Embed Size (px)
Citation preview

20200903_JudiciaryPresBook_FY2021
Palau JR Professional Bldg., Suite 2P.O. Box 10248Koror, Palau 96940Phone: (680) 488-7222Fax: (680) 488-7333
Web calvos.net
Saipan Oleai Center Bldg., San JoseP.O. Box 500035Saipan, MP 96950-0035Phone: (670) 234-5690/9Fax: (670) 234-5696
Guam 115 Chalan Santo PapaP.O. Box FJHagåtña, Guam 96932Phone: (671) 477-9808Fax: (671) 477-4141
Philippines 5th Floor, First Life Center174 Salcedo Street, Legaspi VillageMakati City, PhilippinesPhone: (632) 759-2871/813-1989Fax: (632) 759-3126
St. Luke’sMedical Center
Global City
Rm. 1008 10th FloorMedical Arts Building32nd St. Bonifacio Global CityTaguig City, 1112 PhilippinesPhone: (632) 555-0443/0448Fax: (632) 555-0438
St. Luke’sMedical Center
Quezon City
Rm. 716 7th Floor, North Tower Cathedral Heights Building ComplexSt. Luke’s Medical Center Compound#279 E. Rodriguez Sr. Avenue,Quezon City, PhilippinesPhone: (632) 413-1312Fax: (632) 413-5721
The Medical CityPasig City
Business Center, 9th FloorThe Medical City, Ortigas CenterPasig City, Philippines Phone: (632) 650-0589
Judiciary of GuamOpen EnrollmentFiscal Year 2021
Administered by

Blank Page

Buenas yan Hafa Adai!
We would like to welcome the Judiciary of Guam employees and dependents to our health plan. We look forward to servicing you for FY2021. The landscape of healthcare continues to evolve and we will continue to improve the benefits, services and medical networks available to you.
You are able to choose from two (2) plans: the PPO750 and the HSA2000.Below are some key features of the plans that will be available to you:
•Acomprehensiveandextensivemedicalnetwork
•WellnessRewardsprogram
•100%coverageforPreventiveServiceswithoutmeetingthedeductibleinaccordancewith the United States Preventive Services Task Force (USPSTF), Grade A and B recommendations
•100%Prenatalcarecoveragewithouthavingtomeetthedeductible
•Membership in theCalvo’sLifeStyleClub thatprovidesyounumerous savingsanddiscountsatpopular merchants on Guam
•50%AirAmbulancediscount(pre-approvalandlimitationsapply)
•$500TravelBenefittoParticipatingProvidersinthePhilippinesorinTaiwan (pre-approvalandlimitationsapply)
•AirfaretoourCentersofExcellenceforcertainqualifyingandpre-approvedconditions
Thank you for enrolling with Calvo’s SelectCare!
New business practices have been established such as video conferencing and webinars to better serve you while abiding to the current pandemic protocols. We also improved our web portal for easier interaction.Visitourwebsiteatcalvos.net,toobtainclaimpayments,explanationofbenefits,scheduleof benefits, and other pertinent information.
We encourage you to participate in our customer surveys as they are an important tool in evaluating and improving our services. We thank you in advance for your support and for the trust that you and your family have placed with us.
SiYu’osMa’ase!
We are pleased to announce that we have expanded our off-islandprovider network through a partnership with UnitedHealthcare.
You now have access to services all across the continental United States:1.1 million providers | 560 Centers of Excellence | 6,100 hospitals

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.
Eligibility InformationIn order to enroll in a Calvo’s SelectCare health plan, you and yourdependents must first meet the eligibility requirements defined in theagreementbetweenCalvo’sSelectCareandTheJudiciaryofGuam.
YoumustcompleteanEnrollmentApplicationandsubmititwithanyotherrequireddocumentationduringanOpenEnrollmentperiodorwithin30days from the date you first become eligible for enrollment under the plan.
Subscriber Eligibility Requirements• You must maintain legal residency in the Service Area. Calvo’s
SelectCaremembersmust not be absent from the Service Area formore than 90 consecutive days.
Dependent Eligibility RequirementsAsidefrommeetingtheeligibilityrequirementssetforthbyyouremployer,family members are eligible for coverage as dependents provided they are:
• Yourlegalspouse.
• Yourdomesticpartner:
• Adomesticpartnermustbeatleast18yearsofageandmusthavelived with you for two consecutive years. A notarized affidavit is required.
• A domestic partner may only be added during your employer’sOpenEnrollmentPeriodorwithin30daysfromthedateyoufirstbecome eligible to enroll in the plan.
• Childrenofadomesticpartnerareeligibleforcoveragesolongasthe domestic partner is a covered person.
• Marriedorunmarrieddependentchildrenundertheageof26years.
• Off-island Dependent children or children who reside outside theService area who are between the ages of 19 thru 25 years.
• Coverage for off-island dependent children will terminate uponreachingtheageof26years.
• Fornaturalchildrenwithadifferentlastnamefromyourown,youmustprovide the following:
• Acopyofthebirthcertificatewhichverifiesyouasaparent,or
• A notarized government Paternity Form which verifies you as anatural parent.
• Forotherdependentssuchasstepchildren,legallyadoptedchildren, and children you have been awarded legal guardianship, you must provide the following:
• BirthCertificate.
• Parents’marriagecertificate(whenrequired).
• LegalGuardianshipmustbefor“FullGuardianship”andnotlimitedor shared.A copyof theguardian’s latest income taxfilingor anaffidavitstatingthatthedependentwillbeincludedintheguardian’snexttaxfiling.
• Courtdocumentationsignedbyajudgeorderingadoptionorlegalguardianship.
• Legalguardianshipterminatesnolaterthanage26.
• Unbornchildrenawardedforlegalguardianshiparenoteligibleforcoverage.
• Your disabled dependent childwho is beyond the limiting agemaycontinuetobeeligibleprovidedtheyareincapableofself-sustainingemployment due to mental retardation or physical disability.
• Proofoftotaldisabilityfromalicensedmedicalphysicianisrequiredupon enrollment.
• Proofofdependence,suchasacopyofthesubscriber’staxfilingmayberequired.
Becoming a Member
• Q.M.C.S.O.oracopyofthequalifiedmedicalchildsupportordermustbeprovided.Childrenpermanently residingoutside the service areaareonlyeligibletoenrollintheplaniftheyqualifyundertheQ.M.C.S.O.
Enrollment PeriodYou may elect to enroll on any of these occasions.
• InitialEmployment.Youmayenrollwithin30daysfromthedateyoufirst become eligible to enroll in the plan.
• AnnualOpenEnrollmentPeriod.
• Special Enrollment Periods: Full-time employees and their eligibledependent(s) may enroll outside of open enrollment as a result of a QualifyingEventasdefinedbyH.I.P.A.A.UnderH.I.P.A.A.aQualifyingEventisaneventthatcausesyoutolosecoverageinanotherhealthplan due to:
•Terminationofspouse’scoverageordeathofyourspouse.
•Divorce,AnnulmentorLegalSeparationfromyourspouse.
•MedicareorMedicaideligibilityends.
A Special Enrollment opportunity also occurs if you acquire a newdependent through:•BirthorAdoption.•LegalGuardianship.•Marriage.
EnrollmentApplicationsorChangeofStatus(COS)Formsandanyrequireddocuments must be submitted within 30 days following a QualifyingEvent.IfyouhavelostcoverageinanotherhealthplanduetoaQualifyingEvent,youarealsorequiredtosubmitaH.I.P.A.A.CertificateofCreditableCoveragefromyourpreviousplan.YourpreviousplanisrequiredtoissueaH.I.P.A.A.Certificatetoyouinatimelymanner.
Your coverage will begin on the first day of the first Premium Period followingreceiptofyourEnrollmentApplicationbyCalvo’sSelectCare.
Formoreinformation,pleaserefertothe“SummaryofFederallyMandatedPrograms”sectionofyourMemberthisHandbook.
Adding Dependents and Changes to your CoverageYou are able to enroll your new dependent(s), if you get married, obtain legal guardianship, adopt a child or have a newborn baby as long as they meet theeligibility requirements.Coveragebeginson thefirstdayofaPremium Period, however, coverage for newborn dependents begins at birth, and coverage for adopted dependents begins on the actual date of custody of the dependent.
Ifyoudonotenrollyourdependentswithinthe30dayperiodfromwhenthey first become eligible, you would have to wait to enroll them during thenextOpenEnrollmentPeriod.
Toadddependents,you,asthesubscribermustnotifyCalvo’sSelectCarein the following manner:
• Completea“ChangeofStatus”Form(COS),
• Completea“HealthStatement”Form(whenrequiredbytheplan),
• SubmitallRequiredDocumentationasoutlinedabove,
• Makeyourrequestwithin30daysofyourdependentfirstbecomingeligible.
Updating Your InformationYour Enrollment Application contains pertinent information. Thisinformation is very important because it identifies you and your dependent(s) as eligiblemembers.Please informourCustomerServiceDepartment immediately of any error on yourMember ID Card or anychanges in name, address, phone numbers or email address.
1

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail. 2
Schedule of BenefitsJudiciary of Guam
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
$50 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
$40 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%of the total rental cost or purchase
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
At Primary Care$20 Member Co-Payment
At Specialist Care$40 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Not Covered
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Allergy Testing $500 per member per plan year
Ambulatory Surgi-center Care (Prior Authorization Required) Includes medically necessary anesthesia
Autism Spectrum Disorder CoverageReferral from Primary Care Physician and Prior Authorization from Plan is requiredCoverage is limited to the following maximums per member per benefit year:• $25,000 per benefit year for ages 16-21 years old • $75,000 per benefit year for ages 0-15 years old Services are subject to Plans benefit coverage guidelines and medical necessity
Blood & Blood Derivatives
Breast Reconstructive Surgery (In accordance with 1998 W.H.C.R.A) Includes medically necessary anesthesia
Cardiac Surgery Includes medically necessary anesthesia
Cardiac Rehabilitation (Inpatient)Up to 30 days following bypass surgery or myocardial infarction
Cataract SurgeryIncludes lens implants. Outpatient Only. Includes medically necessary anesthesia
Chemotherapy Benefit
Chiropractic Care
Clinical TrialsIncludes phases I-IV outpatient or inpatient clinic trials that are conducted in relation to treatment of cancer or otherlife-threatening diseases or conditions as approved by the National Institute of Health or the National Cancer Institute
Complex Diagnostic TestingMRI, CT scan, and other diagnostic procedures (Prior Authorization Required)
Durable Medical Equipment (DME)The lesser amount between the Purchase or Rental of crutches, walkers, wheelchairs, hospital beds, suction machines,CPAP machines, BPAP machines, insulin pumps, blood glucose monitors, oxygen and accessories when prescribed by a Physician (Prior Authorization Required)
Elective Surgery (Prior Authorization Required) Includes medically necessary anesthesia
End Stage Renal Disease / Hemodialysis
Foot Care (subject to benefit limitations)Foot Care and Podiatry services
Growth Hormone Therapy
Hearing AidsMaximum $1,000 per member per 24 months. Limited to 1 device every 3 years
Hearing Services
Hospitalization & Inpatient Benefits1. Room & Board for a semi-private room, intensive care, coronary care and surgery2. All other inpatient hospital services including laboratory, x-ray, operating room, anesthesia and medication3. Physician’s hospital services 4. Mental Health and Substance Abuse Admission
Hyperbaric Oxygen Therapy & Wound CareMedically necessary (Prior Authorization Required)
Implants, Orthotics & Prosthetic DevicesCardiac pacemakers, Intraocular lenses, artificial eyes, heart valves, orthopedic internal prosthetic devices, stents, stump hose,cochlear implants, corrective orthopedic appliances and braces (Limitations apply, please refer to contract)
Inhalation Therapy
Infertility Services Diagnosis of Infertility
Maternity Care Labor and Delivery
Nuclear Medicine (Prior Authorization Required)
Occupational Therapy (Prior Authorization Required)
Your Benefits: What the plan covers Participating Providers Non-participating Providers
Deductible Per Individual Member (Class 1)
Deductible Per Family (Classes 2-4)If a member meets their $2,600 deductible, the plan begins to pay for covered services for that individual
Coverage MaximumsIndividual member annual maximum
Out of Pocket Maximums (includes deductible and co-payments)Per Individual member per policy yearPer Family per policy yearMedical and Prescription Out of Pocket Maximums are combined
O�-Island ServicesAny services in the Philippines, Asia, Hawaii, U.S. Mainland and any other foreign participating providers
$2,000
$4,000
None
$4,000$11,900
**$4,000
**$12,000
None
No MaximumNo Maximum
Prior Authorization from your doctor and approval from the Plan is required prior to services rendered at o�-island facilities. Covered benefits at
Participating Philippine Providers are payable 100% after deductible is met
Plan pays 80%, Member pays 20%
Plan pays 80% for the first 20 visits and 50% thereafter
Member pays 10%Member pays 20%Member pays 30%Member pays 30%
$0 Member Co-Payment$0 Member Co-Payment
Member pays 30%Member pays 30%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 100%
Plan pays 80%, Member pays 20%
Member pays all costs above $500Limited to once per plan year
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Member pays 30% of Average Wholesale Price (AWP) plus
any di�erence betweeneligible and billed charges
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Not Covered
Oral and Maxillofacial SurgeryOral surgical procedures, limited to:• Reduction of fractures of the jaws or facial bones• Surgical correction of cleft lip, cleft palate or severe functional malocclusion• Removal of stones from salivary ducts• Excision of leukoplakia or malignancies• Excision of cysts and incision of abscesses when done as independent procedures• Other surgical procedures that do not involve teeth or their supporting structures
Physical Therapy(Prior Authorization Required)
Prescription DrugsRetail Pharmacy (30-day supply)1. Formulary generic drugs per prescription unit 2. Formulary brand name drugs per prescription unit 3. Non-Formulary (Medically Necessary Only and Prior Authorization Required)4. Specialty Drugs (Medically Necessary Only and Prior Authorization Required)
Mail Order Pharmacy (90-day supply)1. Formulary generic drugs per prescription unit 2. Formulary brand name drugs per prescription unit3. Non-Formulary (Medically Necessary Only and Prior Authorization Required)4. Specialty Drugs (Medically Necessary Only and Prior Authorization Required)
Radiation Therapy (Prior Authorization Required)
Reconstructive Surgery• Surgery to correct a functional defect• Surgery to correct a condition that existed at or from birth and is a significant deviation from the common form or norm. Examples of congenital anomalies are protruding ear deformities; cleft lip; cleft palate; birth marks; and webbed fingers and toes
Skilled Nursing FacilityMaximum 60 days per member per plan year (Prior Authorization Required)
Speech Therapy (Prior Authorization Required)
Sterilization Procedures (Prior Authorization Required)1. Vasectomy (Outpatient Only)2. Tubal Ligation (Traditional and with Fulguration)
Diagnostic Sleep Study (Prior Authorization Required)
Travel Benefit• Prior authorization (written approval) and coordination is required from Plan prior to departure from Guam• Applicable only to approved referrals for conditions not treatable on Guam• Airfare and/or lodging expenses coverage for eligible members for approved specialty care visits, consultations, treatments and hospitalization services at Participating Providers in The Philippines or in Taiwan• Executive check-ups, preventive services, primary care services and dental care do not qualify for this benefit • Conditions and limitations apply as specified in the Member Handbook
* Plan pays 70% of eligible charges, Member pays 30% coinsurance of eligible charges plus any di§erence between eligible charges and billed charges. Eligible Charges for Non-Participating Providers are limited to the lesser of actual charges or Medicare’s participating provider fee schedule in the geographic location where the service was rendered unless otherwise provided in the Agreement. The Covered Person pays any excess above Eligible Charges.
** A separate deductible applies for services rendered by Non-Participating Providers
A full list of the Medical Exclusions can be found in the Judiciary of Guam FY2021 Member Handbook.
Deductible does not apply to these benefitswhen you go to a Participating Provider
Participating ProvidersDeductible does not apply
Non-participating Providersafter Deductible is met
Plan pays 100%
Plan pays 100%
Plan pays 100%
Plan pays 100%
Plan pays 100%
Plan pays 100%
$20 Member Co-payment
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Preventive Services (Out-Patient Only)Includes Annual Preventive Exams and Preventive Lab Services (Guam and Philippines only)In accordance with the guidelines established by the U.S. Preventive Services Task Force (USPSTF) Grades A and B recommendations
Outpatient Laboratory (Preventive & Diagnostic)
Immunizations/VaccinationsIn accordance with the guidelines established by the CDC Advisory Committee on Immunization Practices
Pre-Natal CareIncluding Routine Labs and First Ultrasound
Well-Child CareIn accordance with Bright Futures/American Academy of Pediatrics recommendations for Preventive Pediatric Health Care1. Infancy (Newborn to 9 months) - Maximum 7 visits2. Early Childhood (1 to 4 years old) - Maximum 7 visits3. Middle Childhood/Adolescence (5 to 17 years old) - Maximum 1 visit per year
Well-Woman CareIn accordance with the guidelines supported by the Health Resources and Services Administration (HRSA) and the Women’s Health and Cancer Act• Contraceptives including Sterilization and Tubal Ligation if prescribed• Includes coverage for Breast Pumps
Annual Eye ExamOnce per member per plan year
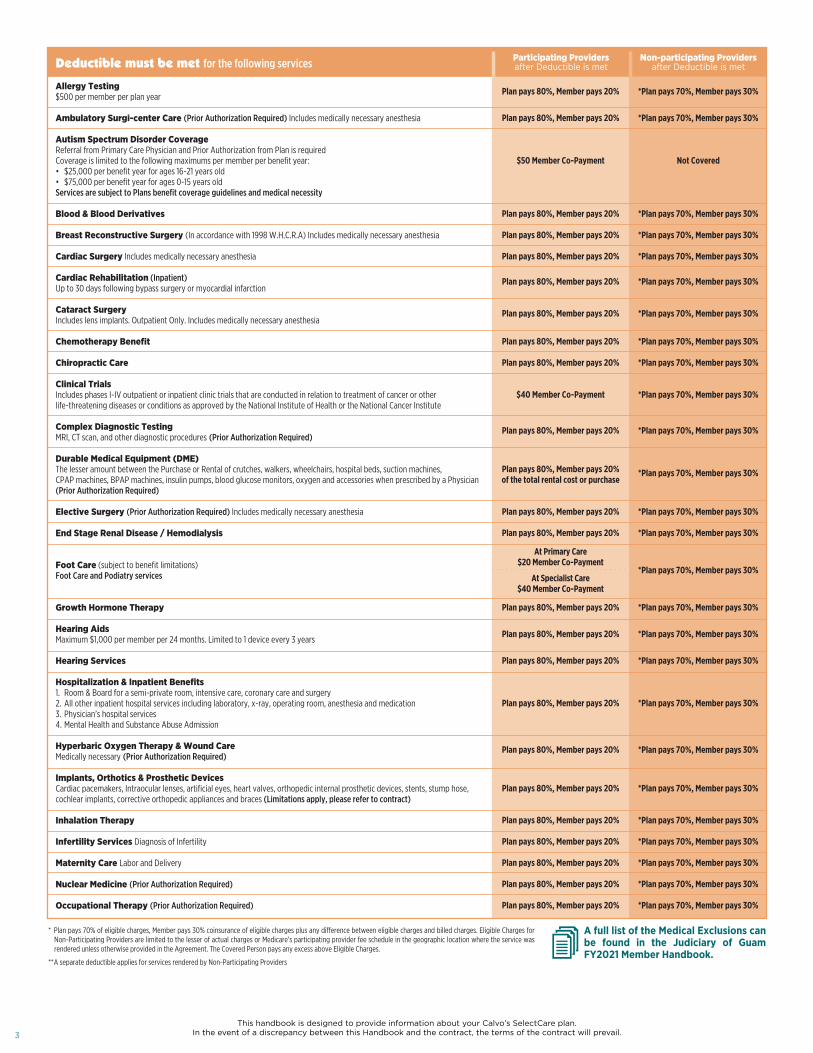
Deductible must be met for the following services Non-participating Providersafter Deductible is met
Participating Providersafter Deductible is met
$20 Member Co-Payment$40 Member Co-Payment$40 Member Co-Payment$50 Member Co-Payment$20 Member Co-Payment
Plan pays 100%Plan pays 100%
$20 Member Co-Payment$20 Member Co-Payment
$75 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 100%
*Plan pays 70%, Member pays 30%
$75 Member Co-payment plus any di�erence in Eligible charges and
billed charges
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Not Covered
Outpatient Physician Care & Services1. Primary Care Visits2. Specialist Care Visits3. Voluntary Second Surgical Opinion4. Urgent Care Visits5. Mental Health Care and Substance Abuse Visits6. Home Health Care Visit (Prior Authorization Required) 7. Hospice Care in Guam only, maximum of $100 per day (Prior Authorization Required)8. Routine Diagnostic Tests (X-ray, ultrasound, ECG, EEG, EMG & non-routine mammogram) 9. Injections (Does not include those on the Specialty Drugs List)
Emergency Care(For an on and o�-island emergencies, plan must be contacted and advised within 48 hours)The co-payment will be waived if you are admitted to the hospital from the emergency room1. On/O§-Island emergency facility, physician services, laboratory, X-Rays
Ambulance Services (Ground transportation only)
Acupuncture
Airfare Benefit to Centers of Excellence onlyFor members who meet qualifying conditions, Plan provides round trip airfare (Plan Approval Required)
This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.3
Deductible must be met for the following services Participating Providersafter Deductible is met
Non-participating Providersafter Deductible is met
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
$50 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
$40 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%of the total rental cost or purchase
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
At Primary Care$20 Member Co-Payment
At Specialist Care$40 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Not Covered
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Allergy Testing $500 per member per plan year
Ambulatory Surgi-center Care (Prior Authorization Required) Includes medically necessary anesthesia
Autism Spectrum Disorder CoverageReferral from Primary Care Physician and Prior Authorization from Plan is requiredCoverage is limited to the following maximums per member per benefit year:• $25,000 per benefit year for ages 16-21 years old • $75,000 per benefit year for ages 0-15 years old Services are subject to Plans benefit coverage guidelines and medical necessity
Blood & Blood Derivatives
Breast Reconstructive Surgery (In accordance with 1998 W.H.C.R.A) Includes medically necessary anesthesia
Cardiac Surgery Includes medically necessary anesthesia
Cardiac Rehabilitation (Inpatient)Up to 30 days following bypass surgery or myocardial infarction
Cataract SurgeryIncludes lens implants. Outpatient Only. Includes medically necessary anesthesia
Chemotherapy Benefit
Chiropractic Care
Clinical TrialsIncludes phases I-IV outpatient or inpatient clinic trials that are conducted in relation to treatment of cancer or otherlife-threatening diseases or conditions as approved by the National Institute of Health or the National Cancer Institute
Complex Diagnostic TestingMRI, CT scan, and other diagnostic procedures (Prior Authorization Required)
Durable Medical Equipment (DME)The lesser amount between the Purchase or Rental of crutches, walkers, wheelchairs, hospital beds, suction machines,CPAP machines, BPAP machines, insulin pumps, blood glucose monitors, oxygen and accessories when prescribed by a Physician (Prior Authorization Required)
Elective Surgery (Prior Authorization Required) Includes medically necessary anesthesia
End Stage Renal Disease / Hemodialysis
Foot Care (subject to benefit limitations)Foot Care and Podiatry services
Growth Hormone Therapy
Hearing AidsMaximum $1,000 per member per 24 months. Limited to 1 device every 3 years
Hearing Services
Hospitalization & Inpatient Benefits1. Room & Board for a semi-private room, intensive care, coronary care and surgery2. All other inpatient hospital services including laboratory, x-ray, operating room, anesthesia and medication3. Physician’s hospital services 4. Mental Health and Substance Abuse Admission
Hyperbaric Oxygen Therapy & Wound CareMedically necessary (Prior Authorization Required)
Implants, Orthotics & Prosthetic DevicesCardiac pacemakers, Intraocular lenses, artificial eyes, heart valves, orthopedic internal prosthetic devices, stents, stump hose,cochlear implants, corrective orthopedic appliances and braces (Limitations apply, please refer to contract)
Inhalation Therapy
Infertility Services Diagnosis of Infertility
Maternity Care Labor and Delivery
Nuclear Medicine (Prior Authorization Required)
Occupational Therapy (Prior Authorization Required)
Plan pays 80%, Member pays 20%
Plan pays 80% for the first 20 visits and 50% thereafter
Member pays 10%Member pays 20%Member pays 30%Member pays 30%
$0 Member Co-Payment$0 Member Co-Payment
Member pays 30%Member pays 30%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 100%
Plan pays 80%, Member pays 20%
Member pays all costs above $500Limited to once per plan year
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Member pays 30% of Average Wholesale Price (AWP) plus
any di�erence betweeneligible and billed charges
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Not Covered
Oral and Maxillofacial SurgeryOral surgical procedures, limited to:• Reduction of fractures of the jaws or facial bones• Surgical correction of cleft lip, cleft palate or severe functional malocclusion• Removal of stones from salivary ducts• Excision of leukoplakia or malignancies• Excision of cysts and incision of abscesses when done as independent procedures• Other surgical procedures that do not involve teeth or their supporting structures
Physical Therapy(Prior Authorization Required)
Prescription DrugsRetail Pharmacy (30-day supply)1. Formulary generic drugs per prescription unit 2. Formulary brand name drugs per prescription unit 3. Non-Formulary (Medically Necessary Only and Prior Authorization Required)4. Specialty Drugs (Medically Necessary Only and Prior Authorization Required)
Mail Order Pharmacy (90-day supply)1. Formulary generic drugs per prescription unit 2. Formulary brand name drugs per prescription unit3. Non-Formulary (Medically Necessary Only and Prior Authorization Required)4. Specialty Drugs (Medically Necessary Only and Prior Authorization Required)
Radiation Therapy (Prior Authorization Required)
Reconstructive Surgery• Surgery to correct a functional defect• Surgery to correct a condition that existed at or from birth and is a significant deviation from the common form or norm. Examples of congenital anomalies are protruding ear deformities; cleft lip; cleft palate; birth marks; and webbed fingers and toes
Skilled Nursing FacilityMaximum 60 days per member per plan year (Prior Authorization Required)
Speech Therapy (Prior Authorization Required)
Sterilization Procedures (Prior Authorization Required)1. Vasectomy (Outpatient Only)2. Tubal Ligation (Traditional and with Fulguration)
Diagnostic Sleep Study (Prior Authorization Required)
Travel Benefit• Prior authorization (written approval) and coordination is required from Plan prior to departure from Guam• Applicable only to approved referrals for conditions not treatable on Guam• Airfare and/or lodging expenses coverage for eligible members for approved specialty care visits, consultations, treatments and hospitalization services at Participating Providers in The Philippines or in Taiwan• Executive check-ups, preventive services, primary care services and dental care do not qualify for this benefit • Conditions and limitations apply as specified in the Member Handbook
$20 Member Co-Payment$40 Member Co-Payment$40 Member Co-Payment$50 Member Co-Payment$20 Member Co-Payment
Plan pays 100%Plan pays 100%
$20 Member Co-Payment$20 Member Co-Payment
$75 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 100%
*Plan pays 70%, Member pays 30%
$75 Member Co-payment plus any di�erence in Eligible charges and
billed charges
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Not Covered
Outpatient Physician Care & Services1. Primary Care Visits2. Specialist Care Visits3. Voluntary Second Surgical Opinion4. Urgent Care Visits5. Mental Health Care and Substance Abuse Visits6. Home Health Care Visit (Prior Authorization Required) 7. Hospice Care in Guam only, maximum of $100 per day (Prior Authorization Required)8. Routine Diagnostic Tests (X-ray, ultrasound, ECG, EEG, EMG & non-routine mammogram) 9. Injections (Does not include those on the Specialty Drugs List)
Emergency Care(For an on and o�-island emergencies, plan must be contacted and advised within 48 hours)The co-payment will be waived if you are admitted to the hospital from the emergency room1. On/O¦-Island emergency facility, physician services, laboratory, X-Rays
Ambulance Services (Ground transportation only)
Acupuncture
Airfare Benefit to Centers of Excellence onlyFor members who meet qualifying conditions, Plan provides round trip airfare (Plan Approval Required)
* Plan pays 70% of eligible charges, Member pays 30% coinsurance of eligible charges plus any di¦erence between eligible charges and billed charges. Eligible Charges for Non-Participating Providers are limited to the lesser of actual charges or Medicare’s participating provider fee schedule in the geographic location where the service was rendered unless otherwise provided in the Agreement. The Covered Person pays any excess above Eligible Charges.
** A separate deductible applies for services rendered by Non-Participating Providers
A full list of the Medical Exclusions can be found in the Judiciary of Guam FY2021 Member Handbook.

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail. 4
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
$50 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
$40 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%of the total rental cost or purchase
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
At Primary Care$20 Member Co-Payment
At Specialist Care$40 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Not Covered
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Allergy Testing $500 per member per plan year
Ambulatory Surgi-center Care (Prior Authorization Required) Includes medically necessary anesthesia
Autism Spectrum Disorder CoverageReferral from Primary Care Physician and Prior Authorization from Plan is requiredCoverage is limited to the following maximums per member per benefit year:• $25,000 per benefit year for ages 16-21 years old • $75,000 per benefit year for ages 0-15 years old Services are subject to Plans benefit coverage guidelines and medical necessity
Blood & Blood Derivatives
Breast Reconstructive Surgery (In accordance with 1998 W.H.C.R.A) Includes medically necessary anesthesia
Cardiac Surgery Includes medically necessary anesthesia
Cardiac Rehabilitation (Inpatient)Up to 30 days following bypass surgery or myocardial infarction
Cataract SurgeryIncludes lens implants. Outpatient Only. Includes medically necessary anesthesia
Chemotherapy Benefit
Chiropractic Care
Clinical TrialsIncludes phases I-IV outpatient or inpatient clinic trials that are conducted in relation to treatment of cancer or otherlife-threatening diseases or conditions as approved by the National Institute of Health or the National Cancer Institute
Complex Diagnostic TestingMRI, CT scan, and other diagnostic procedures (Prior Authorization Required)
Durable Medical Equipment (DME)The lesser amount between the Purchase or Rental of crutches, walkers, wheelchairs, hospital beds, suction machines,CPAP machines, BPAP machines, insulin pumps, blood glucose monitors, oxygen and accessories when prescribed by a Physician (Prior Authorization Required)
Elective Surgery (Prior Authorization Required) Includes medically necessary anesthesia
End Stage Renal Disease / Hemodialysis
Foot Care (subject to benefit limitations)Foot Care and Podiatry services
Growth Hormone Therapy
Hearing AidsMaximum $1,000 per member per 24 months. Limited to 1 device every 3 years
Hearing Services
Hospitalization & Inpatient Benefits1. Room & Board for a semi-private room, intensive care, coronary care and surgery2. All other inpatient hospital services including laboratory, x-ray, operating room, anesthesia and medication3. Physician’s hospital services 4. Mental Health and Substance Abuse Admission
Hyperbaric Oxygen Therapy & Wound CareMedically necessary (Prior Authorization Required)
Implants, Orthotics & Prosthetic DevicesCardiac pacemakers, Intraocular lenses, artificial eyes, heart valves, orthopedic internal prosthetic devices, stents, stump hose,cochlear implants, corrective orthopedic appliances and braces (Limitations apply, please refer to contract)
Inhalation Therapy
Infertility Services Diagnosis of Infertility
Maternity Care Labor and Delivery
Nuclear Medicine (Prior Authorization Required)
Occupational Therapy (Prior Authorization Required)
Participating Providers Non-participating ProvidersAdditional Benefits: What the plan covers (Deductible does not apply)
Plan pays 100%
Discounts vary by program
Plan Pays 100% atParticipating Providers
Plan pays 100% up to $200per member per 24 months
Not Covered
Plan pays 100% up to $200 per member per 24 months through reimbursement, which needs to
be submitted to Plan within90 days from date of service
WELLNESS BENEFITS1. Wellness Programs at Guam SDA Wellness Center Free Programs• Nutrition Consultation• Diabetes Self-Management Training Program• Stop Smoking Program• Childbirth Preparation Class
Discounted Programs• 7-day Shape Up Program • 7-day Detox Program• 7-day Advanced Detox Program• NEWSTART Program
2. Health and Wellness Rewards • Up to $100 per plan year• Please refer to member brochure for Health and Wellness Rewards available
Vision BenefitCoverage for a pair of contact lenses or eyeglasses lens/frames – maximum of $200 per member per 24 months
Deductible must be met for the following services Participating Providersafter Deductible is met
Non-participating Providersafter Deductible is met
Plan pays 80%, Member pays 20%
Plan pays 80% for the first 20 visits and 50% thereafter
Member pays 10%Member pays 20%Member pays 30%Member pays 30%
$0 Member Co-Payment$0 Member Co-Payment
Member pays 30%Member pays 30%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 100%
Plan pays 80%, Member pays 20%
Member pays all costs above $500Limited to once per plan year
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Member pays 30% of Average Wholesale Price (AWP) plus
any di�erence betweeneligible and billed charges
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Not Covered
Oral and Maxillofacial SurgeryOral surgical procedures, limited to:• Reduction of fractures of the jaws or facial bones• Surgical correction of cleft lip, cleft palate or severe functional malocclusion• Removal of stones from salivary ducts• Excision of leukoplakia or malignancies• Excision of cysts and incision of abscesses when done as independent procedures• Other surgical procedures that do not involve teeth or their supporting structures
Physical Therapy(Prior Authorization Required)
Prescription DrugsRetail Pharmacy (30-day supply)1. Formulary generic drugs per prescription unit 2. Formulary brand name drugs per prescription unit 3. Non-Formulary (Medically Necessary Only and Prior Authorization Required)4. Specialty Drugs (Medically Necessary Only and Prior Authorization Required)
Mail Order Pharmacy (90-day supply)1. Formulary generic drugs per prescription unit 2. Formulary brand name drugs per prescription unit3. Non-Formulary (Medically Necessary Only and Prior Authorization Required)4. Specialty Drugs (Medically Necessary Only and Prior Authorization Required)
Radiation Therapy (Prior Authorization Required)
Reconstructive Surgery• Surgery to correct a functional defect• Surgery to correct a condition that existed at or from birth and is a significant deviation from the common form or norm. Examples of congenital anomalies are protruding ear deformities; cleft lip; cleft palate; birth marks; and webbed fingers and toes
Skilled Nursing FacilityMaximum 60 days per member per plan year (Prior Authorization Required)
Speech Therapy (Prior Authorization Required)
Sterilization Procedures (Prior Authorization Required)1. Vasectomy (Outpatient Only)2. Tubal Ligation (Traditional and with Fulguration)
Diagnostic Sleep Study (Prior Authorization Required)
Travel Benefit• Prior authorization (written approval) and coordination is required from Plan prior to departure from Guam• Applicable only to approved referrals for conditions not treatable on Guam• Airfare and/or lodging expenses coverage for eligible members for approved specialty care visits, consultations, treatments and hospitalization services at Participating Providers in The Philippines or in Taiwan• Executive check-ups, preventive services, primary care services and dental care do not qualify for this benefit • Conditions and limitations apply as specified in the Member Handbook
$20 Member Co-Payment$40 Member Co-Payment$40 Member Co-Payment$50 Member Co-Payment$20 Member Co-Payment
Plan pays 100%Plan pays 100%
$20 Member Co-Payment$20 Member Co-Payment
$75 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 100%
*Plan pays 70%, Member pays 30%
$75 Member Co-payment plus any di�erence in Eligible charges and
billed charges
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Not Covered
Outpatient Physician Care & Services1. Primary Care Visits2. Specialist Care Visits3. Voluntary Second Surgical Opinion4. Urgent Care Visits5. Mental Health Care and Substance Abuse Visits6. Home Health Care Visit (Prior Authorization Required) 7. Hospice Care in Guam only, maximum of $100 per day (Prior Authorization Required)8. Routine Diagnostic Tests (X-ray, ultrasound, ECG, EEG, EMG & non-routine mammogram) 9. Injections (Does not include those on the Specialty Drugs List)
Emergency Care(For an on and o�-island emergencies, plan must be contacted and advised within 48 hours)The co-payment will be waived if you are admitted to the hospital from the emergency room1. On/O§-Island emergency facility, physician services, laboratory, X-Rays
Ambulance Services (Ground transportation only)
Acupuncture
Airfare Benefit to Centers of Excellence onlyFor members who meet qualifying conditions, Plan provides round trip airfare (Plan Approval Required)
* Plan pays 70% of eligible charges, Member pays 30% coinsurance of eligible charges plus any di§erence between eligible charges and billed charges. Eligible Charges for Non-Participating Providers are limited to the lesser of actual charges or Medicare’s participating provider fee schedule in the geographic location where the service was rendered unless otherwise provided in the Agreement. The Covered Person pays any excess above Eligible Charges.
** A separate deductible applies for services rendered by Non-Participating Providers
A full list of the Medical Exclusions can be found in the Judiciary of Guam FY2021 Member Handbook.

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.5
Schedule of BenefitsYour Benefits: What the plan covers Participating Providers Non-participating Providers
Deductible Per Individual Member (Class 1)
Deductible Per Family (Classes 2-4)If a member meets their $750 deductible, the plan begins to pay for covered services for that individual
Coverage MaximumsIndividual member annual maximum
Medical Out of Pocket Maximums (includes deductible and co-payments)Per Individual member per policy yearPer Family per policy year
Prescription Out of Pocket Maximums (includes co-payments)Per Individual member per policy year Per Family per policy year
O�-Island ServicesAny services in the Philippines, Asia, Hawaii, U.S. Mainland and any other foreign participating providers
$750
$1,500
None
$2,000$6,000
$1,500$3,000
**$1,500
**$4,500
None
No MaximumNo Maximum
No MaximumNo Maximum
Prior Authorization from your doctor and approval from the Plan is required prior to services rendered at o -island facilities. Covered benefits at
Participating Philippine Providers are payable 100% after deductible is met
Deductible does not apply to these benefitswhen you go to a Participating Provider
Participating ProvidersDeductible does not apply
Non-participating Providersafter Deductible is met
Plan pays 100%
Plan pays 100%
Plan pays 100%
Plan pays 100%
Plan pays 100%
Plan pays 100%
Plan pays 100%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Preventive Services (Out-Patient Only) Includes Annual Preventive Exams and Preventive Lab Services (Guam and Philippines only)In accordance with the guidelines established by the U.S. Preventive Services Task Force (USPSTF) Grades A and B recommendations
Outpatient Laboratory (Preventive & Diagnostic)
Immunizations/VaccinationsIn accordance with the guidelines established by the CDC Advisory Committee on Immunization Practices
Pre-Natal CareIncluding Routine Labs and First Ultrasound
Well-Child CareIn accordance with Bright Futures/American Academy of Pediatrics recommendations for Preventive Pediatric Health Care1. Infancy (Newborn to 9 months) - Maximum 7 visits2. Early Childhood (1 to 4 years old) - Maximum 7 visits3. Middle Childhood/ Adolescence (5 to 17 years old) - Maximum 1 visit per year
Well-Woman CareIn accordance with the guidelines supported by the Health Resources and Services Administration (HRSA) and the Women’s Health and Cancer Act• Contraceptives including Sterilization and Tubal Ligation if prescribed• Includes coverage for Breast Pumps
Sterilization Procedures (Prior Authorization Required)1. Vasectomy (Outpatient Only)2. Tubal Ligation (Traditional and with Fulguration)
$20 Member Co-payment
$20 Member Co-Payment$40 Member Co-Payment$40 Member Co-Payment$50 Member Co-Payment$20 Member Co-Payment
Plan pays 100%Plan pays 100%
$20 Member Co-Payment$20 Member Co-Payment
$75 Member Co-payment
Plan pays 80%, Member pays 20%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
$75 Member Co-payment plus any di erence in Eligible charges and
billed charges
*Plan pays 70%, Member pays 30%
Annual Eye ExamOnce per member per plan year
Outpatient Physician Care & Services1. Primary Care Visits2. Specialist Care Visits3. Voluntary Second Surgical Opinion4. Urgent Care Visits5. Mental Health Care and Substance Abuse Visits6. Home Health Care Visit (Prior Authorization Required) 7. Hospice Care in Guam only, maximum of $100 per day (Prior Authorization Required) 8. Routine Diagnostic Tests (X-ray, ultrasound, ECG, EEG, EMG & non-routine mammogram) 9. Injections (Does not include those on the Specialty Drugs List)
Emergency Care(For an on and o� island emergencies, plan must be contacted and advised within 48 hours)The co-payment will be waived if you are admitted to the hospital from the emergency room1. On/O¡-Island emergency facility, physician services, laboratory, X-Rays
Ambulance Services (Ground transportation only)
Deductible does not apply to these benefitswhen you go to a Participating Provider
Participating ProvidersDeductible does not apply
Non-participating Providersafter Deductible is met
Member pays 10%Member pays 20%Member pays 30%Member pays 30%
$0 Member Co-Payment$0 Member Co-Payment
Member pays 30%Member pays 30%
Member pays all costs above $500Limited to once per plan year
Member pays 30% of Average Wholesale Price (AWP) plus
any di erence betweeneligible and billed charges
Not Covered
Prescription DrugsRetail Pharmacy (30-day supply)1. Formulary generic drugs per prescription unit 2. Formulary brand name drugs per prescription unit 3. Non-Formulary (Medically Necessary Only and Prior Authorization Required)4. Specialty Drugs (Medically Necessary Only and Prior Authorization Required)
Mail Order Pharmacy (90-day supply)1. Formulary generic drugs per prescription unit 2. Formulary brand name drugs per prescription unit3. Non-Formulary (Medically Necessary Only and Prior Authorization Required)4. Specialty Drugs (Medically Necessary Only and Prior Authorization Required)
Travel Benefit• Prior authorization (written approval) and coordination is required from Plan prior to departure from Guam• Applicable only to approved referrals for conditions not treatable on Guam• Airfare and/or lodging expenses coverage for eligible members for approved specialty care visits, consultations, treatments and hospitalization services at Participating Providers in The Philippines or in Taiwan• Executive check-ups, preventive services, primary care services and dental care do not qualify for this benefit• Conditions and limitations apply as specified in the Member Handbook
* Plan pays 70% of eligible charges, Member pays 30% coinsurance of eligible charges plus any di¡erence between eligible charges and billed charges. Eligible Charges for Non-Participating Providers are limited to the lesser of actual charges or Medicare’s participating provider fee schedule in the geographic location where the service was rendered unless otherwise provided in the Agreement. The Covered Person pays any excess above Eligible Charges.
** A separate deductible applies for services rendered by Non-Participating Providers
A full list of the Medical Exclusions can be found in the Judiciary of Guam FY2021 Member Handbook.

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail. 6
Deductible must be met for the following services Participating Providersafter Deductible is met
Non-participating Providersafter Deductible is met
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 100%
Plan pays 80%, Member pays 20%
$50 Member Co-pay
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
$40 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%of the total rental cost or purchase
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
At Primary Care$20 Member Co-Payment
At Specialist Care$40 Member Co-Payment
Plan pays 80%, Member pays 20%
Acupuncture
Allergy Testing $500 per member per plan year
Airfare Benefit to Centers of Excellence onlyFor members who meet qualifying conditions, Plan provides round trip airfare (Prior Authorization Required)
Ambulatory Surgi-center Care (Prior Authorization Required)
Autism Spectrum Disorder CoverageReferral from Primary Care Physician and Prior Authorization from Plan is requiredCoverage is limited to the following maximums per member per benefit year:• $25,000 per benefit year for ages 16-21 years old • $75,000 per benefit year for ages 0-15 years old Services are subject to Plans benefit coverage guidelines and medical necessity
Blood & Blood Derivatives
Breast Reconstructive Surgery (In accordance with 1998 W.H.C.R.A) Includes medically necessary anesthesia
Cardiac Surgery Includes medically necessary anesthesia
Cardiac Rehabilitation (Inpatient)Up to 30 days following bypass surgery or myocardial infarction
Cataract SurgeryIncludes lens implants. Outpatient Only. Includes medically necessary anesthesia
Chemotherapy Benefit
Chiropractic Care
Clinical TrialsIncludes phases I-IV outpatient or inpatient clinic trials that are conducted in relation to treatment of cancer or otherlife-threatening diseases or conditions as approved by the National Institute of Health or the National Cancer Institute
Complex Diagnostic TestingMRI, CT scan, and other diagnostic procedures (Prior Authorization Required)
Durable Medical Equipment (DME)The lesser amount between the Purchase or Rental of crutches, walkers, wheelchairs, hospital beds, suction machines,CPAP machines, BPAP machines, insulin pumps, blood glucose monitors, oxygen and accessories when prescribed by a Physician (Prior Authorization Required)
Elective Surgery (Prior Authorization Required) Includes medically necessary anesthesia
End Stage Renal Disease / Hemodialysis
Foot Care (subject to benefit limitations)Foot Care and Podiatry services
Growth Hormone Therapy
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Not Covered
*Plan pays 70%, Member pays 30%
Not Covered
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80% for the first 20 visits and 50% thereafter
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
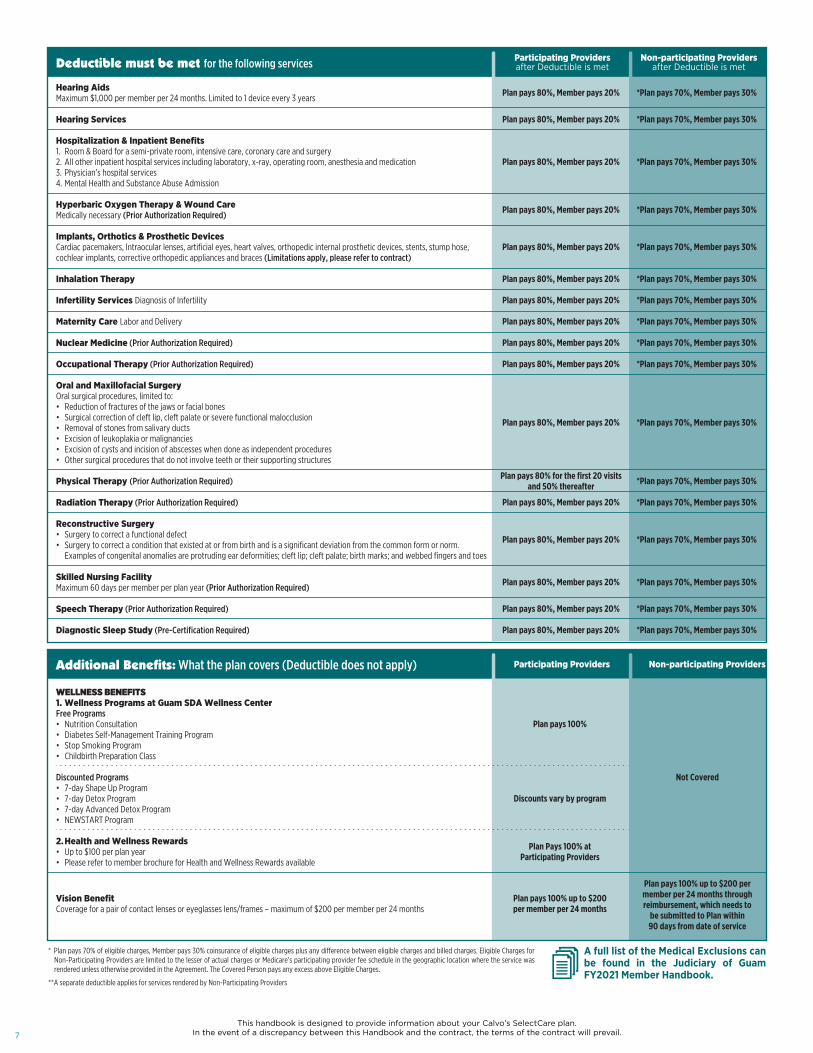
Hearing AidsMaximum $1,000 per member per 24 months. Limited to 1 device every 3 years
Hearing Services
Hospitalization & Inpatient Benefits1. Room & Board for a semi-private room, intensive care, coronary care and surgery2. All other inpatient hospital services including laboratory, x-ray, operating room, anesthesia and medication3. Physician’s hospital services 4. Mental Health and Substance Abuse Admission
Hyperbaric Oxygen Therapy & Wound CareMedically necessary (Prior Authorization Required)
Implants, Orthotics & Prosthetic DevicesCardiac pacemakers, Intraocular lenses, artificial eyes, heart valves, orthopedic internal prosthetic devices, stents, stump hose, cochlear implants, corrective orthopedic appliances and braces (Limitations apply, please refer to contract)
Inhalation Therapy
Infertility Services Diagnosis of Infertility
Maternity Care Labor and Delivery
Nuclear Medicine (Prior Authorization Required)
Occupational Therapy (Prior Authorization Required)
Oral and Maxillofacial SurgeryOral surgical procedures, limited to:• Reduction of fractures of the jaws or facial bones• Surgical correction of cleft lip, cleft palate or severe functional malocclusion• Removal of stones from salivary ducts• Excision of leukoplakia or malignancies• Excision of cysts and incision of abscesses when done as independent procedures• Other surgical procedures that do not involve teeth or their supporting structures
Physical Therapy (Prior Authorization Required)
Radiation Therapy (Prior Authorization Required)
Reconstructive Surgery• Surgery to correct a functional defect• Surgery to correct a condition that existed at or from birth and is a significant deviation from the common form or norm. Examples of congenital anomalies are protruding ear deformities; cleft lip; cleft palate; birth marks; and webbed fingers and toes
Skilled Nursing FacilityMaximum 60 days per member per plan year (Prior Authorization Required)
Speech Therapy (Prior Authorization Required)
Diagnostic Sleep Study (Pre-Certification Required)
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
$20 Member Co-payment
$20 Member Co-Payment$40 Member Co-Payment$40 Member Co-Payment$50 Member Co-Payment$20 Member Co-Payment
Plan pays 100%Plan pays 100%
$20 Member Co-Payment$20 Member Co-Payment
$75 Member Co-payment
Plan pays 80%, Member pays 20%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
$75 Member Co-payment plus any di�erence in Eligible charges and
billed charges
*Plan pays 70%, Member pays 30%
Annual Eye ExamOnce per member per plan year
Outpatient Physician Care & Services1. Primary Care Visits2. Specialist Care Visits3. Voluntary Second Surgical Opinion4. Urgent Care Visits5. Mental Health Care and Substance Abuse Visits6. Home Health Care Visit (Prior Authorization Required) 7. Hospice Care in Guam only, maximum of $100 per day (Prior Authorization Required) 8. Routine Diagnostic Tests (X-ray, ultrasound, ECG, EEG, EMG & non-routine mammogram) 9. Injections (Does not include those on the Specialty Drugs List)
Emergency Care(For an on and o� island emergencies, plan must be contacted and advised within 48 hours)The co-payment will be waived if you are admitted to the hospital from the emergency room1. On/O¢-Island emergency facility, physician services, laboratory, X-Rays
Ambulance Services (Ground transportation only)
Member pays 10%Member pays 20%Member pays 30%Member pays 30%
$0 Member Co-Payment$0 Member Co-Payment
Member pays 30%Member pays 30%
Member pays all costs above $500Limited to once per plan year
Member pays 30% of Average Wholesale Price (AWP) plus
any di�erence betweeneligible and billed charges
Not Covered
Prescription DrugsRetail Pharmacy (30-day supply)1. Formulary generic drugs per prescription unit 2. Formulary brand name drugs per prescription unit 3. Non-Formulary (Medically Necessary Only and Prior Authorization Required)4. Specialty Drugs (Medically Necessary Only and Prior Authorization Required)
Mail Order Pharmacy (90-day supply)1. Formulary generic drugs per prescription unit 2. Formulary brand name drugs per prescription unit3. Non-Formulary (Medically Necessary Only and Prior Authorization Required)4. Specialty Drugs (Medically Necessary Only and Prior Authorization Required)
Travel Benefit• Prior authorization (written approval) and coordination is required from Plan prior to departure from Guam• Applicable only to approved referrals for conditions not treatable on Guam• Airfare and/or lodging expenses coverage for eligible members for approved specialty care visits, consultations, treatments and hospitalization services at Participating Providers in The Philippines or in Taiwan• Executive check-ups, preventive services, primary care services and dental care do not qualify for this benefit• Conditions and limitations apply as specified in the Member Handbook
Deductible does not apply to these benefitswhen you go to a Participating Provider
Participating ProvidersDeductible does not apply
Non-participating Providersafter Deductible is met
* Plan pays 70% of eligible charges, Member pays 30% coinsurance of eligible charges plus any di¢erence between eligible charges and billed charges. Eligible Charges for Non-Participating Providers are limited to the lesser of actual charges or Medicare’s participating provider fee schedule in the geographic location where the service was rendered unless otherwise provided in the Agreement. The Covered Person pays any excess above Eligible Charges.
** A separate deductible applies for services rendered by Non-Participating Providers
A full list of the Medical Exclusions can be found in the Judiciary of Guam FY2021 Member Handbook.
This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.7
Deductible must be met for the following services Participating Providersafter Deductible is met
Non-participating Providersafter Deductible is met
Additional Benefits: What the plan covers (Deductible does not apply)
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 100%
Plan pays 80%, Member pays 20%
$50 Member Co-pay
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
$40 Member Co-Payment
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%of the total rental cost or purchase
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
At Primary Care$20 Member Co-Payment
At Specialist Care$40 Member Co-Payment
Plan pays 80%, Member pays 20%
Acupuncture
Allergy Testing $500 per member per plan year
Airfare Benefit to Centers of Excellence onlyFor members who meet qualifying conditions, Plan provides round trip airfare (Prior Authorization Required)
Ambulatory Surgi-center Care (Prior Authorization Required)
Autism Spectrum Disorder CoverageReferral from Primary Care Physician and Prior Authorization from Plan is requiredCoverage is limited to the following maximums per member per benefit year:• $25,000 per benefit year for ages 16-21 years old • $75,000 per benefit year for ages 0-15 years old Services are subject to Plans benefit coverage guidelines and medical necessity
Blood & Blood Derivatives
Breast Reconstructive Surgery (In accordance with 1998 W.H.C.R.A) Includes medically necessary anesthesia
Cardiac Surgery Includes medically necessary anesthesia
Cardiac Rehabilitation (Inpatient)Up to 30 days following bypass surgery or myocardial infarction
Cataract SurgeryIncludes lens implants. Outpatient Only. Includes medically necessary anesthesia
Chemotherapy Benefit
Chiropractic Care
Clinical TrialsIncludes phases I-IV outpatient or inpatient clinic trials that are conducted in relation to treatment of cancer or otherlife-threatening diseases or conditions as approved by the National Institute of Health or the National Cancer Institute
Complex Diagnostic TestingMRI, CT scan, and other diagnostic procedures (Prior Authorization Required)
Durable Medical Equipment (DME)The lesser amount between the Purchase or Rental of crutches, walkers, wheelchairs, hospital beds, suction machines,CPAP machines, BPAP machines, insulin pumps, blood glucose monitors, oxygen and accessories when prescribed by a Physician (Prior Authorization Required)
Elective Surgery (Prior Authorization Required) Includes medically necessary anesthesia
End Stage Renal Disease / Hemodialysis
Foot Care (subject to benefit limitations)Foot Care and Podiatry services
Growth Hormone Therapy
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Not Covered
*Plan pays 70%, Member pays 30%
Not Covered
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80% for the first 20 visits and 50% thereafter
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Plan pays 80%, Member pays 20%
Hearing AidsMaximum $1,000 per member per 24 months. Limited to 1 device every 3 years
Hearing Services
Hospitalization & Inpatient Benefits1. Room & Board for a semi-private room, intensive care, coronary care and surgery2. All other inpatient hospital services including laboratory, x-ray, operating room, anesthesia and medication3. Physician’s hospital services 4. Mental Health and Substance Abuse Admission
Hyperbaric Oxygen Therapy & Wound CareMedically necessary (Prior Authorization Required)
Implants, Orthotics & Prosthetic DevicesCardiac pacemakers, Intraocular lenses, artificial eyes, heart valves, orthopedic internal prosthetic devices, stents, stump hose, cochlear implants, corrective orthopedic appliances and braces (Limitations apply, please refer to contract)
Inhalation Therapy
Infertility Services Diagnosis of Infertility
Maternity Care Labor and Delivery
Nuclear Medicine (Prior Authorization Required)
Occupational Therapy (Prior Authorization Required)
Oral and Maxillofacial SurgeryOral surgical procedures, limited to:• Reduction of fractures of the jaws or facial bones• Surgical correction of cleft lip, cleft palate or severe functional malocclusion• Removal of stones from salivary ducts• Excision of leukoplakia or malignancies• Excision of cysts and incision of abscesses when done as independent procedures• Other surgical procedures that do not involve teeth or their supporting structures
Physical Therapy (Prior Authorization Required)
Radiation Therapy (Prior Authorization Required)
Reconstructive Surgery• Surgery to correct a functional defect• Surgery to correct a condition that existed at or from birth and is a significant deviation from the common form or norm. Examples of congenital anomalies are protruding ear deformities; cleft lip; cleft palate; birth marks; and webbed fingers and toes
Skilled Nursing FacilityMaximum 60 days per member per plan year (Prior Authorization Required)
Speech Therapy (Prior Authorization Required)
Diagnostic Sleep Study (Pre-Certification Required)
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
*Plan pays 70%, Member pays 30%
Participating Providers Non-participating Providers
Not Covered
Plan pays 100% up to $200 per member per 24 months through reimbursement, which needs to
be submitted to Plan within90 days from date of service
WELLNESS BENEFITS1. Wellness Programs at Guam SDA Wellness Center Free Programs• Nutrition Consultation• Diabetes Self-Management Training Program• Stop Smoking Program• Childbirth Preparation Class
Discounted Programs• 7-day Shape Up Program • 7-day Detox Program• 7-day Advanced Detox Program• NEWSTART Program
2. Health and Wellness Rewards • Up to $100 per plan year• Please refer to member brochure for Health and Wellness Rewards available
Vision BenefitCoverage for a pair of contact lenses or eyeglasses lens/frames – maximum of $200 per member per 24 months
Plan pays 100%
Discounts vary by program
Plan Pays 100% atParticipating Providers
Plan pays 100% up to $200per member per 24 months
* Plan pays 70% of eligible charges, Member pays 30% coinsurance of eligible charges plus any di£erence between eligible charges and billed charges. Eligible Charges for Non-Participating Providers are limited to the lesser of actual charges or Medicare’s participating provider fee schedule in the geographic location where the service was rendered unless otherwise provided in the Agreement. The Covered Person pays any excess above Eligible Charges.
** A separate deductible applies for services rendered by Non-Participating Providers
A full list of the Medical Exclusions can be found in the Judiciary of Guam FY2021 Member Handbook.

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail. 8
Terms:1. Unused balances are not transferable to the following year.
2. Charges for Non-participating Providers are limited to the lesser of actual charges or the usual, customary and reasonable charge in the geographic location where the service was rendered, unless otherwise provided in the agreement.
3. The covered member pays any excess above Eligible Charges.
4. Plan has no deductible.
5. There are no registration fees for visits to participating providers.
$1,000
Schedule of Benefits
100% of Eligible Expenses
80% of Eligible Expenses
50% of Eligible Expenses
70% of eligible charges(Member pays excess above
Eligible Expenses)
70% of eligible charges(Member pays excess above
Eligible Expenses)
35% of eligible charges(Member pays excess above
Eligible Expenses)
dental1000
Diagnostic & Preventive Care1. Caries Susceptibility Test2. Exams – Includes Treatment Plan; once every 6 months3. Fluoride Treatment – Annually for children up to age 194. Prophylaxis – Cleaning & polishing of teeth; once every 6 months5. Sealants – For permanent molars & pre-molars for children up to age 166. Space Maintainers - For children up to age 16 years; includes adjustments within 6 months of installation7. Study Models8. X-rays (Bite Wing); Maximum of 4 per Plan year9. X-rays (Full Mouth); once every 3 years
Basic & Restorative CareGeneral Services1. Emergency Care (during o�ce hours)2. Pulp Treatment3. Routine Fillings • Amalgam & Composite Resin • Synthetic & Plastic (other than gold & porcelain)
Oral Surgery1. Simple Extractions2. Complicated Extractions3. Tooth Impactions
Periodontal Care1. Periodontal Prophylaxis; Cleaning and polishing once every six months2. Periodontal Treatment
General Anesthesia • Includes Conscious Sedation and Nitrous Oxide • Covered when recommended by attending physician
Pulpotomy & Root Canals/ Endodontic Surgery & Care
Major & Replacement CareFixed Prosthetics1. Crowns and Bridges2. Gold Inlays & Onlays3. Replacement of Crown Restoration; limited once every 5 years
Removable Prosthetics1. Full Dentures; once every 5 years2. Partial Dentures; once every 5 years3. Each Additional Tooth4. Relines5. Denture Repair
Coverage MaximumsIndividual member annual maximum
Participating Providers Non-participating ProvidersWhat the Plan covers:Subject to the Specific limitations which are contained in the Group Health Certificate
Judiciary of Guam
A full list of the Medical Exclusions can be found in the Judiciary of Guam FY2021 Member Handbook.

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.9
Emergency and Urgent Care Facilities
When urgent or emergency care is needed,you have access to the following providers
Dededo Yigo
MangilaoBarrigada
1. Hagåtña2. Agana Heights3. Sinajana4. Mongmong-Toto-Maite5. Tamuning-Tumon Harmon
Merizo
Inarajan
Talofofo
Umatac
Agat
Santa Rita
Yona
Ordot/Chalan PagoPiti
Asan
1.
2.3.
4.
5.
388 Ypao Road, Tamuning
Phone: 646-8881/2Fax: 647-2557
850 Gov. Carlos G. Camacho Rd, Tamuning
Phone: 647-2555/9Fax: 649-5508
Nanbo Guahan Bldg. Ste. 203,250 Rte. 4, Hagåtña
Phone: 475-6500/1/2 Fax: 475-6520
133 Route 3,Dededo
Phone: 645-5500Fax: 645-5501
1244 N. Marine Corps Drive, Upper Tumon
Phone: 647-8261/2Fax: 647-8257

Local, National, and International accessto thousands of doctors, hospitals, dental and vision care providers
PhilippinesCardinal Santos Medical CenterMakati Medical CenterManila Doctor’s HospitalNational Kidney and Transplant InstituteSt. Luke’s Medical Center: Global City, ManilaSt. Luke’s Medical Center: Quezon City, ManilaThe Medical City: Clark Freeport Zone, PampangaThe Medical City: Molo, Iloilo CityThe Medical City: Pasig City, Manila
China Medical University Hospital Shin Kong Wu Ho-Su Memorial HospitalTaiwan Adventist Hospital
Taiwan Hong KongGleneagles Hong Kong HospitalHong Kong Adventist Hospital - Stubbs Road
JapanKameda Medical CenterKameda Kyobashi Clinic
HawaiiKapiolani Medical Centerfor Women & ChildrenShriner's Hospitals for ChildrenStraub Clinic and HospitalThe Cancer Center of HawaiiUniversity Clinical EducationResearch Associates
KoreaSamsung Medical Center
Our comprehensive provider networkoffers choices to quality providers for you!
Philippines Taiwan Hong KongJapan Korea
O�-Island Provider: Center of Excellence O�-Island Provider
Care for O�-Island Services must be pre-approved by Calvo’s SelectCare
Doctor’s Medical Center of ModestoGood Samaritan HospitalLong Beach Memorial Medical CenterSt. Vincent Medical CenterWhite Memorial Medical CenterAdvanced Urology Medical GroupAnaheim Global Medical CenterCedars-Sinai Medical CenterChapman Global Medical CenterChildren’s Hospital of Los AngelesKeck Hospital of USCOrange County Global Medical CenterSharp Chula Vista Medical CenterSharp Coronado Hospital and Medical CenterSharp Memorial HospitalSharp Grossmont HospitalSouth Coast Global Medical CenterSt. John’s Health CenterUSC Norris Cancer Center and HospitalUSC Verdugo Hills Hospital
California
U.S. PPOhave access to over 1.1 million
providers in the U.S.A through the UnitedHealthcare Medical Network
Participating providers may change from time to time, so please contact our o�ce for any updates
This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail. 10
Emergency and Urgent Care Facilities
When urgent or emergency care is needed,you have access to the following providers
Dededo Yigo
MangilaoBarrigada
1. Hagåtña2. Agana Heights3. Sinajana4. Mongmong-Toto-Maite5. Tamuning-Tumon Harmon
Merizo
Inarajan
Talofofo
Umatac
Agat
Santa Rita
Yona
Ordot/Chalan PagoPiti
Asan
1.
2.3.
4.
5.
388 Ypao Road, Tamuning
Phone: 646-8881/2Fax: 647-2557
850 Gov. Carlos G. Camacho Rd, Tamuning
Phone: 647-2555/9Fax: 649-5508
Nanbo Guahan Bldg. Ste. 203,250 Rte. 4, Hagåtña
Phone: 475-6500/1/2 Fax: 475-6520
133 Route 3,Dededo
Phone: 645-5500Fax: 645-5501
1244 N. Marine Corps Drive, Upper Tumon
Phone: 647-8261/2Fax: 647-8257

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.11
Providers: Participating Guam Doctors and Dentists
CardiologyGiambartolome, AlessandroInaba, YoichiKim, ByungsooPrieto, AlejandroQuiros, Juan - VISITINGWiedermann, Joseph
DermatologyLaTour, Donn - VISITINGProdanovic, Edward - VISITINGYang, Hoseong Steve
E.N.T. (Otolaryngology)Castro, JerryRyu, David
EndocrinologyAlford, ErikaRubio, Joel
Family PracticeAdolphson, AraniaAkimoto, VincentAkoma, UgochukwuAnderson, MarkArnott, TimothyBryson, JulieCampus, HieuCook-Hyunh, MarianaCruz, LuisFlores, LisaFrickel, WendyGalgo, Geo�reyGerling, WilliamHancock, WilliamLee, DeloresLoder, BryceLom, JitkaLujan, DavinaManlucu, LuellaMariano, MariaMiyagi, ShishinNamm, JulieNguyen, Hoa VanNguyen, LuanRaab, JeremyRichardson, IanRobinson, MichaelSamaniego, MariaSantos, PatrickSchroeder Jr., EdmundTerlaje, RicardoThanapandian, Kamala
GastroenterologyFarrell, Frank - VISITING
GeriatricsLiu, Pei-ChangOuhadi, FarazSchroeder Jr., Edmund
HematologyFriedman, SamuelSanchez-Varela, Ana
Infectious DiseaseMedicineMagcalas, EdgardoUrsales, Anna LeighYamamoto, Michelle
Internal MedicineAgustin, MichaelAlford, ErikaAlly, InsafAlvez, LauraArcilla, LeopoldoChang, YoungChenet, AlixCruz, Je�reyCruz, OliviaDuenas, Vincent A.Guzman, PabloInaba, YoichiKang, JiyeongLim, DorisLim Jr., JohnnyLizama, Florencio Larry T.Magcalas, EdgardoNerves, Robert C.Osman, SharleenOuhadi, FarazPreston, DonaldRubio, JoelSafa, SaiedSamonte, RomeoSistoza, LilybethTaitano, John RayTrinh, TienUrsales, Anna LeighVilla, EdenYamamoto, Michelle
NephrologyAlvez, LauraDissadee, ManaNerves, Robert C.Osman, Sharleen
Philips, SherifSafa, Saied
NeurologyCarlos, RamelHale, Justin
OB/GYNBez, EllenBieling, FriedrichBordallo, Annie U.Gabel, Je�reyHirata, Greigh - VISITINGJyung, JinMiller, VanessaSidell, JonathanShieh, ThomasSwena, DeborahTodd, RoseUnderwood, Teresa
OncologyAu, Kin-SingCoty, PaulFriedman, SamuelGuzman, PabloHuang, ChenKo, Song-ChuSanchez-Varela, Ana
OphthalmologyBurton, Gregory P.DeBenedictis, MarjorieFlowers, CharlesHorio, BlakeJack, RobertLombard, PeterMargalit, EyalNg, Eugene - VISITINGParks, David - VISITINGSmith, AnthonyWresh, Robert
OrthopedicsArafiles, RubenCunningham, GlennGalang, CarmelinoKim, Andrew
Pain ManagementGaerlan, Maria Stella
PediatricsBlancaflor, MariaCarrera, YolandaDel Rosario, Amanda
Domalanta, DinaFojas, MilliecorGarcia, AntonioGarrido, JohnLinsangan, GladysManaloto, CristinaSantos, EdnaSarmiento, DennisUm, MichaelWalker, Jasmine
Physical Medicine & RehabilitaionGaerlan, Maria Stella
PodiatryBorja, TeresaKim, SungwookPrins, DustinSangalang, MelindaSilan, NoelTutnauer, Philip
Pulmonology/Critical CareAgustin, MichaelAguon, JoleenGonzalez-Huertas, JoseHernandez, Elizabeth
RadiologyAllen, ScottBerg, NathanielBocobo, GeorgeKhandelwal, AshishLizama, VincentMallikarjunappaMartinez, RobertoNguyen, TuanPackianathan, XavierPiana, PeachyPomeranz, StevenSchneider, MichaelShay, Je�erySpak, EricTan, KennethTaylor, LauraThorisson, HjaltiYoung, John
Sleep MedicineBarthlen, GabrieleLin, Shin HaoSchumann, Richard
Surgery-Cardiac/ ThoracicYap, Alexander
Surgery-GeneralBandy, NicholasCruz, MichaelEusebio, ChristianEusebio, Ricardo B.Go, PeterHelm, JosephIm, SunggeunKobayashi, RonaldLeon Guerrero, AlexandraLi, Doris SophiaMedina, DanielOh, DanielRahmani, KiaSandy, GisellaSaw, Eng
Surgery-Hand & MicrosurgeryLandstrom, Jerone
Surgery-NeurologicalHayashida, StevenNyame, VerradWeingarten, David
Surgery-Plastic &ReconstructiveFegurgur, John
Surgery VascularEusebio, RicardoKobayashi, Ronald
UrologyFenton, AnnPetero, Virgilio
Wound CareAcuna, Edna
General DentistryBrady, TimothyFamily Dental CenterFernandez, MichaelGentleCare Dental AssociatesHafa Adai Family Dental, P.CHarmon Loop Dental O�ce
Isa Dental ClinicIsland DentalLee, Thomas K.Malabanan Jr., BenMangilao Dental ClinicOrdot Dental ClinicParadise Smiles Dental Clinic
Premier DentistryReflection Center Dental CareSeventh Day Adventist DentalVeloria, Tom S.Yang, Robert J.Yasuhiro, Stanley
EndodonticsPremier Dentistry
Pediatric DentistryIsa Dental ClinicKim, BackhabwhaPediatric Dental Center
PeriodonticsGatewood, RobertRhim, SongHayashi, Chie
Providers may change from time to time, we encourage you to call our customer service department.
Dentists
Doctors
Providers marked with an asterisk (*) are Medicare ProvidersParticipating providers may change from time to time, so please contact our o�ce for any updates

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail. 12
Participating Clinics
Providers: Participating Clinics, Hospitals, Pharmacies and ServicesProviders may change from time to time, we encourage you to call our customer service department.
Providers marked with an asterisk (*) are Medicare ProvidersParticipating providers may change from time to time, so please contact our o�ce for any updates
Participating Guam PharmaciesCommunity Pharmacy- American Medical Center (Tumon)- Guam Adult & Pediatric Clinic
Evergreen Pharmacy & Supplies
Express Med Pharmacy- American Medical Center (Mangilao)- Dededo
Guam Medical Pharmacy
Guam Rexall Drugs
Harmon Drugs
ITC Pharmacy- ITC Building- Photo Town Plaza
K-Mart Pharmacy
Mega Drugs- Daily Plaza Bldg- Oka Plaza Building- FHP Health Center
Minutes Rx Pharmacy
Oka Pharmacy
Pacific Healthcare Pharmacy
Perezville Pharmacy
Polymedic Pharmacy
Sagan Amot Pharmacy
Seventh Day AdventistPharmacy
Super Drug- Dededo Payless- IHP Medical Group- Oka Payless- Maite Payless- Yigo Payless
Benefits provided by:
Pharmacy Benefits ManagerBIN: 003650 Processor Control: 64
Allied ServicesAcupunctureBaik, Jong SunChong, RichardYu, Jong
AudiologyKo�end, Renee*
ChiropracticArthur, SteveBeckwith, NicholasDimalanta, Albert J.Gregory, BarbaraGregory, Robert W.Larkin, GaryLarkin, Lani F.Larkin, ScottMartin, FrancoiseMiller, Gregory J.*Nicdao, PlacidoWhite, Roderick
Durable Medical EquipmentGuam Med*Health Services of the Pacific*Healthcare Specialties*Isla Home Infusion, Inc.Medquest Medical Supply
Home Health CareGuam Visiting Nurses*Health Services of the Pacific*Isla Home InfusionParadise Home Care
LaboratoryDiagnostic Laboratory Services& Bio Path*- American Medical Center*- Dededo Polymedic Clinic*- Express Care Health & Skin Care*- GITC Bldg*- Guam Adult & Pediatric Clinic*- Guam Medical Health Care Center*- Guam Medical Plaza*- IHP Medical Group*- PeMar Place*- Sagan Amot Pharmacy*- The Doctor’s Clinic*- Young Chang, M.D.*
Mental HealthAguon, RishaAquino, JoBethBaleto, JesseBaza, Joleen
Baza, LisaBellis, KirkBordallo, SandraChargualaf, MelissaCristobal-Lujan, HopeGuilliot, RosemarieHunterspeaks OrganizationKallingal, GeorgeLeitheiser, AndreaLizama, TriciaNatividad, LisaLindaPangelinan, RusellPerez, LilliRapadas, JuanRosario-Sanchez, KatrinaSantos, JamelaSwaddell, JoanTolentino, Doris
OpticalAgahan OpticalFHP Vision Center*Garcia OpticalIdeal OpticalIdeal Vision CenterLombard Health*New 20/20 Vision CenterSeventh Day Adventist Eye Clinic*Vision Express
Physical TherapyBright, KimCampos, LeonardChan, KeithChong, Dae-IIClaros, RyanGolez, Rolan*Guam Regional Medical City*Health Services of the Pacific*Kim, Justin*O’Connor, ShannonPanepucci, ChristopherPagaduan, MarcSantos, Isaias*Sibug, Mary AnnS.O.A.R. Physical Therapy
RadiologyGuam Medical Imaging Center*Guam Radiology Consultants*MDX Imaging*Pacific Radiology, Inc.*The Doctor’s Clinic*
Sleep CenterGuam Sleep Center*Pacific Sleep CarePacific Sleep Center
Speech PathologyDuenas, Nicole
Guam MemorialHospital Authority
Guam RegionalMedical City
Adult Health Care Clinic*American Medical Center*American Pediatric Clinic, LLCBlue Ocean Medical GroupByungsoo Kim, M.D.*Cancer Center of Guam, LLP*Central Medical Clinic*Center for Women's HealthDededo Polymedic ClinicEvergreen Health CenterExpress Care Health &Skin Care CenterGuam Adult & Pediatric ClinicGuam Behavioral Health &Wellness Center*Guam Dermatology InstituteGuam Dialysis Center*Guam E.N.T., LLC*
Guam Foot Clinic*Guam Hearing Doctors*Guam Medical CareGuam Medical Health Care CenterGuam Medical Imaging Center*Guam Orthopedic Clinic*Guam Radiology Consultants*GRMC Specialty Care Center*Guam SDA Clinic*Guam Sleep Center*Guam Specialist Group, PLLC*Guam Surgical Group*Guam Surgicenter, LLC*Guam Urology, LLC*Hagatna MED Clinic*Harmon PediatricsHealth Partners, LLC*Health Services of the Pacific*
Hepzibah Family Medicine Clinic*Isla PediatricsIsland Cancer Center*Island Eye Center*Island Foot Specialists*Island Surgical Center*Latte Stone Cancer Care*Leopoldo Arcilla, M.D.*Lombard Health*Marianas Footcare Clinic*Marianas Physicians GroupMDX Imaging*Micronesia Medical andAnesthesia Assoc., PLLC*MPG Pediatrics, PCNorthern RegionCommunity Health CenterOlivia Cruz, M.D.
OmniHealth Wound Care & Hyperbaric MedicineOne Love PediatricsPacific Cardiology Consultants*Pacific Hand Surgery Center*Pacific Medical Group*Pacific Radiology, Inc.Pacific Retina Group, LLC*Pacific Retina Specialists*Pacific Sleep CarePacific Sleep CenterPediatric & Asthma Clinic, PCRenal Centers of Guam*Romeo Samonte, M.D.*Sagua ManaguSDA Wellness CenterSouthern RegionCommunity Health Center
St. Anthony’s ClinicSt. Lucy’s Eye Clinic*The Doctor’s Clinic*The Neurology Clinic*The Pediatric and Adolescent ClinicThe Weingarten Institutefor Neuroscience*The Women’s ClinicThomas Shieh, M.D.Tumon Kidney Center*Tumon Medical O¥ceTumon Pediatric ClinicU.S. Renal CareFinegayan Dialysis*U.S. Renal Care Sinajana Dialysis*United Family Medical CenterYoung Chang, M.D.
In-Area Hospitals

Airfare Benefit
This benefit applies to our Center of Excellence Network only. Pre-certification and Pre-approval is required.
• The member needing care• An escort to provide assistance• A medical escort, if medically necessary
When certain critical conditions occur, you may qualify for round trip airfare to include:
Air Ambulance Discount
Air Ambulance Carrierand Plan approval required.
Certain qualifying conditions apply.
50% OFFAir Ambulance
Services!
$500 Travel Benefit
To be applied toward the cost of either (a) round trip airfare between Guam and Manila, Philippines or Taiwan; (b) ground transportation between the airport and the hospital or; (c) lodging in Manila or in Taiwan.
The following requirements apply:
• Calvo’s SelectCare will reimburse members up to the $500 allowance under this travel benefit.
• One time, per member, per year.
• For pre-authorized, specialty care visits, consultations, treatments and hospitalization at participating providers in the Philippines. Applicable only to approved referrals for conditions not treatable on Guam.
• Excludes emergencies, Preventive Services/Executive Check-ups, home health, hospice, maternity and dental-related services.
• Cannot be used in conjunction with the Airfare Benefit.
• Members are responsible for making their travel arrangements. Members are also responsible for any transportation and lodging expenses in excess of $500 and any penalties/fees incurred due to member changes.
Calvo’s SelectCare on the Web
Members can get information and access via the internet:
• View Claims Information
• Find a Provider
• Look through your Benefits
• Review your Member Handbook
• View the Summary of Benefits Coverage
• View your digital member card on your device
Visit calvos.net today!
• Stay on top of medication refills• Show your doctor exactly what medications you are taking• Pull up your medication history anytime• Learn about medication side e�ects & interactions and much more• Compare drug prices• On-the-go access to your personalized health information
The OptumRx Mobile App isdesigned for wellness on-the-go
Download the app to take advantage ofthe benefits your pharmacy plan o�ers
Prescriptions Drug costs add up.Our mail service pharmacy can helpyou save money.The convenient and cost-e�ective wayto get your prescriptions filled!
Low Cost Mail-Order Prescription
This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.13

Calvo’s SelectCare on the Web
Members can get information and access via the internet:
• View Claims Information
• Find a Provider
• Look through your Benefits
• Review your Member Handbook
• View the Summary of Benefits Coverage
• View your digital member card on your device
Visit calvos.net today!
• Stay on top of medication refills• Show your doctor exactly what medications you are taking• Pull up your medication history anytime• Learn about medication side e�ects & interactions and much more• Compare drug prices• On-the-go access to your personalized health information
The OptumRx Mobile App isdesigned for wellness on-the-go
Download the app to take advantage ofthe benefits your pharmacy plan o�ers
Prescriptions Drug costs add up.Our mail service pharmacy can helpyou save money.The convenient and cost-e�ective wayto get your prescriptions filled!
Low Cost Mail-Order Prescription
This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail. 14

Wellness and Fitness
Our wellness programs provide a very dynamic and rewardingopportunity for our members to improve their lifestyle and become healthier.
Healthy Coaching: Wellness Classes
Health Risk Assessment
• Get reports uncovering risks you may not know about• Identify health concerns that need your attention• Find out your next steps to getting and staying healthy• Share your reports with your doctor
• Classes are on a First-Come, First-Served Basis
• Must present Calvo’s SelectCare identification card at reception area
FREE to all Calvo’s SelectCare Members!
For more information, please contact Customer ServicePhone: 671-477–9808 Email: [email protected]
Have fun and invigorate your body with one of our many fitness classes. With classes like Zumba, Hip Box, Kids Kickboxing, and Water Aerobics, you’re guaranteed an exciting workout. Designed to suit all ages and abilities, all classes are delivered by high-quality, professionally certified instructors.
You could be at risk for cancer or heart disease. Do you know how to reduce this risk? Health Risk Assessments are an easy way to discover your potential risks.
Go to calvos.net and take our simple, secure, online health assessment. All answers are confidential. See questions about your health habits and history.
Programs at 50% Discount:Newstart, Seven-day Detox,7-Day Shape Up
Free Programs: Wellness Consultation,Diabetes Management Program, Stop Smoking, Childbirth Preparation ClassFree classes on a first come, first served basis!
Some programs require fees and/or
co-pays and pre-approval
by plan
This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.15

Health and Wellness Rewards
Take your Health Risk Assessment on
our website www.calvos.net
Contact your primary care physician to schedule your
USPSTF Exam
Complete our Deductible/Reimbursement
form online and attacha copy of your lab resultsto the form and submit
to our o�ce.
Register with one of our wellness partners and complete the program
Once you’ve completed the program, complete our
Deductible/Reimbursement form online and attach
certificate of completionand submit to our o�ce.
Enroll with one ofour fitness partners
Complete our Deductible/Reimbursement form online and attach gym
enrollment, receipt of payment, and submit
to our o�ce.
Subscribers and spouses/co-habiting partners (18 years or older) can participate in multiple wellness incentive programs that will allow them to earn up to a maximum of $100 per member for the benefit year by completing any of the following actions:
Incentive amounts will be calculated 60 days after the end of the policy or contract period or year, and payment will be made within 30 days after the calculation date. Members must complete a claim reimbursement form and submit to Calvo’s SelectCare along with proper documentation in order to claim benefit. Services must be provided by a participating provider.
• Complete the online Health Risk Assessment Completion of the online HRA is a requirement to be eligible for any wellness rewards.
• Get an annual USPSTF Exam
• Complete a Health Management Program with a participating Wellness Provider
• Gym enrollment with one of our Fitness Partners
Fitness Partners
CustomFitness
$50 a MonthNo Enrollment Fee!
AniguaMon-Fri | 5:30am-7:30pm
Saturday | 6am-12pmSunday | 7am – 11am
Tel: 989-0436
ParadiseFitness Center
$25 a MonthNo Enrollment Fee!
HagåtñaMon-Thur | 4am-10pm
Friday | 4am-9pmSaturday | 7am-5pmSunday | 7am-12pm
Tel: 475-2100/1
DededoFriday | Open til 9pm
Sat and Sun | 7am-7pmOPEN 24 HOURS
Monday thru ThursdayTel: 635-2100/1
SynergyStudio
$20 per monthNo Enrollment Fee
HagåtñaMonday-Friday:
5am-8am and 4pm-8pmSaturday | 8am-12pm
Tel: 472-9642
East AganaMon-Thur | 6pm-9pm
Every Saturday | 8am-12pmEvery Sunday | 9am-12pm
Tel: 635-2100/1
UnifiedFitness
$50 a MonthNo Enrollment Fee!
TamuningMon-Thurs | 5:15am-8:15pm
Friday | 5:15am-7:15pmSaturday | 7:15am-1:00pm
Sunday | ClosedTel: 969-8641
STEELAthletics
$40 per monthNo Enrollment Fee
TamuningMonday-Friday:
5:30am-1pm and 4pm-9pmSat & Sun | 6am-11am
Tel: 922-8888
Discounted Membership forJudiciary of Guam Subscribers and Spouses/Co-habiting Partners
This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail. 16

Class 1: EE (Employee)
Class 2: EE and Spouse
Class 3: EE and Child(ren)
Class 4: EE and Family
$1.25
$5.39
$6.23
$8.25
$56.04
$116.07
$89.94
$161.44
$3.64
$17.94
$14.68
$24.03
Bi-Weekly Rates
FY2021 Insurance Rates
This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.17

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.
What do I need to do to schedule an appointmentat a Participating Provider o-island, including Philippines?Contact Customer Service to coordinate your appointment dates and travel dates at least 2 weeks before your preferred travel date. Please provide to Calvo’s SelectCare a copy of your Referral for services along with your preferred travel dates. We recommend that you do not purchase your ticket until your appointment dates are set. Also, allow more time to arrange appointments during high demand seasons such as Summer, Christmas and Spring break.
When is Pre-Certification (prior approval) of a service or procedure required?A Pre-Certification is required when your physician requests, for you, services such as diagnostic procedures, home health care, physical therapy, durable medical equipment, Brand name drugs not listed in the Drug Formulary or Specialty Drug list. Refer to the “List of Procedures & CPT Codes requiring Pre-Certification” section in your member handbook.
How long does it take to receive a reimbursement for a claim I filed?If you submitted all required documentation, as indicated on the “Completing your Deductible / Reimbursement Claim Form” section in your member handbook, your claim will be processed within 10-12 working days for claims from local providers or 20-30 working days for claims from O�-island/Foreign providers. You will receive a reimbursement or an Explanation of Benefits in the mail.
Why am I receiving a bill from the lab for my Annual Examlabs that should be covered at 100%? What Preventive servicesare covered by the plan?The plan covers Preventive labs in accordance with the U.S. Preventive Service Task Force Recommendations A and B. You can obtain a list of recommended services in the Additional Resources section on our website at www.calvos.net.
Will the plan pay for my lodging and transportation when I go to a Participating Provider o-island, including Philippines?Lodging and transportation are not covered by the plan with the exception of those benefits specifically allowed by the $500 Travel Benefit and the AirFare Benefit. These two benefits also have certain limits and conditions.
How do I know if my prescription medication is covered by the plan?Medications covered by Calvo’s SelectCare are listed in our Prescription Drug Formulary in the Additional Resources section on our website at www.calvos.net. Coverage or reimbursement for prescription drugs purchased outside of the service area is limited to a 30-day supply.
Can other individuals, such as family members, including the subscriber of my plan, obtain information on my Health Insurance account? Your privacy is our priority. The plan will not release information to individuals not authorized on your account. You can obtain the HIPAA Privacy Authorization form in the Additional Resources section on our website at www.calvos.net. Note that authorization is limited and does not include disclosure of your personal claims information.
What if my member ID card is missing or stolen?Please call us at 477-9808 or email [email protected] and request for a replacement card. You should receive it in the mail within 2 weeks.
Up to what age can I cover my dependent child in my plan?Insured parents will be allowed to keep their children on their health plan until age 26.
How do I find Participating Providers in my plan network?You can refer to your Calvo’s SelectCare member handbook for a list of network providers. If you do not have a member handbook, you can
retrieve it on our website at www.calvos.net. Please note that not all plans have access to the same provider network.
How can I add my newborn child to my insurance plan?You must submit your child’s birth certificate along with a completed Enrollment/Change of Status form within 30 days from the date of birth. You can obtain an Enrollment/Change of Status form on our website at www.calvos.net. If you miss the 30-day window, you will have to wait until next Open Enrollment to add your child.
What is needed to file a Deductible / Reimbursement claim?Please refer to the “Deductible/Reimbursement Request Form” in the Additional Resources section on our website at www.calvos.net. All required information and documentation stated on the Form must be provided in order for the plan to accept, review and reimburse your claim.
Medicare Part A & B are my Primary insurance, am I liablefor paying my Medicare deductible and/or co-payment?How about my Medicare D deductible and/or co-payment?Your plan will cover the cost of your Medicare A & B deductible and/or co-payment, but you may still be liable for your Medicare D deductible and/or co-payment depending on your plan.
How long is a standard Preventive Exam at St. Luke’sMedical Center or The Medical City (TMC) in Philippines?For patients below 50 years old, you will only need up to 3 days to complete the Exam. The initial Exam procedures will only take a few hours and 3 days later, when your results are available, a Wellness physician will discuss them with you. For patients 50 years old and above, you will need up to a week if additional procedures must be completed, such as a Colonoscopy.
What does the plan cover if I want to have an “Executive Check-up” package oered by St. Luke’s Medical Center or The Medical City (TMC)?The plan will cover only the costs of the items included in the U.S. Preventive Service Task Force Recommendations A and B. You will have to pay for the excess cost of the package you select.
How can my child attending college in the U.S.establish a Primary Care Physician?We have contracted with the UnitedHealthcare PPO network to extend services to children attending college in the U.S. Mainland. For access, go to the UnitedHealthcare website at http://us1.welcometouhc.com/home, choose a provider under “Option PPO”, and advise us of provider’s name so we can issue a verification and authorization to access the provider.
Do I have to notify the plan if I have an Emergency o-island?Yes, in order for the plan to cover your bona fide Emergency service, you will have to notify us within 48 hours of an Emergency. Failure to notify the Plan will result in a denial of benefits.
How much money should I bring when seeking treatment at a Participating Provider o-island, including Philippines?Please bring enough money to cover your remaining deductible and out-of-pocket expenses for the plan year and remember to consider costs for lodging, food and transportation in your chosen area. Please refer to “Your Payment Responsibilities” section in your member handbook for additional information.
How long should I plan on staying when seeking treatment at a Participating Provider o-island, including Philippines?For basic, outpatient procedures, you should plan to stay for at least a week. For more invasive procedures that require a longer recovery period or inpatient admission, you should plan to stay at least 2 weeks. However, we recommend that you consult your physician for your particular case.
Frequently Asked Questions
18

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.
Five Healthy ReminderTips:•Practiceselfcareandgetyourannualcheckup•Eatcleanbyconsumingreal,wholefoods•Exercisebychoosingsomethingfun•Get7–8hoursofsleeppernight•ThinkPositive!Startoffyourdayonapositivenote
Thank you for choosing Calvo’s SelectCareHealthcare that’s always there for you!
19
Notes

This handbook is designed to provide information about your Calvo’s SelectCare plan.In the event of a discrepancy between this Handbook and the contract, the terms of the contract will prevail.

20200903_JudiciaryPresBook_FY2021
Palau JR Professional Bldg., Suite 2P.O. Box 10248Koror, Palau 96940Phone: (680) 488-7222Fax: (680) 488-7333
Web calvos.net
Saipan Oleai Center Bldg., San JoseP.O. Box 500035Saipan, MP 96950-0035Phone: (670) 234-5690/9Fax: (670) 234-5696
Guam 115 Chalan Santo PapaP.O. Box FJHagåtña, Guam 96932Phone: (671) 477-9808Fax: (671) 477-4141
Philippines 5th Floor, First Life Center174 Salcedo Street, Legaspi VillageMakati City, PhilippinesPhone: (632) 759-2871/813-1989Fax: (632) 759-3126
St. Luke’sMedical Center
Global City
Rm. 1008 10th FloorMedical Arts Building32nd St. Bonifacio Global CityTaguig City, 1112 PhilippinesPhone: (632) 555-0443/0448Fax: (632) 555-0438
St. Luke’sMedical Center
Quezon City
Rm. 716 7th Floor, North Tower Cathedral Heights Building ComplexSt. Luke’s Medical Center Compound#279 E. Rodriguez Sr. Avenue,Quezon City, PhilippinesPhone: (632) 413-1312Fax: (632) 413-5721
The Medical CityPasig City
Business Center, 9th FloorThe Medical City, Ortigas CenterPasig City, Philippines Phone: (632) 650-0589
Judiciary of GuamOpen EnrollmentFiscal Year 2021
Administered by
Office locations to better serve you










![t4JbÃBBQ by [57'Lx;ä] GUAM PLAZA FIESTA RESORT …ƒBBQ by [57'Lx;ä] GUAM PLAZA FIESTA RESORT 45 PACIFIC ISLANDS P.I.C. ROYAL ORCHID GUAM HOTEL HILTON GUAM GUAM REEF & ONWARD SHERATON](https://img.pdfslide.us/doc/110x75/5afde0387f8b9a256b8c45ee/t4jbbbq-by-57lx-guam-plaza-fiesta-resort-by-57lx-guam-plaza-fiesta-resort.jpg)