Embed Size (px)
Citation preview

.
Overview & Update on the Utilization of theNatriuretic Peptides in Heart Failure
June 28, 2016
Linda C. Rogers, PhD, DABCC, FACB

Page 2Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
Agenda
• Overview of the Natriuretic Peptides and Efficacy studies• Similarities and Differences• Confounders• Clinical Studies of Entresto and Implications for
Measurement of the Natriuretic Peptides

Page 3Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
Cardiac Natriuretic Peptides
Physiological role:
• Natriuresis, i.e., discharge of sodium by urinary excretion
• Regulates blood volume through osmotic hemodynamics
Peptide Stimulus for ReleaseANP Atrial DistensionBNP Ventricular OverloadCNP Endothelial Stress
ANPANP
BNPBNP
CNP
Weber, et al. Heart 2006;92:843-9.

Page 4Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
Physiology of BNP control
Na+
Na+
Na+
Renin-angiotensin-aldosteronesystem (RAAS)
Weber, et al. Heart 2006;92:843-9.

Page 5Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.5 Unrestricted © Siemens Healthcare Diagnostics Inc. 2014 All rights reserved. Artifact #A91DX CAI-140459-UC1-4A00
BNP32 aa½ life = 20 minEnzymatic, receptor, and renal clearancePhysiologically active
NT-proBNP76 aa½ life = 120 minRenal clearancePhysiologically inactive
—COOH H2N
Cardiac myocyte
Natriuretic Peptides
Pre-proBNP (134 aa)
80
90
100
108—COOH
S P K M V Q G S GCF
CRK
M D R I S SSSG
LCC K V L R R H
Hemodynamic StressIschemia
CardiotoxicitySepsis
ProBNP (108 aa)
Blood stream
Enzymaticcleavage
Martinez-Rumayor et al. Am J Cardiol 2008;101[suppl]:3A-8ABoerrigter, et al. Heart Fail Clin. Oct 2009; 5(4): 501–514.
H2N1
10 70
76
H P L G S P G S A S Y T L R A P R
Signal peptide(26 aa)

Page 6Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
6 Siemens Healthcare Diagnostics
Elimination Paths of BNP and NT-proBNP Impacts Half Life
BNP NT-proBNP
Half-Life = 60 – 120 minutes
+ +
Half-Life = 20 minutesWeber, et al. Heart 2006;92:843-9.

Page 7Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
Decision Cut Points for Ruling Out Heart Failure
NT-proBNP BNP
Age < 75 yrs: ≤ 125 pg/mLAge ≥ 75 yrs: ≤ 450 pg/mL
< 100 pg/mL
These are the only accepted cut points,regardless of manufacturer.
Source: Siemens IFU’s

Page 8Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
BNP and NT-proBNP Physiology
Pre-proBNP
Dilation of the left ventricle increases cardiacpre-proBNP gene expression.
The amount of pre-proBNP released into thecirculation is directly proportional to the extentof heart wall stretch.
Thus, natriuretic peptide levels are an accuratereflection of the severity of heart failure.

Page 9Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
9 Siemens Healthcare Diagnostics
Breathing Not Proper Study: BNP
• BNP is a useful test to distinguish patients with heart failure from thosewithout heart failure.
• BNP is useful for both systolic and nonsystolic heart failure, even thoughnonsystolic heart failure diagnosis is more difficult to make and is ofternincorrectly excluded in the presence of normal left ventricular systolicfunction.
• BNP cannot reliably distinguish systolic dysfuncion from nonsystolicdysfunction: a measurement of left ventricular dysfunction is required tomake this distinction and guide therapy accordingly.
Maisel, et al. J Am Coll Cardiol. 2003;41:2010-7.

Page 10Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
10 Siemens Healthcare Diagnostics
PRIDE Study Supports the Clinical Utility of NT-proBNP
• NT-proBNP testing alone was superior to clinical judgment alone fordiagnosing acute CHF.
• NT-proBNP plus clinical judgment was superior to NT-proBNP or clinicaljudgment alone.
• NT-proBNP measurement is a valuable addition to standard clinicalassessment for the identification and exclusion of CHF in theemergency department setting.
Januzzi, Am J Cardiol 2005;95:948-954

Page 11Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.11 Unrestricted © Siemens Healthcare Diagnostics Inc. 2014 All rights reserved. Artifact #A91DX CAI-140459-UC1-4A00
a. McCullough PA, et al. Circulation. 2002;106:416-22.b. Januzzi JL, et al. Am J Cardiol. 2005;95:948-54.
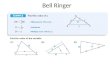
ROC Curves Estimating Clinical Probability of Heart Failure
1 − Specificity
BNP Studya PRIDE Studyb
Sen
sitiv
ity
0.0 0.60.4 0.8 1.00.20.00.1
0.3
0.6
0.40.5
0.70.80.91.0
0.2
0.0 0.60.4 0.8 1.00.20.00.1
0.3
0.6
0.40.5
0.70.80.91.0
0.2BNP + clinical assessment, AUC = 0.93 NT-proBNP + clinical assessment, AUC = 0.96
Clinical assessment alone, AUC = 0.86 Clinical assessment alone, AUC = 0.90
BNP alone, AUC = 0.90 NT-proBNP alone, AUC = 0.94

Page 12Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
12 Siemens Healthcare Diagnostics
Clinical Confounders to NP Interpretation
AFib
High BMICKD
Age-associated increases

Page 13Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
13 Siemens Healthcare Diagnostics
NP’s in CKD
• BNP and NT-proBNP were elevated in kidney dysfunction even in theabsence of systolic heart failure (SHF).
• NT-proBNP elevated more than BNP.
• Further research and association guidelines are necessary for clinicalguidance.
Jafri, et al. BMC Nephrol. 2013;14:117-26

Page 14Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
14 Siemens Healthcare Diagnostics
Impact of NPs in Patients with Renal Dysfunction and Dyspnea
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
> 89 89-60 59-30 < 30
NT-
proB
NP
(pg/
mL)
eGFR (mL/min/1.73m2)
0
250
500
750
1,000
1,250
1,500
1,750
2,000
2,250
> 89 89-60 59-30 < 30
BN
P(p
g/m
L)
eGFR (mL/min/1.73m2)
Chenevier-Gobeaux et al. Clin Chim Acta 2005;361:167-75.
NT-proBNPBNP
Non-cardiac dyspneaCardiac dyspnea
Manufacture decision cut-points are unchanged

Page 15Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
15 Siemens Healthcare Diagnostics
Natriuretic Peptides in Obese Patients with CHF
Krauser, et al. Am Heart J. 2005;149:744-50.
BNP
Weight Categories (BMI)
1000
500
2000
0
BN
P(p
g/m
L) 2500
3000
3500
1500
£ 25 25-29.9 ³ 30
p < 0.001NT-proBNP
£ 25 25-29.9 ³ 30Weight Categories (BMI)
NT-p
roBN
P(p
g/mL)
10000
5000
20000
0
25000
30000
15000
p < 0.001
Manufacture decision cut-points are unchanged

Page 16Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
16 Siemens Healthcare Diagnostics
1.01.3 1.5
2.6
1.0
2.0
2.9
4.5
0.0
0.51.01.52.0
2.53.03.54.04.5
5.0
Q1 Q2 Q3 Q4
Adj
uste
dR
isk
Rat
ion
BNP NT-proBNP
Association Between Natriuretic Peptides and 1-Year Mortality
N = 383
De Filippi, et al. Clin Chem 2007; 53:1511-19.
QuartileBNP
pg/mLNT-proBNP
pg/mLQ1 < 88 < 472Q2 88 – 333 472 – 1728Q3 334 – 800 1729 – 6000Q4 > 800 > 6000

Page 17Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
Comparing BNP versus NT-proBNP
Similarities DifferencesBoth show similar clinical diagnostic performancefor HF.
NT-proBNP appears more impacted by age(requiring age-specific cut-points).
Both demonstrate prognostic performance(although NT-proBNP may outperform BNP).
NT-proBNP has greater analytical stability (24hours at room temp vs. 4 hours for BNP and NT-proBNP may have greater stability when storedfrozen).
Studies for both suggest potential utility fortherapeutic monitoring.
Absolute values are very different due to alternatemechanisms of clearance.
Performance of both may be impacted by CKD(although NT-proBNP perhaps more so).
BNP values are typically in the hundreds whileNTproBNP can be in the thousands.
Both may have clinical utility outside of HF (likeACS).

Page 18Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
Intended Use
LCZ696*A combination of sacubitril, a neprilysin inhibitor, and valsartan,an angiotensin II receptor blocker, indicated to reduce the risk ofcardiovascular death and hospitalization for heart failure in patients withchronic heart failure (NYHA Class II–IV) and reduced ejection fraction.Usually administered in conjunction with other heart failure therapies,in place of an ACE inhibitor or other ARB.
*trade name Entresto
ACE: angiotensin-converting enzyme; ARB: angiotensin receptor blocker

Page 19Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
Mechanism of Action of LCZ696
ValsartanBlocks the angiotensin II type-1 (AT1) receptor, inhibitingangiotensin II and the release of aldosterone.
NeprilysinAn endopeptidase that breaks down vasoactive peptides(BNP, bradykinin, and adrenomedullin); its inhibition maytherefore reduce remodeling, vasoconstriction, and renalsodium retention and improve outcomes in HFrEF.
Inhibition of neprilysin by LBQ657, the active metaboliteof sacubitril, increases the levels of these peptides,decreasing vasoconstriction, sodium retention, andmaladaptive remodeling.
LCZ696
AngiotensinReceptor Blocker
Inhibitionof Neprilysin
SacubitrilValsartan

Page 20Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
The PARAMOUNT Trial
The angiotensin receptor-neprilysin inhibitor LCZ696 in heart failure withpreserved ejection fraction: a phase 2 double-blind randomized controlled trial.
Prospective comparison of ARNI (angiotensin receptor-neprilysin inhibitor)with ARB (angiotensin receptor blocker) on Management Of heart failUre withpreserved ejectioN fracTion (PARAMOUNT).
Solomon SD, Zile M, Pieske B, et al.Lancet. 2012;380(9851):1387–1395.

Page 21Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
PARAMOUNT Trial: Inclusion and Exclusion Criteria
Key Inclusion Criteria
• Age ≥40 years
• Documented stable chronic heart failure (NYHAII–IV) with signs and symptoms of HF (dyspnea onexertion, orthopnea, paroxysmal nocturnaldyspnea, peripheral edema)
• LVEF ≥45%
• Plasma NT-proBNP >400 pg/mL at screening
• On diuretic therapy prior to visit 1, controlledsystolic BP (<140 mmHg, or <160 mmHg ifon three meds)
• eGFR ≥30 mL/min/1.73 m2 (MDRD)
• Patients with a K ≤5.2 mmol/L at visit 1
Key Exclusion Criteria
• Patients with a prior LVEF <45% at ANY time
• Patients who required treatment with both an ACEinhibitor and an ARB
• Isolated right HF due to pulmonary disease
• Dyspnea and/or edema from noncardiac causes,such as lung disease, anemia, or severe obesity
• Presence of valvular heart disease, hypertrophiccardiomyopathy, infiltrative cardiomyopathy, restrictivecardiomyopathy, or pericardial disease
• Coronary disease requiring revascularizationduring the study

Page 22Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
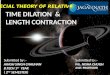
PARAMOUNT TrialPrimary Endpoint: Significant Reduction of NT-proBNP at 12 Weeks
HR = 0.77 (0.64–0.92)P = 0.005
• Patients with HFpEF taking ENTRESTO reducedNT-proBNP to a greater extent than valsartan after 12weeks of therapy.
• This reduction became evident at 4 weeks and wassustained to 36 weeks, although the between-groupdifference was no longer significant.
• There was also a reduction in left atrial size, indicative ofreverse left atrial remodeling and improvement in NYHAclass in patients randomly assigned to ENTRESTO after 36weeks compared with those randomly assigned tovalsartan.
• ENTRESTO was well tolerated.
• These findings suggest that ENTRESTO may havebeneficial effects in patients with HFpEF and that furthertesting of this drug may be warranted in patients with thiscondition.

Page 23Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
PARADIGM-HF Trial
N Engl J Med 2014; 371:e15September 11, 2014

Page 24Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
Aim of the PARADIGM-HF Trial
Prospective Comparison of ARNI with ACEI to Determine Impacton Global Mortality and Morbidity in Heart Failure Trial (PARADIGM-HF)
400 MG DAILY
Specifically designed to replace current use of ACE inhibitors and angiotensinreceptor blockers as the cornerstone of the treatment of heart failure.
ARNI: Angiotensin receptor-neprilysin inhibition; ACEI: angiotensin-converting enzyme inhibition
LCZ69620 MG DAILY
Enalapril

Page 25Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
PARADIGM-HF Trial Was Designed toShow Incremental Effect on Cardiovascular Death
Primary Endpoint
• Primary endpoint was cardiovascular death or hospitalizationfor heart failure, but PARADIGM-HF was designed as acardiovascular mortality trial.
• The sample size of the trial was determined by effect oncardiovascular mortality, not the primary endpoint.
• The Data Monitoring Committee was allowed to stop the trialonly for a compelling effect on cardiovascular mortality (inaddition to the primary endpoint).
• Difference in cardiovascular mortality of 15% betweenLCZ696 and enalapril was prospectively identified as beingclinically important.
Secondary Endpoints
• All-cause mortality.
• Change from baseline in the clinicalsummary score of the Kansas CityCardiomyopathy Questionnaire (KCCQ)at 8 months.
• Time to new onset of atrial fibrillation.
• Time to first occurrence of a protocol-defined decline in renal function.

Page 26Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
PARADIGM-HF
558 (13.3%)
693 (16.5%)
914 (21.8%)
1117 (26.5%)
N Engl J Med. 2014 Sep 11;371:e15.
HR = 0.80 (0.73–0.87)P = 0.0000002
Number needed to treat = 21
HR = 0.80 (0.71–0.89)P = 0.00004
Number needed to treat = 32

Page 27Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
537 (12.8%)
658 (15.6%)
711 (17.0%)
835 (19.8%)
PARADIGM-HF
N Engl J Med 2014; 371:e15September 11, 2014

Page 28Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
PARADIGM-HF: Cause of Death and Hospitalization Data
PARADIGM-HF Cause of Death and Hospitalization Datavs. Current Standard of Care ACEi Enalapril
McMurray et al. NEJM 2014;371:993–1004; Packer et al. Circulation 2015;131:54-61

Page 29Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
Change in KCCQ Score at 8 Months
LCZ696
Enalapril
LCZ696 improved the symptoms and physical limitationsof heart failure more than enalapril, p = 0.001.

Page 30Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
PARADIGM-HF: Conclusions
In comparison with guideline-recommended doses of an ACE inhibitor, combinedinhibition of both the angiotensin receptor and neprilysin was more effective not only inreducing all-cause and cardiovascular mortality, but also in reducing the risks and rates ofmultiple manifestations of clinical deterioration of surviving patients with heart failure. Theeffect of LCZ696 to stabilize the course of heart failure is likely to have importantramifications for both quality of life and resource utilization in this disorder.

Page 31Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
PARADIGM-HF Trial
Circulation. 2015;131:54–61.

Page 32Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
The Effect of LCZ696 on NT-proBNP and BNP
In contrast, in comparison with enalapril,patients receiving LCZ696 had consistentlylower levels of NT-proBNP (reflecting reducedcardiac wall stress) and troponin (reflectingreduced cardiac injury) throughout the trial.
The contrasting effects of LCZ696 on thetwo types of natriuretic peptides represent animportant finding, because the levels of thetwo peptides characteristically parallel eachother during the course of heart failure.
However, because BNP (but not NT-proBNP)is a substrate for neprilysin, levels of BNP willreflect the action of the drug, whereas levelsof NT-proBNP will reflect the effects of thedrug on the heart.
LCZ696 Enalapril

Page 33Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
Summary
PARAMOUNT Trial
• Patients with HFpEF taking ENTRESTO ascompared to valsartan reduced NT-proBNP to agreater extent than valsartan after 12 weeks oftherapy.
• This reduction became evident at 4 weeks and wassustained to 36 weeks, although the between-groupdifference was no longer significant.
• There was also a reduction in left atrial size,indicative of reverse left atrial remodeling andimprovement in NYHA class in patients randomlyassigned to ENTRESTO after 36 weeks comparedwith those randomly assigned to valsartan.
• ENTRESTO was well tolerated.
• These findings suggest that ENTRESTO may havebeneficial effects in patients with HFpEF and thatfurther testing of this drug may be warranted inpatients with this condition.
• ENTRESTO is not currently approved for treatmentof patients with HFpEF.
PARADIGM-HF Trial
• LCZ696 was more effective than enalapril for patients withHFrEF in reducing the risk of CV death and HFhospitalization, reducing the risk of CV death, reducingthe risk of HF hospitalization, reducing all-cause mortality,and incrementally improving symptoms and physicallimitations.
• LCZ696 was better tolerated than enalapril and less likelyto cause cough, hyperkalemia, or renal impairment.
• Less likely to be discontinued due to an adverse event.
• More hypotension, but no increase in discontinuations.
• Not more likely to cause serious angioedema.
• However, because BNP (but not NT-proBNP) is asubstrate for neprilysin, levels of BNP will reflect theaction of the drug, whereas levels of NT-proBNP willreflect the effects of the drug on the heart.
• ENTRESTO was FDA-approved to treat chronic HFpatients with reduced HFrEF.

Page 34Restricted © Siemens Healthcare Diagnostics Inc., 2015 All rights reserved.
• Linda C. Rogers, PhD, DABCC, FACBSenior Clinical Consultant
• Siemens Healthcare
• Scientific & Clinical Affairs
• Phone: (949)421-9101Email: [email protected]
Contact