hood is often a risk factor.34-36 In this study, there were no cases of sudden, unexplained death
Cum
ulat
ive
Ris
k of
Dea
th
0.5
0.3
0.4
0.2
0.0
0.1
0 5 10 15 20 35 4025 30
Years after the Onset of Epilepsy
All epilepsy-related deaths
Sudden, unexplained deaths
Figure 2. Cumulative Risk of All Epilepsy-Related Deaths and Sudden, Unexplained Deaths in Subjects with Epilepsy.
Data shown are for patients at risk (i.e., receiving medication, with or with-out 5-year terminal remission).
The New England Journal of Medicine Downloaded from nejm.org on October 20, 2015. For personal use only. No other uses without permission.
Copyright © 2010 Massachusetts Medical Society. All rights reserved.

Mortality in Childhood-Onset Epilepsy
n engl j med 363;26 nejm.org december 23, 2010 2529
among children younger than 14 years of age who had idiopathic or cryptogenic epilepsy; however, the risk of sudden, unexplained death and other epilepsy-related deaths was relatively high among adults with active epilepsy.
Our data alone do not provide support for ag-gressive treatment to prevent sudden, unexplained death in patients with epilepsy. However, studies of epilepsy surgery in adults with medically re-fractory partial epilepsy have shown that the rates of sudden, unexplained death are substantially
lower among those who become seizure-free after surgery than among those who do not,35 sug-gesting that the risk is potentially modifiable.
Supported by a grant from the Finnish Epilepsy Research Foundation.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
We thank Hannu Kalimo, M.D., Ph.D., professor of neuropa-thology, and Pekka Saukko, M.D., Ph.D., professor of forensic medicine, for collecting the autopsy data; Hans Helenius, M.Sc., for statistical advice; Olli Kaleva, B.A., for computations; and Dale Hesdorffer, Ph.D., for her constructive suggestions.
References
1. Leestma JE, Walczak T, Hughes JR, Kalelkar MB, Teas SS. A prospective study on sudden unexpected death in epilepsy. Ann Neurol 1989;26:195-203.2. Lhatoo SD, Johnson AL, Goodridge DM, MacDonald BK, Sander JW, Shorvon SD. Mortality in epilepsy in the first 11 to 14 years after diagnosis: multivariate analy-sis of a long-term, prospective, population-based cohort. Ann Neurol 2001;49:336-44.3. Walczak TS, Leppik IE, D’Amelio M, et al. Incidence and risk factors in sudden unexpected death in epilepsy: a prospective cohort study. Neurology 2001;56:519-25.4. Ficker DM, So EL, Shen WK, et al. Population-based study of the incidence of sudden unexplained death in epilepsy. Neurology 1998;51:1270-4.5. Zielinski JJ. Epilepsy and mortality rate and cause of death. Epilepsia 1974; 15:191-201.6. Hauser WA, Annegers JF, Elveback LR. Mortality in patients with epilepsy. Epilepsia 1980;21:399-412.7. Cockerell OC, Johnson AL, Sander JW, Hart YM, Goodridge DM, Shorvon SD. Mortality from epilepsy: results from a prospective population-based study. Lan-cet 1994;344:918-21.8. Cockerell OC, Johnson AL, Sander JW, Shorvon SD. Prognosis of epilepsy: a review and further analysis of the first nine years of the British National General Practice Study of Epilepsy, a prospective popula-tion-based study. Epilepsia 1997;38:31-46.9. Derby LE, Tennis P, Jick H. Sudden unexplained death among subjects with re-fractory epilepsy. Epilepsia 1996;37:931-5.10. Tennis P, Cole TB, Annegers JF, Leest-ma JE, McNutt M, Rajput A. Cohort study of incidence of sudden unexplained death in persons with seizure disorder treated with antiepileptic drugs in Saskatchewan, Canada. Epilepsia 1995;36:29-36.11. Shackleton DP, Westendorp RGJ, Trenité DGA, Vandenbroucke JP. Mortali-ty in patients with epilepsy: 40 years of follow up in a Dutch cohort study. J Neu-rol Neurosurg Psychiatry 1999;66:636-40.
12. Brorson LO, Wranne L. Long-term prognosis in childhood epilepsy: survival and seizure prognosis. Epilepsia 1987;28: 324-30.13. Berg AT, Shinnar S, Testa FM, Levy SR, Smith SN, Beckerman B. Mortality in childhood-onset epilepsy. Arch Pediatr Adolesc Med 2004;158:1147-52.14. Shinnar S, O’Dell C, Berg AT. Mortal-ity following a first unprovoked seizure in children: a prospective study. Neurology 2005;64:880-2.15. Callenbach PMC, Westendorp RGJ, Geerts AT, et al. Mortality in children with epilepsy: the Dutch Study of Epilepsy in Childhood. Pediatrics 2001;107:1259-63.16. Camfield CS, Camfield PR, Veugelers PJ. Death in children with epilepsy: a popu-lation-based study. Lancet 2002;359:1891-5.17. Donner EJ, Smith CR, Snead OC III. Sudden unexplained death in children with epilepsy. Neurology 2001;57:430-4.18. Nashef L, Fish DR, Garner S, Sander JW, Shorvon SD. Sudden death in epilep-sy: a study of incidence in a young cohort with epilepsy and learning difficulty. Epi-lepsia 1995;36:1187-94.19. Annegers JF. United States Perspec-tive on Definitions and Classifications. Epilepsia 1997;38:Suppl:S9-S12.20. Sillanpää M, Jalava M, Kaleva O, Shin-nar S. Long-term prognosis of seizures with onset in childhood. N Engl J Med 1998;338:1715-22.21. Sillanpää M, Shinnar S. Status epilep-ticus in a population-based cohort with childhood-onset epilepsy in Finland. Ann Neurol 2002;52:303-10.22. Sillanpää M, Jalava M, Shinnar S. Epi-lepsy syndromes in patients with child-hood-onset seizures in Finland. Pediatr Neurol 1999;21:533-7.23. Commission on Epidemiology and Prognosis, International League Against Epilepsy. Guidelines for epidemiologic stud-ies on epilepsy. Epilepsia 1993;34:592-6.24. Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for revised
clinical and electroencephalographic clas-sification of epileptic seizures. Epilepsia 1981;22:489-501.25. Idem. Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsia 1989;30:389-99.26. Berg AT, Berkovic SF, Brodie MJ, et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE Commission on Clas-sification and Terminology, 2005-2009. Epilepsia 2010;51:676-85.27. Nashef L. Sudden unexpected death in epilepsy: terminology and definitions. Epilepsia 1997;38:Suppl:S6-S8.28. Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958;53:457-81.29. Elandt-Johnson RC, Johnson NL. Sur-vival models and data analysis. New York: John Wiley, 1980:150-80.30. Cox DR. Regression models and life-tables. J R Stat Soc [B] 1972;34:187-220.31. Fleiss JL, Levin B, Cho Paik M. Statisti-cal methods for rates and proportions. 3rd ed. Hoboken, NJ: John Wiley, 2003:638.32. Foreman AJ, Lai GP, Miller DP. Sur-viving left truncation using PROC PHREG. In: SAS/STAT user’s guide, ver-sion 9. Cary, NC: SAS Institute, 2003. (http://mayoresearch.mayo.edu/mayo/ research/biostat/sasmacros.cfm.)33. Central Statistical Office of Finland. Statistical yearbook of Finland. 2003. (http://pxweb2.stat.fi/sahkoiset_julkaisut/vuosikirja2004/2003/vkirja.pdf.)34. Tomson T, Walczk T, Sillanpää M, Sander JW. Sudden unexpected death in epilepsy: a review of incidence and risk factors. Epilepsia 2005;46:Suppl 11:54-61.35. Sperling MR, Feldman H, Kinman J, Liporace JD, O’Connor MJ. Seizure con-trol and mortality in epilepsy. Ann Neurol 1999;46:45-50.36. Nilsson L, Farahmand BY, Persson PG, Thiblin I, Tomson T. Risk factors for sud-den unexpected death in epilepsy: a case-control study. Lancet 1999;353:888-93.Copyright © 2010 Massachusetts Medical Society.
The New England Journal of Medicine Downloaded from nejm.org on October 20, 2015. For personal use only. No other uses without permission.
Copyright © 2010 Massachusetts Medical Society. All rights reserved.